1 unicef sudan
TRANSCRIPT

1
©U
NIC
EF
Su
dan
/Bo
s
NUTRITION 2020
UNICEF SUDAN

2
TABLE OF CONTENTS
ACRONYMS ................................................................................................................................................................ 3
EXECUTIVE SUMMARY .............................................................................................................................................. 4
THE SITUATION IN SUDAN ........................................................................................................................................ 5
RESULTS ................................................................................................................................................................... 10
PARTNERSHIPS ......................................................................................................................................................... 12
EVIDENCE GENERATION .......................................................................................................................................... 12
CHALLENGES ............................................................................................................................................................ 13
LESSONS LEARNED .................................................................................................................................................. 13
FUTURE WORK PLAN ............................................................................................................................................... 14
CASE STUDY: DIET DIVERSITY .................................................................................................................................. 16
STORY: IT TAKES A VILLAGE TO RAISE A CHILD ...................................................................................................... 18
EXPRESSION OF THANKS ......................................................................................................................................... 21
FEEDBACK FORM ..................................................................................................................................................... 21
FINANCIAL ANALYSIS ............................................................................................................................................... 22
Cover photo: a mother support group discusses nutrition challenges in their village in Kassala.
NUTRITION ANNUAL REPORT

3
ACRONYMS CMAM Community Management of Acute Malnutrition CSO Civil Society Organisation FMOH Federal Ministry of Health HDI Human Development Index HNO Humanitarian Needs Overview IDP Internally Displaced Persons IYCF Infant and Young Child Feeding MICS Multiple Index Cluster Survey MoH Ministry of Health MoU Memorandum of Understanding MUAC Mid-Upper Arm Circumference NGO Non-Governmental Organisation ORE Other Resources Emergency (emergency thematic funding) ORR Other Resources Regular (thematic funding) OTP Outpatient Therapeutic Programme RR Regular Resources RUTF Ready-to-Use Therapeutic Food S3M Simple Spatial Survey Method SAM Severe Acute Malnutrition SC Stabilisation Centre SDG Sustainable Development Goals (or Sudanese Pound) SMoH State Ministry of Health UNFPA United Nations Population Fund UNHCR United Nations Refugee Agency UNICEF United Nations Children’s Fund USD United States Dollar WASH Water, Sanitation and Hygiene WFP World Food Programme WHO World Health Organisation

4
EXECUTIVE SUMMARY
A year after the start of the political transition and the signing of a peace agreement, humanitarian needs continue to rise across the country. These needs are primarily driven by poverty, conflict and climate change, and are exacerbated by decades long underdevelopment. The Sudan 2021 Humanitarian Needs Overview (HNO) points to 12.7 million people – 28 per cent of the population – in need of humanitarian assistance throughout 2021. This is 3.4 million people more compared to 2020. In the past 30 years, malnutrition rates have sadly not improved in Sudan. Worse still, the number of children who are stunted and wasted has actually increased since 1987, especially in Sudan’s conflict-ridden Darfur region as well as the eastern states. Sudan has one of the largest numbers of malnourished children in the world. A striking three million children under-five suffer from malnutrition, of which more than half a million from severe acute malnutrition. Without treatment these children are at risk of severe illness, developmental delays and death.
Despite the challenging operational environment and COVID-19 pandemic, UNICEF screened millions of children for malnutrition and reached children suffering from severe acute malnutrition (SAM) with therapeutic food and care, even in the most hard-to-reach areas. To achieve these goals, UNICEF worked with a large number of partners, including governmental and non-governmental organizations, UN agencies, as well as communities.
▪ 3.5 million children under-five years of age were screened for malnutrition (50 per cent girls). A total of 255,010 children were found to be suffering from severe acute malnutrition and treated through 1,660 outpatients therapeutic programme (OTPs) centres in comparison with around 257,000 children treated in 2019. Of the children receiving treatment, 234,855 girls and boys were completely cured of severe acute malnutrition (versus 212,000 cured in 2019).
▪ UNICEF procured a total of 7,000 metric tons (504,000 cartons) of ready-to-use therapeutic food (RUTF). In addition, therapeutic milk, medication for both in-patient and out-patient care, stabilisation centre kits (for children suffering from severe acute malnutrition with medical complications), anthropometric equipment and registers were secured.
▪ Promoting proper infant and young child feeding (IYCF) practices continued in 2020, with 730,360 mothers and fathers accessing IYCF counselling in 2020 (882,511 caregivers were reached in 2019).
▪ Eleven stabilisation centres in the Darfur states were supported with supplies (e.g. medicines and running costs) for inpatient care for children suffering from SAM with medical complications, with UNICEF acting as the provider of last resort – and fulfilling its Core Commitments to Children (CCC).
▪ Based on the available data, the total inpatient admission of SAM cases with medical complication across the five Darfur states was 6,898 children. Admission of SAM cases in the supported stabilisation centres reached 5,257 children representing 64.6 per cent of the total admission in the Darfur region. The overall performance indicators for the targeted stabilisation centres were aligned with Sphere standards with a cure rate of 95.5 per cent, defaulter rate at 1.7 per cent, and death rate at 2.8 per cent.
▪ An out-patient therapeutic programme (OTP) center mapping and functionality status matrix was developed and updated regularly. Despite the COVID-19 pandemic, 96 per cent of OTPs remained functional in 2020. To strengthen supplies chain management system, the following was achieved so far:
▪ UNICEF supported the carrying-out of supply chain review for nutrition supplies/RUTF, to develop
recommendations for improvement of the nutrition supply chain management and view the
possibility of its integration into the national system for medical supplies. In addition to supporting
the Federal Ministry of Health with the development of a supply chain management training manual
and facilitating the implementation of cascade trainings at different levels, UNICEF strengthened the
capacity of 286 ministry staff in Gezira, Khartoum, Kordofan, Northern State, North Darfur, River Nile
State, and South Darfur.
▪ To improve warehousing capacities, UNICEF supported State Ministries of Health in improving the warehouse conditions across twelve states. The rehabilitation work was completed in twenty warehouses: Gedaref, Kassala, North Darfur, Red Sea, South Darfur, South Kordofan, and West

5
Kordofan. Currently, there is ongoing rehabilitation works in eighteen warehouses in Central Darfur, East Darfur, Gedaref, Kassala, Red Sea, North Kordofan, South Kordofan and West Kordofan. Four warehouses in Kassala state are under technical assessment.
▪ UNICEF stepped in to support the transportation of nutrition supplies beyond state-levels through
long-term agreements with local transporters to facilitate timely transportation of supplies from the
state to the locality and OTP-level.
▪ Fighting supply leakage and misuse: UNICEF took the initiative to develop an action plan for fighting supply leakage at national and sub-national levels. UNICEF continues its strategic partnerships and technical cooperation with the different stakeholders in order to scale-up nutrition interventions, through strengthening the health system, improving access to hard-to-reach population groups, and advocacy for domestic resource mobilisation. Given that 65 per cent of the Sudanese population are under 25 years of age, getting things right for children, adolescents and youth in the immediate and longer term, will to a great degree determine how successful Sudan will be in the future. Urgent action is needed to make a critical difference in the most vulnerable children’s lives in the next months, and years to come.
THE SITUATION IN SUDAN
Sudan is the third largest country in Africa occupying approximately 1.9 million square kilometres (almost half the size of the European Union) and is home for a rapidly growing population of 41 million people. More than half of Sudan’s population are children. Spurred by a high population growth of 2.4 per cent, Sudan is experiencing a demographic shift towards a youth-based population. However, limited livelihood opportunities exist for youth, resulting in an increased risk of militarisation and recruitment of unemployed adolescents and youth into militias as well as in temporary and permanent migration within Sudan but also increasingly beyond its borders
Bordering some of East Africa’s most unstable countries, Sudan receives high numbers of refugees from neighbouring Ethiopia, Eritrea, Chad, Central African Republic and South Sudan. At the beginning of 2021, Sudan hosted more than one million refugees and asylum seekers, including more than 810,000 South Sudanese refugees; the second largest figure in the region (after Uganda)1 as well as some 60,000 Ethiopian refugees who recently fled conflict in the Tigray region. As such, Sudan is both a temporary and a long-term host country for refugees, asylum seekers, and migrants as many choose to move onwards to North Africa and Europe and Sudan stands prominently at the crossroads of the large, complex and constantly evolving Horn of Africa migration route.
Migration and displacement are fueled by political instability, poverty, conflict and climate change. The already dire situation of children and families has been exacerbated amid the ongoing severe and acute economic crisis. National poverty levels have risen drastically, with the most vulnerable populations bearing its brunt. Incomes, wages and purchasing power have fallen, driving 9.6 million people - almost a quarter of the entire population of Sudan - to severe food insecurity. With over half of households not able to meet basic daily food requirements2. Vulnerable communities have resorted to reducing meals, switching to cheaper and less nutritious foods, selling livelihood and household assets, to the detriment of future generations and at the risk of creating poverty traps3. Others have spent less on health and education and have for example withdrawn their children from schools.
COVID-19: an additional burden Sudan’s health system is on the brink of collapse with significant shortages of medicines across the primary health care system and hospitals. In 2020, thirteen out of Sudan’s eighteen states, experienced one or more outbreaks of chikungunya, dengue fever, rift valley fever or diphtheria. Medical facilities across the country faced shortages of essential drugs, further weakening the national
1 UNHCR: Sudan Population Dashboard: Refugees and Asylum-seekers (as of 28 February 2019). 2 Integrated Food Security Phase Classification estimates from World Food Programme (WFP), 2019. West Darfur State was not analysed by the state-level
technical working group; counting West Darfur, figures were estimated around 6.2 million. 3 Impact of economic crisis: household economic situation and coping mechanisms: Khartoum state.

6
response. The economic crisis has dangerously degraded the already weak, underdeveloped and heavily underfunded primary healthcare system and weak, ageing water and sanitation services.
The COVID-19 pandemic compounded the already dire public health situation in the country. A crude case fatality at 6.4 per cent, among the highest among affected countries globally and the worst one in the Middle East and North Africa region. UNICEF has shifted personnel and resources towards the efforts to prevent and reduce the spread of COVID-19 in-country and to prepare and strengthen Sudan’s capacity to respond to the crisis, while also looking to secure the continuity of other ongoing and critical humanitarian life-saving response activities.
Current momentum
Yet in this glooming picture there is hope. The new transitional government, and signed peace
agreement present an unprecedented opportunity to get things right. Establishing peace, ending the economic crisis, as well as the engagement and empowerment of young people and women who were so critical to the change process, have been clearly put at the fore by Abdalla Hamdok, Prime Minister for the Transitional Government of Sudan.
The current momentum calls for action to capitalise on a potential shift to an enabling environment. It presents an opportunity to work on sustaining peace, capacity-strengthening and community empowerment. Going beyond treating the symptoms of vulnerability - such as acute malnutrition, poor health status or poor learning achievements - and focusing on opportunities to strengthen the capacities of service providers, systems and communities.
UNICEF, given its mandate spans across the humanitarian-development-peace continuum, continues to take a lead role in working in close collaboration with key UN and NGO partners in developing a humanitarian, development and peace nexus (HDPN) approach to coordination and programming in Sudan. This includes response to emergencies and lifesaving needs, investment in preparedness and resilience, seeking durable solutions for displaced people, supporting conflict prevention, social cohesion and peacebuilding, planning for longer-term development, and building and working with national capacities.
NUTRITION In the past 30 years, malnutrition rates have not improved in Sudan, and worse still, the number of children who are stunted (too short for their age) and wasted (too thin for their height) has actually increased since 1987, especially in Sudan’s conflict-ridden Darfur region and in the eastern states.
▪ The national prevalence rate of global acute malnutrition (GAM) is 13.6 per cent and places Sudan
above the WHO threshold in seven out of eighteen states4.
▪ Three million children under-five years of age suffer from wasting (too thin for their height). ▪ 574,000 children suffer from severe acute malnutrition (SAM) and are eleven times more likely to die
than healthy children.
▪ Sudan is one of the 14 countries where 80 per cent of the world’s stunted children live5 and 128 of
Sudan’s 188 localities have a stunting rate of above 30 per cent, which means that in some cases almost half of children under-five years old will have poorer health, impaired mental and physical
development and will never reach their full potential6.
Good nutrition is closely linked to exclusive breastfeeding. In Sudan, only 62.3 per cent of all babies are exclusively breastfed for six months. Regarding Infant and young child feeding practices, out of all children below the age of two, only 25.4 per cent enjoyed age appropriate dietary diversity and 63.2 per cent age appropriate meal frequency.
4 Simple Spatial Survey Method (S3M-II), 2018. The WHO threshold for wasting is very low if GAM is less than 2.5 per cent, low if between 2.5 and 5 per cent,
medium from 5 to 10 per cent, high from 10 to less than 15 per cent, and very high from 15 and above. 5 Ministry of Health, ‘Sudan National Simple Spatial Surveying (S3M) Method’, 2013. 6 S3M II (2018)

7
Only 3.2 per cent of households consume adequately iodised salt, and 39.8 per cent of children aged under-five received a vitamin A supplement in the last six months. The low exclusive breastfeeding and complementary feeding levels reflect suboptimal infant feeding practices. This situation is particularly harmful to children under-five, who are at the stage of rapid growth and have high nutritional requirements. The poor levels of dietary diversity in children is also reflected in very low levels of dietary diversity amongst women of reproductive age (15-49). On average in all of Sudan only 8.5 per cent of women consumed the minimum dietary diversity.
Inadequate dietary intake, suboptimal infant and young child feeding, maternal malnutrition and illnesses/diseases such as diarrheal diseases (all outlined above) are immediate causes of undernutrition in Sudan. Infections increase nutrient requirements and prevent the absorption of foods consumed, while poor dietary intakes result in reduced immunity to infections. This triggers further weight loss and reduced resistance to further infections. 7 8 Environmental enteropathy, a sub-clinical disorder primarily due to poor sanitation and resulting in intestinal infections, is also an important immediate cause of malnutrition and stunting in children occasioned by chronic problems with nutrient absorption.
The underlying causes of malnutrition are multi-sectoral in nature. Inadequate household income and food insecurity leads to little variety of food. Poor access to basic sanitation and water services is another underlying cause. The correlation between increased use of basic sanitation and water services and the reduction of stunting among children under-five is well evidenced in Sudan. Many cultural practices undermine good nutrition, including caregivers’ limited knowledge of malnutrition, early marriage (and childbirth, which affects children’s birth weight) and poor education levels among mothers, which directly affect the nutrition status of young children. Less than half of the population has access to basic services despite efforts to expand the health, nutrition and water and sanitation services and to integrate nutrition into healthcare.
Close to half of Sudan’s population lives below the poverty line. Lack of financial investment of the government in social sectors, a high inflation rate and an ongoing broader economic crisis, have increased the vulnerabilities of families and children. Insecurity and conflict continue to displace millions of people. Extreme climatological trends, exacerbated by climate change, have powerful consequences on nutritional status, including droughts and floods; loss of agricultural production and household income; and food price rises.
In 2021, UNICEF and partners continue combining efforts to prevent and treat malnutrition to contribute to Sustainable Development Goal (SDG) Two: end hunger, achieve food security and improve nutrition and sustainable agriculture.
7 Black, RE, Allen, LH, Bhutta, ZA et al. 2008. Maternal and Child Undernutrition: Global and regional exposures and health consequences. 8 Lancet Series on Nutrition, Maternal and Child Undernutrition, 2013.

8
Figure one: areas in Sudan where children are suffering from global acute malnutrition (top) and severe acute malnutrition (below). Especially, the eastern states (Kassala, Red Sea) are affected as well as the Darfur states.

9
©U
NIC
EF
Su
dan
/Bo
s
A child received therapeutic food and care In a stabilisation centre in Abu Shouk IDP camp in North Darfur.
10
RESULTS
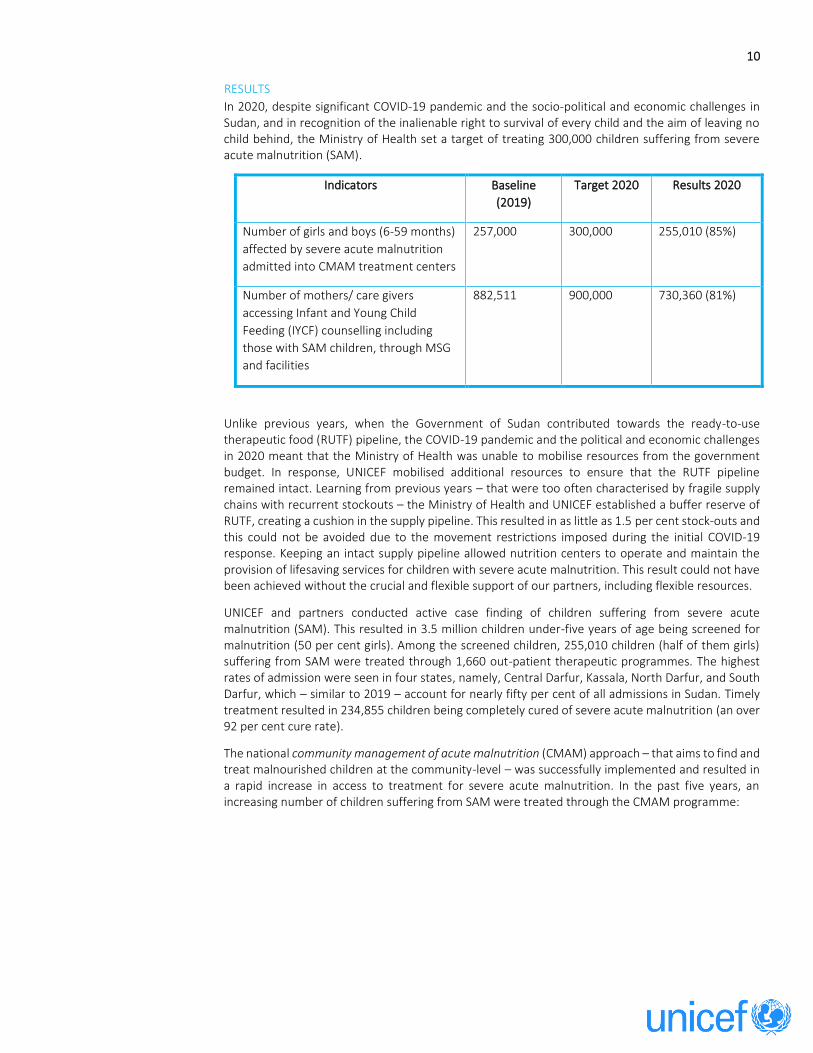
In 2020, despite significant COVID-19 pandemic and the socio-political and economic challenges in Sudan, and in recognition of the inalienable right to survival of every child and the aim of leaving no child behind, the Ministry of Health set a target of treating 300,000 children suffering from severe acute malnutrition (SAM).
Indicators Baseline
(2019)
Target 2020 Results 2020
Number of girls and boys (6-59 months)
affected by severe acute malnutrition
admitted into CMAM treatment centers
257,000 300,000 255,010 (85%)
Number of mothers/ care givers
accessing Infant and Young Child
Feeding (IYCF) counselling including
those with SAM children, through MSG
and facilities
882,511 900,000 730,360 (81%)
Unlike previous years, when the Government of Sudan contributed towards the ready-to-use therapeutic food (RUTF) pipeline, the COVID-19 pandemic and the political and economic challenges in 2020 meant that the Ministry of Health was unable to mobilise resources from the government budget. In response, UNICEF mobilised additional resources to ensure that the RUTF pipeline remained intact. Learning from previous years – that were too often characterised by fragile supply chains with recurrent stockouts – the Ministry of Health and UNICEF established a buffer reserve of RUTF, creating a cushion in the supply pipeline. This resulted in as little as 1.5 per cent stock-outs and this could not be avoided due to the movement restrictions imposed during the initial COVID-19 response. Keeping an intact supply pipeline allowed nutrition centers to operate and maintain the provision of lifesaving services for children with severe acute malnutrition. This result could not have been achieved without the crucial and flexible support of our partners, including flexible resources.
UNICEF and partners conducted active case finding of children suffering from severe acute malnutrition (SAM). This resulted in 3.5 million children under-five years of age being screened for malnutrition (50 per cent girls). Among the screened children, 255,010 children (half of them girls) suffering from SAM were treated through 1,660 out-patient therapeutic programmes. The highest rates of admission were seen in four states, namely, Central Darfur, Kassala, North Darfur, and South Darfur, which – similar to 2019 – account for nearly fifty per cent of all admissions in Sudan. Timely treatment resulted in 234,855 children being completely cured of severe acute malnutrition (an over 92 per cent cure rate).
The national community management of acute malnutrition (CMAM) approach – that aims to find and treat malnourished children at the community-level – was successfully implemented and resulted in a rapid increase in access to treatment for severe acute malnutrition. In the past five years, an increasing number of children suffering from SAM were treated through the CMAM programme:

11
Figure two: SAM admission trend in the period 2010 to 2020
The increase in admission and cure rate, despite a challenging year, could be attributed to UNICEF’s doubled efforts to support the out-patient therapeutic feeding programme, for example by keeping the ready-to-use therapeutic food (RUTF) pipeline intact.
UNICEF procured a total of 7,000 metric tons (504,000 cartons) of ready-to-use therapeutic food (RUTF). RUTF is a peanut-butter paste with essential minerals and vitamins that helps children suffering from severe acute malnutrition to regain their strength. UNICEF also managed to secure supplies, including medication, for both outpatient therapeutic feeding programme centers and stabilisation centers. UNICEF is supporting a diet diversity project in Kassala, in collaboration with the State Ministry of Agriculture and State Ministry of Health and partners. Initiatives have been adopted and a series of awareness raising, and training sessions were conducted. Through demonstrations and discussions, mothers were taught about the importance of adequate nutrition, dietary diversity and the health implications of an inappropriate diet. The trainings involved practical demonstrations on how to cook balanced meals while maintaining their best nutritional value. Women were also taught on how to do home gardening. Those sessions have been conducted in 40 communities with full support from the established mother support groups. Field observations reflected that food and nutritional security for those communities were enhanced through improved access and quality of food. Many cultural practices undermine good nutrition, including limited knowledge of undernutrition, lack of time for care and poor education levels among mothers. Therefore, UNICEF and partners provided 730,360 mothers with information on infant and young child feeding (IYCF). These mothers now have improved knowledge and skills on issues like exclusive breastfeeding, appropriate complementary feeding, feeding of sick children and hygiene during feeding. The network of 7,700 mother support groups (with an average of ten members per group) greatly improved community-based nutrition interventions. The mother support groups were able to conduct initial screenings of children with severe acute malnutrition and referred these children to nutrition centres in their communities. They also promoted exclusive breastfeeding and provided peer support for mothers of children discharged from nutrition centres. To enhance the efficiency of the community management of acute malnutrition (CMAM) programme in improving supply chain management, UNICEF also contributed to supporting evidence generation and supported a detailed review of the supply chain for nutrition commodities. The review’s recommendations will be implemented in 2021 and will focus on improving the current supply chain management system (for example, improving the stock reporting system, identifying and addressing capacity gaps for supply chain management) as well as long-term recommendations to include nutrition supplies within the national medical supply fund system. Recognising the need for delivery to end users (beneficiaries), UNICEF supported improvements in warehousing and logistics support for the timely delivery of ready-to-use therapeutic food to states and villages.
47
,65
9
76
,12
0
10
2,0
09
12
2,9
19
13
6,8
38
16
7,1
78
22
4,5
17
22
7,4
19
24
4,7
96
25
7,0
00
25
5,0
10
2 0 1 0 2 0 1 1 2 0 1 2 2 0 1 3 2 0 1 4 2 0 1 5 2 0 1 6 2 0 1 7 2 0 1 8 2 0 1 9 2 0 2 0

12
PARTNERSHIPS UNICEF continued its fruitful partnership with the Government of Sudan, non-governmental (NGO) partners and sister UN agencies to enhance the joint response to malnutrition in Sudan.
UNICEF, WFP and the World Health Organisation (WHO) worked closely and in a complementarity manner to finalise the Simple, Spatial Survey (S3M-II) micronutrient analysis, ensuring:
▪ Functionality of the Scaling-Up Nutrition (SUN) related UN network. ▪ Support of the CMAM evaluation. ▪ Development of nutrition related guidance/operational guidelines (including COVID-19 related). ▪ Management of SAM children with cholera.
Further, UNICEF is working on the following joint initiatives: Micronutrient supplementation of the social behaviour change communication strategy and Zero Hunger strategy. The strategy was developed to promote food fortification and the objective was to raise community awareness on the importance of fortified food and increase demand and consumption, it also aimed to build capacity of service providers on food fortification. The Zero Hunger strategy review (2017 - 2030) is conducted to address determinants of hunger in Sudan, with the aim to help the Government and Sudan and partners to formulate effective and viable complementary and supplementary programmes and plans for realisation of ‘zero hunger’ in Sudan by 2030. The review has focused on five targets of Sustainable Development Goal 2 (stop hunger and access to food; nutrition; agricultural productivity and income of small-scale food producers; food production systems and agricultural practices; and genetic diversity).
UNICEF developed CMAM site mapping, which is providing detailed information on service delivery sites including out-patient therapeutic programmes (OTPs) led by UNICEF, therapeutic supplementary feeding programmes (TSFP) led by WFP, and stabilisation centers for SAM cases with medical complications led by UNICEF and WHO.
UNICEF and WFP are working to launch the joint global initiative of ‘complementary feeding bowl’, which will improve complementary feeding practices with the involvement of WHO. UNICEF and UNHCR continued their collaboration in addressing the health and nutrition needs for refugees over all Sudan. Together with UN sister agencies, UNICEF supported the development of the 2019-2022 universal salt iodisation memorandum of understanding (MoU) and the activation of the ‘universal salt iodisation’ committee, aiming to improve the status of iodised salt production.
Other critical partners have included the European Union, the Governments of Canada, Germany, Japan, Sweden, the United Kingdom, the United States, humanitarian pooled funds – the Central Emergency Reserve Fund and Sudan Humanitarian Fund. UNICEF also launched a partnership with private sector companies, aiming to address the underlying causes of malnutrition and aiming to improve the health and nutrition status of children and women.
UNICEF is also scaling-up its partnership with key national non-governmental organisations (NGOs) such as Almanar, Anhar, Patient Helping Fund, Maarif, CAFA, WAAD, National Initiative Development Organisation (NIDO), Operation for Development and Seaker, as well as International NGOs such as American Refugee Committee, Concern, Islamic Relief Worldwide, Relief International Save the Children, and World Relief. Currently UNICEF has 28 partners (9 international and 19 national) working in health and nutrition interventions. All partners are delivering integrated health and nutrition projects as well as further integration with water, sanitation and hygiene (WASH) and communication for development (C4D). NGO partners reported very good performance indicators as per the Sphere standards.
EVIDENCE GENERATION UNICEF has the led the process in taking the recommendations of the supply chain review forward, in term of improving supply chain management at all levels. This includes: proper forecasting, timely procurement, proper timely preposition for all nutrition supplies specially for the areas affected by seasonal floods, proper transportation conditions, improving warehousing conditions, stock tracking and reporting, capacity development of key stockholders on proper supplies management. UNICEF

13
supported the re-launching of the CMAM evaluation field work once the movement restrictions related to COVID-19 were lifted. The evaluation will provide the needed guidance on the way forward regarding CMAM roadmap and acceleration plan for prevention and response to wasting.
The Simple Spatial Survey Method (S3M II) report was finalised and published. The report provides the needed multi-sectoral information to guide evidence-based planning. In addition, the micronutrients analysis component under S3M II was carried-out and provides critical information on nutrition status in Sudan.
CHALLENGES ▪ Sudan’s challenging context remains, with the fragility of the health system, the sharply deteriorating
socioeconomic-political situation with lack of fuel and cash, together with the progressive high inflation rates and disease outbreaks. All of this was exacerbated by the COVID-19 pandemic and the unprecedented flooding in all states.
▪ No children were reached with doses of vitamin A in 2020. Only one round of ‘national immunisation days’ were implemented towards the end of the year. However, the intention is for vitamin A doses to be given together with the second round of NIDs, at the beginning of 2021.
▪ The country is currently undergoing an important transition from a military rule to a civilian one. The transition itself has posed some challenges on programme implementation. The government has undergone a reshuffling of its leadership in the different line ministries. The federal and state ministries, being among those affected, have a new set of leadership officials posing a challenge on the pace of programme implementation. UNICEF continues to build on the capacity of the Ministry of Health on nutrition, and advocates with the Government of Sudan for increased commitment and contribution to critical programmes like the community-management of acute malnutrition (CMAM).
▪ The monitoring and data reporting system remains a challenge when it comes to data quality and timelines, however, UNICEF is working with governmental and non-governmental partners to investigate ways to find solutions to this challenge. For example, UNICEF supported the Federal Ministry of Health to build the capacity of 36 state-level monitors on proper monitoring and the use of checklists. Furthermore, UNICEF is providing the needed support to partners to conduct regular field monitoring visits to strengthen the quality of service provision.
▪ Most of the contributions UNICEF Sudan receives for nutrition are humanitarian (short-term) funds, which are less suitable/effective in addressing the underlying causes of malnutrition.
▪ Cultural and behavioural practices, which hinder communities from adopting proper feeding practices for mothers and children. Also, early marriage and childbirth, which jeopardises the health of mother and child. UNICEF supported the Federal and State Ministries of Health to expand the mother support group cadre to strengthen the provision of information on optimal infant and young children feeding practices. So far 7,700 mother support groups were established in comparison with 3,500 groups in 2019. Furthermore, simple, practical, and context-specific information as made available through different communication channels (digital, broadcast, social media, radio, television load speakers) to contribute to address the cultural and behavioural challenges.
LESSONS LEARNED ▪ Early actions taken to mitigate the impact of COVID-19 on lifesaving health and nutrition interventions
proved to be effective. UNICEF and partners worked with the Ministry of Health and reviewed service guidelines to enable safe delivery of nutrition services in Sudan. This was followed by massive capacity-building activities, equipping health and nutrition care providers with necessary skills to deliver services in the context of COVID-19. Furthermore, nutrition services extended to COVID-19 treatment centres in several states, to allow for continuation of nutrition support even when caregivers are affected by the disease. These early actions have helped maintain high coverage of nutrition service, with minimal impact on results achieved compared to 2019.
▪ Community participation and involvement is crucial for improving maternal and child health and children’s nutrition status. The ‘diet diversity’ project – which allowed communities to identify their nutrition needs – implemented in Kassala state was a real example of successful community collaboration to improve child nutritional status. Encouraging not only participation but also community leadership was the element of success to this project. In 2020, mother support groups in

14
the Kassala state promoted diet diversity through cooking demonstrations and home gardening interventions, which is a step forward to improving the nutrition status of mothers and children.
▪ Parents of children suffering from severe acute malnutrition were engaged in mid-upper arm circumference (MUAC) screening and follow-up. This reduced the risk of COVID-19 infection as parents were now able to screen their children themselves in their home-setting. Besides mothers, UNICEF also started engaging fathers in health and nutrition matters affecting their children. For example, both mothers and fathers were provided with counselling services on community management of acute malnutrition, infant and young child feeding practices (special men to men sessions), and common health concerns and diseases affecting the lives of children and their family members.
▪ The establishment of a buffer reserve of ready-to-use therapeutic food (RUTF) continued to be crucial for creating a cushion in the supply pipeline that allowed ensuring close to zero stock-outs. Further, UNICEF stepped in to provide out-patient treatment programmes (OTPs) with essential drugs, which allowed health centres to operate and maintain the provision of lifesaving services for children with severe acute malnutrition and was reflected in increased admission numbers and improvement in the cure rates.
▪ It was necessary for UNICEF to step-in and provide operational, technical and financial support for eleven stabilisation (in-patient) centres in Darfur. After ensuring sound institutional and technical capacity, UNICEF has handed over those facilities to the Government of Sudan at the end of 2020. However, UNICEF will continue providing technical and supply support and lobby to engage other partners to support the stabilisation centres. This support leads to increased admission rates and quality of services (the total admissions in the eleven stabilisation centers represents 65 per cent from the total in-patient admission of SAM cases across the Darfur states, with a cure rate of 94.9 per cent). However, there remains a need to ensure greater accountability to stabilisation centres by hospital management and state-level authorities to ensure their sustainability.
▪ Regular sub-national nutrition coordination meetings improved state-level coordination. Yet, coordination needs to be strengthened even more to allow for joint planning and integrated interventions, which are crucial for achieving durable impact. In addition, monitoring, reporting and functioning data systems are essential for strengthening the health system. Those aspects clearly need to be improved and to be integrated within one health system.
▪ Timely delivery of procured quantities of nutrition supplies is necessary to avoid any risk of stock-out.
FUTURE WORK PLAN In 2021, UNICEF will continue enhancing its strategic partnerships and technical cooperation with a wide range of stakeholders including the Global Fund, sister UN agencies (OCHA, WHO, UNFPA, UNHCR, WFP) to deliver services, and will continue developing partnerships with non-governmental and civil society organisations in the most hard-to-reach areas to scale-up integrated lifesaving health and nutrition interventions.
The year 2021 will be transformational for the new leaders and staff in the Ministry of Health at national and state-level, after a challenging 2020. UNICEF will support the transitional Government of Sudan in strengthening monitoring and data management systems to improve the quality of services. Further, UNICEF will continue its work with the State Ministries of Health on strengthening the supply chain management at all levels. UNICEF will also continue advocating for increased government contributions to essential health and nutrition interventions and supplies.
UNICEF and partners will strengthen social mobilisation interventions for community participation and demand creation. This includes scaling-up diet diversity related interventions and adopting additional mechanisms to prevent supply leakages. Further, UNICEF and partners will work on strengthening multi-sectoral integration and coordination at all levels, including joint planning and prioritisation, as well as geographical convergence.
UNICEF will continue working on improving the quality of the community management of acute malnutrition (CMAM) programme, as well as on strengthening active case finding and improving referral pathways. UNICEF will support the Government of Sudan to develop and update strategies

15
and road maps for infant and young child feeding (IYCF) and CMAM programmes as well as advocating for establishing a routine system for vitamin A supplementation for children under-five.
Given that 65 per cent of the Sudanese population are under 25 years of age, getting things right for children, adolescents and youth in the immediate and longer term, will to a great degree determine how successful Sudan will be in the future. Urgent action is needed to make a critical difference in the most vulnerable children’s lives in the next months, and years to come.

16
CASE STUDY: DIET DIVERSITY The prevalence of stunting among children under-five years of age in Sudan has reached 36.4 per cent, with 16 per cent severely stunted and 20.4 per cent moderately stunted, affecting approximately 2.8 million children under-five in Sudan. Diet diversity and stunting Poor diet diversity constitutes one of the key drivers for stunting, with children surviving on limited poorly diversified meal options. As per S3M II results, Kassala state was ranked as one of the states with highest rates of stunting in Sudan (coming fourth after North Darfur, Gedaref and Red Sea states). When comparing stunting rates and the diversity of a child's diet, the S3M II results revealed a negative association between stunting rates and diet diversity. The less diversified the food is, the higher stunting rates will be. In Kassala, with only one quarter of children receiving adequately diversified food, almost 44 per cent of children are stunted. Key determinants of stunting in Kassala include poor complementary feeding practices and poor diet diversity with an average of 16.3 per cent of children receiving the minimum acceptable diet. Moreover, only 3.4 per cent consume plant sources of vitamin A
Diet diversity project: a multi-sectoral collaboration The Ministry of Health, UNICEF and partners in Kassala came together and identified ‘diet diversity’ as an area for multisectoral collaboration. The state of Kassala took the initiative to address this problem by working with existing mother support groups to improve dietary diversity status of their children. Objectives
▪ Raise awareness of mothers on optimal infant and young children feeding practices and the importance of diet diversity on the growth of their children.
▪ Empower women to produce nutritious foods through home gardening. ▪ Build capacity of mothers on preparation of diversified nutritious diets. ▪ Enhance collaboration and coordination between different sectors
Project implementation The initiative was implemented in 40 communities including the small village of Wood in Khashm El Girba locality of Kassala state. The name of the village (meaning ‘compassion’) characterises the community, as the people living in the village were known for their high spirit of compassion and support for one another.
Figure three: comparison between Stunting and Diet Diversity States' results - S3MII 2018 Sudan

17
UNICEF in collaboration with Kassala’s State Ministry of Health and Ministry of Agriculture, conducted a training on dietary diversity, which included the importance of dietary diversity, practical cooking demonstrations of balanced meals, and practical demonstrations of growing vegetables at home.
Mothers take action A few months later, the results of the community capacity-building efforts were very evident as witnessed by Somaia Hammad, a member of the mother support group in Wood village. Somaia who is a mother of two children, was trained on dietary diversity, food preparation and home gardening. She was inspired by the training and became very active and enthusiastic to the level that she took the initiative to grow some vegetables in the back yard of her house. Later, Somaia became a role model in her community, and other mothers were inspired and learned from her. Somaia said ‘We greatly benefited from this training; our diet has diversified. In the past we did not eat the purslane plant, but now it’s part of our diet and my family enjoys it. Also, we did not like pumpkins in the past, but cooking pumpkins using this new way (‘madida’) is very delicious, and we like it.’ Having been a true witness of the benefits of this training, Somaia invited other mother support groups to witness her success and many women followed her lead.
So far, 290 mothers established home farms in 40 communities. Out of them, 133 mothers started the harvesting of their home-grown crops. Field observations reflected that food and nutritional status for those families has been enhanced through improving access to and quality of food. Evidence has shown that a diet comprising at least four food groups a day is associated with improved growth in young children. Introducing children to healthy and diverse foods at an early age also helps to establish taste preferences and good eating habits later in life. Lessons learned The effective engagement of key stakeholders from the early stages (government and non-government, communities) played an important role in moving this initiative forward. Somaia’s leading role also proved than just one person can start a movement. Mother support groups at community-level, are an effective platform for addressing stunting and other child nutrition issues.

18
Communities are capable of contributing to achieve desired SDGs results. They are open, eager and willing to learn, implement and lead successful community health and nutrition initiatives. Multi-sectoral collaboration (for example with WASH) is a key for rapid success. It allows for quick wins through combing different expertise in a child-centered approach.
STORY: IT TAKES A VILLAGE TO RAISE A CHILD
Over the past decades, Kassala State, in Eastern Sudan has faced a persistent nutrition crisis, with increasing stunting rates affecting an estimated 44 per cent of children under-five years of age. Malnutrition is largely caused by poor water and sanitation conditions, high disease prevalence, increased food costs, poverty, and lack of food variety and essential nutrients. Inadequate complementary feeding practices and poor dietary diversity are among the key determinants of stunting in Kassala, with only 16.3 per cent of children receiving the minimum acceptable diet.
Hamid Nagmos, 50 years old, holds his grandchild, as a health worker takes his mid-upper arm circumference (MUAC) measurements that show if a child is malnourished, in Abu Dahan village in
Kassala, the capital of the state of Kassala in Eastern Sudan.
UNICEF Sudan, in collaboration with the Federal Ministry of Health, works to treat and prevent malnutrition in Sudan through the provision of both nutrition specific interventions such as the treatment of severely malnourished children, micronutrient supplementation, counselling on good infant and young child feeding and care practices as well as nutrition sensitive interventions including vaccinations.

19
While Hamid Nagmos, 50 years old, holds his grandchild, a health worker checks vitals of the child in Abu Dahan village in Kassala, the capital of the state of Kassala in Eastern Sudan.
With help from Hamid Nagmos, the grandfather of the child, a health worker weighs the child in Abu Dahan village in Kassala, the capital of the state of Kassala in Eastern Sudan.

20
With help from Hamid Nagmos, the grandfather of the child, a health worker weighs the child in Abu Dahan village in Kassala, the capital of the state of Kassala in Eastern Sudan.
With help from Hamid Nagmos, the grandfather of the child, a health worker measures child's height in Abu Dahan village in Kassala, the capital of the state of Kassala in Eastern Sudan.
For more stories, please check UNICEF Sudan’s website: stories
Awab receives treatment in Otash camp.

21
EXPRESSION OF THANKS UNICEF Sudan would like to extend its heartfelt appreciation to all donor partners who continued to support us or even scaled-up their support during 2020. It was not an easy year, yet UNICEF and partners reached millions of girls and boys with (often) lifesaving interventions, which would not have been possible without the generous funding received. Thanks to the support, UNICEF can continue its mission to meeting the needs and fulfilling the rights of the most vulnerable children, their families and communities. Thematic or flexible funding for UNICEF’s health interventions is crucial as it provides us with greater flexibility to respond to the needs of children in a timely, well-planned and efficient manner. It allows us to have a bigger and more effective impact on the lives of vulnerable and marginalised populations in a highly volatile, complex and dynamically evolving context like Sudan.
FEEDBACK FORM UNICEF is working to improve the quality of our reports and would highly appreciate your feedback.
The form is available on line at this link: English version or French version.

22
FINANCIAL ANALYSIS TABLE ONE: Planned health and nutrition budget for 2020 (in US dollars)
Output Source of funds Planned budget for 2020 Funded Shortfall
Output 1.3 Severe Acute Malnutrition
RR 1,000,000 357,394 642,606
ORR 3,834,045 376,009 3,458,036
ORE 36,979,649 14,183,695 22,795,954
Total Total 41,813,694 14,917,098 26,896,596
TABLE TWO: Thematic contributions received for nutrition in 2020 (in US dollar)
Donors Grant Number* Contribution Amount
Programmable Amount
SIDA - Sweden SC189903
521,003 484,533
Total
521,003
484,533
TABLE THREE: Thematic expenses for nutrition in 2020 (in US dollars)
Row Labels Expense
Other Resources - Emergency 10,555
21-04 Prevention of stunting and other forms of malnutrition 428
21-05 Treatment of severe acute malnutrition 10,127
Other Resources - Regular 439,796
21-04 Prevention of stunting and other forms of malnutrition 40,256
21-05 Treatment of severe acute malnutrition 399,540
Grand Total 450,351
TABLE FOUR: Expenses for nutrition in 2020 (in US dollars)
Row Labels Expense
Other Resources - Emergency 22,444,253
21-04 Prevention of stunting and other forms of malnutrition 461,971
21-05 Treatment of severe acute malnutrition 21,982,282
Other Resources - Regular 1,120,243
21-04 Prevention of stunting and other forms of malnutrition 607,493
21-05 Treatment of severe acute malnutrition 512,750
Regular Resources 862,231
21-04 Prevention of stunting and other forms of malnutrition 45,619
21-05 Treatment of severe acute malnutrition 816,612
Grand Total 24,426,727

23
TABLE FIVE: Expenses by specific intervention codes in 2020 (in US dollars)
Row Labels Expense
21-04-01 Breastfeeding protection, promotion and support (including work on Code)
324,952
21-04-02 Diet diversity in early childhood (children under 5), includes complementary feeding and MNPs
48,367
21-04-03 Vitamin A supplementation in early childhood (children under 5) 143,486
21-04-05 Maternal nutrition, including information, supplementation and counselling
58,444
21-04-06 Salt iodisation and other large-scale food fortification 14,071
21-04-07 National multisectoral strategies and plans to prevent stunting (excludes intervention-specific strategies)
6,099
21-04-08 Data, research, evaluation, evidence generation, synthesis, and use for prevention of stunting and other forms of malnutrition
276,930
21-04-99 Technical assistance - Prevention of stunting and other forms of malnutrition
85,266
21-05-01 Care for children with severe acute malnutrition 19,609,176
21-05-02 Capacity building for nutrition preparedness and response 1,647,325
21-05-03 Nutrition humanitarian cluster/humanitarian sector coordination 12,345
21-05-04 Data, research, evaluation, evidence generation, synthesis, and use for SAM and nutrition in emergencies
26,459
21-05-99 Technical assistance - Treatment of severe acute malnutrition 198,385
Grand Total 22,451,305
TABLE SIX: Planned nutrition budget for 2021 (in US dollars)
Output RR OR ORE Grand Total
Output 1.3 Severe Acute Malnutrition 0.00 0.00 23,965,000 23,965,000
Total Budget 0 0 23,965,000 23,965,000
All expenses are provisional and subject to change.

24

25
Contact Address Saja Abdullah
Deputy Representative a.i.
Email: [email protected]
UNICEF Sudan P.O Box 1358, Khartoum, Sudan

26
United Nations Children’s Fund
Sudan Country Office
PO Box 1358
Gerief west [Manshiya],
First District H, Plot 6/3
Telephone: +249 (0) 156 553 670
Facsimile: +249 (0) 183 587 741
www.unicef.org/sudan
© United Nations Children’s Fund
(UNICEF)
United Nations Children’s Fund
Sudan Country Office
PO Box 1358
Gerief west [Manshiya],
First District H, Plot 6/3
Telephone: +249 (0) 156 553 670
Facsimile: +249 (0) 183 587 741
www.unicef.org/sudan
© United Nations Children’s Fund
(UNICEF)