2 cde credits peer-reviewed ce - inibsa...
TRANSCRIPT

Bioactive Material Considerations for Vital Pulp-Capping ProtocolsMark L. Cannon, DDS, MS
Published by Dental Learning Systems, LLC © 2017
B I O A C T I V E R E S T O R AT I V E
eBookCE Continuing Dental Education
JANUARY 2017 • V4 • N67
P E E R - R E V I E W E DPEER-REVIEWED2 C D E C R E D I T S
W W W . C D E W O R L D . C O M

JANUARY 2017
eBookCE Continuing Dental Education
PEER-REVIEWED
CDEWorld eBooks and Bioactive Material Consider-ations for Vital Pulp-Capping Protocols are published by Dental Learning Systems, LLC.
Copyright ©2017 by Dental Learning Systems, LLC. All rights reserved under United States, International and Pan-American Copyright Conventions. No part of this pub-lication may be reproduced, stored in a retrieval system or transmitted in any form or by any means without prior written permission from the publisher.
PHOTOCOPY PERMISSIONS POLICY: This publi cation is registered with Copyright Clearance Center (CCC), Inc., 222 Rosewood Drive, Danvers, MA 01923. Permission is granted for photo copying of specified articles provided the base fee is paid directly to CCC.
The views and opinions expressed in the articles appear-ing in this publication are those of the author(s) and do not necessarily reflect the views or opinions of the editors, the editorial board, or the publisher. As a matter of policy, the editors, the editorial board, the publisher, and the university affiliate do not endorse any products, medical techniques, or diagnoses, and publication of any material in this journal should not be construed as such an endorsement.
WARNING: Reading an article in CDEWorld and Bioac-tive Material Considerations for Vital Pulp-Capping Protocols does not necessarily qualify you to integrate new techniques or procedures into your practice. Dental Learning Systems, LLC expects its readers to rely on their judgment regarding their clinical expertise and recom-mends further education when necessary before trying to implement any new procedure.
Printed in the U.S.A.
Dental Learning Systems, LLCP.O. Box 510Newtown, PA 18940Phone - 267-291-1150
PUBLISHER Dental Learning Systems, LLC
BRAND MANAGER, CDEWorld Elizabeth Weisbrod
SPECIAL PROJECTS MANAGER Justin Romano
SPECIAL PROJECTS COORDINATOR Angela Buziak
EDITOR Bill Noone
DESIGN Jennifer Barlow
CE COORDINATOR Hilary Noden
CEODaniel W. Perkins
PARTNERAnthony A. Angelini
PRESIDENT/COOKaren A. Auiler
Approval does not imply acceptance by a state or provisional board of dentistry or AGD endorsement. The current term of approval extends from 1/1/2017 to 12/31/2022. Provider #: 209722.
Dental Learning Systems, LLC, is an ADA CERP Recognized Provider. ADA CERP is a service of the American Dental Association to assist dental professionals in identifying quality providers of continuing dental education. ADA CERP does not approve or endorse individual courses or instructors, nor does it imply acceptance of credit hours by boards of dentistry. Concerns or complaints about a CE provider may be directed to the provider or to ADA CERP at ADA.org/CERP
2 CDEWORLD.COM
About the AuthorMark L. Cannon, DDS, MSProfessor, Northwestern University, Feinberg School of Medicine in the Division of Dentistry, Department of Otolaryngology, Chicago, Illinois
DISCLOSURE: Dr. Cannon received an honorarium for his preparation and presentation of the webinar on which this course is based.
Bioactive Material Considerations for Vital Pulp-Capping Protocols

CDEWORLD.COMVOLUME 4 • NUMBER 67 3
P E E R - R E V I E W E D2 C D E C R E D I T S
Bioactive Material Considerations for Vital Pulp-Capping ProtocolsM a r k L . C a n n o n , D D S , M S
ABSTRACTPerforming successful pulp-capping procedures is predicated on many factors, including selecting appropriate materials. In the past two decades, dental product manufacturers have demonstrated significant interest in developing materials that are biocompatible, bioactive, and non-cytotoxic and support dentin bridge formation. Today, a variety of bioactive dental restorative materials are available that promote remineralization and inhibit tooth demineralization. More recently introduced bioactive pulp-capping materials contain calcium silicate, contribute to a more biomimetic restoration, mimic the physical characteristics of tooth structure, and stabilize and protect dental hard tissues. This article reviews the development of bioactive pulp-capping materials in response to demanding clinical requirements.
LEARNING OBJECTIVES• Identify characteristics required of materials
used in pulp-capping procedures.• Explain the mechanisms involved in the dentin
mineralization process.• Describe the role of different bioactive pulp-
capping material properties in dentin bridge formation.
• Discuss the bioactive properties of hydraulic calcium-silicate cements.
Vital pulp tissue supports the long-term function of a tooth by contributing to the production of secondary dentin,
peritubular dentin, and reparative dentin when biologic and pathologic stimuli are introduced. Pulp tissue moistens the dentin, helping to en-sure its resistance and toughness, and otherwise enables teeth to withstand mastication forces.1 Therefore, restorative treatments that preserve pulp vitality—such as those incorporating vital pulp capping—are ideal.1,2
When a proper biologic seal is established and maintained to prevent infiltration of contami-nants (eg, bacteria), dental pulp can inherently heal itself through cellular differentiation and bridge formation.1,2 Unfortunately, bacterial mi-croleakage into the pulp via dentinal tubules, as well as procedures performed without proper isolation and/or properly sealing the entire dentin interface during restoration, can result in pulp necrosis and treatment failure.1-4 Ensuring he-mostatis is significantly important to the success of pulp-capping procedures (Figure 1 through Figure 5), as is the ability of pulp-capping ma-terials to prevent bacterial microleakage from penetrating through the dentinal tubules and into the pulp.1,2,4,5
Performing successful pulp-capping proce-dures is predicated on many factors, including establishing thorough hemostasis and selecting appropriate pulp-capping materials. Such ma-terials must be able to relieve clinicians of the challenges they face and not demonstrate char-acteristics such as cytotoxicity, poor handling

4 JANUARY 2017CDEWORLD.COM
properties, low initial mechanical strength, long setting times, and degradation over time.6
CHALLENGES WITH TRADITIONAL PULP-CAPPING MATERIALSFor example, modern dental adhesives that con-tain hydroxyethyl methacrylate (HEMA) and which are commonly used in pulp-capping pro-cedures have been found to be cytotoxic against an established cell line.7 In fact, in one investiga-tion designed to test cellular toxicity of modern dentin adhesives, the respective cell densities and number of normal, altered, and dead cells were determined and compared with control cell
cultures. Statistical analysis of the data showed that all materials tested caused cytotoxic effects, but there were statistically significant differences between the cytotoxicity of the products tested, suggesting some were less cytotoxic than others.8
The cytotoxicity of HEMA in relation to mito-chondrial fibroblasts, in particular, has also been studied. By measuring succinate dehydrogenase activity, higher concentrations of HEMA were shown to greatly reduce the health of mitochon-dria, which is not conducive to pulp capping. It was concluded that the risk of acute cytotoxicity to HEMA through dentin was probably low, but
1 2
3 4 5
Fig 1. A patient presented with non-symptomatic carious pulp exposure. All the decay was removed. Complete hemostasis was achieved using 3% sodium hypochlorite. Fig 2. Once hemostasis was established, pulp capping was performed by applying a light-cured, resin-based, tricalcium- and dicalcium-silicate filled liner in a thin layer as a barrier to protect the dental pulpal complex. The liner was then light-cured. Fig 3. The tooth was restored in layers and, at the 6-month recall, was totally asymptomatic. Good marginal integrity was maintained. Fig 4. At 6 years post-treatment, the tooth remained completely asymptomatic; marginal integrity remained acceptable. Fig 5. The 6-year radiograph confirmed the dentin bridge formation achieved with the tricalcium- and dicalcium-silicate material.

CDEWORLD.COMVOLUME 4 • NUMBER 67 5
that decreased dentin thickness, lack of polym-erization, or extended exposure times might increase risk significantly.9
Therefore, dental product manufacturers have demonstrated significant interest in developing materials that are biocompatible and bioac-tive, promote dentin bridge formation, and are non-cytotoxic.10 These have included bioactive molecules which, when initially investigated, demonstrated that the formation of homogeneous and mineralized reparative dentin could be in-duced by adding bioactive molecules to pulp-capping protocol.11 The mechanisms at play in this mineralization process involved the recruit-ment of cells that subsequently differentiated
into osteoblast-like cells, ultimately producing a mineralized extracellular matrix.11,12
It was later determined that direct pulp cap-ping with materials like calcium hydroxide—or implanting bioactive molecules in the pulp—may induce reparative dentin formation, as well as coronal or radicular pulp mineralization.13 However, formation of a dentin bridge, pulp obliteration, or total mineralization of the root canal was found to be dependent upon the type of bioactive molecule used, as well as the condi-tion of the underlying pulp.12-14
Today, a variety of bioactive dental restor-ative materials are available that promote
6 7
8 9 10
Fig 6. Patient presented with a failed amalgam restoration. Patient experienced spontaneous pain and could not eat. Although the first inclination may have been to perform endodontics, re-restoration was performed. Fig 7. Upon removal of the failed amalgam restoration, remnants of the previously placed and now broken-down calcium-hydroxide liner were observed, along with recurrent caries and stained margins in the left lobe from microleakage. Fig 8. The calcium-hydroxide liner was removed, as was the underlying carious dentin. The microleakage stain on the left lobe was removed after photographing. Fig 9. After etching, resin-modified calcium-silicate filled liner was placed and light-cured for 20 seconds. Fig 10. Post-treatment view of the molar that was restored using a universal composite. After composite placement, occlusion was adjusted slightly into the cuspal contact.

6 JANUARY 2017CDEWORLD.COM
remineralization and inhibit tooth demineral-ization. Containing fluoride and/or calcium, these materials range from bonding agents to resin composites, resin cements to sealants, and glass-ionomer cements to pulp-capping materi-als.15 Calcium release and the ability to sustain a positive alkalinity has been found necessary for ionic exchange, calcium deposition, and the de-velopment of new dentin so that a dental bridge can be formed.16,17
Although materials containing calcium hydroxide have been used in pulp-capping techniques and demonstrated success,1 debates regarding the compound’s suitability for this ap-plication have focused on its disintegration and breakdown over time (Figure 6 through Figure 10), as well as its tendency to pull from cavity walls during polymerization.1,18,19 Additionally, the ability of calcium hydroxide to promote scle-rotic and reparative dentin formation, dentino-genesis, and dentin bridge formation has been questioned.20
BIOACTIVE CALCIUM-SILICATE PULP-CAPPING MATERIALSMore recently researched bioactive restorative resin composites are those containing calcium-silicate, which, in a simulated oral environment, were shown not to be inert.21 Such a material that could form apatite on the surface would be beneficial for gap closure at resin–dentin inter-faces, generating better bond strengths over time and preventing bond degradation.21 Evaluations of microtensile bond strength and microhard-ness demonstrated that calcium-silicate–filled composite resins performed better than etch-and-rinse adhesives and produced a therapeutic and protective effect on the micromechanical properties of mineral-depleted resin–dentin interfaces.22 The implication is that calcium-silicate dental restorative materials can create a more biomimetic restoration, mimic the physical characteristics of tooth structure, and stabilize and protect dental hard tissues.22
Hydraulic calcium-silicate cements, otherwise known as mineral trioxide aggregate cements, are composed mainly based on di- and tri-cal-cium silicate, Al- and Fe-silicate (eg, Portland cement).23 Originally introduced in the 1990s, hydraulic calcium-silicate cements have tradi-tionally demonstrated biocompatibility, accept-able mechanical properties, and setting and seal-ing abilities in moist and blood-contaminated environments.23 They also release more calcium than conventional calcium-hydroxide pulp-cap-ping materials.24 However, limitations of early product offerings included low radiopacity, poor handling qualities, and long setting times.23
In recent years, hydraulic calcium-silicate ce-ments have been enhanced with setting modula-tors, radiopacifying agents, and other additives to the extent that their biological and transla-tional characteristics lend to their applications in root-end filling, pulp capping, scaffolds for pulp regeneration, and as root canal sealers.23 Essentially, these new hydraulic calcium-silicate cements are biointeractive (ie, ion-releasing), bioactive (ie, apatite-forming), and functional.24 They upregulate the differentiation of osteo-blasts, fibroblasts, cementoblasts, odontoblasts, pulp cells, and stem cells. Additionally, because they can induce the formation of a calcium-phosphate/apatite coating when immersed in biological fluids, their ability to promote cal-cium-phosphate deposits implies their potential application in dentin remineralization and tissue regeneration.23 The high rate of calcium release and rapid apatite formation demonstrated by hydraulic calcium-silicate cements further sup-ports their use as scaffolds to induce new dentin bridge formation, as well as clinical healing.24
Studies of a commercially available light-cur-able pulp-capping material composed of resin and calcium silicate have shown that the mate-rial demonstrates high calcium-releasing abili-ties, low solubility, and durable bond strengths and is able to alkalinize surrounding fluids.25,26
CDEWORLD.COMVOLUME 4 • NUMBER 67 7
These properties, in addition to the material’s low suppression of mitochondrial health (ie, it demonstrates low cytotoxicity), are highly beneficial in direct pulp-capping treatments.27
Its calcium release stimulates hydroxyapatite, secondary dentin bridge formation, and cre-ation of a protective seal, while alkalinization promotes healing and apatite formation.25,28
11 12
13 14 15
16 17 18
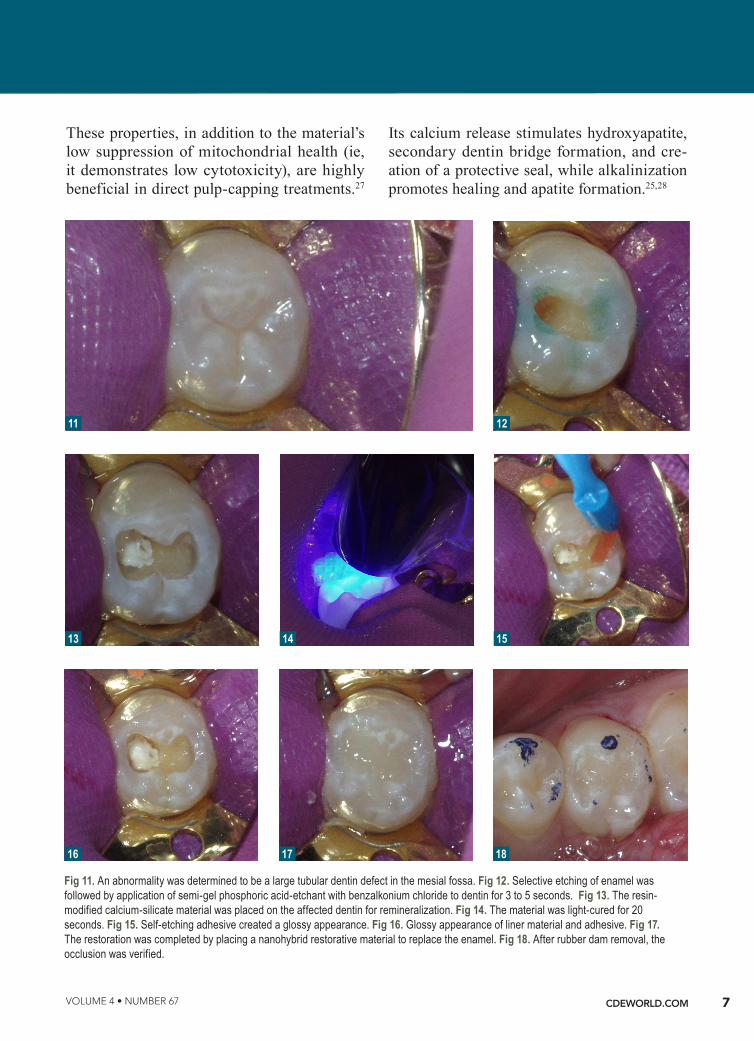
Fig 11. An abnormality was determined to be a large tubular dentin defect in the mesial fossa. Fig 12. Selective etching of enamel was followed by application of semi-gel phosphoric acid-etchant with benzalkonium chloride to dentin for 3 to 5 seconds. Fig 13. The resin-modified calcium-silicate material was placed on the affected dentin for remineralization. Fig 14. The material was light-cured for 20 seconds. Fig 15. Self-etching adhesive created a glossy appearance. Fig 16. Glossy appearance of liner material and adhesive. Fig 17. The restoration was completed by placing a nanohybrid restorative material to replace the enamel. Fig 18. After rubber dam removal, the occlusion was verified.

8 JANUARY 2017CDEWORLD.COM
CASE PRESENTATIONRadiographic examination of a patient’s tooth revealed an abnormality that was subsequently evaluated using a laser caries detection aid. A reading of 68 was obtained. A large tubular dentin defect in the mesial fossa was identified; therefore, the decision was made to treat the tooth (Figure 11).
The tooth was prepared, with care taken not to expose the pulp or remove all of the large tubular dentin, but only those aspects that were soft. This would promote remineralization via application of the aforementioned apatite-stimulating, light-cured, resin-modified calcium-silicate material (TheraCal®, Bisco, www.bisco. com).The enamel was etched for 30 seconds, after which the dentin was etched for 3 to 5 seconds (Figure 12).
The calcium-releasing resin-modified calci-um-silicate material was placed on the affected dentin for remineralization (Figure 13). The material was light-cured for 20 seconds with at least 500 mW/cm2 (Figure 14).
To begin the restorative process, a self-etching adhesive was placed, creating a glossy appear-ance to the calcium-silicate liner, and the ad-hesive was light-cured (Figure 15 and Figure 16). A nanohybrid restorative material was then placed to replace the enamel (Figure 17). Upon completion of the restoration, the rubber dam was removed, the occlusion verified (Figure 18), and the restoration polished.
CONCLUSIONWhen bioactive restorative materials are used for vital pulp-capping protocol, beneficial out-comes result from the induction of physical and chemical processes that mimic those of natural teeth. Although the success of pulp-capping procedures is predicated on many factors—such as ensuring hemostasis and proper isolation—selecting a material that is biocompatible and bioactive, promotes dentin
bridge formation, and is non-cytotoxic can help to stabilize and protect dental hard tissues for the long term.
REFERENCES1. Stockton LW. Vital pulp capping: a worthwhile procedure. J Can Dent Assoc. 1999;65(6):328-331.
2. Stanley HR. Pulp capping: conserving the dental pulp. Can it be done? Is it worth it? Oral Surg Oral Med Oral Pathol. 1989;68(5):628-639.
3. Cox CF. Biocompatibility of dental materials in the absence of bacterial infection. Oper Dent. 1987;12(4):146-152.
4. Bergenholtz G, Cox CF, Loersche WJ, Syed SA. Bacterial leakage around dental restorations: its effect on the dental pulp. J Oral Pathol. 1982;11(6):439-450.
5. Pashley DH. The effects of acid etching on the pulpodentin complex. Oper Dent. 1992;17(6):229-242.
6. Chang KC, Chang CC, Chen WT, et al. Development of calcium phosphate/sulfate biphasic cement for vital pulp therapy. Dent Mater. 2014;30(12):e362-e370.
7. Koliniotou-Koubia E, Dionysopoulos P, Koulaouzidou EA, et al. In vitro cytotoxicity of six dentin bonding agents. J Oral Rehabil. 2001;28(10):971-975.
8. Szep S, Kunkel A, Ronge K, Heidemann D. Cytotoxicity of modern dentin adhesives—in vitro testing on gingival fibroblasts. J Biomed Mater Res. 2002;63(1):53-60.
9. Bouillaguet S, Wataha JC, Hanks CT, et al. In vitro cytotoxicity and dentin permeability of HEMA. J Endod. 1996;22(5):244-248.
10. Moore AN, Perez SC, Hartgerink JD, et al. Ex vivo model-ing of multidomain peptide hydrogels with intact dental pulp. J Dent Res. 2015;94(12):1773-1781.
11. Goldberg M, Six N, Decup F, et al. Application of bio-active molecules in pulp-capping situations. Adv Dent Res. 2001;15:91-95.
12. Goldberg M, Six N, Decup F, et al. Bioactive molecules and the future of pulp therapy. Am J Dent. 2003;16(1):66-76.
13. Goldberg M, Smith AJ. Cells and extracellular matrices of dentin and pulp: a biological basis for repair and tissue engineering. Crit Rev Oral Biol Med. 2004;15(1):13-27.
14. Oguntebi B, Clark A, Wilson J. Pulp capping with Bioglass

CDEWORLD.COMVOLUME 4 • NUMBER 67 9
and autologous demineralized dentin in miniature swine. J Dent Res. 1993;72(2):484-489.
15. Chen L, Shen H, Suh BI. Bioactive dental restorative materials: a review. Am J Dent. 2013;26(4):219-227.
16. Okabe T, Sakamoto M, Takeuchi H, Matsushima K. Effects of pH on mineralization ability of human dental pulp cells. J Endod. 2006;32(3):198-201.
17. Hakki SS, Bozkurt BS, Ozcopur B, et al. The response of cementoblasts to calcium phosphate resin-based and calcium silicate-based commercial sealers. Int Endod J. 2013;46(3):242-252.
18. Goracci G, Mon G. Scanning electron microscopic evaluation of resin-dentin and calcium hydroxide-dentin interface with resin composite restorations. Quintessence Int. 1996;27(2):129-135.
19. Cox CF, Sübay RK, Ostro E, et al. Tunnel defects in dentin bridges: their formation following direct pulp capping. Oper Dent. 1996;21(1):4-11.
20. Cox CF, Suzuki S. Re-evaluating pulp protection: calcium hydroxide liners vs. cohesive hybridization. J Am Dent Assoc. 1994;125(7):823-831.
21. Profeta AC. Preparation and properties of calci-um-silicate filled resins for dental restoration. Part I: chemical-physical characterization and apatite-form-ing ability. Acta Odontol Scand. 2014;72(8):597-606.
22. Profeta AC. Preparation and properties of calcium-silicate filled resins for dental restoration. Part II: micro-mechanical behaviour to primed mineral-depleted dentine. Acta Odontol Scand. 2014;72(8):607-617.
23. Prati C, Gandolfi MG. Calcium silicate bioactive cements: Biological perspectives and clinical applications. Dent Mater. 2015;31(4):351-370.
24. Gandolfi MG, Siboni F, Botero T, et al. Calcium silicate and calcium hydroxide materials for pulp capping: biointerac-tivity, porosity, solubility and bioactivity of current formula-tions. J Appl Biomater Funct Mater. 2015;13(1):43-60.
25. Gandolfi MG, Siboni F, Prati C. Chemical-physical prop-erties of TheraCal, a novel light-curable MTA-like material for pulp capping. Int Endod J. 2012;45(6):571-579.
26. Croll TP, Berg JH, Donly KJ. Dental repair material: a resin-modified glass-ionomer bioactive ionic resin-based composite. Compend Conti Educ Dent. 2015;36(1):60-65.
27. Bianchi L, Ribeiro AP, de Oliveira Carrilho MR, et al. Transdentinal cytotoxicity of experimental adhesive systems of different hydrophilicity applied to ethanol-saturated dentin. Dent Mater. 2013;29(9):980-990.
28. Gandolfi MG, Spagnuolo G, Siboni F, et al. Calcium silicate/calcium phosphate biphasic cements for vital pulp therapy: chemical-physical properties and human pulp cells response. Clin Oral Investig. 2015;19(8):2075-2089.

10 JANUARY 2017CDEWORLD.COM
TO TAKE THE QUIZ, VISITCDEWORLD.COM/EBOOKS/CE/67
QuizCDE 2 CDE Credits
Bioactive Material Considerations for Vital Pulp-Capping ProtocolsMark L. Cannon, DDS, MS
1. Pulp tissue moistens the dentin, helping to ensure its: A. cytotoxicity. B. resistance and toughness. C. inability to repel contaminants. D. degradation over time.
2. Bacterial microleakage into the pulp via dentinal tubules can result in:
A. highly successful treatment outcomes. B. complete hemostasis. C. good mechanical strength. D. pulp necrosis.
3. The presence of hydroxyethyl methacrylate (HEMA) in pulp-capping procedures has been found to:
A. sustain the health of mitochondria. B. promote dentin bridge formation. C. be cytotoxic against an established cell line. D. increase dentin thickness.
4. Dental product manufacturers have demonstrated interest in developing materials that are biocompatible and bioactive and:
A. have low mechanical strength. B. promote dentin bridge formation. C. have long setting times. D. degrade rapidly.
5. Today, a variety of bioactive dental restorative materials are available that promote remineralization and inhibit:
A. tooth demineralization. B. calcium release. C. development of new dentin. D. ionic exchange.
6. The ability of calcium hydroxide to promote sclerotic and reparative dentin formation, dentinogenesis, and dentin bridge formation:
A. is irrefutable. B. has been questioned. C. has been proven beyond any doubt. D. has never been studied.
7. Introduced in the 1990s, hydraulic calcium-silicate cements have traditionally demonstrated:
A. biocompatibility. B. acceptable mechanical properties. C. setting and sealing abilities in moist and blood-
contaminated environments. D. All of the above
8. Applications for hydraulic calcium-silicate cements include:
A. root-end filling. B. pulp capping. C. scaffolds for pulp regeneration. D. All of the above
9. Hydraulic calcium-silicate cements’ use as scaffolds to induce new dentin bridge formation is supported by their high rate of:
A. calcium release and rapid apatite formation. B. solubility. C. cellular cytotoxicity. D. All of the above
10. Among the factors on which the success of pulp-capping procedures is predicated is:
A. proper isolation. B. avoiding hemostasis. C. ensuring bacterial microleakage into the pulp. D. suppressing apatite formation.
TO TAKE THE QUIZ, VISITCDEWORLD.COM/EBOOKS/CE/67
Approval does not imply acceptance by a state or provisional board of dentistry or AGD endorsement. The current term of approval extends from 1/1/2017 to 12/31/2022. Provider #: 209722.
Dental Learning Systems, LLC, is an ADA CERP Recognized Provider. ADA CERP is a service of the American Dental Association to assist dental professionals in identifying quality providers of continuing dental education. ADA CERP does not approve or endorse individual courses or instructors, nor does it imply acceptance of credit hours by boards of dentistry. Concerns or complaints about a CE provider may be directed to the provider or to ADA CERP at ADA.org/CERP
This article provides 2 hours of CE credit from Dental Learning Systems, LLC. To participate in the CE lesson for a fee of $0, please log on to http://cdeworld.com. Course is valid from 1/1/17 to 1/31/20. Participants must attain a score of 70% on each quiz to receive credit. Participants will receive an annual report documenting their accumu-lated credits, and are urged to contact their own state registry boards for special CE requirements.