1.0 intended use the afp eiagen kit has been designed …s april 2006/eiagen... · 2016-08-05 ·...
TRANSCRIPT

1.0 INTENDED USEThe AFP EIAgen kit has been designed for the quantitative determination of Alpha-fetoprotein in human serum, plasma or amniotic fluid.The standards are calibrated against the WHO 1st International Reference Preparation(IRP) for human AFP (72/225).
2.0 SUMMARY AND EXPLANATION OF THE TESTAlpha-fetoprotein (AFP) is a fetal serum protein which circulates in trace amountsin healthy adults (2). AFP is produced mainly by the fetal yolk sac and fetal liverand to a lesser extent by the fetal gastrointestinal tract and kidneys (3). It is asingle chain glycoprotein with a molecular weight of approximately 65-70 kilodaltons.The physico-chemical properties and amino acid composition of AFP are similar tothose of serum albumin (4), from which it is antigenically distinct (5).Clinical interest in AFP is in oncology where serum AFP is used for the diagnosisand monitoring of tumours (6, 7, 8) and in prenatal screening where amniotic fluidAFP is used to screen for foetal abnormalities such as spina bifida and Down’sSyndrome (9).Fetal plasma AFP diffuses into the fetal urine and is excreted into the amniotic fluidfrom where it diffuses into the maternal circulation. The concentration of AFP in thefetal plasma peaks (2-3 mg/ml) at 12 - 14 weeks and then rapidly falls (9). The levelsin the amniotic fluid are parallel to those in the fetal plasma, but are about two ordersof magnitude lower (µg range) than fetal plasma concentration. In contrast, maternalserum AFP concentrations increase geometrically until 30 weeks gestation and thendecline (10). Following birth, AFP levels in both mother and newborn return rapidlyto basal levels (<10 ng/ml).Approximately 70% of patients with primary hepatocellular carcinoma show elevatedlevels of AFP (7). Levels of 1,000 - 10,000 ng/ml have been reported (11). In thecase of testicular teratoma a direct relationship has been observed between incidenceof elevated AFP levels and the stage of disease (12). No increased AFP levels arefound in testicular seminomas (13). The application of AFP measurement to themanagement of carcinoma patients has been well documented (14). Failure of AFPlevels to return to normal post-operatively suggests the presence of residual tumour.Increased serum AFP levels have also been observed in benign conditions e.g. acuteviral infections, chronic active hepatitis and cirrhosis. Elevated amniotic fluid AFPhas also been found in other serious conditions e.g. fetal death, omphalocele andTurner’s syndrome.
3.0 PRINCIPLE OF THE METHODThe AFP EIAgen assay is based on the two steps immunoenzymatic sandwichprinciple, in conjunction with the Biotine-Streptavidin technology.Two monoclonal anti-AFP of high affinity and specificity are used: one is labelledwith Horse Radish Peroxidase (HRP) and the other with Biotin, while the microplatewells are coated with Streptavidin.Samples, calibrators and controls are dispensed into the wells, followed by theBiotin anti-AFP conjugate.During the incubation the monoclonal bind the AFP molecule to one specific sites,and contemporaneously, the Streptavidin immobilizes the forming immunologicalcomplex to the wells through the binding to the biotin moiety of the biotinilatedantibody.After washing to eliminate the not reacted species the second monoclonal conjugatedto HRP is added.After the second incubation the wells are washed to remove the unbound labelledantibodies and the mixture of chromogen/substrate is added.The reaction is then blocked by adding the Stop Solution and the developed colouris measured photometrically. The intensity of the colour is directly proportional,within the working range of the assay, to the concentration of AFP in the sample.The concentration of AFP in a patient sample or controls is then determined byinterpolation on the calibration curve.
4.0 REAGENTS - STORAGE AND HANDLINGThe EIAgen AFP kit contains sufficient reagents for 96 wells. On receipt, store thekit and each reagent at 2...8°C, stable up to the expiration date on the labels.If not otherwise specified, also, after the first opening all the reagent are alsostable up to the expiry date printed on the labels, provided they are stored asindicated and no contaminations accur during the pipetting.
4.1 Streptavidin Microplate
The bag contains a microplate of 12 strips x 8 wells.Each well is coated with Streptavidin and it may be used individually. Allow microplateto warm to room temperature (18... 25°C) before use. After the first opening theunused strips are stable for 2 months at 2...8°C, provided they are stored in theplastic bag with the dessicant.
4.2 AFP Calibrators
6 vials of AFP Calibrators containing 0- 5- 25- 125- 250- 500 IU/ml (1st IRP 72/225)in horse serum with Sodium Azide (0.09% w/w) and Proclin 300 (0.0025% v/v) aspreservatives. 0.5 ml for each Calibrator. Ready for use. Mix gently before use.
4.3 AFP Diluent
1 vial of AFP Diluent containing horse serum with Sodium Azide (0.09% w/w) andProclin 300 (0.0025% v/v) as preservatives. 13 ml. Ready for use. Mix gentlybefore use.
4.4 Biotine-AFP Conjugate
1 vial containing a monoclonal antibody to AFP labeled with Biotin in Tris bufferwith bovine serum albumin (BSA) and Proclin 300 (0.0025% v/v) as preservative.13 ml. Ready for use. Mix gently before use.
4.5 HRP-AFP Conjugate
1 vial containing a monoclonal antibody to AFP labeled with Hoerseradish Peroxidasein Tris buffer with bovine serum albumin (BSA) and Proclin 300 (0.0025% v/v) aspreservative. 13 ml. Ready for use. Mix gently before use.
1 / 4
MT PLATE
CAL A...F
Biotine-AFP Conjugate
HRP-AFP Conjugate
96 Tests
FOR IN VITRO DIAGNOSTIC USE ONLY
Store at 2...8°C
SYMBOL USED ON LABELS
LI4017KREF
en
EIAgen AFP
Adaltis Italia S.p.A.Via Cristoni, 1240033 Casalecchio di Reno - (BO) ItalyTel. +39-051-6136511 - Fax +39-051-575280www.adaltis.com
Manufactured by:Production PlantVia L. Einaudi, 700012 Guidonia Montecelio - (Rome)Italy
∑∑∑∑∑
Temperature limitation (store at 2...8°C)
Streptavidin Microplate
Attention, See Instruction for Use
AFP Calibrator B
AFP Calibrator C
AFP Calibrator D
AFP Calibrator E
AFP Calibrator F
Catalogue Code
Expiry date (Use by...)
Number of tests
Lot number
AFP Calibrator A
In vitro diagnostic medical device(In vitro diagnostic use)
AFP Diluent
Manufactured by...
Wash Solution 10x
8°C
2°C
R E F
LOT
IVD
Substrate HS
Stop Solution
∑∑∑∑∑
!!!!!
Biological Risk
CONJ BIOT
Avoid exposure to direct sunlight
CONJ HRP
MT PLATE
CONJ BIOT
CONJ HRP
SUBS TMB
SOLN STOP
BUF WASH 10 X
DIL SPE
DIL SPE
CAL A
CAL B
CAL C
CAL D
CAL E
CAL F
2 / 4
4.6 Washing Solution 10x
1 vial of Washing Solution 10x containing Tween 20 (0.1%) and Amphotericin-B(2.5 µg/ml) in citrate-borate buffer. 50 ml.Dilute the contents of the vial to a volume of 500 ml with distilled or deionizedwater. Mix well. After dilution store at 2...8°C for 2 months or at room temperaturefor 5 days.
4.7 Substrate HS
1 vial of Substrate HS containing 0.26 mg/ml of 3,3’,5,5’ Tetramethylbenzidin(TMB) and 0.01% w/v of Hydrogen peroxide (H2O2), in citrate buffer. 13 ml.Ready for use. Mix gently before use.
4.8 Stop Solution
1 vial of Stop Solution containing Sulfuric acid (H2SO4) 0.3 mol/l. 13 ml.Ready for use. Mix gently before use.
5.0 MATERIALS AND EQUIPMENT REQUIRED
5.1 Materials Provided
Material Quantity Code
Streptavidin Microplate One bag LSSTREPPBAFP Calibrator A 0.5 ml LS4017SK-AAFP Calibrator B 0.5 ml LS4017SK-BAFP Calibrator C 0.5 ml LS4017SK-CAFP Calibrator D 0.5 ml LS4017SK-DAFP Calibrator E 0.5 ml LS4017SK-EAFP Calibrator F 0.5 ml LS4017SK-FAFP Diluent 13.0 ml LS4017SK0Biotine-AFP Conjugate 13.0 ml LS4017BKHRP-AFP Conjugate 13.0 ml LS4017EKWashing Solution 10X 50.0 ml LSWASHKSubstrate HS 13.0 ml LSTMBH2O2HKStop Solution 13.0 ml LSSTOPK
5.2 Materials and Equipment Not Provided● Distilled or deionized water.● Precision 0.025, 0.1 ml pipette with disposable tips.● 0.1 ml repeating dispenser or positive displacement pipettes for addition of
Conjugate, Substrate and Stop Solution.● Automatic plate washer.● Microtiter incubator.● Microtiter plate reader, equipped for the measurement of the absorbance at
450 nm (reference filter at 620 nm).● Adsorbent pad or paper.● Control sera (recommended).
6.0 WARNING, PRECAUTIONS AND LIMITATIONSFor in vitro diagnostic use.Only experienced laboratory personnel should use this test and handling shouldbe in agreement with GLP.
6.1 Safety Precautions● Do not pipet by mouth.● Do not smoke, eat or apply cosmetics in areas in which patients samples or
kit reagents are handled.● Cuts, abrasions, and other skin lesions should be properly protected with an
appropriate waterproof dressing.● Take care to avoid self-inoculation, splashing of mucous membranes or
generation of aerosols.● Laboratory gloves should be worn while handling patient samples or disposing
of solid or liquid wastes.● Avoid microbial contamination of standards during pipetting by using disposable
pipet tips.● Disposal of all waste should be in accordance with local regulations.
6.2 Potential Biohazard WarningSome reagents used may have been prepared from pools of human serum. Eachunit of blood used to prepare these pools were tested and found non reactive forsyphilis, for the presence of Hepatitis B Surface Antigen (HBsAG) and for antibodiesto Human Immunodeficiency Virus (HIV 1 and 2) using an FDA approved method.Because no test can offer complete assurance that Hepatitis B virus, HIV or otherinfectious agents are absent, these reagents should be considered as potentiallybiohazardous and handled with the same precautions as applied to any serum orplasma samples. Some reagents such as calibration standards and control maycontain materials of human tissue origin. At present there is no standard test methodfor the presence of HIV in such material. It is therefore recommended that thesereagents are also considered as potentially biohazardous.Such materials should be handled according to good laboratory practices, as describedin CDC (Center for Disease Control, Atlanta U.S.) document: Universal precautionsfor prevention of transmission of human immunodeficiency virus, hepatitis B virus,and other blood bourne pathogens in healthcare setting “MMWR” 37:377-387, 1999.
6.3 Sodium Azide (NaN3) WarningSodium azide is present as a preservative in the standard matrix at a concentrationof no more than 0.09% w/w. Sodium azide may react with lead and copper plumbingto form explosive metal azides. Liquid and solid wastes should be disposed ofsafely, in accordance with local regulations. Azide at concentration higher than0.1% w/w interfere in this assay, therefore the assay of control sera or samplescontaining the above compound may give overestimated results.
Risk PhrasesR 21/22 Harmfull in contact with skin and if swallowed.Safety PhrasesS 26 In case of contact with eyes, rinse immediately with plenty of water and
seek medical advice.S 28.1 After contact with skin, wash immediately with plenty of water.S 46 If swallowed seek medical advice immediately and show the container or
label.
6.4 Sulphuric Acid (H2SO4) WarningSulphuric Acid is present in the Stop Solution at a concentration of no more than0.3 mol/l. Do not pipette by mouth.Risk PhrasesR 36/38 Irritating to eyes and skin.Safety PhrasesS 26 In case of contact with eyes, rinse immediately with plenty of water and
seek medical advice.
6.5 3-3’-5-5’ Tetramethylbenzidine (TMB) WarningTMB (3-3’-5-5’ Tetramethylbenzidine) is present in the Substrate HS. Avoid contactof this reagent with skin and mucous membranes. Should this occur, wash thoroughlywith cold tap water. Do not pipette by mouth.
6.6 LimitationsDo not use EDTA as an anticoagulant at concentration higher than 5 g/l. Dilutionswhich provide values less than the detection limit of the assay should not be used.Since the enzymatic reaction is temperature dependent, different absorbances canbe obtained according to the laboratory temperature.As with all immunoassays, the results of this test can be influenced by factorspresent in some patients‘ specimens. The reagents for this assay have been formulatedto minimise interference from heterophilic antibodies and from non-specific proteinbinding. However, in common with other two-site immunoassay methods, individualsample results may be affected.For diagnostic purposes, the results obtained from this assay should always be usedin combination with the clinical examination, patient medical history, and other findings.Procedural directions must be followed exactly as any modification of the proceduremay change the results.Use of reagents, disposables or spare parts other than those supplied by authorizeddistributor may produce incorrect results.Patients who have received mouse monoclonal antibodies for either diagnosis ortherapy can develop human anti-mouse antibodies (HAMA). HAMA can produceeither falsely high or falsely low values in immunoassays which use mouse monoclonalantibodies (15, 16). Samples containing HAMA should not be assayed with theEIAgen AFP assay.
6.7 Indications of Substrate deterioration● The Substrate single solution is colourless or slightly yellow-blue. If accidental
contamination occur, the solution starts to develop a blu colour and musttherefore be discarded.
● The Substrate single solution is not sensitive to light. Direct sunlight canhowever oxidize the solution to a blue colour. Such a colour disappears after4 hours storage in the dark after which the solution can again be used.
● On aging the substrate may became of slight yellow-orange colour. This doesnot affect its performances.
● Should only part of the Substrate vial content be used, in order to avoidcontamination, transfer the volume needed into a clean plastic containerwhich has previously been washed with ethanol and rinsed with high-qualitydistilled water.
7.0 SPECIMEN COLLECTION AND STORAGE
7.1 SerumCollect 5 ml of venous blood in a glass tube without additives. Allow to clot at roomtemperature. Centrifuge, separate the serum fraction, and store.
7.2 PlasmaCollect 5 ml of venous blood in a glass or plastic tube containing heparin or citrateas an anticoagulant. Centrifuge, separate the serum fraction, and store.
7.3 Amniotic FluidCollect amniotic fluid samples into a sterile plastic tube without additives.
7.4 DilutionSerum and plasma samples with concentrations expected to be greater than 500IU/ml should be diluted in the AFP Diluent before assay.Amniotic fluid should be diluted at least 1:100.
7.5 StorageSerum, plasma and amniotic fluid specimens are stable for up to 24 hours at2...8°C. For longer storage, aliquot and store at -20°C for up to 90 days.Avoid repeated freezing and thawing.
7.6 Known InterferenceAvoid using the following types of serum or plasma samples as these may giveincorrect results:Grossly hemolyzed samples;Grossly lipemic samples:Grossly icteric samples;EDTA anticoagulated plasma samples with EDTA concentration higher than 5 g/lshould not be used.If amniotic fluid specimens are contamined with blood, the origin of hemoglobinshould be determined.Owing to high circulating levels of AFP in fetal plasma,pecimens contaminated with fetal blood should not be used.
SUBS TMB
SOLN STOP
BUF WASH 10 X

8.0 ASSAY PROCEDURE
8.1 Preparation for Assay1. Allow reagents to warm to room temperature and mix gently before using.2. For each assay, prepare the following groups of wells and place in the strip
holder:● 2 wells for the chromogen blank (optional for QC);● 2 wells for Bo (zero concentration of antigen);● 2 wells for each calibrator concentration;● 2 wells for each serum, plasma or control.
For the chromogen blank pipette 0.1 ml of Substrate HS and 0.1 ml of Stop Solutioninto the two wells.
8.2 Pipetting and Incubation steps1. Pipette 0.025 ml of calibrators, samples and controls into the appropriately
wells of the strip.2. Pipette 0.1 ml of Biotine-AFP conjugate into each wells.3. Gently shake the entire plate using a side-to-side motion or an orbital shaker
for 10 seconds.4. Incubate at 37°C for 30 minutes.5. Washing: discard the incubation solution, Rinse the wells with the Washing
Solution three times and remove any residual liquid.6. Pipette 0.1 ml of HRP-AFP conjugate into each wells.7. Gently shake the entire plate using a side-to-side motion or an orbital shaker
for 10 seconds.8. Incubate at 37°C for 30 minutes.9. Washing: discard the incubation solution, Rinse the wells with the Washing
Solution three times and remove any residual liquid.10. Pipette 0.1 ml of Substrate HS into each wells and gently shake.11. Incubate at room temperature for 15 minutes.12. Stop reaction by adding 0.1 ml of Stop Solution to each wells in the sequence
and at the same frequency used to pipette the Substrate HS.13. Shake the microplate gently being careful to avoid splashing.14. Read to 450 nm within 1 hour from dispensing the Stop Solution.
8.3 Procedural Notes1. Room temperature is defined between 18°C and 25°C.2. A standard curve must be run in each assay to assure valid results.3. Reagents from different Kits and lots should not be mixed.4. Add the reagents in the same order as the calibrators and samples.5. It is recommended to time the addition of the chromogen/substrate solution
and stop solution until familiar with the method (i.e. if the chromogen/substratesolution is dispensed into the wells every 3 seconds one from each other, thestop solution should also be dispensed in the same order and at the samefrequency).
6. The total dispensing time of calibrators, controls and speciments for a wholeplate should not exceed 15 minutes.
7. Washing procedure: for the washing procedure, the use of an automatic platewash equipment is recommended. After washing, tap the inverted plate onabsorbent paper to remove any residual from the wells. Three washings arerequired.
9.0 CALIBRATIONAFP Calibrators are calibrated against the 1st IRP 72/225.1.0 IU AFP EIAgen Calibrator = 1.0 IU 1st IRP 72/225For conversion to ng/ml, multiply the AFP results in IU/ml by 1.21.
10.0 QUALITY CONTROLIt is recommended that each laboratory routinely use quality control materials andestablish its own control ranges. Multi-level controls should be used in each AFP run.The AFP values obtained for the quality control material should not repeatedly falloutside the control ranges established in each laboratory.
11.0 CALCULATION OF RESULTS
11.1 Optical Density (OD) ConversionThe Optical Density (OD) of the calibrators at 500 IU/ml may result around 2.5. Ifthe reader can read ODs up to 2.5, then the reading at 450 nm (wavelength of thepeak) and at 620 nm (reference filter for the subtraction of interference of theplastic) is sufficient. Should the reader not be able to read up to 2.5, then the userhas two choices:1. omitting to run the calibrator at 500 IU/ml.2. running also the calibrator at 500 IU/ml and then reading, in addition at 450 nm,
also at 405 nm (in the peak shoulder) always aginst the subtraction filter at620 nm. Identify the wells with OD higher than 2.0 at 450 nm both forcalibrators and samples record the corrisponding OD at 405 nm and multiplythese ODs by the conversion factor 3.0 since:OD 450 nm = OD 405 nm x 3.0 (for this substrate)
The automatic instruments: Labotech, Allertech and Personal Lab can automaticallyread contemporaneously at 450- 405 and 620 nm and multiply by 3.0 the ODs at405 nm which result higher than 2.0 at 450 nm, once this option is selected.
11.2 Data Reduction - Manual MethodCalculate, as previously described, the mean OD at 450 nm of calibrators andsamples. Plot the mean ODs of calibrators versus the respective AFP concentrationon logit/log or semilog graph paper and determine the concentration of AFP in thesample by interpolation from calibration curve. The results can also be calculatedwith normal programs for automatic data processing, i.e. 4 Parameters, Spline.
11.3 Data Reduction - Automated MethodUse the 4 parameters logistic - preferred - or the smoothed cubic spline function ascalculation algorithm
11.4 Samples with ODs higher than calibrator at 500 IU/mlShould AFP value exceed the highest calibrator value, dilute the sample with thediluent or zero calibrator and re-run the assay multiply the result obtained by thesample dilution factor.
11.5 Typical Calibrator Curve
Calibrator (IU/ml) Manual Method Labotech MethodOD 450 nm OD 450 nm
0 0.018 0.0385 0.130 0.137
25 0.445 0.442125 1.408 1.493250 2.050 1.938500 2.662 2.503
12.0 EXPECTED VALUESNormal range for healthy (non-pregnant) subjects is <10 IU/ml AFP.The values given are indicative only and may vary from other published data, asthe concentration of AFP measured in individuals varies with different methods.It is recommended that each laboratory establishes its own reference values.
12.1 Factors Associated with Increased ValuesElevated AFP levels have been observed with high frequency in serum frompatients with hepatocellular carcinoma and certain germ-cell tumours of the testesand ovaries (6, 7). Elevated AFP levels have also been observed in non-malignantconditions such as viral hepatitis (18) and liver cirrhosis (19).In certain fetal abnormalities, notably open neural tube defects (NTD), elevatedAFP levels have been observed in both amniotic fluid (9) and maternal serum (20).High maternal serum AFP concentrations have also been observed in other fetaldistress conditions such as omphalocele (21) and threatened abortion (22), and inmultiple pregnancies (23).Endogenous factors e.g. human anti-mouse antibodies, in human serum have beenobserved to cause falsely elevated antigen values in immunoassays (16).
12.2 Factors Associated with Decreased ValuesLow maternal serum and amniotic fluid AFP values have been observed in molarpregnancy and in Down’s syndrome (24).Endogenous factors e.g. human anti-mouse antibodies, in human serum have beenobserved to cause falsely decreased antigen levels in immunoassays (16).
13.0 PERFORMANCE CHARACTERISTICSThe EIAgen AFP assay has been designed so that the “High-Dose Hock” effect,characteristic of immunometric assays, will not interfer with AFP values up to350000 IU/ml.
13.1 Accuracy - Recovery TestRecovery test was performed by adding purified AFP to pooled serum samples.The neat and spiked samples were measured in the EIAgen AFP assay.Recovery data
Sample AFP Added AFP Measured % Recovery(IU/ml) (IU/ml)
1 0 5.00 -46.40 45.50 98.1090.30 88.60 98.10
178.10 172.30 96.70353.70 350.80 99.20
2 0 52.70 -46.40 99.60 104.2090.30 137.00 98.80
178.10 225.00 100.20353.70 370.00 93.40
3 0 42.00 -46.40 80.60 94.6090.30 118.30 92.20
178.10 199.20 92.80353.70 359.60 92.80
13.2 Accuracy - Dilution TestThree serum samples containing elevated concentration of AFP were diluted withAFP Diluent and assayed at multiple dilutions.Dilution data
Sample Dilution AFP AFPFactor Expected Recovered % Recovery
(IU/ml) (IU/ml)
- - 191.20 -A 1:2 95.60 91.90 96.1
1:4 47.80 45.70 95.61:8 23.90 24.80 103.8
1:16 11.95 11.40 95.41:32 5.98 6.50 108.8
- - 120.70 -B 1:2 60.35 58.60 97.1
1:4 30.18 29.62 98.21:8 15.09 15.02 99.6
1:16 7.54 7.53 99.81:32 3.77 3.82 101.3
- - 115.00 -C 1:2 57.48 57.52 100.1
1:4 28.74 26.63 92.71:8 14.37 13.70 95.3
1:16 7.18 6.21 86.41:32 3.59 3.16 88.0
3 / 4

13.3 PrecisionWithin-assay (Intra-assay) coefficient of variation was evaluated on serum poolsand Control sera measured 20 times in the same assay within assay precisionresults are shown below:
Manual Method
Sample N. Mean ± 1SD %C.V.(IU/ml)
Level 1 20 27.0 ± 1.63 6.0Level 2 20 76.8 ± 4.55 5.9Level 3 20 198.0 ± 15.71 7.9
Between assay (Inter-assay) coefficient of variation was evaluated on serumpools and Control sera measured in more than 10 AFP EIAgen runs. Between assayprecision results are shown below:
Manual Method
Sample N. Mean ± 1SD %C.V.(IU/ml)
Level 1 13 27.0 ± 1.58 5.7Level 2 13 83.8 ± 7.92 9.4Level 3 13 213.5 ± 17.93 8.4
13.4 SensitivityThe sensitivity of the assay, definited as the concentration of AFP equivalent tothe mean absorbance of Zero plus two standard deviations based on 20 replicatesof a zero analyte sample, is typically <0.05 IU/ml using manual and automated(Labotech) methods.
13.5 SpecificityThe specificity of AFP EIAgen assay was assessed by measuring the apparentAFP response caused by high levels of various potentially cross reactive analytes.
Analyte Concentration Apparent %CrossAFP Value Reactivity
(IU/ml)
hCG 500 µIU/ml (1st IRP 75/537) N.D. -CA 125 15000 U/ml N.D. -CA 19-9 20000 U/ml 1.94 0.01Estriol 500000 ng/ml N.D. -Estradiol 500000 ng/ml N.D. -
N.D.= Not Determinable
13.6 Correlation with Other MethodsThe EIAgen AFP assay was compared with a RIA Method (AFP Bridge) and a EIAmethod (SR1 AFP). The regression analysis of the data gave the following results:
y = 1.00x - 1.15r = 0.96x = Reference RIA Method (AFP Bridge)y = EIAgen AFPn = 73
y = 0.86x -1.32r = 0.98x = Reference EIA Method (SR1 AFP)y = EIAgen AFPn = 76
14.0 AUTOMATIONApplication protocols for the proper automation on the Adaltis microplate analyzersare available upon request at Adaltis directly.
15.0 BIBLIOGRAPHY1. SIZARET, P., ANDERSON, S.G., The International Reference Preparation for
alpha-fetoprotein. J. Biol. Standardization 4:149, 1976.2. ABELEV, G.I., Production of embryonal serum Alpha-globulin by hepatomas.
Review on Experimental and Clinical Data. Cancer Res. 28:1344, 1968.3. MACKIEWICZ, A., BREBOROWICZ,.I, The in-vitro production of Alpha-
fetoprotein variants by human fetal organs. Oncodev. Biol. Med. 1:251, 1980.4. URANO, Y., SAKAI, M., WATANABE, K., TAMAOKI, T., Tandem arrangements
of the Albumin and Alpha-fetoprotein genes in the human genome. Gene 22:225,1984.
5. RUOSLAHTI, E., SEPPALA, M., Studies of carcino-fetal proteins. Physical andChemical properties of human Alpha-fetoprotein. Int. J. Cancer 7:218, 1971.
6. MASOPUST, T., KITHIER, K., RADL, J., KOUTECKY, J., KOTAL, L., Occurrenceof fetoprotein in patients with neoplasma and non-neoplastic diseases. Int. J.Cancer 3:364, 1968.
7. WALDMANN, T.A., MCINTIRE, K. R., The use of a radioimmuno-assay forAlpha-fetoprotein in the diagnosis of malignancy. Cancer 34:1510, 1974.
8. ABELEV, G. I., Alpha-fetoprotein in ontogenesis and its association with malignanttumours. Adv. Cancer Res. 14:295, 1971.
9. BROCK, D. J. H., Mechanism by which amniotic fluid Alpha-fetoprotein may beincreased in fetal abnormalities. Lancet (ii): 345, 1976.
10. GITLIN, G., Normal biology of Alpha-fetoprotein. Ann. N. Y. Acad. Sci. 259:7,1975.
11. RUOSLAHTI, E., HIRAR, H., Alpha-fetoprotein: Physiology and Pathologyduring pregnancy and application to antenatal diagnosis. Scand. J. Immunol.8:3, 1978.
12. MASSEYEFF, R. F., Alpha-fetoprotein: Use in screening. In Immunodiagnosisof Cancer. HERBERMAN, R.B., and MCINTIRE, R. K., (Eds) Marcell DekkerInc. New York pp 117 - 129, 1979.
13. SCARDINO, R. T., COX, H. D., WALDMANN, T. K., McINTIRE, K.P.,MITTEMEYER, B., JAVADPOUR, N. , The value of serum tumour markers in thestaging and prognosis of germ cell tumours of the testis. J. Urol. 118:994, 1977.
14. LANGE, P. H., MCINTIRE, K. R., WALDMANN, T. A., HAKALA, T.R., FRALEY,E.E., Serum Alpha-fetoprotein and human chorionic gonadotrophin in the diagnosisand management of non-seminomatous germ cell testicular cancer. New Engl.J. Med. 295:1237, 1976.
15. KINDERS, R.J., HASS, G.M., Interference in immunoassay by human anti-mouse antibodies. Eur. J. Cancer. 26 (5):647, 1990.
16. BOSCATO, L.M., STUART, M.C., Incidence and specificity of interference intwo-site immunoassays. Clin. Chem. 32 (8): 1491, 1986.
17. HORACEK, K.L., PEPPERELL, R.J., HAY, D.L., BARRIE, J.V., BATTERY,B.W., Detection of feto-maternal hemorrhage by measurement of maternalserum AFP. Lancet (ii) : 200, 1976.
18. KEW, M.C., PURVES, L.R., BERSOHN, I., Serum alpha-fetoprotein levels inacute viral hepatitis. Gut 14:939, 1973.
19. SAKAMOTO, S., YACHI, A., ANZAI, T., WADA, T., Alpha-fetoprotein producingcells in hepatitis and in liver cirrhosis. Ann. N.Y. Acad. Sci. 259:253, 1975.
20. MACRI, J.N., WEISS, R.R., Prenatal serum alpha-fetoprotein screening forneural tube defects. Obstet. Gynecol. 59:633, 1982.
21. PALOMAKI, G.E., HILL, L.E., KNIGHT, G.J., HADDOW, J.E., CARPENTER,M., Second trimester maternal serum alpha-fetoprotein levels in pregnanciesassociated with gastroschisis and omphalocele. Obstet. Gynecol. 71:906, 1988.
22. WALD, N., BARKER, S., CUCKLE, H., BROOK, D.J.H., STIRRAT, S.M., Maternalserum alpha-fetoprotein and spontaneous abortion. Br. J. Obstet. Gynecol.84:357, 1977.
23. REDFORD, D.H., WHITFIELD, C.R., Maternal serum alpha-fetoprotein in twinpregnancies uncomplicated by neural tube defect. Am. J. Obstet. Gynecol.152(5):550, 1985.
24. DAVENPORT, D.M., MACRI, J.N., The clinical significance of low maternalserum alpha-fetoprotein. Am. J. Obstet. Gynecol. 146:657, 1983.
936LI4017K/040705
4 / 4

Adaltis Italia S.p.A.Via Cristoni, 1240033 Casalecchio di Reno - (BO) ItalyTel. +39-051-6136511 - Fax +39-051-575280www.adaltis.com
Hersteller:ProduktionsstätteVia L. Einaudi, 700012 Guidonia Montecelio - (Rome)Italy
1.0 VERWENDUNGDas Testsystem EIAgen AFP dient der quantitativen Bestimmung von Alpha-Fetoprotein in humanem Serum, Plasma oder Fruchtwasser.Die Kalibratoren sind gegen die 1.IRP für humanes AFP 72/225 (WHO) standardisiert.
2.0 PHYSIOLOGIEAlpha-Fetoprotein (AFP) ist ein fetales Serum-protein, das bei gesunden Erwachsenenin geringen Mengen im Blut zirkuliert (2). AFP wird haupt-sächlich im Dottersack undin der fetalen Leber produziert, in geringerer Menge auch im fetalenGastrointestinaltrakt und in den Nieren (3). Es ist ein einkettiges Glykoprotein miteinem Molekular-gewicht von 65000-70000 Dalton. Die physiko-chemischenEigenschaften und die Aminosäuren-zusammensetzung von AFP sind ähnlich wie beimSerumalbumin (4), die antigenen Eigenschaften sind aber unterschied-lich (5).Klinisches Interesse an AFP besteht auch im onkologischen Bereich, wo dieSerumbestimmung für die Diagnose und Überwachung von Tumoren eingesetztwird (6, 7, 8) und im pränatalen Screening, wobei die Bestimmung von AFP inFruchtwasser zum Screening für foetale Anomalitäten wie Spina bifida und Down-Syndrom eingesetzt wird.Das fetale Plasma-AFP wird über den fetalen Urin ins Fruchtwasser ausgeschieden;von dort gelangt es über die Plazenta in den mütterli-chen Blutkreislauf. In der 12.-14. Schwangerschafts-woche erreicht das AFP im fetalen Plasma seine höchsteKonzentration (2-3 mg/ml) und fällt dann rapide ab (9). Die Werte im Fruchtwasserverlaufen parallel zu denen im fetalen Plasma, liegen aber etwa um die Hälfteniedriger (im µg Bereich). Im Gegensatz dazu steigt die AFP-Konzentration immütterlichen Serum kontinuierlich bis zur 30. SSW an und fällt danach ab (10).Nach der Geburt fallen die AFP-Werte sowohl bei der Mutter als auch beim Kindschnell auf die Basalwerte zurück (< 10 ng/ml).Bei ca. 70 % der Patienten mit primären hepato-zellulären Tumoren sind erhöhteAFP-Werte nachweisbar (7); es wird von Werten zwischen 1000 und 10000 ng/mlberichtet (11). Bei testikulären Teratomen besteht eine direkte Korrelation zwischendem Auftreten erhöhter AFP-Werte und dem Stadium der Erkrankung (12). Beitestikulären Seminomen werden keine erhöhten AFP-Werte gefunden (13). DerNutzen der AFP-Bestimmung bei Tumorpatienten ist gut belegt (14). Wenn AFP-Werte postoperativ nicht in den Normalbereich zurückkehren, deutet dies auf dasVorhandensein eines Tumorrestes hin.Auch bei benignen Erkrankungen wie akuten Virusinfektionen, chronischerVirushepatitis und bei Leberzirrhose wurden erhöhte AFP-Werte im Serum beobachtet.Bei fetaler Fehlentwicklung wie Omphalocele oder Turner Syndrom sowie beiintrauterinem Tod wurden erhöhte AFP-Werte im Fruchtwasser gefunden.
3.0 TESTPRINZIPDer Testsatz EIAgen AFP ist ein Two-Step-Assay nach dem Sandwich-Prinzip inVerbindung mit der Biotin-Streptavidin-Technologie.Es werden zwei monoklonale Anti-AFP-Antikörper von hoher Affinität und Spezifitätverwendet: einer ist an Meerrettich-Peroxidase gekoppelt und der andere an Biotin.Die Wells der Mikrotiterplatte sind mit Streptavidin beschichtet.Proben, Kalibratoren und Kontrollen werden in die Wells pipettiert, gefolgt von eineBiotin-Anti-AFP-Konjugat.Während der Inkubation bindet der Antikörper an ein spezifisches Epitop des AFP-Moleküls und gleichzeitig immobilisiert das Streptavidin den immunologischenKomplex an die Wells, durch die Bindung an den Biotinteil des Biotin-gekoppeltenAntikörpers.Nach dem Waschen zur Entfernung des Nichtgebundenen wird der zweite, an HRP-gekoppelte Antikörper zugefügt. Nach der zweiten Inkubation und nach Waschenwird die Mischung aus Chromogen/Substrat zugefügt. Die Reaktion wird durchZugabe der Stopplösung beendet und die entstandene Farbe photometrisch gemessen.Die Farbintensität ist innerhalb des Messbereichs des Assays direkt proportionalzur AFP-Konzentration in der Probe. Die AFP-Konzentration in den Patientenprobenund Kontrollen wird durch Interpolation aus der Standardkurve ermittelt.
4.0 REAGENZIEN – LAGERUNG UND HANDHABUNGDer Testsatz EIAgen AFP enthält Reagenzien für 96 Einzelbestimmungen. Der Kitist bei 2...8°C bis zum angegebenen Verfallsdatum haltbar. Falls nicht andersangegeben, sind die Reagenzien auch nach dem ersten Öffnen bis zum auf denEtiketten angegebenen Verfallsdatum haltbar, vorausgesetzt, sie werden wieangegeben gelagert und während des Pipettierens erfolgt keine Kontamination
4.1 Streptavidin Microplate
Die Packung enthält eine Mikrotiterplatte mit 12 Streifen x 8 Wells (einzeln brechbar),beschichtet mit Streptavidin. Vor Gebrauch auf Raumtemperatur (18...25°C) bringen.Nach dem ersten Öffnen sind die Streifen bei 2...8°C 2 Monate haltbar,Vorausgesetzt, sie werden mit dem beigefügten Trockenmittel in der gutverschlossenen Originalpackung gelagert.
4.2 AFP Calibrators
Kalibratoren; 6 Fläschchen mit AFP in den Konzentrationen 0- 5- 25- 125- 250- 500IU/ml (1. IRP 72/225), in Pferdeserum mit 0,09 % Natriumazid und 0,0025 % Proclin300. Je 0,5 ml/Fläschchen. Gebrauchsfertig. Vor Gebrauch vorsichtig mischen.
4.3 AFP Diluent
Probenverdünnungslösung; 1 Fläschchen AFP Diluent enthält Pferdeserum mit0,09 % Natriumazid und 0,0025 % Proclin 300 als Konservierungsmittel. 13 ml.Gebrauchsfertig. Vor Gebrauch vorsichtig mischen.
4.4 Biotine-AFP Conjugate
Konjugat; 1 Fläschchen, enthält einen monoklonalen Antikörper gegen AFP, gekoppeltmit Biotin, in Tris-Puffer mit Rinderserumalbumin (BSA) und 0,0025 % Proclin 300als Konservierungsmittel. 13 ml. Gebrauchsfertig. Vor Gebrauch vorsichtig mischen.
4.5 HRP-AFP Conjugate
Konjugat; 1 Fläschchen, enthält einen monoklonalen Antikörper gegen AFP, gekoppeltmit Meerrettichperoxidase (HRP), in Tris-Puffer mit Rinderserumalbumin (BSA) und
1 / 4
Biotine-AFP Conjugate
HRP-AFP Conjugate
96 Bestimmungen
NUR ZUR IN-VITRO DIAGNOSTIK
Lagerung bei 2...8 °C
SYMBOLE, DIE AUF DEN ETIKETTEN VERWENDET WERDEN
LI4017KREF
de
EIAgen AFP∑∑∑∑∑
Lagerung bei... (2...8°C)
Streptavidin Microplate
Achtung, Gebrauchsanweisungbeachten
AFP Calibrator B
AFP Calibrator C
AFP Calibrator D
AFP Calibrator E
AFP Calibrator F
Bestellnummer
Verwendbar bis...
Anzahl der Bestimmungen
Lotnummer
AFP Calibrator A
In-vitro Diagnostikum
AFP Diluent
Hersteller...
Wash Solution 10x
8°C
2°C
R E F
LOT
IVD
Substrate HS
Stop Solution
∑∑∑∑∑
!!!!!
Biogefährdung
Nicht direktem Sonnenlicht aussetzen
MT PLATE
CAL A...F
CONJ BIOT
CONJ HRP
MT PLATE
CONJ BIOT
CONJ HRP
SUBS TMB
SOLN STOP
DIL SPE
BUF WASH 10 X
CAL A
CAL B
CAL C
CAL D
CAL E
CAL F
DIL SPE

0,0025 % Proclin 300 als Konservierungsmittel. 13 ml. Gebrauchsfertig. Vor Gebrauchvorsichtig mischen.
4.6 Washing Solution 10x
Waschpufferkonzentrat, 10fach konzentriert; enthält 0,1 % Tween 20 und 2,5 µg/mlAmphotericin-B, in Citrat-Borat-Puffer. 50 ml. Verdünnen Sie den Inhalt mit 450 mldestilliertem oder deionisiertem Wasser. Gründlich mischen. Lagerung nachVerdünnung 2 Monate bei 2...8°C oder 5 Tage bei Raumtemperatur.
4.7 Substrate HS
Substrat; 1 Fläschchen mit 0,26 mg/ml 3,3',5,5'-Tetramethylbenzidin und 0,01 %Wasserstoffperoxid (H
2O
2), in Citrat-Puffer. 13 ml.
Gebrauchsfertig. Vor Gebrauch vorsichtig mischen.
4.8 Stop Solution (H2SO4)
Stopplösung; 1 Fläschchen mit 0,3 mol/l Schwefelsäure (H2SO4). Gebrauchsfertig.Vor Gebrauch gründlich mischen.
5.0 BENÖTIGTE MATERIALIEN UND ZUBEHÖR
5.1 Packungsinhalt
Reagenz Inhalt Code
Streptavidin Microplate 1 Beutel LSSTREPPBAFP Calibrator A 0,5 ml LS4017SK-AAFP Calibrator B 0,5 ml LS4017SK-BAFP Calibrator C 0,5 ml LS4017SK-CAFP Calibrator D 0,5 ml LS4017SK-DAFP Calibrator E 0,5 ml LS4017SK-EAFP Calibrator F 0,5 ml LS4017SK-FAFP Diluent 13 ml LS4017SK0Biotine-AFP Conjugate 13 ml LS4017BKHRP-AFP Conjugate 13 ml LS4017EKWashing Solution 10x 50 ml LSWASHKSubstrate HS 13 ml LSTMBH2O2HKStop Solution 13 ml LSSTOPK
5.2 Zusätzlich benötigtes Material● Destilliertes oder deionisiertes Wasser● Präzisionspipette mit Einmal-Spitzen für 0,025 ml und 0,1ml● Dispenser für 0,1 ml● Automatischer Plattenwasher● Photometer für Mikrotiterplatten für die Messung bei 450 nm (mit Referenzfilter
bei 620 nm)● Saugfähiges Papier● Kontrollseren
6.0 HINWEISE UND VORSICHTSMASSNAHMENNur zur In-vitro-Diagnostik bestimmt.Mit diesem Test sollte nur Fachpersonal arbeiten. Der Umgang sollte nachMaßgabe der „Guten Laborpraxis” (GLP) erfolgen.
6.1 Sicherheitsmaßnahmen• Reagenzien nicht mit dem Mund pipettieren.• Während der Handhabung von Patientenproben und Reagenzien nicht rauchen,
essen oder trinken und keine Kosmetika anwenden.• Hautverletzungen sollten wasserdicht geschützt sein.• Kontakt mit Augen, Haut oder Schleimhaut vermeiden.• Beim Umgang mit Proben oder Abfall sollten Schutzhandschuhe getragen werden.• Mikrobielle Verunreinigung der Reagenzien durch Verwendung von Einmal-
Pipettenspitzen vermeiden.• Die Abfallentsorgung sollte gemäß der lokalen und nationalen Gesetze und
Vorschriften erfolgen.
6.2 Bestandteile humanen UrsprungsEinige Reagenzien enthalten Bestandteile, die aus humanen Serumpools gewonnenwurden. Jede dafür verwendete Blutprobe wurde individuell mit einer von der FDAzugelassenen Methode auf Syphilis, Hepatitis-B-Oberflächenantigen (HBsAg) undAnti-HIV 1 und 2 überprüft und negativ gefunden. Da keine Testmethode eineabsolute Sicherheit bieten kann, dass keine Hepatitis B-Virus, HIV oder andereInfektionserreger vorhanden sind, sollten diese Reagenzien als potentiell infektiosbetrachtet und mit derselben Vorsicht wie die Patientenproben behandelt werden.Einige Reagenzien, wie z.B. die Kalibratoren, enthalten Materialien, die aus humanemGewebe stammen. Z.Z. gibt es noch keine Standardtestmethode für den Nachweisvon HIV in solchen Materialien. Es wird daher empfohlen, auch diese Reagenzienals potentiell infektiös zu betrachten.Diese Reagenzien sollten entsprechend der „Guten Laborpraxis” (GLP) und evt.nationaler Sicherheitsrichtlinien für potentiell infektiöse Materialien gehandhabt werden(z.B. USA Center for Disease Control/National Institutes of Health Manual „Biosafetyin Microbiological and Biomedical Laboratories”, 4. Aufl. 1999).
6.3 NatriumazidDie Kalibratoren enthalten Natriumazid. Natriumazid kann mit Blei und Kupferexplosive Metallazide bilden. Reagenzienreste sollten daher mit reichlich Wasserverdünnt beseitigt werden. Nicht mit Haut oder Schleimhaut in Berührung bringen.Azide in einer Konzentration von >0,1 % interferieren in diesem Assay. Daherkönnen Kontrollen oder Proben, die eine höhere Konzentration haben, zu falschhohen Ergebnissen führen.Risiko-Sätze:R-21/22 Gesundheitsschädlich beim Ver-schlucken.Sicherheits-Sätze:S-26 Bei Berührung mit Augen gründlich mit Wasser abwaschen und Arzt
konsultieren.S-28.1 Bei Berührung mit der Haut gründlich mit viel Wasser abwaschen.S-46 Bei Verschlucken sofort ärztlichen Rat einholen und Verpackung oder
Etikett vorzeigen.
6.4 Schwefelsäure (H2SO4)Die EIAgen Stopplösung enthält Schwefelsäure. Vorsicht, ätzend. Nicht mit demMund pipettieren.Risiko-Sätze:R-36/38 Reizt die Augen und die Haut.Sicherheits-Sätze:S-26 Bei Berührung mit Augen gründlich mit Wasser abwaschen und Arzt
konsultieren.
6.5 3,3’,5,5’-TetramethylbenzidinDie Substratlösung enthalt 3,3’,5,5’-Tetramethylbenzidin. Nicht mit Haut oderSchleimhaut in Berührung bringen. Bei Kontakt sofort gründlich mit kaltem Wasserabwaschen. Nicht mit dem Mund pipettieren.
6.6 Grenzen des VerfahrensVerwenden Sie kein EDTA als Antikoagulans in einer Konzentration > 5 g/ml. SetzenSie keine Verdünnungen ein, die zu Konzentrationen unterhalb der Nachweisgrenzedieses Assays führen.Da die enzymatische Reaktion temperaturabhängig ist, können Extinktionenentsprechend der Raumtemperatur im Labor unterschiedlich ausfallen. Wie beiallen Immunoassays können die Ergebnisse dieses Tests durch Faktoren beeinflusstwerden, die in einigen Patientenproben vorhanden sind. Die Reagenzien diesesAssays sind ausgelegt, um Interferenzen durch heterophile Antikörper und ausunspezifischer Bindung zu minimieren. Trotzdem können einzelne Proben betroffensein, wie bei anderen Two-Site Immunoassays auch.Zur Erstellung der Diagnose sollte die Bestimmung von AFP immer nur in Verbindungmit anderen Laborwerten und klinischen Informationen verwendet werden.Die Arbeitsanleitung ist genau zu beachten; eine sorgfältige Arbeitstechnik ist fürkorrekte Ergebnisse erforderlich. Eine Änderung der Testdurchführung kann zufalschen Ergebnissen führen.Die Verwendung von anderen Reagenzien, Einwegmaterialien oder Ersatzteilen, alsdie von autorisierten Vertreibern, können zu falschen Ergebnissen führen.Patienten, die zu diagnostischen oder therapeutischen Zwecken monoklonale Maus-Antikörper erhalten haben, können Anti-Maus-Antikörper (HAMA) entwickeln. HAMAkönnen in Immunoassays, die monoklonale Maus-Antikörper verwen-den, sowohlzu falsch hohen als auch zu falsch niedrigen Ergebnissen führen (15, 16).Proben, die HAMA enthalten, sollten nicht in den EIAgen AFP-Assay eingesetztwerden.
6.7 Anzeichen für vorzeitigen Verfall des Substrates1. Die Substratlösung ist farblos oder leicht gelb-blau. Bei einer Kontamination
entwickelt sie eine Blaufärbung; die Lösung sollte dann nicht mehr verwendetwerden.
2. Die Substratlösung ist nicht lichtempfindlich; dennoch kann eine direkteSonneneinstrahlung zu einer Oxidation der Lösung und damit zu einer Blaufärbungführen. In diesem Fall verschwindet die Verfärbung nach einer Lagerung für 4Stunden im Dunkeln; die Lösung ist dann wieder verwendbar.
3. Wenn das Substrat älter wird, kann es leicht gelb-orange werden. Dies hatkeinen Einfluss auf die Testdurchführung.
4. Falls Sie nur einen Teil des Substrates verwenden, transferieren Sie dasbenötigte Volumen in einen sauberen Plastikbehälter, der mit Ethanolausgewaschen und danach mit destilliertem Wasser von hoher Qualitätausgespült wurde, um eine Kontamination zu vermeiden.
7.0 VORBEREITUNG UND LAGERUNG DER PROBEN
7.1 Serum5 ml venöses Blut in Glas- oder Plastikröhrchen ohne Zusätze bei Raumtemperaturzur Gerinnung bringen. Nach der Zentrifugation die Serumfraktion abtrennen.
7.2 Plasma5 ml venöses Blut in Glas- oder Plastikröhrchen mit Heparin oder Citrat alsAntikoagulans zentrifugieren und die Plasmafraktion abtrennen.
7.3 FruchtwasserFruchtwasser in einem sterilen Plastikröhrchen ohne Zusätze sammeln.
7.4 VerdünnungSerum- oder Plasmaproben mit einer zu erwartenden Konzentration >500 IU/mlsollten vor der Testdurchführung mit AFP Diluent verdünnt werden.Fruchtwasser sollte mindestens 1:100 verdünnt werden.
7.5 LagerungSerum- Plasma- und Fruchtwasserproben können bis zu 24 Stunden bei 2...8°Coder bis zu 90 Tage in Aliquots bei -20°C gelagert werden. Nicht wiederholt auftauenund einfrieren.
7.6 Bekannte InterferenzenVermeiden Sie die Verwendung folgender Proben, da sie zu falschen Ergebnissenführen können:Stark hämolysierte, lipämische oder ikterische Proben.Plasmaproben mit einer EDTA-Konzentration (als Antikoagulans) > 5 g/l.
8.0 TESTDURCHFÜHRUNG
8.1 Vorbereitung des Testansatzes1. Alle Reagenzien auf Raumtemperatur bringen und vor Gebrauch vorsichtig
mischen.2. Bereiten Sie für jeden Testansatz wollte Gruppen von Wells vor und platzieren
Sie sie in die Halterung:● 2 Wells für das Chromogen Blank (optional für die QC)● 2 Wells für B0 (Nullkonzentration des Antigens)● 2 Wells für jede Kalibratorkonzentration● 2 Wells für jede Probe oder Kontrolle
3. Für den Photometer-Leerwertabgleich (Chromogen Blank) pipettieren Sie 100µl Substrat und 100 µl Stopplösung in die 2 Wells.
2 / 4
SUBS TMB
SOLN STOP
BUF WASH 10 X

8.2 Pipettier- und Inkubationsschritte1. 0,025 ml der Kalibratoren, Proben und Kontrollen in die entsprechenden Wells
pipettieren.2. 0,1 ml Biotine-AFP Conjugate in alle Wells pipettieren.3. Die Platte vorsichtig durch seitliche Bewegung schütteln oder 10 Sekunden
auf einem Horizontalschüttler.4. 30 Minuten bei 37 °C inkubieren.5. Dekantieren Sie den Inhalt der Wells durch Umdrehen der Platte und 3-4-
maliges festes Aufklopfen auf Absorptionspapier, um die Flüssigkeit undLuftblasen gründlich zu entfernen.
6. Füllen Sie die Wells 3-mal mit verdünntem Waschpuffer. Dekantieren Siejeweils den Inhalt der Wells durch Umdrehen der Platte und 3-4-maliges festesAufklopfen auf Absorptionspapier.
7. 0,1 ml HRP-AFP Conjugate in alle Wells pipettieren.8. Die Platte vorsichtig durch seitliche Bewegung schütteln oder 10 Sekunden
auf einem Horizontalschüttler.9. 30 Minuten bei 37 °C inkubieren.10. Dekantieren Sie den Inhalt der Wells durch Umdrehen der Platte und 3-4-
maliges festes Aufklopfen auf Absorptionspapier, um die Flüssigkeit undLuftblasen gründlich zu entfernen.
11. Füllen Sie die Wells 3-mal mit verdünntem Waschpuffer. Dekantieren Siejeweils den Inhalt der Wells durch Umdrehen der Platte und 3-4-maliges festesAufklopfen auf Absorptionspapier.
12. 0,1 ml Substrate HS in alle Wells pipettieren und vorsichtig schütteln.13. 15 Minuten bei Raumtemperatur inkubieren.14. Pipettieren Sie 0,1 ml Stopplösung in derselben Reihenfolge wie das Substrat
in alle Wells.15. Schütteln Sie die Mikrotiterplatte vorsichtig, um den Inhalt zu mischen. Achten
Sie darauf, dass Sie nichts vom Inhalt verschütten.16. Messen Sie die Extinktion innerhalb einer Stunde nach Zugabe der Stopplösung
auf einem Photometer für Mikrotiterplatten bei 450 nm.
HINWEISE:1. Raumtemperatur ist definiert als 18...25°C.2. Um gültige Ergebnisse zu erhalten, muss für jeden Testansatz eine
Standardkurve erstellt werden.3. Verwenden Sie keine Reagenzien aus verschiedenen Kits oder Lots.4. Pipettieren Sie die Reagenzien in derselben Reihenfolge und im selben
Zeitabstand wie die Kalibratoren und Proben.5. Es wird empfohlen, dass Sie die Zugabe des Substrates und der Stopplösung
zeitlich überwachen, bis Sie mit der Methode vertraut sind. (Wenn Sie z.B. dasSubstrat im Abstand von 3 Sekunden pipettieren, sollten Sie die Stopplösungin derselben Reihenfolgen und im selben Zeitabstand pipettieren.)
6. Die gesamte Pipettierzeit für Kalibratoren und Proben für eine ganze Plattesollte nicht länger als 15 Minuten dauern.
7. Waschen: Für das Waschen wird ein automatischer Mikrotiterplatten-Washerempfohlen. Klopfen Sie nach dem Waschen die umgedrehte Platte aufsaugfähiges Papier auf, um Flüssigkeitsrest zu entfernen. Es sind 3Waschgänge erforderlich.
9.0 STANDARDISIERUNGDie AFP-Kalibratoren sind gegen die 1.IRP 72/225 standardisiert.1,0 IU AFP Calibrator = 1,0 IU 1.IRP 72/225Für eine Umrechnung in ng/ml multiplizieren Sie das Ergebnis in IU/ml mit 1,21.
10.0 QUALITÄTSKONTROLLEJedes Labor sollte routinemäßig bei jedem Testansatz Kontrollmaterial ausverschiedenen Bereichen einsetzen. Die Werte für die Kontrollen und andereKontrollseren sollten innerhalb der ermittelten Vertrauensbereiche liegen. Für dieQualitätskontrolle gelten die entsprechenden nationalen Richtlinien und Gesetze.
11.0 BERECHNUNG DER ERGEBNISSE
11.1 Umrechnung der Optischen DichteOptische Dichten über 2,0 l iegen außerhalb des Messbereichs einigerMikrotiterplatten-Reader. Daher ist es notwendig, für ODs > 2,0 eine Messung bei405 nm (Peak-Schulter) zusätzlich zur Messung bei 450 nm (Peak-Wellenlänge) undbei 620 nm (Referenzfilter für die Subtraktion von Störungen durch das Plastik)durchzühren.Für Mikrotiterplatten-Reader, die nicht bei 3 Wellenlängen gleichzeitig messenkönnen, sollte man folgendermaßen vorgehen:- Messen Sie die Mikrotiterplatte bei 450 nm und 620 nm.- Messen Sie erneut bei 405 nm und 620 nm.- Suchen Sie die Wells mit ODs höher als 2,0 bei 450 nm heraus.- Multiplizieren Sie die ODs dieser Wells, die bei 405 nm gemessen wurden, mit
dem Umrechnungsfaktor 3,0:OD450 nm = OD405 nm X 3.0
Warnhinweis: Der Umrechnungsfaktor 3.0 ist nur ein Vorschlag. Für eine optimaleRichtigkeit sollte der Benutzer seinen eigenen gerätespezifischen Umrechnungsfaktorberechnen.
11.2 DATENAUSWERTUNG – Manuelle MethodeSubtrahieren Sie die OD der Blank von den OD-Mittelwerten der Kalibatoren undProben.Tragen Sie die ODs der Kalibratoren auf y-Achse gegen die Konzentrationen auf dery-Achse auf (logit/log). Die Konzentrationen für die Patientenproben können ausdieser Kurve abgelesen werden.
11.3 DATENAUSWERTUNG – Automatisierte MethodeSubtrahieren Sie die OD der Blank von den ODs der Kalibatoren und Proben.Verwenden Sie (vorzugsweise) die 4-Parameterlogistik oder Kubic-Spline für dieKurvenglättung als Kalkulationsalgorithmus.
11.4 VERDÜNNUNGSollte die AFP-Konzentration höher als der höchste Kalibrator sein, verdünnen Siedie Probe mit dem Diluent oder dem Nullkalibrator, wiederholen Sie die Messung undmultiplizieren Sie das Testergebnis mit dem Verdünnungsfaktor.
11.5 TYPISCHE STANDARDKURVE
Calibrator (IU/ml) Manuelle Methode Labotech MethodeOD 450 nm OD 450 nm
0 0,018 0,0385 0,130 0,137
25 0,445 0,442125 1,408 1,493250 2,050 1,938500 2,662 2,503
12.0 ZU ERWARTENDE WERTEDer Normalbereich für Gesunde (Nichtschwangere) liegt bei < 10 IU/ml AFP.Die angegebenen Werte dienen nur der Orientierung und können von anderenpublizierten Daten abweichen, da die AFP-Messung methodenabhängig ist.Es wird empfohlen, dass jedes Laboratorium seinen eigenen Referenzbereicheermittelt.
12.1 Erhöhte WerteHäufig werden bei Patienten mit hepatozellulären und bestimmten testi-kulären oderovariellen Karzinomen erhöhte AFP-Werte gefunden (6, 7). Auch bei benignenErkrankungen wie Virus-hepatitis (18) und Leber-zirrhose (19) können erhöhte AFP-Werte auftreten. Außerdem werden bei bestimmten fetalen Fehlentwicklungen,insbesondere bei Neuralrohrdefekten, erhöhte Werte im Frucht-wasser (9) und immütterlichen Serum (20) beobachtet. Hohe AFP-Konzentrationen im mütter-lichenSerum treten auch bei anderen fetalen Entwicklungsstörungen wie Omphalocele(21), bei drohendem Abort (22) oder bei Mehrlings-schwangerschaften auf (23).Endogene Faktoren, z.B. humane Anti-Maus-Antikörper, können in Immunoassayszu falsch hohen Werten führen (16).
12.2 Erniedrigte WerteErniedrigte Werte im mütterlichen Serum und im Fruchtwasser werden bei Blasenmoleund bei Down Syndrom gefunden (24).Endogene Faktoren, z.B. humane Anti-Maus-Antikörper, können in Immunoassayszu falsch niedrigen Werten führen (16).
13.0 TESTCHARAKTERISTIKADer EIAgen AFP-Assay ist so ausgelegt, dass der „High-Dose-Hook-Effekt”, derfür immunometrische Assays charakteristisch ist, bis zu einer AFP-Konzentrationvon 350000 IU/ml nicht zu Interferenzen führt.
13.1 Richtigkeit - WiederfindungIn einer Wiederfindungsstudie wurde gereinigtes AFP zu Poolseren hinzugefügt undmit dem AFP-Assay gemessen.
Probe zugefügtes AFP gemessenes AFP Wiederfindung(IU/ml) (IU/ml) %
1 0 5,00 -46,40 45,50 98,1090,30 88,60 98,10
178,10 172,30 96,70353,70 350,80 99,20
2 0 52,70 -46,40 99,60 104,2090,30 137,00 98,80
178,10 225,00 100,20353,70 370,00 93,40
3 0 42,00 -46,40 80,60 94,6090,30 118,30 92,20
178,10 199,20 92,80353,70 359,60 92,80
13.2 Richtigkeit – Linearität von VerdünnungenDrei Serumproben mit hohen AFP-Konzentrationen wurden mit AFP Diluent verdünntund in mehreren Verdünnungsstufen gemessen.
Probe Verd.- AFP AFPFaktor erwartet gemessen Wiederfindung
(IU/ml) (IU/ml) %
- - 191,20 -A 1:2 95,60 91,90 96,1
1:4 47,80 45,70 95,61:8 23,90 24,80 103,8
1:16 11,95 11,40 95,41:32 5,98 6,50 108,8
- - 120,70 -B 1:2 60,35 58,60 97,1
1:4 30,18 29,62 98,21:8 15,09 15,02 99,6
1:16 7,54 7,53 99,81:32 3,77 3,82 101,3
- - 115,00 -C 1:2 57,48 57,52 100,1
1:4 28,74 26,63 92,71:8 14,37 13,70 95,3
1:16 7,18 6,21 86,41:32 3,59 3,16 88,0
3 / 4

13.3 PräzisionDie Interassay-Variation wurde in Serumpools und Kontrollseren durch 20facheBestimmung in einem Testansatz ermittelt.
Manuelle Methode
Probe N. MW ± 1SD %C.V.(IU/ml)
Level 1 20 27,0 ± 1,63 6,0Level 2 20 76,8 ± 4,55 5,9Level 3 20 198,0 ± 15,71 7,9
Die Interassay-Variation wurde in Serumpools und Kontrollseren in mehr als 10Testansätzen ermittelt.
Manuelle Methode
Probe N. MW ± 1SD %C.V.(IU/ml)
Level 1 13 27,0 ± 1,58 5,7Level 2 13 83,8 ± 7,92 9,4Level 3 13 213,5 ± 17,93 8,4
13.4 Untere NachweisgrenzeDie untere Nachweisgrenze dieses Assays ist definiert als der kleinste von Nullunterscheidbare Wert und wurde aus dem Extinktionsmittelwert der 20fachenBestimmung des Nullkalibrators plus 2 Standardabweichungen berechnet. Sie liegtfür diesen Assay bei <0,05 IU/ml, sowohl nach der manuellen als auch nach derautomatisierten Methode (Labotech).
13.5 SpezifitätDie Spezifität dieses Assays wurde durch Zugabe potentiell kreuzreagierenderSubstanzen und anschließende AFP-Messung ermittelt.
Substanz Konzentration scheinbare %Kreuz-AFP Konzentration reaktion
(IU/ml)
hCG 500 µIU/ml (1.IRP 75/537) n.n. -CA 125 15000 U/ml n.n. -CA 19-9 20000 U/ml 1,94 0,01Estriol 500000 ng/ml n.n. -Estradiol 500000 ng/ml n.n. -
n.n.= nicht nachweisbar
13.6 Korrelation mit anderen MethodenDer AFP EIAgen Assay wurde mit einem RIA (AFP Bridge) und einem anderen EIA(SR1 AFP) verglichen. Eine Regressionsanalyse führte zu folgenden Ergebnissen.
y = 1,00x - 1,15r = 0,96x = Referenz RIA (AFP Bridge)y = EIAgen AFPn = 73
y = 0,86x -1,32r = 0,98x = Referenz EIA (SR1 AFP)y = EIAgen AFPn = 76
14.0 AUTOMATISIERUNGTestprotokolle für die Automatisierung auf Mikrotiterplatten-Analysengeräten vonAdaltis (Labotech, PersonalLAB und Nexgen) sind auf Anfrage direkt bei Adaltiserhältlich.
15.0 LITERATUR1. SIZARET, P., ANDERSON, S.G., The International Reference Preparation for
alpha-fetoprotein. J. Biol. Standardization 4:149, 1976.2. ABELEV, G.I., Production of embryonal serum Alpha-globulin by hepatomas.
Review on Experimental and Clinical Data. Cancer Res. 28:1344, 1968.3. MACKIEWICZ, A., BREBOROWICZ,.I, The in-vitro production of Alpha-
fetoprotein variants by human fetal organs. Oncodev. Biol. Med. 1:251, 1980.4. URANO, Y., SAKAI, M., WATANABE, K., TAMAOKI, T., Tandem arrangements
of the Albumin and Alpha-fetoprotein genes in the human genome. Gene 22:225,1984.
5. RUOSLAHTI, E., SEPPALA, M., Studies of carcino-fetal proteins. Physical andChemical properties of human Alpha-fetoprotein. Int. J. Cancer 7:218, 1971.
6. MASOPUST, T., KITHIER, K., RADL, J., KOUTECKY, J., KOTAL, L., Occurrenceof fetoprotein in patients with neoplasma and non-neoplastic diseases. Int. J.Cancer 3:364, 1968.
7. WALDMANN, T.A., MCINTIRE, K. R., The use of a radioimmuno-assay forAlpha-fetoprotein in the diagnosis of malignancy. Cancer 34:1510, 1974.
8. ABELEV, G. I., Alpha-fetoprotein in ontogenesis and its association with malignanttumours. Adv. Cancer Res. 14:295, 1971.
9. BROCK, D. J. H., Mechanism by which amniotic fluid Alpha-fetoprotein may beincreased in fetal abnormalities. Lancet (ii): 345, 1976.
10. GITLIN, G., Normal biology of Alpha-fetoprotein. Ann. N. Y. Acad. Sci. 259:7,1975.
11. RUOSLAHTI, E., HIRAR, H., Alpha-fetoprotein: Physiology and Pathologyduring pregnancy and application to antenatal diagnosis. Scand. J. Immunol.8:3, 1978.
12. MASSEYEFF, R. F., Alpha-fetoprotein: Use in screening. In Immunodiagnosisof Cancer. HERBERMAN, R.B., and MCINTIRE, R. K., (Eds) Marcell DekkerInc. New York pp 117 - 129, 1979.
13. SCARDINO, R. T., COX, H. D., WALDMANN, T. K., McINTIRE, K.P.,MITTEMEYER, B., JAVADPOUR, N. , The value of serum tumour markers in thestaging and prognosis of germ cell tumours of the testis. J. Urol. 118:994, 1977.
14. LANGE, P. H., MCINTIRE, K. R., WALDMANN, T. A., HAKALA, T.R., FRALEY,E.E., Serum Alpha-fetoprotein and human chorionic gonadotrophin in the diagnosisand management of non-seminomatous germ cell testicular cancer. New Engl.J. Med. 295:1237, 1976.
15. KINDERS, R.J., HASS, G.M., Interference in immunoassay by human anti-mouse antibodies. Eur. J. Cancer. 26 (5):647, 1990.
16. BOSCATO, L.M., STUART, M.C., Incidence and specificity of interference intwo-site immunoassays. Clin. Chem. 32 (8): 1491, 1986.
17. HORACEK, K.L., PEPPERELL, R.J., HAY, D.L., BARRIE, J.V., BATTERY,B.W., Detection of feto-maternal hemorrhage by measurement of maternalserum AFP. Lancet (ii) : 200, 1976.
18. KEW, M.C., PURVES, L.R., BERSOHN, I., Serum alpha-fetoprotein levels inacute viral hepatitis. Gut 14:939, 1973.
19. SAKAMOTO, S., YACHI, A., ANZAI, T., WADA, T., Alpha-fetoprotein producingcells in hepatitis and in liver cirrhosis. Ann. N.Y. Acad. Sci. 259:253, 1975.
20. MACRI, J.N., WEISS, R.R., Prenatal serum alpha-fetoprotein screening forneural tube defects. Obstet. Gynecol. 59:633, 1982.
21. PALOMAKI, G.E., HILL, L.E., KNIGHT, G.J., HADDOW, J.E., CARPENTER,M., Second trimester maternal serum alpha-fetoprotein levels in pregnanciesassociated with gastroschisis and omphalocele. Obstet. Gynecol. 71:906, 1988.
22. WALD, N., BARKER, S., CUCKLE, H., BROOK, D.J.H., STIRRAT, S.M., Maternalserum alpha-fetoprotein and spontaneous abortion. Br. J. Obstet. Gynecol.84:357, 1977.
23. REDFORD, D.H., WHITFIELD, C.R., Maternal serum alpha-fetoprotein in twinpregnancies uncomplicated by neural tube defect. Am. J. Obstet. Gynecol.152(5):550, 1985.
24. DAVENPORT, D.M., MACRI, J.N., The clinical significance of low maternalserum alpha-fetoprotein. Am. J. Obstet. Gynecol. 146:657, 1983.
936LI4017K/040705
4 / 4
Vertrieb in Deutschland:Adaltis Deutschland GmbHMerzhauser Str. 13479100 FreiburgTel.: 0761-4581-0Fax: 0761-4581-190e-mail: [email protected]

96 Tests
SOLO PER USO DIAGNOSTICO IN VITRO
Conservare a 2...8°C
SIMBOLI UTILIZZATI SULLE ETICHETTE
∑∑∑∑∑LI4017KREF
it
EIAgen AFP
Adaltis Italia S.p.A.Via Cristoni, 1240033 Casalecchio di Reno - (BO) ItaliaTel. +39-051-6136511 - Fax +39-051-575280www.adaltis.com
Prodotto da:Stabilimento di ProduzioneVia L. Einaudi, 700012 Guidonia Montecelio - (Roma)Italia
1.0 USO DEL PRODOTTOIl kit AFP EIAgen permette la determinazione quantitativa di Alfa-fetoproteina nelsiero umano, nel plasma o nel liquido amniotico.I calibratori sono calibrati secondo la 1st Preparazione di Riferimento Internazionale(IRP) di AFP umana (72/225) approvata dall’Organizzazione Mondiale della Sanità(WHO).
2.0 SPIEGAZIONE DEL TESTL’ alfa-fetoproteina (AFP) è una proteina del siero fetale che circola in tracce anchenegli adulti sani (2). AFP è prodotta principalmente dalla membrana vitellina fetalee dal fegato fetale e in piccola quantità dal tratto gastrointestinale e dai reni fetali(3). È una glicoproteina a singola catena di circa 65-70 kDs. Le proprietà chimico-fisiche e la composizione aminoacidica di AFP sono simili a quelle dell’albuminasierica (4), dalla quale si differenzia dal punto di vista antigenico (5).La determinazione di AFP nel siero è impiegata nella diagnosi e nel monitoraggio deitumori (6, 7, 8) e nello screening prenatale per valutare la presenza di anormalitàfetali quali la spina bifida o la Sindrome di Down (9).AFP dal plasma fetale diffonde nell’urina fetale che viene secreta nel liquidoamniotico da dove diffonde nella circolazione materna. La concentrazione di AFPnel plasma fetale raggiunge un picco (2-3 mg/ml) dalla 12ma alla 14ma settimanaquindi decresce rapidamente (9). I livelli del liquido amniotico si muovono in paralleloa quelli del plasma fetale, anche se inferiori di due ordini di grandezza (µg). Alcontrario, la concentrazione di AFP nel siero materno aumentano geometricamentefino alla 30ma settimana di gestazione e quindi decresce (10).Alla nascita, I livelli di AFP sia nella madre sia nel neonato si portano rapidamentea livelli basali (<10 ng/ml).Circa il 70% dei pazienti con carcinoma epatocellulare mostrano livelli elevati diAFP (7). Livelli di 1,000 - 10,000 ng/ml sono stati registrati (11). In caso di teratomatesticolare si è osservata una relazione diretta tra livelli elevati di AFP e stadio dellamalattia (12). Non si registrano aumenti di AFP in caso di seminoma testicolare(13). L’impiego della misurazione di AFP nel monitoraggio di pazienti affetti dacarcinoma è ben documentata (14). Il non ritorno a livelli normali di AFP testimonial’insuccesso dell’evento operatorio e la presenza di tumore residuo.L’aumento di AFP si osserva anche in condizioni benigne quali infezioni virali acute,epatiti croniche attive e cirrosi. Livelli amniotici elevati si registrano in gravi condizioniquali la morte fetale, l’onfalocele e la sindrome di Turner.
3.0 PRINCIPIO DEL TESTIl kit EIAgen AFP è un dosaggio immunoenzimatico in due passaggi basato sulprincipio sandwich associato al sistema Biotina-Streptavidina.Il saggio utilizza due anticorpi monoclonali anti-AFP ad alta affinità e specificità:uno marcato con Perossidasi estratta dalla radice del rafano (HRP) e l’altro marcatocon Biotina, mentre la micropiastra è sensibilizzata con Streptavidina.I campioni, i calibratori ed i controlli sono dispensati nei pozzetti e quindi incubati conl’anticorpo biotinilato. Durante l’incubazione l’anticorpo lega ai siti specifici le molecoledi AFP, e contemporanemente, la Streptavidina immobilizza l’immunocomplessoformato attraverso il legame del motivo biotinilato presente sull’anticorpo.Dopo I lavaggi per rimuovere gli anticorpi non complessati segue un’incubazionecon l’anticorpo coniugato con HRP.Al termine della seconda incubazione I pozzetti sono lavati e quindi incubati con ilcromogeno/substrato.La reazione colorimetrica si blocca con Stop Solution e la soluzione finale è misuratafotometricamente.L’intensità della colorazione è proporzionale alla quantità di AFP presente nei campioni,entro i limiti di sensibilità del dosaggio. La concentrazione di AFP dei campioni e deicontrolli si determina per interpolazione dalla curva di calibrazione.
4.0 REAGENTI - PREPARAZIONE E CONSERVAZIONEIl kit EIAgen AFP contiene reagenti sufficienti per l’allestimento di 96 pozzetti.Conservare il kit a 2...8°C, stabile fino alla data di scadenza riportata sulla confezione.Se non specificato, dopo prima apertura i reagenti sono stabili fino alla data discadenza riportata sull’etichetta, conservare come indicato ed evitare contaminazioni.
4.1 Streptavidina Micropiastre
Una micropiastra pronta all’uso 12 strips x 8 pozzetti.Ogni pozzetto è sensibilizzato con Streptavidina e può essere utilizzato individualmente.Attendere che la micropiastra sia a temperatura ambiente (18... 25°C) prima dell’uso.Dopo prima apertura I pozzetti inutilizzati sono stabili per 2 mesi a 2...8°C, conservarenella confezione in presenza dell’essiccante.
4.2 AFP Calibratori
6 flaconi (0.5 ml/ciascuno) contenenti AFP a 0- 5- 25- 125- 250- 500 IU/ml (1st IRP72/225) in siero di cavallo con Sodio Azide (0.09% w/w) e Proclina 300 (0.0025% vv)come conservanti. Pronto all’uso. Agitare prima dell’uso.
4.3 AFP Diluente
1 flacone di diluente contenente siero di cavallo con Sodio Azide (0.09% w/w) eProclina 300 (0.0025% v/v) come conservanti. 13 ml. Pronto all’uso. Agitare primadell’uso.
4.4 Biotina-AFP Coniugato
1 flacone contenente anticorpi monoclonali anti-AFP coniugati con Biotina in tamponeTris con albumina sierica bovina (BSA) e Proclina 300 (0.0025% v/v) comeconservanti. 13 ml. Pronto all’uso. Agitare prima dell’uso.
4.5 HRP-AFP Coniugato
1 flacone contenente anticorpi monoclonali anti-AFP marcati con HRP in tamponeTris con albumina sierica bovina (BSA) e Proclina 300 (0.0025% v/v) comeconservante. 13 ml. Pronto all’uso. Agitare prima dell’uso.
1 / 4
MT PLATE
CAL A...F
Limitazioni di temperatura(conservare a 2...8°C)
Attenzione, Leggere le Istruzioni per l’Uso
AFP Calibratore B
AFP Calibratore C
AFP Calibratore D
AFP Calibratore E
AFP Calibratore F
Codice Catalogo
Data di scadenza (Utilizzare entro...)
Numero di tests
Numero di Lotto
AFP Calibratore A
Dispositivo Diagnostico in vitro(Solo per uso diagnostico in vitro)
AFP Diluente
Prodotto da...
8°C
2°C
R E F
LOT
IVD
∑∑∑∑∑
!!!!!
Streptavidina Micropiastre
HRP-AFP Coniugato
Biotina-AFP Coniugato
Substrato HS
Soluzione Bloccante
Soluzione di Lavaggio 10x
Rischio Biologico
Evitare l’esposizione diretta allaluce solare
CONJ BIOT
CONJ HRP
MT PLATE
CONJ BIOT
CONJ HRP
BUF WASH 10 X
SUBS TMB
SOLN STOP
CAL A
CAL B
CAL C
CAL D
CAL E
CAL F
DIL SPE
DIL SPE

2 / 4
4.6 Soluzione di Lavaggio 10x
1 flacone contenente Washing Solution 10x, Tween 20% (0.1%) e Anfotericina-B(2.5 µg/ml) in tampone citrato-borato. 50 ml.Diluire il contenuto del flacone fino a 500 ml con acqua distillata o deionizzata.Miscelare bene. Dopo diluizione conservare a 2...8°C fino a 2 mesi o a temperaturaambiente fino a 5 giorni.
4.7 Substrato HS
1 flacone di Substrate HS contenente 0.26 mg/ml di 3,3’,5,5’ Tetrametilbenzidina(TMB) e 0.01% w/v di Perossido d’Idrogeno (H2O2), in tampone citrato. 13 ml.Pronto all’uso. Agitare prima dell’uso.
4.8 Soluzione Bloccante
1 flacone di Stop Solution contenente Acido Solforico (H2SO4) 0.3 mol/l. 13 ml.Pronto all’uso. Agitare prima dell’uso.
5.0 MATERIALI RICHIESTI E E FORNITI CON IL KIT
5.1 Materiali forniti
Materiale Quantità Codice
Streptavidina Micropiastre Una confezione LSSTREPPBAFP Calibratore A 0.5 ml LS4017SK-AAFP Calibratore B 0.5 ml LS4017SK-BAFP Calibratore C 0.5 ml LS4017SK-CAFP Calibratore D 0.5 ml LS4017SK-DAFP Calibratore E 0.5 ml LS4017SK-EAFP Calibratore F 0.5 ml LS4017SK-FAFP Diluente 13.0 ml LS4017SK0Biotina-AFP Coniugato 13.0 ml LS4017BKHRP-AFP Coniugato 13.0 ml LS4017EKSoluzione di Lavaggio 10X 50.0 ml LSWASHKSubstrato HS 13.0 ml LSTMBH2O2HKSoluzione Bloccante 13.0 ml LSSTOPK
5.2 Materiali necessari non forniti con il kit● Acqua distillata o deionizzata.● Pipette di precisione da: 0.025 ml e 0.1 ml; puntali monouso.● Dispensatore o multicanale da 0.1 ml per la dispensazione di Conjugate,
Substrate and Stop Solution.● Lavatore automatico per micropiastre.● Incubatore per micropiastre.● Lettore per micropiastre capace di leggere contemporaneamente a 450, e 620 nm.● Carta assorbente;● Carta millimetrata.● Sieri di controllo (consigliati).
6.0 AVVERTENZE, PRECAUZIONI E LIMITIQuesto materiale è solo per uso diagnostico in vitro.Il kit è per solo uso professionale, deve quindi essere esclusivamente utilizzatoda personale esperto di laboratorio, in conformità alle norme GLP.
6.1 Norme di sicurezza● Non pipettare a bocca.● Non fumare, mangiare o applicare cosmetici nelle aree dove si maneggiano i
campioni od i reagenti.● Proteggere con protezioni resistenti all’acqua tagli, abrasioni e altri lesioni
cutanee.● Evitare inoculazione, contatto con le mucose o formazione di aerosol.● Utilizzare i guanti durante il maneggiamento dei campioni o di rifiuti liquidi o
solidi.● Evitare contaminazioni microbiche dei calibratori durante le pipettate, utilizzare
puntali monouso.● Seguire le regolamentazioni locali per lo smaltimento dei rifiuti.
6.2 Rischio biologico - PrecauzioniAlcuni reagenti usati nel Kit sono stati preparati con siero o plasma umano. Sia il sieroche il plasma umani sono stati testati con un metodo approvato dalla Food and DrugAdministration (FDA) e sono risultati non reattivi agli anticorpi HIV-1/2, all’ HCV eall’antigene di superficie dell’Epatite B (HBsAg). Poichè nessun metodo offre lacompleta certezza che HIV-1/2, HCV, HBsAg o altri agenti infettanti siano completa-mente assenti, questi reagenti devono essere considerati potenzialmente infetti equindi manipolati come raccomandato nel manuale “Biosafety in Microbiologicaland Biomedical Laboratories,” 4th Edition, 1999.
6.3 Sodio Azide (NaN3) - PrecauzioniLa Sodio Azide è presente nei calibratori ad una concentrazione non superiore a0.09% w/v. La Sodio azide può reagire con tubature di scarico in piombo e rameformando azidi metalliche altamente esplosive. Eseguire lo smaltimento degli scartisolidi o liquidi seguendo le regolamentazioni locali. Concentrazioni di Azide superiorea 0.1% interferiscono con il dosaggio, perciò il dosaggio di siero o di plasmacontenente le sopra citate concentrazioni potrebbero essere sovrastimate.Frasi di rischioR-21/22 Dannoso a contatto con la pelle e se ingeritoFrasi di sicurezzaS-26 In caso di contatto con gli occhi, sciacquare immediatamente con tanta
acqua e consultare un medico.S-28.1 Dopo il contatto con gli occhi, sciacquare immediatamente con tanta acqua.S-46 Se ingerito consultare subito un medico, mostrandogli il contenitore o
l’etichetta.
6.4 Acido Solforico (H2SO4) - PrecauzioniL’Acido Solforico è presente nella Stop Solution a una concentrazione non superiorea 0.3 mol/l. Non pipettare a bocca.Natura dei rischi:R 36/38 Irritante per gli occhi e la pelleConsigli di prudenza:S 26 In caso di contatto con gli occhi, lavare immediatamente e abbondantemen-
te con acqua e consultare un medico.
6.5 3-3’-5-5’ Tetrametilbenzidina (TMB) - PrecauzioniTMB (3-3’-5-5’ Tetrametilbenzidina) è presente in Substrate HS. Evitare il contattocon la pelle e le mucose. In caso di contatto sciacquare abbondantemente conacqua fredda. Non pipettare a bocca.
6.6 LimitazioniNon utilizzare EDTA come anticoagulante ad una concentrazione superiore a 5 g/l.Non utilizzare diluizioni che riducano i valori al di sotto dei limiti di sensibilità deldosaggio.Poiché le reazioni enzimatiche sono sensibili alla temperatura, la temperatura presentenel laboratorio può influenzare i valori di assorbanza.La temperatura presente nel laboratorio può influenzare i valori di assorbanza.Come per tutti i dosaggi immunoenzimatici, i risultati di questo test possono essereinfluenzati da fattori presenti nel siero del paziente. Sebbene la formulazione deireagenti sia stata studiata per minimizzare le interferenze dovute sia alla presenza dianticorpi eterofili che di legami aspecifici, non si può escludere che, come per tutti isistemi “Sandwich” un singolo campione possa esserne inficiato.A scopo diagnostico, i risultati ottenuti da questo dosaggio devono sempre essereutilizzati unitamente all‘esame clinico, all‘anamnesi del paziente e ad altre indagini dilaboratorio.Seguire scrupolosamente le istruzioni per l’uso poiché qualsiasi modifica può produrreun cambiamento nei risultati.L’uso di reagenti, materiale di consumo o parti di ricambio se non forniti dal distributoreautorizzato possono determinare risultati non corretti.Pazienti sottoposti a trattamento con anticorpi monoclonali (Topo) sia a scopo diagnosticoche terapeutico possono aver sviluppato anticorpi anti-topo (HAMA). Nei sistemi cheutilizzano anticorpi monoclonali, la presenza di HAMA nel campione può determinaresia falsi valori positivi (elevati) che negativi (bassi) (15, 16). I campioni provenienti datali pazienti, contenenti HAMA, non devono essere dosati nel sistema EIAgen AFP.
6.7 Indicazioni sul deterioramento del substrato● La soluzione di substrato è incolore o di un colore giallo-blu debole. In caso di
contaminazione accidentale la soluzione inizia a sviluppare il colore e deveessere necessariamente smaltita.
● La soluzione di substrato non è sensibile alla luce. La luce diretta tuttavia puòossidare la soluzione in una soluzione blu. Tale colore scompare dopo circa 4ore di permanenza al buio trascorso questo periodo il substrato può essereancora utilizzato.
● Con il passare del tempo il substrato può diventare giallo-arancione. Talefenomeno non altera le proprietà della soluzione.
● Utilizzare solo la quantità necessaria di substrato. Per evitare contaminazioni,trasferire il volume necessario in un contenitore di plastica precedentementelavato con etanolo e sciacquato con acqua distillata.
7.0 RACCOLTA DEI CAMPIONI E CONSERVAZIONE
7.1 SieroPrelevare 5 ml di sangue venoso in una provetta di vetro senza additivi. Lasciarecoagulare a temperatura ambiente. Centrifugare, separare la frazione di siero econservarlo.
7.2 PlasmaPrelevare 5 ml di sangue venoso in una provetta di vetro o plastica contenenteeparina o citrato come anticoagulanti. Centrifugare, separare la frazione di siero econservarlo.
7.3 Liquido AmnioticoPrelevare campioni di liquido amniotico in provette di plastica sterili senza additivi.
7.4 DiluizioniDiluire i campioni di siero e plasma per i quali si sospettano concentrazioni superioria 500 IU/ml con AFP Diluent prima del dosaggio.Il liquido amniotico deve essere diluito almeno 1:100.
7.5 ConservazioneI campioni di siero, plasma e liquido amniotico sono stabili fino a 24 ore a 2...8°C.Per periodi più lunghi si consiglia di aliquotare e congelare a -20°C fino a 90 giorni.Evitare ripetuti cicli di congelamento e scongelamento.
7.6 Interferenze NoteEvitare l’uso dei seguenti tipi di siero o plasma:Campioni emolizzatiCampioni lipemiciCampioni ittericiSe i campioni di liquido amniotico sono contaminati da sangue, determinare l’originedell’emoglobina. Non utilizzare campioni contaminati da sangue fetale poichécaratterizzato da livelli elevati di AFP.
8.0 PROCEDURA
8.1 Preparazione del saggio1. Lasciare che i reagenti raggiungano la temperatura ambiente e miscelare
delicatamente prima dell’uso.2. Per ogni dosaggio preparare i seguenti gruppi di pozzetti da posizionare sul
supporto:● 2 pozzetti per il cromogeno (bianco; opzionale)● 2 pozzetti per Bo (concentrazione zero dell’antigene);● 2 pozzetti per ogni calibratore;● 2 pozzetti per ogni campione di siero, di plasma e per ogni controllo.
Per il bianco pipettare 0.1 ml di Substrate HS e 0.1 ml di Stop Solution in ognipozzetto.
SUBS TMB
SOLN STOP
BUF WASH 10 X

3 / 4
8.2 Procedura di Esecuzione1. Pipettare 0.025 ml di calibratori, campioni e controlli negli appositi pozzetti.2. Pipettare 0.1 ml di Biotin-AFP conjugate in ogni pozzetto.3. Agitare delicatamente la micropiastra su di un agitatore per 10 secondi.4. Incubare a 37°C per 30 minuti.5. Lavaggio: eliminare la soluzione di incubazione, lavare I pozzetti con Washing
Solution tre volte e asciugare i pozzetti su carta assorbente.6. Pipettare 0.1 ml di HRP-AFP conjugate in ogni pozzetto.7. Agitare delicatamente la micropiastra su di un agitatore per 10 secondi.8. Incubare a 37°C per 30 minuti.9. Lavaggio: eliminare la soluzione di incubazione, lavare I pozzetti con Washing
Solution tre volte e asciugare i pozzetti su carta assorbente.10. Pipettare 0.1 ml di Substrate HS in ogni pozzetto e agitare delicatamente.11. Incubare a temperatura ambiente per 15 minuti.12. Bloccare la reazione con 0.1 ml di Stop Solution per pozzetto, dispensare con
la stessa sequenza e frequenza utilizzata per dispensare Substrate HS.13. Agitare delicatamente, evitare spruzzi.14. Leggere a 450 nm entro 1 ora dall’aggiunta di Stop Solution.
8.3 Note Procedurali1. Per temperatura ambiente si intende la temperatura compresa tra 18°C e
25°C.2. Costruire per ogni dosaggio una curva di calibrazione.3. Non mescolare reagenti di kit o lotti diversi.4. Dispensare i reagenti nello stesso ordine per calibratori e campioni.5. Si consiglia di misurare il tempo durante la dispensazione del cromogeno/
substrato e della stop solution (per esempio se il cromogeno/substrato èdispensato nei pozzetti ad intervalli di 3 secondi l’uno dall’altro anche la stopsolution deve essere dispensata seguendo lo stesso ordine e la stessafrequenza).
6. Si consiglia di non superare i 15 minuti nella dispensazione dei calibratori, deicontrolli e dei campioni per un’intera micropiastra.
7. Lavaggi: si consiglia l’utilizzo di un lavatore automatico per micropiastre. Dopoi lavaggi sbattere la micropiastra su materiale assorbente per rimuovere illiquido residuo. Sono richiesti tre lavaggi.
9.0 CALIBRAZIONEAFP Calibrators sono calibrati secondo la 1st IRP 72/225.1.0 µIU AFP EIAgen Calibrator = 1.0 IU 1st IRP 72/225Per la conversione in ng/ml moltiplicare i risultati di AFP in IU/ml per 1.21.
10.0 CONTROLLO DI QUALITÀSi consiglia ad ogni laboratorio di stabilire i propri intervalli di affidabilità e l’uso dicontrolli multipli in ogni dosaggio.I valori di AFP ottenuti per il materiale del controllo qualità non dovrebbero cadereripetutamente al di fuori dell’intervallo di valori di controllo stabiliti da ogni laboratorio.
11.0 CALCOLO DEI RISULTATI
11.1 Conversione della ODLa densità ottica (OD) del calibratore a 500 IU/ml dovrebbe risultare circa 2.5. Seil lettore è in grado di leggere fino a 2.5, è sufficiente effettuare letture a 450 nm(lunghezza d’onda corrispondente al picco) e a 620 nm (filtro di riferimento persottrarre eventuali interferenze della plastica). Nel caso il lettore non sia in grado dileggere fino a 3.0, è possibile a scelta:1. omettere il calibratore a 500 IU/ml.2. includere il calibratore a 500 IU/ml ed effettuare anche una lettura a 405 nmsottraendo sempre eventuali interferenze della plastica lette a 620 nm. Identificarei pozzetti che, letti a 450 nm, presentano OD superiore a 2.0 sia tra i calibratori siatra i campioni. Selezionare le corrispondenti OD lette a 405 nm e moltiplicarle per unfattore 3 (dove OD 450/OD 405 = 3.0):
OD 450 nm = OD 405 nm * 3.0
Gli strumenti automatici: Labotech, Allertech e Personal Lab leggonocontemporaneamente a 450- 405 e 620 nm e moltiplicano per il fattore 3.0 le OD a405 nm che risultano superiori a 2.0 a 450 nm, se correttamente impostate.
11.2 Elaborazione dei Dati - Metodo ManualeCalcolare le OD medie a 450 nm dei campioni e dei calibratori. Tracciare una curvadi calibrazione facendo corrispondere alla media delle densità ottiche (OD) ottenuteper i calibratori la rispettiva concentrazione di AFP (utilizzare una scala logaritmicao semilogaritmica). Determinare la concentrazione di AFP dei campioni interpolandoi valori di densità ottica (OD) ottenuti a 450 nm sulla curva di calibrazione.
11.3 Elaborazionedei Dati - Metodo AutomaticoUtilizzare i 4 parametri logistici o la funzione monotona curvilinea cubica comealgoritmo di calcolo.
11.4 Campioni con OD superiori rispetto al calibratore a 500 IU/mlDiluire i campioni nei quali si sospetta OD superiore a quella del calibratore piùconcentrato con diluente o con il calibratore zero, quindi dosare nuovamente.Moltiplicare il risultato ottenuto per il fattore di diluizione.
11.5 Tipica Curva di Calibrazione
Calibratore (IU/ml) Metodo Manuale Metodo LabotechOD 450 nm OD 450 nm
0 0.018 0.0385 0.130 0.137
25 0.445 0.442125 1.408 1.493250 2.050 1.938500 2.662 2.503
12.0 VALORI ATTESII livelli normali di AFP in soggetti sani (non in gravidanza) sono <10 IU/ml.I valori riportati sono solo indicativi e possono discostarsi da altri dati pubblicati,poiché a concentrazione di AFP misurata varia in relazione al metodo impiegato perla determinazione.Ogni laboratorio dovrebbe stabilire i propri intervalli di riferimento.
12.1 Fattori Associati a Livelli ElevatiLivelli elevati di AFP si osservano con alta frequenza nel siero di pazienti affetti dacarcinoma epatocellulare o in certi tumori delle cellule germinali dei testicoli o delleovaie (6, 7), ma anche in condizioni non maligne come l’epatite virale (18) e lacirrosi epatica (19).In certe anormalità fetali, in particolare difetti dell’apertura del tubo neurale (NTD),si osservano livelli elevati di AFP nel liquido amniotico (9) e nel siero materno (20).In caso di onfalocele (21), di minaccia di aborto (22) e di gravidanze multiple (23) ilivelli di AFP nel siero materno sono alti.Fattori endogeni come anticorpi umani anti-topo presenti nel siero umano causanofalsi positivi negli immunodosaggi (16).
12.2 Fattori Associati a Livelli BassiLivelli di AFP bassi nel siero materno e nel liquido amniotico si osservano ingravidanza molare e nella sindrome di Down (24).Fattori endogeni come anticorpi umani anti-topo presenti nel siero umano causanofalsi negativi negli immunodosaggi (16).
13.0 EFFICIENZA DEL TESTIl kit EIAgen AFP è stato studiato in modo tale che l’effetto gancio ad alte dosi,caratteristico degli immunodosaggi, non interferisca con la determinazione di AFPfino a 350000 IU/ml.
13.1 Accuratezza - Test di RecuperoIl test di recupero è stato eseguito addizionando AFP purificato ad un pool dicampioni di siero.I campioni addizionati e non addizionati sono stati dosati con il kit EIAgen AFP.Dati di Recupero
Campione AFP Aggiunto AFP Misurato % Recupero(IU/ml) (IU/ml)
1 0 5.00 -46.40 45.50 98.190.30 88.60 98.1
178.10 172.30 96.7353.70 350.80 99.2
2 0 52.70 -46.40 99.60 104.290.30 137.00 98.8
178.10 225.00 100.2353.70 370.00 93.4
3 0 42.00 -46.40 80.60 94.690.30 118.30 92.2
178.10 199.20 92.8353.70 359.60 92.8
13.2 Accuratezza - Test di DiluizioneTre campioni di siero contenenti elevate concentrazioni di AFP sono stati diluiti conAFP Diluent e dosati a diverse diluizioni.Dati di diluizione
Campione Fattore di AFP Atteso AFP %Diluizione (IU/ml) Recuperato Recupero
(IU/ml)
- - 191.20 -A 1:2 95.60 91.90 96.1
1:4 47.80 45.70 95.61:8 23.90 24.80 103.8
1:16 11.95 11.40 95.41:32 5.98 6.50 108.8
- - 120.70 -B 1:2 60.35 58.60 97.1
1:4 30.18 29.62 98.21:8 15.09 15.02 99.6
1:16 7.54 7.53 99.81:32 3.77 3.82 101.3
- - 115.00 -C 1:2 57.48 57.52 100.1
1:4 28.74 26.63 92.71:8 14.37 13.70 95.3
1:16 7.18 6.21 86.41:32 3.59 3.16 88.0
13.3 PrecisioneLa precisione intrasaggio è stata valutata su pools di siero e sieri di controllomisurati 20 volte nella stessa seduta analitica.
Metodo Manuale
Campione N. Media ± 1SD %C.V.(IU/ml)
Livello 1 20 27 ± 1.63 6.0Livello 2 20 76.8 ± 4.55 5.9Livello 3 20 198 ±15.71 7.9

4 / 4
La precisione intersaggio è stato valutato su pools di siero e sieri di controllomisurati in più di 10 sedute analitiche diverse.
Metodo Manuale
Campione N. Media ± 1SD %C.V.(IU/ml)
Livello 1 13 27 ± 1.58 5.7Livello 2 13 83.8 ± 7.92 9.4Livello 3 13 213.5 ±17.93 8.4
13.4 SensibilitàLa sensibilità del dosaggio, definita come la concentrazione di AFP equivalente allamedia dell’assorbanza dello Zero più 2 deviazioni standard basata su 20 replicati delcampione zero, è <0.05 IU/ml impiegando il metodo manuale e automatico (Labotech).
13.5 SpecificitàLa specificità del kit EIAgen AFP è stata valutata misurando la risposta di AFPcausata da alti livelli di sostanze potenzialmente cross-reattive.
Analita Concentrazione Valore %CrossApparente di ReattivitàAFP (IU/ml)
hCG 500 µIU/ml (1st IRP 75/537) N.D. -CA 125 15000 U/ml N.D. -CA 19-9 20000 U/ml 1.94 0.01Estriol 500000 ng/ml N.D. -Estradiol 500000 ng/ml N.D. -
N.D.: Non Determinabile.
13.6 Correlazione con Altri MetodiIl kit EIAgen AFP è stato comparato a un metodo RIA (AFP Bridge) ed a un metodoEIA (SR1 AFP). L’analisi di regressione ha riportato i seguenti risultati:
y = 1.00x - 1.15r = 0.96x = Metodo di riferimento RIA (AFP Bridge)y = EIAgen AFPn = 73
y = 0.86x -1.32r = 0.98x = Metodo di riferimento EIA (SR1 AFP)y = EIAgen AFPn = 76
14.0 AUTOMAZIONEI protocolli di applicazione per una corretta automazione sugli analizzatori Adaltissono disponibili su richiesta diretta alla Adaltis.
15.0 BIBLIOGRAFIA1. SIZARET, P., ANDERSON, S.G., The International Reference Preparation for
alpha-fetoprotein. J. Biol. Standardization 4:149, 1976.2. ABELEV, G.I., Production of embryonal serum Alpha-globulin by hepatomas.
Review on Experimental and Clinical Data. Cancer Res. 28:1344, 1968.3. MACKIEWICZ, A., BREBOROWICZ,.I, The in-vitro production of Alpha-
fetoprotein variants by human fetal organs. Oncodev. Biol. Med. 1:251,1980.
4. URANO, Y., SAKAI, M., WATANABE, K., TAMAOKI, T., Tandem arrangementsof the Albumin and Alpha-fetoprotein genes in the human genome. Gene22:225, 1984.
5. RUOSLAHTI, E., SEPPALA, M., Studies of carcino-fetal proteins. Physicaland Chemical properties of human Alpha-fetoprotein. Int. J. Cancer 7:218,1971.
6. MASOPUST, T., KITHIER, K., RADL, J., KOUTECKY, J., KOTAL, L., Occurrenceof fetoprotein in patients with neoplasma and non-neoplastic diseases. Int. J.Cancer 3:364, 1968.
7. WALDMANN, T.A., MCINTIRE, K. R., The use of a radioimmuno-assay forAlpha-fetoprotein in the diagnosis of malignancy. Cancer 34:1510, 1974.
8. ABELEV, G. I., Alpha-fetoprotein in ontogenesis and its association withmalignant tumours. Adv. Cancer Res. 14:295, 1971.
9. BROCK, D. J. H., Mechanism by which amniotic fluid Alpha-fetoprotein maybe increased in fetal abnormalities. Lancet (ii): 345, 1976.
10. GITLIN, G., Normal biology of Alpha-fetoprotein. Ann. N. Y. Acad. Sci. 259:7,1975.
11. RUOSLAHTI, E., HIRAR, H., Alpha-fetoprotein: Physiology and Pathologyduring pregnancy and application to antenatal diagnosis. Scand. J. Immunol.8:3, 1978.
12. MASSEYEFF, R. F., Alpha-fetoprotein: Use in screening. In Immunodiagnosisof Cancer. HERBERMAN, R.B., and MCINTIRE, R. K., (Eds) Marcell DekkerInc. New York pp 117 - 129, 1979.
13. SCARDINO, R. T., COX, H. D., WALDMANN, T. K., McINTIRE, K.P.,MITTEMEYER, B., JAVADPOUR, N. , The value of serum tumour markers inthe staging and prognosis of germ cell tumours of the testis. J. Urol. 118:994,1977.
14. LANGE, P. H., MCINTIRE, K. R., WALDMANN, T. A., HAKALA, T.R., FRALEY,E.E., Serum Alpha-fetoprotein and human chorionic gonadotrophin in thediagnosis and management of non-seminomatous germ cell testicular cancer.New Engl. J. Med. 295:1237, 1976.
15. KINDERS, R.J., HASS, G.M., Interference in immunoassay by human anti-mouse antibodies. Eur. J. Cancer. 26 (5):647, 1990.
16. BOSCATO, L.M., STUART, M.C., Incidence and specificity of interference intwo-site immunoassays. Clin. Chem. 32 (8): 1491, 1986.
17. HORACEK, K.L., PEPPERELL, R.J., HAY, D.L., BARRIE, J.V., BATTERY,B.W., Detection of feto-maternal hemorrhage by measurement of maternalserum AFP. Lancet (ii) : 200, 1976.
18. KEW, M.C., PURVES, L.R., BERSOHN, I., Serum alpha-fetoprotein levels inacute viral hepatitis. Gut 14:939, 1973.
19. SAKAMOTO, S., YACHI, A., ANZAI, T., WADA, T., Alpha-fetoprotein producingcells in hepatitis and in liver cirrhosis. Ann. N.Y. Acad. Sci. 259:253, 1975.
20. MACRI, J.N., WEISS, R.R., Prenatal serum alpha-fetoprotein screening forneural tube defects. Obstet. Gynecol. 59:633, 1982.
21. PALOMAKI, G.E., HILL, L.E., KNIGHT, G.J., HADDOW, J.E., CARPENTER,M., Second trimester maternal serum alpha-fetoprotein levels in pregnanciesassociated with gastroschisis and omphalocele. Obstet. Gynecol. 71:906,1988.
22. WALD, N., BARKER, S., CUCKLE, H., BROOK, D.J.H., STIRRAT, S.M.,Maternal serum alpha-fetoprotein and spontaneous abortion. Br. J. Obstet.Gynecol. 84:357, 1977.
23. REDFORD, D.H., WHITFIELD, C.R., Maternal serum alpha-fetoprotein intwin pregnancies uncomplicated by neural tube defect. Am. J. Obstet. Gynecol.152(5):550, 1985.
24. DAVENPORT, D.M., MACRI, J.N., The clinical significance of low maternalserum alpha-fetoprotein. Am. J. Obstet. Gynecol. 146:657, 1983.
936LI4017K/040705

1 / 4
Conjugado AFP-Biotina
Conjugado AFP-HRP
96 pruebas
PARA USO DIAGNÓSTICO IN VITRO ÚNICAMENTE
Conservar entre 2...8 °C
SÍMBOLOS UTILIZADOS EN LAS ETIQUETAS
LI4017KREF
es
EIAgen AFP∑∑∑∑∑
Límites de temperatura(conservar entre 2...8°C)
Microplaca Estreptavidina
Atención, consulte lasinstrucciones de uso
Calibrador B AFP
Calibrador C AFP
Calibrador D AFP
Calibrador E AFP
Calibrador F AFP
Código del catálogo
Fecha de caducidad(utilizar antes de...)
Número de pruebas
Número de lote
Calibrador A AFP
Dispositivo médico para diagnóstico invitro (diagnóstico in vitro solamente)
Diluyente AFP
Fabricado por...
Solución de Lavado 10x
8°C
2°C
R E F
LOT
IVD
Sustrato HS
Solución de Parada
∑∑∑∑∑
!!!!!
Riesgo biológico
Adaltis Italia S.p.A.Via Cristoni, 1240033 Casalecchio di Reno - (BO) ItalyTel. +39-051-6136511 - Fax +39-051-575280www.adaltis.com
Fabricado por:Planta de ProducciónVia L. Einaudi, 700012 Guidonia Montecelio - (Rome)Italy
Evite la exposición a la luz solar directa
1.0 USO PREVISTOEl kit AFP EIAgen permite determinar la cantidad de alfa fetoproteína en suero,plasma o líquido amniótico humano.Los estándares se han calibrado en función de OMS 1ª Preparación de referenciainternacional (IRP) para AFP humana (72/225).
2.0 RESUMEN Y EXPLICACIÓN DE LA PRUEBALa alfa fetoproteína (AFP) es una proteína sérica fetal que circula en trazas enadultos sanos (2). La AFP se produce principalmente en el saco vitelino y en elhígado fetal y, en menor medida, en el tubo gastrointestinal fetal y en los riñones (3).Se trata de una glucoproteína de cadena sencilla con un peso molecular aproximadode 65-70 kilodaltones.Sus propiedades fisicoquímicas y su composición de aminoácidos son similares alas de la albúmina sérica (4), con respecto a la cual tiene antígenos distintos (5).El interés clínico de la alfa fetoproteína se encuentra en la oncología, donde la AFPsérica se utiliza para diagnosticar y controlar tumores (6, 7, 8), además del screeningprenatal, en que la AFP del líquido amniótico se utiliza para detectar anomalías comola espina bífida o el síndrome de Down (9).La AFP plasmática fetal se disemina en la orina del feto y se excreta al líquidoamniótico, desde donde pasa a la circulación sanguínea materna. Su concentraciónen el plasma fetal alcanza un nivel máximo (2 a 3 mg/ml) en las semanas 12 o 14 ydespués cae rápidamente (9). Estos niveles en el líquido amniótico se correspondencon la concentración plasmática fetal, aunque son inferiores en dos unidades demagnitud (rango en µg). Por contraste, la concentración de AFP en el suero maternoaumenta geométricamente hasta la trigésima semana de gestación y después decli-na (10). Después del parto, tanto en la madre como en el recién nacido la AFP vuelverápidamente a su nivel basal (<10 ng/ml).Aproximadamente el 70% de los pacientes con carcinoma hepatocelular primariopresenta niveles altos de AFP (7). Se han comunicado valores entre 1.000 y 10.000ng/ml (11). En los casos de teratoma testicular, se ha observado una relación directaentre la incidencia de altos niveles de AFP y las etapas de la enfermedad (12). Noaparece una concentración de AFP incrementada en los seminomas testiculares (13).La medición de alfa fetoproteína aplicada al tratamiento de pacientes con carcinomase encuentra bien documentada (14), y cuando la AFP no retorna a niveles normalesdespués de una intervención quirúrgica, puede sospecharse la presencia de un tumorresidual.Un alto nivel sérico de AFP también se observa en condiciones más benignas, comoinfecciones virales agudas, hepatitis crónica activa o cirrosis. Los niveles altos enlíquido amniótico también aparecen en condiciones graves, por ejemplo, muertefetal, onfalocele o el síndrome de Turner.
3.0 PRINCIPIO DEL PROCEDIMIENTOEl ensayo AFP EIAgen está basado en el principio de sandwich inmunoenzimático dedos fases, junto con la tecnología estreptavidina-biotina.Se emplean dos anti-AFP monoclonales de alta afinidad y especificidad: uno de losanticuerpos está marcado con peroxidasa de rábano (HRP) y el otro con biotina,mientras que los tubos de la microplaca se han sensibilizado con estreptavidina.En los tubos se dispensan muestras, calibradores y controles, seguidos del conjugadoanti-AFP biotina.Durante la incubación, los dos anticuerpos monoclonales se unen a la molécula deAFP en dos sitios diferentes y específicos; al mismo tiempo, la estreptavidinainmoviliza en las paredes de los tubos el sandwich inmunológico que se está forman-do gracias a su afinidad por la biotina del anticuerpo biotinilado.Después de lavar para eliminar las muestras que no han sufrido reacción, se añadeel segundo conjugado monoclonal a HRP.Tras la segunda incubación, los tubos se lavan para eliminar los anticuerpos marcadosno unidos y se añade la mezcla de sustrato cromogénico.A continuación, la reacción se bloquea añadiendo la solución de interrupción y el colordesarrollado se mide fotométricamente. La intensidad del color desarrollado esdirectamente proporcional en el rango de trabajo del ensayo a la concentración deAFP en la muestra. La concentración de AFP en la muestra o control de un pacientese determina por interpolación en la curva de calibración.
4.0 REACTIVOS: CONSERVACIÓN Y MANIPULACIÓNEl kit EIAgen AFP contiene reactivos para 96 tubos. Conserve el kit a una tempera-tura de 2...8°C para que se mantenga estable hasta la fecha de caducidad indicadaen la etiqueta.Si no se especifica otra cosa, después de abrirlos por primera vez, todos los reactivospermanecen estables hasta la fecha de caducidad impresa en las etiquetas, siempreque se conserven según las indicaciones y no se produzca contaminación al utilizarla pipeta.
4.1 Microplaca Estreptavidina
La bolsa contiene una microplaca de 12 tiras x 8 tubos.Cada tubo se ha sensibilizado con estreptavidina y debe utilizarse individualmente.Espere hasta que la microplaca alcance la temperatura ambiente (de 18...25°C) antesde usarla. Una vez abiertas, las tiras que no se utilizan permanecen estables durante2 meses a una temperatura de 2...8°C si se guardan en la bolsa de plástico con eldesecante.
4.2 Calibradores AFP
6 frascos de calibradores AFP que contienen 0- 5- 25- 125- 250- 500 IU/ml (1ª IRP 72/225) en suero equino con azida sódica (0,09% p/p) y Proclin 300 (0,0025% v/v) comoconservantes. 0,5 ml para cada calibrador. Listo para el uso. Mezcle ligeramenteantes del uso.
4.3 Diluyente AFP
1 frasco de diluyente AFP que contiene suero equino y azida sódica (0,09% p/p) yProclin 300 (0,0025% v/v) como conservantes. 13 ml. Listo para el uso. Mezcleligeramente antes del uso.
MT PLATE
CAL A...F
MT PLATE
CONJ BIOT
CONJ HRP
DIL SPE
SUBS TMB
SOLN STOP
CAL A
CAL B
CAL C
CAL D
CAL E
CAL F
DIL SPE
BUF WASH 10 X

4.4 Conjugado AFP-Biotina
1 frasco que contiene un anticuerpo monoclonal unido a AFP marcada con biotina entampón Tris con albúmina sérica bovina (BSA) y Proclin 300 (0,0025% v/v) comoconservantes. 13 ml. Listo para el uso. Mezcle ligeramente antes del uso.
4.5 Conjugado AFP-HRP
1 frasco que contiene un anticuerpo monoclonal unido a AFP marcada con peroxidasade rábano en tampón Tris con albúmina sérica bovina (BSA) y Proclin 300 (0,0025%v/v) como conservantes. 13 ml. Listo para el uso. Mezcle ligeramente antes del uso.
4.6 Solución de Lavado 10x
Un frasco de solución de lavado 10x que contiene Tween 20 (0,1%) y anfotericina-B(2,5 µg/ml) en tampón de citrato-borato. 50 ml.Diluya el contenido del frasco en 450 ml de agua destilada o desionizada y mezclebien. Tras la dilución, consérvelo a 2...8°C durante 2 meses o a temperatura ambien-te durante 5 días.
4.7 Sustrato HS
Un frasco de sustrato HS que contiene 0,26 mg/ml de 3,3’,5,5’ tetrametilbenzidina(TMB) y 0,01% p/v de peróxido de hidrógeno (H2O2) en tampón de citrato. 13 ml.Listo para el uso. Mezcle ligeramente antes del uso.
4.8 Solución de Parada
Un frasco de solución de parada que contiene 0,3 mol/l de ácido sulfúrico (H2SO4).13 ml.Listo para el uso. Mezcle ligeramente antes del uso.
5.0 MATERIALES Y EQUIPO NECESARIOS
5.1 Materiales Suministrados
Material Cantidad Código
Microplaca Estreptavidina Una bolsa LSSTREPPBCalibrador A AFP 0,5 ml LS4017SK-ACalibrador B AFP 0,5 ml LS4017SK-BCalibrador C AFP 0,5 ml LS4017SK-CCalibrador D AFP 0,5 ml LS4017SK-DCalibrador E AFP 0,5 ml LS4017SK-ECalibrador F AFP 0,5 ml LS4017SK-FDiluyente AFP 13,0 ml LS4017SK0Conjugado AFP-Biotina 13,0 ml LS4017BKConjugado AFP-HRP 13,0 ml LS4017EKSolución de Lavado 10X 50,0 ml LSWASHKSustrato HS 13,0 ml LSTMBH2O2HKSolución de Parada 13,0 ml LSSTOPK
5.2 Materiales y Equipo Necesarios no Suministrados● Agua destilada o desionizada.● Pipeta de precisión de 0,025, 0,1 ml con puntas desechables.● Dispensador repetitivo de 0,1 ml o pipetas de desplazamiento positivo para
añadir conjugado, sustrato y solución de interrupción.● Sistema de lavado automático de placa.● Incubador de placa de microtitulación.● Lector de placa de microtitulación equipado para medir la absorbancia a 450 nm
(filtro de referencia a 620 nm).● Almohadilla o papel absorbente.● Suero de control (recomendado).
6.0 ADVERTENCIAS, RECAUCIONES Y LIMITACIONESPara uso diagnóstico in vitro.Sólo el personal de laboratorio experimentado debe utilizar esta prueba y lamanipulación debe hacerse de acuerdo con GLP.
6.1 Medidas de seguridad● No utilice la pipeta con la boca.● No fume, coma ni se maquille en zonas en las que se manipulen muestras de
pacientes o reactivos del kit.● Los cortes, arañazos y cualquier otra lesión de la piel deben estar correctamente
protegidos con indumentaria impermeable.● Tenga cuidado para no autoinocularse y evite cualquier salpicadura de las
membranas mucosas o que se generen vapores.● Deben utilizarse guantes de laboratorio cuando se manipulen muestras de
pacientes y se eliminenresiduos tanto sólidos como líquidos.
● Evite la contaminación microbiana de estándares al utilizar la pipeta; para ello,emplee puntas desechables.
● La eliminación de todos los residuos ha de realizarse conforme a la normativalocal.
6.2 Advertencia sobre riesgos biológicos potencialesAlgunos reactivos utilizados pueden haberse preparado a partir de bancos de suerohumano. Cada unidad de sangre en estos bancos se analizó y encontró no reactivapara sífilis, además de analizarse la presencia del antígeno de superficie (HBsAG) dela hepatitis B y la presencia de anticuerpos del virus de inmunodeficiencia humana(VIH 1 y 2) con un método aprobado por la FDA. Dado que no existe ninguna pruebaque garantice la total ausencia de VIH, del virus de la hepatitis B u otros agentesinfecciosos, es preciso considerar que estos reactivos tienen un posible riesgobiológico y durante su manipulación se deben adoptar las mismas precauciones quecon cualquier muestra de suero o plasma. Algunos reactivos, como los de calibración,estándares o control, pueden contener materiales cuyo origen proceda de tejidoshumanos. Hasta el momento, no existe un método estándar para analizar la presenciade VIH en dichos materiales. Por ello, es recomendable que estos reactivos tambiénsean considerados de posible riesgo biológico.
Se exige seguir una práctica de laboratorio adecuada para manipular tales materiales,según lo descrito en el documento del Centro de Control de Enfermedades (Centerfor Diseases Control, CDC) de Atlanta: Universal precautions for prevention oftransmission of human immunodeficiency virus, hepatitis B virus, and other bloodbourne pathogens in healthcare setting “MMWR” 37:377-387, 1999.
6.3 Advertencia sobre la azida sódica (NaN3)La azida sódica es un conservante presente en la matriz estándar en una concentraciónnunca superior al 0,09% p/p. La azida sódica puede dar lugar a la formación de azidasexplosivas de cobre o plomo en las tuberías. Los residuos líquidos y sólidos se debeneliminar de una manera segura cumpliendo las normas locales. Azida en unaconcentración superior al 0,1% p/p interfiere en este ensayo; por lo tanto, el análisisde sueros o muestras de control que contienen el compuesto anterior puede arrojarresultados sobrestimados.Frases de advertencia de riesgoR 21/22 Nocivo en contacto con la piel y por ingestión.Frases de advertencia de seguridadS-26 En caso de contacto con los ojos, lávense inmediata y abundantemente con
agua y acúdase a un médico.S 28.1 En caso de contacto con la piel, lávese inmediata y abundantemente con
agua.S-46 En caso de ingestión, acuda inmediatamente al médico y muéstrele la
etiqueta o el envase.
6.4 Advertencia sobre el ácido sulfúrico (H2SO4)El ácido sulfúrico está presente en la solución de interrupción en una concentraciónno superior a 0,3 mol/l. No utilice la pipeta con la boca.Frases de advertencia de riesgoR 36/38 Irritante para los ojos y la piel.Frases de advertencia de seguridadS-26 En caso de contacto con los ojos, lávese de inmediato con agua abundante
y acuda a un médico.
6.5 Advertencia sobre 3-3’-5-5’ tetrametilbenzidina (TMB)TMB (3-3’-5-5’ tetrametilbenzidina) está presente en el sustrato HS. Impida que estereactivo entre en contacto con la piel y las membranas mucosas. En caso de queesto suceda, lávese completamente con agua corriente fría. No utilice la pipeta conla boca.
6.6 LimitacionesNo utilice EDTA como anticoagulante en una concentración superior a 5 g/l. Lasdiluciones con valores inferiores al límite de detección del ensayo no deben utilizarse.Puesto que la reacción enzimática depende de la temperatura, se pueden obtenerdiferentes absorbancias según la temperatura del laboratorio.Como ocurre en todos los inmunoensayos, los factores presentes en algunas de lasmuestras extraídas al paciente pueden alterar los resultados del ensayo. La formulaciónde los reactivos de este ensayo tiene por objeto minimizar la interferencia de anticuerposheterofílicos y de la unión de proteínas no específicas. A pesar de esto, los resultadosde muestras separadas pueden presentar variaciones, como sucede con otras técnicasde inmunoensayo de 2 localizaciones.Para fines de diagnóstico, los resultados del ensayo tendrán que complementarsecon análisis clínicos, el historial médico del paciente y otros datos recopilados.Es preciso seguir exactamente las instrucciones, ya que cualquier variación podríaalterar los resultados.El uso de reactivos, productos desechables y piezas de repuesto distintos a lossuministrados por el proveedor autorizado puede producir resultados incorrectos.Los pacientes que han recibido anticuerpos monoclonales procedentes del ratón parafines de diagnóstico o tratamiento pueden desarrollar anticuerpos humanos anti-ratón(HAMA). Estos anticuerpos pueden generar resultados falsamente altos o bajos eninmunoensayos en los que se utilizan anticuerpos monoclonales del ratón (15-16). Porconsiguiente, las muestras que contienen HAMA no deben utilizarse con el ensayoEIAgen AFP.
6.7 Factores de deterioro del sustrato● La solución única de sustrato es incolora o ligeramente amarilloazulada. Si se
produce contaminación accidental, la solución comienza a adquirir un color azuly, en este caso, será preciso desecharla.
● La solución única de sustrato no es sensible a la luz. Sin embargo, la luz solardirecta puede oxidar la solución y tornarla de color azul. Este color desaparecetranscurridas 4 horas de almacenamiento en la oscuridad, después de lascuales podrá volver a utilizarse la solución.
● Con el paso del tiempo, el sustrato puede adquirir un ligero coloramarilloanaranjado. Esto no afecta a su rendimiento.
● Si sólo va a utilizarse parte del frasco de sustrato, para que no se produzcacontaminación, traslade el volumen necesario a un envase de plástico limpiopreviamente lavado con etanol y enjuagado con agua destilada de calidadsuperior.
7.0 OBTENCIÓN Y CONSERVACIÓN DE LAS MUESTRAS
7.1 SueroExtraiga 5 ml de sangre venosa y guarde la muestra en un tubo de vidrio sin aditivos.Deje que coagule a temperatura ambiente. Centrifugue, separe la fracción sérica yguarde la muestra.
7.2 Plasma Extraiga 5 ml de sangre venosa y guarde la muestra en tubo de vidrio o plástico quecontenga heparina o citrato como anticoagulante. Centrifugue, separe la fracciónsérica y guarde la muestra.
7.3 Líquido AmnióticoExtraiga muestras de líquido amniótico y guárdelas en tubos de plástico estéril sinaditivos.
7.4 DiluciónLas muestras de suero y plasma cuya concentración se prevé que supere los 500IU/ml deben diluirse con diluyente AFP antes del ensayo.El líquido amniótico debe diluirse, como mínimo, a 1:100.
CONJ BIOT
CONJ HRP
SUBS TMB
SOLN STOP
2 / 4
BUF WASH 10 X

7.5 ConservaciónLas muestras de suero, plasma y líquido amniótico permanecen estables durante 24horas a una temperatura de 2...8°C. El tiempo máximo de conservación una vezfraccionada la muestra es de 90 días a -20°C.No aplique ciclos de congelación y descongelación repetidos.
7.6 InterferenciasEvite utilizar los siguientes tipos de muestras de suero o plasma, ya que podríaobtener resultados incorrectos:Muestras muy hemolizadasMuestras altamente lipémicasMuestras altamente ictéricasNo deben utilizarse las muestras de plasma anticoagulado EDTA con una concentraciónde EDTA superior a 5 g/l.Si muestras de líquido amniótico se contaminan con sangre, será preciso determinarel origen de la hemoglobina. Debido a los altos niveles de circulación de AFP en elplasma fetal, no deben utilizarse las muestras contaminadas con sangre fetal.
8.0 PROCEDIMIENTO DE ENSAYO
8.1 Preparativos Para el Ensayo1. Espere hasta que los reactivos se encuentren a la temperatura ambiente y
mézclelos suavemente antes de usarlos.2. Antes de cada ensayo, prepare los siguientes grupos de tubos y colóquelos en
el soporte:● 2 tubos para ensayo en blanco cromogénico (opcional para QC);● 2 tubos B0 (concentración de antígenos nula);● 2 tubos para cada concentración de calibrador;● 2 tubos para cada muestra de suero, plasma o control.Para el ensayo en blanco cromogénico, vierta con la pipeta 0,1 ml de sustratoHS y 0,1 ml de solución de interrupción en los dos tubos.
8.2 Uso de la Pipeta e Incubación1. Añada con la pipeta 0,025 ml de calibradores, muestras y controles en los tubos
correspondientes de la tira.2. Vierta con la pipeta 0,1 ml de conjugado AFP-biotina en cada tubo.3. Agite suavemente toda la placa con un movimiento de lado a lado o utilizando un
agitador orbital durante 10 segundos.4. Incube durante 30 minutos a 37°C.5. Lavado: deseche la solución de incubación, enjuague los tubos con la solución
de lavado tres veces y elimine todo líquido residual.6. Vierta con la pipeta 0,1 ml de conjugado AFP-HRP en cada tubo.7. Agite suavemente toda la placa con un movimiento de lado a lado o utilizando un
agitador orbital durante 10 segundos.8. Incube durante 30 minutos a 37°C.9. Lavado: deseche la solución de incubación, enjuague los tubos con la solución
de lavado tres veces y elimine todo líquido residual.10. Utilice la pipeta para añadir 0,1 ml de sustrato HS en cada tubo y agite
suavemente.11. Incube a temperatura ambiente durante 15 minutos.12. Detenga la reacción añadiendo 0,1 ml de solución de interrupción a cada tubo en
la secuencia y con la misma frecuencia utilizadas para agregar con la pipeta elsustrato HS.
13. Agite suavemente la microplaca con cuidado de no salpicar.14. Consulte la lectura a 450 nm en el transcurso de 1 hora desde la dispensación
de la solución de interrupción.
8.3 Notas Sobre el Procedimiento1. Por temperatura ambiente se entiende el rango de temperaturas comprendido
entre 18...25°C.2. Para garantizar la obtención de resultados válidos es preciso dibujar una curva
estándar en cada ensayo.3. No se pueden mezclar reactivos de kits y lotes diferentes.4. Los reactivos deben añadirse en el mismo orden que los calibradores y las
muestras.5. Se recomienda cronometrar la agregación de la solución de sustrato cromogénico
y de la solución de interrupción hasta que se familiarice con el método (es decir,si la solución de sustrato cromogénico se dispensa en los tubos cada 3 segundos,la solución de interrupción también ha de dispensarse en el mismo orden y conla misma frecuencia.
6. El tiempo total de dispensación de los calibradores, controles y muestras porplaca no debe superar los 15 minutos.
7. Procedimiento de lavado: para el procedimiento de lavado, se recomiendaemplear un equipo de lavado automático de placa. Después del lavado, golpeeligeramente la placa invertida sobre papel absorbente para eliminar todo residuode los tubos. Es preciso realizar tres lavados.
9.0 CALIBRACIÓNLos calibradores AFP se calibran en función de la 1ª IRP 72/225.Calibrador AFP EIAgen 1,0 IU = 1ª IRP 72/225 1,0 IUPara convertir a ng/ml, multiplique los resultados de AFP en IU/ml por 1,21.
10.0 CONTROL DE CALIDADEs aconsejable que cada laboratorio utilice periódicamente materiales de control decalidad y establezca un rango de control propio. Los controles en diferentes nivelesdeben aplicarse siempre.Los valores de AFP obtenidos para el material de control de calidad no pueden quedarrepetidamente fuera del rango de control establecido por cada laboratorio.
11.0 CÁLCULO DE RESULTADOS
11.1 Conversión de densidad óptica (DO)La densidad óptica (DO) de los calibradores a 500 IU/ml puede ser de 2,5aproximadamente. Si el lector puede detectar DOs hasta 2,5, la lectura a 450 nm(longitud de onda del pico) y a 620 nm (filtro de referencia para la sustracción deinterferencia del plástico) es suficiente. Si el lector no es capaz de leer hasta 2,5, elusuario tiene dos opciones:
1. suprimir la aplicación del calibrador a 500 IU/ml.2. aplicar el calibrador a 500 IU/ml y, a continuación, leer además de a 450 nm,
también a 405 nm (en el límite del pico) y a 620 nm siempre respecto al filtro desustracción. Identifique los tubos con DO superior a 2,0 a 450 nm tanto paracalibradores como para muestras, registre la DO correspondiente a 405 nm ymultiplique estas DOs por el factor de conversión 3,0, ya que:DO 450 nm = DO 405 nm x 3,0 (para este sustrato)
Instrumentos automáticos: Labotech, Allertech y Personal lab pueden leer de formaautomática y simultánea a 450-405 y a 620 nm, y multiplicar por 3,0 las DOs a 405nm que sean superiores a 2,0 a 450 nm, si se selecciona esta opción.
11.2 Método Manual de Reducción de DatosCalcule, como se ha descrito previamente, la DO media a 450 nm de calibradores ymuestras. Represente las DOs medias de calibradores frente a la respectivaconcentración de AFP en papel gráfico logit/log o semilog y determine la concentraciónde AFP en la muestra por interpolación a partir de una curva de calibración. Losresultados también se pueden calcular con programas normales de tratamiento dedatos automáticos, como por ejemplo, 4 Parameters, Spline.
11.3 Método Automatizado de Reducción de DatosUtilice la logística de 4 Parameters (preferentemente), o la función spline cúbica desuavizado como algoritmo de cálculo.
11.4 Muestras con DOs Superiores al Calibrador a 500 IU/mlSi el valor de AFP supera el valor de calibrador máximo, diluya la muestra con eldiluyente o el calibrador cero y vuelva a aplicar el ensayo; a continuación, multipliqueel resultado obtenido por el factor de dilución de la muestra.
11.5 Curva de Calibración Típica
Calibrador (IU/ml) Método Manual Método LabotechDO 450 nm DO 450 nm
0 0,018 0,0385 0,130 0,137
25 0,445 0,442125 1,408 1,493250 2,050 1,938500 2,662 2,503
12.0 VALORES PREVISTOSEl rango de normalidad de AFP en personas sanas (no embarazadas) es de <10 IU/ml.Los valores proporcionados son orientativos y pueden diferir de otros datos publicadosdebido a que las concentraciones de AFP medidas varían en función del métodoempleado.Es aconsejable que cada laboratorio defina un rango de referencia propio.
12.1 Factores Asociados con Valores ElevadosMuy frecuentemente se han observado niveles de AFP elevados en el suero depacientes con carcinoma hepatocelular y determinados tumores de células germinalesde testículos y ovarios (6, 7).Los altos niveles de AFP también se han detectado en estados no malignos, como lahepatitis vírica (18) y la cirrosis hepática (19).En determinadas anomalías del feto, especialmente en los defectos del tubo neural(NTD), los niveles de AFP altos se observan tanto en el líquido amniótico (9) comoen el suero materno (20). La alta concentración de AFP en el suero materno tambiénaparece en otras situaciones de sufrimiento fetal, como el onfalocele (21) o laamenaza de aborto (22), y en los embarazos múltiples (23). Se ha detectado que algunos factores endógenos, como los anticuerpos humanosanti-ratón en suero humano, generan valores falsamente elevados de antígenos enlos inmunoensayos (16).
12.2 Factores Asociados con Valores ReducidosSe han observado valores reducidos de AFP en suero materno y líquido amnióticodurante el embarazo por mola y en el síndrome de Down (24).Se ha detectado que algunos factores endógenos, como los anticuerpos humanosanti-ratón en suero humano, generan valores falsamente bajos de antígenos en losinmunoensayos (16).
13.0 CARACTERÍSTICAS DEL ENSAYOEl kit EIAgen AFP ha sido diseñado de manera que el efecto de “gancho”, característicode los ensayos inmunométricos, no interfiera con los valores de AFP de hasta350000 IU/ml.
13.1 Precisión de la Prueba de RecuperaciónEn los experimentos de recuperación realizados se añadió AFP purificada a un bancode muestras de suero.Las muestras puras y añadidas se midieron en el ensayo EIAgen AFP.Datos de Recuperación
Muestra AFP Añadida AFP Medida % de Recuperación(IU/ml) (IU/ml)
1 0 5,00 -46,40 45,50 98,1090,30 88,60 98,10
178,10 172,30 96,70353,70 350,80 99,20
2 0 52,70 -46,40 99,60 104,2090,30 137,00 98,80
178,10 225,00 100,20353,70 370,00 93,40
3 0 42,00 -46,40 80,60 94,6090,30 118,30 92,20
178,10 199,20 92,80353,70 359,60 92,80
3 / 4
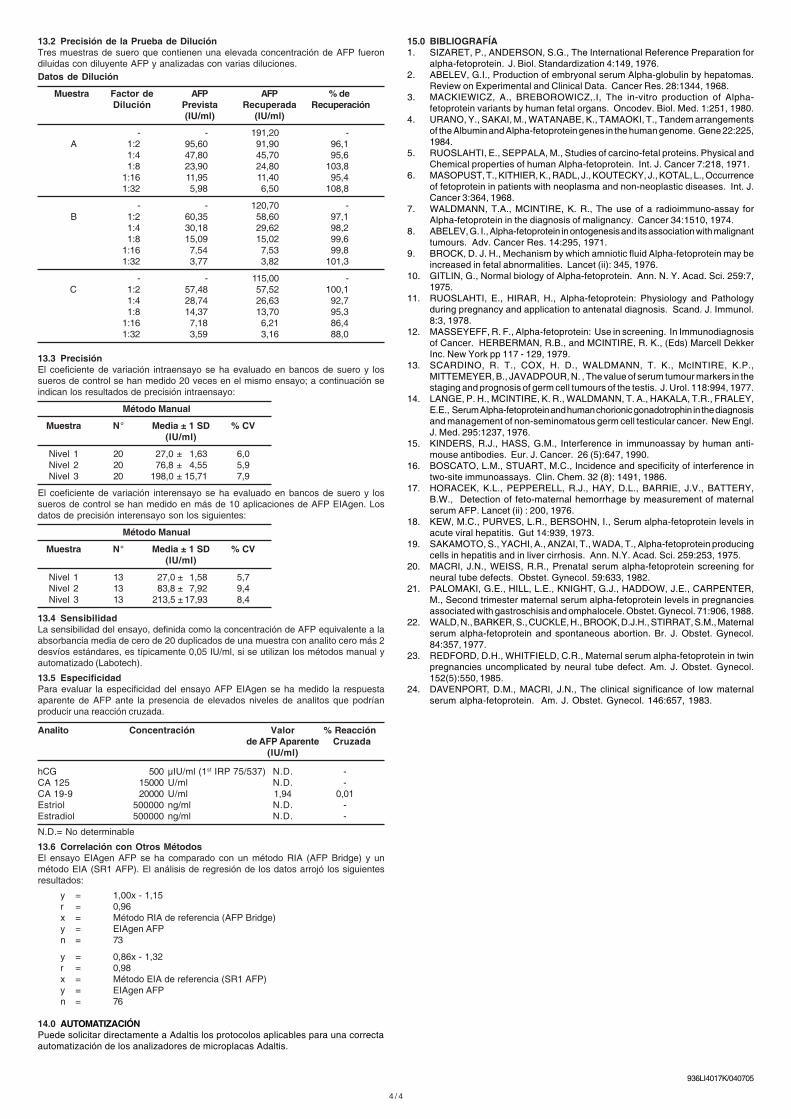
13.2 Precisión de la Prueba de DiluciónTres muestras de suero que contienen una elevada concentración de AFP fuerondiluidas con diluyente AFP y analizadas con varias diluciones.Datos de Dilución
Muestra Factor de AFP AFP % deDilución Prevista Recuperada Recuperación
(IU/ml) (IU/ml)
- - 191,20 -A 1:2 95,60 91,90 96,1
1:4 47,80 45,70 95,61:8 23,90 24,80 103,8
1:16 11,95 11,40 95,41:32 5,98 6,50 108,8
- - 120,70 -B 1:2 60,35 58,60 97,1
1:4 30,18 29,62 98,21:8 15,09 15,02 99,6
1:16 7,54 7,53 99,81:32 3,77 3,82 101,3
- - 115,00 -C 1:2 57,48 57,52 100,1
1:4 28,74 26,63 92,71:8 14,37 13,70 95,3
1:16 7,18 6,21 86,41:32 3,59 3,16 88,0
13.3 PrecisiónEl coeficiente de variación intraensayo se ha evaluado en bancos de suero y lossueros de control se han medido 20 veces en el mismo ensayo; a continuación seindican los resultados de precisión intraensayo:
Método Manual
Muestra N° Media ± 1 SD % CV(IU/ml)
Nivel 1 20 27,0 ± 1,63 6,0Nivel 2 20 76,8 ± 4,55 5,9Nivel 3 20 198,0 ± 15,71 7,9
El coeficiente de variación interensayo se ha evaluado en bancos de suero y lossueros de control se han medido en más de 10 aplicaciones de AFP EIAgen. Losdatos de precisión interensayo son los siguientes:
Método Manual
Muestra N° Media ± 1 SD % CV(IU/ml)
Nivel 1 13 27,0 ± 1,58 5,7Nivel 2 13 83,8 ± 7,92 9,4Nivel 3 13 213,5 ± 17,93 8,4
13.4 SensibilidadLa sensibilidad del ensayo, definida como la concentración de AFP equivalente a laabsorbancia media de cero de 20 duplicados de una muestra con analito cero más 2desvíos estándares, es típicamente 0,05 IU/ml, si se utilizan los métodos manual yautomatizado (Labotech).
13.5 EspecificidadPara evaluar la especificidad del ensayo AFP EIAgen se ha medido la respuestaaparente de AFP ante la presencia de elevados niveles de analitos que podríanproducir una reacción cruzada.
Analito Concentración Valor % Reacciónde AFP Aparente Cruzada
(IU/ml)
hCG 500 µIU/ml (1st IRP 75/537) N.D. -CA 125 15000 U/ml N.D. -CA 19-9 20000 U/ml 1,94 0,01Estriol 500000 ng/ml N.D. -Estradiol 500000 ng/ml N.D. -
N.D.= No determinable
13.6 Correlación con Otros MétodosEl ensayo EIAgen AFP se ha comparado con un método RIA (AFP Bridge) y unmétodo EIA (SR1 AFP). El análisis de regresión de los datos arrojó los siguientesresultados:
y = 1,00x - 1,15r = 0,96x = Método RIA de referencia (AFP Bridge)y = EIAgen AFPn = 73
y = 0,86x - 1,32r = 0,98x = Método EIA de referencia (SR1 AFP)y = EIAgen AFPn = 76
14.0 AUTOMATIZACIÓNPuede solicitar directamente a Adaltis los protocolos aplicables para una correctaautomatización de los analizadores de microplacas Adaltis.
4 / 4
15.0 BIBLIOGRAFÍA1. SIZARET, P., ANDERSON, S.G., The International Reference Preparation for
alpha-fetoprotein. J. Biol. Standardization 4:149, 1976.2. ABELEV, G.I., Production of embryonal serum Alpha-globulin by hepatomas.
Review on Experimental and Clinical Data. Cancer Res. 28:1344, 1968.3. MACKIEWICZ, A., BREBOROWICZ,.I, The in-vitro production of Alpha-
fetoprotein variants by human fetal organs. Oncodev. Biol. Med. 1:251, 1980.4. URANO, Y., SAKAI, M., WATANABE, K., TAMAOKI, T., Tandem arrangements
of the Albumin and Alpha-fetoprotein genes in the human genome. Gene 22:225,1984.
5. RUOSLAHTI, E., SEPPALA, M., Studies of carcino-fetal proteins. Physical andChemical properties of human Alpha-fetoprotein. Int. J. Cancer 7:218, 1971.
6. MASOPUST, T., KITHIER, K., RADL, J., KOUTECKY, J., KOTAL, L., Occurrenceof fetoprotein in patients with neoplasma and non-neoplastic diseases. Int. J.Cancer 3:364, 1968.
7. WALDMANN, T.A., MCINTIRE, K. R., The use of a radioimmuno-assay forAlpha-fetoprotein in the diagnosis of malignancy. Cancer 34:1510, 1974.
8. ABELEV, G. I., Alpha-fetoprotein in ontogenesis and its association with malignanttumours. Adv. Cancer Res. 14:295, 1971.
9. BROCK, D. J. H., Mechanism by which amniotic fluid Alpha-fetoprotein may beincreased in fetal abnormalities. Lancet (ii): 345, 1976.
10. GITLIN, G., Normal biology of Alpha-fetoprotein. Ann. N. Y. Acad. Sci. 259:7,1975.
11. RUOSLAHTI, E., HIRAR, H., Alpha-fetoprotein: Physiology and Pathologyduring pregnancy and application to antenatal diagnosis. Scand. J. Immunol.8:3, 1978.
12. MASSEYEFF, R. F., Alpha-fetoprotein: Use in screening. In Immunodiagnosisof Cancer. HERBERMAN, R.B., and MCINTIRE, R. K., (Eds) Marcell DekkerInc. New York pp 117 - 129, 1979.
13. SCARDINO, R. T., COX, H. D., WALDMANN, T. K., McINTIRE, K.P.,MITTEMEYER, B., JAVADPOUR, N. , The value of serum tumour markers in thestaging and prognosis of germ cell tumours of the testis. J. Urol. 118:994, 1977.
14. LANGE, P. H., MCINTIRE, K. R., WALDMANN, T. A., HAKALA, T.R., FRALEY,E.E., Serum Alpha-fetoprotein and human chorionic gonadotrophin in the diagnosisand management of non-seminomatous germ cell testicular cancer. New Engl.J. Med. 295:1237, 1976.
15. KINDERS, R.J., HASS, G.M., Interference in immunoassay by human anti-mouse antibodies. Eur. J. Cancer. 26 (5):647, 1990.
16. BOSCATO, L.M., STUART, M.C., Incidence and specificity of interference intwo-site immunoassays. Clin. Chem. 32 (8): 1491, 1986.
17. HORACEK, K.L., PEPPERELL, R.J., HAY, D.L., BARRIE, J.V., BATTERY,B.W., Detection of feto-maternal hemorrhage by measurement of maternalserum AFP. Lancet (ii) : 200, 1976.
18. KEW, M.C., PURVES, L.R., BERSOHN, I., Serum alpha-fetoprotein levels inacute viral hepatitis. Gut 14:939, 1973.
19. SAKAMOTO, S., YACHI, A., ANZAI, T., WADA, T., Alpha-fetoprotein producingcells in hepatitis and in liver cirrhosis. Ann. N.Y. Acad. Sci. 259:253, 1975.
20. MACRI, J.N., WEISS, R.R., Prenatal serum alpha-fetoprotein screening forneural tube defects. Obstet. Gynecol. 59:633, 1982.
21. PALOMAKI, G.E., HILL, L.E., KNIGHT, G.J., HADDOW, J.E., CARPENTER,M., Second trimester maternal serum alpha-fetoprotein levels in pregnanciesassociated with gastroschisis and omphalocele. Obstet. Gynecol. 71:906, 1988.
22. WALD, N., BARKER, S., CUCKLE, H., BROOK, D.J.H., STIRRAT, S.M., Maternalserum alpha-fetoprotein and spontaneous abortion. Br. J. Obstet. Gynecol.84:357, 1977.
23. REDFORD, D.H., WHITFIELD, C.R., Maternal serum alpha-fetoprotein in twinpregnancies uncomplicated by neural tube defect. Am. J. Obstet. Gynecol.152(5):550, 1985.
24. DAVENPORT, D.M., MACRI, J.N., The clinical significance of low maternalserum alpha-fetoprotein. Am. J. Obstet. Gynecol. 146:657, 1983.
936LI4017K/040705

Adaltis Italia S.p.A.Via Cristoni, 1240033 Casalecchio di Reno - (BO) ItalyTel. +39-051-6136511 - Fax +39-051-575280www.adaltis.com
Fabricado por:Unidade de FabricoVia L. Einaudi, 700012 Guidonia Montecelio - (Rome)Italy
1 / 4
Conjugado Biotina-AFP
Conjugado HRP-AFP
96 Testes
APENAS PARA USO DIAGNÓSTICO “IN VITRO”
Conserve a 2...8°C
SIMBOLO USADO NOS RÓTULOS
LI4017KREF
pt
EIAgen AFP∑∑∑∑∑
Limite de temperatura(conservar a 2...8°C)
Microplaca de Estreptavidina
Atenção, consulte as Instruções deUtilização
AFP - Calibrador B
AFP - Calibrador C
AFP - Calibrador D
AFP - Calibrador E
AFP - Calibrador F
Código do Catálogo
Prazo de validade (Usar até...)
Número de testes
Número do Lote
AFP - Calibrador A
Dispositivo médico de diagnóstico invitro (Uso diagnóstico in vitro)
Diluente AFP
Fabricado por...
Solução de Lavagem 10x
8°C
2°C
R E F
LOT
IVD
Substrato HS
Solução de Paragem
∑∑∑∑∑
!!!!!
Risco biológico
1.0 UTILIZAÇÃO PREVISTAO kit EIAgen AFP foi concebido para a determinação quantitativa da Alfa-fetoproteínano soro humano, plasma ou líquido amniótico.Os padrões são calibrados contra a 1ª Preparação de Referência Internacional (PRI)da OMS, para a AFP humana (72/225).
2.0 RESUMO E EXPLICAÇÃO DO TESTEA alfa-fetoproteína (AFP) é uma proteína do soro fetal, que circula em quantidadesmínimas nos adultos saudáveis (2). A AFP é produzida essencialmente pelo sacovitelino do feto e pelo fígado do feto e, em menor grau, pelo tracto gastrointestinal erins do feto (3). Trata-se de uma glicoproteína de cadeia simples, com um pesomolecular de aproximadamente 65-70 kilodaltons. As propriedades físico-químicas ea composição aminoácida da AFP são semelhantes às da albumina do soro (4), daqual é antigenicamente distinta (5).O interesse clínico na AFP é na oncologia onde a AFP do soro é usada para odiagnóstico e a monitorização de tumores (6,7,8) e no rastreio pré-natal onde a AFPdo líquido amniótico é usada para detectar anormalidades no feto, como a espinhabífida e o Síndroma de Down (9).A AFP do plasma fetal distribui-se pela urina fetal e é excretado no líquido amniótico,de onde se distribui pela circulação materna. A concentração de AFP no plasma fetalatinge o seu pico (2-3 mg/ml) às 12-14 semanas e depois decresce rapidamente (9).Os níveis no líquido amniótico são paralelos aos do plasma fetal, mas são cerca dedois graus de magnitude mais baixos (intervalo µg ) do que a concentração de plasmafetal. Ao contrário, as concentrações de AFP no soro materno aumentam geometri-camente até às 30 semanas de gestação e depois entram em declínio (10). Após onascimento, os níveis de AFP na mãe e no recém-nascido regressam rapidamenteaos níveis basais (< 10 ng/ml).Aproximadamente 70% dos doentes com carcinoma hepatocelular primário apresentaníveis elevados de AFP (7). Foram relatados níveis de 1,000 - 10,000 ng/ml (11). Nocaso de teratoma testicular, observou-se uma relação directa entre a incidência dosníveis elevados de AFP e o estágio da doença (12). Não se observou o aumento dosníveis de AFP nos seminomas testiculares (13). A aplicação da medição AFP emdoentes com carcinoma tem sido bem documentada (14). O facto dos níveis de AFPnão retomarem os valores normais após a operação sugere a presença de tumorresidual.Observaram-se também níveis aumentados de AFP no soro em condições benignas,como por exemplo infecções virais agudas, hepatite activa crónica e cirrose. Tambémse observaram níveis elevados de AFP no líquido amniótico noutras situaçõesgraves, como morte fetal, onfalocele e síndroma de Turner.
3.0 PRINCÍPIO DO MÉTODOO ensaio AFP EIAgen baseia-se no princípio de sanduíche imunoenzimática de duasetapas, em conjunto com a tecnologia Biotina-Estreptavidina.São utilizados dois anticorpos monoclonais anti-AFP de elevada afinidade eespecificidade: um é marcado com Peroxidase de Armorácio (HRP) e o outro émarcado com Biotina, enquanto que os poços das microplacas são revestidos comEstreptavidina.As amostras, calibradores e controlos são distribuídos pelos poços, seguidos peloconjugado anti-AFP Biotina.Durante a incubação o anticorpo monoclonal liga a molécula de AFP a um localespecífico e, ao mesmo tempo, a Estreptavidina fixa o complexo imunológico emformação aos poços, através da ligação do anticorpo biotinilado à fracção da biotina.Após a lavagem para eliminação das espécies não reactivas, adiciona-se o segundoanticorpo monoclonal conjugado com HRP.Após a segunda incubação, os poços são lavados para remover os anticorposmarcados não ligados e, em seguida, adiciona-se a mistura de cromogénio/substrato.A reacção é então bloqueada ao adicionar-se a Solução de Paragem e a cordesenvolvida é medida por fotometria. A intensidade da cor é directamente proporcional(dentro do intervalo de trabalho do ensaio) à concentração de AFP na amostra. Aconcentração de AFP numa amostra da paciente ou nos controlos é então determinadapor interpolação na curva de calibração.
4.0 REAGENTES - ARMAZENAMENTO E MANUSEAMENTOO kit EIAgen AFP contém reagentes suficientes para 96 poços. Ao recebê-lo, conser-ve o kit e cada um dos reagentes a 2...8°C, os quais permaneceram estáveis até aoprazo de validade constante dos rótulos.Se não for especificado o contrário, todos os reagentes são estáveis após a aberturaaté ao prazo de validade indicado nos rótulos, desde que sejam conservados comoindicado e não ocorram contaminações durante a pipetagem.
4.1 Microplaca de Estreptavidina
O saco contém uma microplaca de 12 tiras x 8 poços.Cada um dos poços é revestido com Estreptavidina e pode ser utilizado individual-mente. Ponha a microplaca a aquecer até atingir a temperatura ambiente (18... 25°C)antes de ser utilizada. Após a primeira abertura as tiras não utilizadas permanecemestáveis durante 2 meses a 2...8°C, desde que sejam conservadas na bolsa deplástico com o dessecante.
4.2 Calibradores AFP
6 frascos de Calibradores AFP contendo 0- 5- 25- 125- 250- 500 IU/ml (1ª PRI 72/225)em soro de cavalo com Azida Sódica (0,09% w/w) e Proclin 300 (0,0025% v/v) comoconservantes. 0,5 ml para cada Calibrador. Pronto a usar. Misture suavemente antesde utilizar.
4.3 Diluente AFP
1 frasco de Diluente AFP contendo soro de cavalo e Azida Sódica (0,09% w/w) eProclin 300 (0,0025% v/v) como conservantes. 13 ml Pronto a usar. Misture suavementeantes de utilizar.
4.4 Conjugado Biotina-AFP
1 frasco contendo um anticorpo monoclonal anti-AFP marcado com Biotina emtampão Tris com albumina de soro de bovino (BSA) e Proclin 300 (0,0025%) v/v),como conservante. 13 ml Pronto a usar. Misture suavemente antes de utilizar.
MT PLATE
CAL A...F
CONJ BIOT
Evite a exposição à luz solar directa
MT PLATE
CONJ BIOT
CONJ HRP
SUBS TMB
SOLN STOP
CAL A
CAL B
CAL C
CAL D
CAL E
CAL F
BUF WASH 10 X
DIL SPE
DIL SPE

4.5 Conjugado HRP-AFP
1 frasco contendo um anticorpo monoclonal anti-AFP marcado com Peroxidase deArmorácio em tampão Tris com albumina de soro de bovino (BSA) e Proclin 300(0,0025%) v/v), como conservante. 13 ml Pronto a usar. Misture suavemente antesde utilizar.
4.6 Solução de Lavagem 10x
Um frasco de Solução de Lavagem 10x, contendo Tween 20 (0,1%) e Amfotericina-B (2,5 µg/ml) em tampão citrato-borato. 50 ml.Dilua o conteúdo do frasco num volume de 450 ml de água destilada ou desionizada.Misture bem. Após a diluição armazene a 2...8°C durante 2 meses ou à temperaturaambiente durante 5 dias.
4.7 Substrato HS
Um frasco de Substrato HS contendo 0,26 mg/ml de 3,3’,5,5’ Tetrametilbenzidina(TMB) e 0,01% w/v de peróxido de hidrogénio (H2O2), em tampão citrato. 13 ml.Pronto a usar. Misture suavemente antes de utilizar.
4.8 Solução de Paragem
Um frasco de Solução de Paragem contendo 13 ml de Ácido Sulfúrico (H2SO
4) a 0,3
mol/l. Pronto a usar. Misture suavemente antes de utilizar.
5.0 MATERIAIS E EQUIPAMENTO NECESSÁRIOS
5.1 Materiais Fornecidos
Material Quantidade Código
Microplaca de Estreptavidina Um saco LSSTREPPBAFP - Calibrador A 0,5 ml LS4017SK-AAFP - Calibrador B 0,5 ml LS4017SK-BAFP - Calibrador C 0,5 ml LS4017SK-CAFP - Calibrador D 0,5 ml LS4017SK-DAFP – Calibrador E 0,5 ml LS4017SK-EAFP - Calibrator F 0,5 ml LS4017SK-FDiluente AFP 13,0 ml LS4017SK0Conjugado Biotina-AFP 13,0 ml LS4017BKConjugado HRP-AFP 13,0 ml LS4017EKSolução de Lavagem 10x 50,0 ml LSWASHKSubstrato HS 13,0 ml LSTMBH2O2HKSolução de Paragem 13,0 ml LSSTOPK
5.2 Materiais e Equipamento Não Fornecidos● Água destilada ou deionizada● Pipeta de precisão 0.025 de 0,1 ml com pontas descartáveis.● Pipetas de deslocação positiva ou distribuição repetitiva de 0,1 ml, para adição
de Conjugado, Substrato e Solução de Paragem.● Lavador de placa automático● Incubador de Microtitulação● Leitor de placa de microtitulação, equipado para a medição da absorvância a
450nm (filtro de referência a 620 nm).● Compressa ou papel adsorvente● Soros de Controlo (recomendados).
6.0 ADVERTÊNCIAS, PRECAUÇÕES E LIMITAÇÕESApenas para uso diagnóstico in vitro.Este teste apenas deverá ser utilizado por pessoal laboratorial experiente,devendo o manuseamento estar em conformidade com as boas práticas delaboratório.
6.1 Precauções de Segurança● Não utilize a boca na pipetagem.● Não fume, coma ou aplique cosméticos em áreas de manuseamento de amostras
dos doentes ou reagentes dos kits.● Cortes, abrasões e outras lesões dérmicas devem ser protegidas adequadamente
com uma compressa à prova de água.● Tenha cuidado para evitar a auto-inoculação, salpicos nas membranas mucosas
ou a geração de aerossóis.● Deve usar luvas de laboratório enquanto manuseia as amostras dos doentes ou
elimina resíduos sólidos ou líquidos.● Evite a contaminação microbiana dos padrões durante a pipetagem, usando
pontas de pipeta descartáveis.● A eliminação de todos os resíduos deve estar em conformidade com os
regulamentos locais.
6.2 Advertência Contra Potencial Risco BiológicoAlguns dos reagentes usados podem ter sido preparados a partir de pools de sorohumano. Cada uma das unidades de sangue usadas para preparar estes pools foitestada para a presença de sífilis, para a presença do Antigénio de Superfície daHepatite B (HbsAG) e de anticorpos do Vírus da Imunodeficiência Humana (HIV1 e2) usando métodos aprovados pela FDA, tendo o resultado sido negativo. Dado quenenhum teste oferece a garantia absoluta da ausência do vírus da Hepatite B, doHIV, ou de outros agentes infecciosos, estes reagentes devem ser consideradoscomo potencial risco biológico e manuseados com as mesmas precauções aplicadasàs amostras de soro ou plasma. Alguns reagentes, como os padrões de calibração eos controlos, podem conter materiais de origem humana. Presentemente não existequalquer método de teste padrão para detectar a presença de HIV neste tipo dematerial. Deste modo, recomenda-se que estes reagentes sejam considerados comopassíveis de constituir perigo biológico.Estes materiais devem ser manuseados de acordo com as boas práticas de laboratório,como descrito no documento CDC (Center for Disease Control – Centro de Controloda Doença, Atlanta, EUA): Universal precautions for prevention of transmission ofhuman immunodeficiency virus, hepatitis B virus, and other blood bourne pathogensin healthcare setting “MMWR” 37:377-387, 1999.
6.3 Advertência sobre Azida Sódica (NaN3)A azida sódica está presente como conservante na matriz padrão, numa concentraçãonão superior a 0,09% w/w. A azida sódica pode reagir com as canalizações de chumboe cobre, formando azidas metálicas explosivas. Os resíduos líquidos e sólidosdevem ser eliminados de forma segura, de acordo com os regulamentos locais. Aazida em concentrações superiores a 0,1% w/w interfere nos resultados deste ensaio;assim, o ensaio dos soros ou amostras de controlo que contenham o compostomencionado acima pode produzir resultados sobrestimados.Frases de RiscoR 21/22 Nocivo em contacto com a pele e se engolido.Frases de SegurançaS 26 Em caso de contacto com os olhos, enxagúe imediatamente com uma
quantidade abundante de água e procure aconselhamento médico.S 28.1 Após contacto com a pele, lave imediatamente com bastante água.S 46 Se engolido, procure imediatamente aconselhamento médico e mostre a
embalagem ou o rótulo.
6.4 Aviso sobre o Ácido Sulfúrico (H2SO4)O ácido sulfúrico está presente na Solução de Paragem a uma concentração nãosuperior a 0,3 mol/l. Não pipete com a boca.Frases de riscoR 36/38 Irritante para os olhos e pele.Frases de segurançaS 26 Em caso de contacto com os olhos, enxagúe imediatamente com muita
água e procure apoio médico.
6.5 Advertência sobre a 3-3’-5-5’ Tetrametilbenzidina (TMB)A 3-3’-5-5’ Tetrametilbenzidina (TMB) está presente no Substrato HS. Evite o contactodeste reagente com a pele ou membranas mucosas. Se tal ocorrer, laveabundantemente com água fria da torneira. Não utilize a boca na pipetagem.
6.6 LimitaçõesNão utilize EDTA como anticoagulante a uma concentração superior a 5g/l. As diluiçõesque fornecem valores inferiores ao limite de detecção do ensaio não devem serutilizadas. Dado que a reacção enzimática está dependente da temperatura, podemser obtidas absorvâncias diferentes de acordo com a temperatura do laboratório.Tal como acontece com todos os imunoensaios, os resultados deste teste podem serinfluenciados por factores presentes em algumas amostras obtidas de doentes. Osreagentes deste ensaio não foram formulados para minimizar interferências causadaspor anticorpos heterofílicos e pela ligação da proteína não específica. Contudo, talcomo acontece com outros métodos de imunoensaio de dois locais, os resultadosdas amostras individuais podem ser afectados.Para fins de diagnóstico, os resultados obtidos através deste ensaio devem sersempre avaliados em conjunto com o exame clínico do doente, o historial do pacientee outros achados clínicos.As indicações processuais devem ser seguidas na íntegra, dado que qualquermodificação do procedimento pode alterar os resultados.O uso de reagentes e peças descartáveis ou de reposição diferentes das fornecidaspelo distribuidor autorizado pode produzir resultados incorrectos.Os doentes que receberam anticorpos monoclonais de rato, para procedimentos dediagnóstico ou terapêuticos, podem desenvolver anticorpos anti-rato humanos (AARH).Os AARH podem produzir valores elevados falsos ou valores baixos falsos emimunoensaios que utilizam anticorpos monoclonais de rato (15,16). As amostras quecontêm AARH não devem ser ensaiadas com o ensaio EIAgen AFP.
6.7 Indicações de deterioração do substrato● A solução de Substrato simples é incolor ou ligeiramente amarela-azulada. Se
ocorrer contaminação acidental, a solução começa a desenvolver uma cor azule deve ser deitada fora.
● A solução de Substrato simples não é sensível à luz. A luz solar directa pode, noentanto, oxidar a solução para uma cor azul. Essa cor desaparece se a soluçãofor mantida em local escuro durante 4 horas, após as quais a solução pode sernovamente utilizada.
● Com o envelhecimento do substrato este pode adquirir uma cor ligeiramenteamarela-alaranjada. Isto não afecta o seu desempenho.
● Se utilizar apenas parte do conteúdo do frasco de Substrato, para evitar acontaminação, transfira o volume necessário para um recipiente de plásticolimpo, que tenha sido lavado previamente com etanol e enxaguado com águadestilada de alta qualidade.
7.0 COLHEITA E ARMAZENAMENTO DAS AMOSTRAS
7.1 SoroRecolha 5 ml de sangue venoso num tubo de vidro sem aditivos. Deixe que estecoagule à temperatura ambiente. Centrifugue, separe a fracção do soro e armazene.
7.2 PlasmaRecolha 5 ml de sangue venoso num tubo de vidro ou plástico contendo heparina oucitrato como anticoagulante. Centrifugue, separe a fracção do soro e armazene.
7.3 Líquido AmnióticoRecolha amostras de líquido amniótico para dentro de um tubo de plástico estéril,sem aditivos.
7.4 DiluiçãoAs amostras de soro e plasma com concentrações que se esperam ser acima de 500mIU/ml, devem ser diluídas no Diluente AFP, antes do ensaio.O líquido amniótico deve ser diluído numa proporção de pelo menos 1:100.
7.5 ArmazenamentoAs amostras de soro, plasma e líquido amniótico estão estáveis até um máximo de24 horas a 2...8°C. Para um armazenamento mais prolongado, separe em alíquotase armazene a -20°C durante no máximo 90 dias.Evite o congelamento e o descongelamento repetido.
7.6 Interferências ConhecidasEvite a utilização dos seguintes tipos de amostras de soro ou plasma, visto quepodem produzir resultados incorrectos:Amostras excessivamente hemolizadasAmostras excessivamente lipémicas
CONJ HRP
SUBS TMB
SOLN STOP
2 / 4
BUF WASH 10 X

Amostras excessivamente ictéricasAs amostras de plasma anticoagulado com EDTA com concentrações de EDTAsuperiores a 5g/l não devem ser utilizadas.Se o líquido amniótico for contaminado com sangue, a origem da hemoglobina deveser determinada. Devido aos níveis elevados de AFP em circulação no plasma fetal,as amostras contaminadas com sangue fetal não devem ser usadas.
8.0 PROCEDIMENTO DO ENSAIO
8.1 Preparação do Ensaio1. Ponha os reagentes a aquecer à temperatura ambiente e misture suavemente
antes da utilização.2. Para cada ensaio, prepare os seguintes grupos de poços e coloque-os no
suporte da tira:● 2 poços para o cromogénio branco (opcional para CQ);● 2 poços para Bo (concentração zero do antigénio);● 2 poços para cada concentração de calibrador;● 2 poços para cada soro, plasma ou controlo.Para o cromogénio branco pipete 0,1 ml de Substrato HS e 0,1 ml de Solução deParagem para dentro dos dois poços.
8.2 Passos da pipetagem e incubação1. Pipete 0,025 ml dos calibradores, amostras e controlos nos poços da tira
adequados.2. Pipete 0,1 ml de conjugado de Biotina -AFP em cada poço.3. Agite suavemente a placa usando um movimento lado-a-lado ou um agitador
orbital durante 10 segundos.4. Incube a 37ºC durante 30 minutos5. Lavagem: descarte a solução de incubação, enxagúe os poços três vezes com
a Solução de Lavagem e remova qualquer resíduo de líquido.6. Pipete 0,1 ml de conjugado de HRP -AFP em cada poço.7. Agite suavemente a placa usando um movimento lado-a-lado ou um agitador
orbital durante 10 segundos.8. Incube a 37°C durante 30 minutos9. Lavagem: descarte a solução de incubação, enxagúe os poços três vezes com
a Solução de Lavagem e remova qualquer resíduo de líquido.10. Pipete 0,1 ml de Substrato HS em cada poço e agite suavemente.11. Incube à temperatura ambiente durante 15 minutos.12. Interrompa a reacção adicionando 0,1 ml de Solução de Paragem a cada poço,
na mesma sequência e frequência usada para pipetar o Substrato HS.13. Agite suavemente a microplaca, tendo cuidado para evitar o derrame.14. Leia a 450 nm no espaço de 1 hora após a adição da Solução de Paragem.
8.3 Notas Processuais1. A temperatura ambiente é definida entre 18...25°C.2. Deve ser executada uma curva padrão em cada ensaio, de forma a assegurar
resultados válidos.3. Não se deve misturar reagentes de diferentes kits e lotes.4. Adicione os reagentes pela mesma ordem dos calibradores e das amostras.5. É recomendável cronometrar a adição da solução substrato/cromogénio e da
solução de paragem até estar familiarizado com o método (isto é, se a soluçãosubstrato/cromogénio for distribuída nos poços com intervalos de 3 segundos,a solução de paragem também deverá ser distribuída na mesma ordem e coma mesma frequência).
6. O tempo total despendido para a distribuição dos calibradores, controlos eamostras numa placa inteira, não deve exceder 15 minutos.
7. Procedimento de Lavagem: para o procedimento de lavagem recomenda-se umequipamento de lavagem de placa automático. Após a lavagem, bata na placainvertida em cima de papel absorvente para remover qualquer resíduo dospoços. São necessárias três lavagens.
9.0 CALIBRAÇÃOOs calibradores AFP são calibrados contra a 1ª PRI 72/225.1,0 IU Calibrador EIAgen AFP = 1,0 IU 1ª PRI 72/225Para conversão em ng/ml, multiplique os resultados AFP em IU/ml por 1.21.
10.0 CONTROLO DE QUALIDADERecomenda-se que cada laboratório utilize por rotina os seus materiais para o controlode qualidade e estabeleça os seus próprios intervalos de controlo. Devem utilizar-secontrolos de níveis múltiplos em cada ensaio.Os valores AFP obtidos para o material de controlo de qualidade não devem recairrepetidamente fora dos intervalos de controlo estabelecidos em cada laboratório.
11.0 CÁLCULO DE RESULTADOS
11.1 Conversão da Densidade Óptica (DO)A Densidade Óptica (DO) dos calibradores a 500 mIU/ml pode resultar em cerca de2,5. Se o leitor conseguir ler as DOs acima de 2,5, então a leitura a 450 nm(comprimento de onda do pico) e a 620 nm (filtro de referência para a subtracção dainterferência do plástico) é suficiente. Se o leitor não conseguir ler acima de 2,5,então o utilizador tem duas opções:1. omitir para executar o calibrador a 500 mIU/ml.2. executar o calibrador a 500 mIU/ml e efectuar a leitura a 450 nm e também a
405 nm (no “ombro do pico”), sempre contra o filtro de subtracção a 620 nm.Identificar os poços com DOs acima de 2,0 a 450 nm para os calibradores epara as amostras, registar a DO correspondente a 405 nm e multiplicar estasDOs pelo factor de conversão 3,0, dado que:DO 450 nm = DO 405 nm x 3,0 (para este substrato).
Os instrumentos automáticos: Allertech e Personal Lab conseguem ler automatica-mente e ao mesmo tempo a 450 -405 e 620 nm e multiplicar por 3,0 as DOs a 405nmque apresentam resultados acima de 2,0 a 450 nm, quando esta opção é seleccionada.
11.2 Redução de Dados - Método ManualCalcule, como previamente descrito, a média DO a 450 nm dos calibradores e dasamostras. Trace as DOs médias dos calibradores versus a respectiva concentraçãode AFP, em papel gráfico logarítmico ou semi-logarítmico, e determine a concentraçãode AFP na amostra, por interpolação a partir da curva de calibração. Os resultadostambém podem ser calculados com programas normais para processamentoautomático de dados, isto é, 4 Parâmetros e Spline.
11.3 Redução de Dados - Método AutomáticoUse os 4 parâmetros logísticos - preferencial - ou a função “cubic spline” comoalgoritmo de cálculo.
11.4 Amostras com DOs acima do Calibrador a 500 mIU/mlSe o valor AFP exceder o valor do calibrador mais elevado, dilua a amostra com odiluente e realize novamente o ensaio. Multiplique o resultado obtido pelo factor dediluição da amostra.
11.5 Curva de Calibrador Típica
Calibrador (IU/ml) Método Manual Método LabotechDO 450 nm DO 450 nm
0 0,018 0,0385 0,130 0,137
25 0,445 0,442125 1,408 1,493250 2,050 1,938500 2,662 2,503
12.0 VALORES ESPERADOSO intervalo normal para pacientes saudáveis (não grávidas) é de < 10 IU/ml de AFP.Os valores fornecidos são apenas indicativos e podem variar de outros dadospublicados, dado que a concentração de AFP medida em indivíduos varia consoanteos diferentes métodos empregues.Recomenda-se que cada laboratório estabeleça os seus próprios valores de referência.
12.1 Factores Associados ao Aumento dos ValoresObservaram-se com bastante frequência níveis elevados de AFP no soro de doentescom carcinoma hepatocelular e alguns tumores de células germinativas dos testículose ovários (6,7). Também se observaram níveis elevados de AFP em condições nãomalignas, tal como na hepatite viral (18) e na cirrose hepática (19).Em algumas anormalidades fetais, nomeadamente nos defeitos do tubo neural aberto(DTN), foram observados níveis elevados de AFP, no líquido amniótico (9) e no soromaterno (20). Foram também observadas concentrações elevadas de AFP no soromaterno, noutras condições de irregularidade fetal como: onfalocete (21), ameaça deaborto (22) e na gravidez múltipla (23).Verificou-se que factores endógenos, tais como os anticorpos anti-rato humanosexistentes no soro humano, causam valores de antigénio falsamente elevados nosimunoensaios (16).
12.2 Factores Associados ao Decréscimo dos ValoresForam observados valores baixos de AFP no soro materno e líquido amniótico nagravidez molar e na síndroma de Down (24).Verificou-se que factores endógenos, como os anticorpos anti-rato humanos existentesno soro humano, causam valores de antigénio falsamente decrescidos nosimunoensaios (16).
13.0 CARACTERÍSTICAS DE DESEMPENHOO ensaio EIAgen AFP foi concebido para que o efeito de “gancho “, característico dosensaios imunométricos, não interfiram com os valores AFP até ao máximo de350000 IU/ml.
13.1 Precisão - Teste de RecuperaçãoRealizou-se o teste de recuperação adicionando AFP purificada a amostras de sororetiradas de um pool de soros.As amostras limpas e fortalecidas foram medidas no ensaio EIAgen AFP.Dados da Recuperação
Amostra AFP Adicionada AFP Medida % Recuperação(IU/ml) (IU/ml)
1 0 5,00 -46,40 45,50 98,1090,30 88,60 98,10
178,10 172,30 96,70353,70 350,80 99,20
2 0 52,70 -46,40 99,60 104,2090,30 137,00 98,80
178,10 225,00 100,20353,70 370,00 93,40
3 0 42,00 -46,40 80,60 94,6090,30 118,30 92,20
178,10 199,20 92,80353,70 359,60 92,80
3 / 4
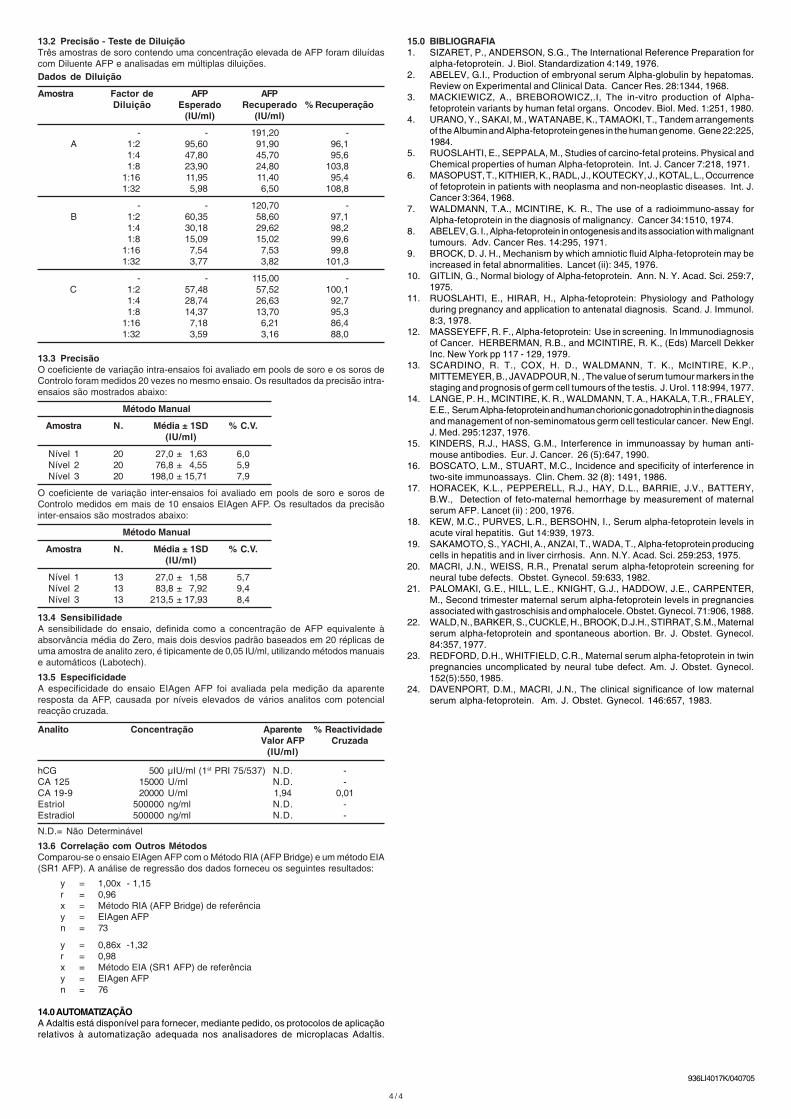
13.2 Precisão - Teste de DiluiçãoTrês amostras de soro contendo uma concentração elevada de AFP foram diluídascom Diluente AFP e analisadas em múltiplas diluições.Dados de Diluição
Amostra Factor de AFP AFPDiluição Esperado Recuperado % Recuperação
(IU/ml) (IU/ml)
- - 191,20 -A 1:2 95,60 91,90 96,1
1:4 47,80 45,70 95,61:8 23,90 24,80 103,8
1:16 11,95 11,40 95,41:32 5,98 6,50 108,8
- - 120,70 -B 1:2 60,35 58,60 97,1
1:4 30,18 29,62 98,21:8 15,09 15,02 99,6
1:16 7,54 7,53 99,81:32 3,77 3,82 101,3
- - 115,00 -C 1:2 57,48 57,52 100,1
1:4 28,74 26,63 92,71:8 14,37 13,70 95,3
1:16 7,18 6,21 86,41:32 3,59 3,16 88,0
13.3 PrecisãoO coeficiente de variação intra-ensaios foi avaliado em pools de soro e os soros deControlo foram medidos 20 vezes no mesmo ensaio. Os resultados da precisão intra-ensaios são mostrados abaixo:
Método Manual
Amostra N. Média ± 1SD % C.V.(IU/ml)
Nível 1 20 27,0 ± 1,63 6,0Nível 2 20 76,8 ± 4,55 5,9Nível 3 20 198,0 ± 15,71 7,9
O coeficiente de variação inter-ensaios foi avaliado em pools de soro e soros deControlo medidos em mais de 10 ensaios EIAgen AFP. Os resultados da precisãointer-ensaios são mostrados abaixo:
Método Manual
Amostra N. Média ± 1SD % C.V.(IU/ml)
Nível 1 13 27,0 ± 1,58 5,7Nível 2 13 83,8 ± 7,92 9,4Nível 3 13 213,5 ± 17,93 8,4
13.4 SensibilidadeA sensibilidade do ensaio, definida como a concentração de AFP equivalente àabsorvância média do Zero, mais dois desvios padrão baseados em 20 réplicas deuma amostra de analito zero, é tipicamente de 0,05 IU/ml, utilizando métodos manuaise automáticos (Labotech).
13.5 EspecificidadeA especificidade do ensaio EIAgen AFP foi avaliada pela medição da aparenteresposta da AFP, causada por níveis elevados de vários analitos com potencialreacção cruzada.
Analito Concentração Aparente % ReactividadeValor AFP Cruzada
(IU/ml)
hCG 500 µIU/ml (1st PRI 75/537) N.D. -CA 125 15000 U/ml N.D. -CA 19-9 20000 U/ml 1,94 0,01Estriol 500000 ng/ml N.D. -Estradiol 500000 ng/ml N.D. -
N.D.= Não Determinável
13.6 Correlação com Outros MétodosComparou-se o ensaio EIAgen AFP com o Método RIA (AFP Bridge) e um método EIA(SR1 AFP). A análise de regressão dos dados forneceu os seguintes resultados:
y = 1,00x - 1,15r = 0,96x = Método RIA (AFP Bridge) de referênciay = EIAgen AFPn = 73
y = 0,86x -1,32r = 0,98x = Método EIA (SR1 AFP) de referênciay = EIAgen AFPn = 76
14.0 AUTOMATIZAÇÃOA Adaltis está disponível para fornecer, mediante pedido, os protocolos de aplicaçãorelativos à automatização adequada nos analisadores de microplacas Adaltis.
4 / 4
15.0 BIBLIOGRAFIA1. SIZARET, P., ANDERSON, S.G., The International Reference Preparation for
alpha-fetoprotein. J. Biol. Standardization 4:149, 1976.2. ABELEV, G.I., Production of embryonal serum Alpha-globulin by hepatomas.
Review on Experimental and Clinical Data. Cancer Res. 28:1344, 1968.3. MACKIEWICZ, A., BREBOROWICZ,.I, The in-vitro production of Alpha-
fetoprotein variants by human fetal organs. Oncodev. Biol. Med. 1:251, 1980.4. URANO, Y., SAKAI, M., WATANABE, K., TAMAOKI, T., Tandem arrangements
of the Albumin and Alpha-fetoprotein genes in the human genome. Gene 22:225,1984.
5. RUOSLAHTI, E., SEPPALA, M., Studies of carcino-fetal proteins. Physical andChemical properties of human Alpha-fetoprotein. Int. J. Cancer 7:218, 1971.
6. MASOPUST, T., KITHIER, K., RADL, J., KOUTECKY, J., KOTAL, L., Occurrenceof fetoprotein in patients with neoplasma and non-neoplastic diseases. Int. J.Cancer 3:364, 1968.
7. WALDMANN, T.A., MCINTIRE, K. R., The use of a radioimmuno-assay forAlpha-fetoprotein in the diagnosis of malignancy. Cancer 34:1510, 1974.
8. ABELEV, G. I., Alpha-fetoprotein in ontogenesis and its association with malignanttumours. Adv. Cancer Res. 14:295, 1971.
9. BROCK, D. J. H., Mechanism by which amniotic fluid Alpha-fetoprotein may beincreased in fetal abnormalities. Lancet (ii): 345, 1976.
10. GITLIN, G., Normal biology of Alpha-fetoprotein. Ann. N. Y. Acad. Sci. 259:7,1975.
11. RUOSLAHTI, E., HIRAR, H., Alpha-fetoprotein: Physiology and Pathologyduring pregnancy and application to antenatal diagnosis. Scand. J. Immunol.8:3, 1978.
12. MASSEYEFF, R. F., Alpha-fetoprotein: Use in screening. In Immunodiagnosisof Cancer. HERBERMAN, R.B., and MCINTIRE, R. K., (Eds) Marcell DekkerInc. New York pp 117 - 129, 1979.
13. SCARDINO, R. T., COX, H. D., WALDMANN, T. K., McINTIRE, K.P.,MITTEMEYER, B., JAVADPOUR, N. , The value of serum tumour markers in thestaging and prognosis of germ cell tumours of the testis. J. Urol. 118:994, 1977.
14. LANGE, P. H., MCINTIRE, K. R., WALDMANN, T. A., HAKALA, T.R., FRALEY,E.E., Serum Alpha-fetoprotein and human chorionic gonadotrophin in the diagnosisand management of non-seminomatous germ cell testicular cancer. New Engl.J. Med. 295:1237, 1976.
15. KINDERS, R.J., HASS, G.M., Interference in immunoassay by human anti-mouse antibodies. Eur. J. Cancer. 26 (5):647, 1990.
16. BOSCATO, L.M., STUART, M.C., Incidence and specificity of interference intwo-site immunoassays. Clin. Chem. 32 (8): 1491, 1986.
17. HORACEK, K.L., PEPPERELL, R.J., HAY, D.L., BARRIE, J.V., BATTERY,B.W., Detection of feto-maternal hemorrhage by measurement of maternalserum AFP. Lancet (ii) : 200, 1976.
18. KEW, M.C., PURVES, L.R., BERSOHN, I., Serum alpha-fetoprotein levels inacute viral hepatitis. Gut 14:939, 1973.
19. SAKAMOTO, S., YACHI, A., ANZAI, T., WADA, T., Alpha-fetoprotein producingcells in hepatitis and in liver cirrhosis. Ann. N.Y. Acad. Sci. 259:253, 1975.
20. MACRI, J.N., WEISS, R.R., Prenatal serum alpha-fetoprotein screening forneural tube defects. Obstet. Gynecol. 59:633, 1982.
21. PALOMAKI, G.E., HILL, L.E., KNIGHT, G.J., HADDOW, J.E., CARPENTER,M., Second trimester maternal serum alpha-fetoprotein levels in pregnanciesassociated with gastroschisis and omphalocele. Obstet. Gynecol. 71:906, 1988.
22. WALD, N., BARKER, S., CUCKLE, H., BROOK, D.J.H., STIRRAT, S.M., Maternalserum alpha-fetoprotein and spontaneous abortion. Br. J. Obstet. Gynecol.84:357, 1977.
23. REDFORD, D.H., WHITFIELD, C.R., Maternal serum alpha-fetoprotein in twinpregnancies uncomplicated by neural tube defect. Am. J. Obstet. Gynecol.152(5):550, 1985.
24. DAVENPORT, D.M., MACRI, J.N., The clinical significance of low maternalserum alpha-fetoprotein. Am. J. Obstet. Gynecol. 146:657, 1983.
936LI4017K/040705