2 hour surgical complications
DESCRIPTION
SYSTEMIC HOST FACTORS What Works in a Private Practice Setting and What Doesn’tTRANSCRIPT

Complications: How to Treat and Avoid
PART 1- SYSTEMIC HOST FACTORS
What Works in a Private Practice
Setting and What Doesn’t

Disclosure
• Full time private practice
• Not employed by any company or University
• Have not received any personal grants
• Have received sponsorship from multiple
Dental companies for seminar related activities
• Utilize multiple implant systems

“Surgical Complications”
Seminar Objectives:
• Utilize an “Evidence Based Approach”

Evidence-based Dentistry
Clinical Judgment
Patient
Values
Evidence-
based Treatment
Best Available Evidence

“Surgical Complications”
Seminar Objectives:
• Utilize an “Evidence Based Approach”
• Review complications reported in the literature
• Show complications in Private Practice settings
• Identify protocols and risk factors impacting on success
• Describe techniques that can minimize complications
• Demonstrate treatment to deal with complications
• Reveal the value of a Dental Implant Management
Software (DIMS) program, called “TRITON DIMS”

How to Cover the Material in 90 Minutes!
•“Bottom Line”
summaries
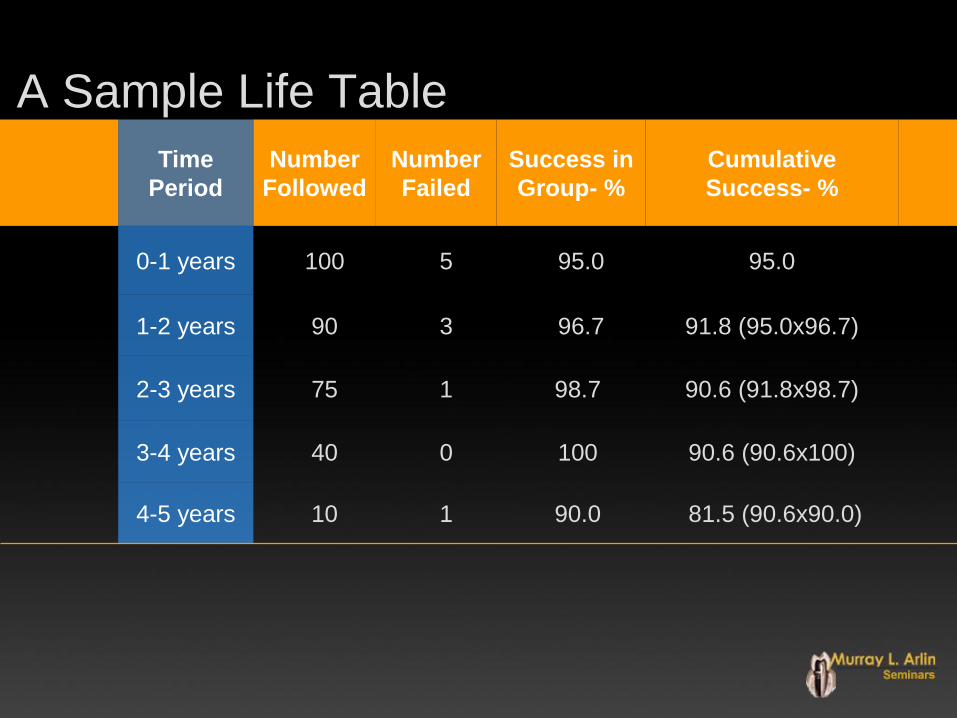
Time
Period
Number
Followed
Number
Failed
Success in
Group- %
Cumulative
Success- %
0-1 years 100 5 95.0 95.0
1-2 years 90 3 96.7 91.8 (95.0x96.7)
2-3 years 75 1 98.7 90.6 (91.8x98.7)
3-4 years 40 0 100 90.6 (90.6x100)
4-5 years 10 1 90.0 81.5 (90.6x90.0)
A Sample Life Table

Information Sources
• Published studies
• Clinical experience

Information Sources: Key publications
• Consensus Conferences /
Systematic Literature Reviews: • Esposito at al, Eur J Oral Sci 1998
• Goodacre et al, J Prosthet Dent, V. 90, #2, 2003
• Annals of Periodontology, J. Periodontol: V.8, 2003
• ITI Consensus Conference JOMI, V. 19, Supp. 2004
• Clin Oral Impl Res, December 2004
• EAO Consensus conference, Feb. 2006
• AO Consensus Conference (SSID), JOMI, V. 22, Suppl, 2007

Information Sources: Key publications
• Advantages of “Systematic
Literature Reviews”: • Stringent inclusion and exclusion criteria
• Interpretations scrutinized to minimize bias
• Data subject to intense statistical scrutiny
• “Meta-analysis” utilized when possible
• (combining data from several similar studies)
• ( see SSID, JOMI 2007;22 (suppl): 11-18)

State of the Science on Implant Dentistry: SSID-Concensus Conference
different evaluation groups
• Section I: Time to Loading
• Section II: Bone Augmentation
• Section III: Implants vs Teeth: Single
• Section IV: Implants vs Endodontic Treatment
• Section V: Prosthesis Type - Fully Edentulous
• Section VI: Prosthesis Type - Partially Edentulous
• Section VII: Smoking / Diabetes / Periodontitis
• Section VIII: Timing-Implant Placement Post Extraction

Published Studies: Applicability to Private Practice?
• All implants included?
• Only the best clinicians?
• Risky patients excluded?
• Risky procedures excluded?
• Statistical vs Clinical significance?
• Clinical protocols similar to private practice?

WHAT FOLLOWS ARE TWO
EXAMPLES OF POORLY
DESIGNED CLINICAL
STUDIES RESULTS ARE
MEANINGLESS

Branemark Implants
in Type IV Bone
• 2 stage surgical protocol
• Up to 5 year follow up
• 44% failure/maxilla (23/52)
• 37% failure / mandible (11/30)
- Jaffin and Berman, J. Periodontol 1991; 62:2-4
“recently, self-tapping fixtures were utilized.”
mixed conventional and self tapping-implants !
INVALID MIX OF IMPLANT TYPES

Branemark Implants
in the Posterior Maxilla
• Up to 12 year follow up
• 660 implants in 202 patients
• 99.4% success at 5 years
• 93.4% success at 10 years
- Bahat, Int J Oral Maxillofac Implants 2000
“if the implant did not arrest at full length under
a force of 40 Ncm, the implant was removed ”
PRIMARY STABILITY BEYOND WHAT YOU EXPECT IN PRIVATE
PRACTICE TO IMPROVE RESULTS !

Information Sources
• Published studies
• Clinical experience

Clinical Experience
• Decisions are partly based on clinical experience
• Procedures are often repeated if they work
• Procedures are abandoned if they don’t work
Private Practice Empiricism
• may not identify subtle variables impacting success!
Controlled Private Practice
• can identify variables applicable to private practices

Private Practice “CONTROLLED” Studies:
Challenges
• Commitment to time and cost
• Adherence to standardized protocols
• Thorough documentation
• recording / analysis / reporting
• Patient compliance (e.g. follow-up)

*Private Practice: Clinical Protocol
• Over 6,800 implants placed
• Local anaesthetic
• Aseptic surgical technique
• “Risky” patients included
• “Risky” protocols included
• Multiple implant designs
• Multiple restorative dentists
* Dr. Murray Arlin, full time Periodontal Practice

*Private Practice:
Implant Placement Protocols
• Standard (healed sites)
• Immediate extraction
• Early extraction
• Immediate replacement
• Delayed replacement
*Dr. Murray Arlin, full time Periodontal Practice

*Private Practice: Implant Systems
• Nobel Biocare (Replace)
• Zimmer (Screw-vent/Advent)
• Straumann ITI (TPS, SLA)
• Implant Innovations (3i)
• Bio Horizons
• Imtec (mini)
* Dr. Murray Arlin, full time Periodontal Practice

*Private Practice: Documentation
• All implants documented (over 6,800)
• Data entry on “Triton-DIMS”
• Relational data base
• User defined attributes
• User defined queries
• Reports eg. Life Tables
* Dr. Murray Arlin, full time Periodontal Practice

Assessing “Real Science”:
Poor Studies, Industry Ties
Taking Toll
Jayne Hamilton
California Dental Association Journal,
January, 2004, Vol. 32, #1
EXAMPLE OF CLINICAL STUDIES

EXAMPLE OF CLINICAL STUDIES
EXAMPLE OF CLINICAL STUDIES

• Comparison of TPS vs SLA
Straumann implants. A 9 year study
• Performance of TiUnite Replace
Nobel-Biocare Implants. A 5 year study
EXAMPLES OF ADDITIONAL
CLINICAL STUDIES
USING THE DATA BASE

Surgical Complications
Host
Factors
Systemic
Factors
Local
Factors
Contributing
Etiology Non Host
Factors
Operator
Related
Biomaterial
Related
(Based on Etiology)

Surgical Complications:
Host Factors
• Systemic
• Age / health • Previous periodontitis
• Smoking
• Genetics/Immunity
• Local
• Bone quality/quantity
• Excessive loading
• Poor plaque control
• Keratinized gingiva

Human Mesenchymal Cells (HMC)
in Bone Marrow
0
0.00001
0.00002
0.00003
0.00004
0.00005
0.00006
0.00007
0.00008
0.00009
0.0001
Newborn Teen 35 YRS. 50 YRS. 80 YRS.
% HMC
1/ 2,000,000 1/ 400,000 1/ 250,000
1/ 100,000
1/ 10,000

Host Factors: Contributing to Implant Failure
• Age has no apparent influence • 8 STUDIES SUPPORT THE ABOVE
• Smith et al., 1992, Jemt, T., 1993 Esposito et al., 1998
• Bragger et al., 2000, de Baat et al 2000, Becker et al., 2001
• Wagenberg and Froum, 2006, Hermann et al, 2006
• 3 STUDIES SUPPORT AGE IS A FACTOR Brocard et al,2000, Berge et al, 2000, Moy, P., 2005

8 years
FUNCTION
ELDERLY
PATIENT

ELDERLY PATIENT

Host Factors: Contributing to Implant Failure
• Insufficient evidence for:
• Malabsorption , Immunologic disorders
• Sjogren’s, Lupus, Lichen Planus
• Osteoporosis, Osteopenia
• Corticosteroids, Estrogen-HRT
• > failures Maxilla: Post Menopause-HRT
• *Diabetes (controlled?)
» Minsk et al, 1998 Snauwaert et al, 2000,
» Chuang et al, 2001, August et al, 2001, Moy et al, 2006
» Farzad et al 2002,* Kotsovillis et al, 2006, **SSID, JOMI 2007

Diabetes / Implants
(Review)
• Accepted 11 experimental and 8 clinical studies
• Not feasible to perform a meta analysis
• Experimental Studies: impaired bone healing
• Clinical Studies: no contraindication
if controlled
• “A Comprehensive and Critical Review of Dental Implant
Placement in Diabetic Animals and Patients”, Kotsovilis, Karoussis and Fourmousis, Clin Oral Impl Res, Oct. 2006

Exclusion Criteria for Implants
• Pregnancy
• Alcoholism
• Drug abuse
• Severe infection
• Uncontrolled Diabetes
• IV Bisphosphonate Tx.
• Metabolic bone disorder
• Renal failure
• Severe liver disease
• Current chemotherapy
• Severe radiation
• Psychiatric instability

Types of Bisphosphonates
• Alendronate: Oral (Osteoporosis)
• Tiludronate: Oral (Paget’s)
• Risedronate: Oral (Osteoporosis and Paget’s)
• Etidronate: Oral and IV (not common)
• Pamidronate: IV (Osteoporosis, Malignancy)
• Zolendronic Acid: IV (Malignancy)
• Hwang and Wang, Implant Dentistry, 2006

Bisphosphonates and Osteonecrosis
of the Jaws: Systematic Review
• Greatest risk: IV nitrogen containing Bisphosphonates (94%)
• IV: Multiple myeloma, skeletal metastatic carcinoma
• Oral: osteopenia and osteoporosis
• Oral administration: (cases reported as of March 2006)
• Risedronate (Actonel):12, Ibandronate (Boniva):1
• Aldronate (Fosamax):170= 0.7 in 100,000 cases (2 years)
• Woo, Hellstein and Kalmar, Ann Intern Med, 2006

Surgical Complications:
Host Factors
• Systemic
• Age/health
• Previous periodontitis
• Smoking
• Genetics/Immunity
• Local
• Bone quality/quantity
• Excessive loading
• Poor plaque control
• Keratinized gingiva

History of Previous Periodontitis: (Correlation with Implant Failure)
• Correlation with failure: case report (1990) • Malmstrom et al J Perio, 1990
• No strong correlation with failure (1995-2006)
• Nevins and Langer, J Periodontol., 1995
• Ellegaard et al, Clin Oral Impl Res, 1996
• Liljenberg et al, J Clin Perio., 1997
• Mengel et al., J Periodontol., 1996 & 2000
• Paknejad, A., COIR 2006,
• Correlation with > biological complications (1997-2006) • Ellegaard et al, Clin Oral Impl Res, 1997
• Polizzi et al, Clin Impl Dent Rel Res, 2000
• Brocard et al, JOMI, 2000, Hardt et al, COIR, 2002
• Karoussis et al, Clin Oral Impl Res, 2003 and 2004
• Rosenberg et al, JOMI, 2004, Baelum and Ellegaard, J Periodontol, 2004
• Mengel and Flores-de-Jacoby, J Periodontol, 2005
• Ellegaard et al, Clin Oral Impl Res, 2006, Roos et al, Clin Perio, 2006
• Paknejad, A., COIR 2006, Klokkevold and Han, SSID, JOMI, 2007

History of Previous Periodontitis: (Correlation with Implant Complications)
• 1 and 10 year exams,
ongoing periodontal care
• 8 “periodontitis” patients - 21
ITI implants (PCP)
• 45 “non-periodontal” patients
- 91 ITI implants (PHP)
• Higher failure rate and
Peri-implantitis in PCP
PCP PHP
Survival 90.5% 96.5%
Clinical
Success 81% 96.7%
Peri-implantitis 28.6% 5.8%
• Karoussis et al, Clin Oral Impl Res,V 14, #3, June 2003
“Long-term Implant Prognosis in Patients With and Without a history of
Chronic Periodontitis:A 10 year prospective study”
CHRONIC HEALTHY

History of Previous Periodontitis: (Correlation with Implant Complications)
• Private practice, 13 year study period
• 1,511 implants in 334 patients
• 151 compromised (PCP), 923 implants
• 183 healthy (PHP), 588 implants
• Higher Failures with PCP vs PHP
• “Early” Failures similar in both
groups
• “Late” Failures primarily the HA
group
PCP PHP
Overall Survival 90.6% 93.7%
HA Implant
Survival
81% 92.6%
• Rosenberg et al, JOMI, V 19, #6, 2004
“A Comparison of Characteristics of Implant Failure and Survival in Periodontally
Compromised and Periodontally Healthy Patients: A Clinical Report”
CHRONIC HEALTHY

History of Previous Periodontitis: (Correlation with Implant Complications)
• “The level of implant SUCCESS may be LESS for patients with a history of treated periodontitis”
• Success & survival cannot be predicted for untreated
• Complications may be more prevalent in the maxilla
• “periodontitis has to be considered a risk factor”
Klokkevold and Han, SSID, JOMI, 2007

Surgical Complications:
Host Factors
• Systemic
• Age/health
• Previous periodontitis
• Smoking
• Genetics/Immunity
• Local
• Bone quality/quantity
• Excessive loading
• Poor plaque control
• Keratinized gingiva

Implant Success:
Current smokers / Risk Factor
• Bain and Moy, JOMI 1993
• De Bruyn and Collaert, COIR, 1994
• Gorman et al, Impl Dent, 1994
• Duyck and Naert, Cl O Invest, 1998
• Sennerby and Roos, Int J Prosth, 1998
• Minsk et al, Comp Con Ed Dent, 1998
• El Askary et al, Impl Dent, 1999
• Wallace, R.H., Eur J Pr. Dent, 2000
• Ekfeldt et al, Clin Oral Impl Res, 2001
• Chuang et al, J Dent Res, 2001, 2002
• Vehemente et al, J Oral Impl 2002
• Berge et al, Clin Oral Impl Res., 2002
• Kan et al, J Prosth Dent, 2002
• Van Steenberghe et al, COIR, 2002
• Nociti et al, J Periodontol, 2002
• Goodacre et al, J Pr Dent, 2003
• Kourtis et al, Impl Dent 2004
• Karoussis et al, COIR, 2004
• Cesar-Neto et al, JOMI, 2005
• Moy et al, JOMI 2005
• Nitzan et al, JOMI, 2005
• Mundt et al, JOMI 2006
• McDermott et al, JOMI 2006
• Zabaras et al, Abst, COIR, 2006
• Wagenberg & Froum, JOMI, 2006
• Ellegaard et al, Clin Oral Impl Res, 2006
• Roos-Jansaker et al, J Clin Perio, 2006
• McDermott et al, JOMI, 2006
• Zabaras et al, (Abst), COIR, 2006
• Nozawa et al, (Abst), COIR, 2006
• Klokkevold & Han, JOMI, SSID, 2007
EVIDENCE IS OVERWHELMING

Implants # Placed # Lost % Lost
Non
Smokers 4,682 239 5%
Smokers 1,668 178 11%
Diabetics
1,053 93 9%
• J. Prost. Dent., 2003, Goodacre et. al.
9 Studies-Implant Loss: Smokers / Diabetes

3
4
1 2
PROGRESSIVE

3 Years Later
PROGRESSIVE
4
3 4 4

Smoking Risk Factor: Loose Trabecular Bone
(Pooled Data)
• 86.1%-Maxilla-Smokers
• 92.4%-Maxilla-Non Smokers
• 89.7%-Mixed Sites-Smokers
• 93.3%-Mixed Sites- Non Smokers
• Conclusion: “The effect of smoking may
not be as significant for good bone sites”.
Klokkevold and Thomas, SSID, JOMI, 2007

Smoking Risk Factor is
Dose Dependant
• Retrospective, 663 implants, 159 patients
• Survival of 91.8% at 120 months
• 96% mandible, 89% maxilla
• *Smokers-85%, Former-90.4%, Non-96.4%
• *Failure rates were Smoking dose dependant
• Mundt et al, JOMI, 2006, “Private Practice Results of Screw-Type Tapered
Implants: Survival and Evaluation of Risk Factors”

Implant Survival: Smoking Cessation
• Smoking Cessation May Decrease Implant Complications
• e.g. *1 week pre op, 8 weeks post op
• De Bruyn and Collaert, Clin Oral Impl Res, 1994
• *Bain, CA, JOMI 1996
• Cesar-Neto et al, JOMI, 2005
• Mundt et al, JOMI, 2006

Rough Surfaced Implants: Beneficial Effect with Smokers?
• 100% survival of Osseotite implants: posterior maxilla & mandible • Grunder et al, Comp Cont Educ Den, 1999
• *Less crestal bone loss with TiUnite vs Machined and most
pronounced differences in smokers (1.08mm vs 1.83mm) • Watzak et al, Clin Oral Impl Res, December 2006
• *Higher Survival: Osseotite vs Machined (98.7% vs 93.45%) • Bain et al, 2005, Meta Analysis
• Higher Survival: Osseotite vs Machined (96.3% vs 94.4%) • Wagenberg and Froum, JOMI, 2006
• Conclusion:
• Rough surfaces, e.g. TiUnite & Osseotite, may be beneficial
to smokers to reduce crestal bone loss & failures.

Surgical Complications:
Host Factors
• Systemic
• Age/health
• Previous periodontitis
• Smoking
• Genetics/Immunity
• Local
• Bone quality/quantity
• Excessive loading
• Poor plaque control
• Keratinized gingiva

The Nightmare Case!
Negative Genetic Factor?

First Stage

First Stage

3 Weeks Post

3 Weeks Post

7 Months Post Explant

First Stage (#2)

First Stage (#2)

3 Weeks Post (#2)

3 Weeks Post (#2)


3 Years in Temps 2 SURVIVED

1 Year Post Prosthetics

2 Years Final Prosthetics

2 Years Final Prosthetics

Surgical Complications
Host
Factors
Systemic
Factors
Local
Factors
Contributing
Etiology Non Host
Factors
Operator
Related
Biomaterial
Related
(Based on Etiology) Summary:

Summary: Host Systemic Factors
• No apparent significant effect:
• Age / Controlled Diabetes / Many systemic conditions
• Higher implant failure and complication rates with:
• Diabetes-uncontrolled (most studies)
• Post menopausal: on HRT (some studies)
• Previous and ongoing periodontitis
• May be more pronounced: long term , maxilla, very rough surfaces
• Smoking (most studies)
• Dose dependant, cessation helps
• Reduced failures with rough implants
• Genetic predisposition?
• Responsible for cluster failures?
• Synergistic with smoking?

Surgical Complications
Host
Factors
Systemic
Factors
Local
Factors
Contributing
Etiology Non Host
Factors
Operator
Related
Biomaterial
Related
(Based on Etiology)
PART 2

Surgical Complications
Host
Factors
Systemic
Factors
Local
Factors
Contributing
Etiology
(Based on Etiology)
PART 2
LOCAL FACTORS