1 ayesha-periodontal ligament
TRANSCRIPT

Presented by:
Dr.Ayesha Taha
JR I
Department of Pedodontics
and Preventive Dentistry
SPPGIDMS, Lucknow
•Periodontal ligament is a part of the Periodontium.
• Periodontal Ligament is a dense fibrous connective tissue that occupies the periodontal space which is located between the cementum and the alveolar bone.
• It extends coronally to the most apical part of lamina propria of gingiva .
• At apically it extends till the apical part foramen and is continuous with the dental pulp.
• The average width of periodontal ligament space is documented to be about 0.2 mm, though considerable variation exists.
Periodontium
Gingiva
Periodontal Ligament
Alveolar Bone
Cementum
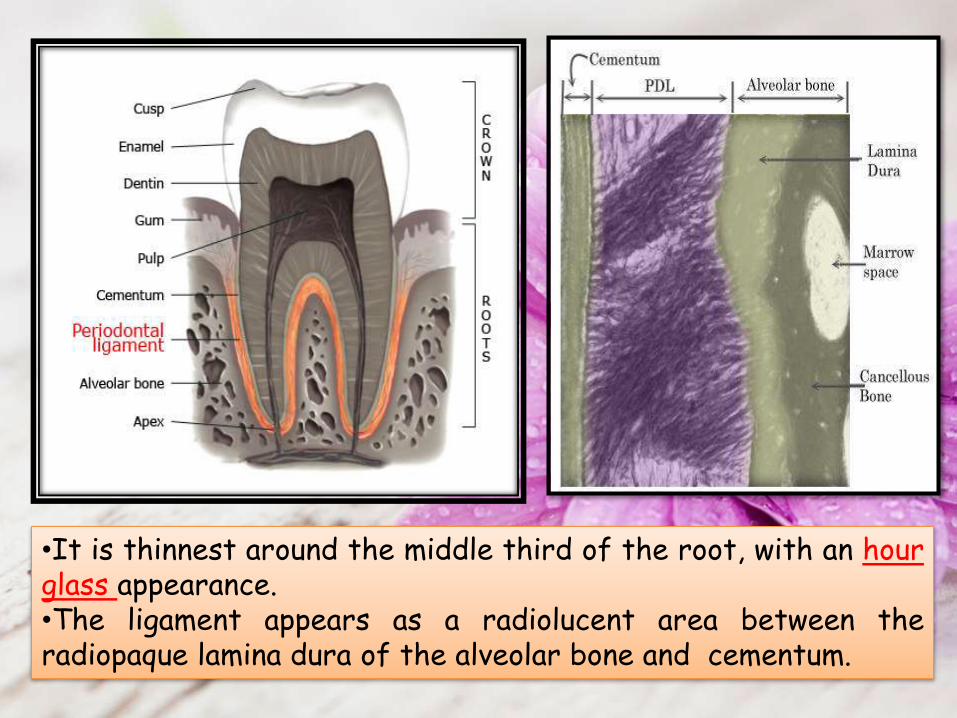
•It is thinnest around the middle third of the root, with an hourglass appearance.•The ligament appears as a radiolucent area between theradiopaque lamina dura of the alveolar bone and cementum.

• Immediately before tooth eruption and for sometimes thereafter, active fibroblasts adjacent to cementum of the coronal third of root, appear to become aligned in an oblique direction to long axis of the tooth
•Later the first collagen fiber bundles of the ligament becomes discernible.•These are the precursors of the alveolar crest fibre bundle group.
•Cemental and alveolar fibers continue to elongate towards each , to meet and fuse .

•As the first occlusal contact of the tooth occurs with its antagonist the principal fibres around the coronal third of root, horizontal group are almost completely developed .
•Oblique fibres are still being developed in middle third of root.
•With the formation of Apical fibre group, the definitive periodontal ligament architecture is established.

The Periodontal Ligament is formed of
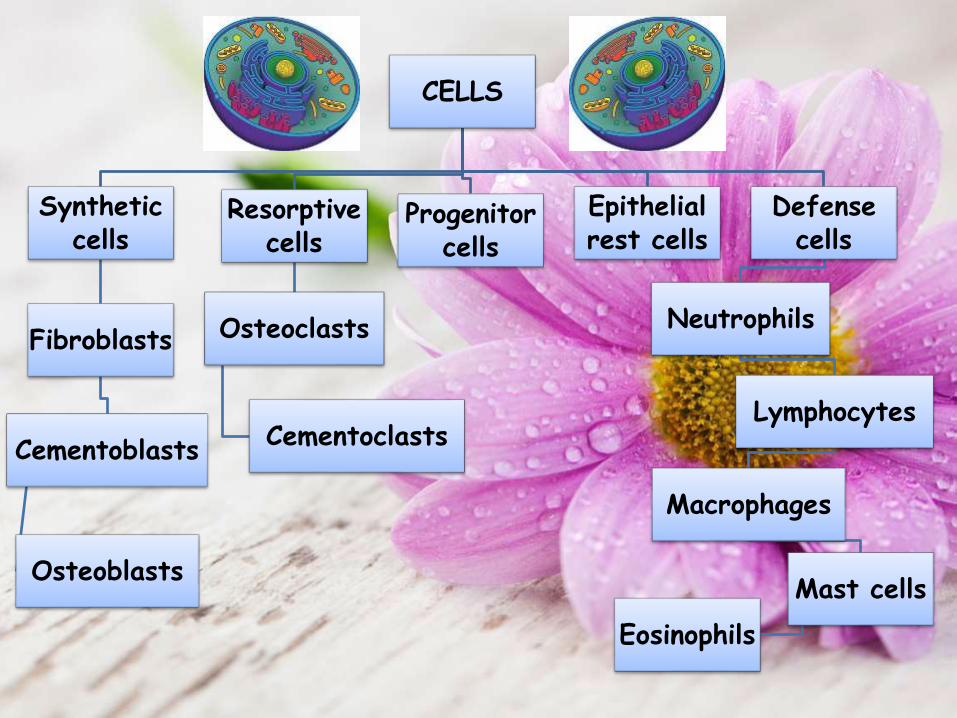
• Synthetic cells
• Resorptive cells
• Progenitor cells
• Cells rests of Malassez
• Defense cells
CELLS
• Fibers
• Ground substances
• Blood vessels, Nerves & Lymphatics.
EXTRACELLULAR
SUBSTANCES
CELLS
Synthetic cells
Fibroblasts
Cementoblasts
Osteoblasts
Resorptive cells
Osteoclasts
Cementoclasts
Progenitor cells
Epithelial rest cells
Defense cells
Neutrophils
Lymphocytes
Macrophages
Mast cells
Eosinophils

•Predominant cell in the pdl .
•These fibroblasts origin from the Ectomesenchyme of investing layer of dental papilla and from the dental follicle.
•These fibroblasts are regularly distributed throughout the ligament and are oriented with their long axis parallel to the direction of collagen fibrils .

• Fibroblasts of pdl generate an organizational pattern as they have ability to both synthesize and shape the proteins of the extracellular matrix .
• Certain Fibrils form bundles get inserted into tooth and bone and are known as SHARPEY’S fibers .
• Once embedded in the wall of alveolus or tooth, these fibers calcify to a certain degree and are associated with an abundance of non collagenous proteins found in the bone i.e. osteopontin and bone sialoprotein .
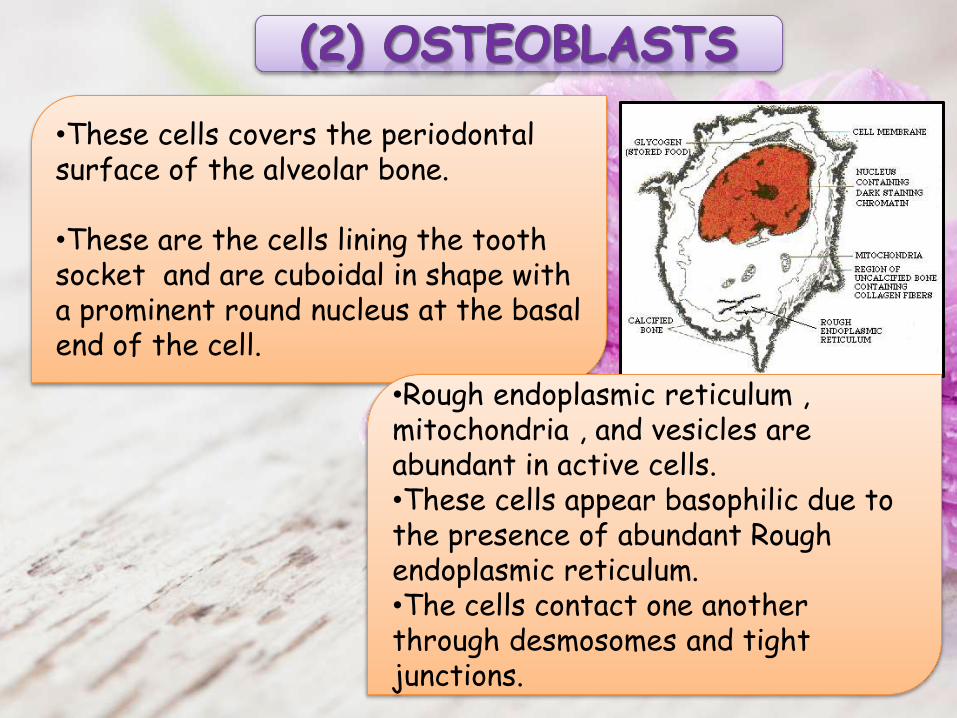
•These cells covers the periodontal surface of the alveolar bone.
•These are the cells lining the tooth socket and are cuboidal in shape with a prominent round nucleus at the basal end of the cell.
•Rough endoplasmic reticulum , mitochondria , and vesicles are abundant in active cells.•These cells appear basophilic due to the presence of abundant Rough endoplasmic reticulum.•The cells contact one another through desmosomes and tight junctions.
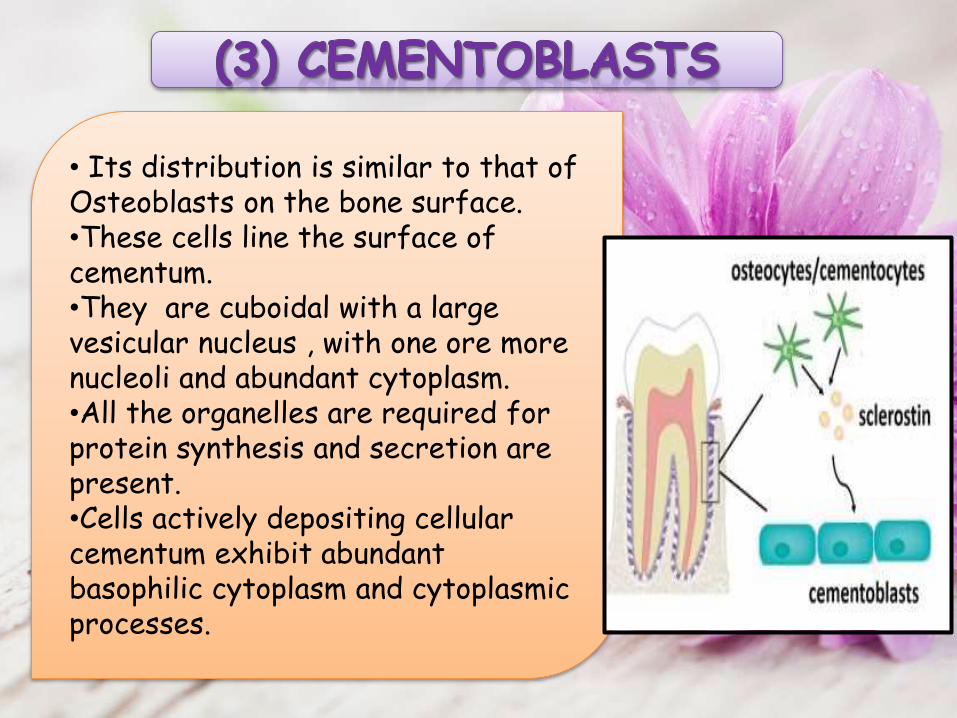
• Its distribution is similar to that of Osteoblasts on the bone surface.•These cells line the surface of cementum.•They are cuboidal with a large vesicular nucleus , with one ore more nucleoli and abundant cytoplasm. •All the organelles are required for protein synthesis and secretion are present.•Cells actively depositing cellular cementum exhibit abundant basophilic cytoplasm and cytoplasmic processes.

•These resorb bone and tend to be large and multinucleated but can also be small and mononuclear .•Multinucleated Osteoclasts are formed by fusion of precursor cells similar to circulating monocytes.•The part of plasma membrane lying adjacent to bone that is being resorbed is raised in characteristic folds and is termed the Ruffled or Striated border.
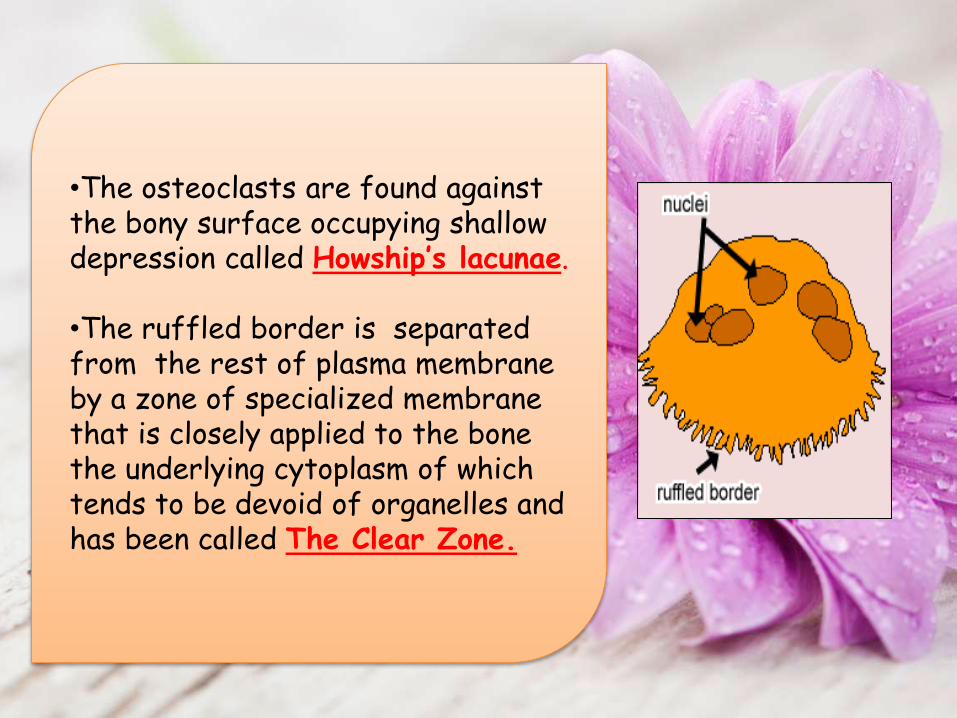
•The osteoclasts are found against the bony surface occupying shallow depression called Howship’s lacunae.
•The ruffled border is separated from the rest of plasma membrane by a zone of specialized membrane that is closely applied to the bone the underlying cytoplasm of which tends to be devoid of organelles and has been called The Clear Zone.

•As cementum does not remodel, Cementoclasts are not usually found in the ligament.•These cells only occur in certain pathologic conditions, during resorption of deciduous teeth and when regressive forces are applied on a tooth such as orthodontic therapy.•These Cementoclasts resembles Osteoclasts and are located in depressions in cementum resembling Howship’s lacuna.•These cells not only resorb cementum, they can destroy dentin and enamel as well thus they are also called Odontoclasts.

•All connective tissues including periodontal ligament contain progenitors cells that have the capacity to undergo mitotic division .
•If they were not present there would be no cells available to replace differentiated cells lying at the end of their life span or as a result of trauma.
•These are undifferentiated mesenchymal cells.

•The ligament contains epithelial cells that are found close to the cementum.•At the time of cementum formation the continuous layer of epithelium that covers the surface of newly formed dentin breaks into lacelike strands.•The epithelial rests persist as a network of strands islands or tube like structures near and parallel to the surface of the root.•Their function is not yet clear but they could be involved in periodontal repair and regeneration .
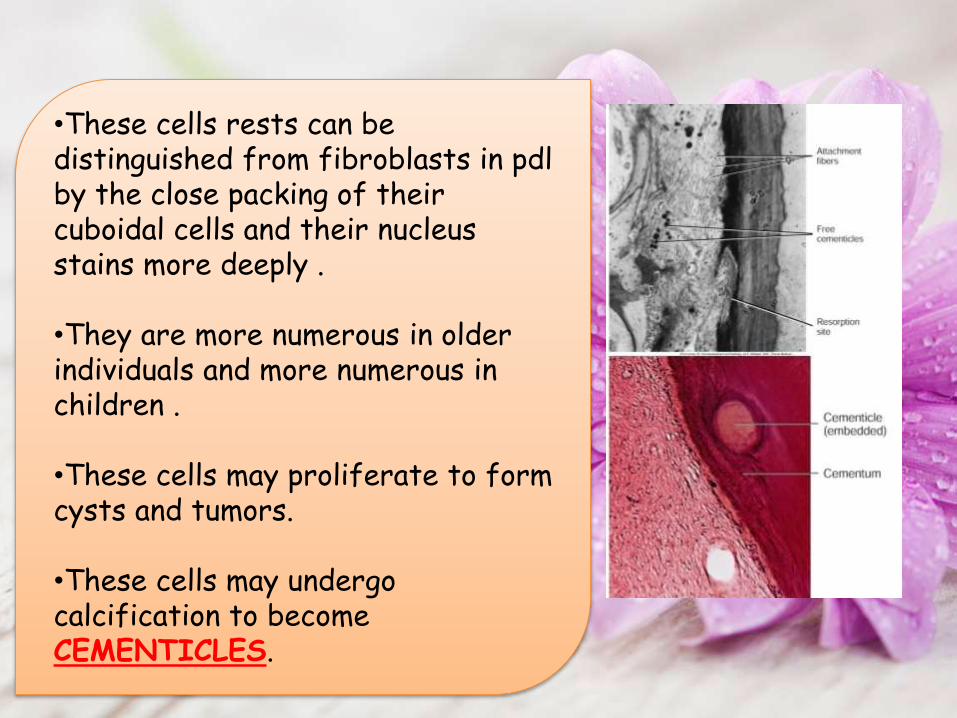
•These cells rests can be distinguished from fibroblasts in pdl by the close packing of their cuboidal cells and their nucleus stains more deeply .
•They are more numerous in older individuals and more numerous in children .
•These cells may proliferate to form cysts and tumors.
•These cells may undergo calcification to become CEMENTICLES.
•Neutrophils are the most abundant (40% to 75%) type of white blood cells in mammals and form an essential part of the innate immune system.
•Neutrophils are a type of phagocyte.
•Neutrophils are recruited at the site of injury within minutes following trauma, and are the hallmark of acute inflammation.
•A lymphocyte is subtypes of white blood cell in a human’s immune system.
•These are agranulocytes.
•The three major types of lymphocyte are T cells, B cells and natural killer (NK) cells.
•Lymphocytes can be identified by their large nucleus.

•Found in the ligament and are predominantly located adjacent to blood vessels.•Are capable of phagocytosis.•Derived from blood monocytes.•It has a nucleus, horseshoe or kidney shaped with peripheral chromatin.
•In periodontal ligament macrophages play dual role:-•1. Phagocytosing dead cells2. Secreting growth factor that regulate the proliferation of adjacent fibroblasts.
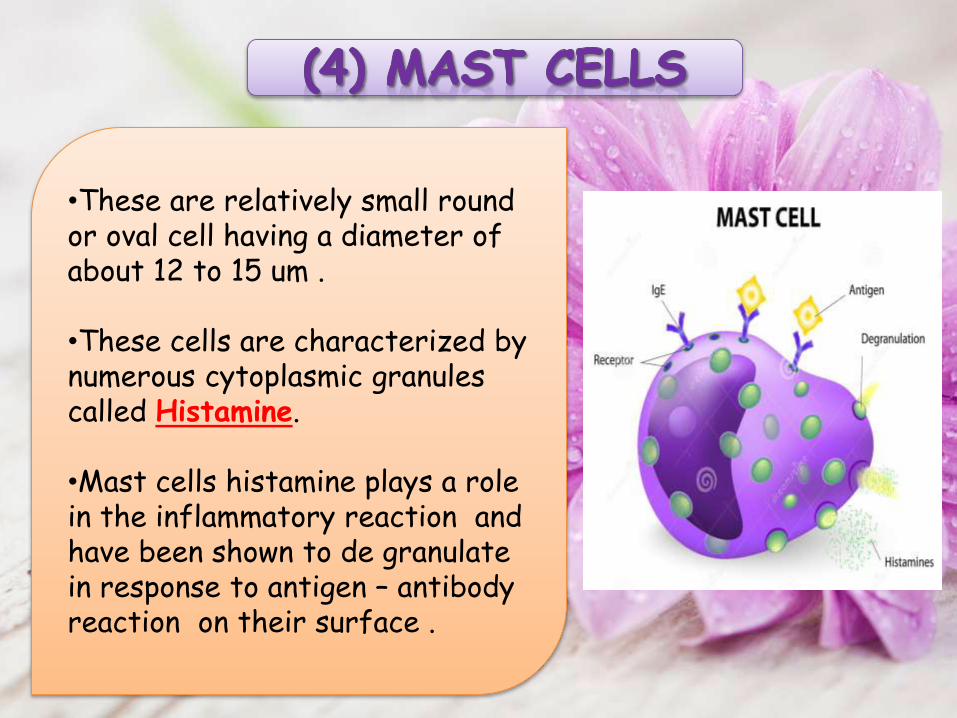
•These are relatively small round or oval cell having a diameter of about 12 to 15 um .
•These cells are characterized by numerous cytoplasmic granules called Histamine.
•Mast cells histamine plays a role in the inflammatory reaction and have been shown to de granulate in response to antigen – antibody reaction on their surface .
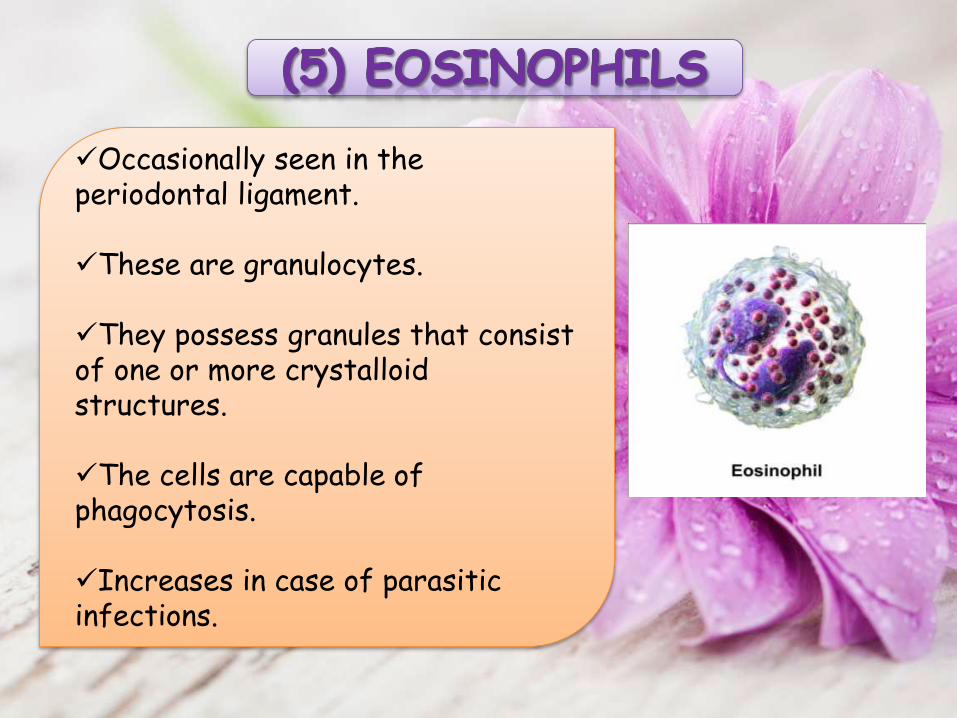
Occasionally seen in the periodontal ligament.
These are granulocytes.
They possess granules that consist of one or more crystalloid structures.
The cells are capable of phagocytosis.
Increases in case of parasitic infections.
Extracellular Substance
Fibers Ground Substances
Nerves, vessels,
Lymphatics

Fibers
Collagen
Elastic
Reticular Secondary
Indifferent plexus
Oxytalan

•The main types of collagen in the pdl are TYPE I and TYPE III.
•More than 70 % of pdl is TypeI . •Type I is uniformly distributed in the ligament .•Type III collagen accounts for about 20 % of collagen fibers•Type IV and VII are associated with epithelial cell rests and blood vessels.•Type XIII collagen is believed to occur within the pdl only when ligament is fully functional .

•The collagen is gathered to form bundles approximately 5 um in diameter. These bundles are termed as PRINCIPAL FIBERS. •Within each collagen bundle , subunits are present called collagen fibrils.
Principal Fibers
Alveolar Crest
Horizontal Oblique ApicalInter
radicular
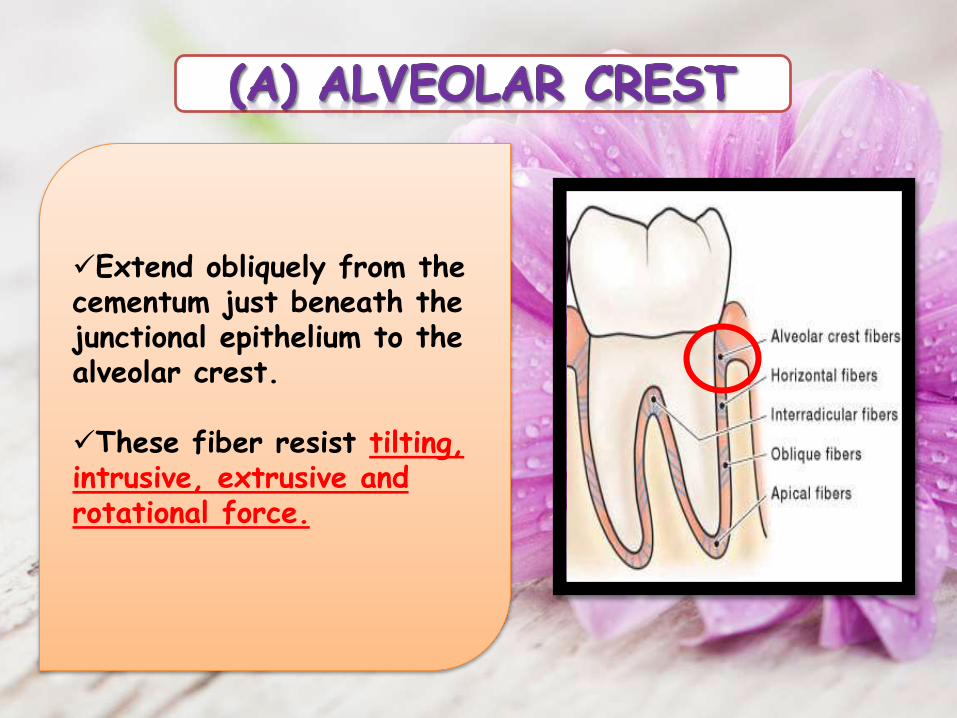
Extend obliquely from the cementum just beneath the junctional epithelium to the alveolar crest.
These fiber resist tilting, intrusive, extrusive and rotational force.
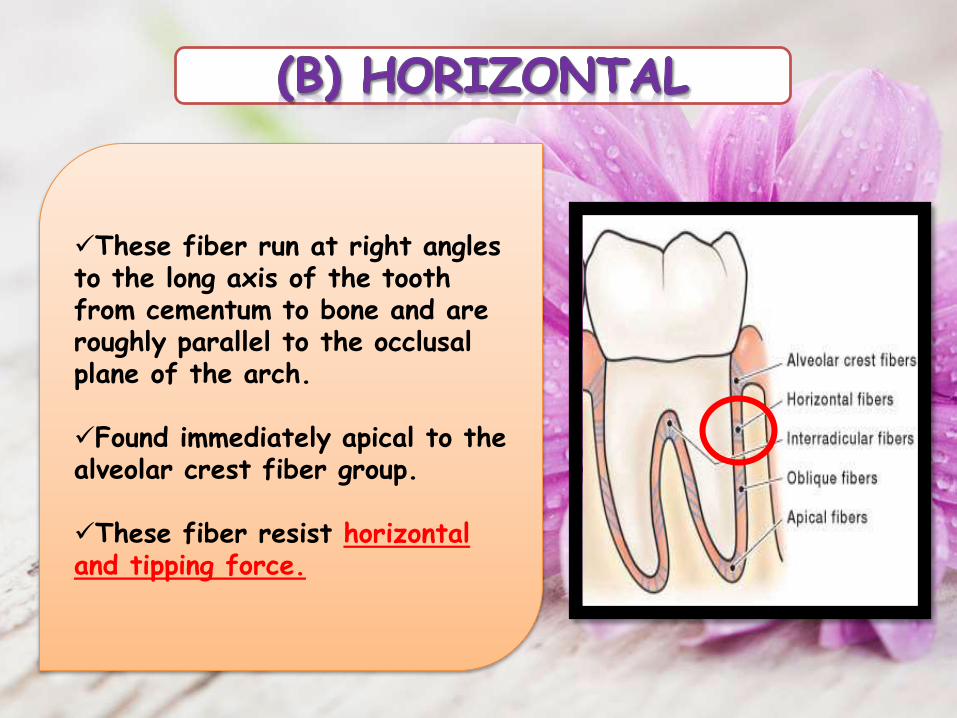
These fiber run at right angles to the long axis of the tooth from cementum to bone and are roughly parallel to the occlusal plane of the arch.
Found immediately apical to the alveolar crest fiber group.
These fiber resist horizontal and tipping force.

Oblique group are more numerous and occupy 2/3rd of the ligament.
These fibers are inserted into the alveolar bone at a position coronal to their attachment to cementum, thereby resulting in their oblique orientation within the periodontal space.
These fiber resist vertical and intrusive forces.

Apical group radiating from cementum around the apex of the root to the bone, forming the base of the socket.
The apical fiber resist the forces of luxation.
These fibers are not seen in the incompletely formed root.
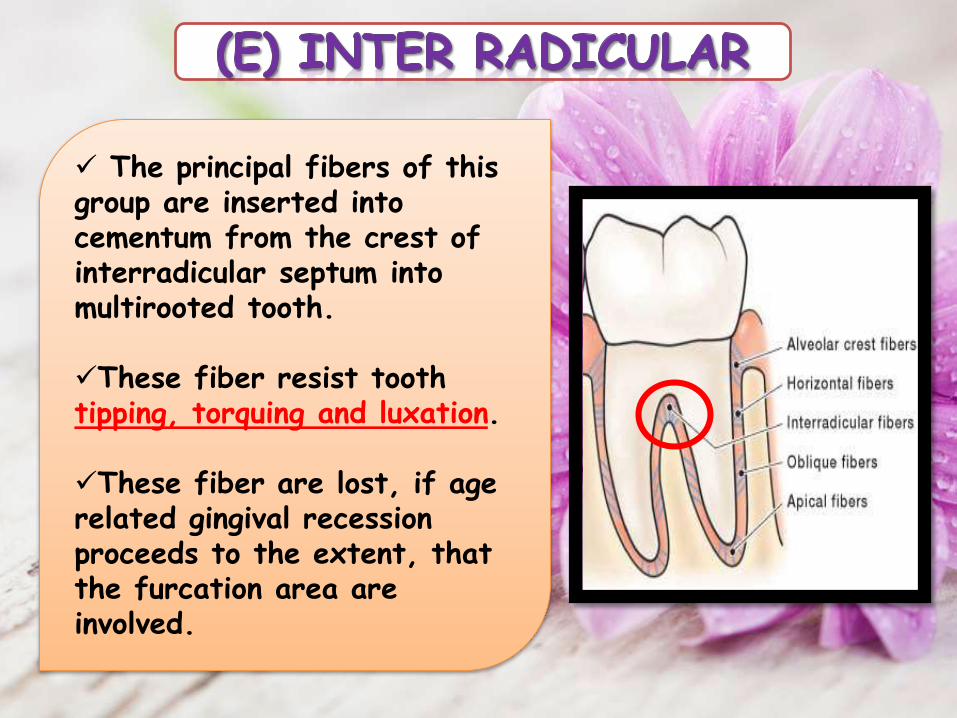
The principal fibers of this group are inserted into cementum from the crest of interradicular septum into multirooted tooth.
These fiber resist tooth tipping, torquing and luxation.
These fiber are lost, if age related gingival recession proceeds to the extent, that the furcation area are involved.
•There are three types of elastic fibers which are histochemically and ultrastructurally different.
•Mature Elastic fibers , Eulanin fibers and the Oxytalan fibers .
•Eulanin fibers and Oxytalan fibers have been described as immature elastic fibers.
•Mature elastic fibers consist of microfibrillar component surrounding an amorphous core of elastin protein .

These are immature collagen fibers with argyrophilic staining properties and are related to basement membrane of blood vessels and epithelial cells which lie within the periodontal ligament.
Located between and among the principalfibers.
Fibers are relatively non-directional and randomly oriented.
Appear to transverse the periodontal ligament space coronoapically and are often associated with path of vasculature and nervous elements.
Small collagen fiber associated with the large collagen fibers.

Oxytalan fibers are bundles of microfibrills.
These fibers are approximately 0.5μm to 2.5 μm in diameter.
They tend to run in axial direction one end being embedded in cementum or possibly bone, and other in the wall of blood vessels.
They have found to be thicker and more numerous in teeth that are subjected to high load.
•Amorphous background material that binds tissues and fluids.
•Major constituent of the Periodontal ligament.
•Similar to most connective tissue ground substance.
•Dermatan sulfate is the major glycosaminoglycan.
•When function of pdl increases, its size increases.
•However, in reduction of function, Pdl narrows and fiber bundles decreases in number and thickness.

•The blood supply is rich becausethe PDL has a very high turnoveras a tissue.
•The posterior supply is moreprominent than the anterior.
•The mandibular is moreprominent than the maxillary.
•A network of lymphatic vessels, following the path ofblood vessels, provides the lymph drainage of theperiodontal ligament.
•The flow is from the ligament towards and into theadjacent alveolar bone.
•Generally follow the blood vessels.
•Nerve are derived from the second and third divisions of
the fifth cranial nerve.
•Nerve fibers can be large myelinated or small non
myelinated fibers.
•Nerve end as knobs or spindles.
•Large nerve are responsible for discerning touch while
the smaller ones perceives pain.
Supportive
Sensory
Nutritive
Homeostatic
Eruptive
Supportive
Whenever a tooth is moved in its socket, theperiodontal ligament that is found around the root,gets compressed and therefore provides support forthe tooth.
The numerous collagen fibers that occur in theperiodontal ligament act as a cushion to withstandmasticatory forces.
The periodontal ligaments are so arranged thatfunctional pressure on the teeth from any directionproduces tension of certain fibers.

Therefore pressure on thetooth crown is transmitted tothe bone of the socket.
Thus PDL behaves assuspensory ligament
The ground substances presentbetween the fibers ofperiodontal ligament is rich inwater and therefore add up tothe support.

Sensory
Periodontal ligament is richly innervated.
It provides an excellent Proprioceptive mechanismwhich helps in estimating the amount of pressure onmastication, and detect even the mildest force actsupon a tooth.

Nutritive
The periodontal ligament has a good blood supplywhich provides nutrition for various cells of theperiodontium such as the cementocytes and thesuperficial osteocytes.
Whenever heavy forces are applied on a tooth theperiodontal ligament may get necrosed.
Homeostatic
Its is evident that the cells of pdl have the ability to resorb and synthesize the extracellular substance of the connective tissue of the ligament , alveolar bone and cementum
Pressure on the periodontal ligament tends to cause bone resorption.
Although the cementum is more resistant to resorption, it can neverthless exhibit resorption under severe pressure.
These Resorptive processes are brought about by cells present in the periodontal ligament.

Eruptive
During the development of the tooth, the cells ofperiodontal ligament produce cementum and bone ofthe tooth socket.
The periodontal ligament contains Cementoblasts andOsteoblasts that can form new cementum and bonerespectively.

The periodontal ligament ages as in all other tissuesof the body.
Cell number and cell activity changes with aging.
One of the prominent age changes is seen in thecalcified tissue of the periodontium, the bone and thecementum is scalloping and the periodontal ligamentfibers are attached to the peaks of this scallopedthan over the entire surface as seen in the youngerperiodontium.

With aging the activity of the periodontal ligamenttissue decreases because restricted diets andtherefore normal functional stimulation of the tissueis diminished.
Any loss of gingival height related to gingival andperiodontal diseases promotes destructive changes inthe periodontal ligament.

•The periodontal ligament is made up of collagen fibers in a proteoglycans stroma and many types of connective tissue cells as in any other soft fibrous connective tissue elsewhere in the body .
•But it has cells that form and resorb cementum and bone and the collagen fibers in a specific orientation connecting the two mineralized tissues that makes it unique.
•The tissue hydrostatic pressure is high. The tissue is extremely cellular with fibroblast showing many intercellular contacts well innervated with many mechanoreceptors and highly vascular unlike any other connective tissue in the adult.
•The features being high cellularity, very high rates of turnover and with significant amount of type III collagen.
•The collagen fibers are also sharp with unimodal size and frequency.
•The ground substance of pdl occupies large volume with high content of glucornate rich proteoglycans and glycoprotein- tenascin and fibronectin .

The primary role of the periodontal socket is to support the tooth in the bony socket. Its thickness varies in different individuals in different teeth in the same person and in different locations on the same tooth .
1)Acute trauma to the periodontal ligament, accidentalblows, or rapid mechanical separation may producepathologic changes such as -
Fractures or resorption
of cementum
Tear of fiber bundles
Hemorrhage Necrosis

•2. Orthodontic tooth movement depends on resorption and formation of alveolar bone and periodontal ligament. These activities can be stimulated by properly regulated pressure and tension.
•If the movement of teeth is within physiologic limits the initial compression of pdl on the pressure side is compensated for by bone resorption whereas on the tension side bone apposition is seen .
•ResorptionCOMPRESSION
SIDE
•DepositionTENSION
SIDE


3. Application of large forces results in necrosis of pdl and alveolar bone on the pressure side and movement of the tooth will occur after the necrotic bone has been resorbed by Osteoclasts located on its endosteal surface.
4 . Inflammatory diseases of the pulp progress to the apical periodontal ligament and replace its fiber bundles with granulation tissue. This lesion is called a periapical granuloma may contain epithelial cells •These may undergo proliferation and produce a periapical cyst.

5 . Chronic inflammatory disease such as Periodontitis is common pathology related to pdl . The toxins released from the bacteria in the dental plaque and metabolites of the host’s defense mechanism destroy the pdl and the adjacent bone very frequently. This leads to tooth mobility and further loss of tooth .
6 . To repair the existing destruction of pdl can be quite challenging. It involves limiting the disease process and to regenerate the host tissues to their original form in such a way that reattachment of pdl to bone becomes possible.
•The periodontal ligament is a fibrous connective tissue forming important part of the Periodontium.
•Without it tooth is support less.
•Cell of the periodontal ligament are Pluri-potent and helps in the regeneration of all the components of Periodontium lost in the periodontal disease process.

•A better understanding of cell and molecular biology of developing and regenerating periodontium offers newer avenues to regenerate the pdl.
•Newer options of treatment are made available from time to time.
•Yet safeguarding the integrity of the pdl and alveolar bone is still one of the most important challenge .

•FerminA, Carranza, Newmann, Takei; clinical periodontology
;9thedition;45–51.
•FerminA.Carranza,Newmann,Takei;clinicalperiodontology;10thedition;6
8–92.
•R.Tencate,AntonioNanci;oralhistology,development,structure&function;
6thedition;111–143
•Hagel-Bradway S, Dziak R: Regulation of bone cells metabolism, J Oral
Pathol Med 18:344,1989
•Junqueria LC, Carneiro J, Kelley RO: Basic Histology, ed6, Norwalk,
Conn, 1989, Appleton & Lange.

• Nanci A. Periodontium: Ten Cate’s Oral Histology. 6th Edition.
Elsevier; 2005. 145-200.
• Avery J K, Histology of Periodontal ligament, Oral Development
and Histology.2nd Edition. Thieme Medical Publications 1994. 153-
172.
• Bhaskar S N, Periodontal ligament, Orban’s Oral Histology And
Embryology. 12th Edition. Elsevier publications 2008.45-84
• Bhalaji SI. Periodontal ligament. Dental Anatomy histology and
development. 1st Edition. Arya publications; 2003. 295-302.
•Kumar GK. Periodontal ligament. Orban’s Oral Histology and
Embryology. 12th Edition. Elsevier Publications; 2006. 137-154.

Perfection is not attainable But
If we chase Perfection we can achieve Excellence