1 2a principles interchangeability testing
DESCRIPTION
Principles Interchangeability TestingTRANSCRIPT
Alfredo García – Arieta, PhD
WHO Workshop on Assessment of Bioequivalence Data, 31 August – 3 September, 2010, Addis Ababa
Principles of Interchangeability Testing

WHO Workshop on Assessment of Bioequivalence Data 31 August – 3 September, 2010, Addis Ababa
WHO GuidelineWHO Guideline
Annex 7 of WHO Technical Report Series, No. 937, 2006
Multisource (generic) pharmaceutical products:guidelines on registration requirements to establish interchangeability
WHO Workshop on Assessment of Bioequivalence Data 31 August – 3 September, 2010, Addis Ababa
Additional GuidanceAdditional Guidance
Proposal to waive in vivo bioequivalence requirements for WHO Model List of Essential Medicines immediate release, solid oral dosage forms (Annex 8)
Additional guidance for organizations performing in vivo bioequivalence studies (Annex 9)
Guidance on the selection of comparator pharmaceutical products for equivalence assessment of interchangeable multisource (generic) products (Annex 11)
WHO Workshop on Assessment of Bioequivalence Data 31 August – 3 September, 2010, Addis Ababa
Additional GuidanceAdditional Guidance
http://apps.who.int/prequal/– Bioequivalence Trial Information Form (BTIF)– Biowaiver Application Form: Biopharmaceutics Classification System (BCS)– Biowaiver Application Form: Additional Strengths– Note to applicants on the choice of comparator products for the
Prequalification Programme• Recommended comparator products: medicines for HIV/AIDS and related diseases• Recommended comparator products: anti-tuberculosis medicines• Recommended comparator products: anti-malarial medicines• Recommended comparator products: Reproductive Health medicines• Recommended comparator products: Influenza-specific antiviral medicines
– General notes on Biopharmaceutics Classification System (BCS)-based biowaiver applications
– Biopharmaceutics Classification System (BCS)-based biowaiver applications: anti-tuberculosis medicines
WHO Workshop on Assessment of Bioequivalence Data 31 August – 3 September, 2010, Addis Ababa
European Union GuidelinesEuropean Union Guidelines
Guideline on the investigation of bioequivalence (2010)
Note for guidance on modified release oral and transdermal dosage form: section II (1999).
Question and answer documents
Draft Guideline on the Validation of Bioanalytical Methods
NfG on the clinical requirements for locally applied, locally acting products containing known constituents (1995)
Guideline on the requirements for clinical documentation for orally inhaled products (OIP) including the requirements for demonstration of therapeutic equivalence between two inhaled products for use in the treatment of asthma and COPD in adults and for use in the treatment of asthma in children and adolescents (2009)
WHO Workshop on Assessment of Bioequivalence Data 31 August – 3 September, 2010, Addis Ababa
US FDA Guidance for IndustryUS FDA Guidance for Industry
Bioavailability and Bioequivalence Studies for Orally Administered Drug Products — General Considerations (2003)
Food-Effect Bioavailability and Fed Bioequivalence Studies (2002).
Waiver of In Vivo Bioavailability and Bioequivalence Studies for Immediate-Release Solid Oral Dosage Forms Based on a Biopharmaceutics Classification System (2000)
Extended Release Oral Dosage Forms: Development, Evaluation, and Application of In Vitro/In Vivo Correlations (1997)
Bioanalytical Method Validation (2001)
Bioavailability and Bioequivalence Studies for Nasal Aerosols and Nasal Sprays for Local Action (Draft 2003)
WHO Workshop on Assessment of Bioequivalence Data 31 August – 3 September, 2010, Addis Ababa
Purpose of WHO GuidelinesPurpose of WHO Guidelines
One of WHO’s constitutional functions is to provide objective and reliable information and advice in the field of human health, a responsibility that it fulfils in part through its programme of publications
The Organization seeks through its publications to support national health strategies and address the most pressing public health concerns of populations around the world.
WHO Workshop on Assessment of Bioequivalence Data 31 August – 3 September, 2010, Addis Ababa
Recommendations for the National Authorities
Recommendations for the National Authorities
The national health and drug regulatory authorities should ensure that all pharmaceutical products subject to their control conform to acceptable standards of safety, efficacy and quality, and that all premises and practices employed in the manufacture, storage and distribution of these products comply with good manufacturing practice (GMP) standards so as to ensure the continued conformity of the products with these requirements until they are delivered to the end-user.
WHO Workshop on Assessment of Bioequivalence Data 31 August – 3 September, 2010, Addis Ababa
Recommendations for the National Authorities
Recommendations for the National Authorities
All pharmaceutical products, including multisource products, should be used in a country only after approval by the local authority
Regulatory authorities should require the documentation of a multisource pharmaceutical product to meet the following:
– GMP;– quality control specifications; and– pharmaceutical product interchangeability.
WHO Workshop on Assessment of Bioequivalence Data 31 August – 3 September, 2010, Addis Ababa
Recommendations for the National Authorities
Recommendations for the National Authorities
Multisource pharmaceutical products need to conform to the same appropriate standards of quality, efficacy and safety as those required of the innovator’s (comparator) product.
In addition, reasonable assurance must be provided that the multisource product is therapeutically equivalent and interchangeable with the comparator product.
WHO Workshop on Assessment of Bioequivalence Data 31 August – 3 September, 2010, Addis Ababa
Clarification of two important concepts:“Prescribability” and “Switchability”
Clarification of two important concepts:“Prescribability” and “Switchability”
Bioequivalent products have efficacy and safety profiles similar to that of the reference product.
Bioequivalence is direct proof that the multisource product can be used for new patients with the same benefit and risk: “Prescribability” (new prescriptions, without any adjustment in dose or other additional therapeutic monitoring)
A patient already under treatment with the reference product can generally be switch to the multisource product: “Switchability” (additional prescriptions)
Bioequivalence is also generally considered as indirect proof of “switchability” between generics / multisource products
WHO Workshop on Assessment of Bioequivalence Data 31 August – 3 September, 2010, Addis Ababa
More terminologyMore terminology
Bioequivalence = Therapeutic equivalence– Biological equivalence– More frequent in North-America– Clinical or PD studies are also methods to show bioequivalence
in addition to PK studies
Bioequivalence = Therapeutic equivalence demonstrated by means of pharmacokinetic studies
– Bioavailability is equivalent.– European Union– Products showing equivalence with clinical or PD studies are
not considered as “generics”
WHO Workshop on Assessment of Bioequivalence Data 31 August – 3 September, 2010, Addis Ababa
Types of in vivo bioequivalence studiesTypes of in vivo bioequivalence studies
Pharmacokinetic studies
Pharmacodynamic studies and
Comparative clinical trials
In vitro studies– In vitro studies are rarely validated as surrogate of BE– But if validated, they are the most sensitive
• BCS Biowaiver, IVIVC, binding studies for cholestyramine…
Sensitivity to detect differences
WHO Workshop on Assessment of Bioequivalence Data 31 August – 3 September, 2010, Addis Ababa
Clinical or PD variables are less sensitiveClinical or PD variables are less sensitive
Bioinequivalent products could be considered therapeutic equivalent with clinical endpoints if such a study were performed
– Bioequivalent: 90% CI of AUC and Cmax for T/R within 80-125– Non-bioequivalent: 90% CI inside and outside of 80-125%– Bioinequivalent: 90% CI completely outside of 80-125%
Therapeutic equivalence can be concluded between immediate release and prolonged release formulations
Therapeutic equivalence can be concluded with different drug substances (e.g. omeprazole, lansoprazole, etc.)
WHO Workshop on Assessment of Bioequivalence Data 31 August – 3 September, 2010, Addis Ababa
Therapeutic equivalenceTherapeutic equivalence
Direct practical demonstration of therapeutic equivalence in a clinical study usually requires large numbers of patients.
Such studies in humans can be financially daunting, are often unnecessary and may be unethical
WHO Workshop on Assessment of Bioequivalence Data 31 August – 3 September, 2010, Addis Ababa
Therapeutic equivalence vs. BioequivalenceTherapeutic equivalence vs. Bioequivalence
For these reasons the science of bioequivalence testing has been developed over the last 40 years.
According to the tenets of this science, therapeutic equivalence can be assured when the multisource product is both pharmaceutically equivalent/alternative and bioequivalent.
Bioequivalence based on blood level determination of Cmax and AUC has become the most commonly used and successful biomarker for safety and efficacy of the drug product.
WHO Workshop on Assessment of Bioequivalence Data 31 August – 3 September, 2010, Addis Ababa
Definition of BioequivalenceDefinition of Bioequivalence
Two pharmaceutical products are bioequivalent if they are:
– Pharmaceutically equivalent or pharmaceutical alternatives, and
– their bioavailabilities, in terms of peak (Cmax and Tmax) and total exposure (area under the curve (AUC)) after administration of the same molar dose under the same conditions, are similar to such a degree that their effects can be expected to be essentially the same.
WHO Workshop on Assessment of Bioequivalence Data 31 August – 3 September, 2010, Addis Ababa
Bioequivalence Basic AssumptionBioequivalence Basic Assumption
If two pharmaceutical products produce an essentially similar plasma concentration - time course in a given subject, then, essentially similar concentrations at the site(s) of action and essentially similar therapeutic outcome will be obtained.
Therefore, PK may be used instead of therapeutic result in pharmaceutical products with systemic action
WHO Workshop on Assessment of Bioequivalence Data 31 August – 3 September, 2010, Addis Ababa
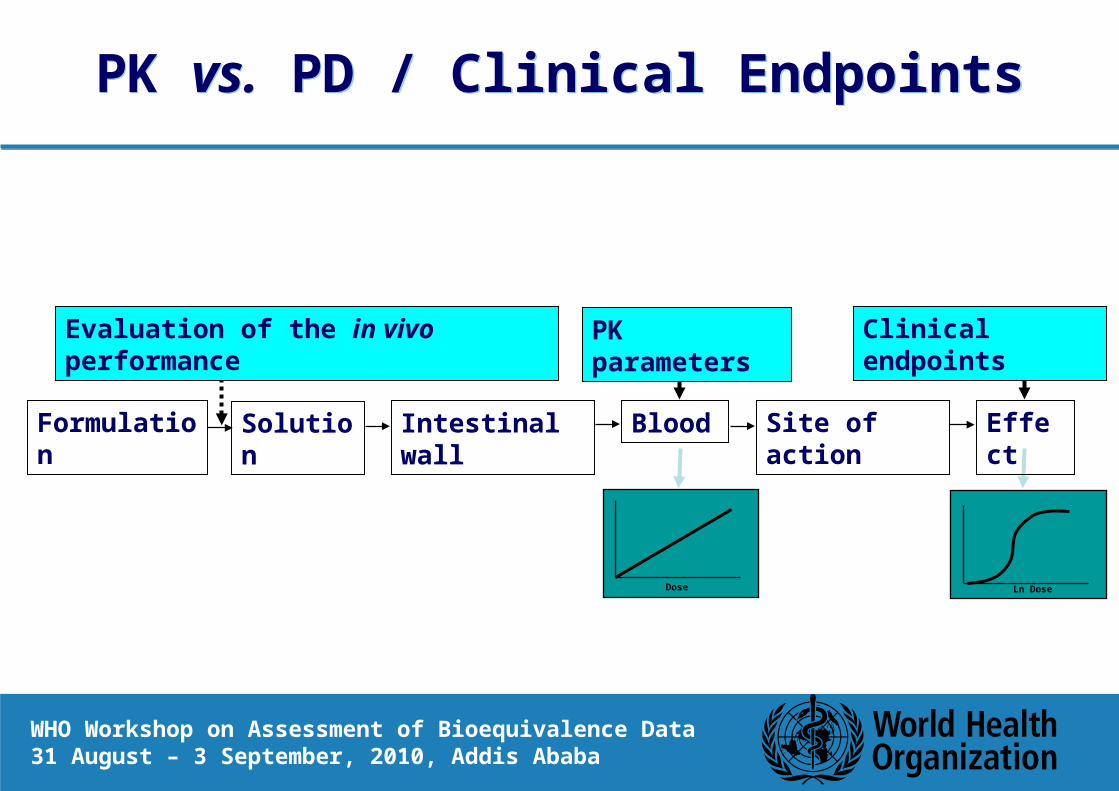
PK vs. PD / Clinical EndpointsPK vs. PD / Clinical Endpoints
Dose Ln Dose
Formulation Solution Intestinal wall Blood Site of action Effect
Evaluation of the in vivo performance PK parameters Clinical endpoints
WHO Workshop on Assessment of Bioequivalence Data 31 August – 3 September, 2010, Addis Ababa
Scope of the Bioequivalence GuidelineScope of the Bioequivalence Guideline
This guidance is generally applicable to orally administered multisource products, as well as to non-orally administered pharmaceutical products for which systemic exposure measures are suitable for documenting bioequivalence (e.g. transdermal delivery systems and certain parenteral, rectal and nasal pharmaceutical products).
WHO Workshop on Assessment of Bioequivalence Data 31 August – 3 September, 2010, Addis Ababa
Scope of the Bioequivalence GuidelineScope of the Bioequivalence Guideline
Systemic action– Oral Immediate Release or Modified Release Products– Transdermal products with systemic action– Certain parental products (e.g. prolonged release),– Rectal, nasal, etc. with systemic effect
Local action– Inhalation products
• For systemic safety (FDA, Canada, EU)• Lung deposition (total and pattern of deposition in EU) as surrogate of efficacy
– Nasal products• For systemic safety (nasal suspensions in FDA draft guidance)
– Gastrointestinal tract (certain drug specific guidance in FDA webpage)• For systemic safety + in vitro dissolution
WHO Workshop on Assessment of Bioequivalence Data 31 August – 3 September, 2010, Addis Ababa
Therapeutic equivalence with Clinical or PD endpoints
Therapeutic equivalence with Clinical or PD endpoints
Systemic action, but no measurable concentrations
Products for local action – Except solutions with the same composition (Q1+Q2)– PD design for cutaneous corticosteroids (skin blanching assay)
• In addition Q1+Q2 in EU– PD design for bronchodilators
• Bronchoconstriction or Bronchodilation– Clinical variables required in other cases
• No FDA model for Inhaled Corticosteroids (NOe)• Dermatopharmacokinetics and Dermal Microdyalisis for cutaneous?
– In vitro acceptable in very few cases (e.g. sevelamer)
WHO Workshop on Assessment of Bioequivalence Data 31 August – 3 September, 2010, Addis Ababa
Excluded Products from Bioequivalence Guidelines
Excluded Products from Bioequivalence Guidelines
For yet other classes of products, including many biologicals such as vaccines, animal sera, products derived from human blood and plasma, and products manufactured by biotechnology, the concept of interchangeability raises complex considerations that are beyond the scope of this document, and these products are consequently excluded from consideration.
WHO Workshop on Assessment of Bioequivalence Data 31 August – 3 September, 2010, Addis Ababa
BiowaiverBiowaiver
Proportional formulations– Bioequivalence has been shown with one strength (most sensitive strength)– Same manufacturing process– Similar dissolution profile
Certain dosage forms (e.g. oral solutions– For some classes of product, including – most evidently – parenteral
formulations of highly water-soluble compounds, interchangeability is adequately assured by implementation of GMP and evidence of conformity with relevant pharmacopoeial specifications.
BCS Biowaivers– In selected cases, in vitro comparison of dissolution profile of the
multisource product with that of the comparator product, or dissolution studies, may be sufficient to provide indication of equivalence.

WHO Workshop on Assessment of Bioequivalence Data 31 August – 3 September, 2010, Addis Ababa
Biowaiver for certain dosage formsBiowaiver for certain dosage forms
Pharmaceutical equivalence may be enough in case of: – Oral aqueous solutions (excluding active excipients)– Aqueous Intravenous solutions (similar excipients)– Aqueous Intramuscular / Subcutaneous solutions (similar excipients and
viscosity)– Oily Intramuscular / Subcutaneous solutions (same oil)– Aqueous Otic / Ophthalmic solutions– Cutaneous solutions (if same Qualitative and Quantitative composition)– Nasal Solutions (if same Q1 and Q2 + in vitro testing for device
performance) – Powders / Granules for reconstitution as solution– Gases
WHO Workshop on Assessment of Bioequivalence Data 31 August – 3 September, 2010, Addis Ababa
4. When equivalence studies are not necessary4. When equivalence studies are not necessary
No PropofolNo Docetaxel
The following types of multisource pharmaceutical product are considered to be equivalent without the need for further documentation:
(a) when the pharmaceutical product is to be administered parenterally (e.g. intravenously, subcutaneously or intramuscularly) as an aqueous solution containing the same API in the same molar concentration as the comparator product and the same or similar excipients in comparable concentrations as in the comparator product.
Certain excipients (e.g. buffer, preservative and antioxidant) may be different provided it can be shown that the change(s) in these excipients would not affect the safety and/or efficacy of the pharmaceutical product

WHO Workshop on Assessment of Bioequivalence Data 31 August – 3 September, 2010, Addis Ababa
Section 4 bSection 4 b
(b) when pharmaceutically equivalent products are solutions for oral use (e.g. syrups, elixirs and tinctures), contain the API in the same molar concentration as the comparator product, and contain essentially the same excipients in comparable concentrations.
Excipient(s) known to affect gastrointestinal (GI) transit, GI permeability and hence absorption or stability of the API in the GI tract should be critically reviewed;
WHO Workshop on Assessment of Bioequivalence Data 31 August – 3 September, 2010, Addis Ababa
Section 4 c - dSection 4 c - d
(c) when pharmaceutically equivalent products are in the form of powders for reconstitution as a solution and the resultant solution meets either criterion (a) or criterion (b) above;
(d) when pharmaceutically equivalent products are gases;
WHO Workshop on Assessment of Bioequivalence Data 31 August – 3 September, 2010, Addis Ababa
Section 4 eSection 4 e
(e) when pharmaceutically equivalent products are otic or ophthalmic products prepared as aqueous solutions and contain the same API(s) in the same molar concentration and essentially the same excipients in comparable concentrations.
Certain excipients (e.g. preservative, buffer, substance to adjust tonicity or thickening agent) may be different provided their use is not expected to affect safety and/or efficacy of the product
Device: volume, handling
WHO Workshop on Assessment of Bioequivalence Data 31 August – 3 September, 2010, Addis Ababa
Section 4 fSection 4 f
(f) when pharmaceutically equivalent products are topical products prepared as aqueous solutions and contain the same API(s) in the same molar concentration and essentially the same excipients in comparable concentrations;
Different excipients probably have different absorption
enhancing effect
WHO Workshop on Assessment of Bioequivalence Data 31 August – 3 September, 2010, Addis Ababa
Section 4 gSection 4 g
Toxicity of preservatives:Chlorobutanol and benzalconium
(g) when pharmaceutically equivalent products are aqueous solutions for nebulizer inhalation products or nasal sprays, intended to be administered with essentially the same device, and contain the same API(s) in the same concentration and essentially the same excipients in comparable concentrations.
The pharmaceutical product may include different excipients provided their use is not expected to affect safety and/or efficacy of the product.
Salbutamol solution for nebilisation with
or without benzalconium
WHO Workshop on Assessment of Bioequivalence Data 31 August – 3 September, 2010, Addis Ababa
Section 4Section 4
For situations (b), (c), (e), (f) and (g) above, it is incumbent upon the applicant to demonstrate that the excipients in the pharmaceutically equivalent product are essentially the same and in concentrations comparable to those in the comparator product or, where applicable (i.e. (e) and (g)), that their use is not expected to affect the safety and/or efficacy of the product.
In the event that this information cannot be provided by the applicant and the drug regulatory authority does not have access to the relevant data, it is incumbent upon the applicant to perform appropriate studies to demonstrate that differences in excipients or devices do not affect product performance.

WHO Workshop on Assessment of Bioequivalence Data 31 August – 3 September, 2010, Addis Ababa
Bioequivalence cannot be assumedBioequivalence cannot be assumed
Pharmaceutical equivalent does not necessarily imply therapeutic equivalence
Differences in:– Raw materials
• Drug (e.g. particle size, polymorphism, etc.)• Excipients (e.g. grade)
– Formulation / composition• Q1 and Q2 (effect on in vivo dissolution and absorption)
– Manufacturing process (e.g. dry vs. wet granulation)– Equipment– Site of Manufacturing– Batch size
May affect the bioavailability of pharmaceutical equivalents or pharmaceutical alternatives.
Then, bioequivalence has to be demonstrated
Reference Test
Pharmaceutical Equivalent Products
Possible Differences
Drug particle size, ...
Excipients
Manufacturing process
Equipment
Site of manufacture
Batch size ….
Documented Bioequivalence= Therapeutic Equivalence
WHO Workshop on Assessment of Bioequivalence Data 31 August – 3 September, 2010, Addis Ababa
Bioequivalence / Comparative Bioavailability is required
Bioequivalence / Comparative Bioavailability is required
In vivo documentation of equivalence is needed when there is a risk that possible differences in bioavailability may result in therapeutic inequivalence.
When the innovator develops a new formulation– During the drug-development process (before approval)– As a variation of the marketed product after approval
When the innovator develops a new dosage form– Line extension
When a multisource (generic) product is applied for marketing authorisation
WHO Workshop on Assessment of Bioequivalence Data 31 August – 3 September, 2010, Addis Ababa
InterchangeabilityInterchangeability
The concept of interchangeability includes the equivalence of the dosage form as well as of the indications and instructions for use.
– If BE is shown, it is equivalent in all indications if used according to the instructions of use.
– Some indications may be protected by patent– Interchangeability
• If both products in the same dosage form in some countries (e.g. USA)• Between capsules and tablets (e.g. Canada)• All oral immediate release dosage forms (e.g. EU)
WHO Workshop on Assessment of Bioequivalence Data 31 August – 3 September, 2010, Addis Ababa
Final conceptsFinal concepts
Average Bioequivalence:– ABE compares population mean values of AUC, Cmax, …
Population Bioequivalence:– Proposal to compare population mean values and total variability– To improve assurance of prescribability. Not used.
Individual Bioequivalence:– Proposal to compare mean values, intra-subject variability and subject-by-
formulation interaction.– To improve switchability. Not used.– Aggregate criterion more permissive than ABE– Unnecessary. SxF interaction mostly an artifact
WHO Workshop on Assessment of Bioequivalence Data 31 August – 3 September, 2010, Addis Ababa
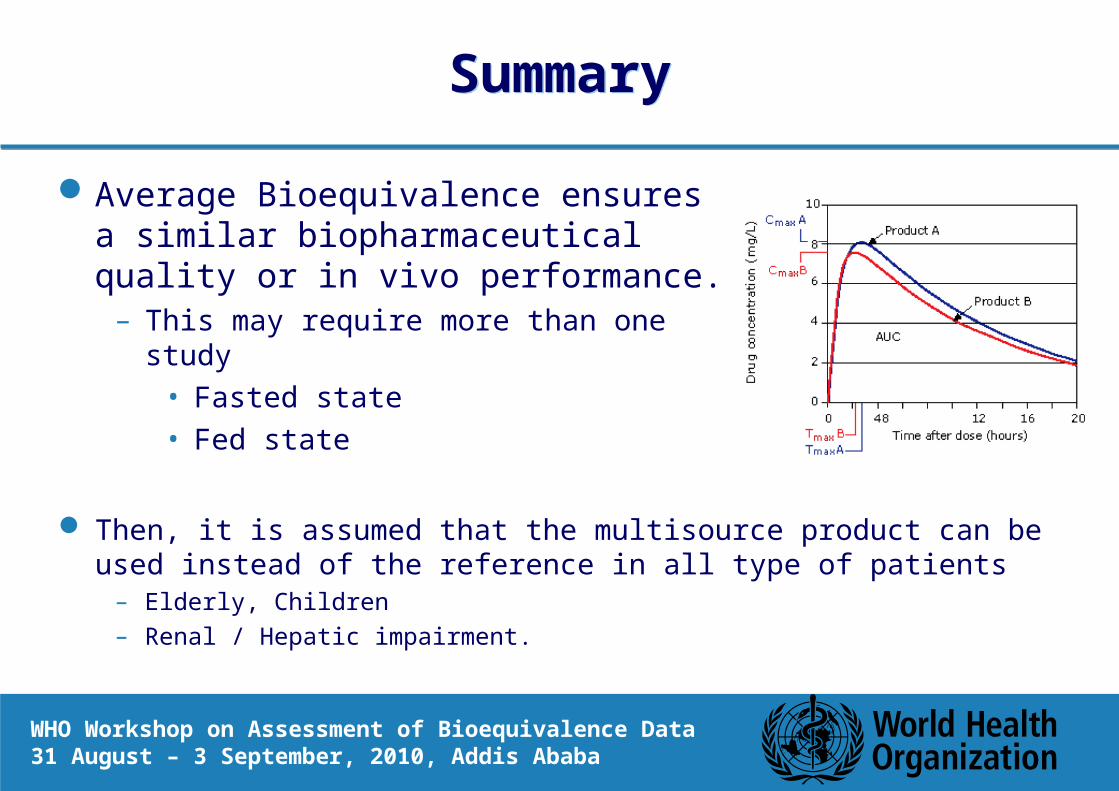
SummarySummary
Average Bioequivalence ensures a similar biopharmaceutical quality or in vivo performance.
– This may require more than one study• Fasted state• Fed state
Then, it is assumed that the multisource product can be used instead of the reference in all type of patients
– Elderly, Children– Renal / Hepatic impairment.

WHO Workshop on Assessment of Bioequivalence Data 31 August – 3 September, 2010, Addis Ababa
Thank you very much for your attention!Thank you very much for your attention!