1 aerosol transmissible disease standard riverside county department of public health 2010
TRANSCRIPT

1
AEROSOL TRANSMISSIBLE
DISEASESTANDARD
Riverside County
Department of Public Health
2010

Learning Objectives
At the conclusion of this presentation participants will be able to:
1. Identify at least 3 common Aerosol Transmissible Diseases (ATD) that present a risk in the workplace.
2. Identify the levels for potential exposure of employees to ATD based on job responsibilities.
2

Learning Objectives (continued)
3. Discuss the difference between droplet precautions and airborne infection isolation.
4. Discuss appropriate action to take if exposed to an ATD in the workplace.
5. Discuss the recommended Personal Protective Equipment (PPE) for Novel Influenza Viruses.
3

Disease Trends
4

Tuberculosis RateRiverside County, 1997-2009
5
0
2
4
6
8
10
12
14
'98 '99 '00 '01 '02 '03 '04 '05 '06 '07 '08 '09
Year
Rat
e pe
r 10
0,00
0 po
pula
tion
Riverside County California HP 2010

MULTI DRUG RESISTANT (MDR) Riverside County - TB Cases 2000-2009
6
3
2
0
1 1 1
6
1
0
1
0
1
2
3
4
5
6
2000 2001 2002 2003 2004 2005 2006 2007 2008 2009
2000200120022003200420052006200720082009

Vaccine Preventable Diseases
Incident of Reportable Vaccine Preventable Diseases, Riverside County 2003-2009
7

Pertussis Cases by Year 1999-2010 Riverside County
Data through July 15, 2010
8For current numbers go to http://www.rivcoph.org/pertussis/index.html

H1N1 Riverside CountyApril 2009 –March 31, 2010
• Total Cases: 2,573
– Number Hospitalized: 389
– Number of Deaths: 40
9

What is an Aerosol Transmissible Disease
• A disease or pathogen that is transmissible by aerosols (gaseous suspension of fine solid or liquid particles)
• Airborne precautions: small droplets, or droplet nuclei
• Droplet precautions: larger droplets, 5 microns or greater
10
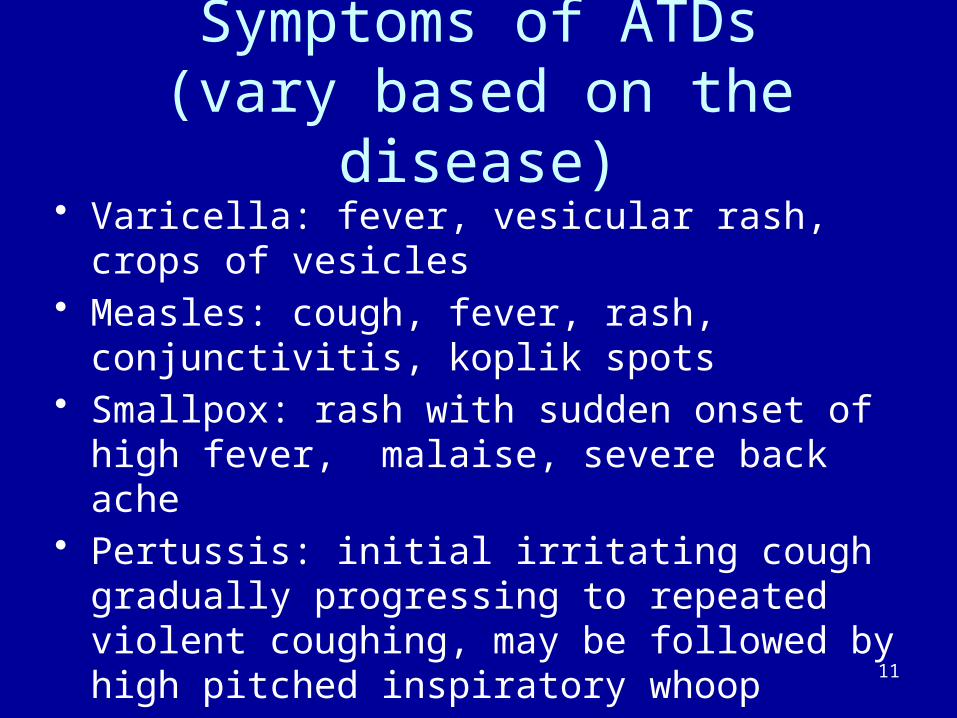
Symptoms of ATDs(vary based on the disease)
• Varicella: fever, vesicular rash, crops of vesicles• Measles: cough, fever, rash, conjunctivitis, koplik
spots• Smallpox: rash with sudden onset of high fever,
malaise, severe back ache• Pertussis: initial irritating cough gradually
progressing to repeated violent coughing, may be followed by high pitched inspiratory whoop
11
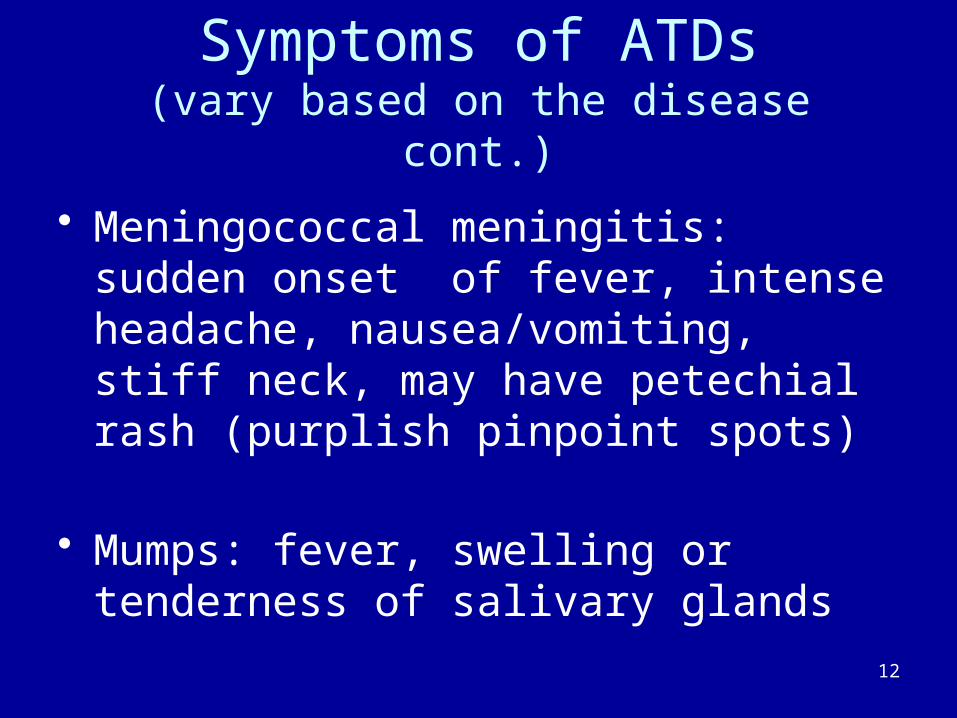
Symptoms of ATDs(vary based on the disease cont.)
• Meningococcal meningitis: sudden onset of fever, intense headache, nausea/vomiting, stiff neck, may have petechial rash (purplish pinpoint spots)
• Mumps: fever, swelling or tenderness of salivary glands
12

Symptoms of ATDs(vary based on the disease)
• Tuberculosis: productive cough, fever, unexplained weight loss
Overview of Tuberculosis
– TB is caused by Mycobacterium tuberculosis– Can cause infection in almost any organ of
the body (secondary infections)– Spread by droplet nuclei from infected person
13
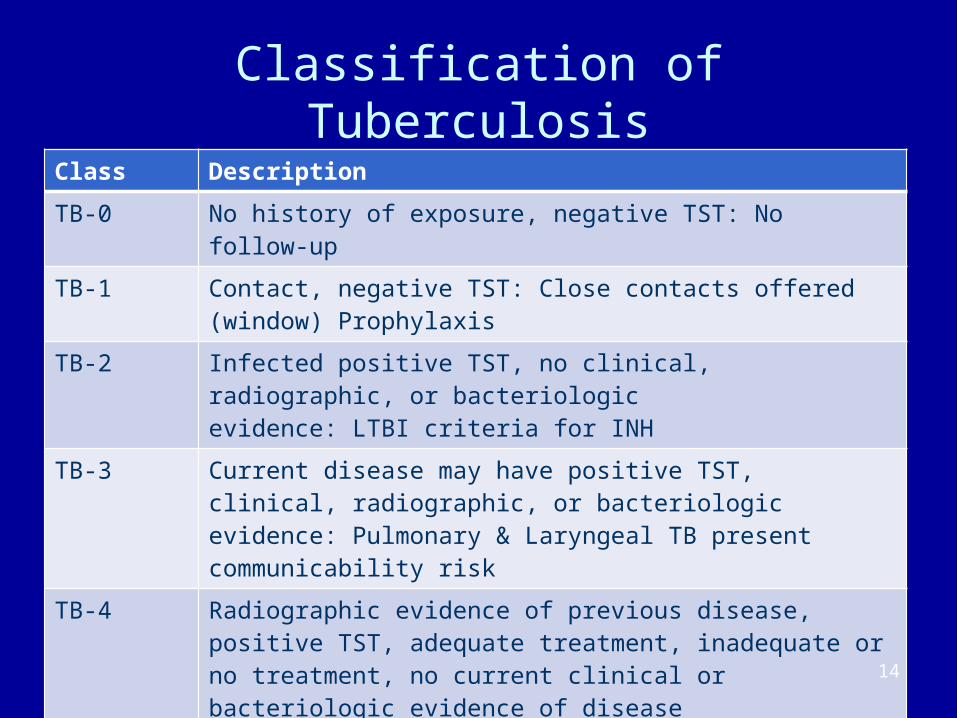
Classification of Tuberculosis
Class Description
TB-0 No history of exposure, negative TST: No follow-up
TB-1 Contact, negative TST: Close contacts offered (window) Prophylaxis
TB-2 Infected positive TST, no clinical, radiographic, or bacteriologicevidence: LTBI criteria for INH
TB-3 Current disease may have positive TST, clinical, radiographic, or bacteriologic evidence: Pulmonary & Laryngeal TB present communicability risk
TB-4 Radiographic evidence of previous disease, positive TST, adequate treatment, inadequate or no treatment, no current clinical or bacteriologic evidence of disease
TB-5 Diagnosis pending, may have a positive TST, abnormal CXR, cannot rule out active process: cough, wt loss, fever, hemoptysis, noc sweats, positive smear or culture, ID pending
14
Risk of Developing TB
• Persons at high risk for developing TB once infected:
• HIV/AIDS – 10% risk per year• Recently infected • People who inject illicit drugs • History of inadequately treated TB
15

Risk of Developing TB (Cont.)
• Risk of Developing TB– Certain medical conditions
• Diabetes• End-stage renal disease• Pulmonary fibrosis or silicotic process on
chest x-ray• Gastrectomy
– Certain Drugs• High dose cortisone/prednisone• Methotrexate
16

Precautions for ATDs• Airborne Infection Isolation (AII)
– Negative Pressure Isolation– UV light (TB)– N-95 Respirator
• Required for Diseases such as:– Measles– Novel Influenza– Smallpox– Tuberculosis
17

Pandemic H1N1 Influenza
18

H1N1 Virus
• Is a type A Influenza Virus
• Human Infections occur and can spread from person to person through coughing and sneezing.
19

H1N1 Virus (continued)
• A person can be infectious 1 day before and up to 7-10 days after onset of symptoms
• Symptoms: Fever > 100° F and an upper respiratory illness with cough, may also have nausea, vomiting, diarrhea or a sore throat
20

21
Specific Infection Control Precautions Needed for Novel Influenza Viruses
Standard Precautions Effective Hand Hygiene (before and after
all patient contact)
Contact Precautions Use gloves and gown for all patient
contact
22
Precautions needed for Novel Influenza (continued)
Eye Protection• Wear when within 6 feet of the patient
Airborne Precautions• Place the patient in a negative pressure
isolation room• Use at least a NIOSH approved N-95
respirator

23
Vaccinia Virus
Virus used to make Smallpox vaccine does not contain Smallpox virus. Similar to Smallpox virus, but less harmful.
The vaccination site contains vaccinia virus starting four (4) days after vaccination and up to twenty-one (21) days.
• Not airborne – (Smallpox is airborne)• Requires contact precautions

24
Example of Vaccinia Virus infection.
Abdomen and chest of a 2-year-old boy with a rash of dimpled lesions caused by eczema vaccinatum— a rare severe adverse reaction
caused by exposure to the vaccinia virus. Photo courtesy of John Marcinak

Droplet Precautions
• Droplet precautions include procedures designed to reduce the risk of transmission of infectious agents through contact with secretions.
• Required for diseases such as:– Meningococcal disease (H. influenzae; Neisseria
meningitidis)– Rubella– Mumps– Pneumonic Plague– Pertussis
25

Source Control Measures For Persons with ATDs
• Procedures to minimize the spread of airborne particles and droplets
• Important to educate patients with ATDs to cover their cough and effective hand hygiene
• Patients must wear surgical mask not N-95 respirators
• Information can be communicated to patients via posters/signs
26

27

Scope of the ATD Standard
• A variety of health care facilities, services, operations
• Hospitals, clinics• Public health services (e.g. communicable
disease, contact tracing or screening)• High risk environments
– Corrections– Homeless shelters– Drug treatment
28

Four Types of Employers defined by the Cal/OSHA ATD Standard
• Referring employers: don’t provide care beyond initial to cases and suspected cases of AirIDs diseases, and don’t do high hazard procedures on them
• Full standard: hospitals and others that are not referring employers
• Laboratories• Conditionally exempt: dentists and outpatient
medical specialty practices that don’t treat ATDs and have screening procedures
29
Required Elements of the ATD Standard
(Title 8, California Code of Regulations, Section 5199)
• Identification of an Administrator • Written procedures/plans• Source control• Engineering, work practice, administrative
controls and PPE• Respirators• Communication• Training
30

Required Elements of the ATD Standard (cont.)
(Title 8, California Code of Regulations, Section 5199)
• Recordkeeping • Medical services
• Vaccinations• Annual TB testing• Post exposure follow up• Precautionary removal• Respirator medical evaluations, if applicable
31

Required Training• Employers shall ensure that all employees with
occupational exposure participate in a training program • Employers shall provide training as follows:
– At the time of initial assignment to tasks where occupational exposure may take place
– At least annually thereafter, not to exceed 12 months from the previous training
– When changes, such as introduction of new engineering or work practice controls, modification of tasks or procedures or institution of new tasks or procedures, affect the employee's occupational exposure or control measures. The additional training may be limited to addressing the new exposures or control measures
32

Required Training(cont.)
– Training material appropriate in content and vocabulary to the educational level, literacy, and language of employees shall be used
– An opportunity for interactive questions and answers with a person who is knowledgeable in the subject matter as it relates to the workplace that the training addresses and who is also knowledgeable in the employer’s infection control procedures
* The standard outlines the minimum elements that must be included in the training program (refer to the ATD Standard, pages 23-24)
33

Exposure Determination Table
34
High Hazard Procedures
• Sputum induction• Transporting infectious ATD patients• Process ATP-L in the laboratory• Repairing, replacing or maintaining air
systems or equipment that may contain ATDs
35

List of Assignments or Tasks Requiring Personal Protective Equipment
36
Respiratory Protection Program
• All HCWs with occupational exposure to ATDs must be fit-tested with a N-95 respirator
• Multiple use vs. Single use• Effective September 1, 2010 Powered Air
Purifying Respirators (PAPR) must be used for high hazard procedures
37

Respiratory Protection Program(cont.)
– Exception 1: If performed in a booth, hood enclosure –may use N-95 respirator
– Exception 2: Paramedics and other personnel in field operations may use a P-100 respirator
38

Specific Requirements for Laboratories
• The ATD Standard requires lab employers to use feasible engineering and work practice controls to limit exposure and to provide PPE and respirators when that equipment is necessary to control exposures
• The Public Health Laboratory is required to develop, implement and annually review a written Biosafety Plan (BSP) that includes the following:• Safe handling procedures and list of prohibited practices• Engineering controls, including containment facilities such
as biosafety cabinets• Procedures requiring the use of PPE and/or respirators
39

Specific Requirements for Laboratories (cont.)
– Effective decontamination/disinfection procedures– A requirement that all incoming materials
containing ATPs-L be treated as containing the virulent or wild-type pathogen, until proven otherwise
– Inspection procedures to be performed annually– Emergency procedures for uncontrolled releases
within the lab & untreated releases outside the lab, including reporting incidents to the local health officer
40

Medical Services for HCWs
• Medical surveillance – TB– Routine screening– Post-exposure screening– HCWs with significant TST or Blood Assay Test (BAT)
• Latent TB Infection vs. TB Disease• Risk Assessment for TB
– MDR – TB– TB converters
5 to 10% will progress to active TB in 1-2 years
41

42
Medical Services for HCWs(cont.)
• Effective September 1, 2010 , recommended vaccinations shall be made available to all employees who have occupational exposure after the employee has received the training required in subsection (c) or (i) and within 10 working days of initial assignment unless:– The employee has previously received the
recommended vaccination(s) and is not due to receive another vaccination dose
– A PLHCP has determined that the employee is immune in accordance with applicable public health guidelines
– The vaccine(s) is contraindicated for medical reasons

Medical Services for HCWs (cont.)
• Recommended Vaccinations– Influenza – One dose annually– Measles – Two doses– Mumps – Two doses– Rubella – One dose– Tdap – One dose, booster as recommended– Varicella – Two doses
• Additional vaccine doses must be made available to employees within 120 days of the issuance of new applicable public health guidelines recommending additional dose
43

Medical Services for HCWs (cont.)
• Declination statement required for employees who decline a recommended and offered vaccination (refer to Policy DOPH P-102)
• Must sign a statement for each declined vaccine• Disease Control must inform Administration,
Human Resources and Occupational Health if a recommended vaccine is not available
• Must check on vaccine availability at least every 60 calendar days and inform employees when available
44

Occupational Exposure• Work activity or conditions create an elevated risk of
contracting disease if protective measures are not in place– Elevated exposure risk vs. other public contact
operations• Presumed for at least some employees in every facility,
service or operation listed in (a)(1)• Examples:
– Direct contact with cases or suspected cases of ATDs – Works within range of at-risk populations (e.g. homeless shelter
staff)– Laboratory areas where ATPs-L are handled– Contaminated equipment (e.g. AIIR ventilation systems)
45

Post Exposure Follow-up for ATDs
• Administrative procedures– Employees must notify supervisor – Supervisor evaluates exposure and ensures
required paperwork is completed– Follow workers compensation procedures– Must determine if employee had a significant
occupational exposure– Must implement corrective measures if
indicated
46

Precautionary Removal from Work
• When a post exposure evaluation is done for exposure to ATDs, or TB conversion, an assessment must be made to determine if precautionary removal is needed to prevent potential disease transmission
• If the PLHCP or the Public Health Officer recommends precautionary removal, DOPH must maintain employee earnings, seniority and other benefits until the employee is cleared
47

Post Exposure Follow-up for ATDs (cont.)
Depends on the ATD• Novel Influenza
– Evaluation for post-exposure prophylaxis with anti-viral medication
– Monitoring for development of signs and symptoms
– Assess for need to exclude from work for 7-10 days
48

Post Exposure Follow-up for ATDs (cont.)
• Pertussis
– Evaluation for post exposure treatment with recommended antibiotics
– Monitoring for development of signs and symptoms
– Assess for need to exclude from work
49

Post Exposure Follow-up for ATDs (cont.)
• Varicella
– Evaluation for antiviral therapy or varicella vaccination (if given within 3 days)
– Monitoring for development of signs and symptoms
– Assess for need to exclude from work (day 10-21)
50

Post Exposure Follow-up for ATDs (cont.)
• Measles
– Evaluation for measles vaccination or IG to be given 72 hours of exposure
– Monitoring for development of signs and symptoms
– Assess for need to exclude from work
51

Referral of Patients with ATDs
• As part of the referral process, must notify receiving HCF, PT has or suspected to have an ATD.
• Transporting personnel (e.g. ambulance, air transport) must be informed patient has/may have ATD
• Patient must wear a surgical mask for transport
52

Containment of ATDs
• Triage of persons with respiratory symptoms to be done by designated licensed staff
• Non-licensed staff must be educated to screen persons with respiratory symptoms and refer to licensed staff for triage
• Symptomatic patients must be placed in a negative pressure isolation room or outside
• Prompt medical evaluation must be done by a licensed health care professional
53

Surge Procedures
• All DOPH employees are designated as disaster workers and are expected to respond in an emergency
• Staff must complete NIMS/SEMS training and core public health competencies at level I, II or III as determined by supervisor/manager
• Each branch is to maintain an emergency notification system
• Specific procedures for stockpiling and accessing respiratory protection and PPE are part of the SNS and DOPH Emergency Response Plans
54

Zoonotic ATD Standard
• Zoonotic diseases /pathogens that are transmissible from animal to humans
• Capable of causing human disease that may be transmitted by droplets or an airborne route– Examples include:
• SARS• TB• H1N1 Influenza
55

Scope of Zoonotic ATD Standard
• Services that capture, sample, transport or dispose of birds and other wildlife
• Farms producing animals or animal products• Slaughterhouses• Veterinary animal inspection• Importers of live or untreated animals or animal products• Zoos• Animal parks• Pet stores• Laboratory operations
56

Requirements of the Zoonotic ATD Standard
• Establish procedures that minimize production of aerosols
• Controls for cleaning and decontaminating• PPE and respiratory protection• Posting of signs in areas containing identified or
suspected cases• Training• Recordkeeping• Provision of medical services to exposed workers
57

A COMPLETE COPY OF THE AEROSOL TRANSMISSIBLE DISEASE EXPOSURE
CONTROL PLAN
IS AVAILABLE AT CHA INSIDER’S PAGE
(under policies, procedures and guidelines tab)
http://intranet.rccha.org
58
QUESTIONS
59