1 genomic medicine of the future uterine lavage in vivo fertilization pgd/pgs without ivf john e....
TRANSCRIPT

1
Genomic Medicine of the Future
UTERINE LAVAGEIN VIVO FERTILIZATIONPGD/PGS WITHOUT IVF
John E. Buster, M.D., Professor Obstetrics and Gynecology, Warren Alpert Medical School of Brown University,
Women and Infants Hospital, Providence, RI

2
Disclosure
The speaker is Founder and Chief Medical Officer for Previvo Genetics, LLC

3
PGD/PGS WITHOUT IVF
• PGD (Affected child, parents, or carrier)
• PGS (Aneuploidy)
• Recurrent miscarriage
• Some infertility
• Method of embryo donation-No IVF
• Fertility preservation


55
Historical Overview of Uterine Lavage
In 1984 A UCLA research team performed the world’s first ever donor human embryo transfer using “uterine
lavage” for recovery of an in vivo blastocyst




9

10

11

12

13

14

15

16
Data from Initial StudiesMorphology of human ova recovered by uterine lavage from fertile
women with single spontaneous ovulations and timed inseminations abstracted from five reports from two independent centers
Insem Total Ova Unidvid Frag 2-18 Morula Blast
UCLA (1-3) 84 35 6 2 17 2 8
Pavia (4,5) 64 26 2 5 6 6 7
Total 148* 67* 8 7 23 8 15
1. Buster JE et al: Am J Obstet. Gynecol. 1985, 153:211-7.2. Sauer MV et al: Fertil Steril. 1987, 47:324-5.3. Sauer MV et al: Obstet Gynecol. 1988, 71:804-6.
4. Formigli L et al: Fertil Steril. 1987, 47:162-7.5. Formigli L et al: Personal Communication, 1988. * Recovery efficiency for all ova was 67/148 or 45%.

17
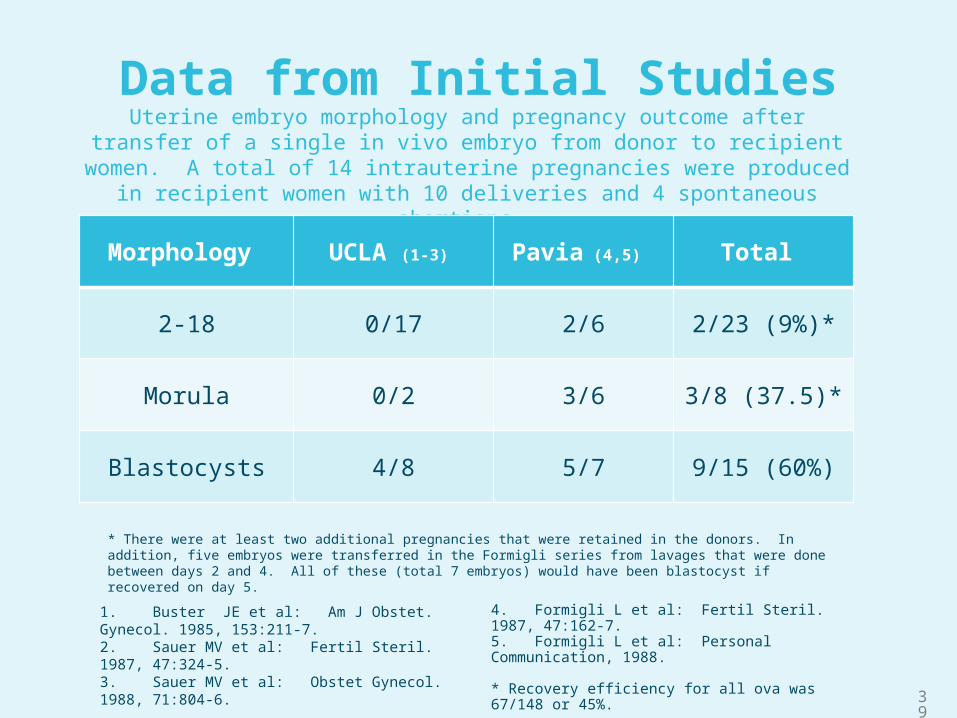
Data from Initial StudiesUterine embryo morphology and pregnancy outcome after transfer of a single in vivo embryo from donor to recipient women. A total of 14 intrauterine pregnancies were
produced in recipient women with 10 deliveries and 4 spontaneous abortions.
Morphology UCLA (1-3) Pavia (4,5) Total
2-18 0/17 2/6 2/23 (9%)*
Morula 0/2 3/6 3/8 (37.5)*
Blastocysts 4/8 5/7 9/15 (60%)
1. Buster JE et al: Am J Obstet. Gynecol. 1985, 153:211-7.2. Sauer MV et al: Fertil Steril. 1987, 47:324-5.3. Sauer MV et al: Obstet Gynecol. 1988, 71:804-6.
4. Formigli L et al: Fertil Steril. 1987, 47:162-7.5. Formigli L et al: Personal Communication, 1988. * Recovery efficiency for all ova was 67/148 or 45%.
* There were at least two additional pregnancies that were retained in the donors. In addition, five embryos were transferred in the Formigli series from lavages that were done between days 2 and 4. All of these (total 7 embryos) would have been blastocyst if recovered on day 5.

18
1980’s vs 2015Uterine Lavage was 30 years ahead of its time
1980’s 2015
Crude devices 45% recovery Advanced Catheter/controller unit: 90% +
Superovulation not safe Superovulation safe
Retained/ectopic pregnancy risk Antagonist shut down minimal pregnancy risk
Crude devices, lavage trauma, large fluid volumes, limited flow control
2nd generation devices/controller, atraumatic, small flluid volumes, precise fluid control
PGD/PGS Genomic technology severely limited PGD/PGS Genomic technology highly evolved
Negative Public opinion Supportive public opinion

19

Uterine Lavage: A Novel PortalTo The Human Embryonic Genome
“In Vivo PGD And PGS Without IVF”

IN VIVO PGD & PGS WITHOUT IVF
Antagonist FSH.
Partner IUI
Blastocysts Recovered
PGS: Euploid blasts vitrified
PGD: Unaffected blasts identified
SET: Unaffected blasts.
-
Cryopreservation
Trophectoderm Bx and Dx
Lavage
Insemination
Superovulation
Single Embryo Transfer

22

In Vivo Insemination Fertilization

24

Uterine Lavage/Recovery


CRYOPRESERVATION
Using established technology. . .To be returned in the next cycle. . .
Or many years later. . .


Transfer

Advantages of the Procedure
Uterine Lavage
• Office procedure• No operating room • No anesthesia• Highly automated• Economical • Recovers in vivo blastocysts
30

Advantages of the Procedure
• High Transfer efficiencies• Multiple trophectoderm cells for diagnosis• Efficient cryopreservation and thawing• In vivo fertilization, no IVF• SET reduction/elimination of multiples
Day 5 In Vivo Blastocysts
31

32
Why in vivo Blasts Matter
1. Conception in vivo: Vitality uncompromised by IVF culture
2. In vivo blastocyst implantation/pregnancy rates > IVF
3. Trophectoderm for diagnosis:
a. Shipped for analysis anywhere
b. Blastocyst bx safer/more informative than cleavage
5. Vitrification with return to patient after Dx
6. Positive Public Perception: Moral ethical genetic plan for pregnancy-not an established pregnancy. Can end need for pregnancy termination in practice of genetic medicine.
The Single Most Important Rationale for Uterine Lavage is Access to the In Vivo Blastocyst

33
Comparative Trials In Animal Models:In Vivo Embryos Outperform IVF
• IVF embryos lower implantation/development/births
• IVF embryos developmentally delayed
• IVF blasts fewer cells per embryo
• IVF embryos improve when transferred to in vivo
• IVF culture induces aberrant gene expression
• Limited human trials (1980’s): Single in vivo blast transfers 60% ongoing pregnancies

34
IVF Embryos Lower Implantation/Development/Births
• Bovine: In vivo increased implantation Farin PW et. al. 1991
• Porcine: In vivo higher transfer efficiencies
Stokes PJ et al. 2005. • Mouse: In vivo blastocysts formed
fetuses at higher rates than IVF blastocysts
Thouas et al, Reproduction 2003

35
IVF Embryos Are Developmentally Delayed
• Ovine : In vivo blasts increased hatching rates
• Garcia-Garcia et al, Anim Reprod Sci 2007
• Mouse: IVF reduced blast formation rates
Jurisicova et al, Mol Hum Reprod 1998

36
IVF Blasts Have Fewer Cells Per Embryo
• Mice: In vitro cultured blastocysts have fewer cells at comparable stage than in vivo
Colver et al, Fertil Steril 1991

37
IVF Embryos Improve When Transferred To An In Vivo Environment
• Ovine: In vitro blastocysts have higher survival when transferred to an in vivo environment
Garcia-Garcia et al, Theriogenology 2005
• Mouse: Low viability in vitro embryos have restored viability after transfer to an in vivo enviroment
Evsikov, et al, J Exp Zool 1996

38
IVF Culture Induces Aberrant Gene Expression
• Porcine: In vitro embryos have aberrant expression of transcriptional regulators in excess of in vivo
Hyttel et al, Hum Reprod 2000
39
Data from Initial StudiesUterine embryo morphology and pregnancy outcome after transfer of a single in vivo embryo from donor to recipient women. A total of 14 intrauterine pregnancies were
produced in recipient women with 10 deliveries and 4 spontaneous abortions.
Morphology UCLA (1-3) Pavia (4,5) Total
2-18 0/17 2/6 2/23 (9%)*
Morula 0/2 3/6 3/8 (37.5)*
Blastocysts 4/8 5/7 9/15 (60%)
1. Buster JE et al: Am J Obstet. Gynecol. 1985, 153:211-7.2. Sauer MV et al: Fertil Steril. 1987, 47:324-5.3. Sauer MV et al: Obstet Gynecol. 1988, 71:804-6.
4. Formigli L et al: Fertil Steril. 1987, 47:162-7.5. Formigli L et al: Personal Communication, 1988. * Recovery efficiency for all ova was 67/148 or 45%.
* There were at least two additional pregnancies that were retained in the donors. In addition, five embryos were transferred in the Formigli series from lavages that were done between days 2 and 4. All of these (total 7 embryos) would have been blastocyst if recovered on day 5.

40
Clinical Applications
• PGD (Affected child, parents, or carrier)
• PGS (Aneuploidy disorders)
• Recurrent miscarriage
• Some infertility
• Method of embryo donation-No IVF
• Fertility preservation

Future Clinical Impact
• Medical device is the only portal to the human embryonic genome in vivo.
• Embryonic diagnosis in vivo will become more widely available
• First pregnancies and births should immediately follow blast recoveries expected in 2015
• Will facilitate study of human in vivo implantation and embryonic development never before possible

2015
• Full Validation of Uterine Lavage System• Lavage Cycle Effectiveness
• Effective Blastocyst Recovery
• Limited Market Release
• First Pregnancies
• Publications
• Further Platform Validations
