1 a therapeutic platelet strategy journal club – feb 21, 2007 kristine roland md frcpc tm...
TRANSCRIPT
1
A Therapeutic Platelet Strategy
Journal Club – Feb 21, 2007
Kristine Roland MD FRCPCTM Resident, UBC

2
Context
Prophylactic plt transfusion strategies for thrombocytopenic pts are standard practice
The appropriate plt count ‘trigger’ has evolved:
- Gaydos et al, NEJM 1962: observed that serious bleeding in pts with acute leukemia rare when plts > 20 x 109/L
- Numerous studies indicate threshold of 10 x 109/L is safe:Heckman KD et al, J Clin Oncol 1997
Rebulla P et al, NEJM 1997Zumberg MS et al, Biol Blood Marrow Transplant 2002Callow CR et al, Br J Haematol 2002

3
Context
Does reducing the trigger from 20 to 10 improve plt utilization?
- Hersh et al 1998: mathematical modeling predicts a 14.5% decrease in plt utilization
- Rebulla 21.5% reduction in plt usageHeckman 35% fewer transfusions (not significant)Callow 36% reduction (compared to retrospective)Zumberg no difference
4
Context
Other factors impact utilization: frequency of checking plt counts, development of additional risk factors for bleeding, compliance with guidelines
Two studies in the recent issue of Transfusion (Feb 2007) report poorer than expected compliance with prophylactic thresholds:
- Greeno et al – overall 28% compliance (up to 43% on Heme/Onc service)
- Cameron et al – overall 22% compliance (and reasons for non-compliance were poorly documented)

5
Context
Mark Brecher editorial (Transfusion Feb 2007):
If goal is to reduce plt utilization, other approaches may need to be investigated
- Lower plt doses (PLADO study underway)
- Employing a therapeutic strategy vs the prophylactic strategy …
6
The Study:
A therapeutic platelet transfusion strategy is safe and feasible in patients after autologous peripheral blood stem cell transplantation
Wandt H et alBone Marrow Transplantation (2006) 37:387-392
Objective: “ assess the safety and feasibility of a therapeutic platelet transfusion strategy”

7
Population
Single-centre study from Germany 106 pts prospectively enrolled after 2001 Adults undergoing autologous PBSCT- range 18-70 years, median 54 years- male: female 2:1 - MM (43%), lymphoma (32%), acute leukemia (16%), solid
tumour (8%)- total of 140 transplant procedures (76 pts received 1
transplant; 30 received 2 or 3)- 87 pts received chemo; 19 pts received chemo +TBI
Exclusion criteria: AL-amyloid, aspergillus infxn, cerebral lesion, prior life-threatening bleeding during chemo
8
Intervention
daily morning plt counts twice daily clinical exam for hemorrhage therapeutic platelet transfusion if bleeding
WHO ≥ grade II* prophylactic platelet transfusion if plt < 10 x
109/L and unstable†
all plts were ABO-compatible apheresis LR
PRBC transfusion to maintain Hb > 80g/L
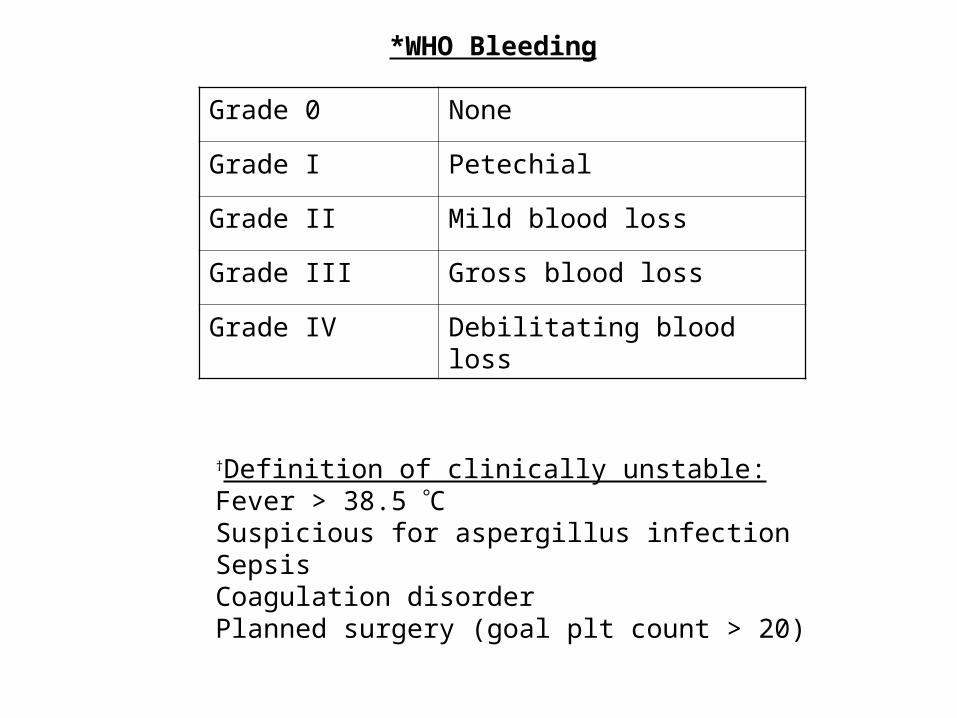
Grade 0 None
Grade I Petechial
Grade II Mild blood loss
Grade III Gross blood loss
Grade IV Debilitating blood loss
†Definition of clinically unstable:Fever > 38.5 CSuspicious for aspergillus infectionSepsisCoagulation disorderPlanned surgery (goal plt count > 20)
*WHO Bleeding
10
Matched pair analysis
Retrospectively reviewed 60 transplant procedures matched for the first 60 procedures in the prospective cohort
Matched for: gender, Dx, conditioning
These historical patients would have received prophylactic platelet transfusions routinely for morning plt < 10 x 109/L
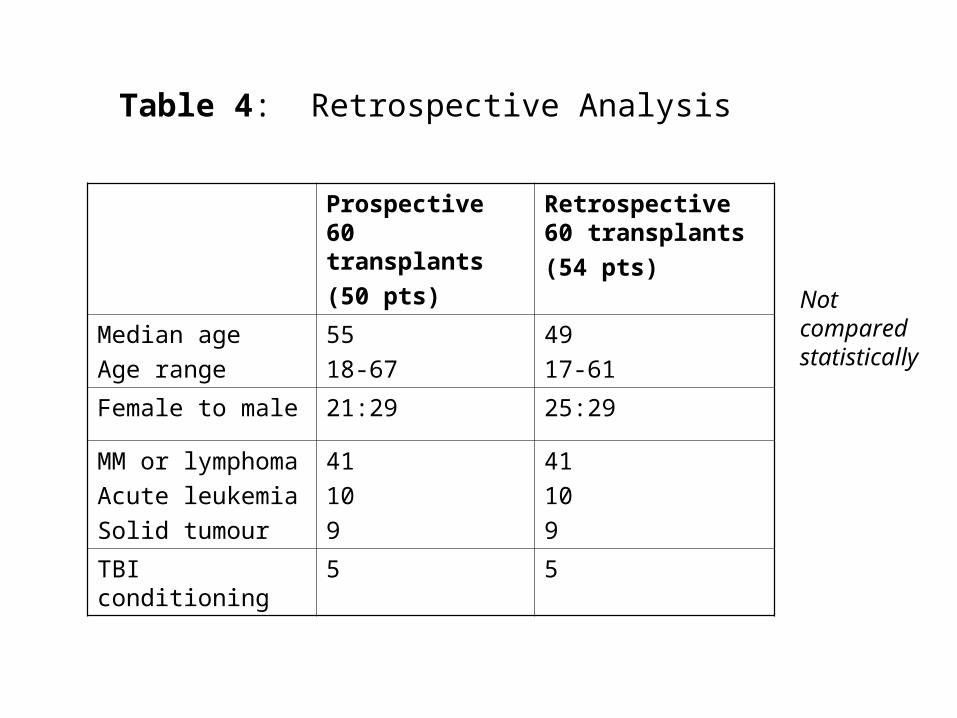
Prospective 60 transplants(50 pts)
Retrospective 60 transplants(54 pts)
Median ageAge range
5518-67
4917-61
Female to male 21:29 25:29
MM or lymphomaAcute leukemiaSolid tumour
41109
41109
TBI conditioning 5 5
Table 4: Retrospective Analysis
Not comparedstatistically
12
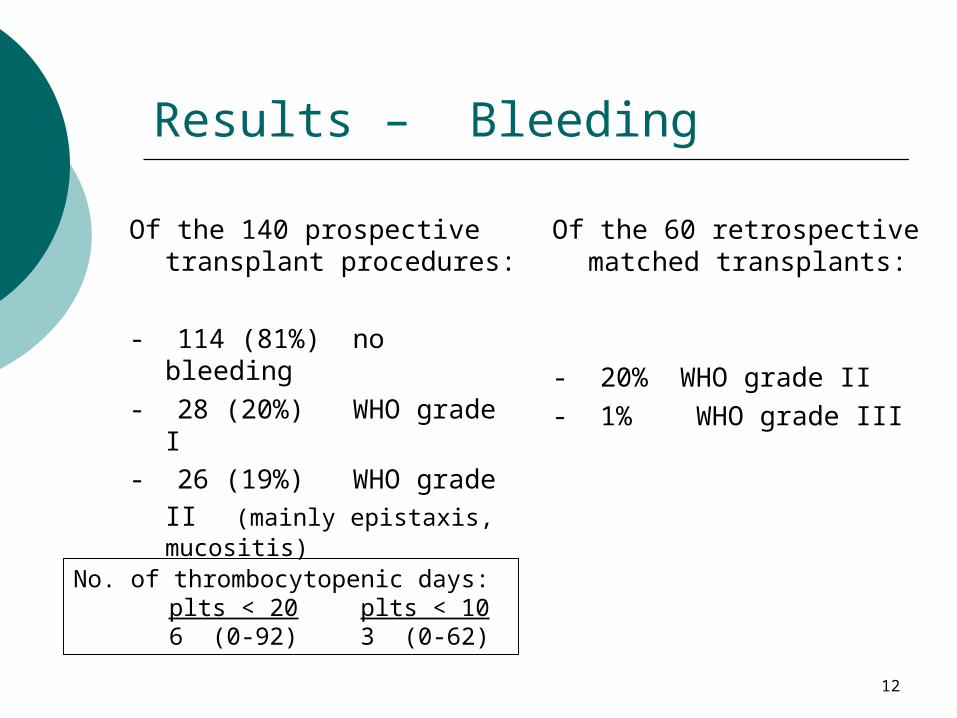
Results – Bleeding
Of the 140 prospective transplant procedures:
- 114 (81%) no bleeding- 28 (20%) WHO grade I
- 26 (19%) WHO grade II (mainly epistaxis, mucositis)
Of the 60 retrospective matched transplants:
- 20% WHO grade II- 1% WHO grade III
No. of thrombocytopenic days:plts < 20 plts < 106 (0-92) 3 (0-62)

13
Results – Transfusions
48 (34%) of 140 transplants could be performed without a plt transfusion.
Of the total 235 plt units that were transfused:
81 therapeutic vs 154 prophylactic- main indications for prophylactic were fever and
septicemia- but 27% of transfusions given for no clear reason

14
Analysis by Dx and conditioning
MMother
47%22%
P < 0.05
Non-TBITBI
37%0%
P < 0.05
Percentage of transplants (n = 140) NOT requiring platelet transfusion
TBI associated with increased mucositis-related bleeding
Mann-Whitney U-test
15
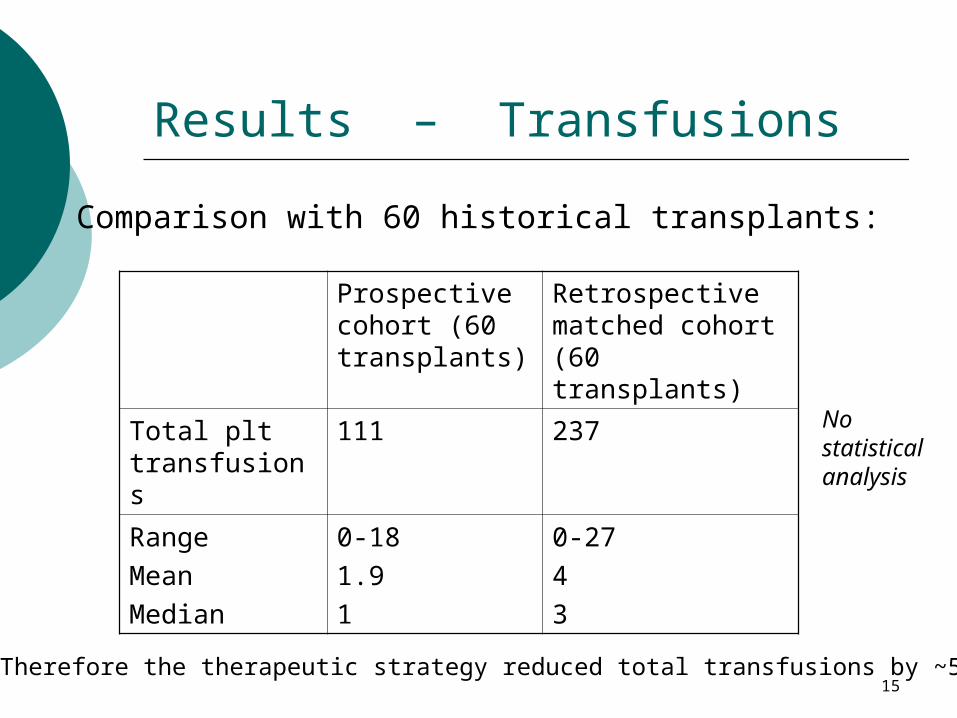
Results – Transfusions
Prospective cohort (60 transplants)
Retrospective matched cohort (60 transplants)
Total plt transfusions
111 237
RangeMeanMedian
0-181.91
0-2743
Therefore the therapeutic strategy reduced total transfusions by ~50%
Comparison with 60 historical transplants:
Nostatisticalanalysis

16
Authors’ conclusions
A therapeutic plt transfusion strategy is safe in autologous PBSCT patients
- No major bleeding (WHO grade III or IV)- Only 19% minor bleeding (WHO grade II)
A therapeutic strategy reduces the total number of plt transfusions compared to a prophylactic strategy
Pts treated with TBI conditioning regimens more likely to require plt transfusion
17
Critical Appraisal Was there randomization?- No; prospective observational cohort (n=140) and a
smaller cohort (n=60) of matched historical transplants
Was follow-up complete?- In the prospective cohort, pts followed until plt count
> 20 for 2-3 consecutive days- No pts lost after enrolment
Was there blinding?- No; treating physicians needed to be aware of plt
transfusion protocol- Bleeding recorded by responsible physician and reviewed
by one of the authors (HW or KS)
18
Critical Appraisal
Were the two groups matched?- First 60 transplants matched for gender, Dx, and TBI
conditioning but prospective cohort slightly older (mean 55 vs 49) – no p value given
- presumably the two groups were treated similarly except for plt transfusion strategy
Outcomes- Not clear whether all the outcomes reported were
predefined at start of study- e.g. # of transfusions related to Dx and conditioning – was
this posthoc analysis? Was study powered to detect differences?
19
Critical Appraisal Can results be applied to patient care?- Applies to adults undergoing autologous PBSCT- This study used only LR apheresis plts- Pts with prior life-threatening bleeding were excluded,
and 34% of all transplants were performed without transfusions – was this a lower risk pt population?
Were all important outcomes considered?- Safety: bleeding complications and number of
thrombocytopenic days- no mention of days in hospital or overall mortality
- Plt utilization: reduced number of plt transfusions compared to historical controls- significant rate of off-protocol transfusions
20
ASH 2006: Abstract #577 Oral Session
Interim analysis of a prospective randomised study comparing a therapeutic platelet transfusion strategy with the prophylactic platelet transfusion standard in patients after autologous peripheral stem cell transplantation (ASCT).
Schaefer-Eckart K, Wendelin K, Wilhelm M, Mahlknecht MU, Conradi R, Schaich M, Leimer L, Wandt H.
21
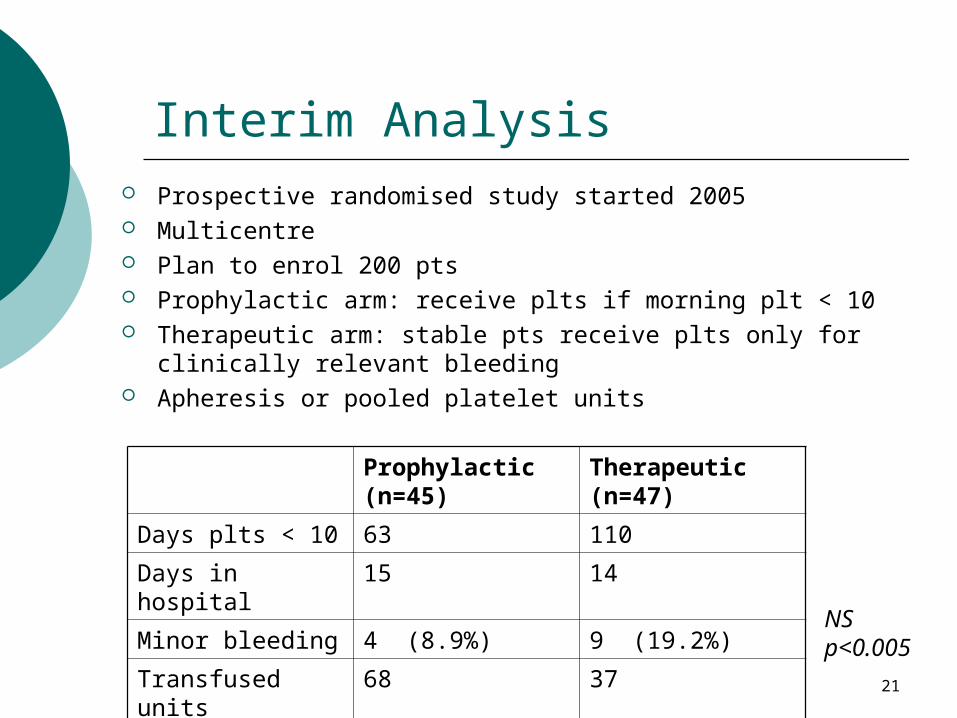
Interim Analysis Prospective randomised study started 2005 Multicentre Plan to enrol 200 pts Prophylactic arm: receive plts if morning plt < 10 Therapeutic arm: stable pts receive plts only for clinically
relevant bleeding Apheresis or pooled platelet units
Prophylactic (n=45)
Therapeutic (n=47)
Days plts < 10 63 110
Days in hospital 15 14
Minor bleeding 4 (8.9%) 9 (19.2%)
Transfused units 68 37NSp<0.005
22
THE END
Thank you!
Comments and questions …