11 introduction to metabolic acidosis
TRANSCRIPT

277
S. Faubel and J. Topf 11 Metabolic Acidosis: The Overview
11
WARNING: It has been longer since freshman chemistry than you realize. We stronglyadvise reading Chapter 10, Introduction to Acid-Base before advancing beyond this point.
Metabolic Acidosis:11 The Overview
278
The Fluid, Electrolyte and Acid-Base Companion
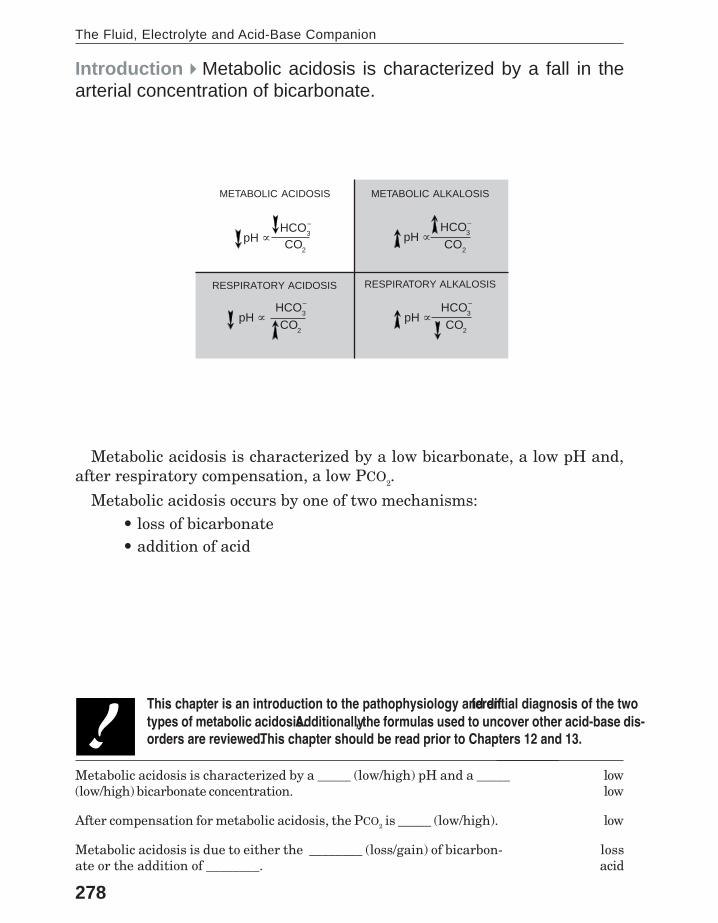
Metabolic acidosis is characterized by a low bicarbonate, a low pH and,after respiratory compensation, a low PCO2.
Metabolic acidosis occurs by one of two mechanisms:• loss of bicarbonate• addition of acid
Introduction�Metabolic acidosis is characterized by a fall in thearterial concentration of bicarbonate.
METABOLIC ALKALOSIS
RESPIRATORY ALKALOSISRESPIRATORY ACIDOSIS
METABOLIC ACIDOSIS
This chapter is an introduction to the pathophysiology and differential diagnosis of the twotypes of metabolic acidosis. Additionally, the formulas used to uncover other acid-base dis-orders are reviewed. This chapter should be read prior to Chapters 12 and 13.
Metabolic acidosis is characterized by a _____ (low/high) pH and a _____(low/high) bicarbonate concentration.
After compensation for metabolic acidosis, the PCO2 is _____ (low/high).
Metabolic acidosis is due to either the ________ (loss/gain) of bicarbon-ate or the addition of ________.
lowlow
low
lossacid
pH ∝ HCO3
–
CO2
pH ∝ HCO3
–
CO2
pH ∝ HCO3
–
CO2
pH ∝ HCO3
–
CO2
279
S. Faubel and J. Topf 11 Metabolic Acidosis: The Overview
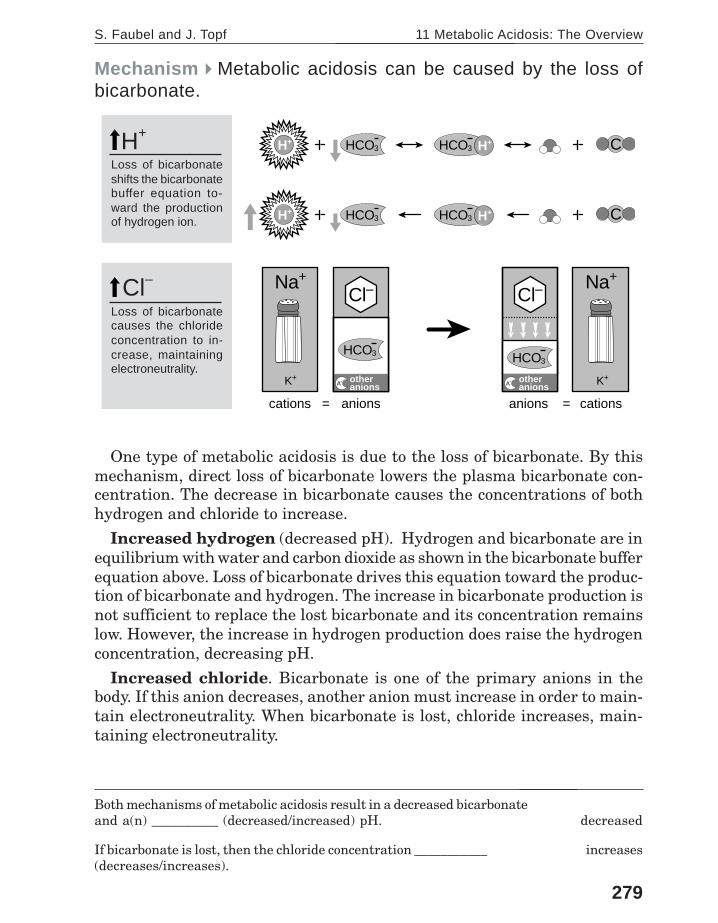
Mechanism�Metabolic acidosis can be caused by the loss ofbicarbonate.
One type of metabolic acidosis is due to the loss of bicarbonate. By thismechanism, direct loss of bicarbonate lowers the plasma bicarbonate con-centration. The decrease in bicarbonate causes the concentrations of bothhydrogen and chloride to increase.
Increased hydrogen (decreased pH). Hydrogen and bicarbonate are inequilibrium with water and carbon dioxide as shown in the bicarbonate bufferequation above. Loss of bicarbonate drives this equation toward the produc-tion of bicarbonate and hydrogen. The increase in bicarbonate production isnot sufficient to replace the lost bicarbonate and its concentration remainslow. However, the increase in hydrogen production does raise the hydrogenconcentration, decreasing pH.
Increased chloride. Bicarbonate is one of the primary anions in thebody. If this anion decreases, another anion must increase in order to main-tain electroneutrality. When bicarbonate is lost, chloride increases, main-taining electroneutrality.
Both mechanisms of metabolic acidosis result in a decreased bicarbonateand a(n) __________ (decreased/increased) pH.
If bicarbonate is lost, then the chloride concentration ___________(decreases/increases).
aaadecreased
increases
Loss of bicarbonateshifts the bicarbonatebuffer equation to-ward the productionof hydrogen ion.
HCO3 H+HCO3H+ C
HCO3 H+HCO3H+ C
cations = =anions
HCO3
Cl–Na+
K+
cationsanions
HCO3
Cl–Na+
K+A- other�
anions A- other�anions
H+
Loss of bicarbonatecauses the chlorideconcentration to in-crease, maintainingelectroneutrality.
Cl–

280
The Fluid, Electrolyte and Acid-Base Companion
HCO3–
cations = =anions
Na+
K+
anions cations
Na+
K+
HCO3
Cl–
A- other�anions
HCO3
Cl–
A- other�anions
Addition of an acid shiftsthe bicarbonate bufferequation toward the pro-duction of water and car-bon dioxide. The reactionconsumes bicarbonate, de-creasing its concentration.
Addition of an acid is theaddition of an H+ and its ac-companying anion. Whenan acid is added, its anionaccumulates in the plas-ma; the Cl– concentrationdoes not change.
Mechanism�Metabolic acidosis can be caused by the additionof acid.
The other type of metabolic acidosis is due to the addition of acid. For thepurpose of understanding metabolic acidosis, an acid is defined as a hydro-gen cation and its accompanying anion. In this type of metabolic acidosis,the addition of acid directly raises the hydrogen ion concentration (lowerspH). The increase in hydrogen causes the bicarbonate concentration to de-crease. Due to the presence of increased anions, the chloride concentrationdoes not change.
Decreased bicarbonate. Hydrogen and bicarbonate are in equilibriumwith water and carbon dioxide as shown in the bicarbonate buffer equationabove. The addition of acid (hydrogen ion), shifts the reaction toward theproduction of water and carbon dioxide. Bicarbonate decreases as it is con-sumed buffering hydrogen.
Increased anions. As acid is added, the accompanying anions accumu-late in the plasma. Even though the bicarbonate concentration is low, thechloride concentration does not change because the accompanying anionsmaintain electroneutrality.
An acid consists of two components: a(n) ___________ ion andan accompanying ________.
In metabolic acidosis due to the addition of acid, the bicarbonateconcentration ____________ (decreases/increases) as it is con-sumed buffering hydrogen.
hydrogenanion
decreases
HCO3 H+HCO3H+ C
HCO3 H+HCO3H+ C
Anions

281
S. Faubel and J. Topf 11 Metabolic Acidosis: The Overview
=anions cations
Na+
K+
HCO3
Cl–
A- other�anions
.
Diagnosis�The anion gap is a tool used in the evaluation ofmetabolic acidosis.
NORMAL ANION GAP INCREASED ANION GAP
Metabolic acidosis due to the loss of bicarbonate or the addition of acidcan be distinguished by the anion gap.
The anion gap is a clinical tool based on the principle of electroneutralitywhich is used to detect an increase in plasma anions other than Cl– andHCO3
– . The formula is shown above. Normally, the anion gap is between 5and 12 mEq/L.
In metabolic acidosis due to the loss of bicarbonate, the anion gap re-mains within the normal range. The anion gap is normal because a rise inchloride compensates for the fall in bicarbonate. This type of acidosis isknown as non-anion gap metabolic acidosis or hyperchloremic acidosis.
In metabolic acidosis due to the addition of acid, the anion gap increasesbecause the addition of acid includes the addition of anions. The increasedanion gap indicates the presence of these additional anions in the plasma. Thistype of acidosis is known as anion gap metabolic acidosis.
Because it so effectively narrows the differential diagnosis, calculatingthe anion gap is the first step in the evaluation of metabolic acidosis.
Anion gap = Na+ – (Cl– + HCO3– )
LOSS OF BICARBONATE ADDITION OF ACID
The formula for anion gap is _____________________.
Calculate the anion gap: Na+ = 140 mEq/L, Cl– = 118 mEq/L andHCO3
– = 15 mEq/L. This is a(n) ________ gap metabolic acidosis.
Calculate the anion gap: Na+ = 140 mEq/L, Cl– = 101 mEq/L andHCO3
– = 12 mEq/L. This is a(n) ________ gap metabolic acidosis.
Na+ – (Cl– + HCO3–)
anion gap = 7non-anion
anion gap = 27anion
The concept of anion gap was introduced in Chapter 1, Moles and Water page 21.
= cationsanions
HCO3
Cl–Na+
K+A- other�
anionsHCO3
A-H+
A- H+

282
The Fluid, Electrolyte and Acid-Base Companion
= cationsanions
HCO3
Cl–Na+
K+A- other�
anions
Etiologies�Non-anion gap metabolic acidosis is caused by theloss of bicarbonate.
GI LOSS OF HCO3– RENAL LOSS OF HCO
3–
Renal tubular acidosis (RTA)proximal (type 2 RTA)distal (type 1 RTA)hypoaldosteronism (type 4 RTA)
GI lossdiarrheasurgical drainsfistulasureterosigmoidostomyobstructed ureteroileostomycholestyramine
Non-anion gap metabolic acidosis is due to the loss of bicarbonate fromeither the GI tract or kidney. The differential diagnosis of non-anion gapmetabolic acidosis is listed above.
In non-anion gap metabolic acidosis, the anion gap is less than 12 mEq/L.
Non-anion gap metabolic acidosis is due to the ________ of bicar-bonate from either the ____ tract or the ________.
In non-anion gap metabolic acidosis, the chloride concentration is__________.
lossGI; kidney
increased
All of the causes of non-anion gap metabolic acidosis are reviewed in detail in Chapter 12,Metabolic Acidosis: Non-Anion Gap.

283
S. Faubel and J. Topf 11 Metabolic Acidosis: The Overview
=anions cations
Na+
K+
HCO3
Cl–
A- other�anions
Etiologies�Anion gap metabolic acidosis is caused by the addi-tion of acid.
Anion gap metabolic acidosis is due to the addition of acid. The additionalacid is either endogenous (produced by the body) or exogenous (ingested). Inanion gap metabolic acidosis, the anion gap is greater than 12 mEq/L.
There are four fundamental processes that cause anion gap metabolicacidosis: lactic acidosis, ketoacidosis, renal failure and ingestions. A handymnemonic for the differential diagnosis of anion gap metabolic acidosis isPLUM SEEDS.
Paraldehyde ............................................... Ingestion
Lactic Acidosis ............................................ Lactic acidosis
Uremia ........................................................ Renal Failure
Methanol ..................................................... Ingestion
Salicylate poisoning ................................... IngestionEthanol ....................................................... Ketoacidosis
Ethylene glycol ........................................... Ingestion
DKA ............................................................ Ketoacidosis
Starvation ................................................... Ketoacidosis
C
CO
O
CH3
CH2
O O
C
CHO CH3
CH2
O O
H
CH3
CH3
CH2
KETOACIDOSIS
RENAL FAILURE
Oxygen
LACTIC ACIDOSIS
INGESTIONS
lactic; ketoacidosis,renal failure; ingestions
PLUM SEEDS
Anion gap metabolic acidosis is caused by one of four funda-mental processes: _________ acidosis, _____________, _______ ______ and _____________.
A good mnemonic is _________________.
All of the causes of anion gap metabolic acidosis are reviewed in detail in Chapter 13,Metabolic Acidosis: Anion Gap.

284
The Fluid, Electrolyte and Acid-Base Companion
Compensation�The compensation for metabolic acidosis is anincrease in ventilation which decreases PCO2.
Regardless of the anion gap, compensation for the low bicarbonate found inboth types of metabolic acidosis is a decrease in PCO2. PCO2 decreases throughan increase in ventilation. The expected fall in PCO2 in metabolic acidosis ispredicted by the following equation.
In metabolic acidosis, if the PCO2 is ________ than the expectedvalue, a concurrent respiratory alkalosis is present.
If the HCO3– is 12 mEq/L, what is the expected PCO2? If the PCO2
is 19 mmHg, what other disorder is also present?
lower
24 to 28 mmHgrespiratory alkalosis
If the PCO2 falls within the expected range, appropriate compensation hasoccurred.
If the PCO2 is above or below the PCO2 predicted by the formula, a concur-rent respiratory acid-base disorder is present. If the PCO2 is lower than pre-dicted, a respiratory alkalosis is also present; if the PCO2 is higher thanexpected, a respiratory acidosis is also present.
16 2218 201410 12
4038363432302826242220181614
86 24 26
4442
RESPIRATORY
ALKALOSIS
RESPIRATORY
ACIDOSIS
Bicarbonate (mEq/L)
PC
O2 (m
mH
g)
Normal
Metabolic
acid
osis
METABOLIC ACIDOSIS
Expected PCO2 = (1.5 × HCO3
–) + 8 ± 2CCC

285
S. Faubel and J. Topf 11 Metabolic Acidosis: The Overview
Just as assessing compensation can uncover a concomitant respira-tory acid-base disorder, determining the corrected bicarbonate can un-cover a concomitant metabolic acid-base disorder (i.e., non-anion gapmetabolic acidosis or metabolic alkalosis). The formula is shown above.
The corrected bicarbonate is the bicarbonate before the anion gapacidosis began. If the corrected bicarbonate is above the normal rangeof bicarbonate concentration (22 to 28 mEq/L), a concurrent metabolicalkalosis is present; if the corrected bicarbonate is below the normalbicarbonate range, a concurrent non-anion gap metabolic acidosis is present.
The following case illustrates how two metabolic acid-base disorderscan be present at the same time:
MJ is an 18-year-old diabetic who develops infectious diarrhea whichcauses a non-anion gap metabolic acidosis. Because she is not feelingwell, she stops taking her insulin. She then develops diabetic ketoaci-dosis (DKA), causing an anion gap metabolic acidosis. When she pre-sents to the hospital, her bicarbonate is 10 and the anion gap is 22. Thecorrected bicarbonate is 10 + (22-12) or 20 mEq/L. This means thatbefore she developed DKA, the bicarbonate was 20 mEq/L. 20 mEq/L isbelow the normal range for bicarbonate indicating that a non-anion gapmetabolic acidosis is also present. In this patient, it is from diarrhea.
Another equation that can be used to assess the presence of an addi-tional metabolic acid-base disorder in anion gap metabolic acidosis isthe delta-delta. The formula is shown above. If the ratio is less thanone, a concurrent non-anion gap metabolic acidosis is present. If theratio is greater than two, a concurrent metabolic alkalosis is present.
Using the example above, the delta-delta is (22 – 12) ⁄ (24 – 10) =10 ⁄ 14 = 0.7. Since 0.7 is less than one, a non-anion gap metabolic acido-sis is also present, as determined by the corrected bicarbonate above.
Clinical correlation: In anion gap metabolic acidosis, the correct-ed bicarbonate or delta-delta can be used to uncover an additionalmetabolic acid-base disorder.
CORRECTED BICARBONATE
• if > 28, then a metabolic alkalosis is present• if < 22, then a non-anion gap metabolic acidosis is present
measured HCO3– + (anion gap – 12)
DELTA-DELTA
measured anion gap – ideal anion gap
ideal HCO3– – measured HCO3
–=∆ gap
∆ HCO3–
• if > 2, then a metabolic alkalosis is present• if < 1, then a non-anion gap metabolic acidosis is present

286
The Fluid, Electrolyte and Acid-Base Companion
Summary�Metabolic acidosis: the overview.
Metabolic acidosis is one of the four primary acid-base disorders. It isrecognized by a low pH and a low plasma bicarbonate.
In metabolic acidosis, the decreased bicarbonate concentration can be dueto either the loss of bicarbonate or the addition of an acid.
The anion gap is a tool that can distinguish between the two fundamentalprocesses which cause metabolic acidosis.
Compensation for metabolic acidosis from any etiology is increased venti-lation to lower the PCO2 and raise the pH. In metabolic acidosis, the carbondioxide falls by a predictable amount depending on the plasma bicarbonateconcentration. If the PCO2 is not within the predicted range, a respiratoryacid-base disorder is present in addition to metabolic acidosis. In anion gapmetabolic acidosis, the corrected bicarbonate can be used to uncover a con-current metabolic alkalosis or non-anion gap metabolic acidosis.
=anions cations
Na+
K+
HCO3
Cl–
A- other�anions
= cationsanions
HCO3
Cl–Na+
K+A- other�
anions
or
LOSS OF BICARBONATE
NON-ANION GAPADDITION OF ACID
ANION GAP
cations = anions
Na+
K+
HCO3
Cl–
A- other�anions
Renal tubular acidosisproximaldistalhypoaldosteronism
GI loss of bicarbonatediarrheafistulasureterosigmoidostomyobstructed ureteroileostomycholestyramine
NON-ANION GAP METABOLIC ACIDOSIS
ParaldehydeLactic AcidosisUremiaMethanol
StarvationEthanolEthylene glycolDKASalicylate poisoning
ANION GAP METABOLIC ACIDOSIS
pH ∝ HCO3
–
CO2
pH ∝ HCO3
–
CO2
pH ∝ HCO3
–
CO2
pH ∝ HCO3
–
CO2
metabolic acidosis metabolic alkalosis respiratory acidosis respiratory alkalosis
METABOLIC ACIDOSIS
Expected PCO2 = (1.5 × HCO3
–) + 8 ± 2
CORRECTED BICARBONATE
Measured HCO3
– + (Anion gap – 12)
The causes of both non-anion gap and anion gap metabolic acidosis are listedbelow. The next two chapters will look at the individual disorders in detail.