1st worldwide internet syyp gmposium on drug--induced...
TRANSCRIPT

1st Worldwide Internet Symposium on Drug1st Worldwide Internet Symposium on Drug--Induced QT Induced QT y p gy p g QQProlongation, October 2007Prolongation, October 2007
Drug induced LQT Syndrome: Sotalol ExperienceDrug-induced LQT-Syndrome: Sotalol-Experience, Heart failure, Susceptibility to drug induced LQT
Stefan KääbLudwig-Maximilians Universität München
Klinikum Grosshadern, Med. Klinik [email protected]
LMU
no conflicts of interest to disclose

Objective and Outline• review data on Sotalol as an examplary agent of drug-induced LQT
syndrome
• introduce the multifactorial nature of drug-induced LQT syndrome,
highlighting hypertrophy and heart failure as important co-factors for
TdP in the conte t of dr gs ith QT prolonging potential (i ETdP in the context of drugs with QT-prolonging potential (i.E.
Sotalol)
Sotalol as a tool to study altered repolarization and susceptibility to• Sotalol as a tool to study altered repolarization and susceptibility to
TdP in the context of QT prolonging drugs
common genetic variants modulate myocardial repolarization and• common genetic variants modulate myocardial repolarization and
define intrinsic individual susceptibility to drug-induced LQT
syndromesyndrome

Sotalol induced changes in myocardial l i ti i h lth l trepolarization in healthy volunteers
(n=39)
Couderc JP et al. J Electrocardiol 2003; 36:115-120
QTc and area-based repolarization parameters are affected by sotaloli di ti d i d d h i T h lindicating drug induced changes in T-wave morphology

Sotalol induced changes in QTcSotalol induced changes in QTc--Interval Interval i t i l d t i l h th i ti ti t i l d t i l h th i ti tin atrial and ventricular arrhythmia patients in atrial and ventricular arrhythmia patients
(n=209) (n=209)
160 mg b.i.dDischarge 80 mg b.i.d.Discharge
Baseline
QTc (ms)
Kim RJ, et al., Pace 2006; 29:1219-1225

Yield of in-hospital monitoring for initiation of sotalol in atrial arrhythmia patientsof sotalol in atrial arrhythmia patients
(n=120)
• new or increased ventricular arrhythmias in n=7 (5.8%) (TdP in n=2)
• significant bradycardia in n=20 (16.7 %)
• excessively prolonged QTc interval in n=8 (6.7 %)
Ch MK t l J A C ll C di l 1998 32 169 176Chung MK, et al., J Am Coll Cardiol 1998;32:169-176

Proarrhythmia with sotalol• pooled analysis of n=1.288 patients enrolled in premarketing trials
showed new or increased ventricular arrhythmia occurred in 4.3% (1.9% classified as torsades de pointes)1( p )
• the survival with oral d-sotalol (SWORD) trial demonstrated increased mortality in remote myocardial infarction group with LVEF between
230-40% (RR=7.9) with increased risk in women2
• in general proarrhythmia is reported with a range of 1% to 8% for sotalolsotalol
• sotalol causes a concentration dependent lengthening of the QT interval, increasing action potential duration and refractory periods predominantly by blocking the delayed rectifier potassium current (IKr)
1Soyka LF et al., Am J Cardiol 1990; 65:74A-81A2Pratt CM, et al., Am J Cardiol 1998; 81:869-876

Increased short-term variability of repolarization rather than QT prolongation predicts d-sotalol induced
t d d i t i d ith h i AV bl ktorsades de pointes in dogs with chronic AV block induced LV-hypertrophy
Thomsen MB, et al., Circulation 2004; 110:2453-2459

LV-Hypertrophy and congestive heart failure b d d f f i d LQTcan be regarded as forms of acquired LQT
syndrome and thus are specific risk factors f d i d d LQT dfor drug induced LQT syndrome

Heart Heart FailureFailure
neurohumoral neurohumoral pump failurepump failure electrical failureelectrical failure
DepolarizationDepolarization RepolarizationRepolarization
activationactivationstretchstretch
ImbalanceImbalance
(substrate)(substrate)
hemodynamic hemodynamic
short termshort termlong long termterm (trigger)(trigger)
EADEAD InhomogeneityInhomogeneity( ti( ti t l)t l)compensationcompensation (spatio(spatio--temporal)temporal)
altered gene expressionaltered gene expression
Torsades de Pointes TachycardiaTorsades de Pointes Tachycardiapolymorphic VTpolymorphic VTdd di d thdd di d thsudden cardiac deathsudden cardiac death
modified from: Marban E, J Cardiovasc Electrophysiol, 1999;10:1425-8

Prolongation of APD due to reduced IProlongation of APD due to reduced Ito1to1in isolated human cardiomyocytes in congestive heart failurein isolated human cardiomyocytes in congestive heart failurey y gy y g
12
pF] NonFailing
Failing
6
8
10
nsity
Ito
[pA/
p Failing
0
2
4Den
Center0
Density Ito Human Ventricle
Beuckelmann DJ, Näbauer M, Erdmann E. Circ Res 73:379 (1993) Beuckelmann DJ, Näbauer M, Erdmann E. Circ Res 73:379 (1993)

Transmural Dispersion of Repolarization in Heart Failure
Tachycaria induced HF modelTachycaria induced HF model
canine LV wedge preparationscanine LV wedge preparations
APD contour maps
APD recordingsg
F. Akar and D. Rosenbaum, Circ. Res. 2003; 93:638-645

Excessive AP-Prolongation by K+ channel block (CsCl) in congestive heart failure – evidence for reduced g
repolarization reserve
700
800
(ms)
Control + CsCl
400
500
600
APD
90
(
100
200
300
Control Myocytes Failing Myocytes0
Pak P, et al., JACC (1997)Pak P, et al., JACC (1997)dog ventricular myocytes

Hypertrophy and Congestive Heart Failure in Humans: an Acquired Form of Long-QT-Syndrome
Congestive Heart FailureLV-Hypertrophy
6006001/2 ]
600
400
500
600
400
500
600
tion
[mse
c1
400
500
600
440 ms
200
300
400
200
300
400
QTc
- D
ura
200
300
400
0
100
200
0
100
200
0
100
200
Singh JP, et al. , Choy AM et al.,
Choy Roden
0Singh
0QTc-Duration
0 Survivers (2-4 years)
Other Cardiac Death SCD, VT
g , ,JACC 29: 778 (1997) Fu G-S, et al. , Eur Heart J 18:281 (1997)
y ,Circulation 96:2149 (1997)

Heart Heart FailureFailure
Genetics of acquired LQT Syndrome ?Genetics of acquired LQT Syndrome ?
neurohumoral neurohumoral pump failurepump failure electrical failureelectrical failure
DepolarizationDepolarization RepolarizationRepolarization
Genetics of acquired LQT Syndrome ?Genetics of acquired LQT Syndrome ?
activationactivationstretchstretch
ImbalanceImbalance
(substrate)(substrate)
hemodynamic hemodynamic
short termshort termlong long termterm (trigger)(trigger)
EADEAD InhomogeneityInhomogeneity( ti( ti t l)t l)Search for genetics of heart failureSearch for genetics of heart failurecompensationcompensation (spatio(spatio--temporal)temporal)Search for genetics of heart failureSearch for genetics of heart failure
Search for genetics of altered repolarizationSearch for genetics of altered repolarizationaltered gene expressionaltered gene expression
Torsades de Pointes TachycardiaTorsades de Pointes Tachycardiapolymorphic VTpolymorphic VTdd di d thdd di d thsudden cardiac deathsudden cardiac death
modified from: Marban E, J Cardiovasc Electrophysiol, 1999;10:1425-8

Case Report
• 25 y, female patient
• ARDS, Sepsis
• Cardiomyopathy
• repetitive polymorphic VTrepetitive polymorphic VT
• TdP CPR• TdP, CPR Hinterseer et al., Br J Anaesth 2006

A tibi ti ThA tibi ti ThAntibiotic Therapy:Antibiotic Therapy:CefotiamCefotiamGentamycineGentamycine
16.04.16.04.
GentamycineGentamycineErythromycineErythromycine

TEE from April 17th. : LVEDD 60 ms, FS<10%

April 17th : Torsades de Pointes ArrhythmiaApril 17th : Torsades de Pointes Arrhythmia
QTc=510 msQTc=510 msQTc 510 msQTc 510 ms
•• polymorphic ventricular tachycardiapolymorphic ventricular tachycardia•• changing amplitude and QRSchanging amplitude and QRS axisaxis•• changing amplitude and QRSchanging amplitude and QRS--axisaxis•• prolonged QT inervalprolonged QT inerval•• initial shortinitial short--longlong--shortshort--sequencesequence•• initial shortinitial short--longlong--shortshort--sequencesequence

Cardiological Evaluation(5 weeks past acute illness)(5 weeks past acute illness)
• ECG :
regular SR, HR 80/min, left axis deviation,QTc 423 ms
• cardiac catheterization & EP study:
no structural heart diseaseno sustained arrhythmia induceabley
• echocardiography:
within normal limits

Testing Myocardial Repolarisation Reserve by i.v. Sotalol
pre Sotalol post SotalolG.F. (25 y)
by i.v. Sotalol
IIQTc 420ms QTc 510ms
V2
Control:
II
Control:
QT 450
V2QTc 410 ms QTc 450ms
according to protocol in Kaab et al, Eur Heart J. 2003; 24: 649-657

Sotalol testing unmasks reduced repolarization reserve in patients with history of drug induced LQT syndrome
600
650
600
650Study GroupControl Group
550
600
550
600
450
500
450
500 QTc [ms]
400 400
300
350
300
350
postprepostpreSotalol
postpreSotalol
postpre
Kääb et al., Eur Heart J, 2003;24:649-657

Repolarization ReserveRepolarization Reserve
n n
Electrolyte Electrolyte disturbancedisturbance
Genetic Disposition Genetic Disposition female genderfemale gendergenetic variants ?genetic variants ?
ispe
rsio
nis
pers
ion
on
on ↑↑
gg
f QTc
f QTc↑↑,
d, dpo
lariz
atio
pola
rizat
io&
SC
D&
SC
D
DrugsDrugsCardiac DiseaseCardiac Disease
number of risk factorsnumber of risk factors
risk
oris
k o
of re
pof
rep
TdP
&Td
P &
CNS diCNS di S t d f tiS t d f ti P hi t i DiP hi t i DiCNS diseaseCNS disease System dysfunctionSystem dysfunction Psychiatric DiseasePsychiatric Disease
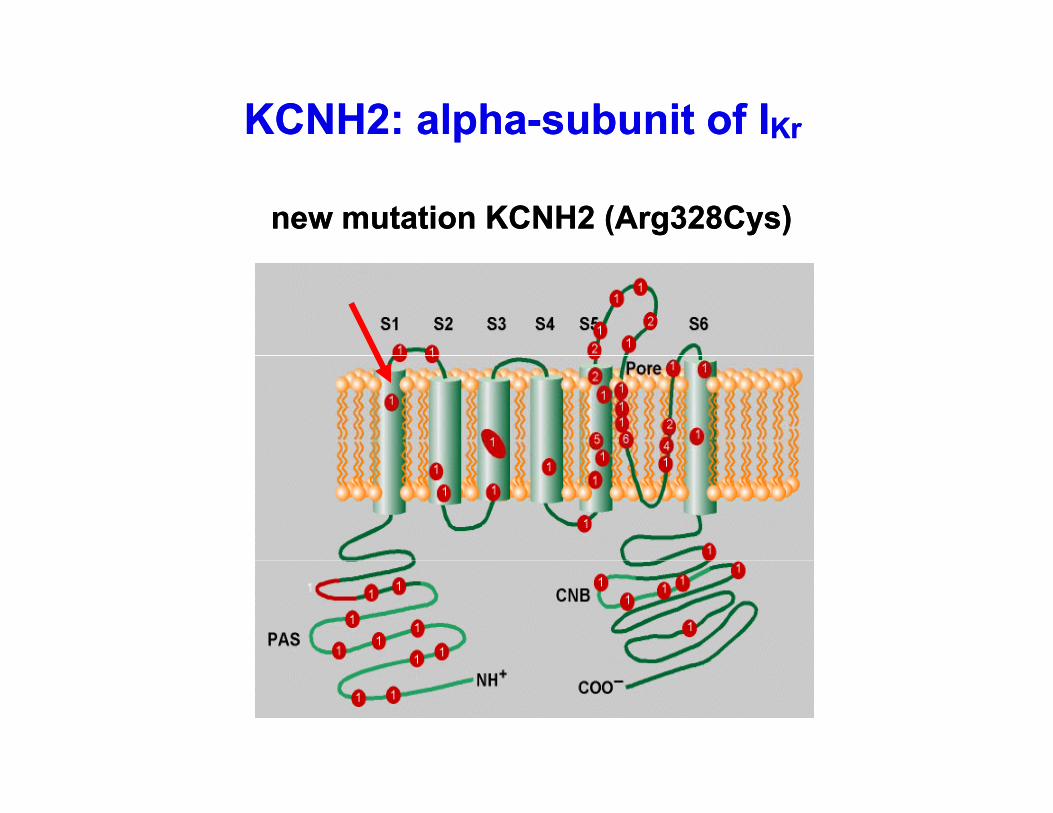
KCNH2: alphaKCNH2: alpha--subunit of Isubunit of IKrKr
new mutation KCNH2 (Arg328Cys)new mutation KCNH2 (Arg328Cys)

Family
?
mutation KCNH2 (Arg328Cys)mutation KCNH2 (Arg328Cys)
? QTc 395QTc 395
QTc 423QTc 423 ???? QTc 420QTc 420
QTc 463QTc 463 QTc 416QTc 416QTc 430QTc 430QTc 428QTc 428QTc 439QTc 439

Questions
• Is genetic susceptibility to acquired LQTIs genetic susceptibility to acquired LQT syndrome relevant?
• What is the substrate of genetic susceptibility to acquired LQT syndrome?susceptibility to acquired LQT syndrome?

Monogenic and Complex Genetic Diseases
relative risk attributed to genetic variant Human Genetics
M i “
Continuous distributionof genetic variants
RR 1000RR 1000 Arrhythmogenic RightArrhythmogenic Right--Ventricular DysplasiaVentricular Dysplasia
„Mutations“gshaped by
mutation and selection
RR 100RR 100
RR 10RR 10
LongLong--QT SyndromeQT SyndromeHypertrophic CardiomyopathyHypertrophic Cardiomyopathy
Genetic Epidemiology„Polymorphisms“
RR 5RR 5
RR 2RR 2
F V LeidenF V LeidenQT prolonging QT prolonging SNPsSNPs
50 %50 %10 %10 %0,001 %0,001 % 0,01 %0,01 % 0,1 %0,1 % 1 %1 %RR 1RR 1
Prevalence in populationPrevalence in population
monogenicpolygenic
adapted from : N.E. Morton et al.

QTc Associated with Risk of SCD in the General Population (Rotterdam Study, n=4.344)
Log Survival FunctionLog Survival Function QTc normal m: ≤ 430f
QTc normalQTc normal
f: ≤ 450QTc borderline m: 431- 450
f: 451- 470QTc abnormal m: > 450
f: > 470 QTc borderlineQTc borderline
QTc abnormalQTc abnormal
QTc and Risk for SCD(< Median age 55-68 y)
borderline 1 6 (0 9 3 1)borderline(n=1.109 / 514)
1.6 (0.9-3.1)3.7 (1.1-14.0)
abnormal 2.5 (1.3-4.7)
FollowFollow--up (days)up (days)(6.7 (6.7 ±± 2.3 years)2.3 years)
(n=681 / 212) 8.0 (2.1-31.3)
Straus et al., JACC 2006;47:362-7

Genetic Variants and Risk for ArrhythmiasGenetic Variants and Risk for Arrhythmias
Common Disease Common Variant (?)Common Disease Common Variant (?)Common Disease Common Variant (?)Common Disease Common Variant (?)
•• From Rare to Common DiseasesFrom Rare to Common Diseases
•• From Rare to Common Gene VariantsFrom Rare to Common Gene Variants
Genetic susceptibility to Arrhythmias in the context of drugsmay follow the common disease common variant hypothesisy yp

LDLD--mapping in 4 LQT disease genesmapping in 4 LQT disease genes
chr11:2,450,000 | chr11:2,850,000 |chr11:2,550,000 | chr11:2,650,000 | chr11:2,750,000 |
KCNQ1 (11p15.5-p15.4)450 kb
• • • • •
16 Exons
81 SNPs
5‘
1 2 34
5 6 7 8 9 10 11 12
rs757092rs23017000.04480.2780
rs7396770.01600.2570
rs7570920.01290.0007
+1.67 ms
rs4639240.04050.8865
rs25191840.00180.4870
rs757092+1.67 ms/allele0.5% variance
p=2.3*10-5
n=3,966
chr7:150,000,000 | chr7:150,090,000 |
KCNH2 (7q36)
120 kb
5‘
chr21:34,700,000 | chr21:34,800,000 |
KCNE2 (21q22.11-q22.12) KCNE1
173 kb
5‘ 5‘
,
•• • • •
15 Exons
59 SNPs
5‘
1
2
3 45
6 7
• ••
2+3 Exons
34 SNPs
5‘ 5‘
1 2 3 4 5 6 7 89
rs8856840.01080.1665
rs9566420.02730.9998
rs18051230.02230.0017
-1.83 ms
rs38007790.04600.7194
rs17999830.03480.8917
rs28344560.00790.4451
rs28344880.01710.4825
rs7279570.00810.0498
+1.49 ms
Pfeufer et al., Circ Res. 2005K897T

Common variants (SNPs) in LQT disease genes modulate QT interval in the general population
Combined effect of 3 SNPs (6 alleles) on QT-interval
QT l i ll l QT RAS SDQT-prolonging allele QTc_RAS ± SD n
0 412.3 ± 13.8 70
1 415.8 ± 17.1 432
2 416.7 ± 16.4 905
3 417.7 ± 17.3 955
4 420.3 ± 17.7 561
5 420.4 ± 19.7 162
6 426.6 ± 18.2 19Analysis of 174 LD based SNPs in 4 LQT-disease genes shows positive
association in 3 loci and explains 15 ms of QT-interval variancePfeufer et al. Circ Res 2005

Hypotheses on genetic disposition to acquired LQTSHypotheses on genetic disposition to acquired LQTS
common gene variants in LQT disease genes and
genes modulating cardiac repolarization or cardiac
electrical properties are associated with risk for
arrhythmia in acquired LQT syndrome
(e.g. in the context of QT prolonging drugs)(e.g. in the context of QT prolonging drugs)

Searching for novel genesSearching for novel genes involved in QT regulation as the surrogate
marker for cardiac repolarizationmarker for cardiac repolarization
w/ hypothesis -> disease genes
w/o hypothesis -> genome wideyp g

GWA of QT interval in the General Population (KORA) using 100 K SNP Chip
Stage 1• n=103/103 from each extreme
(top and bottom 7.5th %tile)
Stage 2• n=300/300 from each extreme
• relaxed exclusion criteria
Stage 3• n=3,966, KORA S4 survey• relaxed exclusion criteria
Three stage design:
( p )• strict exclusion criteria
• females only• Genomewide genotyping
(s AF,pacer, pregnancy)• females only
• SNPs that passed stage 1
(s AF,pacer, pregnancy)• both genders
• SNPs that passed stage 2
m 5th%tileBCC…
Uppeaa
m 5th%tileBCC…
Uppeaa
m 5th%tileBCC…
Uppeaa
m 5th%tileBCC…
Uppeaa
m 5th%tileBCC…
Uppeaa
m 5th%tileBCC…
Uppeaa
m 5th%tileBCC…
Uppeaa
m 5th%tileBCC…
Uppeaa
m 5th%tileBCC…
Uppeaa
m 5th%tileBCC…
Uppeaa
m 5th%tileBCC…
Uppeaa
m 5th%tileBCC…
Uppeaa
m 5th%tileBCC…
Uppeaa
m 5th%tileBCC…
Uppeaa
m 5th%tileBCC…
Uppeaa
m 5th%tileBCC…
Uppeaa
QTc_RAS QTc_RAS QTc_RAS
NOS1AP (C ) d l t QT i t l b 5 10 (1 5% )NOS1AP (Capon) modulates QT interval by 5-10 ms (1,5% var.)An hypothesis free genome wide association study was useful to identify a novel gene variant that modulates QT in the general population and may be a risk factor for drug induced LQT syndrome
Arking, Pfeufer et al., Nat. Genet 2006;38:644-651
risk factor for drug induced LQT syndrome

Summaryt l l t ti d d t l th i f th QT i t l i i• sotalol causes a concentration dependent lengthening of the QT interval, increasing
action potential duration and refractory periods predominantly by blocking the delayed
rectifier potassium current (IKr)
• for sotalol proarrhythmia is reported with a range of 1% to 8%
• hypertrophy and heart failure are acquired states with reduced repolarization reserve
due to downregulation of repolarizing currents and thus are important co factors fordue to downregulation of repolarizing currents and thus are important co-factors for
TdP in the context of drugs with QT-prolonging potential (i.E. Sotalol)
• Sotalol as a predominantly IKr blocking agent is a valid tool to study altered
repolarization and susceptibility to TdP in the context of QT prolonging drugs
• common genetic variants modulate myocardial repolarization, define intrinsic
individual repolarization stability and are likely to define intrinsic individualindividual repolarization stability and are likely to define intrinsic individual
susceptibility to drug-induced LQT syndrome
• Combinations of multiple extrinsic and intrinsic factors (multiple allels) are defining the
overall individual risk for drug induced LQT syndrome

CollaborationsVanderbilt UniversityDan Roden
Amsterdam University
LMU München GroßhadernMed. Klinik IMoritz Sinner
Johns Hopkins University& McKusick-Nathan InstituteDan E. ArkingWendy PostAmsterdam University
Arthur WildeConnie Beccina
University Münster
Martin HinterseerBritt-Maria Beckmann
TU München IHG, & GSF
Wendy PostW.H. Linda KaoAravinda Chakravarti
U i it M di l C tUniversity MünsterEric Schulze-Bahr
Nantes, INSERMJean-Jaques Schott
Arne PfeuferShapour JalilzadehMahmut AkyolThomas Meitinger
University Medical Center UtrechtMarc VosMorten ThomsenJean Jaques Schott
Denis Escande (†)
Johns Hopkins UniversityCardiology
Thomas Meitinger
GSF, EPI & IMEI Siegfried Perz Th Illi
University of RochesterJean-Philippe CoudercWojciech ZarebaCardiology
Peter M. SpoonerGordon TomaselliEduardo Marbán
Thomas IlligH.-Erich Wichmann
Wojciech ZarebaArthur Moss
University MiamiRobert MyerburgNanette Bishopric

Grant Support
German National Genome Research Network
http://www.allianceagainstscd.org/