2-vni_na_icc_lr_2011
DESCRIPTION
z cgaxcsgaxcgsacgxasTRANSCRIPT

Non-Invasive Positive Pressure
Ventilation in Heart Failure Patients:
For Who, Wy & When?
Quais os doentes com insuficiência cardíaca
que beneficiam de ventilação não-invasiva?
L u i s R a p o s o
U N I C A R V | H o s p i t a l d e S a n t a C r u z | C H L O
REUNIÃO CONJUNTA DOS GRUPOS DE ESTUDO
DE CUIDADOS INTENSIVOS CARDÍACOS E DE
FISIOPATOLOGIA DO ESFORÇO E
REABILITAÇÃO CARDÍACA
O L H Ã O | 2 7 e 2 8 d e J a n e i r o 2 0 1 2

Increasing prevalence of chronic kidney dysfunction
NIV has been has an important clinical role in
both acute decompensate congestive HF & in
chronic stable patients with BDS
Acute/decompensated heart failure (mostly ALE)
Basic pathophysiology of cardiogenic acute lung edema
Beneficial effects of positive pressure ventilation
CPAP vs BiPAP vs Standard of Care
Chronic/stable heart failure
Cardio-respiratory interactions & BDS in chronic HF patients
Potential benefits of positive pressure ventilation
Non-Invasive Positive Pressure Ventilation
Definition
Basic principles & practical setup and hints

Increasing prevalence of chronic kidney dysfunction
Acute/decompensated heart failure
Basic pathophysiology of cardiogenic acute lung edema
Beneficial effects of positive pressure ventilation
CPAP vs BiPAP vs Standard of Care
Chronic/stable heart failure
Cardio-respiratory interactions & BDS in chronic HF patients
Potential benefits of positive pressure ventilation
Non-Invasive Positive Pressure Ventilation
Definition
Basic principles & practical setup and hints
NIV has been has an important clinical role in
both acute decompensate congestive HF & in
chronic stable patients with BDS

Increased hospital stay and costs
Increased mortality
Increasing prevalence of chronic kidney dysfunction
Non-Invaive positive pressure ventilation (NPPV) is a way
of assuring positive pressure in the airways throughout
the entire respiratory cycle without intubation
Trauma to the oro-pharynx and airway
Excessive hypotension
Arrythmia
Inability to cough: accumulation of respiratory debris
Nosocomial pneumonia
Dysphonia, granuloma formation…
NIV AVOIDS the risks associated with ETI

Increasing prevalence of chronic kidney dysfunction
Non-Invaive positive pressure ventilation (NPPV) is a way
of assuring positive pressure in the airways throughout
the entire respiratory cycle without intubation

Poulton EP, Lancet 1936;228:981-983
NPPV is not a new concept: it’s use began
during the first half of the 20th century

Increasing prevalence of chronic kidney dysfunction
Non-Invaive positive pressure ventilation (NPPV) is a way
of assuring positive pressure in the airways throughout
the entire respiratory cycle without intubation
Bi-level Positive Airway Pressure
(IPAP + EPAP)
Continuous Positive Airway Pressure
(CPAP)
Pressure regulated volume ventilation

Increasing prevalence of chronic kidney dysfunction
Non-Invaive positive pressure ventilation (NPPV) is a way
of assuring positive pressure in the airways throughout
the entire respiratory cycle without intubation
Continuous Positive Airway Pressure
The most commonly used method: minimal training
Relatively simple, “portable” devices
Not “true” mechanical ventilation, as inspiratory
effort depends entirely on the patient
Positive pressure produced by a unidirectional valve:
may use a “fan” or O2 (Boussignac) to generate
flow/pressure
Mixture in the facial mask may facilitate
re-inspiration of CO2 (caution in hypercapneic pts!)

Increasing prevalence of chronic kidney dysfunction
Non-Invaive positive pressure ventilation (NPPV) is a way
of assuring positive pressure in the airways throughout
the entire respiratory cycle without intubation
Less commonly used: requires more extensive
training, team experience & more expensive
equipment
Usually employs typical ICU ventilators
Helps inspiratory effort with patient triggered
preset pressure during inspiration (IPAP)
Theoretically “more physiological”
Allows higher tidal volumes (potential advantage in hypercapneic/acidotic pts!)
Bi-level Positive Airway Pressure

Increasing prevalence of chronic kidney dysfunction
Acute/decompensated heart failure
Basic pathophysiology of cardiogenic acute lung edema
Beneficial effects of positive pressure ventilation
CPAP vs BiPAP vs Standard of care
Chronic/stable heart failure
Cardio-respiratory interactions & BDS in chronic HF patients
Potential benefits of positive pressure ventilation
Non-Invasive Positive Pressure Ventilation
Definition
Basic principles & practical setup and hints
NIV has been has an important clinical role in
both acute decompensate congestive HF & in
chronic stable patients with BDS


Increasing prevalence of chronic kidney dysfunction
Pulmonary Edema is a frequent manifestation
of Heart Failure & halves a dire prognosis
Available at
http://www.escardio.org/guidelines-surveys/ehs/heart-failure/Documents/EHS_HFII_MainPublication.pdf
30 European countries;
133 centres;
3580 pts

Increasing prevalence of chronic kidney dysfunction
Positive pressure improves ventilation by
counteracting the pathophysiological pathways
in acute cardiogenic lung edema
Opens flooded & collapsed alveoli
Increases functional residual capacity
Decreases “dead space”
Decreases intra-pulmonary shunt
Increases tidal volume

Increasing prevalence of chronic kidney dysfunction
Kelly et al. Eur Heart J 2002;23:1379-1386
Randomised controlled trial of continuous positive airway pressure and
standard oxygen therapy in acute pulmonary oedema; effects on plasma
brain natriuretic peptide concentrations.
Positive pressure improves ventilation by
counteracting the pathophysiological pathways
in acute cardiogenic lung edema
CPAP
O2

Increasing prevalence of chronic kidney dysfunction
Positive pressure improves ventilation by
counteracting the pathophysiological pathways
in acute cardiogenic lung edema

Increasing prevalence of chronic kidney dysfunction
Raposo L, Rev Port Cardiol, 2003; 22 (Supl III): III-102 (Abstract)
Positive pressure improves ventilation by
counteracting the pathophysiological pathways
in acute cardiogenic lung edema

Increasing prevalence of chronic kidney dysfunction
Positive pressure ventilation has
favorable effects on the loading conditions
of the failing Left Ventricle

Increasing prevalence of chronic kidney dysfunction
23 trials
1985-2003
Evidence from RCTs and Meta-analysis
strongly favors the use of NPPV for the
treatment of acute decompensated HF/APE

Despite theoretical advantages, overall, BiPAP
does not seem to bee superior to CPAP
Critical Care 2006, 10:R69 (doi:10.1186/cc4905)
Available at: http://ccforum.com/content/10/2/R69

Despite theoretical advantages, BiPAP dit not prove
to be superior to CPAP in hypercapneic patients
Critical Care 2006, 10:R69 (doi:10.1186/cc4905)
Available at: http://ccforum.com/content/10/2/R69
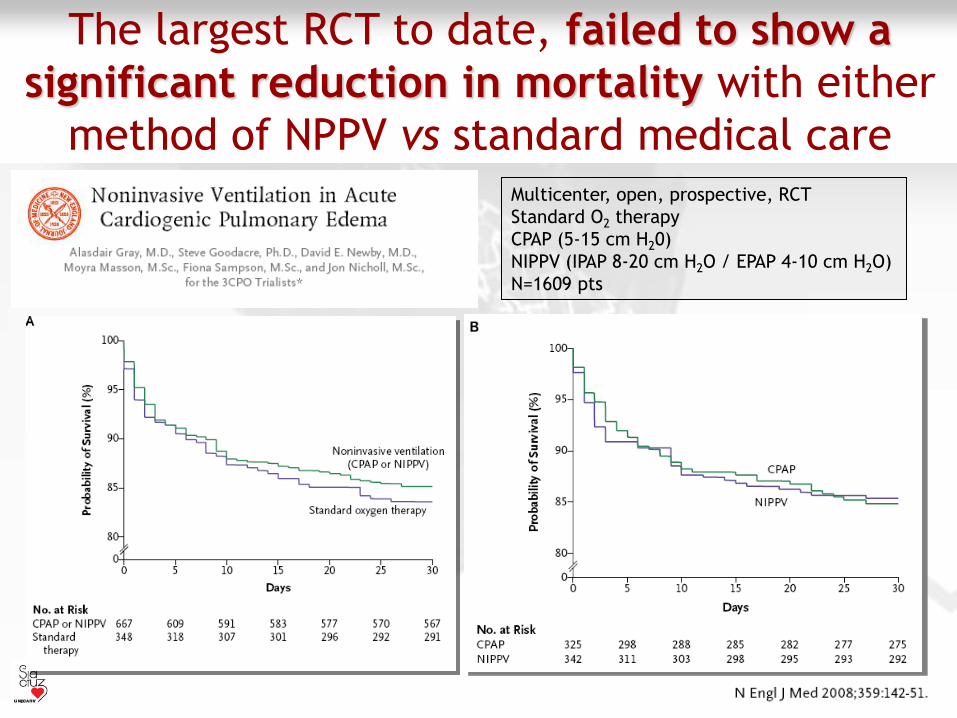
The largest RCT to date, failed to show a
significant reduction in mortality with either
method of NPPV vs standard medical care Multicenter, open, prospective, RCT
Standard O2 therapy
CPAP (5-15 cm H20)
NIPPV (IPAP 8-20 cm H2O / EPAP 4-10 cm H2O)
N=1609 pts

Increasing prevalence of chronic kidney dysfunction

147.362 records, with 114,756 (78%) cases of ADHF admitted from the ED
Ventilation in 2,430 pts (6.5%) - 1,760 (72.4%) NIV & 670 (27.6%) ETI without an NIV trial.
1,688 (95.9% of NIV pts) managed only by NIV (NIV success)
72 (4.1% of NIV) failed NIV and subsequently received ETI (NIV failure).
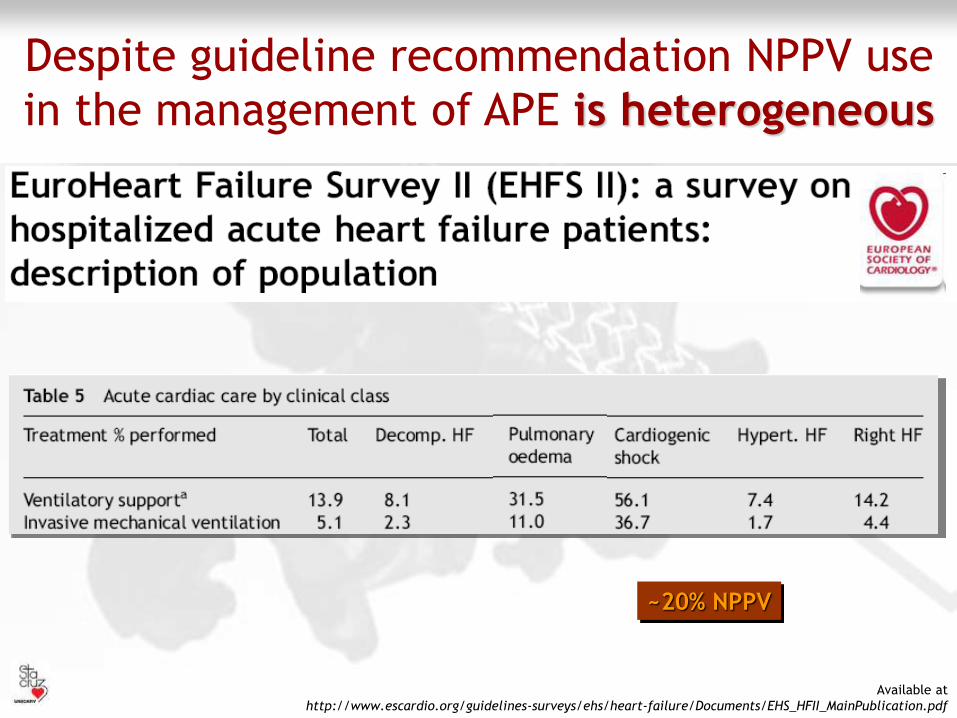
Despite guideline recommendation NPPV use
in the management of APE is heterogeneous
Increasing prevalence of chronic kidney dysfunction
Available at
http://www.escardio.org/guidelines-surveys/ehs/heart-failure/Documents/EHS_HFII_MainPublication.pdf
Despite guideline recommendation NPPV use
in the management of APE is heterogeneous
~20% NPPV

When to use & how to do it?
Indications for Noninvasive Ventilation Indications
• Inadequate response to initial standard therapy
• At risk for endotracheal intubation
• Respiratory rate ≥ 30
• Persistent 02 saturation ≤ 90% or PaO2/FiO2<200 on >4 L/min oxygen
• Mild hypercapnia (CO2<45 mmHG) or acidosis (ph<7.3) - preferably IPAP?
• Sense of respiratory muscle fatigue
Contraindications
• Lack of training
• Apnea & Hemodynamic instability
• Inability to protect the airway and Uncontrollable vomiting
• Abnormal facial anatomy
• Recent GI or upper airway surgery (< 7 days)
• Altered mental status or uncooperative and inability to tolerate the mask
• Need for immediate ETI due to worsening instability
• Very severe obstructive airway disease

When to use & how to do it?
Continuous Positive Airway Pressure
• Start with 5-7.5 cm H20
• Increase in increments of 2 cm H20, as tolerated and indicated
• FiO2 >40%
Bi-Level Positive Airway Pressure / Noninvasive Pressure Support Ventilation
• Initial inspiratory pressure of 8–10 cm H20
• Increase in increments of 2–4 cm H20 (Max ~20 cm H20) aiming at TV>7ml/Kg
• Initial expiratory pressure of ~4-5 cm H20
• Maximum inspiratory pressure is 24 cm H20 and expiratory pressure 20 cm H20
• FiO2 >40%
Noninvasive Ventilation Settings

When to use & how to do it?
Improvement Criteria
• Heart rate <100 bpm
• Respiratory rate <30/min
• Ability to maintain SpO2>90% on spontaneous breathing FiO2 <40-50% (mask)
• Improvement in dyspneia, without use of ancillary muscles
Factors associated with the success of noninvasive ventilation
• Patient-ventilator synchrony /acceptance of the technique by the patient
• Glasgow coma score over 9 & APACHE II score < 21.
• Few secretions
• No pneumonia
• baseline Hypercapnia and initial pH above 7.1
• Good response in the 1st hour of T/ with correction of acidosis & hypoxemia
• Arterial hypertension at baseline
Monitoring and withdraw

Increasing prevalence of chronic kidney dysfunction
Acute/decompensated heart failure
Basic pathophysiology of cardiogenic acute lung edema
Beneficial effects of positive pressure ventilation
CPAP vs BiPAP vs Standard of care
Chronic/stable heart failure
Cardio-respiratory interactions & BDS in chronic HF patients
Potential benefits of positive pressure ventilation
Non-Invasive Positive Pressure Ventilation
Definition
Basic principles & practical setup and hints
NIV has been has an important clinical role in
both acute decompensate congestive HF & in
chronic stable patients with BDS

Sleep Disordered Breathing (SDB) is highly
prevalent in chronic HF patients and is associated
with poor QOL and increased mortality
80% prevalence

Sleep Disordered Breathing (SDB) is highly
prevalent in chronic HF patients and is associated
with poor QOL and increased mortality
Impact of CPAP Treatment
Adjusted HR 2.9 (95% CI 1.1-3-5; p=0.0023)
296 CHF patients
Median LVEF=33%
In-lab polysomnography

In Chronic HF patients with SDB, treatment effect
of nocturnal CPAP is higher in those with the
central type of sleep apnea – The CANPAP Trial
258 HF patients with Central sleep apnea (nº episodes of apnea/hypopnea 40±16 per hour of sleep)
Ejection fraction 24.5±7.7%
FUP 3 months
Increase in the 6 min walk test distance
Decrease in norepinephrine
No benefit in hard clinical endpoints (mortality & transplant rate)

In Chronic HF patients with SDB, treatment effect
of nocturnal CPAP is higher in those with the
central type of sleep apnea – The CANPAP Trial
HR 0.37 (95% CI 0.14-0.96; p=0.043)
vs control (nonCPAP pts)

Aorta
Conclusions & Take-Home messages
NPPV provides excellent clinical results when proper patient selection
is accounted for and treatment is initiated early in an adequate
“window of opportunity” by an experienced team
It can dramatically improve ventilation and cardiac performance
(except in severe diastolic dysfunction, hypovolemia or severe LV systolic failure)
NIV is associated with highly significant reductions in the need for ETI
(up to 55%!) and may reduce early mortality
Either technique appears equally effective, but CPAP is cheaper, easer
to use and requires less training
There is no clear cut evidence that NPSV actually increases the risk of
new myocardial infarction, but caution is advised when treating
acute MI or severe CAD patients (increase in LV transmural pressure….)