15-weglinski-what's new in malignant...
TRANSCRIPT
What’s New in Malignant Hyperthermia
Margaret Weglinski, M.D. Department of Anesthesiology & Perioperative Medicine
Mayo Clinic Rochester, MN
Anaesthetic Deaths in a Family
21 yo male with fracture of tibia/fibula 10 relatives died during or after ether Local anesthesia for appendectomy New agent used (halothane) Developed MH, but survived Later completed surgery under spinal anesthesia
Denborough MA and Lovell RRH. Lancet 1960; 2:45 Denborough MA et al. Br J Anaesth 1962; 34:395-6
Lessons Learned
Patients otherwise healthy until exposed to certain anesthetic agents Temperature elevation is a hallmark High mortality rate Possible to abort the syndrome with early recognition and treatment Genetic component (autosomal dominant pattern)
Outline
Review – Pathophysiology – Clinical presentation – Management of crisis Update – Ryanodex – Genetic testing – MH in ambulatory surgery centers – “Awake” MH

What is MH?
“MH is a serious and potentially life-threatening hypermetabolic skeletal muscle disorder induced in response to certain anesthetics in genetically susceptible individuals”
Wong CA, Denholm B. Anesthesiology News, December 2011
MH Triggers
Inhaled volatile general anesthetics – Desflurane, sevoflurane, isoflurane, halothane,
etc. Succinylcholine
JAMA. 293(23):2918-2924, June 15, 2005.
Litman RS, Rosenberg H. JAMA 2005;293,2918
Clinical Presentation of MH
Presentation may vary (both in symptoms and timing) Patient may have had GA in the past without difficulty Disorders associated with MH – Central Core Disease – King Denborough Syndrome

Clinical Presentation of MH
Increase in end-tidal CO2 – Most reliable initial clinical sign – CO2 production exceeds capacity to
compensate with ventilator changes – Soda lime is rapidly exhausted and warm to
touch
Clinical Presentation of MH
Temperature – Muscle contraction is major source of heat
production – Heat causes further rise in metabolic activity
and stimulates procoagulant pathways – Where to monitor temperature
MH swine model: skin temperature does not correlate with core temperature
Iaizzo PA et al. Anesth Analg 1996;82:782-9
Clinical Presentation of MH
Temperature – MH Deaths Related to Inadequate
Temperature Monitoring, 2007-2012 Hyperthermia was first sign of MH in 1/3 of patients Hyperthermia was one of three early signs of MH in 2/3 of patients Survival related to core temperature monitoring
– MHAUS: Monitoring standards should require core temperature monitoring for all GA lasting 30 minutes or longer
Larach MG et al. Anesth Analg 2014;119:1359-66
Clinical Presentation of MH
Muscle rigidity – Masseter muscle spasm after succinylcholine – Generalized muscle rigidity
Highly specific for MH
Rhabdomyolysis – Tea-colored urine – Hyperkalemia (peaked T-waves, arrhythmias)
Clinical Presentation of MH
Laboratory findings – ABG: increased PaCO2 – Metabolic (lactic) acidosis – Evidence of rhabdomyolysis
Hyperkalemia Increased plasma creatine kinase Myoglobin in blood and urine
– Abnormal coagulation tests
Early Diagnosis is Key
Requires vigilance and high index of suspicion MH reaction can become irreversible Exploration of differential diagnosis should not delay initiation of therapy
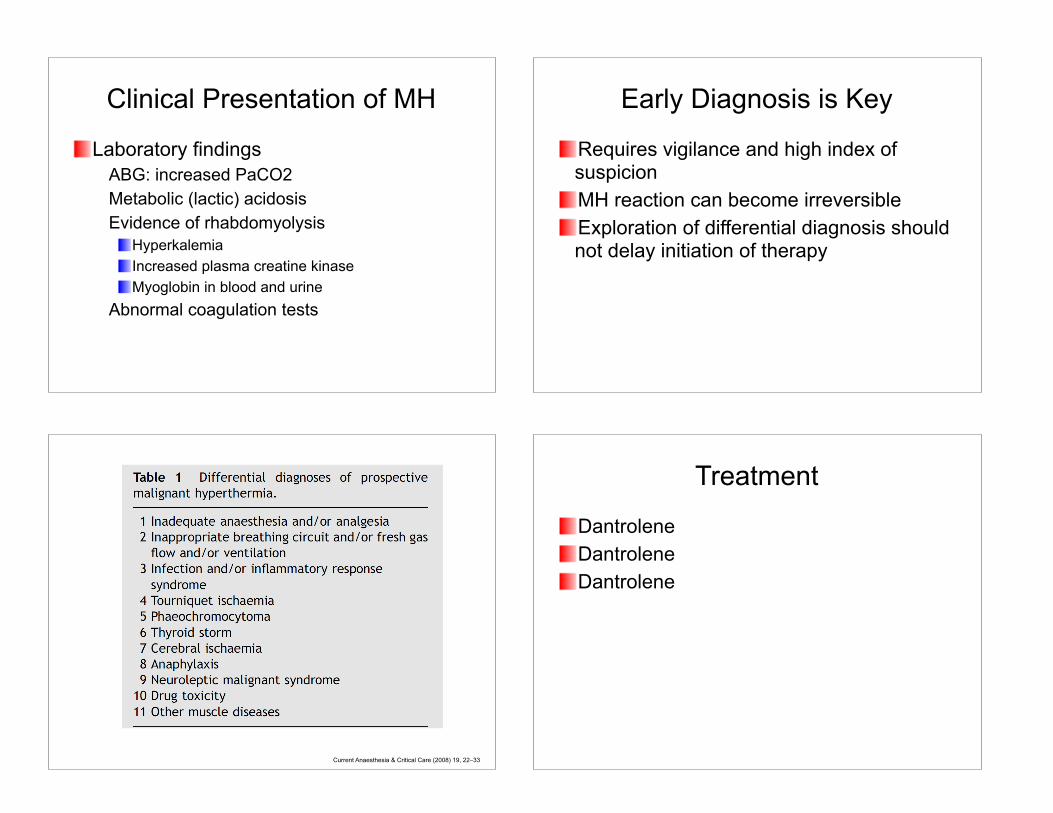
Current Anaesthesia & Critical Care (2008) 19, 22–33
Treatment
Dantrolene Dantrolene Dantrolene
Early Diagnosis and Treatment with Dantrolene is Key
Likelihood of MH complications doubles for every 30-minute delay in dantrolene administration
Larach MG et al. Anesth Analg 2010;110:498-507
Treatment
Discontinue anesthetic triggering agents Hyperventilate with 100% inspired oxygen If surgery must continue, switch to non-triggering anesthetic agents Administer dantrolene
Treatment with Dantrolene
Administer loading bolus of 2.5 mg/kg IV – If no response within minutes, continue with
bolus doses of 2.5 mg/kg (up to 10 mg/kg) Supplied as lyophilized powder (20 mg) – Contains 3 gm mannitol – Sodium hydroxide results in pH 9.5 – Reconstitute with 60 ml sterile water – May be difficult to dissolve – get help!
Treatment with Dantrolene
Generally safe at recommended doses No effect on cardiac or smooth muscle Side effects – Irritation and thrombosis at IV site – Muscle weakness (usually affects limbs, but
respiratory muscles also) – Nausea

Treatment: Cooling
Stop active warming devices (convert to cooling mode if possible) Undrape patient Ice packs (restrict to axilla and groin) IV infusion of cold saline Do not overcool patient (stop at 38.5°C)
Additional Treatment
Collect blood – ABG (acid-base status) – Electrolytes with glucose, BUN, Cr – Creatine kinase (CK) – CBC with platelets, PT, PTT – Myoglobin Insert urinary catheter – Facilitates bladder emptying – Assess for myoglobinuria
Treatment: Hemodynamic Instability
NaHCO3 for metabolic acidosis (+/-) Dysrhythmias – Treat according to ACLS protocol – Avoid calcium-channel blockers
May cause cardiac collapse, acute hyperkalemia
Hyperkalemia – Glucose-insulin – No evidence that calcium exacerbates MH in
this setting
After Initial Reaction is Controlled
Rhabdomyolysis – Follow CK (peaks 12-24 hours after episode) Recrudescence – Maintenance dose of dantrolene
1 mg/kg IV every 6 hours ~ 24-48 hours after last acute sign of MH

Recrudescence
North American MH Registry: 308 patients – 20% had recrudescence – Mean time from initial reaction was 13 hours – Higher rate associated with:
Muscular body type Longer time from induction to initial MH reaction
Burkman JM et al. Anesthesiology 2007;106:901-6
Post-Recovery Management
Patient considers him/herself MHS (as well as family members) – Inform anesthesia/ED personnel – Medic Alert bracelet Refer patient to an MH testing center – Gold standard is muscle biopsy for the
caffeine-halothane contracture test (CHCT) – Five centers perform CHCT in North America Molecular genetic testing
MH Biopsy Testing Centers North America
Morbidity and Mortality
North American MH Registry 1987-2006 – Nonfatal complications in 35% of patients
Cardiac, renal, or hepatic dysfunction Coma or change in level of consciousness Pulmonary edema DIC
MH Mortality – 0.0082 per 100,000 U.S. surgical patients
1% of all anesthesia-related deaths (1999-2005)
Larach MG et al. Anesth Analg 2010;110:498-507 Li G et al. Anesthesiology 2009;110:759-65

RYANODEXNew Formulation of Dantrolene
Dantrolene Formulations
Dantrium/RevontoOne vial contains 20 mg Mix with 60 ml sterile water Contains 3000 mg mannitol Solution pH ~ 9.5 Shelf life 3 years Cost $84/vial (AWP) Remains on formulary for subsequent treatment doses
RyanodexOne vial contains 250 mg Mix with 5 ml sterile water Contains 125 mg mannitol Solution pH ~ 10.3 Shelf life 2 years Cost $3008/vial (AWP) Formulary restriction limiting use to initial dose

Dantrolene Calculations
100 kg patient Loading dose of 2.5 mg/kg = 250 mg – Dantrium/Revonto (20 mg/vial)
Requires 13 vials: 13 x $84 = $1092 (780 cc) – Ryanodex (250 mg/vial)
Requires 1 vial: 1 x $3008 = $3008 (5 cc)GENETIC TESTING FOR MH
How genetics works… Genetics of MH
Primary gene locus: RYR1 – Ryanodine receptor protein forms the calcium
channel – RYR1 is a complex gene (106 exons) on
chromosome 19q.13.1 Secondary gene locus: CACNA1S – Encodes α1 subunit of dihydropyridine receptor
(DHPR) on chromosome 1 Third gene locus: STAC 3 – Chromosome 12 – Native American Myopathy (Lumbee)

JAMA. 293(23):2918-2924, June 15, 2005.
Litman RS, Rosenberg H. JAMA 2005;293,2918
Molecular Genetic Testing: Terminology
Mutation vs. Variant – Mutation = a variant functionally characterized
to be causative of MH using recognized standards
Criteria for establishing a causative genetic marker are rigorous
– Variant = not yet been found to be MH causative
Molecular Genetic Testing
European MH Group As of 6 September 2017 687 mutations on RYR1 gene – 36 known to be causative (diagnostic) 2 causative mutations on CACNA1S gene
Molecular Genetic Testing
Studies of MH families in Australia, New Zealand, North America, Europe, and Great Britain – As many as 60% of families without a variant
in RYR1 or CACNA1S
Bjorksten AR et al. Anaesth Intensive Care 2016;44:762-68

Molecular Genetic Testing
RYR1 gene variants in the United States MHS population – RYR1 examined in 120 MHS subjects – If RYR1 negative, CACNA1S also screened 10 causative mutations found in 26 subjects (22%) Variants of uncertain significance found in 36 subjects (30%)
Brandom BW et al. Anesth Analg 2013;116:00-00
Continuing the Search for Genes Associated with MH
30 MH-positive patients (IVCT) – Complete sequencing of RYR1 and CACNA1S
genes was negative for mutations – Added 7 genes associated with calcium
handling in skeletal muscle SR Findings – 4 rare variants found in 4 different genes
Variants of unknown significance – Each observed in a different patient
Bjorksten AR et al. Anaesth Intensive Care 2016;44:762-68
Molecular Genetic Testing
PreventionGenetics (Marshfield, WI) MNG Labs (Atlanta, GA) Robert Guthrie Biochemical and Molecular Genetics Laboratory, Buffalo General Medical Center, Buffalo, NY University of Minnesota Medical Center MH IN AMBULATORY
SURGERY CENTERS

MH in Ambulatory Surgery Centers (ASCs)
Management of MH crisis in ASCs Care of MH-susceptible patients in ASCs
MH Hotline Case: March 2008
18 yo female: GA for breast augmentation in plastic surgeon’s office O.R. One hour into case: chest wall feels tight and blood is backing up in IV; surgeon asks for muscle relaxation Anesthesiologist gives small dose of succinylcholine
MH Hotline Case
Within 10 min: ETCO2 and HR increase, skin feels warm, jaw rigidity noted MH suspected: volatile agent DC’d, new IV started, 2 vials dantrolene given AED placed on patient: dysrhythmia noted and shock given; NSR regained EMTs arrive at office: cardiac arrest recurs; treat with shock, epi, bicarb
MH Hotline Case
Surgeon rides with patient in ambulance and gives 3rd vial of dantrolene (takes entire supply of dantrolene with him) Third cardiac arrest occurs in ambulance: CPR given for 90 min in ED (wide complex tachycardia evolves into PEA) In ED: temp 42.2°C, K 8.0, ABG: pH 6.5, PaO2 116, PaCO2 120

MH Hotline Case
Cooled to temp 36°C with gastric and rectal ice lavage Continued to give dantrolene and support BP with fluids and pressors Hyperkalemia treated with insulin/glucose infusion and dialysis; K decreased to 4.8 Patient developed DIC and died the following morning
MH Hotline Case
Call from medical examiner What sort of tissue/blood sample was needed to test for MH? Blood sent to University of Pittsburgh Medical Center (Medical Genetics) Patient had RYR1 gene mutation known to be associated with MH
Anesth Analg 2012;114:94-100
Care of MH-Susceptible Patients in ASCs
Is it safe? – Yes, as long as:
Anesthesia machine is properly prepared Non-triggering technique is used Dantrolene is stocked
How long to monitor postoperatively? – Can MH occur postop?

Can MH Occur Postoperatively?
Analysis of 528 cases from MH Registry – 64 possible reports of postop MH
Consensus meeting of 3 authors: 10 cases (1.9%)
10 cases of postop MH – Latency period: 0-40 minutes – All showed characteristic signs of acute MH
None had hyperthermia as presenting sign
Literature review: 3 published reports
Litman RS et al. Anesthesiology 2008;109:825-9
Safe Duration of Postop Monitoring for MH-Susceptible (MHS) Patients
3 studies by Pollock’s group in MHS/related individuals – 2004: Retrospective study of 254 anesthetics
Monitored in PACU for 4 hours: no problems – 2000-2008: Prospective study of 206
anesthetics Monitored in PACU for ≥ 1 hour + step-down 1.5 hr
– 2008-2013: Prospective study of 125 anesthetics
PACU management no different from standard
Barnes C et al. Anaesth Intensive Care 2015;43:98-104
“AWAKE” MH

Awake MH Reaction
2001: First case of nonanesthetic, stress-induced hyperpyrexic death in MHS boy – MH episode during GA for repair of humerus
fracture at age 12 – 8 months later: playing football (temp 80°F)
After game, c/o weakness and muscle stiffness EMT’s: hot, diaphoretic, hyperventilating Seizure and respiratory arrest Could not intubate due to jaw clenching
Tobin JR et al. JAMA 2001;286:168-169
Awake MH ReactionVentricular fibrillation developed; defibrillated At hospital: rectal temp > 42.2°C, ECG showed wide complex bradycardia into vent fibrillation Trachea intubated (no relaxant); hyperkalemia treated; dantrolene given ABG: pH 6.76, PaCO2 115, PaO2 22 K 8.8 and rose to 14.5 mEq/L Resuscitation discontinued after one hour Postmortem exam: rigor in extremities and jaw DNA analysis of patient and father showed causative mutation for MH
Awake MH Reaction
6-yr-old boy playing in splash pool – Lower extremity rigidity; temp 104°F; trismus – ED: temp 108.9°F, RR 60, HR 190, seizures – ETT placed using succinylcholine – Cardiac arrest – could not be resuscitated – Genetic analysis: novel RYR1 variant – Father: same RYR1 variant, positive muscle
contracture test, central core disease
Lavezzi WA et al. Anesth Analg 2013;116:420-23
MH Susceptibility in Patients with Exertional Rhabdomyolysis (ER)
Retrospective study – Patients referred from Jan 2004-Dec 2015
Experienced >2 episodes of ER Diagnosed as MHS by caffeine-halothane contracture test (CHCT) 17 patients from 16 unrelated families
– Findings RYR1 variants detected in 9/17 patients
– Two variants known to be MH-causative mutations CACNA1S variant detected in 1/17 patients
Kraeva N et al. Can J Anesth 2017;64:736-43

The New York Times, July 17, 2017
Relationship of MH with Exertional Rhabdomyolysis (ER) and Exertional Heat Illness (EHI)
Questions (Riazi S et al. Can J Anesth 2014;61:1040-49)
– What percentage of EHI/ER individuals will exhibit causative RYR1 variants?
– What precautions should be taken by MHS individuals with regard to heat/exercise?
– What is the potential utility of dantrolene in the treatment of EHI/ER?
Pharmaceutical Processing, July 27, 2017
Spectrum of Malignant Hyperthermia???
MH Hotline: 1-800-MH-HYPER
www.mhaus.org

2017 MHAUS Scientific ConferenceMinneapolis, MN