16 short course:”critical care in cardiothoracic surgery ...thaists.org/news_files/news_file_626....
TRANSCRIPT

16th Short Course:”Critical Care in Cardiothoracic Surgery” Perfusionist Session:Running ECMO:How I do it
Friday ,May 16,2014 Novotel Bangkok on Siam Square

Who need ECMO?

Respiratory ECMO vs
Cardiac ECMO





VV ECMO vs
VA ECMO

VA ECMO
Veno-Arterial Support (Fem-fem bypass)
Jugular vein
Aorta
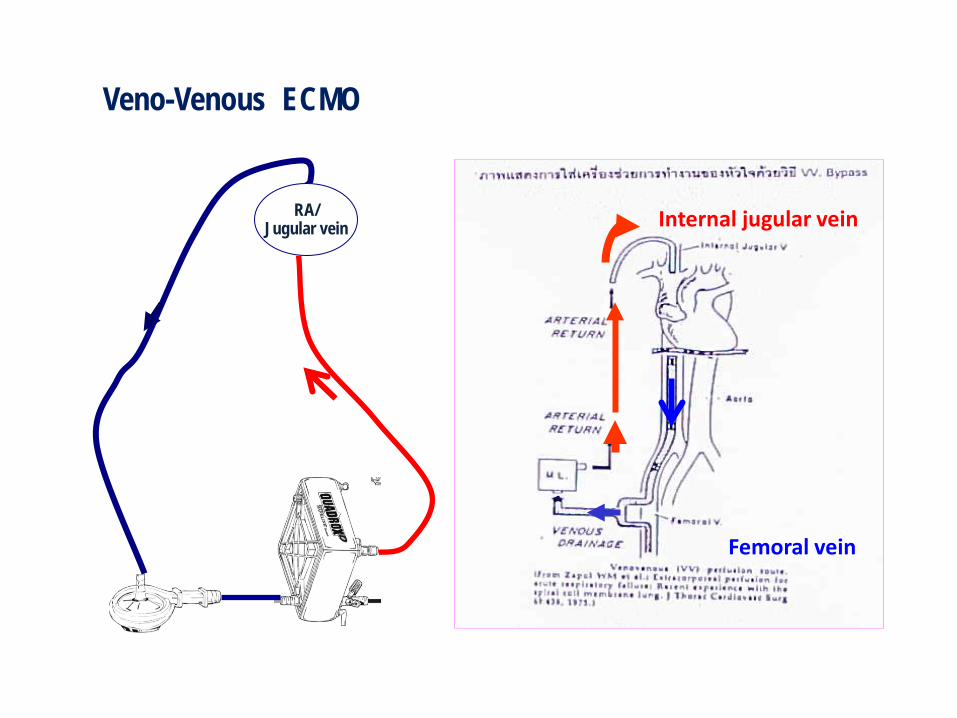
RA/ Jugular vein
Veno-Venous ECMO
Femoral vein
Internal jugular vein

Closed system vs Open system
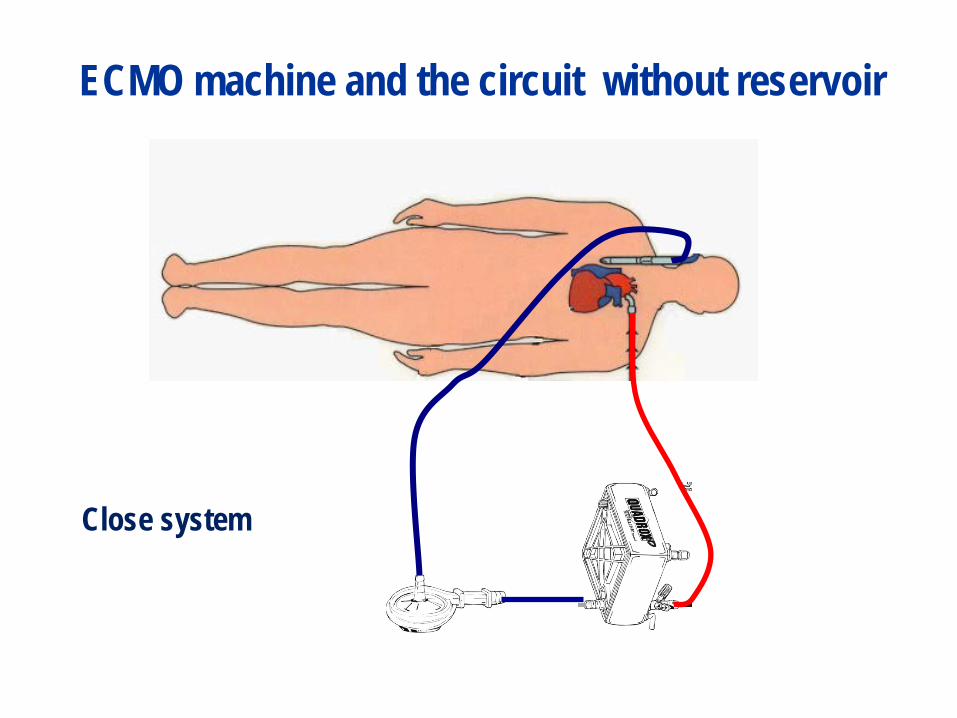
ECMO machine and the circuit without reservoir
Close system

pump
Blood drained from the venous circulation and return to the arterial circulation
oxygenator
ECMO circuit with reservoir Open system
VA ECMO

Cardiac ECMO
RAAorta Central VA ECMO

ECMO equipment and circuit

ECMO Components
Commercial set ราคา 6-80,000 บาท
ไมรวม Hemoconcentrator
Close system

Close system & centrifugal pump

Homemade set รวม Hemoconcentrator ราคา 19,600 บาท
Open system



Parameters for assessment
-HR -BP -CVP -Metabolic acidosis -Capillary refill -Pulses -Temperature of extremities
-Neurological sign status -GI status -Intake&output

Biomarker of systemic circulatory failure

VA ECMO

VV ECMO

VA ECMO
VV ECMO

-Blood flow -Oxygen delivery -Oxygen consumption -Venous saturation -Serum Lactate level -Urine output

3.3 3.3 3.2 3
2.8 3
3.5 3.5 3.5 3.5
0
0.5
1
1.5
2
2.5
3
3.5
4
baseline 6hr 12hr 24hr ECMO day 2 ECMO day 3 ECMO day 4 ECMO day 5 ECMO day 6 ECMO day 7
Pump flow (L/min)
ECMO pump flow target 80-100 cc/kg/min
Blood flow (n=9)

396
667
560 597 592 584
552 581 561
533
0
100
200
300
400
500
600
700
800
baseline 6hr 12hr 24hr ECMO day2
ECMO day3
ECMO day4
ECMO day5
ECMO day6
ECMO day7
Oxygen Delivery during ECMO (n=9)
Normal DO2 520-720 ml/min
DO2 = arterial oxygen content x pump flow x 10

0
20
40
60
80
100
120
140
160
baseline 6hr 12hr 24hr ECMO day 2 ECMO day 3 ECMO day 4 ECMO day 5 ECMO day 6 ECMO day 7
Mean Oxygen consumption during ECMO
VO2 = Art.O2 - Venous O2 content x Flow (L/min) x 10 normal VO2 = 100 -180 ml/min
Oxygen Consumption (VO2) n=9
Increase in metabolism/ Seizures Decrease in Hb /CO
Increase Oxygen depth

Venous saturation (SVO2) n=9
SVO2 65-75% reflective of adequate cardiopulmonary function or ECMO support
0102030405060708090
100
baseline 6hr 12hr 24hr ECMO day 2 ECMO day 3 ECMO day 4 ECMO day 5 ECMO day 6 ECMO day 7
SVO2
mixed venous oxygen saturation (SVO2) เปนคาหนงทแสดงถงความสมดลของ
รางกายระหวางความตองการออกซเจน (oxygen consumption) และการสงออกซเจนไปเลยงเนอเยอตางๆ (oxygen delivery)

Factors affecting DO2,VO2,SVO2
-Hb -PaO2 -Oxygen saturation -Oxygen extraction or O2 demand -Blood flow (CO)

7.4
9.4
8.7
9.0
8.6 8.7
7.9
8.8
8.4
7.9
6.5
7
7.5
8
8.5
9
9.5
10
baseline 6hr 12hr 24hr ECMO day 2 ECMO day 3 ECMO day 4 ECMO day 5 ECMO day 6 ECMO day 7
Mean Hb during ECMO

Degree of hemodilution- low peripheral oxygen delivery
Temperature Systemic vascular resistance-hypoperfusion
Prolong cardiopulmonary bypass time
Vasopressor drugs
Perfusion related factors
Hyperlactatemia
Severe acidosis and tissue hypoxia

15.2
17.8
15.4
19.3 18.4
21 19.5
22 20.6
19.7
0
5
10
15
20
25
baseline 6hr 12hr 24hr ECMO day 2 ECMO day 3 ECMO day 4 ECMO day 5 ECMO day 6 ECMO day 7
Normal Serum Lactate level 0.5-1 mmol/L
Serum Lactate changes during ECMO

ECMO management (ชวยผปวยไดอยางไร?)

0
0.5
1
1.5
2
2.5
3
3.5
4
baseline 6hr 12hr 24hr ECMO day 2 ECMO day 3 ECMO day 4 ECMO day 5 ECMO day 6 ECMO day 7
Pump flow (L/min)
Pump takeover heart function 100%
Increase pump flow rate to maintain blood pressure
X
ECMO pump flow target 100-120 cc/kg/min
Very poor EF ECMO pump flow target 80-100 cc/kg/min
Blood flow (n=9)

396
667
560 597 592 584
552 581 561
533
7.4
9.4 8.7
9.0 8.6 8.7
7.9
8.8 8.4
7.9
0
1
2
3
4
5
6
7
8
9
10
0
100
200
300
400
500
600
700
800
baseline 6hr 12hr 24hr ECMO day 2 ECMO day 3 ECMO day 4 ECMO day 5 ECMO day 6 ECMO day 7
Relationship between mean DO2 and mean Hb level
DO2
Hb
Oxygen Delivery
Hematologic management : Target Hb 12 -15gm%
Massive bleeding & massive transfusion
Maintain DO2 in normal range

1200
1648
1333
1550
1360
1229 1307
1006 1097
1029
42
68
55
62
51
43
49 44
48 45
0
10
20
30
40
50
60
70
80
0
200
400
600
800
1000
1200
1400
1600
1800
baseline 6hr 12hr 24hr ECMO day 2 ECMO day 3 ECMO day 4 ECMO day 5 ECMO day 6 ECMO day 7
MAP & SVR changes during ECMO
SVR MAP
X
X
Antihypotensive Agents

137
104
80 69
54
37
16 5 0 0
-20
0
20
40
60
80
100
120
140
160
baseline 6hr 12hr 24hr ECMO day 2 ECMO day 3 ECMO day 4 ECMO day 5 ECMO day 6 ECMO day 7
Mean Urine output during ECMO (cc/hr) Target 2 cc/kg/hr

nongchana klangsuk,Rajavithi Hospital
• continuous ultrafiltration • Hemodiafiltration • Cell washing / Lactate Removal / (Hemodilution with Hemoconcentration technique)
Filtration Techniques

142 145
139 135 134
138 135
141
149
141
125
130
135
140
145
150
155
baseline 6hr 12hr 24hr ECMO day 2 ECMO day 3 ECMO day 4 ECMO day 5 ECMO day 6 ECMO day 7
Serum Sodium level during ECMO
3.2
4.8 4.3 4.4
4.9 4.7 4.4 4.0
5.8 5.1
0.0
1.0
2.0
3.0
4.0
5.0
6.0
7.0
baseline 6hr 12hr 24hr ECMO day 2 ECMO day 3 ECMO day 4 ECMO day 5 ECMO day 6 ECMO day 7
serum potassium level during ECMO
Changes in small size molecular weight: mean potassium concentration, mean sodium concentration
137
104
80 69
54 37
16 5 0 0
-200
20406080
100120140160
baseline 6hr 12hr 24hr ECMO day 2 ECMO day 3 ECMO day 4 ECMO day 5 ECMO day 6 ECMO day 7
Mean Urine output during ECMO (cc/hr)

0
5
10
15
20
25
baseline 6hr 12hr 24hr ECMO day 2 ECMO day 3 ECMO day 4 ECMO day 5 ECMO day 6 ECMO day 7
Cell washing Technique
Non Lactate remove
Lactate Remove

Left heart decompression during ECMO
PA /Apex venting
OPEN CHEST

Protein derangement during ECMO
Foreign surface contact PLT function Thrombocytopenia Loss of coagulation factors
Minimize by good anticoagulation Use: -albumin / FFP/Platelets -Aprotinin -Methypredisolone (SoluMedrol) -Hemofiltration

Complications
Bleeding
Thrombus
Anticoagulation Anticoagulation

Coagulation monitoring Maintain ACT 180-200 sec Check ACT ทก 2 hrs.
ถาม Bleeding รอบๆ cannulae ใหใช pressure dressing
ถามปญหา heparin resistance ทมสาเหตจาก
AT III ใหFresh Frozen Plasma
หมนตรวจด Clot formation ใน สายและHead pump

Anticoagulation Protocol
• Post operative insertion of ECMO
– No protamine
• Heparin by infusion
– Do not start heparin until bleeding has stopped
– ACT for the first 24 hours 180-200 seconds
• Platelets transfusion ≥100,000/mm3

540
243
194 210
237 258
227 244
229 233
0
100
200
300
400
500
600
baseline 6hr 12hr 24hr ECMO day 2 ECMO day 3 ECMO day 4 ECMO day 5 ECMO day 6 ECMO day 7
mean ACT level during ECMO
Activated clotting time (ACT) 200- 250 sec. Target ACT:
Bleeding
Thrombus
Anticoagulation Anticoagulation

Coagulation monitoring Look for signs of coagulation impairment active bleeding hemorrhagic diathesis
Check: skin & mucosa

Vascular observations of lower limbs Limb temperature Limb colour Pedal pulse Capillary refill Size
Mechanical complications
• Oxygenator malfunction
• Pump malfunction
• Tubing rupture
• Cracks in connectors
• Air / clot in circuit
• Cannulation displacement/ kink
• Power failure

Oxygenator monitoring Check for Clot & thrombus Air Plasma leak

Pump head monitoring
ตรวจสอบทงระบบ คอ pump head, oxygenator & tubing

Connections monitoring

Cannulae and lines monitoring

Notify M.D.
• Vital signs outside of ordered parameters • Any deterioration in assessment status • Bleeding >10 ml/hour from cannulae site • Change in level of sedation

Indicators for improvement
• Indicator of lung recovery – SVO2 – pO2 – pCO2 – Increase compliance – Cleansing chest X-ray
• Improving contractility • Urine out put • Vital signs • Pump blood flow • Blood gas

ประโยชนของ ECMO • Useful therapy for the support of both
cardiac and respiratory failure patients
• Easy & Quickly to deploy (dedicated therapy)
• cheap

Overall out come

Results • Respiratory support
– Neonatal respiratory support 77% survival to discharge
– Paediatric support 56% survival
– Adult 53% survival
• Cardiac support – Neonate 38% survival
– Paediatric 43% survival
– Adult 33% survival

Indications for use : Rajavithi Hospital
a. Bridge to transplantation b. Perioperative Hemodynamic instability c. Postoperative myocardial / lung dysfunction

Operations (1 Jan 2554- 31 Dec 2556)
Age Bypass time
Days of support
Type of Support
Result Complications
IE&AVR&shock 40 yrs 3 hrs 45 min 3 AV ECMO A Bleeding
Redo AVR&CABG 65 yrs 1 hrs 57 min 2 AV ECMO A Bleeding
Heart Transplantation 26 yrs 3 hrs45min 2 AV ECMO & IABP
A Bleeding
Redo AVR & root replacement 32 yrs 6hrs48 min 3 AV ECMO & IABP
A* Bleeding & Myocardial
failure
CABG 74 6 hrs 23 min 16 hrs AV ECMO &LVAD& IABP
D Myocardial failure
CTOF 31 yrs 2 hrs12min 5 VV ECMO &RVAD&IABP
D Bleeding& Myocardial
failure
Redo AVR&MVR 40 yrs 6 hrs 40 min 8 AV ECMO D Bleeding
Redo Hemi Arch replacement
66 yrs 5 hrs 45min 8 AV ECMO D Bleeding
Single Lung Transplantation 52 yrs Non CPB 14 AV ECMO D Bleeding
44.5% survival rate in Adult Cardiac ECMO
CVT Unit, Rajavithi Hospital

Operations (1 Jan 2554- 31 Dec 2556)
Age Bypass time
Days of support
Type of Support
Result Complication
Rastelli’s operation 3 yrs 2 hrs19 min 7 AV ECMO A bleeding
Redo Ao. Root replacement &
Aortic Homograft
7 yrs 6 hrs29min 9 AV ECMO
D bleeding
Redo Ao. Root replacement &
Aortic Homograft
6 yrs 5 hrs 26 min 2 AV ECMO D bleeding
33% survival rate in Pediatric Cardiac ECMO

Result ไมดทาไปทาไม? -ใหโอกาส recover (Bridge to -รอ Tx (Bridge to Transplant -ซอเวลา (Bridge to Destinatio

Important: ECMO is offered only to patient/child whose lung and/or heart disease is thought to be reversible.

Gaba DM, Fish KJ, Howard SK: Crisis Management in Anesthesia 1994