1960 summary of disease outbreaks...
TRANSCRIPT

1960 Summary of Disease Outbreaksand a 10-Year Resume
CARL C. DAUER, M.D.
This is the 10th summary of foodborne and water-borne disease outbreaks prepared by the author. Inaddition to presenting data for 1960, it summarizesdata collected during the decade 1951-60. Thesummary also reviews the reporting by individualStates, compares reporting in the United States withthat of England and Wales, and describes the gen¬eral pattern of disease outbreaks in this period.
THE TOTAL NUMBER of outbreaks re¬
ported was considerably lower in 1960 thanin 1959 or 1958 (table 1) principally becauseof a marked decrease in the categories of staphy¬lococcal food poisoning and gastroenteritis,etiology unknown (table 2). It is not presumedthat these decreases indicate significant progressin prevention of these foodborne diseases butrather that reporting was even more incompletethan usual in 1960.
Waterborne Outbreaks
The 11 waterborne disease outbreaks reportedin 1960 included 2 small outbreaks of typhoidfever, 2 cases in one outbreak and 6 in the other;3 of hepatitis; 2 of shigellosis or bacillarydysentery; and 3 of gastroenteritis. Only 1 ofthe 11 outbreaks was attributed to a publicwater supply. A large number of cases of shig¬ellosis occurred after a breakdown in a town'swater treatment plant. All other outbreakswere associated with the use of water from wellsor springs.
Milkborne OutbreaksFluid milk was the vehicle of infection in
only one of the five outbreaks reported. Theother four were attributed to various milk prod¬
ucts. In the instance involving fluid milk, fivecases of staphylococcal food poisoning were
traced to unpasteurized milk from a fresh cow.
Many coagulase-positive staphylococci were iso¬lated from a specimen of the cow's milk. An¬other outbreak of five cases followed consump¬tion of ice cream made with unrefrigerated rawmilk that had been obtained from one cow.
There was no evidence of mastitis in the cow.
In another instance, 10 cases of Salmonella mon-tevideo infection followed the eating of home¬made ice cream made with raw milk and a
cracked egg found in a hen's nest. Five cases
of gastroenteritis of undetermined etiology oc¬
curred in a family group who ate cottage cheesepurchased from a store. The probable source
of infection was not found.
Typhoid Fever
The four outbreaks of typhoid fever reportedincluded one that was clearly waterborne, one
that probably was waterborne, and two thatwere foodborne. In the first outbreak, six users
of well water developed the disease. Investiga¬tion demonstrated that the well was contami¬nated by seepage from a septic tank used by a
known carrier. In the other small outbreak thetwo persons affected lived in crowded, unhygi¬enic surroundings and had used water from a
well that was susceptible to contamination froma septic tank. A resident of the immediate area
who used these sanitary facilities was found tobe a typhoid carrier. One of the foodborne out¬breaks occurred after a wedding reception wherechicken salad sandwiches were served. One of
Dr. Dauer is medical advisor, National Center forHealth Statistics, Public Health Service.
Vol. 76, No. 10, October 1961 915

the women who helped in the preparation of thechicken salad was a carrier. The preliminaryreport showed a total of 30 cases including one
boy who did not attend the reception but pre¬sumably ate one of the sandwiches. The otherfoodborne outbreak occurred among 10 collegestudents who ate in a college dining hall. Acook who worked in the kitchen was found tobe carrying the same phage type of organismthat was isolated from some of the patients.Investigation was hampered by the fact that thestudents developed symptoms after leaving theschool for their summer vacations.
Salmonellosis
Seventeen outbreaks of salmonellosis were re¬
ported. One was considered milkborne, and theremainder were foodborne (table 3). Four ofthe outbreaks were associated with eating poul¬try meat, three with other meat, three withcustard-filled desserts, and two with otherfoods. In four outbreaks the type of food was
not definitely determined but they were consid¬ered to be Salmonella infections because specifictypes of organisms were recovered from affectedpersons. One of the outbreaks associated withcustard-filled desserts was believed to have beencaused by contamination of the food with ratdroppings. In another instance, frozen wholeeggs used in the preparation of cream puffswere thought to be the source of infection.One outbreak was reported in which a food-handler in a bakery had Salmonella diarrhea.He was believed to be the source of infection ofthe cream pie, eclairs, and cake eaten by mem¬bers of several families who purchased the food.In a family outbreak of 10 cases after eatinghomemade ice cream made with raw milk anda cracked egg, S. montevideo was isolated fromspecimens of the ice cream and from stools ofthe patients.Salmonella typhimurium was isolated in five
outbreaks, S. heidelberg in four, and S. enterit-idis, S. manhattan, S. montevideo, S. new-
port, and S. oranieriburg in one each. Thespecific type was not reported in the three re¬
maining outbreaks. The four isolations of S.heidelberg were made in one State while thefive of S. typhimuriwn were made in widelyscattered areas.
Table 1. Foodborne and waterborne diseaseoutbreaks reported in I960, by vehicle ofinfection 1
Area
Total.
New England:Maine_Massachusetts_Connecticut_
Middle Atlantic:New York_New Jersey_Pennsylvania_
East North Central:Ohio_Indiana_Illinois_Michigan_Wisconsin_
West North Central:Minnesota_Iowa_South Dakota_Nebraska_Kansas_
South Atlantic:District of Columbia.Virginia_West Virginia_South Carolina_Florida_
East South Central:Mississippi_
West South Central:Louisiana_Texas_
Mountain:Montana_Idaho_Colorado_
Pacific:Washington_Oregon_California_Alaska_
United States, 1959_United States, 1958_
Water
11
<3
1,784
23
1,51163
98
~~2
53
628
206445
Milkandmilkpro¬ducts
48
20
18
49441
Otherfoods
182
781
18
21
114
14
901
322236
03o
7,434
306201220
1,442569
20291111013
283232715276
461030
1,0003
40
70123
366573
524
1,9302
10, 5959, 925
Includes outbreaks among military personnel.
ShigellosisAll outbreaks of shigellosis reported in 1960
were caused by Shigella sonnei infections. Onewaterborne outbreak following a breakdown in
916 Public Health Reports
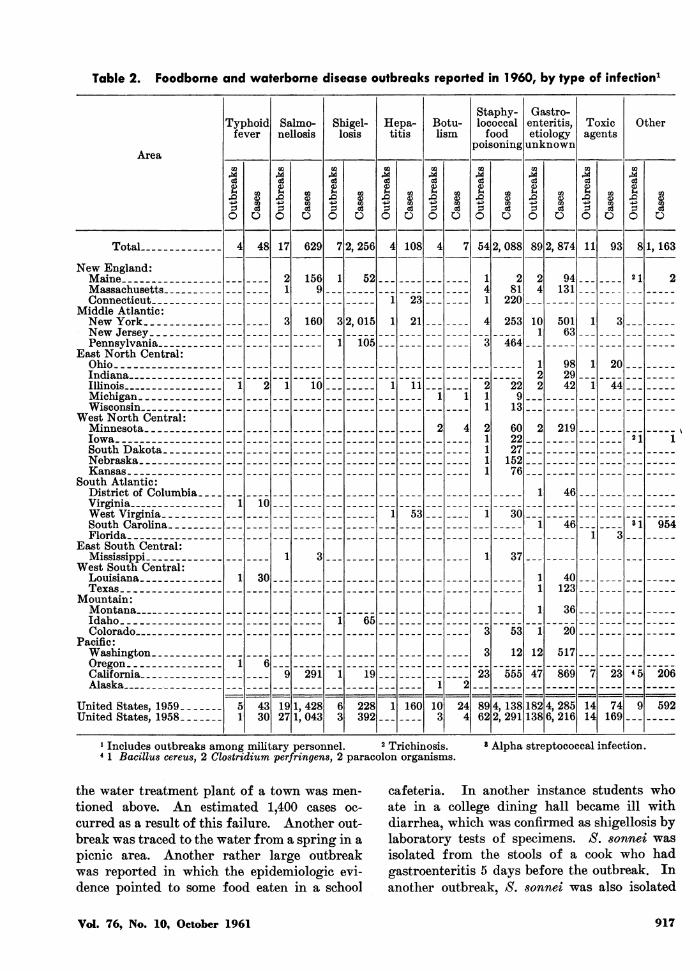
Table 2. Foodborne and waterborne disease outbreaks reported in 1960, by type of infection1
Area
Typhoid|fever
O
Salmo¬nellosis
O
Shigel¬losis
O
Hepa¬titis
c8O
Botu¬lism
c3O
Staphy¬lococcalfood
poisoning
O
Gastro¬enteritis,etiologyunknown
O
Toxicagents
O
Other
TotaL 48 17 629 2, 256 108 54 2, 088 89 2, 874 11 93 8 1,163New England:Maine_Massachusetts_Connecticut_
Middle Atlantic:New York_New Jersey_Pennsylvania_
East North Central:Ohio_Indiana_Illinois_Michigan_Wisconsin_
West North Central:Minnesota_Iowa_South Dakota.Nebraska_Kansas._
South Atlantic:District of Columbia.Virginia_West Virginia_South Carolina.Florida.._
East South Central:Mississippi_
West South Central:Louisiana_Texas_
Mountain:Montana_Idaho_Colorado_
Pacific:Washington_Oregon_California_Alaska_
1569
52
160 2, 01523
21
281
220
253
94131
n
50163
105 464
10 11 229
13
60222715276
982942
20
"44
219n
4610
53 3046 31 954
37
30;
65
291 19 23
53
12
"555
11
1
"l12
47
40123
36
""20517
"869 23
United States, 1959United States, 1958.
4330
1,4281,043
228392
160 244
4,1382,291
182138
4,2856,216
74169
206
592
1 Includes outbreaks among military personnel. 2 Trichinosis.4 1 Bacillus cereus, 2 Clostridium perfringens, 2 paracolon organisms.
Alpha streptococcal infection.
the water treatment plant of a town was men¬
tioned above. An estimated 1,400 cases oc¬
curred as a result of this failure. Another out¬break was traced to the water from a spring in a
picnic area. Another rather large outbreakwas reported in which the epidemiologic evi¬dence pointed to some food eaten in a school
cafeteria. In another instance students whoate in a college dining hall became ill withdiarrhea, which was confirmed as shigellosis bylaboratory tests of specimens. S. sonnei was
isolated from the stools of a cook who hadgastroenteritis 5 days before the outbreak. Inanother outbreak, S. sonnei was also isolated
Vol. 76, No. 10, October 1961 917
from a person who prepared potato salad fora buffet supper in a home.
HepatitisThe total number of hepatitis cases, including
both infectious hepatitis and serum hepatitis,reported in the United States increased fromabout 23,500 in 1959 to about 40,000 in 1960.There was also a relatively large increase incommon-source outbreaks of the disease inwhich water or food was considered to be thevehicle of infection. Epidemiologic investiga¬tions indicated that three outbreaks could beclassed as waterborne and one as foodborne.Two of the three waterborne outbreaks occur¬
red among school children whose drinking wa¬
ter at their schools came from wells. In eachinstance contamination of the wells with sew¬
age was demonstrated. The other outbreakaffected five different groups of persons whohad picnics in a park where, it was stated, thewater supply was inadequately chlorinated.Eleven students who had their meals in a col¬lege dining hall developed infectious hepatitis.Since one of the foodhandlers had been hos¬pitalized with hepatitis about 3 weeks prior toonset in the students, this outbreak probablycan be considered foodborne.
Botulism
Comparatively few cases of botulism were
reported in 1960. Two were in native Alaskan
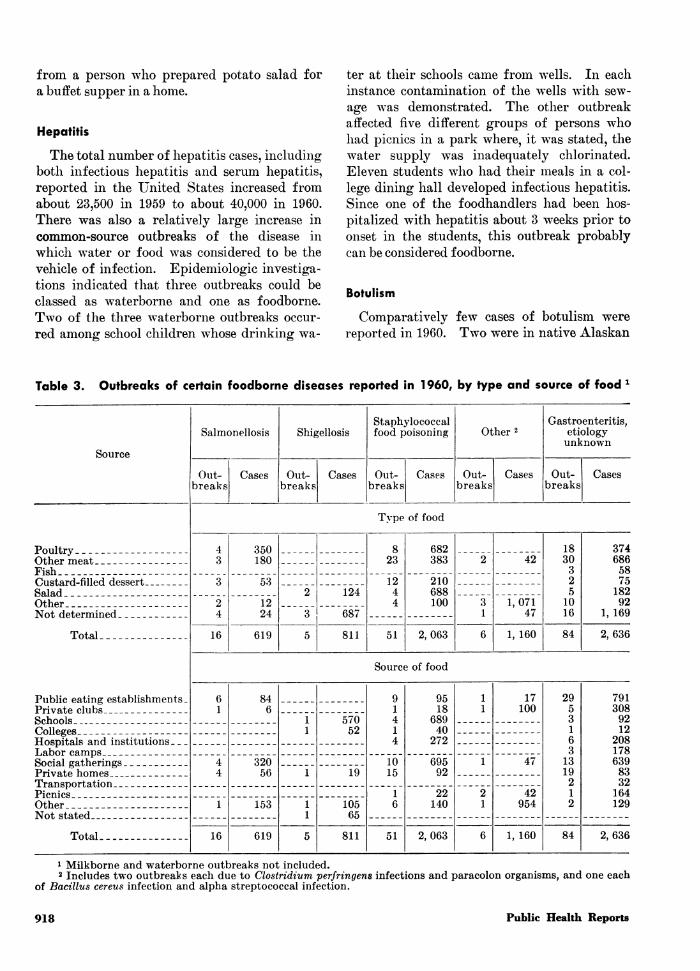
Table 3. Outbreaks of certain foodborne diseases reported in 1960, by type and source of food 1
Source
Poultry_Other meat_Fish_Custard-filled dessert_Salad_Other_Not determined_
Total
Public eating establishments.Private clubs_Schools_Colleges_Hospitals and institutions_Labor camps_Social gatherings_Private homes_Transportation_Picnics_Other_Not stated_
Total.
Salmonellosis
Out¬breaks!
Cases
Shigellosis
Out¬breaks!
Cases
Staphylococcalfood poisoning
Out¬breaks
Cases
Other 2
Out¬breaks
Cases
Gastroenteritis,etiologyunknown
Out¬breaks!
Type of food
16
350180
53
1224
619
124
687
811
23
1244
51
682383
210688100
2,063
42
1,07147
1, 160
Source of food
16
84
32056
153
619
57052
19
10565
811
1015
51
9518
68940
272
69592
22140
2,063
17100
47
42954
1, 160
18303251016
84
2953163
1319212
84
Cases
374686587518292
1, 169
2,636
7913089212
2081786398332164129
2,636
1 Milkborne and waterborne outbreaks not included.2 Includes two outbreaks each due to Clostridium perfringens infections and paracolon organisms, and one each
of Bacillus cereus infection and alpha streptococcal infection.
918 Public Health Reports
women who had eaten home-prepared salmonegg cheese. Frozen chicken pies were thesuspected source of toxin for two cases, frozenciscoes (fish) in two cases, and home-cannedgreen beans in one case. Five of the seven
cases reported were fatal.
Staphylococcal Food PoisoningThe 54 outbreaks of staphylococcal food poi¬
soning reported in 1960 were considerably few¬er than the 89 in 1959. Otherwise thereappeared to be little change from reports forprevious years. However, it may be noted thatthe number of cases per outbreak varied widelyfor the different types of food involved (table3). For instance, 383 cases were reported in 23outbreaks associated with the consumption ofmeat, while 688 cases in 4 outbreaks were tracedto salads. The same disproportions were pres¬ent for places where the food was served or
prepared.
Gastroenteritis, Etiology Unknown
Only about half as many foodborne andwaterborne outbreaks in which the etiology wasnot stated or determined were reported in 1960compared with 1959. The average for theprevious 4 years was 135. In more than halfof the 1960 outbreaks the suspected vehicle ofinfection was poultry or other meat. The pro¬portion caused by cream-filled foods was lessthan usual. About one-third were caused byfood served in public eating establishmentssuch as restaurants and hotels.
Chemical Poisoning and Noxious Foods
Four reports of chemical poisoning associatedwith the consumption of food or drink were
received. In one, a weedkiller containing ar¬
senic was accidentally introduced into the tankof a soft drink dispenser. One person becameill after eating peanut brittle that had been incontact with roach powder containing sodiumfluoride. Seven persons became acutely illafter drinking punch that had been left over¬
night in a copper-lined receptacle. A drinkconcocted by a child caused the death of threeplaymates. An insecticide containing parathion
was believed to have been used in the mixture.Another episode might be classed as chemicalpoisoning. After eating hamburger meat towhich sodium nicotinate had been added beforeits sale, 44 students noticed a flushing anditching of the skin.Two small family outbreaks of mushroom
poisoning were reported with no fatalities.Tung seeds caused severe gastroenteritis in threeworkmen who ate some of the nuts while un¬
loading them from a ship. Members of a fam¬ily complained of dizziness, blurred vision,nausea, and diarrhea after eating portions ofthe tree tobacco plant, Nicotiana glauca, whichwas mistaken for wild "greens." Only one
report was received of poisoning from fish, inthis instance smoked tuna.
Other Disease Outbreaks
In one of the outbreaks included in this cate¬gory, Bacillus cereus was believed to be theprobable etiological agent. Although variousfoods eaten by those affected were examined inthe laboratory, only one, roast beef, yielded a
culture of B. cereus. One of two outbreaks con¬
sidered to be due to Clostridium perfringenswas associated with consumption of roast beef.The other outbreak affected 100 picnickers whoate chile containing ground roast beef. Twooutbreaks due to paracolon organisms affected34 picnickers who ate meat sandwiches and 17persons who ate Chinese food in a restaurant.A large outbreak with 954 cases of an alpha
streptococcal infection occurred on a militaryinstallation. Giblet gravy left unrefrigeratedovernight was thought to be the vehicle ofinfection. The cook who prepared it had sore
throat prior to the outbreak.In contrast to previous years, only three epi¬
demiologic reports of trichinosis cases, were
received in 1960. For this reason the diseaseis included under "Other" in table 2.
Summary of Disease Outbreaks, 1951-60
In the 10-year period ended in 1960 about2,300 outbreaks were reported, 65, or about 3percent, of which were waterborne. The totalnumber of cases recorded was almost 100,000.The actual number of outbreaks and the average
Vol. 76, No. 10, October 1961 919

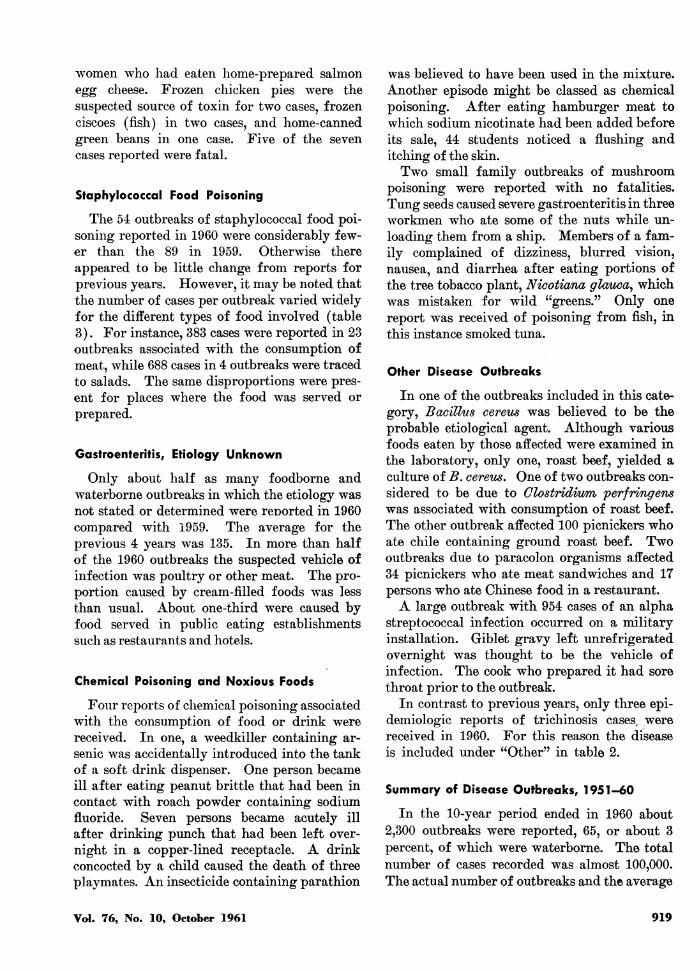
annual number per million population for eachState is shown in table 4 for two 5-year periods.The average number of outbreaks per millionpopulation was calculated for each State so thatmore valid comparisons could be made of thereporting in one State with that in another.The average number of outbreaks per million
population varied widely from State to State.In the 5-year period 1951-55 half of the Stateshad an average of less than one outbreak peryear and only 11 had an average of two or
more. The figures for the second 5-year periodshow that only a few more outbreaks were re¬
ported than in the previous 5 years. Therewere more States with an annual average ofless than one outbreak and only six States with
an average of two or more in this latter period.Twenty-one States reported fewer foodborneand waterborne outbreaks in the second 5-yearperiod than in the first.
It cannot be assumed that States reportingthe larger number of outbreaks per millionpopulation had inferior sanitary conditions inestablishments which prepared or sold foodproducts. They probably had higher rates be¬cause they encouraged and stimulated reportingand investigation to a greater degree than didthe States with lower rates. It has been ap¬parent for some time that certain large citiesreport no outbreaks and some report compara¬tively few. Many episodes are known to be in¬vestigated in some of these cities, but few are
Table 4. Number of foodborne and waterborne disease outbreaks reported and average annualnumber per million population, by State, 1951-55 and 1956-60
Area
Total-
Totalout¬
breaksre¬
ported
New England:Maine_New Hampshire_Vermont_Massachusetts_Rhode Island_Connecticut_
Middle Atlantic:New York_New Jersey_Pennsylvania-
East North Central:Ohio_Indiana-Illinois_Michigan_Wisconsin-
West North Central:Minnesota_Iowa_Missouri_North Dakota_South Dakota_Nebraska_Kansas_
South Atlantic:Delaware_Maryland_District of Columbia.Virginia_West Virginia_
1951-55
1,066
1222
434
25
23739
1827477
13
177
142315
1141910
Aver¬agepermil¬lionpopu¬lation
Totalout¬
breaksre¬
ported
1.4
3.4.8
1. 11.81.02.4
3.0. 1. 1
.41.31. 1.2.7
1. 1. 5.7.6.9. 1.5
.61. 1.2. 61.0
1956-60
1,274
3633
43814
991613
382153139
218
133372
0165
1714
Aver¬agepermil¬lionpopu¬lation
1.5
7.61.01.61.81.81.2
1.2.6.2
.8
.91. 1.3.5
1.2.6.6.9.91.0.2
01. 11.2.91.4
Area
South Atlantic.Con.North Carolina_South Carolina_Georgia_Florida_
East South Central:Kentucky_Tennessee-Alabama_Mississippi_
West South Central:Arkansas_Louisiana_Oklahoma_Texas_
Mountain:Montana_Idaho_Wyoming_Colorado_New Mexico_Arizona_Utah_Nevada_
Pacific:Washington_Oregon_California_Alaska_Hawaii_
Noncontiguous:Puerto Rico_
Totalout¬
breaksre¬
ported
1951-55
1516
12
312246
148310
17376451
4637
2732
Aver¬agepermil¬lionpopu¬lation
Totalout¬
breaksre¬
ported
0.7. 1.3
2. 11.3.3.6
1.6.6.3.2
.32.42. 11.01.6.91.31. 1
3.84.64.62.53.4
<. 1
1956-60
116
1211
16557
51526
292136311
7225
55334
1
Aver¬agepermil¬lionpopu¬lation
0.5.5.6.5
1.0.3.3.7
.5
.9
.2
. 1
.62.81.21.61.4.5.2.7
5.22.87.23.71. 1
<. 1
920 Public Health Reports
reported to State health authorities. It is alsoprobable that many foodborne disease outbreaksoccur, particularly family outbreaks, whichnever come to the attention of local authorities.
It has been variously and conservatively esti¬mated that the actual number of foodborne andwaterborne disease outbreaks is at least 10 to20 times larger than the reported number.This means that the number of cases occur¬
ring annually is of the order of 100,000 to200,000, a figure much greater than the ap¬proximately 10,000 presently reported.Another method of evaluating the reporting
in the United States is to compare its recordwith that of another country. A recent reporton food poisoning in England and Wales (1)shows that the average ammal number of "gen¬eral outbreaks," which are defined as two or
more cases in persons in different families, was9.8 per million population during the 5-yearperiod 1949-53. The rate for the UnitedStates, as shown in table 4, was 1.4 for the pe¬riod 1951-55. The average annual rate was10.6 in England and Wales for 1954-58 as com¬
pared with 1.5 for the United States in 1956-60. Not one of the United States had an
average annual rate equal to that of Englandand Wales as a whole. While procedures forcollecting information on foodborne diseaseand the method used to investigate outbreaksare different in the two countries, the differ¬ences in procedures probably do not explainthe wide differences in numbers of episodes re¬
ported in the two countries, nor may it be as¬
sumed that sanitary conditions in establish¬ments manufacturing, processing, or preparingfoods are much more inferior in the countrywith the higher rate. A more effective systemof collecting information in England and Walesprobably accounts for much of this wide differ¬ence in number of outbreaks.
Changes in Patterns of Infections
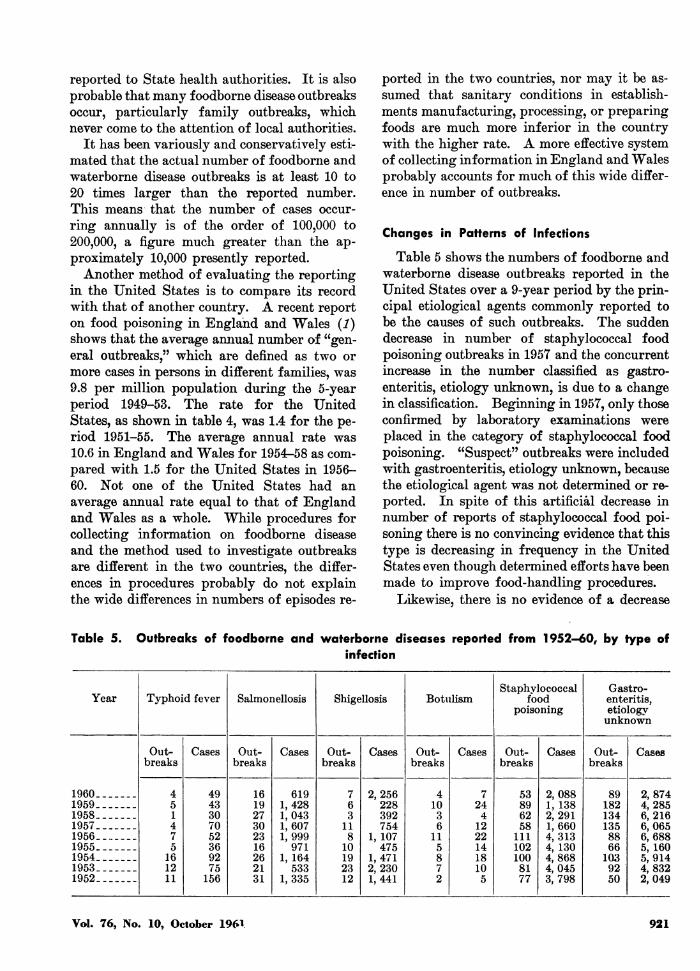
Table 5 shows the numbers of foodborne andwaterborne disease outbreaks reported in theUnited States over a 9-year period by the prin¬cipal etiological agents commonly reported tobe the causes of such outbreaks. The suddendecrease in number of staphylococcal foodpoisoning outbreaks in 1957 and the concurrentincrease in the number classified as gastro¬enteritis, etiology unknown, is due to a changein classification. Beginning in 1957, only thoseconfirmed by laboratory examinations were
placed in the category of staphylococcal foodpoisoning. "Suspect" outbreaks were includedwith gastroenteritis, etiology unknown, becausethe etiological agent was not determined or re¬
ported. In spite of this artificial decrease innumber of reports of staphylococcal food poi¬soning there is no convincing evidence that thistype is decreasing in frequency in the UnitedStates even though determined efforts have beenmade to improve food-handling procedures.
Likewise, there is no evidence of a decrease
Table 5. Outbreaks of foodborne and waterborne diseases reported from 1952-60, by type ofinfection
Year Typhoid fever Salmonellosis Shigellosis BotulismStaphylococcal
foodpoisoning
Gastro¬enteritis,etiologyunknown
1960.1959.1958.1957.1956.1955.1954.1953.1952.
Out¬breaks
451475
161211
Cases Out¬breaks
4943307052369275156
161927302316262131
Cases
6191,4281,0431,6071,999
9711, 164
5331,335
Out¬breaks
763
11810192312
Cases Out¬breaks
2,256228392754
1, 107475
1,4712,2301,441
41036
115872
Cases Out¬breaks
724412221418105
53896258
1111021008177
Cases Out¬breaks
2,0881,1382,2911,6604,3134, 1304,8684,0453,798
891821341358866
1039250
Cases
2,8744,2856,2166,0656,6885, 1605,9144,8322,049
Vol. 76, No. 10, October 1961 921

in the anmount of foodborne disease caused bySalm,onella orgailisms. The wide distributionof the ninny types of this organism in manyspecies of animals with which man lhas contactor may use as food makes it difficult, to pre-vent transmission to mani. The increasing useof chickens, turkeys, and ducks, and their eggsas food also contributes greatly to the incidencebecause these fowl are commonly infected withSalmonella organisms. In addition to the ani-mal sources of infection, human carriers andpatients have many opportunities to contami-nate food.
Etiological agents not previously associatedwith foodborne infection or disease in theUnited States were demonstrated during thepast decade. These included C. perfringens andB. cereus, which have been isolated in severaloutbreaks in recent years. The extent to whichthey contribute to foodborne disease in theUnited States has not been determined.
Since the early 1950's when hepatitis becamereportable in all of the States, it has becomeapparent that the disease is one of high fre-quency and often occurs in localized epidemics.An increasing number of the epidemics inrecent years have been waterborne according toevidence obtained in epidemiologic investiga-tions. Foodborne hepatitis had been suspectedbut good epidemiologic evidence of such trans-mission or association with a specific food wasnot obtained until quite recently.
Need for More Complete Reporting
A lack of enthusiasm regarding any attemptto improve the reporting of foodborne andwaterborne disease is readily apparent in someparts of the United States. Several factors maycontribute to this attitude. One possibility isthat the volume of reported illness has beenrelatively small. There is also a general im-pression that infectious diseases are no longeran important public health problem and thatother disease problems are paramount. Thisimpression may have been formed because ofthe remarkable decline in waterborne outbreaks
of typhoid fever, dysentery, and some otherenteric infections and the virtual disappearanceof milkborne epidemics of diphtheria, strepto-coccal sore throat, and typhoid fever. Alsosome of the infectious diseases have beenbrought under control, the severe effects ofothers have been counteracted by chemotherapy,and a few, such as measles, whooping cough,and streptococcal infections, have declined inseverity.On the other hand, there is good reason to
believe that foodborne diseases and, to a lesserextent, waterborne diseases, are still widelyprevalent; neither can be measured in terms ofreported incidence. Consequently, it can beargued persuasively that there is a real need toimprove the reporting of both waterborne andfoodborne illness as the first step in the develop-ment of effective control measures. There alsois real need to study more intensively and ex-tensively the epidemiology of staphylococcalfood poisoning and Salmonella infections be-cause their causative agents are widely distrib-uted and their ecologic factors are complex.The relationship of the many phage types ofstaphylococci which cause septic infections tofoodborne illness needs to be determined moreaccurately, and the ecology of the hundreds ofsalmonellae serotypes found in man and animalsneeds more extensive study. The relative im-portance and frequency of illness due to etio-logical agents not previously associated withfoodborne disease in the United States shouldbe determined. The increasing frequency ofcommon-source epidemics of infectious hepatitisreported recently suggests the need for morecareful investigation of their epidemiologicfactors. The lack of information on these as-pects of foodborne and waterborne diseases isample justification for making more thoroughepidemiologic and microbiological investiga-tions and for more complete reporting.REFERENCE
(1) Cockburn, W. C.: Food poisoning: reporting andincidence of food poisoning. Roy. SocietyHealth J. 4: 249, July-August 1960.
922 Public Health Reports