1 for us medical response to unsolicited requests for information distribution is strictly...
TRANSCRIPT

1For US Medical Response to Unsolicited Requests for Information
Distribution is Strictly ProhibitedMU-US-0036a
Biogen Portfolio Update
Biogen US MedicalMay 2015
MU-US-0036a

2For US Medical Response to Unsolicited Requests for Information
Distribution is Strictly ProhibitedMU-US-0036a
Guidance for UseThis slide deck is intended to be used in response to an unsolicited request for information when received from a payer customer. This slide deck contains hyperlinks to enable the US Medical colleague (E.g., MSL) to navigate the slide deck with the intent of delivering a narrowly tailored response to a question. It is for reactive use only, and is not intended to be distributed in any format.
Medical Guidance:• When an MSL is asked a question
• Please ask why the question is being asked• Please ask what specific data is being requested• Utilize hyperlinks within the slide deck to tailor a response to the specific
question. • Please do not show the “Table of Contents” hyperlink slide to the customer.• Ensure that the response is clear regarding approved vs investigational
products/indicationsPlease note that the information contained within this slide deck was developed from referenced materials.

3For US Medical Response to Unsolicited Requests for Information
Distribution is Strictly ProhibitedMU-US-0036a
Biogen
About Biogen
Daclizumab HYPOverview of Development
SELECT
DECIDE
Anti-LINGO-1
Tysabri SPMS
Tysabri Acute Ischemic Stroke
Anti-TWEAK
Neublastin
ISIS-SMNRx
BIIB037
BAN2401
BG00011

4For US Medical Response to Unsolicited Requests for Information
Distribution is Strictly ProhibitedMU-US-0036a
Biogen
• Biogen is the world's oldest independent biotechnology company
• Established 1978
• Biogen has >7,500 employees worldwide and >$9.7 billion USD in annual revenues (2014)
*Pharmaceutical Industry Profile 2012, Washington DC, PhARMA, April 2012. Biogen. Available at www.biogencom.
Founded in 1978, we are the
world’s oldest independent
biotechnology company that today
has a rapidly-expanding global
footprint and employs approximately
7,000 people worldwide
Through cutting-edge science and
medicine, we discover, develop and
deliver to patients worldwide innovative
therapies for serious
neurodegenerative, hematologic and
autoimmune diseases

5For US Medical Response to Unsolicited Requests for Information
Distribution is Strictly ProhibitedMU-US-0036a
Approved ProductsM
ult
iple
Scl
ero
sis
Hem
op
hil
ia

6For US Medical Response to Unsolicited Requests for Information
Distribution is Strictly ProhibitedMU-US-0036a
Multiple Sclerosis
Alzheimer’s Disease
Acute Ischemic Stroke
Lupus Nephritis
Idiopathic Pulmonary Fibrosis
Neuropathic Pain
Spinal Muscular Atrophy
Alzheimer's Disease
Biogen Pipeline*
PHASE I PHASE II PHASE III FILED
Multiple Sclerosis
Daclizumab HYP*
Hemophilia A
ALPROLIX*
ELOCTATE*
Hemophilia B
PLEGRIDY
Secondary Progressive Multiple SclerosisTYSABRI
Neublastin
Anti-TWEAK
Anti-LINGO
BG00011
ISIS-SMNRx*
BIIB037*
TYSABRI
Multiple SclerosisBIIB061
E2609*
Alzheimer's DiseaseBAN2401*
FDA APPROVED
FDA APPROVED
Lat
e-S
tag
eE
arly
-Sta
ge
* Partnered program
ISIS-DMPKRx* Myotonic Dystrophy
Systematic Lupus Erthematosus
www.biogen.com*Status as of May 2015
Anti-CD40 Ligand (CDP7657)
FDA APPROVED
Multiple SclerosisAnti-LINGO
Acute Optic Neuritis

7For US Medical Response to Unsolicited Requests for Information
Distribution is Strictly ProhibitedMU-US-0036a
Daclizumab HYP*
Multiple Sclerosis
*Daclizumab HYP is an investigational candidate
8For US Medical Response to Unsolicited Requests for Information
Distribution is Strictly ProhibitedMU-US-0036a
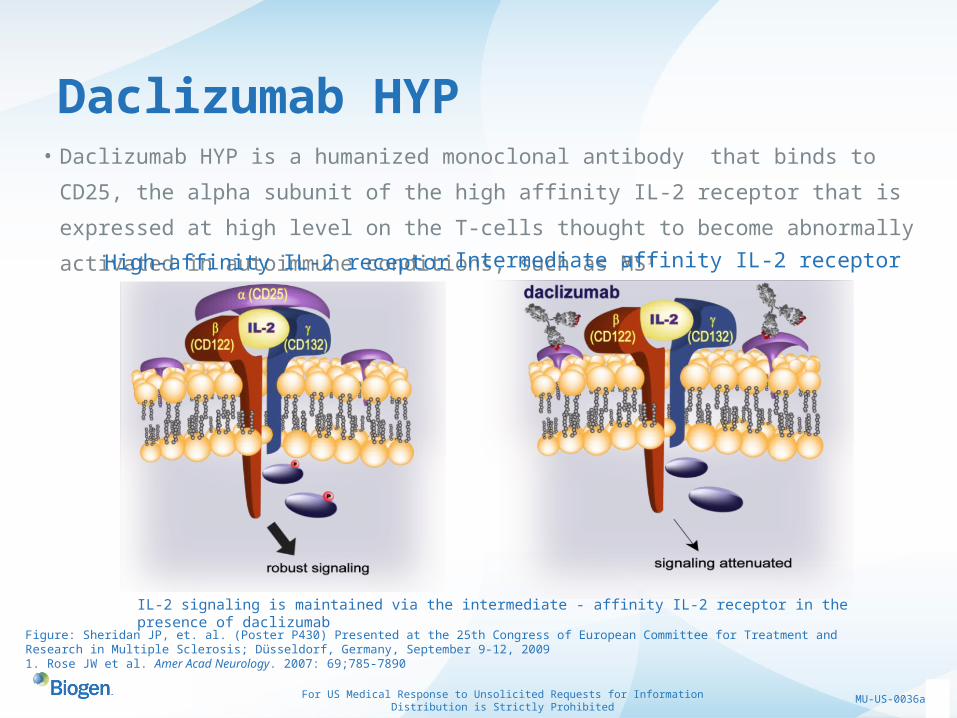
Daclizumab HYP• Daclizumab HYP is a humanized monoclonal antibody that binds to CD25, the alpha
subunit of the high affinity IL-2 receptor that is expressed at high level on the T-cells
thought to become abnormally activated in autoimmune conditions, such as MS1
IL-2 signaling is maintained via the intermediate - affinity IL-2 receptor in the presence of daclizumab
Figure: Sheridan JP, et. al. (Poster P430) Presented at the 25th Congress of European Committee for Treatment and Research in Multiple Sclerosis; Düsseldorf, Germany, September 9-12, 20091. Rose JW et al. Amer Acad Neurology. 2007: 69;785-7890
High-affinity IL-2 receptor Intermediate affinity IL-2 receptor

9For US Medical Response to Unsolicited Requests for Information
Distribution is Strictly ProhibitedMU-US-0036a
γγ
The IL-2 Receptor
IL-2Rα(CD25)
IL-2Rβ(CD122)
γC(CD132)
αIL-2
β
IL-2
β
High-affinityIL-2R
Intermediate-affinityIL-2R
DAC HYP=daclizumab high-yield process; IL=interleukin; R=receptor; γC=common gamma chain1. Wiendl H, Gross CC. Nat Rev Neurol. 2013;9:394-40.
IL-2Rβ(CD122)
γC(CD132)
The high-affinity IL-2R is composed of IL-2Rα, IL-2Rβ, and γC
R IL-2Rα (CD25) has no known signaling function
R IL-2Rβ and γC harbor all signaling capability
The intermediate-affinity IL-2R is composed of IL-2Rβ and γC but lacks the IL-2Rα1

10For US Medical Response to Unsolicited Requests for Information
Distribution is Strictly ProhibitedMU-US-0036a
Daclizumab HYP Proposed Mechanism of Action
IL-2Rα(CD25)
IL-2Rβ(CD122)
γC(CD132)
α
βγ
High-affinityIL-2R
DAC HYP=daclizumbab high-yield process; IL=interleukin; R=receptor; γC=γcommon. Wiendl H, Gross CC. Nat Rev Neurol. 2013;9:394-40.
βγ
Intermediate-affinityIL-2R
IL-2Rβ(CD122)
γC(CD132)
DAC HYP binds the subunit (CD25) of the high-affinity IL-2R and blocks its interaction with IL-2
DAC HYP does not block interaction between IL-2 and intermediate-affinity IL-2R

11For US Medical Response to Unsolicited Requests for Information
Distribution is Strictly ProhibitedMU-US-0036a
Daclizumab HYPOverview of Development1
2006 2007 2008 2009 2010 2011 2012 2013 2014 2015 2016
CHOICE (phase 2)DAC* add-on with IFNβ
SELECT (phase 2)DAC HYP vs placebo
SELECTION (phase 2)
DAC HYP blinded extension of SELECT
SELECTED (phase 2)DAC HYP open-label extension of SELECTION
DECIDE (phase 3)DAC HYP vs IM IFNβ-1a
EXTEND (phase 3)DAC HYP open-label extension of DECIDE
N=621
N=420
N=517
N=1841
N=1204
N=230
*CHOICE used an investigational form of aclizumab different from daclizumab HYP1Status as of May 2015
DAC=daclizumab; HYP=high-yield process; IFN=interferon; IM=intramuscular; RRMS=relapsing-remitting multiple sclerosis.

12For US Medical Response to Unsolicited Requests for Information
Distribution is Strictly ProhibitedMU-US-0036a
SELECT: MRI Substudy Design OverviewSELECT: MRI Substudy Design OverviewSELECT: Design Overview
52-Week Treatment Period
DAC HYP 300 mg SC every q4w
DAC HYP 150 mg SC q4w
Placebo
Primary endpoint
• Annualized RelapseRate
Secondary endpoints
• New Gd+ lesions at weeks 8–24(MRI substudy n=307)
Tertiary endpoint
• EDSS disability progression at week 52• New T2 lesions at week 52
• Proportion of subjects relapsing
• Change in MSIS-29 physical score (quality of life measure)
0 4 8 12 16 20 24 28 32 36 40 44 48 52
Randomization307 patients
Randomizationn=621 patients
Gold R, et al; SELECT study investigators. Lancet. 2013;381:2167-75.

13For US Medical Response to Unsolicited Requests for Information
Distribution is Strictly ProhibitedMU-US-0036a
Series10
0.1
0.2
0.3
0.4
0.5
0.46
0.21 0.23
Ad
juste
d A
RR
SELECT Results: Annualized Relapse Rate (Primary Endpoint)
Placebo (n=196)
DAC HYP 150 mg (n=201)
DAC HYP 300 mg (n=203)
ARR=annualized relapse rate; DAC HYP=daclizumab high-yield process; EDSS=Expanded Disability Status Scale. Gold R, et al; SELECT study investigators. Lancet. 2013;381:2167-75.
*Estimated from a negative binomial regression model adjusted for number of relapses in 1-year period before trial entry, baseline EDSS score (≤2.5 vs >2.5), and age (≤35 vs >35 years)
Adjusted ARR at end of trial (week 52)
54%relative
reduction vs placeboP<0.0001*
50%relative
reduction vs placeboP=0.0002*

14For US Medical Response to Unsolicited Requests for Information
Distribution is Strictly ProhibitedMU-US-0036a
*Estimated from a proportional odds model adjusted for the baseline number of Gd+ lesions
SELECT Results: MRI Outcomes
Placebo (n=195)
DAC HYP 150 mg (n=199)
DAC HYP 300 mg (n=200)
DAC HYP=daclizumab high-yield process; Gd+=gadolinium-enhancing.Gold R, et al; SELECT study investigators. Lancet. 2013;381:2167-75.
Mean number of new Gd+ lesions at week 52
Placebo (n=195)
DAC HYP 150 mg (n=199)
DAC HYP
300 mg (n=200)*Estimated from a negative binomial regression model
adjusted for the baseline number of T2 lesions
Adjusted mean number of new/newly enlarging T2 lesions at week 52
Series10
0.25
0.5
0.75
1
1.25
1.5
1.4
0.3 0.2
Me
an
no
. of
Gd
+ le
sio
ns
79% relative
reduction vs placebo P<0.0001*
86% relative
reduction vs placebo P<0.0001*
Series10
1
2
3
4
5
6
7
8
9
8.1
2.4 1.7A
dju
ste
d m
ea
n n
o.
of
T2
les
ion
s
70% relative
reduction vs placebo P<0.0001*
79% relative
reduction vs placebo P<0.0001*

15For US Medical Response to Unsolicited Requests for Information
Distribution is Strictly ProhibitedMU-US-0036a
Confirmed Disability Progression at End of SELECT
Placebo DAC HYP 150mg DAC HYP 300mg
Proportion with 3-month confirmed disability progression
13.3% 5.9% 7.8%
*Estimated from Cox-proportional hazards model adjusting for baseline EDSS (≤2.5 vs. >2.5), and age (≤35 vs. >35), Gold R, et al; SELECT study investigators. Lancet. 2013;381:2167-75
0.00
0.05
0.10
0.15
0 12 24 36 48 52Time on study (weeks)
Pro
po
rtio
n o
f p
atie
nts
wit
h 1
2-w
eek
con
firm
ed d
isab
ility
pro
gre
ssio
n
43%ReductionP=0.091*
57%ReductionP=0.021*
DAC HYP 150mg DAC HYP 300mg
Placebo
.

16For US Medical Response to Unsolicited Requests for Information
Distribution is Strictly ProhibitedMU-US-0036a
SELECT: Adverse Events That Occurred in >5% of Patients During the Treatment Period
AEPlacebo(n=204)
DAC HYP 150 mg (n=208)
DAC HYP 300 mg(n=209)
MS relapse 38% 23% 20%
Nasopharyngitis 15% 14% 14%
Upper respiratorytract infection
7% 9% 11%
Headache 10% 10% 10%
Pharyngitis 3% 6% 5%
Gold R, et al; SELECT study investigators. Lancet. 2013;381:2167-75.

17For US Medical Response to Unsolicited Requests for Information
Distribution is Strictly ProhibitedMU-US-0036a
SELECT: Adverse Events of Interest
AEPlacebo(n=204)
DAC HYP 150 mg(n=208)
DAC HYP 300 mg(n=209)
Infections 44% 50% 54%
Serious infections 0% 3% 1%
Cutaneous events* 13% 18% 22%
Injection site reaction, erythema, induration
1% 2% 2%
Serious cutaneous events 0% <1% 1%
Malignancy <1% <1% <1%
Death† 0 1 (<1%) 0
*Cutaneous events are those treatment-emergent AEs whose preferred term contains the word dermatitis, rash, or erythema, or whose preferred term is one of the following: drug eruption, drug hypersensitivity, dyshidrosis, eczema, granuloma annulare, pityriasis rosea, psoriasis, skin exfoliation,toxic skin eruption, urticaria. †Patient recovering from serious cutaneous event died due to a complication of psoas abscess and ischemic colitisGold R, et al; SELECT study investigators. Lancet. 2013;381:2167-75.

18For US Medical Response to Unsolicited Requests for Information
Distribution is Strictly ProhibitedMU-US-0036a
Abnormalities of ALT/AST >5× ULN•Typically occurred late in the treatment period (median onset day = 308)
•Median recovery time = 62 days
– 7 patients resumed or continued therapy. None of these patients had a recurrence in the liver function test or abnormality in the next 5 months (the minimum period for which follow-up was available)
SELECT: Incidence of ALT/AST Abnormalities
ALT/ASTPlacebon=204
DAC HYP150 mgn=208
DAC HYP300 mg n=209
1–3× ULN, n (%) 64 (31) 54 (26) 62 (30)
3–5× ULN, n (%) 6 (3) 7 (3) 6 (3)
>5× ULN, n (%) 1 (<1) 9 (4) 8 (4)
ALT=alanine aminotransferase; AST=aspartate aminotransferase; ULN=upper limit of normal.Gold R, et al; SELECT study investigators. Lancet. 2013;381:2167-75

19For US Medical Response to Unsolicited Requests for Information
Distribution is Strictly ProhibitedMU-US-0036a
DAC HYP 300 mg (n=84)
DAC HYP 150 mg (n=86)
DAC HYP 300 mg (n=87)
DAC HYP 150 mg (n=86)
24-week washout (n=86)
24-week washout (n=88)
DAC HYP 150 mg
DAC HYP 300 mg
SELECTION: N=517
0 4 8 12 16 20 24 28 32 36 40 44 48 52
Primary endpoint
• Safety and immunogenicity
SELECT and SELECTION: Design Overview
Gold R et al. Lancet. 2013;381:2167-2175; Giovannoni G et al. Lancet Neurol. 2014;13:472-481.
Primary endpoint
• Annualised relapse rate
DAC HYP 300 mg SC every 4 weeks (n=209)
DAC HYP 150 mg SC every 4 weeks (n=208)
Placebo (n=204)
0 4 8 12 16 20 24 28 32 36 40 44 48 52
SELECT: N=621
Double-Blind Treatment

20For US Medical Response to Unsolicited Requests for Information
Distribution is Strictly ProhibitedMU-US-0036a
SELECTION: Annualized Relapse Rate
DAC HYP results are combined data for patients on continuous treatment with 150 mg or 300 mg.Giovannoni G et al. Lancet Neurol. 2014;13:472-481.
Series10.00
0.10
0.20
0.30
0.40
0.50
0.43
0.150.17
An
nu
aliz
ed R
elap
se R
ate
Year 1Placebo (n=163)
Year 1DAC HYP(n=129)
Year 2DAC HYP(n=129)
21For US Medical Response to Unsolicited Requests for Information
Distribution is Strictly ProhibitedMU-US-0036a
0.0
0.1
0.2
0.3
DAC HYP continuous
0 12 2463 9 15 18 21
DAC HYP
Placebo
Placebo
16%
12%
DAC HYP
DAC HYP after placebo
6%
13%
Placebo patients startDAC HYP
Time on study (months)
Pro
po
rtio
n o
f p
atie
nts
wit
h c
on
firm
ed d
isab
ilit
y p
rog
ress
ion
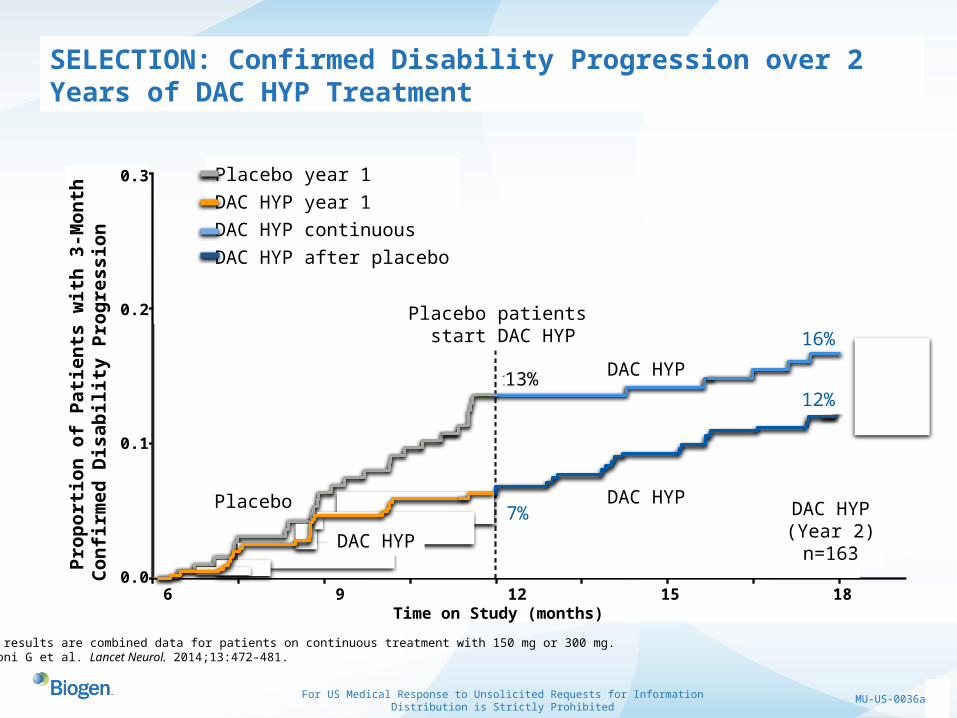
SELECTION: Confirmed Disability Progression over 2 Years of DAC HYP Treatment
Placebo patients start DAC HYP
Placebo
DAC HYP
DAC HYP
Placebo year 1
DAC HYP year 1
DAC HYP continuous
DAC HYP after placebo
16%
13%
7% DAC HYP(Year 2)n=163
0 3 6 9 12 15 18 21 24Time on Study (months)
Pro
po
rtio
n o
f P
atie
nts
wit
h 3
-Mo
nth
Co
nfi
rmed
Dis
ab
ilit
y P
rog
ress
ion
0.3
0.2
0.1
0.0
DAC HYP results are combined data for patients on continuous treatment with 150 mg or 300 mg.Giovannoni G et al. Lancet Neurol. 2014;13:472-481.
12%
DAC HYP

22For US Medical Response to Unsolicited Requests for Information
Distribution is Strictly ProhibitedMU-US-0036a
SELECTION: MRI Assessments After 2 Years
New or Newly Enlarging T2 Lesions
DAC HYP results are combined data for patients on continuous treatment with 150 mg or 300 mg.Giovannoni G et al. Lancet Neurol. 2014;13:472-481.
Series10.0
1.0
2.0
3.0
4.0
5.0
6.0
7.0
8.0
9.0
10.0
8.0
1.91.2M
ean
Nu
mb
er o
f N
ew/E
nla
rgin
g
T2-
Hyp
erin
ten
se L
esio
ns
Year 1Placebo (n=163)
Year 1DAC HYP(n=129)
Year 2DAC HYP(n=129)

23For US Medical Response to Unsolicited Requests for Information
Distribution is Strictly ProhibitedMU-US-0036a
SELECTION: After 24-Week Washout from DAC HYP, Gd+ Lesions were Below Pre-treatment Baseline
1.9
1.2
0.5
0.2
0.4
0.2
1.2
0.9
0.2 0.2
0
0.2
0.4
0.6
0.8
1
1.2
1.4
1.6
1.8
2 SELECT BaselineWk 24Wk 52Wk 72 (End of 24-wk washout)Wk 104 (32-wks after restarting therapy)
DAC HYP 300 mgDAC HYP 150 mg
End of 24 week washout
End of 24 week washout
Nu
mb
er
Ne
w G
d+
Le
sio
ns
(m
ea
n)
Year 1 Year 2 Year 1 Year 2DAC HYP results are combined data for patients on continuous treatment with 150 mg or 300 mg.Giovannoni G et al. Lancet Neurol. 2014;13:472-481.

24For US Medical Response to Unsolicited Requests for Information
Distribution is Strictly ProhibitedMU-US-0036a
SELECTION: Adverse Events of Interest
DAC HYP 150 mg(n=86)
DAC HYP 300 mg (n=84)
DAC HYP 150 mg(n=86)
DAC HYP 300 mg (n=87)
DAC HYP 150 mg(n=86)
DAC HYP 300 mg (n=88)
Serious Infections, n (%) 3 (3) 1 (1) 2 (2) 2 (2) 3 (3) 2 (2)
Serious Cutaneous Events, n (%)
2 (2) 0 0 3 (3) 1 (1) 0
ALT/AST > 5x ULN, n (%) 1 (1) 1 (1) 0 3 (3) 2 (2) 4 (5)
Malignancy, n 0 1 (1) 0 0 0 0
Death* 0 0 0 0 0 1 (1)
DAC HYP StartersYear 1 of DAC HYP
DAC HYP ContinuousYear 2 of DAC HYP
DAC HYP Washout / Reinitiation
ALT, alanine aminotransferase; AST, aspartate aminotransferase; ULN, upper limit of normal
DAC HYP results are combined data for patients on continuous treatment with 150 mg or 300 mg.Giovannoni G et al. Lancet Neurol. 2014;13:472-481.
*One patient in the washout and re-initiation group died because of autoimmune hepatitis after re-initiation of 300 mg daclizumab HYP
25For US Medical Response to Unsolicited Requests for Information
Distribution is Strictly ProhibitedMU-US-0036a
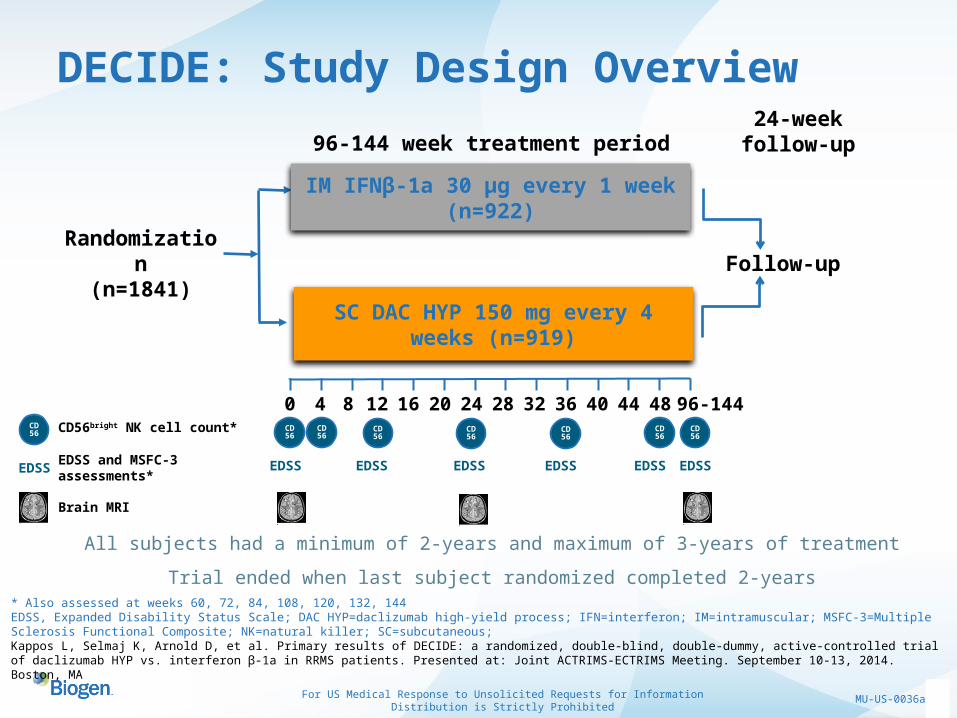
DECIDE: Study Design Overview
All subjects had a minimum of 2-years and maximum of 3-years of treatment
Trial ended when last subject randomized completed 2-years
96-144 week treatment period
Randomization(n=1841)
CD56bright NK cell count* CD56
0 4 8 12 16 20 24 28 32 36 40 44 48 96-144CD56
CD56
CD56
CD56
CD56
CD56
CD56
IM IFNβ-1a 30 μg every 1 week (n=922)
SC DAC HYP 150 mg every 4 weeks (n=919)
Follow-up
Brain MRI
EDSS EDSS and MSFC-3 assessments*
EDSS EDSS EDSS EDSS EDSS EDSS
* Also assessed at weeks 60, 72, 84, 108, 120, 132, 144EDSS, Expanded Disability Status Scale; DAC HYP=daclizumab high-yield process; IFN=interferon; IM=intramuscular; MSFC-3=Multiple Sclerosis Functional Composite; NK=natural killer; SC=subcutaneous; Kappos L, Selmaj K, Arnold D, et al. Primary results of DECIDE: a randomized, double-blind, double-dummy, active-controlled trial of daclizumab HYP vs. interferon β-1a in RRMS patients. Presented at: Joint ACTRIMS-ECTRIMS Meeting. September 10-13, 2014. Boston, MA
24-week follow-up
26For US Medical Response to Unsolicited Requests for Information
Distribution is Strictly ProhibitedMU-US-0036a
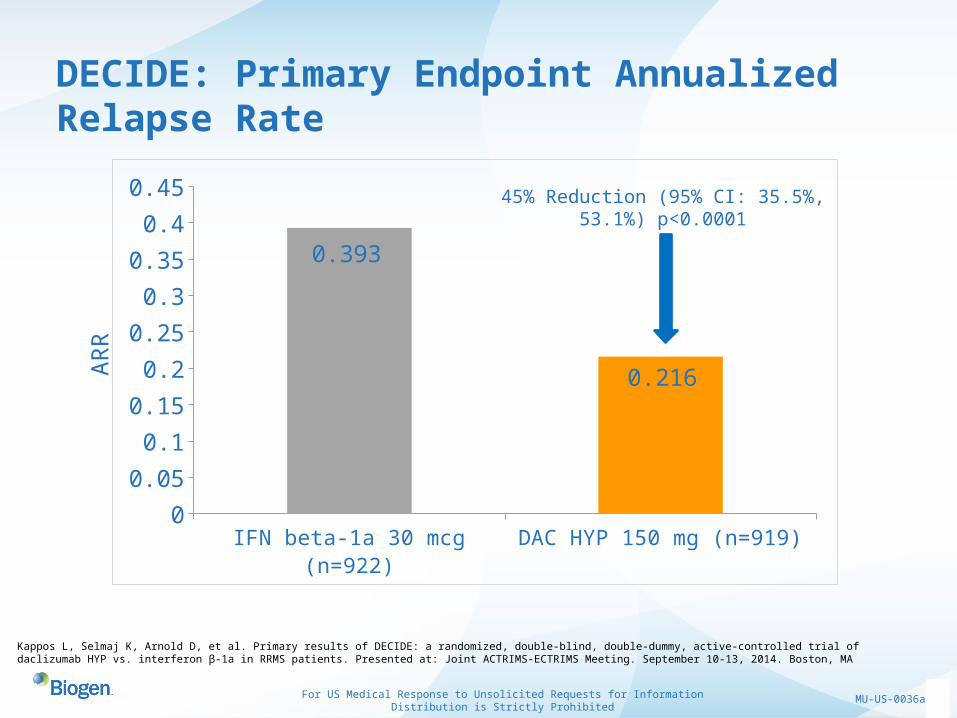
DECIDE: Primary Endpoint Annualized Relapse Rate
Kappos L, Selmaj K, Arnold D, et al. Primary results of DECIDE: a randomized, double-blind, double-dummy, active-controlled trial of daclizumab HYP vs. interferon β-1a in RRMS patients. Presented at: Joint ACTRIMS-ECTRIMS Meeting. September 10-13, 2014. Boston, MA
IFN beta-1a 30 mcg (n=922) DAC HYP 150 mg (n=919)0
0.05
0.1
0.15
0.2
0.25
0.3
0.35
0.4
0.45
0.393
0.216
45% Reduction (95% CI: 35.5%, 53.1%) p<0.0001
AR
R

27For US Medical Response to Unsolicited Requests for Information
Distribution is Strictly ProhibitedMU-US-0036a
DECIDE: MRI Results
Kappos L, Selmaj K, Arnold D, et al. Primary results of DECIDE: a randomized, double-blind, double-dummy, active-controlled trial of daclizumab HYP vs. interferon β-1a in RRMS patients. Presented at: Joint ACTRIMS-ECTRIMS Meeting. September 10-13, 2014. Boston, MA
Series10123456789
10Chart Title
9.4
4.3
*New/Newly Enlarging T2 Lesions54% Reduction
P<0.0001
Series10
0.2
0.4
0.6
0.8
1
1.2Chart Title
1.0
0.4
†New Gd+ Lesions65% Reduction
P<0.0001
Series10
0.51
1.52
2.53
3.54
4.55
Chart Title
4.4
2.1
†New T1 Hypointense Lesions‘blackholes’
52% ReductionP<0.0001
Mea
n nu
mbe
r of
lesi
ons
IFN beta-1a 30 mcg DAC HYP 150 mg
n=841 n=864 n=909 n=900 n=908 n=899
*2-year endpoint† Tertiary Endpoints

28For US Medical Response to Unsolicited Requests for Information
Distribution is Strictly ProhibitedMU-US-0036a
DECIDE: Results Confirmed Disability Progression
Kappos L, Selmaj K, Arnold D, et al. Primary results of DECIDE: a randomized, double-blind, double-dummy, active-controlled trial of daclizumab HYP vs. interferon β-1a in RRMS patients. Presented at: Joint ACTRIMS-ECTRIMS Meeting. September 10-13, 2014. Boston, MA
*3-month confirmed: Patients censored after tentative progression (n-67) analyzed per primary method in the statistical analysis plan; secondary endpoint; all imputed as non-progressors;†6-month confirmed: Patients censored after tentative progression (n=108) imputed per observed rate in trial; tertiary endpoint. Estimated proportions are the average over imputed datasets. For both endpoints risk reduction based on Cox proportional hazards model adjusted for baseline EDSS, history of prior IFN use, and age.

29For US Medical Response to Unsolicited Requests for Information
Distribution is Strictly ProhibitedMU-US-0036a
DECIDE: Overview of Safety
* All deaths were considered unrelated to treatment. The death in the DAC HYP group was due to aspiration pneumonia in a patient who had a MS relapse involving the brain stem and after withdrawing from the study. Deaths in the IFN beta-1a group were due to myocardial infarction, completed suicide, metastatic pancreatic cancer and peritonitis. AE, adverse event; SAE, serious adverse event
Kappos L, Selmaj K, Arnold D, et al. Primary results of DECIDE: a randomized, double-blind, double-dummy, active-controlled trial of daclizumab HYP vs. interferon β-1a in RRMS patients. Presented at: Joint ACTRIMS-ECTRIMS Meeting. September 10-13, 2014. Boston, MA
DECIDE: Overview of Safety
30For US Medical Response to Unsolicited Requests for Information
Distribution is Strictly ProhibitedMU-US-0036a
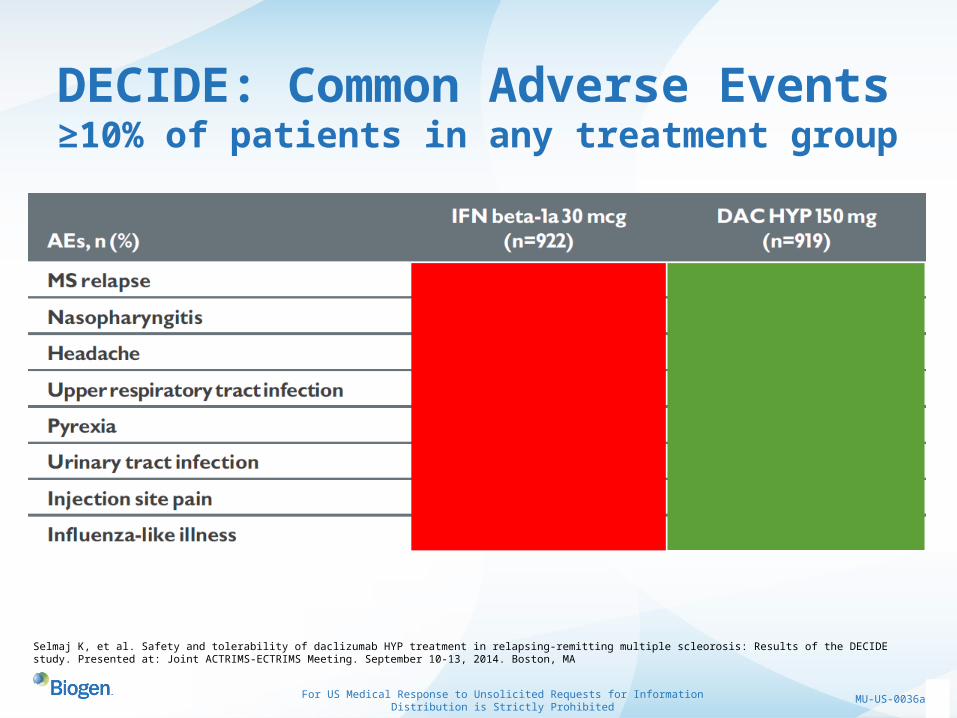
DECIDE: Common Adverse Events≥10% of patients in any treatment group
Selmaj K, et al. Safety and tolerability of daclizumab HYP treatment in relapsing-remitting multiple scleorosis: Results of the DECIDE study. Presented at: Joint ACTRIMS-ECTRIMS Meeting. September 10-13, 2014. Boston, MA

31For US Medical Response to Unsolicited Requests for Information
Distribution is Strictly ProhibitedMU-US-0036a
DECIDE: Adverse Events of Interest
*Clinical assessment of causality based on structured approach (Rockey et al. 2010. Hepatology 51:2117). One case in each group with
causality score of “probable” or higher. ALT, alanine aminotransaminase; AST, aspartate aminotransaminase; ULN, upper limit of normal.
Kappos L, Selmaj K, Arnold D, et al. Primary results of DECIDE: a randomized, double-blind, double-dummy, active-controlled trial of daclizumab HYP vs. interferon β-1a in RRMS patients. Presented at: Joint ACTRIMS-ECTRIMS Meeting. September 10-13, 2014. Boston, MA

32For US Medical Response to Unsolicited Requests for Information
Distribution is Strictly ProhibitedMU-US-0036a
Anti-LINGO-1*
Multiple Sclerosis (MS) & Acute Optic Neuritis (AON)
*Anti-LINGO is an investigational candidate

33For US Medical Response to Unsolicited Requests for Information
Distribution is Strictly ProhibitedMU-US-0036a
Anti-LINGO-1
• Multiple Sclerosis (MS) and Acute Optic Neuritis (AON)
• Current treatments focus on targeting the immunological response
• Anti-LINGO-1 (BIIB033) is the first drug candidate that targets CNS
repair in MS through remyelination1
• LINGO-1 is a CNS-specific, leucine-rich repeat (LRR) and lg-domain,
membrane-associated glycoprotein2
• Hypothesized that blocking the action of LINGO-1 may allow neuronal
repair and remyelination following CNS injury1
Data on File. Biogen.1. Rudick R et al. Expert Opin. Biol. Ther. 2008; 8(10):1561-15702. Mi S, et al. Nature. 2004: 7; 221-228

34For US Medical Response to Unsolicited Requests for Information
Distribution is Strictly ProhibitedMU-US-0036a
Anti-LINGO-1
Ndubaku U, deBellard ME. Acta Histochem. 2008;100:182-195.
Immature oligodentrocytes
Mature oligodendrocyte
Adapted from Jackman N et al. Physiology. 2009;24:290-297; Zhang SC. Nat Rev Neurosci. 2001;2:840-843.
Myelinatingoligodentrocytes
Lingo-1 protein prevents oligodendrocyte maturation
LINGO-1, allrly
LINGO-1, allrly
LINGO-1, allrly
Anti-LINGO-1 antibody binds LINGO-1, allowing oligodendrocytes to mature and function properly

35For US Medical Response to Unsolicited Requests for Information
Distribution is Strictly ProhibitedMU-US-0036a
Co
ntr
ol
RN
Ai
LIN
GO
-1 R
NA
i
P<0.001
No RNAi
Control RNAi
LINGO-1RNAi
0
5
10
15
20
25
Mat
ure
Olig
od
end
rocy
tes
(%
To
tal)
LINGO-1 Blockade Resulted in Oligodendrocyte Differentiation
RNAi=ribonucleic acid interference. Mi S et al. Nat Neurosci. 2005;8:745-751.

36For US Medical Response to Unsolicited Requests for Information
Distribution is Strictly ProhibitedMU-US-0036a
Cuprizone model(1 µg/local)
Lysolecithin model(1 mg/kg/IP)
Experimentalautoimmuneencephalitis (EAE)(3 mg/kg/IP)
Anti-LINGO-1 Antibody Resulted in Remyelination in Animal Models of Demyelination
*
* *
**
Adapted from Mi S et al. Ann Neurol. 2009;65:304-315; Mi S et al. Presented at ECTRIMS; October 13–16, 2010; Gothenburg, Sweden. P731.
*
**
*
Control Anti-LINGO-1
*Demyelinated Axons Remyelinated Axons
*
Control Anti-LINGO-10
20
40
60
80
Mye
lin
ated
Axo
ns
(%)
*P<0.05
Control Anti-LINGO-10
20
40
60
80
Mye
lin
ated
Axo
ns
(%) *P<0.02
Control Anti-LINGO-10
20
40
60
80
Mye
lin
ated
Axo
ns
(%)
*P<0.05

37For US Medical Response to Unsolicited Requests for Information
Distribution is Strictly ProhibitedMU-US-0036a
Anti-LINGO-1 Phase 1 Studies: Safety in Humans
*90% effective concentration.SC=subcutaneous; RRMS=relapsing-remitting MS; SPMS=secondary progressive MS; PK=pharmacokinetics; T1/2=half life.Tran J et al, Neurology Neuroimmunology (N2 Journal) 2014; 1 (18)
Completed Single Ascending Dose (IV And SC) Study in Healthy Volunteers and a Multiple Ascending Dose (2 IV Doses 2 Weeks Apart)
in MS Subjects (RRMS and SPMS)
• In the multiple ascending dose study, common adverse events for anti-LINGO-1 at doses ranging from 0.3 mg/kg–100 mg/kg (combined) vs placebo were
– Urinary tract infection (16% vs 13%)
– Headache (16% vs 13%)
– Upper respiratory tract infection(9% vs 20%)
• PK was linear with a T1/2 typical of a mAb (≈2–3 weeks)
• CSF penetration was low (≈0.1% of serum levels), but concentrations reached levels ≥EC90* values at 10 mg/kg dose
• Findings supported advancing into phase 2 studies

38For US Medical Response to Unsolicited Requests for Information
Distribution is Strictly ProhibitedMU-US-0036a
Anti-LINGO-1 Phase 2 Studies
IM=intramuscular; IFNβ=interferon beta; EDSS=Expanded Disability Status Scale; T25FW=Timed 25-Foot Walking Test; 9HPT=9-Hole Peg Test; PASAT=Paced Auditory Serial Addition Test; DTI=diffusion tensor imaging.Cadavid D et al. Presented at AAN; April 26–May 3, 2014; Philadelphia, PA USA. RENEW: P2.262; SYNERGY: P3.154.
RENEWAcute Optic Neuritis
• Placebo-controlled proof of biology
• Subjects with recent first episode of acute optic neuritis
• Dose: 100 mg/kg q4wks×6
• Endpoints:
– Visual evoked potential (VEP)/multifocal VEP (latency delay)
– Optical coherence tomography (retinal nerve fiber and ganglion cell layer loss)
– Visual function (low contrast letter acuity, visual quality of life)
SYNERGYRelapsing Forms of MS
• Placebo-controlled proof of concept and dose ranging
• Subjects with RRMS and relapsing SPMS receiving IM IFNβ-1a
• Dose: 3, 10, 30, 100 mg/kg q4wks×18
• Physical and cognitive endpoints:
– EDSS/T25FW/9HPT/PASAT composite
– Primary=improvement
– Key secondary=delayed progression
– MS-COG (information processing and learning and memory)
– MRI (MTR, DTI, black holes, atrophy)

39For US Medical Response to Unsolicited Requests for Information
Distribution is Strictly ProhibitedMU-US-0036a
Anti-LINGO-1 Phase 2 AON Study (RENEW)Completed
• Subjects with first episode of acute optic neuritis
• N=82 subjects randomized, 2 arms, 33 sites
• Evaluating efficacy after onset of inflammatory CNS demyelination in a clinically
eloquent area (the optic nerve)
–The visual system affords an opportunity to study the functional consequences of CNS remyelination
»Neurophysiology (VEP/mfVEP)»Survival of retinal ganglion cells (OCT)»Clinical benefit (contrast acuity)
• Top line results revealed evidence of proof of biology for remyelination
• 34% improvement in average FF-VEP latency recovery at 24wks (p-0.0504)
VEP=visual evoked potential; mfVEP=multifocal VEP; OCT=optical coherence tomography.

40For US Medical Response to Unsolicited Requests for Information
Distribution is Strictly ProhibitedMU-US-0036a
Anti-LINGO-1 Phase 2 MS Study (SYNERGY)Fully-enrolled and ongoing*
• Active relapsing forms of MS
• 418 patients enrolled, 5 arms, 72 sites, 12 countries
• Active relapsing MS patients will receive IM IFN beta-1a plus anti-LINGO-1
(4 doses) or IM IFN beta-1a plus placebo
• 18-months treatment duration allows study of clinical benefit
• Allows the study of efficacy in preventive mode (with drug on board before
new lesions develop) but also on pre-existing lesions
• Advanced MRI methodology to study the morphological features of CNS
repair
*As of May 2015

41For US Medical Response to Unsolicited Requests for Information
Distribution is Strictly ProhibitedMU-US-0036a
TYSABRI® (natalizumab)*
Secondary Progressive MS (SPMS)
*Though approved for some indications, TYSABRI is an investigational candidate for SPMS
42For US Medical Response to Unsolicited Requests for Information
Distribution is Strictly ProhibitedMU-US-0036a
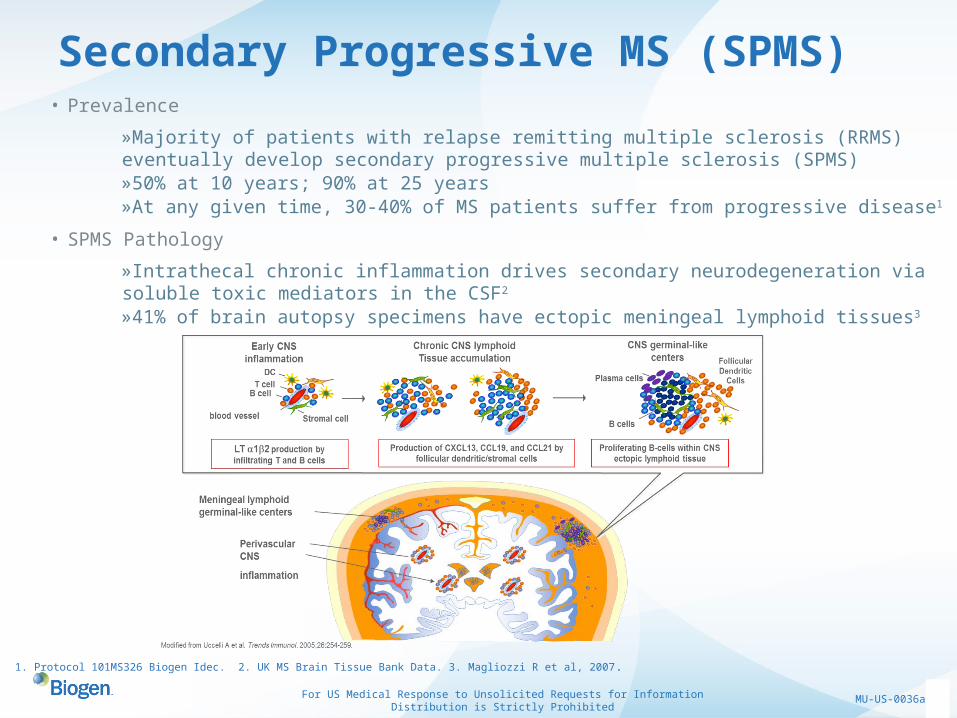
Secondary Progressive MS (SPMS)• Prevalence
»Majority of patients with relapse remitting multiple sclerosis (RRMS) eventually develop secondary progressive multiple sclerosis (SPMS)»50% at 10 years; 90% at 25 years»At any given time, 30-40% of MS patients suffer from progressive disease1
• SPMS Pathology
»Intrathecal chronic inflammation drives secondary neurodegeneration via soluble toxic mediators in the CSF2 »41% of brain autopsy specimens have ectopic meningeal lymphoid tissues3
1. Protocol 101MS326 Biogen Idec. 2. UK MS Brain Tissue Bank Data. 3. Magliozzi R et al, 2007.

43For US Medical Response to Unsolicited Requests for Information
Distribution is Strictly ProhibitedMU-US-0036a
Natural History of MS:Clinical and MRI Measures
Time
Relapsing-Remitting MS
Secondary Progressive MS
Preclinical
MRI ActivityBrain Volume
Relapses/Disability
Dis
abili
ty
MRI T2 lesion load
Data on File. Biogen

44For US Medical Response to Unsolicited Requests for Information
Distribution is Strictly ProhibitedMU-US-0036a
RRMS SPMS: Moving from an Acute, Focal Inflammatory Process to Chronic, Compartmentalized Global Inflammation
RRMS Exacerbation
Major InflammationVery high chemokine levels
Early Progressive MS
Less InflammationModerate-low chemokine
levels
CIS, RRMS
InflammationModerate chemokine levels
Late Progressive MS
Low, but significant chemokine levels
Acute Gd+ Lesions(White Matter)
Meningeal Foci(Grey Matter)
“Chronic lesions”
Cortical Pathology
Illustration by Diego Cadavid and Jeff Browning. Biogen
Meningeal lymphoid germinal-like centers
Perivascular white matter
infiltrates
Modified from Uccelli et al. 2005. Trends Immunol. 26:254-259
45For US Medical Response to Unsolicited Requests for Information
Distribution is Strictly ProhibitedMU-US-0036a
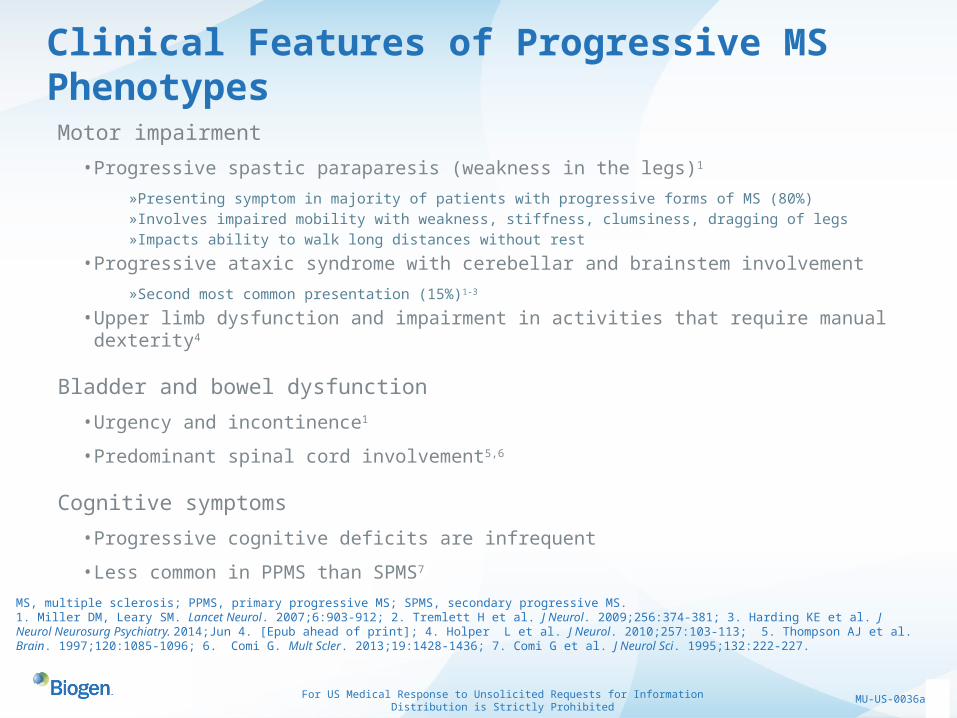
Clinical Features of Progressive MS Phenotypes
MS, multiple sclerosis; PPMS, primary progressive MS; SPMS, secondary progressive MS.1. Miller DM, Leary SM. Lancet Neurol. 2007;6:903-912; 2. Tremlett H et al. J Neurol. 2009;256:374-381; 3. Harding KE et al. J Neurol Neurosurg Psychiatry. 2014;Jun 4. [Epub ahead of print]; 4. Holper L et al. J Neurol. 2010;257:103-113; 5. Thompson AJ et al. Brain. 1997;120:1085-1096; 6. Comi G. Mult Scler. 2013;19:1428-1436; 7. Comi G et al. J Neurol Sci. 1995;132:222-227.
Motor impairment
• Progressive spastic paraparesis (weakness in the legs)1
»Presenting symptom in majority of patients with progressive forms of MS (80%)»Involves impaired mobility with weakness, stiffness, clumsiness, dragging of legs»Impacts ability to walk long distances without rest
• Progressive ataxic syndrome with cerebellar and brainstem involvement
»Second most common presentation (15%)1-3
• Upper limb dysfunction and impairment in activities that require manual dexterity4
Bladder and bowel dysfunction
• Urgency and incontinence1
• Predominant spinal cord involvement5,6
Cognitive symptoms
• Progressive cognitive deficits are infrequent
• Less common in PPMS than SPMS7

46For US Medical Response to Unsolicited Requests for Information
Distribution is Strictly ProhibitedMU-US-0036a
Rationale for Natalizumab Treatment in SPMS
1. Christensen JR et al. Neurology. 2014;82;1499-1507.
2. Sellebjerg et al. Multiple Sclerosis. 2012.18(S4):514-515.
It is believed to prevent trafficking of lymphocytes across blood vessels and into the brain and spinal cord
May also suppress inflammation within the CNS1
• Possible reduction in CXCL13 levels in the CSF of patients with active and progressive MS
• Possible reduction in intrethecal levels of osteopontin, another molecule that has been implicated in MS progression at the experimental level
Post-hoc analyses of relapsing and non-relapsing SPMS studies suggest that natalizumab may be beneficial (T25FW, 9HPT)2

47For US Medical Response to Unsolicited Requests for Information
Distribution is Strictly ProhibitedMU-US-0036a
Ongoing Development & Research
ASCEND Trial Overview
»An investigation of whether TYSABRI treatment slows the accumulation of disability not related to relapses in patients with SPMS
»Primary endpoint: the proportion of subjects experiencing confirmed progression of disability as measured by a composite endpoint
»FDA special protocol assessment (SPA) obtained with accepted regulatory endpoint
»Study fully enrolled in May 2013 (N=889)
»Data readout expected 2015
Data on File. Biogen. SCR=screening; R=randomization; IV=intravenous; q4w=once every 4 weeks.

48For US Medical Response to Unsolicited Requests for Information
Distribution is Strictly ProhibitedMU-US-0036a
TYSABRI® (natalizumab)*
Acute Ischemic Stroke
*Though approved for some indications, TYSABRI is an investigational candidate for acute ischemic stroke

49For US Medical Response to Unsolicited Requests for Information
Distribution is Strictly ProhibitedMU-US-0036a
TYSABRI in Ischemic Stroke
Prevalence
–There are nearly 800,000 strokes of all types per year in the US
–Ischemic stroke accounts for approximately 80%
Treatment
–Recombinant tissue plasminogen activator (rtPA) only approved pharmacological therapy for acute ischemic stroke. Must be used within 3 hours of stroke onset (US Guidelines)
–TYSABRI could be used as an adjunctive therapy with TPA
–Blocking the α4β1 integrin with natalizumab is expected to reduce peri-stroke inflammation and thereby reduce the expansion of the infarct due to inflammation
–Potential to be the first disease-modifying, anti-inflammatory therapeutic for stroke, with better efficacy and safety than TPA
–As a result of acute dosing, PML is not expected to be an observed AE in stroke.
Data On File. Biogen.Roger 2011 (From Protocol 101SK201)

50For US Medical Response to Unsolicited Requests for Information
Distribution is Strictly ProhibitedMU-US-0036a
Clot within artery blocks normal flow to the brain
Loss of blood supply results in ischemia
Two major zones of injury: ● Core ischemic zone
● Ischemic penumbra
Saver JL. Stroke 2006;37:263–6
Blockage Ischemic tissue Ischemic Penumbra Core ischemic zone
Etiology of Acute Ischemic Stroke (AIS)Obstructed blood flow in the brain leads to ischemia
Ischemia = restriction in blood supply to tissues Core ischemic zone = area of severe ischemia (blood flow <10–25%)Ischemic penumbra = rim of mildly-to-moderately ischemic tissue
Infarction
Penumbra
Thrombus

51For US Medical Response to Unsolicited Requests for Information
Distribution is Strictly ProhibitedMU-US-0036a
Golden treatment window during which pharmacologic or mechanical
interventions are most likely to be effective
Etiology of Acute Ischemic Stroke (AIS) Ischemia leads to infarction (neuronal death)
1. The Internet Stroke Center. The Ischemic Penumbra. Available at: www.strokecenter.org. Accessed: Jan 2014; 2. Saunders DE et al. Stroke 1995;26:2272–6
Minutes after blockage, an ischemic cascade is initiated, leading to neuronal death (infarct) at the core zone
Unless blood flow is promptly restored, the penumbra also infarcts, resulting in a larger total infarct volume1
The larger the infarct volume, the worse the clinical outcomes for AIS patients2

52For US Medical Response to Unsolicited Requests for Information
Distribution is Strictly ProhibitedMU-US-0036a
Acute and long-term functional outcomes in AIS Type and degree of long-term disability depend upon area of brain affected and extent of damage
*p=0.001. AIS=acute ischemic stroke; mRS=modified Rankin ScalePetty GW et al. Stroke 2000;31:1062–8
Before stroke Maximal deficit 90 days after stroke 1 year after stroke0
102030405060708090
100
75.6
27.4
53.7 50.3
9.8
43.935.8
41.6
Functional status (mRS) among AIS patients
No significant or slight disability
Moderately severe or severe disability
Pat
ien
ts (
%)
Common long term outcomes
paralysis/problems controlling movement problems using or understanding language
sensory disturbances problems with thinking and memory
emotional disturbances
No significant or slight disability: Rankin score of I or II; Moderately severe or severe disability: Rankin score of IV, V or dead

53For US Medical Response to Unsolicited Requests for Information
Distribution is Strictly ProhibitedMU-US-0036a
Natalizumab as AIS TherapyNatalizumab is believed to block the migration of lymphocytes that are thought to mediate post-AIS inflammatory responses that increase infarct volume
α4β1integrin
VCAM-1
1. Natalizumab, an a α4β1 integrin antibody ( ), binds to α4β1 integrin receptors on all human leukocytes (except polymorphonuclear leukocytes)1
2. Natalizumab binding blocks CNS α4β1 integrin from interacting with its ligand, vascular cell adhesion molecule-1 (VCAM-1), on the endothelial wall1
3. Blocking entry of leukocytes into the brain suppresses the inflammatory activity thought to cause post-AIS increases in infarct volume2
CNS=central nervous system, 1. Rudick RA et al. NEJM 2006;354:911–23; 2. Protocol 101SK201. Data on file. Biogen, Jun 2013

54For US Medical Response to Unsolicited Requests for Information
Distribution is Strictly ProhibitedMU-US-0036a
Primary objective: To assess the effect of natalizumab on infarct volume over first 5 days after stroke
Secondary objectives – to assess: The effect of natalizumab on infarct growth
at multiple time points after ischemic stroke The effect of natalizumab on disability and
neurological function (BI, mRS, NIHSS etc) The safety of natalizumab via physical and
neurological examinations: o vital sign measurements o hematology and blood chemistry o anti-natalizumab antibodies o monitoring of AEs and SAEs
ACTION Phase II StudyEffect of a single dose of natalizumab infarct volume in AIS patients who have either already received, or are ineligible for, IV rt-PA treatment
AIS=acute ischemic stroke; AE=adverse event; BI=Barthel index; mRS=modified Rankin Scale; NIHSS=National Institute of Health Stroke Scale; SAE=serious adverse eventProtocol 101SK201. Data on file. Biogen, Jun 2013; Clinicaltrials.gov NCT0195570, accessed April 25 2014
Baseline
Day 5
5 days

55For US Medical Response to Unsolicited Requests for Information
Distribution is Strictly ProhibitedMU-US-0036a
Anti-TWEAK (BIIB023)*
Lupus Nephritis
*Anti-TWEAK is an investigational candidate. Efficacy and safety have not been established.

56For US Medical Response to Unsolicited Requests for Information
Distribution is Strictly ProhibitedMU-US-0036a
Lupus Nephritis
Prevalence
–Lupus Nephritis (LN) is present in up to 60% of Systemic Lupus Erythematosus (SLE) patients.1 (SLE occurs in approximately 20 to 70 cases per 100,000)2
Treatment
–No indicated therapies
–Treatment regimens include combination Mycophenolate mofetil with prednisone or cyclophosphamide with methypredinisolone
–Suppress the immune system to treat the acute inflammatory injury3
–Limited efficacy with increasing toxicities over time4
1. Cameron J. J of Amer Society of Nephrology. 1999; 10(2):413-4242. Pons-Estel GJ et al. Seminars in Arthritis and Rheumatism. 2010; 39(4): 257-2683. Ortega L et al. Lupus. 2010; 19:557-5744. Waldman M and Appel GB. Kidney International. 2006; 70:1403-1412

57For US Medical Response to Unsolicited Requests for Information
Distribution is Strictly ProhibitedMU-US-0036a
Anti-TWEAK (BIIB023)
• TWEAK is a proinflammatory cytokine
expressed by WBCs and functions as a
soluble cytokine through the fibroblast growth
factor (FGF)-inducible molecule 14 (Fn14)
• Fn14 is highly induced in disease target
tissues and implicated in the pathogenesis of
LN
• Anti-TWEAK is thought to target Fn14 and is
designed to inhibit glomerular and tubular
pathologies1
• Phase II study ongoing and expected to be
completed in 20192
1. Sanz AB et al. Kidney International. 2011; 80:708-7182. www.clinicaltrials.gov NCT01930890Data on File. Biogen.
58For US Medical Response to Unsolicited Requests for Information
Distribution is Strictly ProhibitedMU-US-0036a
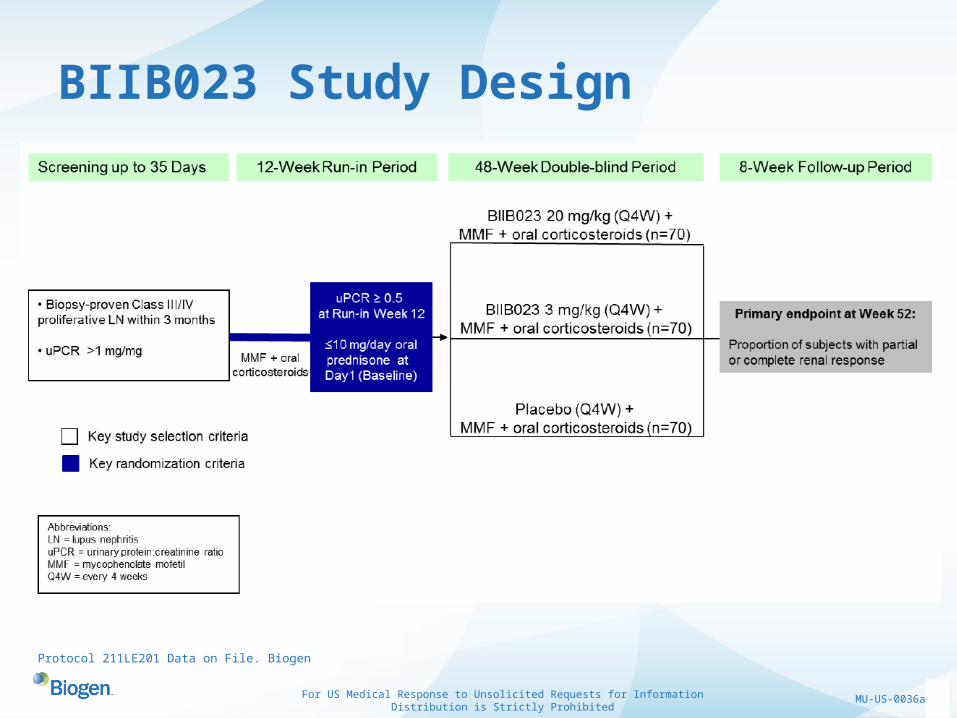
BIIB023 Study Design
Protocol 211LE201 Data on File. Biogen

59For US Medical Response to Unsolicited Requests for Information
Distribution is Strictly ProhibitedMU-US-0036a
Neublastin (BG00010)*
Neuropathic Pain
*Neublastin is an investigational candidate. Efficacy and safety have not been established.

60For US Medical Response to Unsolicited Requests for Information
Distribution is Strictly ProhibitedMU-US-0036a
Neuropathic PainPrevalence
–Estimated 1-2% of population experiences neuropathic pain. Possibly underestimated due to undiagnosed chronic pain1
–Associated with physical injury to a nerve, systemic diseases (e.g. diabetes), autoimmune disorders, infections, etc.2
Treatment
–Current therapies: LYRICA® (pregabalin), NEURONTIN® (gabapentin), CYMBALTA® (duloxetine)
»Poor control of pain with increased side effects3
1. Smith BH and Torrance N. Curr Pain Headache Rep. 2012.2. NINDS.NIH.gov 04-48533. Investigator Brochure V7; Biogen.
LYRICA® and NEURONTIN® are a registered trademarks of Pfizer Inc.; CYMBALTA® is a registered trademark of Eli Lilly and Company

61For US Medical Response to Unsolicited Requests for Information
Distribution is Strictly ProhibitedMU-US-0036a
Neublastin (NBN)
• NBN is a potent cell survival and growth factor which
signals through receptor GFRα3 highly expressed on
pain-sensing neurons1
• Possible targeted alleviation of pain and minimal CNS
side effects were shown in animal studies
• NBN is being investigated as a first-in-class,
potentially restorative treatment for neuropathic pain
and neuropathy associated with nerve damage2
• Phase 2 study expected to be completed 20153
1. Gardell L et al. Nature. 2003; 9:1383-13892. Data on File. Biogen.3. www.clinicaltrials.gov NCT01873404

62For US Medical Response to Unsolicited Requests for Information
Distribution is Strictly ProhibitedMU-US-0036a
Neublastin – Program DevelopmentPhase 1 SAD and MAD studies complete
Phase 2 POC Study in lumbar radiculopathy on-going
–Multi-center, double-blinded, placebo‑controlled study, multi-dose study (~ 168 patients)
–Neublastin (50, 150, 400, 800, and 1200 µg/kg) vs placebo IV three times a week for approximately 13 weeks
–Primary endpoint: Change from baseline in the mean 24-h average general pain intensity score (AGPI) at the end of the treatment week using an 11‑point Numeric Rating Scale (NRS)
Protocol 103NS201 v6

63For US Medical Response to Unsolicited Requests for Information
Distribution is Strictly ProhibitedMU-US-0036a
ISIS-SMNRX*
Spinal Muscular Atrophy
*ISIS-SMNRX is an investigational candidate. Efficacy and safety have not been established.

64For US Medical Response to Unsolicited Requests for Information
Distribution is Strictly ProhibitedMU-US-0036a
Spinal Muscular Atrophy (SMA)
SMA is an autosomal recessive neuromuscular disease. It results in the degeneration of alpha
motor neurons in the spinal cord leading to proximal muscle weakness and paralysis.
– Prevalence
»Approximate incidence is 1 in 6,000 to 1 in 10,000 live births1
– Though classified into three major types, the disorder demonstrates a continuous range of severity and overlap2
1. D’Amico A et al. Orphanet Journal of Rare Diseases. 2011; 6 (71); http://www.ojrd.com/content/6/1/712. Mitchell LR et al, Lancet. 2008; 2120-2133; http://www.ncbi.nlm.nih.gov/books/NBK1352/
Type Other Names Age at Onset Life SpanHighest Function
Achieved
SMA IAcute spinal muscular
atrophy; Werdnig Hoffmann disease
0-6 months <2 years Never sit independently
SMA IIChronic spinal muscular
atrophy; Dubowitz disease7-18 months
Varies from 2 years to the third decade of life
Sit independently, never stand
SMA IIIJuvenile spinal muscular
atrophy; Kugelberg-Welander disease
>18 months Normal Stand and walk alone

65For US Medical Response to Unsolicited Requests for Information
Distribution is Strictly ProhibitedMU-US-0036a
Spinal Muscular Atrophy (SMA)
SMA caused by genetic defects in the SMN1 gene that result in the lack of functional SMN protein» Intervention: Antisense oligonucleotide (ASO) to insert missing exon in “backup”
gene
ISIS-SMNRX is believed to increase production of fully functional SMN protein in model systems
Uniformly 2’-0-methoxyethyl modified (MOE) antisense drug1
Current Treatments:
» No indicated therapies for SMA. Treatment centers around the management of symptoms and preventing complications of SMA
1. Chiriboga, C et al. Results of an Open-Label, Escalating Dose Study to Assess the Safety, Tolerability, and Dose Range Finding of a Single Intrathecal Dose of ISIS-SMN RX in Patients with Spinal Muscular Atrophy. Presented at AAN 2013

66For US Medical Response to Unsolicited Requests for Information
Distribution is Strictly ProhibitedMU-US-0036a
ISIS-SMNRX
• ISIS-SMNRX is currently in Phase 3 trials;
estimated to be completed in 20172
• Granted Orphan Drug Status in US & EU
and Fast Track in the US1
• ISIS-SMNRX is a joint collaboration with
ISIS Pharmaceuticals
1. Darras, B et al. Interim Results of a Phase 2 Study of ISIS-SMNRx in Children with Spinal Muscular Atrophy. Presented at AAN 20142. www.clinicaltrial.gov NCT02193074Data on File. Biogen.

67For US Medical Response to Unsolicited Requests for Information
Distribution is Strictly ProhibitedMU-US-0036a
Phase 2 Multiple-Ascending Dose, Open-Label Study in Medically Stable SMA Patients 2-15 Years of AgeStudy Complete
Objectives
Evaluate the safety and tolerability of multiple intrathecal doses of ISIS-SMNRx
Evaluate CSF, plasma PK, and clinical outcomes related to SMA (including HMFSE)
Darras, B et al. Interim Results of a Phase 2 Study of ISIS-SMNRx in Children with Spinal Muscular Atrophy. Presented at AAN 2014

68For US Medical Response to Unsolicited Requests for Information
Distribution is Strictly ProhibitedMU-US-0036a
Dose and Time Dependent Increases in HFMSE Scores after Multiple Doses of ISIS-SMNR*
Darras, B et al. Interim Results of a Phase 2 Study of ISIS-SMNRx in Children with Spinal Muscular Atrophy. Presented at AAN 2014*Study is now complete; data presented above is for first 3 cohorts, 12 mg data cohort not yet available (as of May 2015)

69For US Medical Response to Unsolicited Requests for Information
Distribution is Strictly ProhibitedMU-US-0036a
ISIS-SMNRx Phase 3 Study (ENDEAR)*
A Phase 3, randomized, double-blind, sham-procedure controlled study in infants with SMA
–Global study in ~110 SMA infants ≤ 7 months old with 2 copies of SMN2
–13 month study duration
Evaluate the efficacy and safety of ISIS-SMNRx
–Primary efficacy endpoint is time to death/permanent ventilation
–Additional efficacy endpoints include CHOP INTEND and motor milestones
Initiated - August 2014
Darras, B et al. Interim Results of a Phase 2 Study of ISIS-SMNRx in Children with Spinal Muscular Atrophy. Presented at AAN 2014*Link to study details at https://clinicaltrials.gov/ct2/show/NCT02193074?term=ENDEAR&rank=1

70For US Medical Response to Unsolicited Requests for Information
Distribution is Strictly ProhibitedMU-US-0036a
ISIS-SMNRx Phase 3 Study (CHERISH)*
A Phase 3, Randomized, Double-blind, Sham-Procedure Controlled Study in Children with SMA
–Global study in ~120 SMA children with SMA
–15 month study duration
Determine the efficacy and safety of ISIS-SMNRx
–Primary endpoint is change in Hammersmith motor function score
Initiated - 2014
Darras, B et al. Interim Results of a Phase 2 Study of ISIS-SMNRx in Children with Spinal Muscular Atrophy. Presented at AAN 2014*Link to study details at https://clinicaltrials.gov/ct2/show/NCT02292537?term=CHERISH&rank=2

71For US Medical Response to Unsolicited Requests for Information
Distribution is Strictly ProhibitedMU-US-0036a
Aducanumab (BIIB037)*
Alzheimer’s Disease
*BIIB037 is an investigational candidate. Efficacy and safety have not been established.

72For US Medical Response to Unsolicited Requests for Information
Distribution is Strictly ProhibitedMU-US-0036a
Alzheimer’s Disease (AD)
1. 2014 Alzheimer’s Disease Facts and Figures. 2. Alzheimer’s Disease International 2010. 3. http://www.nia.nih.gov/alzheimers/topics/treatment*All trademarks for drugs mentioned are the property of their respective owners
Prevalence–Alzheimer’s disease (AD) is the most common cause of dementia, accounting for 60% to 80%
of all cases1
–Estimated that 5.2 million Americans suffer from dementia caused by AD in the US1 and 35.6 million people living with dementia worldwide2
»Estimated to increase to 115.4 million worldwide by 20502
Current Approved Treatments*–Mild to Moderate AD - ARICEPT® (Donepezil), EXELON® (Rivastigmine), RAZADYNE®
(Galantamine)
–Moderate to Severe AD - ARICEPT ® (Donepezil), NAMENDA® (Memantine)
–Current treatments regulate neurotransmitters in the brain which may help to improve thinking, memory, and speaking skills.
–However, current therapies do not modify the underlying disease process and may not be effective for all patients affected by AD2

73For US Medical Response to Unsolicited Requests for Information
Distribution is Strictly ProhibitedMU-US-0036a
Aducanumab (BIIB037)
• AD is defined by the presence of extracellular neuritic
plaques (NPs) containing amyloid beta (Aβ) peptide
and intraneuronal neurofibrillary tangles (NFTs)
composed of tau protein in the brain1
• BIIB037 is a human monoclonal antibody that targets
aggregated forms of beta amyloid
• Therapeutic rationale: Clearance of aggregated Aβ in
the brain will attenuate the neurodegenerative
process and slow the clinical progression of AD2
1. Hardy and Selkoe. Science. 2002; 197(5580):353-356 , 2 Data on File. Biogen.

74For US Medical Response to Unsolicited Requests for Information
Distribution is Strictly ProhibitedMU-US-0036a
Aducanumab (BIIB037)*
• Recently completed a pre-specified interim analysis of Phase 1b
• Phase 1b study is a randomized blinded placebo controlled ascending dose study in prodromal and mild AD patients who are also amyloid positive in the brain at baseline
• Interim analysis indicated that BIIB037 reduced amyloid levels in a dose and time dependent fashion. Other preliminary findings:
–Statistically significant effect on cognition at 54 weeks
–Most significant safety findings have been amyloid-related imaging abnormalities (ARIAs). These events appear to be both dose and ApoE4 dependent, largely mild to moderate and self-resolving
• Continuing the current Phase 1b study in a blinded fashion
• Preparing to implement Phase 3 program
*As of May 2015Data on File. Biogen

75For US Medical Response to Unsolicited Requests for Information
Distribution is Strictly ProhibitedMU-US-0036a
Aducanumab (BIIB037) Interim Phase 1B AnalysisEffect on Mini Mental State Examination (MMSE)
*P<0.05 vs placebo
MMSE = mini-mental state examination; SE = standard error
MMSE is an exploratory endpoint. Analyses based on observed data. ANCOVA for change from baseline with factors of treatment, laboratory ApoE ε4 status (carrier and non-carrier), and baseline MMSE. Efficacy analysis population is defined as all randomized subjects who received ≥1 dose of study medication and had ≥1 post-baseline questionnaire assessment.
Sevigny J, et al. Randomized, Double-blind, Placebo-controlled, Phase 1b Study of Aducanumab (BIIB037), an Anti-Aβ Monoclonal Antibody, in Patients With Prodromal or Mild Alzheimer’s Disease: Interim Results by Disease Stage and ApoE ε4 Status. Presented at 2015 AAN Congress, Washington, DC.
76For US Medical Response to Unsolicited Requests for Information
Distribution is Strictly ProhibitedMU-US-0036a
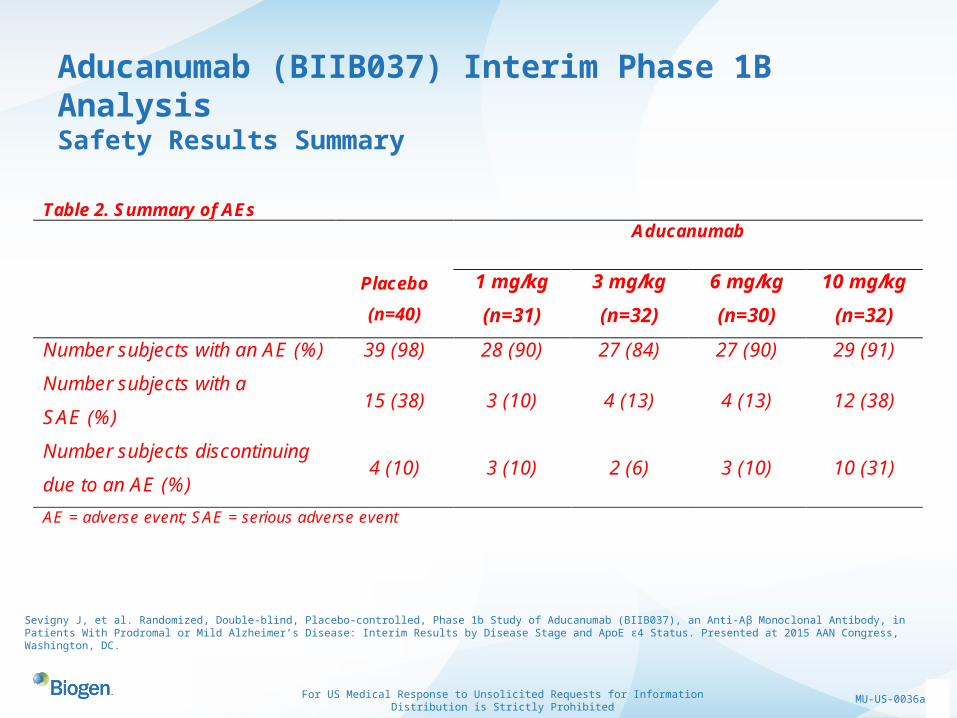
Aducanumab (BIIB037) Interim Phase 1B AnalysisSafety Results Summary
Table 2. Summary of AEs Aducanumab
Placebo
(n=40)
1 mg/kg
(n=31)
3 mg/kg
(n=32)
6 mg/kg
(n=30)
10 mg/kg
(n=32)
Number subjects with an AE (%) 39 (98) 28 (90) 27 (84) 27 (90) 29 (91)
Number subjects with a
SAE (%) 15 (38) 3 (10) 4 (13) 4 (13) 12 (38)
Number subjects discontinuing
due to an AE (%) 4 (10) 3 (10) 2 (6) 3 (10) 10 (31)
AE = adverse event; SAE = serious adverse event
Sevigny J, et al. Randomized, Double-blind, Placebo-controlled, Phase 1b Study of Aducanumab (BIIB037), an Anti-Aβ Monoclonal Antibody, in Patients With Prodromal or Mild Alzheimer’s Disease: Interim Results by Disease Stage and ApoE ε4 Status. Presented at 2015 AAN Congress, Washington, DC.
77For US Medical Response to Unsolicited Requests for Information
Distribution is Strictly ProhibitedMU-US-0036a
BAN2401*
Alzheimer’s Disease
*BAN2401 is an investigational candidate. Efficacy and safety have not been established.

78For US Medical Response to Unsolicited Requests for Information
Distribution is Strictly ProhibitedMU-US-0036a
BAN2401• Suggested that amyloid beta (Aβ)
protofibril, an intermediate in the
aggregation process of the amyloid-β
peptide, initiates and drives the
neurodegenerative process in Alzheimer’s
disease
• BAN2401 is a humanized monoclonal
antibody that specifically targets the
protofibrillar form of Aβ1
• Currently in phase 2 expected to be
completed by 20162
• Collaboration with Eisai Co.
1. www.eisai.com/news/news201044.html, 2. www.clinicaltrials.gov NCT01767311Data on File. Biogen

79For US Medical Response to Unsolicited Requests for Information
Distribution is Strictly ProhibitedMU-US-0036a
BG00011*Idiopathic Pulmonary Fibrosis (IPF)
*BG00011 is an investigational candidate. Efficacy and safety have not been established.

80For US Medical Response to Unsolicited Requests for Information
Distribution is Strictly ProhibitedMU-US-0036a
Idiopathic Pulmonary Fibrosis (IPF)
Prevalence
–Approximately 100,000 people in the United States have IPF
–Most people diagnosed with IPF only live 3 to 5 years after diagnosis. Most common cause of death is respiratory failure1
Figure: National Heart, Lung, and Blood Institute website. “How the Lungs Work”1. United States National Library of Medicine website. “Idiopathic Pulmonary Fibrosis”

81For US Medical Response to Unsolicited Requests for Information
Distribution is Strictly ProhibitedMU-US-0036a
Idiopathic Pulmonary Fibrosis (IPF)• Two therapies recently approved for the treatment of IPF
–ESBRIET® (pirfenidone) was approved in the US on October 15, 2014
»The mechanism of action is unknown1
–OFEV® (nintedanib) was approved in the US on October 16th, 2014
»Nintedanib is a tyrosine kinase inhibitor (TKI) that targets growth factor receptors involved in the mechanisms by which pulmonary fibrosis occurs. It inhibits the platelet-derived growth factor (PDGFR), fibroblast growth factor receptor (FGFR), and vascular endothelial growth factor receptor (VEGFR)2
ESBRIET® is a registered trademark of Intermune. OFEV® is a registered trademark of Boehringer ingelheim1. http://www.roche.com/media/media_releases/2. http://www.boehringer-ingelheim.com/news/news_releases/press_releases/2014/16_october_2014.html

82For US Medical Response to Unsolicited Requests for Information
Distribution is Strictly ProhibitedMU-US-0036a
BG00011 (anti-αvβ6 mAb)• αvβ6 integrin is expressed in low levels on alveolar
epithelial cells in normal healthy adults and is tightly regulated by transforming growth factor-β (TGF-β); αvβ6 is upregulated with tissue injury
• αvβ6 blockade provides a mechanism for injury-specific attenuation of TGF-β activation, inhibiting fibrogenesis
• αvβ6 blockade provides a mechanism for injury-specific attenuation of TGF-β activity1
• BG00011 is a humanized monoclonal antibody targeting integrin αvβ6.
• BG00011, preclinically, exhibits anti-fibrotic activity in models of lung, kidney and liver disease. 2
• Phase 2 studying patients with IPF; estimated completion 20153
1. www.pffsummit.org/assets/pro_sat_1500_biogen_ppt.pdf2. BI1IB Press Release. 2009.3. wwwl.clinicaltrials.gov NCT01371305

83For US Medical Response to Unsolicited Requests for Information
Distribution is Strictly ProhibitedMU-US-0036a
Questions?