12 musculoskeletal injuries 9/19/2016 - munson healthcare presentation.pdf12_musculoskeletal...
TRANSCRIPT

12_Musculoskeletal Injuries 9/19/2016
STN E-Library 2012 1
Nursing Grand Rounds Trauma Lecture
Shamarie Regenold, FNP‐BC
Elizabeth Erickson, PA‐C
Musculoskeletal Injuries
Objectives
At the conclusion of this presentation the participant will be able to:
• Identify the initial assessment for patients with musculoskeletal injury
•Describe upper extremity, lower extremity and pelvic musculoskeletal traumatic injuries and implications for nursing care
•Explain indications and strategies for open and closed reduction of fracture/dislocations
•Discuss the prevention, recognition and interventions for compartment syndrome and rhabdomyolysis
12_Musculoskeletal Injuries 9/19/2016
STN E-Library 2012 2
Resuscitation
A diagnosis of Musculoskeletal Injury may not occur initially, until there is significant blood loss causing
hemodynamic instability.
The Primary Survey in ATLS/ATCN does not include a thorough assessment of musculoskeletal injuries
unless gross bleeding causes a concern.
Radiography may/will confirm musculoskeletal injuries.
Prehospital information can help raise the index of suspicion.
Mechanism of Injury (MOI)
How’s
What’s
Where’s
When’s
Injury Facts
• Injury: The Leading Cause of Death Among Persons ages 1‐44
•800,000 EMT’s in our country significantly impact on the outcomes of trauma victims
•Field Triage is a process whereas the level of injury is determined, medical management is provided, and the right Trauma Center is identified

12_Musculoskeletal Injuries 9/19/2016
STN E-Library 2012 3
2011 Field Triage Decision Scheme
Step One:• Glasgow Coma Scale score of 13 or lower (change from <14),
• Systolic blood pressure of less than 90 mm Hg, or
• Respiratory rate of fewer than 10 or more than 29 breaths/minute (<20 breaths/minute in infants aged <1 year) or need for ventilatory support (criterion added).
Field Triage Decision Scheme
Step Two:• All penetrating injuries to head, neck, torso, and extremities proximal to elbow or knee
• Chest wall instability or deformity (e.g., flail chest)
• 2 or more proximal long‐bone fractures;• Crushed, degloved, mangled, or pulseless extremity • Amputation proximal to wrist or ankle
• Pelvic fractures• Open or depressed skull fractures; or• Paralysis
Step Three MOI Criteria
•Falls •High‐risk auto crash•Automobile vspedestrian/bicyclist thrown, run over, or with significant (>20 miles/hour) impact
•Motorcycle crash faster than 20 miles/hour

12_Musculoskeletal Injuries 9/19/2016
STN E-Library 2012 4
Step Four: Special Considerations
• Older Adults
• Children
• Anticoagulants
• Bleeding disorders
• Burns
• Pregnancy
Initial Management
Blood loss hypovolemia
Pain
Infection
Neurovascular damage
The four priorities of care
Blood Loss Hypovolemia

12_Musculoskeletal Injuries 9/19/2016
STN E-Library 2012 5
Petit Tourniquet ‐ Savigny 1798
Tourniquets
Pelvic Binder

12_Musculoskeletal Injuries 9/19/2016
STN E-Library 2012 6
Covert Blood Loss
•Blood Loss Associated with Fracture in Adults•Fracture site amount of blood loss in mL
•Radius and ulna 150–250•Humerus 250
•Tibia and fibula 500 •Femur 1000
•Pelvis 1500–3000
Blood Loss Hypovolemia
CLASS I CLASS II CLASS III CLASS IV
BloodLoss (ml)%
<75015%
750-150015%-30%
1500-200030-40%
>2000>40%
HR <100 >100 >120 >140
BP normal normal decrease decrease
PP normal decrease decrease decrease
RR 14-20 20-30 30-40 >35
UOP >30 20-30 5-15 negligible
CNS slightlyanxious
mildlyanxious
anxiousconfused
confusedlethargic
Acute Pain from Traumatic Injury
• Leads to stress response that increases heart rate and blood pressure
• Limits recovery
• Improves clinical outcome when managed well

12_Musculoskeletal Injuries 9/19/2016
STN E-Library 2012 7
Pain Assessment
• Numeric Scale
• Visual Analogue Scale
• Faces Pain Scale
Pain Management‐General Rules
Analgesics should be prescribed with a constant concern for detail
Dosing of pain medication should be adapted to the individual
Analgesics should be prescribed according to pain intensity as evaluated by a scale of intensity of pain
Analgesics should be given at regular intervals
Appropriate route for administration of analgesics
Prehospital
Pain starts at the point of injury (POI) and must be controlled from that initiating event
Prehospital practitioner has the first and perhaps only opportunity to break the pain cascade.
Early, effective pain control is essential to successful outcomes after traumatic injury

12_Musculoskeletal Injuries 9/19/2016
STN E-Library 2012 8
Current Acute Care Practice
Severe pain
Moderate Pain
Mild Pain
Strongest Opioid
Stronger Opioid
Mild Opioid
Postoperative Pain
2. Unless contraindicated, patients should receive an around the-clock regimen of NSAIDs, COXIBs, or acetaminophen
1. Epidural or intrathecal opioids, systemic opioid PCA, and regional techniques
Procedural Medications
Etomidate Midazolam
Propofol Ketamine
Fentanyl

12_Musculoskeletal Injuries 9/19/2016
STN E-Library 2012 9
Pain
Standardize medications
Keep airway resuscitative equipment
nearby
Frequent sensory &
motor assessments
Prevent Infection
Sample of Proprietary Wound Irrigation Systems
Bionixmed.com Irrimax.com
ortho.smith-nephew.com
Infection
Antibiotics are often necessary in the prophylaxis and treatment of orthopedic
infections post-operatively
The characteristics of implantable materials makes them a generous host
for bacterial colonization

12_Musculoskeletal Injuries 9/19/2016
STN E-Library 2012 10
Prophylaxis and Surgical Infections
• Staphylococci
• Pseudomonas Aeruginosa
• Klebsiella
• Acinetobacter baumani
Assessment
•What is baseline status?
•Are splints applied correctly
•Past Medical History
Diagnostic Studies
• Plain films
• CT, CT angio
• MRI
• Angiography

12_Musculoskeletal Injuries 9/19/2016
STN E-Library 2012 11
3 Views of the Pelvis
AP View Inlet View Outlet View
Anterior‐Posterior (AP) View of the Pelvis
Oblique’s “Judet”

12_Musculoskeletal Injuries 9/19/2016
STN E-Library 2012 12
AP View of Acetabulum
Selected Injuries
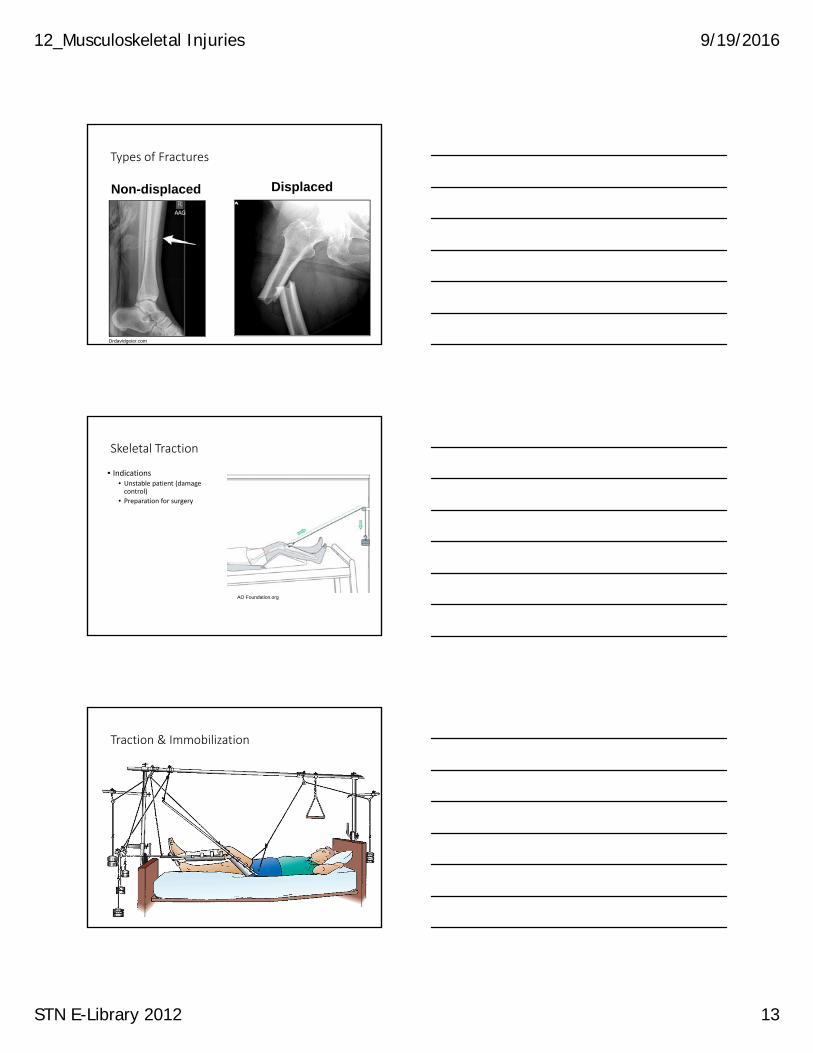
Types of Fractures
Wikimedia.com
12_Musculoskeletal Injuries 9/19/2016
STN E-Library 2012 13
Drdavidgeier.com
Non-displaced Displaced
Types of Fractures
Skeletal Traction
• Indications• Unstable patient (damage control)
• Preparation for surgery
AO Foundation.org
Traction & Immobilization

12_Musculoskeletal Injuries 9/19/2016
STN E-Library 2012 14
Reduction
•Reduction is a medical procedure to restore a fracture or dislocation to the correct alignment. For the fractured bone to heal without any deformity the bony fragments must be re‐aligned to their normal anatomical position
Dislocations
• Shoulder
• Knee
• Hip
• Shoulder
• Knee
• Hip
Knee Dislocation

12_Musculoskeletal Injuries 9/19/2016
STN E-Library 2012 15
Hip Dislocation
Classic presentation
of hip dislocation
Types of Surgical Treatments for Fractures
Intramedullary Nails vs. Screws and Plates

12_Musculoskeletal Injuries 9/19/2016
STN E-Library 2012 16
Gamma Nail in Femoral Head Intramedullary Nail in Femoral Shaft
Screw Holds Intramedullary Nail in Place to Avoid Migration
Open Reduction Internal Fixation (ORIF)
12_Musculoskeletal Injuries 9/19/2016
STN E-Library 2012 17
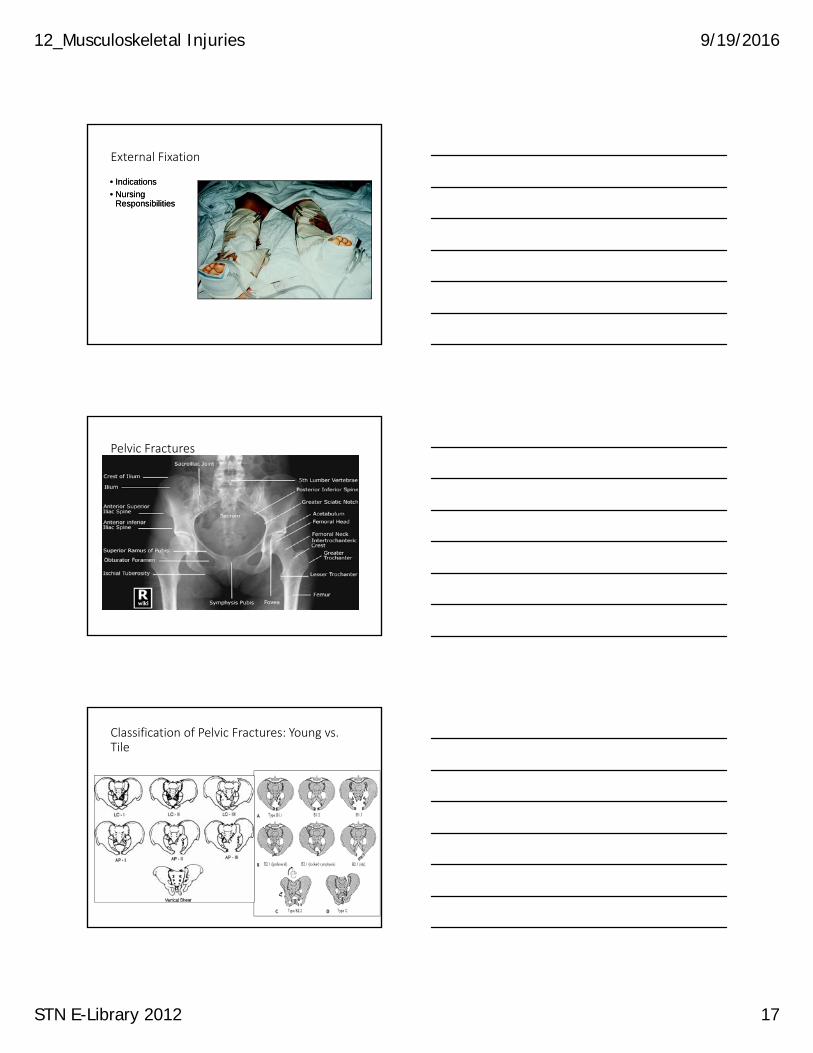
External Fixation
• Indications
• Nursing Responsibilities
• Indications
• Nursing Responsibilities
Pelvic Fractures
Classification of Pelvic Fractures: Young vs. Tile

12_Musculoskeletal Injuries 9/19/2016
STN E-Library 2012 18
Diastasis Symphysis Pubis
Associated Injuries in Order of Frequency
•Closed head injury• Long bone fractures•Peripheral nerve injury•Thoracic injury•Bladder•Spleen• Liver•GI tract•Kidney, Urethra, Mesentery, Diaphragm
Pelvic Fracture Treatment Protocol
Trauma.org

12_Musculoskeletal Injuries 9/19/2016
STN E-Library 2012 19
Angiographic Embolization
Blush
Complex Open Fractures
•Gustilo I : <1 cm wound over Fx
•Gustilo II: >1cm wound over Fx
•Gustilo III: A) Extensive soft tissue
injury
B) Periosteal stripping
C) Arterial injury needing repair
Gustilo Type 1 & Type 2

12_Musculoskeletal Injuries 9/19/2016
STN E-Library 2012 20
Mangled Extremity
Popliteal Artery and Vein Shunted

12_Musculoskeletal Injuries 9/19/2016
STN E-Library 2012 21
Identify the Zone of Injury

12_Musculoskeletal Injuries 9/19/2016
STN E-Library 2012 22
Compartment Syndrome
Capillary Perfusion Pressure- 25 mm Hg
Interstitial Pressure 4-6 mm Hg
http://www.hughston.com/
Compartment Syndrome
Ischemia
Myoglobin Release
Necrosis
Increase Interstitial Edema and Intravascular Viscosity
Increase Permeability
Endothelial Cell Damage
Vasodilatation

12_Musculoskeletal Injuries 9/19/2016
STN E-Library 2012 23
Etiology
Increased Fluid Content in Interstitial Space
Decreased Compartment Size
Signs and Symptoms
•Pain disproportionate to injury!
•Pain with passive stretching
•Neuro compromise
•Tenseness•Unilateral size increase
Wiki.org
High level of suspicion

12_Musculoskeletal Injuries 9/19/2016
STN E-Library 2012 24
Interventions
• Supplemental O2
• Level extremity
• Routine trauma resuscitation
• Extra vigilance in some patients
• Hydration
• Diuresis
• Alkalinization of urine
• Supplemental O2
• Level extremity
• Routine trauma resuscitation
• Extra vigilance in some patients
• Hydration
• Diuresis
• Alkalinization of urine
Delta P+ Diastolic Pressure - Compartment Pressure
Compartment >45 Delta P <40
Measurement Compartment Pressures
Fasciotomy
•Definitive Treatment with limb saving results
•Extends hospital length of stay as it turns a closed injury into an open injury
•Threshold for compartment pressure remains ~ 30 mmHg

12_Musculoskeletal Injuries 9/19/2016
STN E-Library 2012 25
Rhabdomyolysis
Muscle destruction
Adverse drug
reactions
Toxic effects
What is Myoglobin
Iron containing pigment found in skeletal muscle
Especially in those specialized for sustained contraction
Pathophysiology
• Direct toxicity
• Cast formation
• Mechanical obstruction
• Acid urine causes myoglobin to form a gel
• Hypoperfusion from hemorrhage and fluid shifts
• Reperfusion fluid shifts
• Further hypoperfusion

12_Musculoskeletal Injuries 9/19/2016
STN E-Library 2012 26
Causes of Rhabdomyolysis
Rhabdomyolysis
Precipitation is exacerbated by acidic pH of the urine
Myoglobin in the glomerular filtrate precipitates in the tubules and obstructs flow
Results in release of free myoglobin
Breakdown of muscle tissue
Treatment of the Effect of Rhabdomyolysis• Prevent Acute Renal Failure from the effects of myoglobinuria
• Monitor CPK, serum and urine myoglobinuria
• Ensure fluid resuscitation
• Ensure hyperdynamic urine output
• Ensure alkaline urine
• May diurese for mechanical lavage
• Carbonic anhydrase inhibitor

12_Musculoskeletal Injuries 9/19/2016
STN E-Library 2012 27
Key Point
Patient must be adequately volume resuscitated for appropriate “pushing pressure”
Before administering diuretics and mannitol to exert a “pulling pressure”
Propofol Infusion Syndrome (PRIS)
• Adverse drug event with high doses
• Not recommended for infusions > 48 hrs
• Signs of PRIS: hyperkalemia, metabolic acidosis, lipemia, renal failure, cardiovascular collapse, hepatomegaly, rhabdomyolysis
Case Study
• 60 yo Female MVC
• Medical HX: HTN, borderline COPD
• Injuries identified on admission:• Right rib fx: 9‐10
• Left rib fx: multiple
• Large pneumomediastinum
• Herniation of liver through the 9th and 10th ribs
• Scapula fx
12_Musculoskeletal Injuries 9/19/2016
STN E-Library 2012 28
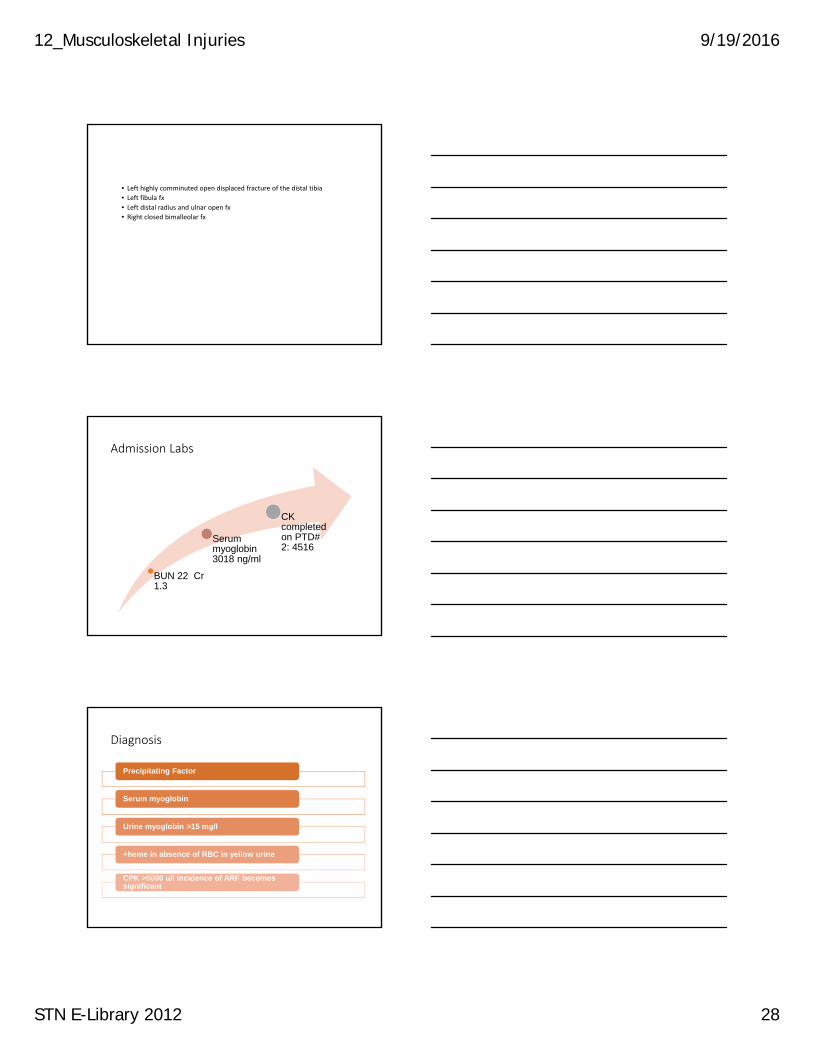
• Left highly comminuted open displaced fracture of the distal tibia
• Left fibula fx
• Left distal radius and ulnar open fx
• Right closed bimalleolar fx
Admission Labs
BUN 22 Cr 1.3
Serum myoglobin 3018 ng/ml
CK completed on PTD# 2: 4516
Diagnosis
Precipitating Factor
Serum myoglobin
Urine myoglobin >15 mg/l
+heme in absence of RBC in yellow urine
CPK >5000 u/l incidence of ARF becomes significant
12_Musculoskeletal Injuries 9/19/2016
STN E-Library 2012 29
Hospital Course
• PTD 5 BUN 60 Cr 5.4 despite aggressive hydration, avoidance of nephrotoxic medications as much as possible, and diuresis
• Dialysis begins on 8/11/16
• Pt. will require ongoing HD post discharge
Early Dialysis
•ARF pts who require RRT have increased morbidity and mortality
•Averting continued rises in creatinine might improve outcome in critically injured trauma patients
•ARF pts who require RRT have increased morbidity and mortality
•Averting continued rises in creatinine might improve outcome in critically injured trauma patients
Deep Vein Thrombosis
Incidence
Signs
Diagnosis
Prophylaxis

12_Musculoskeletal Injuries 9/19/2016
STN E-Library 2012 30
Ongoing Assessments
Traction does move out of place
Pins migrate away from initial sites
Patients re-bleed after surgery
Immobilization does cause pneumonia and deep vein thrombosis.
Neurovascular status changes without warning
Injuries Associated with Musculoskeletal Trauma
Injury Missed/Associated Injury
Clavicular fractureScapular fractureFracture and/or dislocation of shoulder
Major thoracic injury, esp. pulmonary contusion and rib fractures
Displaced thoracic spine fracture Thoracic aortic rupture
Spine fracture Intraabdominal injury
Fracture/dislocation of elbow Brachial artery injuryMedian, ulnar, and radial nerve injury
Femur fracture Femoral neck fracturePosterior hip dislocationIntraabdominal injuries
Posterior knee dislocation Femoral fracturePosterior hip dislocation
Knee dislocation or displaced tibial plateaufracture
Popliteal artery and nerve injuries
Calcaneal fracture Spine injury or fractureFracture dislocation of hind footTibial plateau fracture
Open fracture 70% incidence of associated nonskeletal injury
Summary
•Trauma care begins with standard process for care and destination protocol for pre‐hospital personnel
•The initial management of the patient consists of a thorough assessment of the type and degree of injury, and the need for damage control surgery to maintain homeostasis
•Pain management is a critical aspect in the care of the patient with musculoskeletal injury

12_Musculoskeletal Injuries 9/19/2016
STN E-Library 2012 31
Summary continued…
• The trauma nurse must be familiar with the types of radiographic studies performed and the need for follow studies in certain situations
•Multi‐orthopedic injuries require different treatment strategies: traction, and open or closed reduction
• The nurse must identify limb‐threatening compartment syndrome and patients at risk for rhabdomyolysis
• The nurse must protect the patient from infection, which may progress to osteomyelitis
Drug and Alcohol Abuse in the Trauma Patient
Objectives
• Identifying the patient at risk for withdrawal
• Differentiating withdrawal from head injury symptoms
• Management of the trauma patient during withdrawal from drugs and alcohol

12_Musculoskeletal Injuries 9/19/2016
STN E-Library 2012 32
Breadth of the Issue
CDC. (2015)Prevalence of binge drinking among adults. http://www.cdc.gov/alcohol/data-stats.htm
• 5 or more drinks per occasion in men
• 4 or more drinks per occasion in women
• 15 or more drinks per week for men and 8 or more drinks per week for women
• Binge and Heavy Alcohol use sharply rises in ages 18‐20 and peaks in ages 21‐25 years and slowly tapers off after that
• Illicit drug use began to rise in 2010 with a peak in ages 18‐20

12_Musculoskeletal Injuries 9/19/2016
STN E-Library 2012 33
• SAMHSA and the ACS advocate for mandatory screening methods on every trauma patient
• Screening and Brief intervention are required for Level I and II trauma centers
• Alcohol and Drug levels are ordered on all Level I and II trauma activation patient
CDC. (2016) Division of Population Health, National Center for Chronic Disease Prevention and Health Promotion, Centers for Disease Control and Prevention
• AUDIT‐C• Standardized screening tool
• 3 item screening tool about alcohol consumption
AUDIT‐C
http://cqaimh.org/pdf/tool_auditc.pdf

12_Musculoskeletal Injuries 9/19/2016
STN E-Library 2012 34
12 fl oz ofregular beer
5 fl oz oftable wine
1.5 fl oz shot of80-proof spirits("hard liquor")
• There may need to be follow up questions if your patient has a positive screen
• This will assist you in assessing the risk of withdrawal in your patient
• “When was your last drink?” Mild symptoms usually begin 6‐48 hours after the last drink
• “Have you ever been treated for alcohol withdrawal before?”
• People who have experienced withdrawal symptoms are usually attentive to their bodies signals and can tell you what symptoms they generally experience.
• “Have you ever had an alcohol withdrawal seizure?”Withdrawal can occur even with an elevated BAL (blood alcohol level)

12_Musculoskeletal Injuries 9/19/2016
STN E-Library 2012 35
Adolescents and Children
• CRAFFT‐ score of 1= medium risk, brief intervention, 2+ = high risk, brief intervention and referral
• C ‐ Have you ever ridden in a CAR driven by someone (including yourself) who was "high" or had been using alcohol or drugs?
• R ‐ Do you ever use alcohol or drugs to RELAX, feel better about yourself, or fit in?
• A ‐ Do you ever use alcohol/drugs while you are by yourself, ALONE?
• F ‐ Do you ever FORGET things you did while using alcohol or drugs?
• F ‐ Do your family or FRIENDS ever tell you that you should cut down on your drinking or drug use?
• T ‐ Have you gotten into TROUBLE while you were using alcohol or drugs?
• CIWA used here at Munson
• Currently in the process of being reviewed
• Future changes to come
TBI Patients
• An estimated 36‐51% of patients who sustained a TBI are using substances when this occurs
• Interestingly, the more severe TBI patients had less drug and alcohol use than the population with nothing in their system
Andelic, N. et al. (2010). Effects of acute substance use and pre-injury substance abuse on traumatic brain injury severity in adults admitted to a trauma centre. Journal of Trauma Management & Outcomes, 4;6.

12_Musculoskeletal Injuries 9/19/2016
STN E-Library 2012 36
•Neuroprotective effect of alcohol on the brain•Alcohol causes a blunting of the sympathetic response, causing activation of the stress response after major injury
•The surge in catecholamines causes massive systemic increase in metabolism, leaving less oxygen and glucose for the brain
Assessment for withdrawal in the TBI patient
•TBI patients are typically agitated at times and it is nearly impossible to ascertain the reason
•Benzodiazepines are the preferred treatment for signs and symptoms of withdrawal‐ inhibits nerve‐cell excitability in the brain
• Intubated TBI patients are on heavy sedation and pain management already
• An important consideration in these patients is the initiation of thiamine
• Thiamine helps the brain cells produce energy from sugar.
Martin, P. et al (2004). The role of thiamine deficiency in alcoholic brain disease. http://pubs.niaaa.nih.gov/publications/arh27-2/134-142.htm

12_Musculoskeletal Injuries 9/19/2016
STN E-Library 2012 37
References
Advanced Trauma Life Support For Doctors. 8th ed. New York, New York: American College of Surgeons, 2008.
American Society of Anesthesiologists Task Force on Acute Pain Management. Practice guidelines for acute pain management in the perioperative setting: an updated report. Anesthesiology. 2012; 116(2): 248‐73.
Anterior Pelvic Injuries. Wheeless' on line Web site. http://www.wheelessonline.com/ortho/pelvic_fractures. Updated September 21, 2012. Accessed November 16, 2012.
Bowman, WJ, Nesbitt, ME, and Therian, SP. The effects of standardized trauma training on prehospital pain control: Have pain medication administration rates increased on the battlefield? J Trauma Acute Care Surg. 2012; 73(2 Supp 1): 42‐48.
Brandt, MM, Falvo, AJ, Rubinfield, IS, et al. Renal dysfunction in trauma: even a little costs a lot. J Trauma 2007; 62(6): 1362‐1364.
Dries, DJ. Initial Evaluation of the Trauma Patient e‐Medicine Web site. http://emedicine.medscape.com/article/434707‐overview. Updated September 20, 2012. Accessed November 16, 2012.
Cutts, S, Prempeh, M, and Drew, S. Anterior Shoulder Dislocation. Ann R Coll Surg Engl. 2009 January; 91(1): 2–7.
Davenport, M. Joint Reduction, Hip Dislocation, Posterior e‐Medicine Web site. http://emedicine.medscape.com/article/109225‐overview. Updated February 28, 2012. Accessed November 16, 2012
Fractures of the Pelvis and Acetabulum. OA Centers for Orthopaedics Web site. http://www.orthoassociates.com/SP11B26/ . Updated September 26, 2011. Accessed November 16, 2012.
Gonzalez, D. Crush Syndrome. Critical Care Medicine. 2005; 33(1): S34‐41.
Graf, K. Unstable Pelvic Fractures e‐Medicine Web site. http://emedicine.medscape.com/article/1247426‐overview. Updated August 15, 2011. Accessed November 16, 2012.
Kelleher, HB. Knee Dislocation in Emergency Medicine e Medicine Web site. http://emedicine.medscape.com/article/823589‐overview. Updated January 11, 2011. Accessed November 16, 2012.
Krost,W, Mistovich, J, and Limmer, D. Beyond the Basics: Crush Injuries and Compartment
Syndrome EMSWorld Web site. http://www.emsworld.com/article/10321291/beyond‐the‐basicscrush‐
injuries‐and‐compartment‐syndrome. February 1, 2008. Accessed November 16, 2012.
Malchow, RJ, and Black, IH. The evolution of pain management in the critically ill trauma
patient: Emerging concepts from the global war on terrorism. Crit Care Med. 2008; 36(7 Suppl):
S 346‐357.
McQuillan, KA, Von Rueden, KT, Hartsock, RL, et al. Trauma Nursing: From Resuscitation
Through Rehabilitation (4th ed). W.B. Saunders Co., Philadelphia; 2009.
Sahjian, M, and Frakes, M. Crush Injuries: Pathophysiology and Current Treatment. Advanced
Emergency Nursing Journal. 2007; 29(2): 145‐150.
Tactical Combat Casualty Care Guidelines. http://links.lww.com/TA/A139). Updated August 8,
2011. Accessed November 16, 2012.
The clinical and economic implications of using multi‐modal strategies for postsurgical pain
management. Website. https://www.premierinc.com/advisorlive/Presentations/may‐10‐postsurgical‐
pain‐management‐advisor‐live‐final.pdf . Accessed November 16, 2012.
Vargas‐Schaffer, G. Is the WHO analgesic ladder still valid? Twenty‐four years of experience.
Canadian Family Physician. 2010; 56(6): 514‐517.
Andelic, N. et al. (2010). Effects of acute substance use and pre‐injury substance abuse on traumatic brain injury severity in adults admitted to a trauma centre. Journal of Trauma Management & Outcomes, 4;6.
Martin, P. et al (2004). The role of thiamine deficiency in alcoholic brain disease. http://pubs.niaaa.nih.gov/publications/arh27‐2/134‐142.htm

12_Musculoskeletal Injuries 9/19/2016
STN E-Library 2012 38
CDC. (2016) Division of Population Health, National Center for Chronic Disease Prevention and Health Promotion, Centers for Disease Control and Prevention
CDC. (2015)Prevalence of binge drinking among adults. http://www.cdc.gov/alcohol/data‐stats.htm