1 workplace e nvironmental t obacco s moke and adenocarcinoma of the lung among n onsmoking m en...
TRANSCRIPT

1
Workplace Workplace EEnvironmental nvironmental TTobacco obacco SSmokemoke
and Adenocarcinoma of the Lung and Adenocarcinoma of the Lung Among Among NNonsmoking onsmoking MMenen
Prof. TSE, Lap Ah Shelly 謝立亞 School of Public Health and Primary Care
The Chinese University of Hong KongApril 7-10, 2010, 5th IECOM
Chengdu, China

2
Globally
• There has been growing attention on the potential health effects of environmental tobacco smoke (ETS) over the past few decades.
• More than 40 epidemiological studies have been conducted on the association between exposure to ETS and lung cancer in lifelong nonsmokers and showed an average of 30% increased risk, but the majority of these studies were primarily on nonsmoking females who were married to smokers.

3
Research gaps• Much fewer epidemiological studies of ETS
exposure and lung cancer were reported among males who had never smoked.
• Difficulties were frequently encountered in conducting ETS studies among males due to too few lung cancer cases among lifelong nonsmokers.
• No previous studies have reported specifically the association with adenocarcinoma among nonsmoking males.

4
Objectives
• To explore the association of ETS exposure from household and workplace with lung cancer among nonsmoking Chinese males in Hong Kong by examining the exposure-response relationships
• To study the association with adenocarcinoma of the lung

5
Study design
• A subset of a large scale population-based case-referent study
6
The original cases
• Chinese males, aged 35 to 79 years, newly diagnosed primary carcinomas of the lung (ICD-9 code 162) confirmed by histology.
• Recruited consecutively from the largest oncology centre in Hong Kong from Feb 1, 2004 to September 30, 2006 and were interviewed within 3 months after diagnosis.

7
The non-smoking cases
• Among a total of 1259 eligible cases, 1208 were interviewed with a response rate of 96%.
• We excluded 1076 ever smokers and retained 132 males who reported being lifetime nonsmokers.

8
The non-smoking referents
• Frequency matched in 5-year age groups, randomly selected from residents of districts where the cases came from. All referents must have no history of physician-diagnosed cancer in any site.
• 1069 eligible referents were recruited, with a response rate of 48%.
• We excluded 533 smokers and retained 536 lifetime non-smoking referents.

9
Definition of ‘a non-smoker’
• One who had never smoked as much as 20 packs of cigarettes or 12 oz of tobacco in lifetime, or 1 cigarette a day or 1 cigar a week for 1 year.

10
Assessment of ETS exposure
• Lifetime histories of ETS exposure at home and/or workplace since childhood
• ETS exposure was defined as ever lived or worked with a smoker for at least 1 year and was regularly exposed to tobacco smoke

11
Potential confounding factors
• Indoor air pollutants – Residential radon exposure, years of cooking by
frying, incense burning, and use of mosquito coils
• Dietary habits• Alcohol drinking habits• Past history of lung diseases• Cancer history in first-degree relatives • Exposures to known or suspected
occupational lung carcinogens• Demographics

12
Statistical analysis
• Unconditional multiple logistic regression models
• Exposure-response relationships between lung cancer and ETS exposure– Years of ETS exposure, numbers of smokers,
cigarette pack-years, smoker-years
• Histological subgroup analyses were restricted to adenocarcinoma only

13
Results
• Patient characteristics
• Household ETS exposure
• Workplace ETS exposure
• Combined household and workplace ETS exposure

14
Squamous cell carcinoma, 5, 4%
Large cell carcinoma, 2, 2%
NSCC without classification, 29,
22%
Adenocarcinoma, 89, 67%
Other unspecified carcinoma, 7, 5%
15
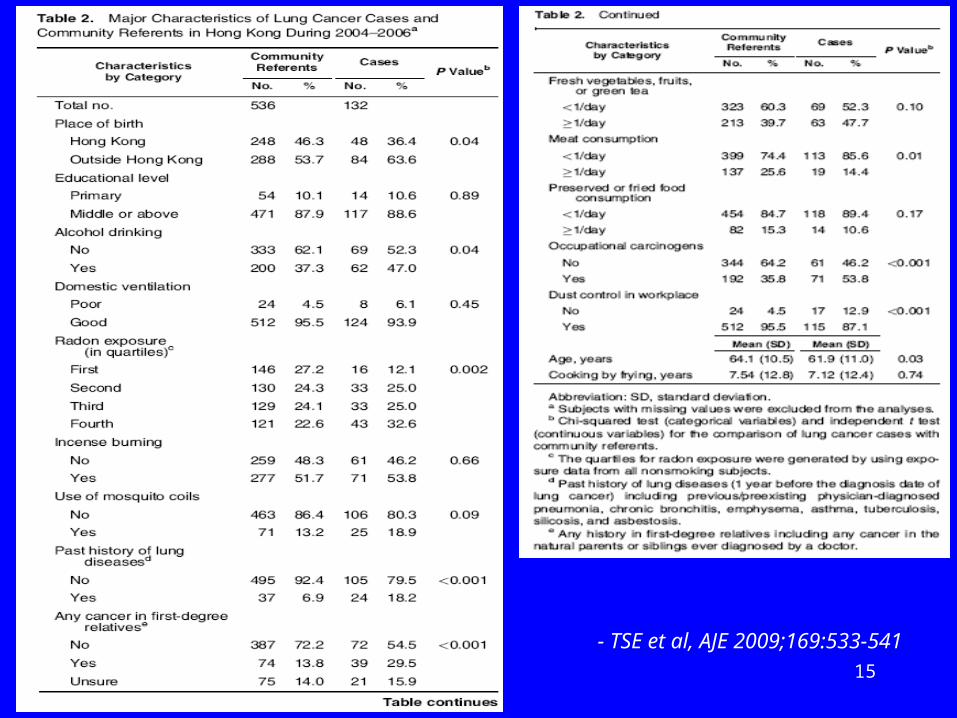
Patient characteristics
Nonsmoking lung cancers = 132 cases
15
- TSE et al, AJE 2009;169:533-541
16- TSE et al, AJE 2009;169:533-541
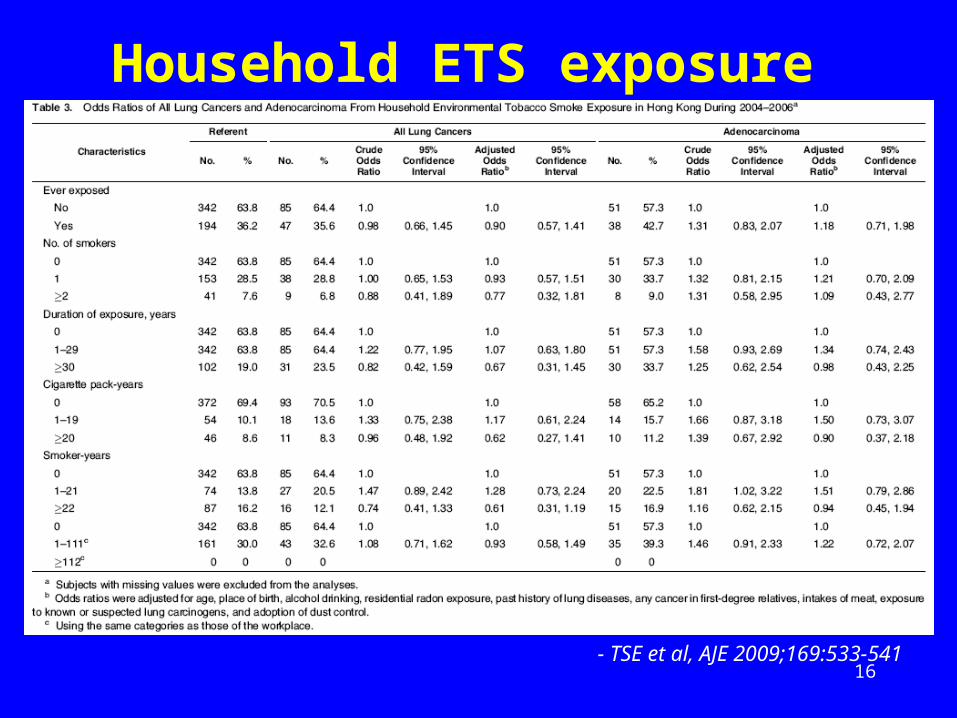
Household ETS exposure

17
- TSE et al, AJE 2009;169:533-541
Workplace ETS exposure
18
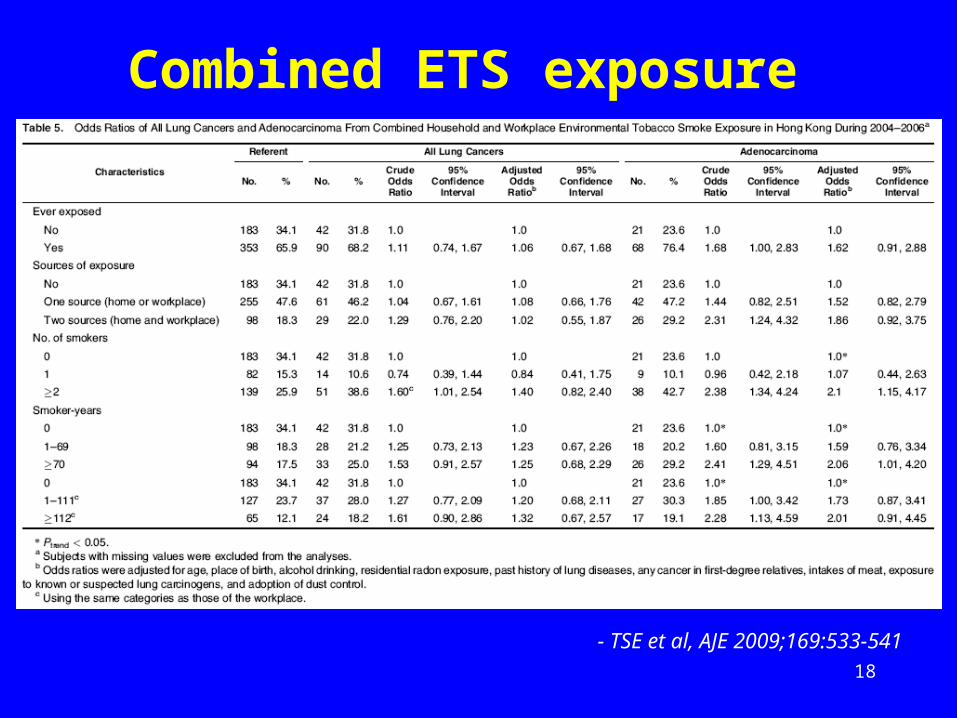
- TSE et al, AJE 2009;169:533-541
Combined ETS exposure

19
0
0.5
1
1.5
2
2.5
3
3.5
Househould
Work
place
Combin
ed
Househould
Work
place
Combin
ed
Sources of ETS expsoure
Od
ds
rati
o
All lung cancers
Adenocarcinoma

20
0
0.5
1
1.5
2
2.5
3
3.5
4
4.5
5
Household
(1)
Household
(>=2)
Work
place
(1)
Work
place
(>=2)
Combin
ed (1)
Combin
ed (>=2)
Household
(1)
Household
(>=2)
Work
place
(1)
Work
place
(>=2)
Combin
ed (1)
Combin
ed (>=2)
No. of smokers
Od
ds
rati
o All lung cancers
Adenocarcinoma

21
All lung cancers
Adenocarcinoma

22
Key messages
• The weak association between all lung cancers and male nonsmokers ever exposed to ETS was wholly contributed by a modest but insignificantly increased risk of adenocarcinoma.
• Despite some associations between exposure amounts and adenocarcinoma risk were observed in the workplace and not from household exposure, there appeared to be a stronger effect for adenocarcinma when sources of ETS exposure were combined.
• A clear exposure-response relationship with increasing level of ETS exposure remained after the adjustment of major potential confounding factors.

23
Discussion
• Previous studies on ETS and lung cancer
• Why OR is higher in workplace?
• Male ETS studies on adenocarcinoma
• Validity, reliability, and limitations

24
Previous studies on lung cancer and household ETS exposure
• A meta-analysis: OR=1.24, 95%CI: 1.13-1.36
• A European multicenter IARC study: OR=1.47, 95%CI: 0.81-2.66
• Some important confounding factors (e.g., any cancer history in first-degree relatives) not being adjusted.

25
Previous studies on lung cancer and workplace ETS exposure
• Only 3 male studies included in a meta-analysis – OR=3.3, 1.6-1.0, p>0.05– Limitations: no histology verification; small
sample size of individual studies.
• A multicenter European IARC study– OR=1.13, 95%CI: 0.68-1.86

26
Why OR is higher in workplace?• ETS exposure (i.e., smoker-years) level of
lung cancer cases from the household (median: 20) was much lower than that from occupational sources (median: 110).
• No significant association with ETS exposure from the household might reflect the difficulties in detecting an observable effect in the low exposure region.

27
Combined index is a better measurement• No male study has looked into the effects of
combined exposures from household and workplaces
• Combined exposure should be a better reflection of total ETS exposure, and hence the associations with combined exposures should be more indicative of the actual effects.

28
Male ETS studies on adenocarcinoma• Another European multicenter study showed
the age-gender-adjusted OR for lung adenocarcinoma to be 1.2 (95%CI: 0.6-2.5), but only 4 male cases were included in the study.

29
The toxicity
• Toxicological data have suggested that exposure to ETS might be consistent with a carcinogenetic effect in the deeper parts of the lung where adenocarcinoma preferentially occurs, owing to the inhalation of small-size particles of ETS (0.15-0.25mm) containing more than 95% gaseous phase of nicotine.
• Our study provides epidemiologic evidence on ETS as a risk factor in the etiology of adenocarcinoma of the lung.

30
Validity and reliability
• Validity– Selection bias – Recall / interviewer bias
• Test-retest reliability– Smoking status– ETS status?
Less likely
Less likely
Very good
??
31
Limitations
• Inadequate sample size of subgroup analysis
• Validation of ETS exposure?
32
Conclusions
• The consistent exposure-response relationships between various indices of combined household/workplace ETS exposure and the risk of adenocarcinoma suggested a probable causal link, which was largely associated with workplace exposure. However, the result would have to be confirmed by future larger studies.

33
Funding
• The work described in this paper was substantially supported by a grant from the Research Grants Council of the Hong Kong Special Administrative Region, China; Project No. CUHK4460/03M. The funding source had no role in the study design, data collection, data analysis, or interpretation of the findings

34
The team
• Prof Ignatius Tak-sun YU
• Dr Joseph S. K. Au
• Mr Kai Shing Yu
• Miss Kit Ping Kwok
• Ms Hong Qiu
• Prof Tze-wai Wong
