1 talking with patients after a medical error: what to do? what to say? julie crosson, md, evans...
TRANSCRIPT
1
Talking with Patients after a Medical Error:
What to do? What to say?
Julie Crosson, MD, Evans Educator Communication SkillsThomas Barber, MD, Evans Educator, Department of Medicine
ML Hannay, M.Ed., Communication & Leadership Specialist
Medicine Grand Rounds, January 6, 2012Boston University School of Medicine
Thank you to The American Academy on Communication in Healthcare, and toDr. Robert Truog, Exec. Dir. Institute for Professionalism and Ethical Practice, HMS
2
Disclosure
I have made medical errors that affected patients.
3
Why a grand rounds on errors?
1. Increase patient trust
2. Decrease doctor isolation and burnout
3. Improve patient safety by talking to colleagues about errors to improve safety outcomes
4
Overview
1. Present case of a medical error
2. Review current data on “Disclosure Gap”
3. Identify benefits and barriers to disclosure and apology
4. Review steps for talking about medical errors with patients and families
5. Reflect on the case
5
Case presentation• 66 yr old man with complex PMH admitted to
medical service in May 2011 for nausea and abdominal pain.
• History of IDDM, CAD s/p CABG and AVR for AS, CVA, PVD, OSA, HTN, hyperlipidemia, anxiety, COPD w 50 pack-year tobacco history
• On 27 medications• Retired, worked unloading trains; lives w
daughter and wife
6
History and Exam• Admitted for ? CVA vs. TIA 3/10. Since then, c/o
persistent nausea, burping, bloating and epigastric pain w/o vomiting. No change in diet or appetite. Normal BM. Confused about meds.
• VS: 197/115, 88, 20 (O2 sat 95% RA) Afebrile• Not acutely ill but uncomfortable. RRR S1S2
normal, 3/6 systolic ejection M, lungs clear, abd w active BS, soft, nondistended, nontender
• Labs: WBC 5.7, hgb 12.5, lytes normal, Gluc 266, amylase, LFTs, cardiac enzymes normal.
7
Imaging• KUB moderate amount of stool, no
obstruction.
• CT abd/pelvis: no obstruction. Cholelithiasis, colonic diverticula w/o diverticulitis, rim enhancing splenic lesion likely hemangioma, oval soft tissue mass in RLL adjacent to the esophagus.
8
Impression• Probable diabetic gastroparesis. He had been
prescribed metaclopromide but was unsure if he was taking this. – Metaclopromide, ondansetron, simethicone given– Control of hyperglycemia– Gastric emptying scan as outpatient– Lactose free diet
“Other issues per house staff. We will try to simplify his complex regimen but defer major decisions to his new PCP and his cardiologists.”
9
Outcomes• Pt discharged after 36 hours, ? improved.• Frequent visits with PCP, endocrinology,
cardiology over the summer• Gastric emptying scan normal. • 23 lb unexplained weight loss between May and
September 2011: Weight loss w/up, including CXR 9/7 normal.
• 9/21/11 PCP paged me: “did you know about the mass in the RLL? It’s documented in the admit note and in the DC summary that this needed f/up. I didn’t know about it till today.”
10
Readmitted to hospital• Pt readmitted to my service 9/21/11 for
urgent w/up. • CT chest w IV contrast: “interval growth of
the RLL spiculated, centrally necrotic soft tissue mass adjacent to the esophagus, now with possible invasion into the esophageal wall. Findings very suspicious for cancer.”
• Metastatic work up initiated.
11
If you were Tom…
• What do you think you should do or say?
• What do you think you would do or say?
• What would your feelings/emotions be?
12
What does a patient want/expect?
• If this occurred to your father/brother, how would he feel?
• What would he want/expect the doctor to do or say?
13
Doctors’ Emotions
Dread
Fear of Punishment (sued)
Isolation
Guilt/Shame (harming a pt)
Anger (poor system set them up)
Powerlessness
Worry (job, reputation)
Self-doubt
“The Second Victim”Wu AW BMJ 2000;320:726-7
Patients’ Emotions
Dread
Fear (retribution form HCWs)
Isolation
Guilt (family: feel they didn’t keep close enough watch on the pt)
Anger
Powerlessness
Worry
NEJM 2007
14
OLD LADY
15
The Recent History of Medical Errors
IOM report 1999: ‘To Err is Human’
– 98,000 deaths/year due to medical errors
– Hospital Safety Movement, systems-based changes: EMR, procedure check lists
– ACGME competencies include quality improvement and improving patient safety
16
Definitions A Medical Error : Failure to complete an action as intended, or the use of a wrong plan to achieve an aim. May or may not result in adverse outcome.
Unanticipated Outcome: A result that differs significantly from what was anticipated.
Omission: Something left undone, neglect of duty.
- Institute or Medicine, To Err is Human 1999- Webster Dictionary
17
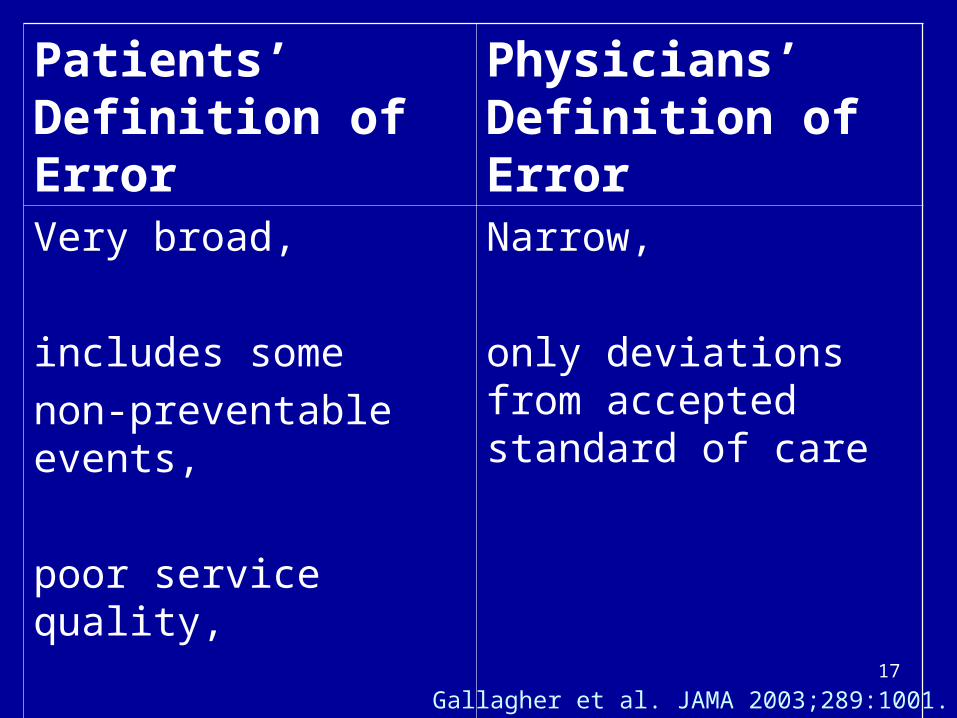
Patients’ Definition of Error
Physicians’ Definition of Error
Very broad,
includes some
non-preventable events,
poor service quality,
poor communication
Narrow,
only deviations from accepted standard of care
Gallagher et al. JAMA 2003;289:1001.
18
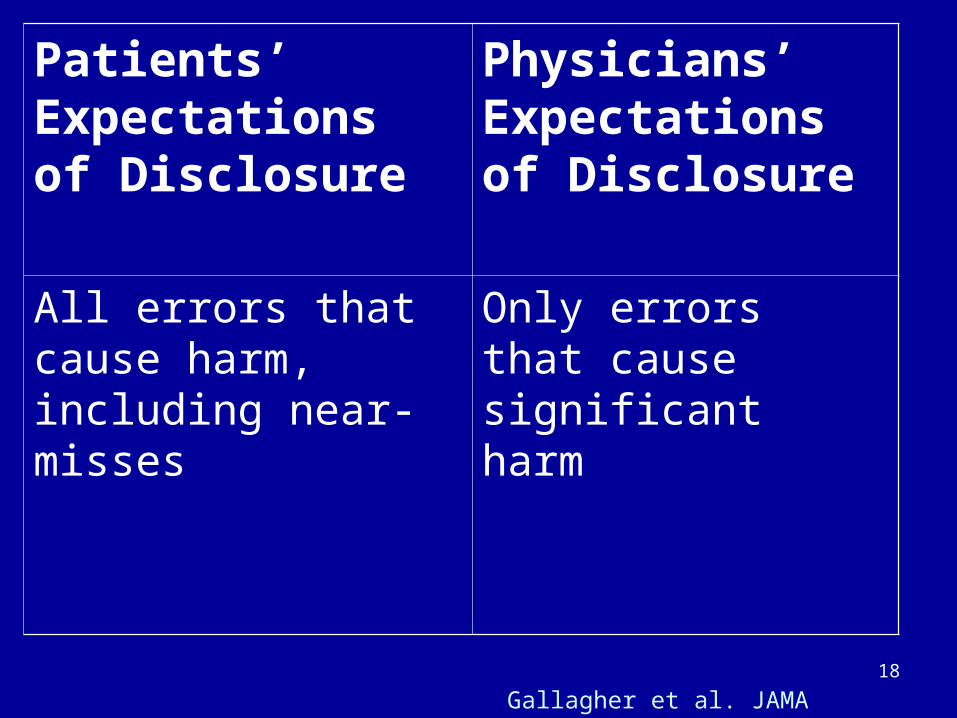
Patients’ Expectations of Disclosure
Physicians’ Expectations of Disclosure
All errors that cause harm, including near-misses
Only errors that cause significant harm
Gallagher et al. JAMA 2003;289:1001.
19
Disclosure GAP
90% of Doctors support
the principle of disclosure
but
Only 30% actually do disclose
20
Barriers to Disclosure
- Skeptical of benefits
- Unnecessary distress to patient and family
- Patients unlikely to find out
- Lawsuits
- Lack of training in error disclosure
NEJM 2004
21
Benefits of Disclosure
• Evidence suggests that skillful conversations and follow-up may reduce the risk of litigation
• Harvard Medical Practice Study only 3-5% of patients injured by negligent care actually sue, NEJM 2004
22
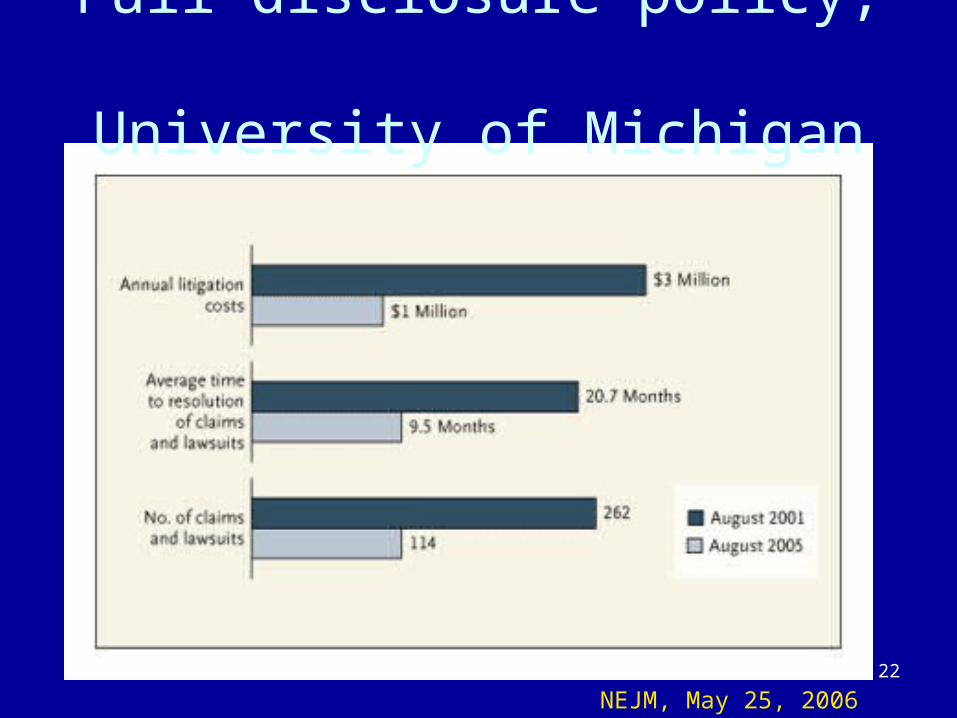
Full disclosure policy, University of Michigan
NEJM, May 25, 2006
23
Benefits of Disclosure
• Staying engaged with patients and restoring trust results in better outcomes for both patients and clinicians
• The right thing to do
Dr. Robert Truog, Institute for Professionalism and Ethical Practice, Harvard Medical School.
24
What Is the Threshold for Disclosure?
“You would want to know about the event, if it had happened to you or a relative, or
It may result in a change in treatment, now or in the future.”
- Dr. Robert Truog, Executive Director
Institute for Professionalism and Ethical Practice,
Harvard Medical School
25
What Information to Disclose
Patients’ Attitudes Physicians’ Attitudes
Tell everythingChoose words
carefully
26
How to Disclose an Error
Patients’ Attitudes Physicians’ Attitudes
Truthfully
Compassionately
Truthfully
Objectively
Professionally
27
Role of Apology
Patients’ Attitudes Physicians’ Attitudes
ExpectedConcerned that
apology creates a legal liability
28
When to Have the Conversation
Patients’ AttitudesPhysicians’
Attitudes
Immediately “When I have all the facts”
29
Back to the case…..
The conversation
30
Next steps
• Primary data collected, information confirmed with PCP
• Evidence of failure to identify very abnormal radiologic finding and to communicate this effectively to PCP
• Requirement to disclose information to patient• Discussion with Risk Management• Stars report• Preparation • Meeting with patient and family• Documentation in record
31
How is our patient now?
• Dx Squamous Cell CA Lung, locally advanced Stage IIIB (T4N1M0), on Gemcitibine protocol
• Tolerating chemo fairly well, but low functional status
• Weight 147 lbs on 1/3/11
32
What are the steps for discussion?
33
What are the steps for discussion?
1. Preparation•Self check-in•Seek assistance from trusted colleague•Review available medical facts•Consult risk management
– page 31-SAFE– Patient Advocate: x4-1778
•Prepare for strong emotions, both from yourself and patient/family
34
2. State What Happened
- Simply
- Slowly
- Avoid medical jargon
- Use pauses
35
3. Apologize
- Focus on patient’s welfare
- “I’m sorry”
36
Two meanings of the words “I’m sorry”
1. Expression of compassion:
“I’m so sorry that this has happened.”
2. Expression of responsibility:
“I gave you the wrong dose. I am truly sorry.”
• The first is always appropriate• The second is appropriate only when it is true
Dr. Robert Truog, Institute for Professionalism and Ethical Practice, Harvard Medical School.
37
How Apologies Fail• “If there was an error…”
• “There was a mistake, but…”
• “The mistake certainly didn’t change the outcome…”
• “Sometimes these things happen…”
Lazare JAMA 2006; 296:1401, Berlinger After Harm. Johns Hopkins, 2005
38
4. Take Responsibility
• Use “I” statements
• Do not blame or speculate
• Do not accept fault unnecessarily
39
5. Assurance
The steps you are going to take to avoid this error occurring in the future
40
6. Invite questions
• 40% of patients stated they wished they had opportunity to ask questions
• “What questions do you have?”
41
7. Make a Follow-up plan
• Discuss together how to meet needs of patient and family
• Plan for next meeting
• Remain accessible
42
8. Document
• Rationale for clinical decisions
• Clinical outcome and plan of care
• Discussion with patient/family– Names/relationships of those present– Questions posed and the answers given
43
9. Debrief
• Back to self check-in
• Discuss with colleague
• Reflection helps us improve
44
The steps for discussion1. Preparation- check-in2. State what happened simply3. Apology4. Take responsibility5. Assurance/Problem Solving6. Invite questions7. Make follow up plan together8. Document9. Debrief
Gallagher, JCOM 2005l12l5:253-259
45
How to take what you know into what you can do
You cannot force yourself to feel something you do not feel
But you can make yourself do right in spite of your feelings
Pearl S. Buck
46
Build on what you already do
• You already use the skills--Giving bad news re: a diagnosis
• Instincts are to show empathy, to tell the truth, to listen to their fears
• Use the relationship building strategies that data shows work to enhance outcomes/compliance
• Build trust prior to as well as after an error
47
Starting the conversation
• Set up—where, when, who?
• 1-1, Doctor/patient , start the conversation 30 seconds
• Debrief patient to doctor, 30 seconds
• What worked/didn’t work?
• Words, Voice Tone/Speed, Non Verbal?
• What % for each (must equal 100%)?
48
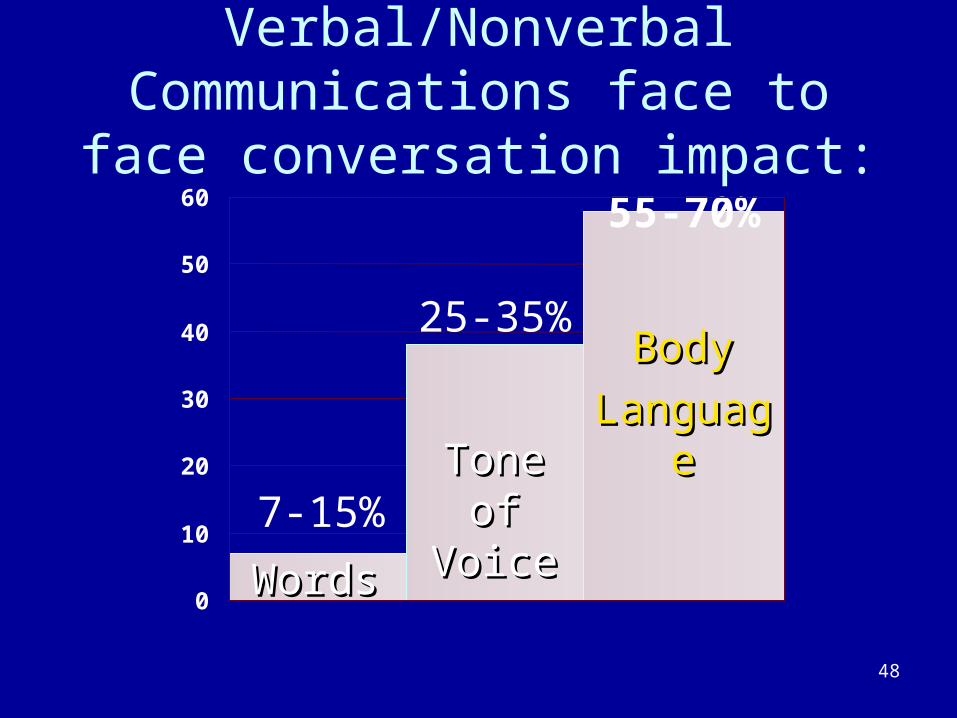
Verbal/Nonverbal Communications face to face conversation impact:
0
10
20
30
40
50
60
7-15%
25-35%
55-70%
WordsWords
Tone of Tone of VoiceVoice
BodyBody
LanguagLanguagee
49
Common Sense
• Is not common practice
• 80% of doing this well is
• Showing up to do it—with behavior that demonstrates your empathy, caring, and concern
50
Authentic Apology: in addition to helping both doctor and patient heal….• …“nothing is more effective in reducing liability
than an authentically offered apology” Michael Woods, MD (Colorado surgeon)
• …my job is much more difficult when doctors fall on the sword….” “The hardest case for me to bring is the case where the defense has admitted error and apologized to the injured patient.” Andrew Meyer, Boston area Medical Malpractice lawyer
51
In summary…• Talking about errors improves our relations with
patients
• Communication skills can be learned and improved with practice
• These conversations are complex and difficult,
use the self check-in and get help
52
What questions
do you have for us?
53
“A stiff apology is a second insult….
The injured party does not want to be compensated because he has been wronged; he wants to be healed because he has been hurt”
- G.K. Chesterson
England 1974-1936
54
Building the Foundation of Trust
• What happens PRIOR to any error matters • Build a solid and positive relationship with the
patient, family members, & your medical team-- prior to any incident
• Patients see selves as equal, as partners/consumers/customers
• Use of internet—assume they have been/will be on it--they know your hospital ratings, errors history, etc.
• Litigation and lack of compliance continues with doctors who don’t apply basic relationship building skills
55
7 Steps to defusing an angry patient/family member
1. Prevention: build trust beforehand
2. Acknowledge feelings/perceptions
3. No interruptions….Let them vent (rule of 3)
4. “Seek first to understand before being understood”….ask open ended questions
5. Offer AUTHENTIC apology
6. NO BLAME NO EXCUSES
7. Solve the problem: offer CHOICES, ALTERNATIVES, FOLLOW UP
56
Future Opportunities :
- Improving support systems for providers
- Improving patient safety via greater transparency
- Professional growth and improving our practice