1. clinical utility of serum ferritin final
TRANSCRIPT

CLINICAL UTILITY OF SERUM FERRITIN
SIDDHARTH MED- 1ST YEAR

OUTLINE
SCOPE AND PURPOSE INTRODUCTION CLINICAL APPLICATION 1. Low serum ferritin 2. High serum ferritin TAKE HOME FLOW CHART
SCOPE AND PURPOSEFerritin measurements and corresponding
cut-offs facilitate the monitoring of iron deficiency trends and the assessment of
the impact of health and nutrition interventions.
Goal is to prevent and control iron deficiency and provide the basis for
advocacy programs for iron deficiency and anemia prevention in vulnerable
populations.

INTRODUCTION Its an iron storage protein.
Its primary role is in iron sequestration.
Iron is toxic, because of its capacity to generate reactive species, which has the capacity to damage DNA and proteins.
Normal range: 50-200 ug/L.
CLINICAL APPLICATIONSLOW
SERUM FERRITI
N
1. Most useful in
iron deficiency (<15ug/L)
2. Hypothyroidism
3. Ascorbate deficiency

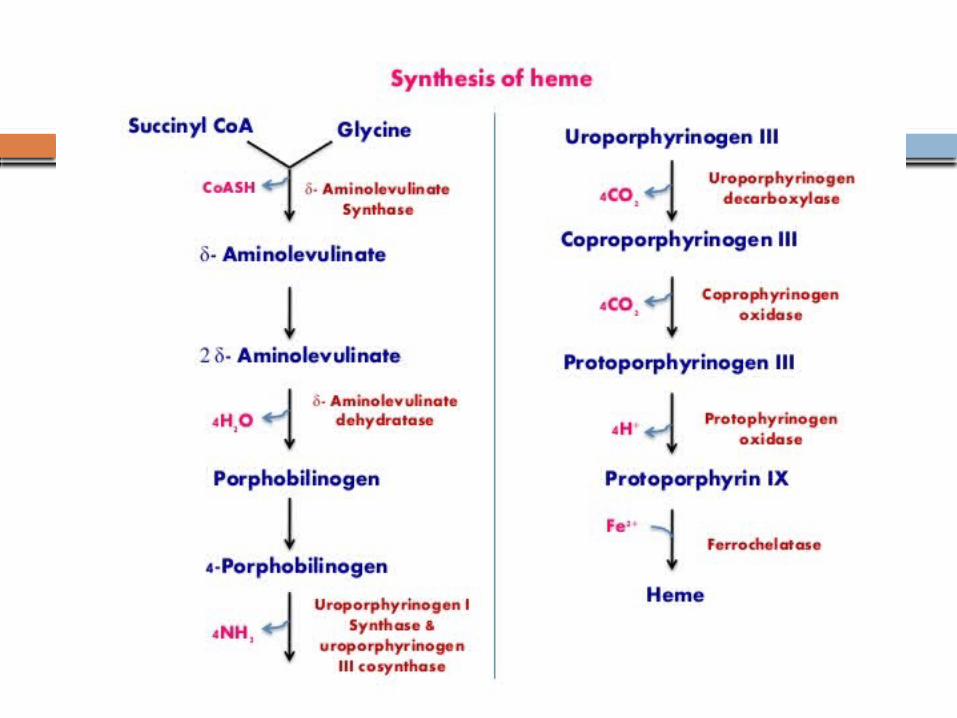
PHYSIOLOGY

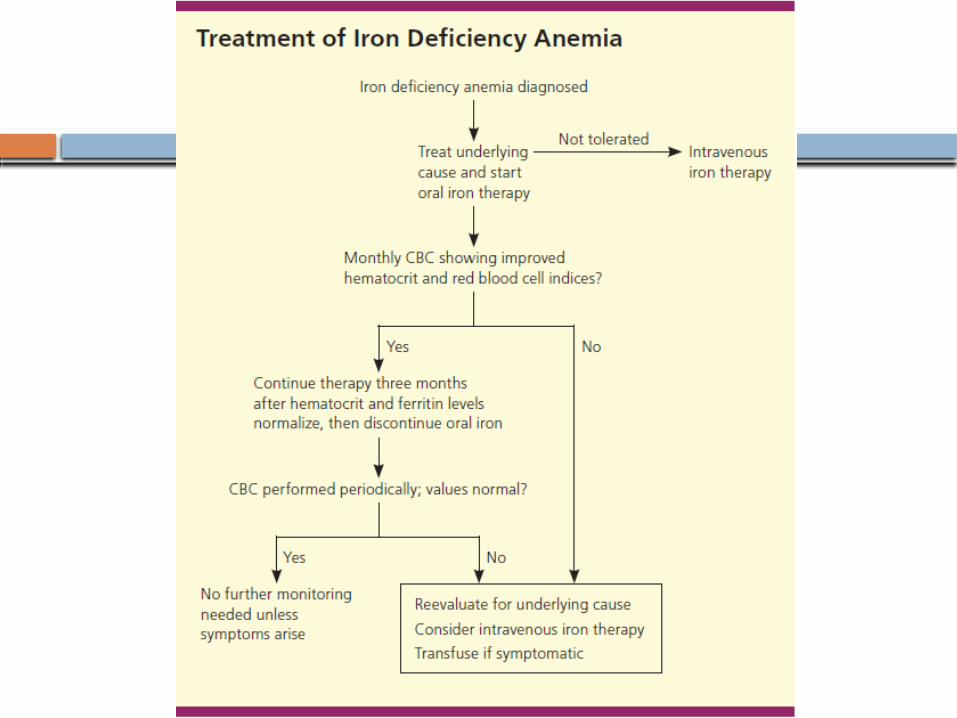
IRON DEFICIENCY ANEMIACAUSES:
1. Increase demand for iron:
-Infancy, adolescence, pregnancy,
erythropoietin therapy.
2. Increased iron loss:
-Acute/chronic blood loss, menses,
blood donation & phlebotomy.
3. Decreased iron intake/absorption
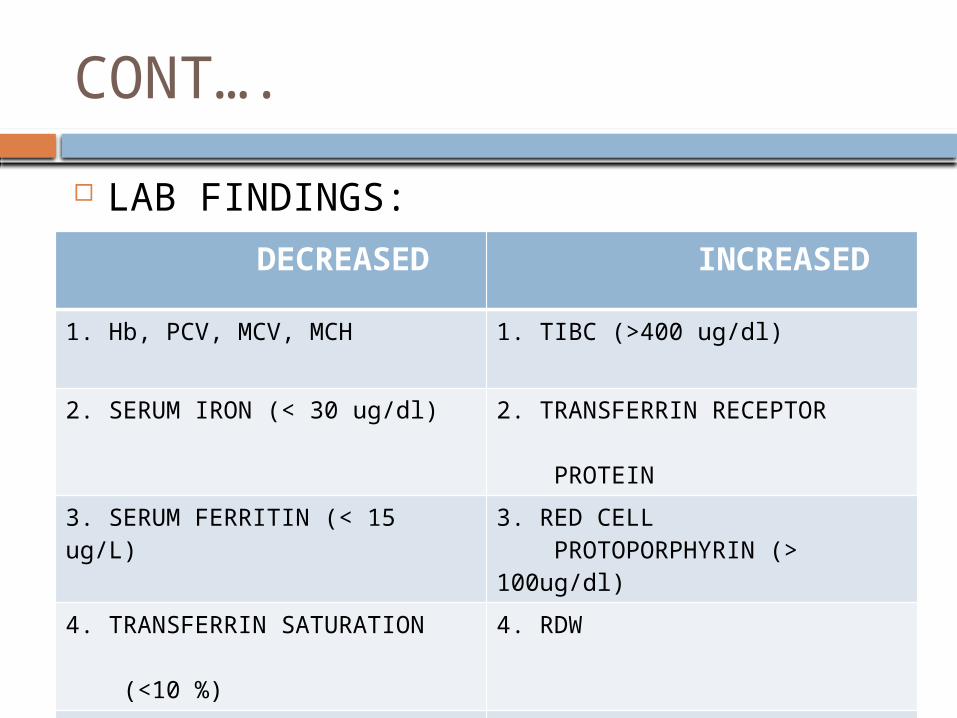
CONT…. LAB FINDINGS: DECREASED INCREASED
1. Hb, PCV, MCV, MCH 1. TIBC (>400 ug/dl)
2. SERUM IRON (< 30 ug/dl) 2. TRANSFERRIN RECEPTOR PROTEIN
3. SERUM FERRITIN (< 15 ug/L) 3. RED CELL PROTOPORPHYRIN (> 100ug/dl)
4. TRANSFERRIN SATURATION (<10 %)
4. RDW
5. BONE MARROW IRON STORES


CONT….
RE iron stores can be estimated from iron stain of bone marrow aspirate or biopsy ( gold std ).
This is largely “replaced by measuring serum ferritin levels”.
Serum ferritin level is a better indicator of iron overload than the marrow stain.

CONT….IRON STORES FERRITIN
LEVELS (ug/L)MARROW IRON STAIN
0 < 15 0
1-300 mg 15-30 TRACE TO 1+
300-800 mg 30-60 2 +
800-1000 mg 60-150 3 +
1-2 g > 150 4 +
IRON OVERLOAD > 500 - 1000 -


CLINICAL IMPORTANCETESTS IRON
DEFICIENCYINFLAMMATION
ANEMIA MILD TO SEVERE MILD
MCV 60-90 80-90
SERUM IRON <30 <50
TIBC >360 <300
SATURATION (%) < 10 10-20
FERRITIN (ug/L) <15 30-200
IRON STORES 0 2-4 +

CLINICAL APPLICATIONSHIGH SERUM
FERRITIN
1. Iron overload
2. Acute inflammatory
conditions
3. Liver disease
4. Alcohol excess
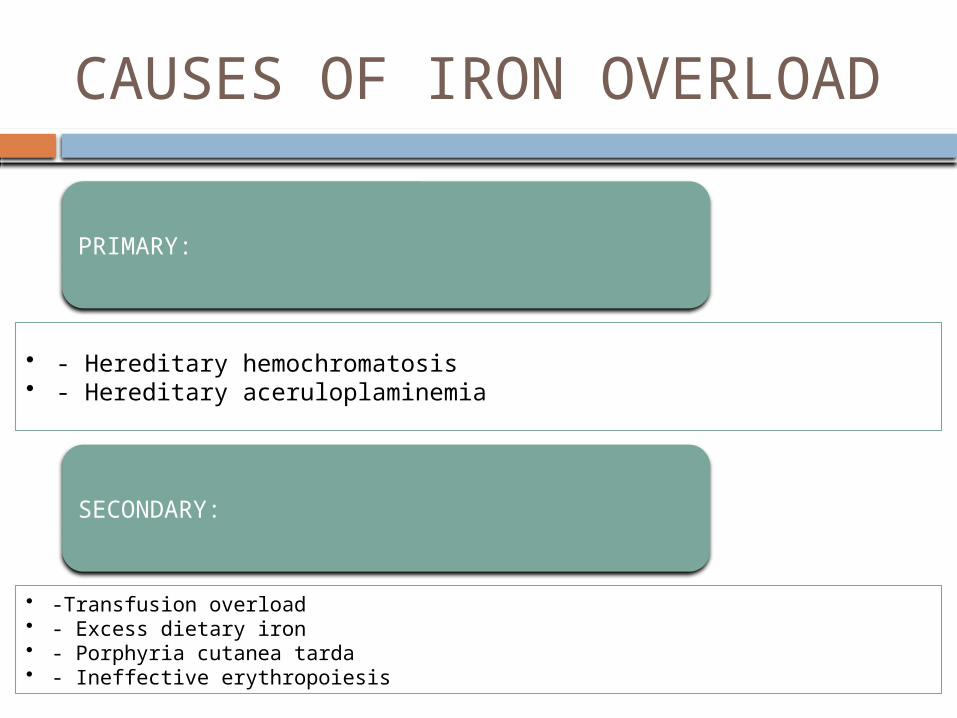
CAUSES OF IRON OVERLOADPRIMARY:
• - Hereditary hemochromatosis• - Hereditary aceruloplaminemia
SECONDARY:
• -Transfusion overload• - Excess dietary iron• - Porphyria cutanea tarda• - Ineffective erythropoiesis

HERIDITARY HEMOCHROMATOSES
Autosomal recessive disorder with mutation in HFE gene (substitution of tyrosine for cysteine at amino acid 282.
Homozygous patients have 50-75 % chance of developing iron overload.
Hetrozygous are unlikely to develop the disease, but transmit gene mutation to the children.

CONT….
Routine screening is recommended in first degree relatives of patients with confirmed diagnosis.
Screening involves use of ferritin and transferin saturation. Current recommendation suggest elevated ferritin with TSAT >45% should prompt genetic confirmation.
Levels >1000 ug/L usually poses high risk for cirrhosis.

WILSONS DISEASE
Rare disorder due to mutation in chromosome 13.
It causes marked hyperferritinemia as well as copper overload.
It can be distinguished from HH by low serum transferrin saturation and an undetectable serum ceruloplasmin concentration.

SECONDARY IRON OVERLOAD
Chronic transfusion therapy is a mainstay of therapy for children and adults with thalassemia major. Iron gets deposited first in RE system prior to loading within the heart and liver. It ultimately results in heart & liver failure.
Excessive intake of dietary iron.

CONT….
Porphyria cutanea tarda usually manifests as cutaneous photosensitivity and hepatic iron overload. It is diagnosed by increased urinary and fecal porphyrin excretion.
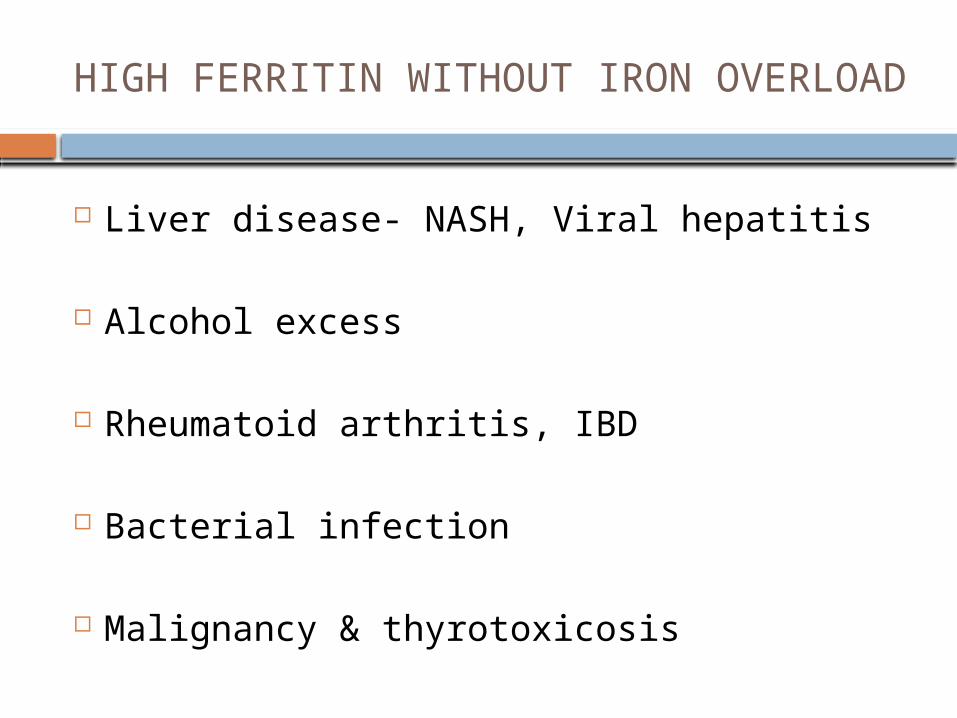
HIGH FERRITIN WITHOUT IRON OVERLOAD
Liver disease- NASH, Viral hepatitis
Alcohol excess
Rheumatoid arthritis, IBD
Bacterial infection
Malignancy & thyrotoxicosis

ANEMIA OF CHRONIC DISEASE
Associated with release of pro-inflammatory cytokines & hepcidin.
Features of anemia are brought about by inadequate iron delivery to the marrow, despite normal or increased iron stores.
Typically serum ferritin levels increase by threefold over basal levels.


CONT….CHRONIC INFECTIONS:
- HIV, Osteomyelitis, Tuberculosis
COLLAGEN VASCULAR DISEASE:
- SLE, RA, POLYMYOSITIS, POLY ARTERITIS NODOSA
CKD, IBD
MALIGNANCY
INFLAMMATORY CONDITIONS
STILLS DISEASE:
1. Characterized by fever, arthritis & rash. 2. Elevated serum ferritin levels were seen in 89 % of these patients in recent
series.3. Whether disproportionate ferritin response is a pathogenic mechanism or
is a by- product of inflammation remains
unknown.

LIVER DISEASES STEATOHEPATITIS: - Increased ferritin with normal
tranferrin saturation is seen with hepatic steatosis.
- It is thought to be due to the combination of disrupted glucose, lipid and iron metabolism.

CONT… VIRAL HEPATITIS:
- Hepatitis A,B,C,D, EBV & CMV will cause an elevation in serum ferritin indicative of liver inflammation.
- Chronic hepatitis C or B may be less obvious clinically & serologies should be checked if there is minimal disturbance of liver enzymes in cases of unexplained hyperferritinemia.
ALCOHOL EXCESS Regular alcohol consumption is
responsible for disruption of normal iron metabolism.
It results in excess iron deposition in the liver, in one third of alcohol subjects.
This elevation of serum ferritin can occur without elevation of other liver enzymes.
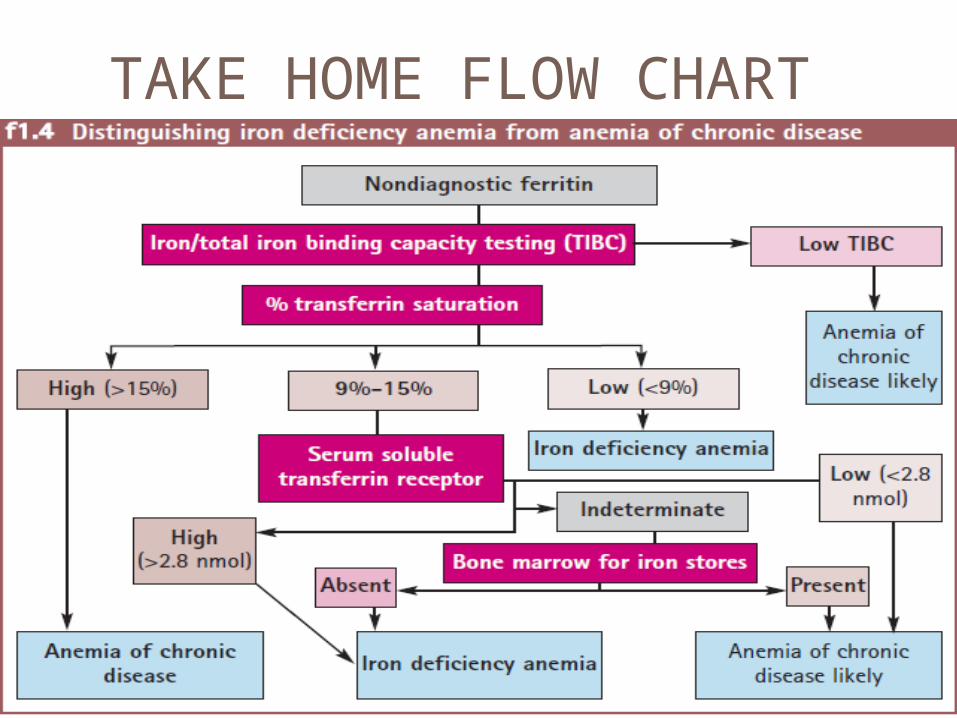
TAKE HOME FLOW CHART
REFERENCES
HARRISONS PRINCIPLES OF INTERNAL MEDICINE.
WINTROBE’S CLINICAL HEMATOLOGY
WILLIAMS MANUAL OF HEMATOLOGY
ASSOCIATION OF HEMATOLOGY 2014

THANK YOU