1 is pharma different from organized crime? who steals more? who kills more? who bribes more? which...
TRANSCRIPT

1
Is Pharma different from organized Crime?
Who steals more?
Who kills more?
Who bribes more?
Which one neutralizes its opponents?
Which one has higher ethical standards?

2
Neutralizing the Naysayers
To silence the voices of leading doctors who speak against drugs:
• Use “task force” to bring over to the other side; neutralize
• Bribe with funding
• Ruin reputation; Discredit
• Gotti is a piker
3
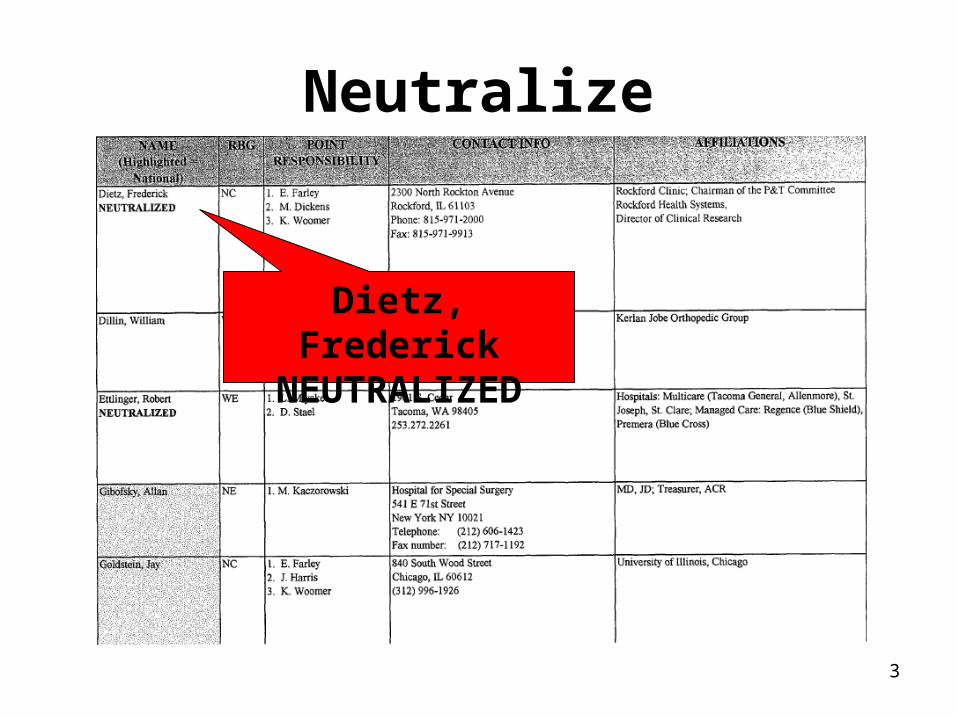
Neutralize
Dietz, FrederickNEUTRALIZED
4
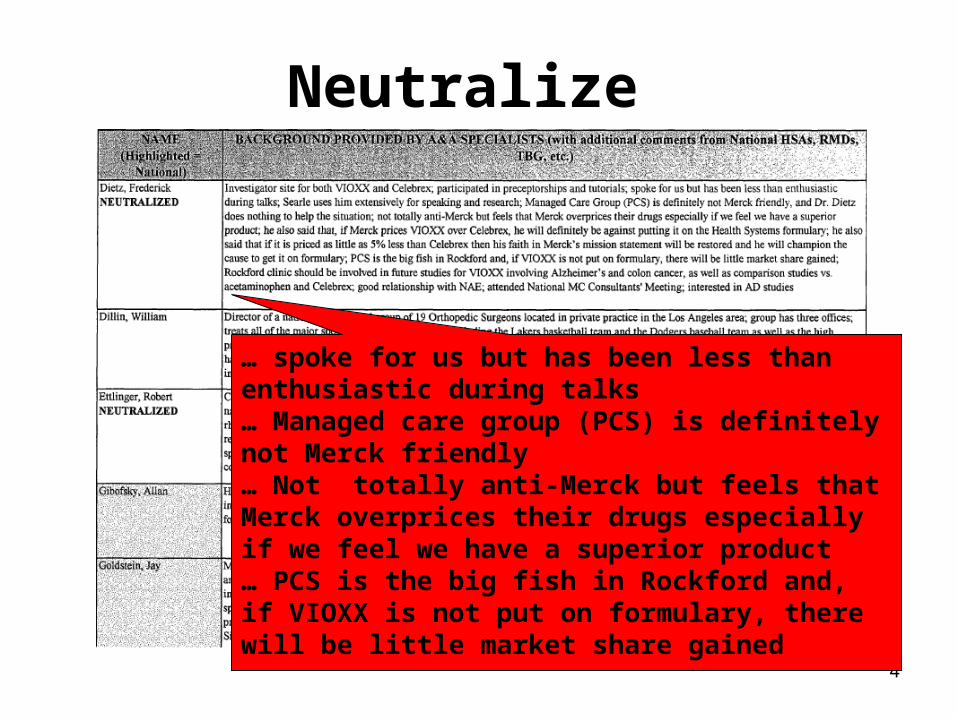
Neutralize
… spoke for us but has been less than enthusiastic during talks… Managed care group (PCS) is definitely not Merck friendly… Not totally anti-Merck but feels that Merck overprices their drugs especially if we feel we have a superior product… PCS is the big fish in Rockford and, if VIOXX is not put on formulary, there will be little market share gained

5
Neutralize
Now an Advocate; clinical trials
6
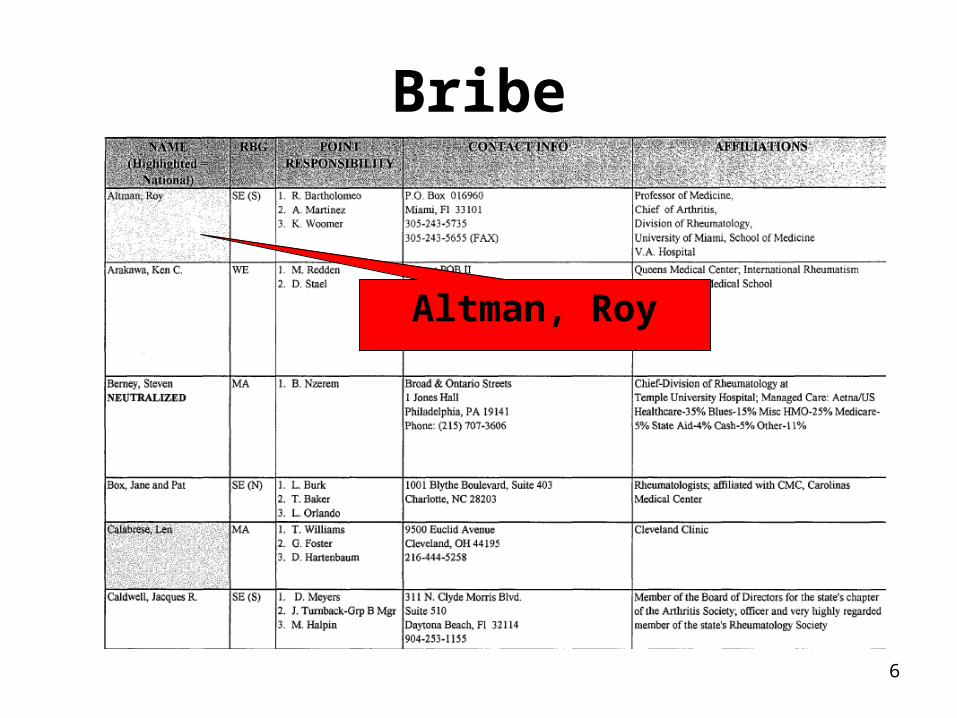
Bribe
Altman, Roy

7
Bribe
… very poor relationship with us, dating back to the early 1980s… a task force has been formed to try and bring him back to neutral in his perception of us… bad feelings from FOSAMAX, but wants to be perceived as non-biased… recommend a brainstorm with local reps, OSRs, and A&A specialists for tactics and may also try Jim Kessinger (past Fosamax launch manager covering Altman) for ideas;Provide OARSE funding every year

8
Bribe
“Show me the money” – Clinical Trials-Funding >$50,000 Rheum Fellowship Program-Task Force to continue to work with him-Task force in place – Dr. Bruce Freundlich, SBD (J.G.) RMD K. Edward, M. Halpin & local reps

9
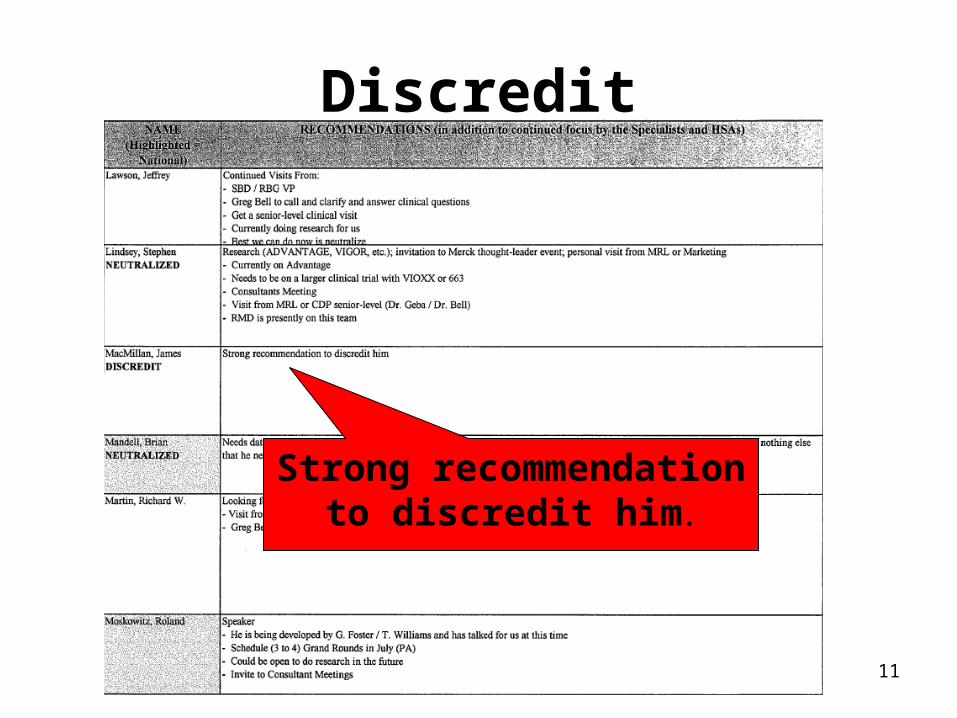
Discredit
MacMillan, JamesDISCREDIT

10
Discredit...speaking extensively for Searle/Pfizer (200 days this year)… numerous reports of biased and inaccurate presentations… gathering information on VIOXX from the Internet… one of Searle’s most frequently used speakers across the nation (and loyally devoted)… loose cannon… no way to win him over and frankly would not want this type of person speaking for my product
11
Discredit
Strong recommendation to discredit him.

12
Is Science different from Religion?
Assuming arguendo that medicine is in part based on science

13
Is Science different from Religion?
We Got RulesWe Got Priests
(high Priests too)We Got Monasteries
We Got BeliefsWe Got Biases
What is the demarcation?
14
WE GOT Cochrane!!!!

15
Cochrane MI Treatment Study
In CCU Home
Deaths 6 8
Red to stop trial Green to continue Yellow for the armadillos

16
‘I showed it to some of the consultants before the meeting and there was an absolute uproar.’
‘that trial is unethical, it must be stopped’.

17
On Bias so I let them go on a bit and blow their
tops, and when they were calming down a bit I apologized that I had shown them the wrong table. I then showed them the correct table, and said didn’t they think it was unethical to continue with coronary care units, but I was unable to convince them . . . it does make the point that there is an enormous amount of emotion about coronary care units.Red if bias different Green to agree Yellow for the armadillos

18
The Big Sellers• Nifedipine• Avandia• Vioxx (celebrex)• Ketek• Vytorin
Why were (are) these big sellers? Think bias.
What else is interesting about these treatments?

19
What’s the Bias?

20
Primum non Nocere A1-c is a surrogate for this endpoint
Just like the Vioxx patients who died without joint pain andThe nifedipine patients who died with normal blood pressure andThe Seldane patients who died without stuffy noses

21
Does this have anything to do with drug trials?
What?
22
Manipulating You• Manipulating the data
• CME
• Ghost writing
• Persuasion
• DTC
• PR
• Bribes

23
Manipulating Studies
• Martin Keller at Brown University:
Efficacy of Paroxetine in the Treatment of Adolescent Major Depression: A Randomized, Controlled Trial
(Journal of the American Academy of Child and Adolescent Psychiatry, July 2001)

24
Continuing Medical Education
• Half of all CME courses are sponsored by pharmaceutical companies
• Drug-industry financing of continuing medical education has nearly quadrupled since 1998, from $302 million to $1.12 billion.

25
On Persuasion
The rule of reciprocity

26
The influence of drug reps
The study:A group of students were given 2 different surveys. • An elected official who awards contracts accepting a
$50 gift from a prospective bidder.• A medical student accepting a $50 gift from a drug
company.
Nurse practitioners were given similar questionnaires.
Is this Wrong?

27
The influence of drug reps
The results:The Medical Students:• Public official’s • Medical student The Nurses:• Nurse Practitioners • Resident • Nurse
85% Wrong
46% Wrong
97% Wrong
64% Wrong
30% Wrong

28
Pens and Pencils Matter
Ad from Pharmaceutical Executive magazine

29
Pens and Pencils Matter“If the pens were handed out to 50 docs per rep or 100,000 docs, then each doc would have to bring in a mere $0.15 worth of new scripts to cover the cost. Say, however, that only 2% 0r 2,000 docs that were given pens are subject to gift influence peddling -- the other 98% of docs threw their pens in the waste basket. These easily-influenced docs would then would have to write $2.00 more scripts for the drug than they normally would to make the pen project break even for the pharma company. That seems like a realistic scenario. “
-from the Pharma Marketing Blog
30
The influence of drug repsSKIP
The study:The Kaiser Family Foundation national survey of physicians, conducted
in 2001 with a sample of about 2600
The results:• 15% rated info from drug reps as “very useful,”; 59% as somewhat
useful• 9% rated that info “very accurate,”; 72% “somewhat accurate”• 92% had accepted free drug samples; 61% had accepted meals, free
travel, or tickets to entertainment events; 12% had received “financial incentives to participate in drug trials.
• 31% thought it was unacceptable for reps to receive information about prescribing habits; 43% said they were bothered by it but understood its purpose; 22% had no problem with the practice.

31
The influence of drug reps:Patient Awareness and Attitude toward
Commercial Gifts
Gift % aware of gift % who don’t approve
% who approve % with no opinion
Dinner 22.4 48.4 34.6 14.6
Baby formula for family use
28.6 44.2 41.4 10.9
Cocktail Party at Conference
Not asked 43.4 40.5 13.0
Golf tourn. at conference
Not asked 41.6 40.3 14.6
Coffee Maker 13.8 40.7 39.1 17.3
Conference expenses
Not asked 32.5 52.7 11.5
Ice cream at convention
Not asked 28.0 55.6 12.8
Ballpoint Pens 55.3 17.5 67.3 13.0
Medical Books 34.6 16.9 70.0 9.9
Drug Samples for office use
87.0 7.6 82.1 9.3

32
Ghostwriting
According to recent studies in JAMA and the British Journal of Psychiatry, between 11% and 50% of articles on pharmaceuticals that appear in major medical journals are ghostwritten.

33
Disease Mongering
“The desire to take medicine is perhaps the greatest feature which distiguishes man from animals”
-Sir William Osler

34
How to Disease Monger: A Summary
It takes 8 years to bring a drug from the lab to the pharmacy, and less than 18 months to obtain a new indication.
How to sell a sickness:• Step 1: Create a new condition, redefine an
existing condition to reduce the stigma, or elevate the importance of an existing condition.
• Step 2: Market the symptoms instead of the drug.
• Step 3: Offer pills to cure the diseaseYou have a blockbuster!

35
Case Study: Social Anxiety Disorder (SAD)
• Once a little known condition. According to DSM4: “extrermly rare,” 1-2%
• GSK hired public relations firm to position SAD as a severe condition”
• Expand disease : Bus & Metro Ads • Supported by Social Anxiety Disorder Coalition,
APA, Anxiety disorders of America Foundation, Freedom from Fear
• PR: – Video news release– Standard release with names of paid
consultants

36
Case Study: Social Anxiety Disorder (SAD)
• SAD became a media frenzy in 1998 just after Paxil was approved to treat the condition
• The slogan? "Imagine Being Allergic to People."
• SAD was positioned as the third most common psychiatric disorder in the U.S., affecting 13.3% of the population.
Today, Paxil is the #2 selling SSRI, behind Eli Lilly’s Prozac.

37
Case Study: Lunesta
• Press releases encourge articles about sleep problems years before approval
• 2001-2003: 600 articles on sleep problems• 2003-2005: >1000 • Duke site of trials release press releases before approval, which mention
drug– “Sleepless at Duke find cure” - Raleigh News & Observer
• Seeding trials ???• Astro-turf National Sleep Foundation
– Big Pharma funded at least 1.2 million per year plus “Poll”– 1996 ½ Americans suffer frequent insomnia & sleeplessness– Under recognized, under-diagnoses, under-treated– 2005 75% sleep problems so bad it interferes with sex
• Thought leaders• APA support

38
Case Study: Lunesta
Approved in May 2005. The next steps in the plan of attack:
• 60 million DTC coming out ad during Desperate Housewives• “Lunesta helps most people sleep all through the night.” • “the first and only prescription approved for long-term use.”• CFO: “Its a drug you can take again and again and again.
45 days later 60,000 new scripts per week

39
Other mass-marketed disorders:
• Premenstrual dysphoric disorder (PMDD)
• Female sexual dysfunction• Irritable bowel syndrome (IBS)• Attention deficit disorder• Generalized anxiety disorder (GAD)• Restless leg syndrome• Persistent genital arousal disorder
(PGAD)
And the list goes on and on . . .

40
Key Elements of Disease Mongering and how the Media Could Do Better

41
The Number Needed to Treat
Defined as the number of patients that would require treatment with a form of medication to reduce the expected number of cases of a defined endpoint by one
It does not account for NNTHarm

42
Would you take this for 5 years if?
• Lowered your chance of a heart attack by:
• Lowered your chance of having a heart attack from:
• Saved 1/100 from having a heart attack
33%
3% to 2%
Who will it be??

43
Misleading StatsCase Study: Lipitor
The Claim: Lipitor “reduces the risk of heart attack by 36
percent…in patients with multiple risk factors for heart disease.“
The Reality:“in a large clinical study, 3 percent [or three out
of every hundred] of patients taking a sugar pill or placebo had a heart attack compared to 2 percent [or two out of every hundred] of patients taking Lipitor."

44
Misleading StatsCase Study: Lipitor
The Math:
• To spare one person a heart attack, 100 people would have to take Lipitor for more than 3 years.
• Working with less than 100 pateints would produce no benefits.
• You can’t help one-third of a person not have a heart attack.
• A success rate of one out of 100 means that “the other 99 got no measurable benefit” from Lipitor.

45
The Number Needed to Treat

46
Prevention vs. Care
Does prevention really save money?
A recent study, lead authored by Joshua T. Cohen and published in the NEJM says no:
• About 19 percent of prevention strategies saved money right off the bat, compared to 18 percent of the treatment strategies.
• About 48 percent of prevention strategies saved lives for less than $50,000 per QALY compared to 50 percent of treatment strategies.
But this is only one interpretation of the data.
47
Prevention vs. Care
A different analysis, using the same data, finds:
• According to economics literature, there are 4 times as many medical treatments being offered patients today that are not cost effective as there are prevention strategies that are not cost effective.
• Indeed, over 80 percent of treatment interventions cost more than they save, just as over 80 percent of prevention interventions cost more than they save.

48
Prevention vs. Care
• Big Pharma beneftis from promoting care as a better solution. More diseases to treat, more money spent on drugs and interventions.
• Dr. Cohen, through his prior work at the Harvard Center for Risk Analysis has conducted research for numerous industrial groups, including housing (lead in children), telecom (cell phones and driving) and food (mercury and fish). The Tufts Center where he now works has received unrestricted educational grants from numerous drug companies.
• Was the data spun to show a bias in favor of care and support a corporate agenda?
49
Other Challenges to Drug Safety
• Controlling the FDA• Off-label marketing• DTC marketing• Pens & pencils matter • Astroturf (fake grassroots organizations)• Control of real grass roots groups • Funding of research• Funding consensus groups• Fake ethics

50
Drugs withdrawn for safety reasons, 1980 - 2005
Drug Approved Therapueitc Class Rating* Approval Phase (yrs)
Zomax (zomiperac) 1980 NSAID P 1.9
Oraflex (benoxaprofen) 1982 NSAID S 2.2
Merital (nomifensine) 1984 antidepressant S 6.0
Suprol (suprofen) 1985 NSAID S 7.2
Seldane (terfenedine) 1985 Antihistamine P 2.2
Enkaid (encainide) 1986 antiarrythmic P 2.9
Hismanal (astemizole) 1988 antihistamine S 3.8
Omniflox (temafloxin) 1992 antiinfective S 2.2
Manoflax (flosequinan) 1992 Vasodilator S 2.2
Propulsid (cisapride) 1993 gastrointestinal S 1.9
Duract (bromfenac) 1997 NSAID S 2.5
Posicor (mibefradil) 1997 antihypertensive S 1.3
Raxar (grepafloxacin) 1997 Antiinfective S 1.0
Trovan (trovafloxacin) ** 1997 Antiinfective S 1.0
Rezulin (troglitazone) 1997 Antidiabetic P 0.5
Baycol (cerivastatin) 1997 Statin S 1.0
Raplon (rapacuronium) 1999 Anesthetic S 1.1
Vioxx (rofecoxib) 1999 NSAID (Cox-2) P 0.5
Lotronext (alosetron)** 2000 Gastrointestinal P 0.6
Bextra (valdecoxib) 2001 NSAID (Cox-2) S 0.8
P=Priority Review, S=Standard Review **Subsequently re-introduced to the market with restricted labeling

51
The Big Picture
• Medical education is designed to reproduce the profession, which is of course the sale of drugs & medical devices & medical procedures.
• That is why medical education focuses on NEW patent drugs and not behavior change, exercise, physical therapy or vitamins (like folic acid, which is very effective at reducing MI risk).

52
"Values are always with us...There can be no view except from a
viewpoint. Prior to answers there must be questions. In the questions raised, the viewpoint has (already)
been chosen and the valuations implied."
-- Gunnar Myrdal