1 emergent and re-emergent challenges in the theory of infectious diseases south africa june, 2007
Post on 22-Dec-2015
214 views
TRANSCRIPT
1 Emergent and re-emergent challenges in
the theory of infectious diseases
www.noveltp.com
South AfricaJune, 2007

2
The theory of infectious diseases has a rich history
Sir Ronald RossSir Ronald Ross 1857-19321857-1932
3
But prediction is difficultBut prediction is difficult
• Disease systems are complex, characterized by nonlinearities and sudden flips
image.guardian.co.uk/

4
• They also are complex adaptive systemscomplex adaptive systems, integrating phenomena at multiple scales
encarta.msn.com
QuickTime™ and aTIFF (Uncompressed) decompressor
are needed to see this picture.
www.who.intwww.nobel.org
lshtm.ac.uk
QuickTime™ and aTIFF (Uncompressed) decompressor
are needed to see this picture.

5
Integrating these multiple scales is one major challenge
• Pathogen
• Host individual
• Host population dynamics
• Pathogen genetics
• Host genetics
• Vector

6
Despite a century of elegant theory, new diseases emerge, old reemerge
http://edie.cprost.sfu.ca/gcnet

7
Significant management puzzles remain
• Whom should we vaccinate?Whom should we vaccinate?
QuickTime™ and aTIFF (Uncompressed) decompressor
are needed to see this picture.
www.calcsea.org

8
Whom should we vaccinate?
• Those at greatest risk?Those at greatest risk?
QuickTime™ and aTIFF (Uncompressed) decompressor
are needed to see this picture.
www.nursingworld.org
QuickTime™ and aTIFF (Uncompressed) decompressor
are needed to see this picture.
9
Whom should we vaccinate?
• Or those who pose greatest risk to others?Or those who pose greatest risk to others?
www-personal.umich.edu/~mejn
QuickTime™ and aTIFF (Uncompressed) decompressor
are needed to see this picture.
10
Other management puzzles:Problems of the Commons
• Individual benefits/costs vs. group benefits/costsIndividual benefits/costs vs. group benefits/costs– VaccinationVaccination– Antibiotic useAntibiotic use
• Hospitals and nursing homes vs. health-care Hospitals and nursing homes vs. health-care providers vs. individualsproviders vs. individuals
These introduce game-theoretic problemsThese introduce game-theoretic problems
11
Antibiotic resistance threatens the effectiveness of our most potent
weapons against bacterial infections
QuickTime™ and aTIFF (Uncompressed) decompressor
are needed to see this picture.

12
Lecture outline
• Periodicities and fluctuationsPeriodicities and fluctuations
• Antibiotic resistance and other problems of the Antibiotic resistance and other problems of the CommonsCommons
13
Many important diseases exhibit oscillations on multiple temporal and
spatial scales

14
Measles in the U.K.; Grenfell et al. 2001 (Nature)
QuickTime™ and aBMP decompressor
are needed to see this picture.

15
Control must deal with temporal and spatial fluctuationsControl must deal with temporal and spatial fluctuations
QuickTime™ and aCinepak decompressor
are needed to see this picture.

16
Influenza global spreadInfluenza global spread
17
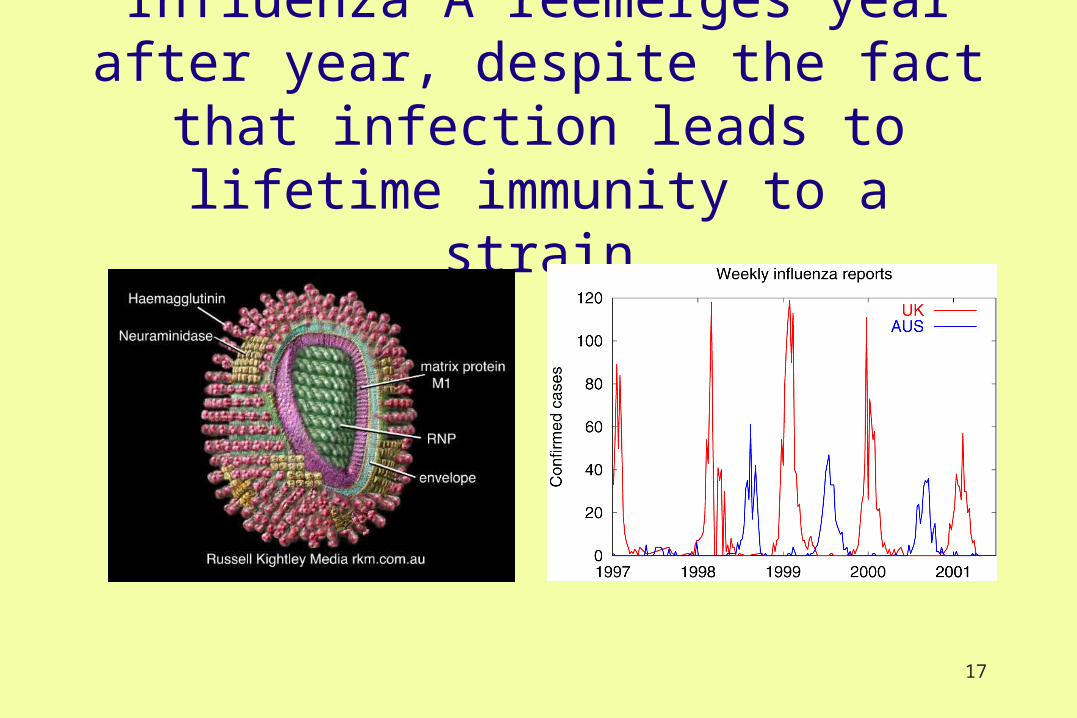
Influenza A reemerges year after year, despite the fact that infection leads to
lifetime immunity to a strain

18
19
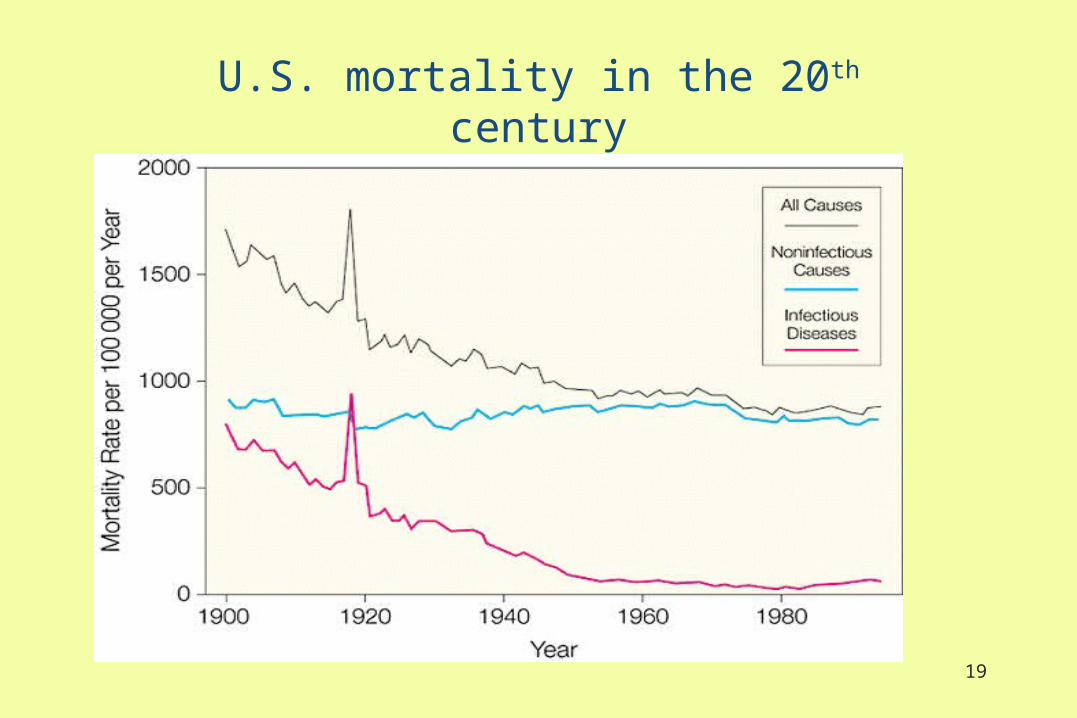
U.S. mortality in the 20th century

20
The “Spanish Flu” of 1918

21

22
Bush, Fitch, Cox

23
Timeseries of viral clusters

24
Fluctuations in influenza A
• Rapid replacement at level of individual strainsRapid replacement at level of individual strains
• Gradual replacement at level of subtypesGradual replacement at level of subtypes
• Recurrence at level of clustersRecurrence at level of clusters

25
Standard SIR Model(No latency)
SusceptibleS RemovedR
Infectious I
26
Simplest model
dI /dt SI I Ideaths recovered

27
R0 N 1
1
Secondaryinfections/
time
Average infectious
period
Thus R0 is the #secondary/primary infection.
Condition for spread in a naïve populationCondition for spread in a naïve population
Rs S
1For spread: For spread:

28
Interpretation if threshold is exceeded
1. 1. With no new recruits, outbreak and collapseWith no new recruits, outbreak and collapse
2.2. With new births, get stable equilibriumWith new births, get stable equilibrium
3.3. Oscillations require a more complicated modelOscillations require a more complicated model

29
Complications
• New immigrantsNew immigrants
QuickTime™ and aTIFF (Uncompressed) decompressor
are needed to see this picture.
www.lareau.org
H.M.S. BountyH.M.S. Bounty

30
Complications
• New immigrantsNew immigrants
• DemographyDemography
QuickTime™ and aTIFF (Uncompressed) decompressor
are needed to see this picture.
www.lareau.org

31
Complications
• New immigrantsNew immigrants
• DemographyDemography
• Heterogeneous mixing patternsHeterogeneous mixing patterns
QuickTime™ and aTIFF (Uncompressed) decompressor
are needed to see this picture.
www.lareau.org
32
Complications
• New immigrantsNew immigrants
• DemographyDemography
• Heterogeneous mixing patternsHeterogeneous mixing patterns
• Genetic changes in hostGenetic changes in host
QuickTime™ and aTIFF (Uncompressed) decompressor
are needed to see this picture.
www.lareau.org

33
Complications
• New immigrantsNew immigrants
• DemographyDemography
• Heterogeneous mixing patternsHeterogeneous mixing patterns
• Genetic changes in hostGenetic changes in host
• Multiple strains/diseasesMultiple strains/diseases
QuickTime™ and aTIFF (Uncompressed) decompressor
are needed to see this picture.
www.lareau.org

34
Complications
• New immigrantsNew immigrants
• DemographyDemography
• Heterogeneous mixing patternsHeterogeneous mixing patterns
• Genetic changes in hostGenetic changes in host
• Multiple strains/diseasesMultiple strains/diseases
• VectorsVectors
QuickTime™ and aTIFF (Uncompressed) decompressor
are needed to see this picture.
www.lareau.org

35
Complications
• New immigrantsNew immigrants
• DemographyDemography
• Heterogeneous mixing patternsHeterogeneous mixing patterns
• Genetic changes in hostGenetic changes in host
• Multiple strains/diseasesMultiple strains/diseases
• VectorsVectors
QuickTime™ and aTIFF (Uncompressed) decompressor
are needed to see this picture.
www.lareau.org

36
Oscillations
• Stochastic factorsStochastic factors
• Seasonal forcing (e.g., in transmission rates)Seasonal forcing (e.g., in transmission rates)
• Long periods of temporary immunityLong periods of temporary immunity
• Other explicit delays (e.g., incubation periods)Other explicit delays (e.g., incubation periods)
• Age structureAge structure
• Non-constant population sizeNon-constant population size
• Non-bilinear transmission coefficientsNon-bilinear transmission coefficients
• Interactions with other diseases/strainsInteractions with other diseases/strains

37
Oscillations
• Stochastic factorsStochastic factors
• Seasonal forcing (e.g., in transmission rates)Seasonal forcing (e.g., in transmission rates)
• Long periods of temporary immunityLong periods of temporary immunity
• Other explicit delays (e.g., incubation periods)Other explicit delays (e.g., incubation periods)
• Age structureAge structure
• Non-constant population sizeNon-constant population size
• Non-(bilinear) transmission coefficientsNon-(bilinear) transmission coefficients
• Interactions with other diseases/strainsInteractions with other diseases/strains

38
Oscillations
• Stochastic factorsStochastic factors
• Seasonal forcing (e.g., in transmission rates)Seasonal forcing (e.g., in transmission rates)
• Long periods of temporary immunityLong periods of temporary immunity
• Other explicit delays (e.g., incubation periods)Other explicit delays (e.g., incubation periods)
• Age structureAge structure
• Non-constant population sizeNon-constant population size
• Non-(bilinear) transmission coefficientsNon-(bilinear) transmission coefficients
• Interactions with other diseases/strainsInteractions with other diseases/strains

39
Oscillations
• Stochastic factorsStochastic factors
• Seasonal forcing (e.g., in transmission rates)Seasonal forcing (e.g., in transmission rates)
• Long periods of temporary immunityLong periods of temporary immunity
• Other explicit delays (e.g., incubation periods)Other explicit delays (e.g., incubation periods)
• Age structureAge structure
• Non-constant population sizeNon-constant population size
• Non-(bilinear) transmission coefficientsNon-(bilinear) transmission coefficients
• Interactions with other diseases/strainsInteractions with other diseases/strains

40
Oscillations
• Seasonal forcing (e.g., in transmission rates)Seasonal forcing (e.g., in transmission rates)
– Can interact with endogenous oscillations to produce Can interact with endogenous oscillations to produce chaoschaos
• Age structureAge structure
– Creates implicit delaysCreates implicit delays
• Interactions with other diseases/strainsInteractions with other diseases/strains
– Includes, therefore, genetic change in pathogenIncludes, therefore, genetic change in pathogen

41
Susceptible
Infectious 2
Recovered 2
Infectious 1
Infectious 1 Recovered 1,2
Recovered 1
Infectious 2
Interacting strains or diseasesInteracting strains or diseases
R2
R1

42
Understanding endogenous oscillations
• Age-structured models can produce damped Age-structured models can produce damped oscillations (Schenzele, Castillo-Chavez et al.)oscillations (Schenzele, Castillo-Chavez et al.)
• Two-strain models can produce damped Two-strain models can produce damped oscillations (Castillo-Chavez et al.) oscillations (Castillo-Chavez et al.)
• Coupling these may lead to sustained periodic or Coupling these may lead to sustained periodic or other oscillationsother oscillations

43
Summary:Understanding endogenous oscillations
• Age-structure Age-structure
• Epidemiology Epidemiology
• GeneticsGenetics
all have characteristic scales of oscillation that can all have characteristic scales of oscillation that can interact with each other, and with seasonal forcing interact with each other, and with seasonal forcing

44
Lecture outline
• Periodicities and fluctuationsPeriodicities and fluctuations
• Antibiotic resistance and other problems of the Antibiotic resistance and other problems of the CommonsCommons

45
Problems of The Commons
• FisheriesFisheries
• AquifersAquifers
• PollutionPollutionQuickTime™ and a
TIFF (Uncompressed) decompressorare needed to see this picture.
www.aisobservers.com

46
Problems of The Commons
• FisheriesFisheries
• AquifersAquifers
• PollutionPollution
• VaccinesVaccines
pubs.acs.org
QuickTime™ and aTIFF (Uncompressed) decompressor
are needed to see this picture.
images.usatoday.com

47
Problems of The Commons
• FisheriesFisheries
• AquifersAquifers
• PollutionPollution
• VaccinesVaccines
• AntibioticsAntibiotics
www.bath.ac.uk

48
Antibiotic resistance is on the rise
www.wellcome.ac.uk

49

50
Would you deny your child antibiotics to maintain global effectiveness?

51
Antibiotic resistance is an increasing problem
We are rapidly losing the benefits We are rapidly losing the benefits antibiotics have given us against a wide antibiotics have given us against a wide
spectrum of diseasesspectrum of diseases

52

53

54
Reasons for rise of antibiotic resistance
• Agricultural usesAgricultural uses
• Overuse by physiciansOveruse by physicians
• Hospital spread (nosocomial infections)Hospital spread (nosocomial infections)
www.history.navy.mil/ac

55
Hospitals are a major source of spread
Methicillin-resistant Staphylococcus aureus (MRSA) and vancomycin-resistant Enterococcus (VRE) isolates by hospital day of admission. Early peak corresponds to patients entering the hospital with MRSA or VRE bacteremia. Later peak likely represents nosocomial acquisition. (San Francisco County)
Huang et al, Emerging Infectious Diseases, 2002

56www.mja.com.au
Antibiotic resistance spreads to novel bacteriaAntibiotic resistance spreads to novel bacteria

57
Antibiotic useAntibiotic use
• Hospitals and communities create a metapopulation framework (Lipsitch et al; Smith Smith et al)
• Spatially- explicit strategies could help
• Economics dominates control
58
Individuals may harbor ARB on admission…carriers
• How do increases in the general population contribute How do increases in the general population contribute to infections by ARB in the hospital, and what can be to infections by ARB in the hospital, and what can be done about it?done about it?
• Develop metapopulation models exploring colonization Develop metapopulation models exploring colonization of hosts by antibiotic resistant strainsof hosts by antibiotic resistant strains

59
Individual movementBasic model structure
Smith et al, PNAS 2004
i indicates group, such as elderlyi indicates group, such as elderlyj,k indicate subpopulations, such as hospital, communityj,k indicate subpopulations, such as hospital, communityq indicates proportion (fixed)q indicates proportion (fixed)Model assumes admit=dischargeModel assumes admit=discharge
kk

60
Bigger hospitals have bigger problems

61
Hospitals in larger cities have larger problems
62
Smith, Levin, Laxminarayan
• Consider a game among hospitalsConsider a game among hospitals
• Compute optimal investment for a single hospital Compute optimal investment for a single hospital in controlling antibiotic resistancein controlling antibiotic resistance
• Compute game-theoretic optimal strategy in a Compute game-theoretic optimal strategy in a mixed population, with discountingmixed population, with discounting
• Investment decreases with city sizeInvestment decreases with city size

63
Conclusions
• Infectious diseases have a rich modeling historyInfectious diseases have a rich modeling history
• Great challenges for behavioral sciencesGreat challenges for behavioral sciences
• Relevant methods will span a broad range Relevant methods will span a broad range