18 october 20101 pregnant women & clinical trials: scientific, regulatory, and ethical...
TRANSCRIPT

18 October 2010 1
Pregnant Women & Clinical Trials: Scientific, Regulatory, and Ethical Considerations
Karen Feibus, MD, Medical Team LeaderPediatric and Maternal Health Staff (PMHS), Maternal Health Team, Office of New Drugs
CDER/FDASara F. Goldkind, MD, MA, Senior Bioethicist
Office of Good Clinical Practice, OC/FDA
Views expressed are those of the speaker and don’t reflect the official position of the FDA

18 October 2010 Issues in Clinical Research: Enrolling Pregnant Women 2
Objectives
Explore ethical considerations for drug development research in pregnant women
Examine different ways to obtain data in pregnant women during various stages of the drug development process
Premarketing vs. postmarketing
Clinical trials vs. epidemiological studies
Enrolling pregnant women vs. continuation of women who become pregnant in a clinical trial
Study design considerations Informed consent
Outcomes measures
Pharmacokinetics

18 October 2010 Issues in Clinical Research: Enrolling Pregnant Women 328 July 2010 Prescribing Risks in Women Veterans of Childbearing Age
3
What should I consider when prescribing for women of childbearing potential?
What is my patient’s underlying medical condition? Is pharmaceutical treatment essential for her long term health
and her daily quality of life?
Is her medical condition well managed on her current medications?
What are the reproductive/developmental risks of her medications?
What is this based on? Are there any other data available that are not in the drug labeling?
Are there other medications that treat her underlying condition that have better developmental risk profiles?
Are these alternatives appropriate for her?
Have I informed my patient about the reproductive risks of her medicines and discussed the relative risk/benefits of appropriate therapies?
If she was pregnant, what would I do differently?

18 October 2010 4
“I Don’t Know”
is not an acceptable or fair answer to these questions.

18 October 2010 Issues in Clinical Research: Enrolling Pregnant Women 5
Basic Principles: an ethical and scientific foundation
Agree with the following principles outlined by Faden, Little, and Lyerly through the Second Wave*:
“Women need effective treatment during pregnancy”
“Fetal safety”: Data are needed on fetal safety Inadequately treated mother compromises fetal well being
“Reticence to prescribe needed medications: the cost of uncertainty”
What are the risks of not treating or under treating the mother’s condition?
“Issues of justice and access to the benefits of research participation”
*Lyerly AD, Little MO, Faden R. The second wave: Toward responsible inclusion of pregnant women in research. Int J Fem Approaches Bioeth 2008 Fall; 1(2): 5-22.

18 October 2010 Issues in Clinical Research: Enrolling Pregnant Women 6
Basic Principles: an ethical and scientific foundation
The most compelling reason to justify the inclusion of pregnant women in a greater number of biomedical studies is the need for evidence gathered under rigorous scientific conditions that place fewer women and their fetuses at risk than the much larger number of pregnant women who will be exposed to the medications once they come to market.
The next logical-and ethical-step is the enrollment and retention of pregnant women in clinical trials.”
*Macklin, R. The art of medicine: Enrolling pregnant women in biomedical research. The Lancet February 20, 2010; 375: 632-3.
18 October 2010 Issues in Clinical Research: Enrolling Pregnant Women 7
Basic Principles: an ethical and scientific foundation
Research in pregnant women should only be done where there is need, but once need is identified, exclusion of pregnant women must be justified.
CIOMS: Pregnant women should be presumed eligible for participation in
biomedical research.
Research in pregnant women should be performed only if: It is relevant to the particular health needs of a pregnant woman or her
fetus, or
It is relevant to the health needs of pregnant women in general, and
When appropriate, it is supported by reliable evidence from animal experiments, particularly as to risks of teratogenicity and mutagenicity.
Protocols should include a plan for monitoring pregnancy outcomes, including maternal health and short-term and long-term health of the child.
*The Council for International Organizations of Medical Sciences (CIOMS) in collaboration with the World Health Organization (WHO), Guideline 17.

18 October 2010 Issues in Clinical Research: Enrolling Pregnant Women 8
In drug regulatory science,Who are pregnant women?
Pregnant women are NOT a separate and distinct population except when a drug specifically treats a condition unique to pregnancy
Pregnant women are a dynamic subset of the adult and adolescent female populations who use drugs and biologics
It is important to ALWAYS consider whether, when, and how to study pregnant women in the drug development process
Adult and adolescent women
Pregnant women

18 October 2010 Issues in Clinical Research: Enrolling Pregnant Women 9
Subpopulation differences:Pregnant women vs. non-pregnant women
Drug efficacy and safety can not be entirely extrapolated from non-pregnant women to pregnant women
Pregnancy physiology affects pharmacology Changes in total body weight and body fat composition
Expansion of plasma volume
Increase cardiac output
Changes in regional blood flow
Increase in GFR Altered GI motility
Decrease in Albumin
Changes in hepatic enzyme activity and drug metabolism by CYP450 system

18 October 2010 Issues in Clinical Research: Enrolling Pregnant Women 10
Stages and phases:the clinical drug development process
When?When? Pre-marketing? Post-marketing?
How?How? Randomized controlled trial vs. cohort or case-control study Careful development program from the outset including statistical
analysis considerations
Who?Who? Pregnant women for whom the study drug offers potential direct benefit
Pregnant women already using the drug therapeutically Women who become pregnant while on study drug
Phase 1 Phase 2 Phase 3 Phase 4
Pre-marketing Post-marketing
Drug approvedfor marketing
18 October 2010 Issues in Clinical Research: Enrolling Pregnant Women 11
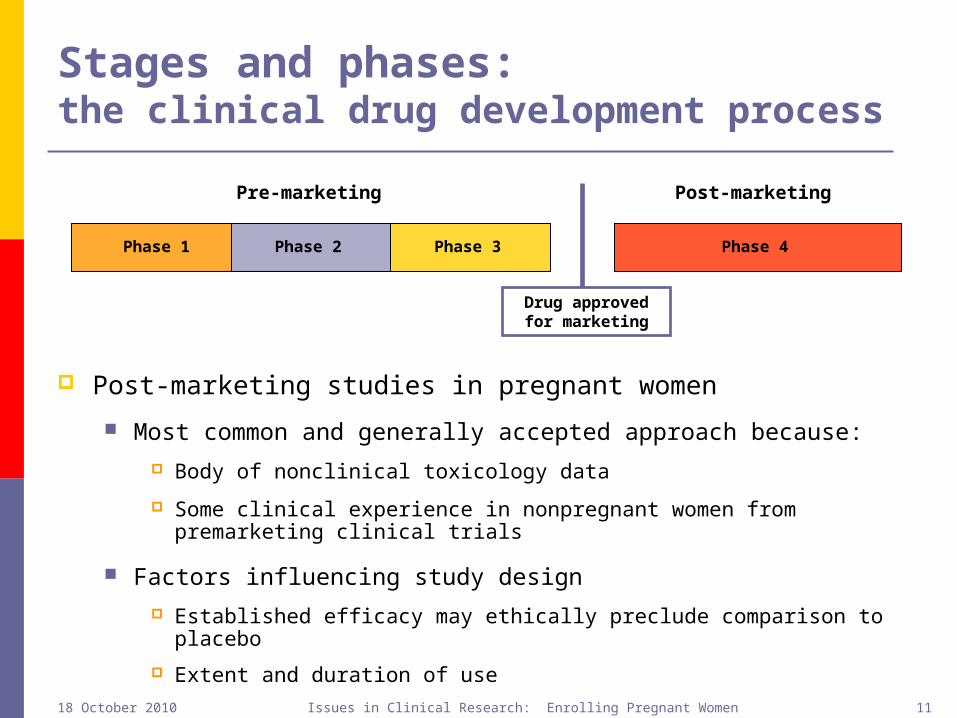
Stages and phases:the clinical drug development process
Post-marketing studies in pregnant women
Most common and generally accepted approach because: Body of nonclinical toxicology data
Some clinical experience in nonpregnant women from premarketing clinical trials
Factors influencing study design Established efficacy may ethically preclude comparison to placebo
Extent and duration of use
Phase 1 Phase 2 Phase 3 Phase 4
Pre-marketing Post-marketing
Drug approvedfor marketing

18 October 2010 Issues in Clinical Research: Enrolling Pregnant Women 12
Post-marketing studies in pregnant women
Pregnancy exposure registry
Prospective cohort study with an internal or external control group
Postmarketing requirements under the FDA Amendments Act of 2007
For drugs marketed for an extent of time
Database studies with mother/baby record linkage
Case control studies
Clinical trials
Placebo control or active control

18 October 2010 Issues in Clinical Research: Enrolling Pregnant Women 13
Stages and phases:the clinical drug development process
Pre-marketing studies: questions to consider:
Are preclinical reproductive and developmental toxicity studies complete and adequate?
Are there positive findings of developmental toxicity in animals?
Are effective alternative therapies with better documented developmental toxicity profiles available?
What are the risk/benefit considerations for mother and fetus with regard to the drug and the condition it is intended to treat?
Phase 1 Phase 2 Phase 3 Phase 4
Pre-marketing Post-marketing
Drug approvedfor marketing

18 October 2010 Issues in Clinical Research: Enrolling Pregnant Women 14
Stages and phases:the clinical drug development process
Pre-marketing studies: questions to consider:
Placebo control or active control with established therapy?
Do pregnant women have access to other effective therapies?
Are there planned PK assessments early in the study to ensure adequate systemic exposure to achieve efficacy (e.g., nested PK study in Phase 3 clinical trial)?
Does the protocol support retention of woman in the clinical trial if pregnancy occurs? (examples on slide 21)
Phase 1 Phase 2 Phase 3 Phase 4
Pre-marketing Post-marketing
Drug approvedfor marketing

18 October 2010 Issues in Clinical Research: Enrolling Pregnant Women 15
Plan ahead: for pregnant women’s participation in clinical trials
Two potential scenarios:
Women who become pregnant during a clinical trial
Clinical trials that enroll pregnant women
18 October 2010 Issues in Clinical Research: Enrolling Pregnant Women 16
Women who become pregnant while in clinical trials
When should a women who becomes pregnant while enrolled in a clinical trial be allowed to continue on study drug?
If the potential benefits of continued treatment outweigh the:
potential risks of ongoing fetal exposure to study drug,
risks of discontinuing maternal therapy, and/or
risks of exposing the fetus to additional drugs if the mother is placed on an alternative therapy
For example, malaria, tuberculosis, cancer

18 October 2010 Issues in Clinical Research: Enrolling Pregnant Women 17
Women who become pregnant while in clinical trials
Consented as a nonpregnant woman
Contraceptive counseling
Potential embryo-fetal toxicity counseling
If become pregnant, need: Pregnancy management counseling New informed consent as pregnant study subject
Discuss alternative therapies and comparative therapeutic risks and benefits
Risk of ongoing fetal exposure to study drug vs. risk of fetal exposure to the study drug and the new alternative therapy.
Risk of untreated maternal disease

18 October 2010 Issues in Clinical Research: Enrolling Pregnant Women 18
Enrolling pregnant women in clinical trials
Pregnant women with a medical condition requiring treatment may be involved in clinical trials if: Access to drug holds out the prospect of direct benefit to the
pregnant woman that is not otherwise available to her
Pregnant women have not clinically responded to other available therapies
Alternative therapies are not effective (e.g., drug allergy, drug intolerance, or drug resistance)
The risk to the fetus is not greater than minimal and important knowledge is acquired (which cannot be obtained by other means)
Adequate preclinical studies (reprotox) are complete
Pregnant women are prescribed the drug for therapeutic reasons

18 October 2010 Issues in Clinical Research: Enrolling Pregnant Women 19
Addressing Challenges to Clinical Research in Pregnant Women
Recruitment and retention for studies conducted in both the premarket and postmarket settings
Identifying potential subjects Educating women
Lack of data on the use of medicines during pregnancy The values of research participation (pregnancy registries,
clinical trials) Sharing and securing personal information
Understanding factors that influence women’s likelihood to enroll and continue in clinical research during pregnancy
Overcoming fears and misconceptions in the research community

18 October 2010 Issues in Clinical Research: Enrolling Pregnant Women 20
Artemether/lumefantrine treatment of malaria in pregnant women
Originally marketed outside the United States
Published and unpublished data on treatment of pregnant women with artemether/lumefantrine
FDA approved in 2009
Pregnancy labeling:
Safety data from an observational pregnancy study of approximately 500 pregnant women who were exposed to Coartem Tablets (including a third of patients who were exposed in the first trimester), and published data of over 1,000 pregnant patients who were exposed to artemisinin derivatives, did not show an increase in adverse pregnancy outcomes or teratogenic effects over background rate.
Clinical trials with PK, efficacy, and safety assessments

18 October 2010 Issues in Clinical Research: Enrolling Pregnant Women 21
Study protocol considerationsfor pregnant women
Protocols should include the following:
Address informed consent Risk/benefit considerations with regard to fetal exposures and maternal
well being Therapeutic alternatives to clinical trial enrollment
Study endpoints and data collection mechanisms to capture maternal, fetal, and neonatal outcomes of interest
Gestational dating Gestational timing and duration of drug exposure Collection of ultrasound reports and results of other prenatal testing Records of maternal complications Pregnancy outcomes
Gestational age at delivery
Delivery complications
Condition of the neonate and complications in the neonatal period

18 October 2010 Issues in Clinical Research: Enrolling Pregnant Women 22
FDA Guidances Pregnancy Exposure Registries:
Guidance for Industry, Establishing Pregnancy Exposure Registries, final published August 2002
Pharmacokinetics: Industry Guidance (draft), Pharmacokinetics in Pregnancy - Study
Design, Data Analysis, and Impact on Dosing and Labeling, draft published October 2004.
Final guidance in clearance – Pharmacokinetics During Pregnancy and the Postpartum Period.
Clinical Lactation Studies: Industry Guidance (draft), Clinical Lactation Studies-Study
Design, Data Analysis and Recommendations for Labeling, draft published February 2005.
Final guidance in clearance
Pregnant women and clinical trials: Industry Guidance, Pregnant Women in Clinical Trials: Scientific
and Ethical Considerations, draft in clearance

18 October 2010 Issues in Clinical Research: Enrolling Pregnant Women 23
Contact information
Karen Feibus, MD, clinical team leader (301)796-0889 [email protected]
Sara F. Goldkind, MD, MS, Senior Bioethicist (301) 796-8342 [email protected]