1 2 copy personal - university of malaya · original research article ... single cone (sc)...
TRANSCRIPT

JABFMeISSN 2280-8000
J Appl Biomater Funct Mater 2016; 14(3): e307-e313
© 2016 Wichtig Publishing
Original research article
root canals, they are incapable of accomplishing a good seal along the dentinal walls of the root canal (9). Because the ad-hesive potential of GP with canal sealers has been shown to be unsatisfactory, resin-coated GP points (EndoREZ® Points [ER Points]) have been introduced (10). ER Points facilitate a chemical bond with any resin-based sealer, thus creating a monoblock (11, 12). The term monoblock refers to the produc-tion of a single unit; however, recently it has been used for the introduction of adhesive root canal obturation materials (13).
The cold lateral compaction (CLC) of GP is considered as one of the most widely accepted canal obturation techniques and is taught in many dental schools (14). This is because of its advantages of controlled placement of GP in the root ca-nal and low cost (15). With this technique, specially designed spreaders are placed as far apically as possible, and the mas-ter core filling is laterally compacted against the canal walls. Then, additional accessory points are inserted and compacted laterally around the master cone (16). The disadvantages of this technique include an increased risk of dentinal damage and vertical root fracture. Additionally, nonfilled spreader tracks are recurrently present in the filling which decreases the obturation quality (17). In contrast, the thermoplasticized GP technique can easily move GP into the canal irregularities, thus replicating the particulars of the root canal system (18). Warm lateral compaction (WLC) of GP is a modification of CLC, which, at the same time, thermoplasticizes the entire GP obtu-ration mass (19). In this technique, a heated spreader is used
DOI: 10.5301/jabfm.5000273
Comparison between gutta-percha and resin-coated gutta-percha using different obturation techniquesNashwan A. Al-Afifi1, Mariam Abdullah1, Samah M. Al-Amery2, Mohamed Abdulmunem1
1 Department of Restorative Dentistry, Faculty of Dentistry, University of Malaya, Lembah Pantai, Kuala Lumpur - Malaysia2 Department of Diagnostic and Integrated Dental Practice, Faculty of Dentistry, University of Malaya, Lembah Pantai, Kuala Lumpur - Malaysia
Introduction
Obturation of the root canal system is one of the impor-tant steps in root canal treatment. Obturation is considered as a function in which portals of entry between the canal and the periodontium are eliminated (1). In general, obturation in-volves a combination of core material, such as gutta-percha (GP) and a sealer (2). A good root canal obturating material should be well adapted to the canal walls and its irregularities. Thus, the entire length of the canal is densely compacted with a homogeneous mass of core filling material. Consequently, the quantity of core material should be maximized while the quantity of sealer should be minimized (3, 4). GP has been accepted as the gold standard root filling material (5), and the material against which most others are compared (6-8). Although GP and root canal sealers are used to obturate the
abstractBackground: The aim of this study was to evaluate and compare the obturation quality between canals obturated with gutta-percha/AH Plus sealer (GP group) and resin-coated GP/EndoREZ® sealer (ER group).Methods: A total sample of 90 mandibular premolar teeth was divided into 2 groups (2 × 45 canals): the GP group and ER group. Each group was further divided into 3 subgroups (n = 15): cold lateral compaction (CLC), warm lateral compaction (WLC) and single cone (SC). The teeth were subsequently embedded in resin and sectioned horizontally at 1, 3, 6 and 9 mm. All sections were then viewed with a stereomicroscope at ×40 magnification. The area occupied by core filling materials was determined using Cell^D software.Results: With CLC, the percentage of core filling materials in the ER group was significantly higher than in the GP group at the 1- and 3-mm levels. Similarly, with WLC, the percentage of core filling material in the ER group was significantly higher than in the GP group at the 1-, 3- and 9-mm levels. With SC, the percentage of core filling materials in the ER group was significantly higher than in the GP group at all levels.Conclusions: It can be concluded that the resin-coated GP/EndoREZ® sealer is superior to the gutta-percha/AH Plus in the percentage of core filling material.Keywords: AH Plus, EndoREZ, Gutta-percha, Obturation
Accepted: January 8, 2016Published online: May 2, 2016
Corresponding author:Dr. Nashwan A. Al-AfifiFaculty of DentistryUniversity of Malaya50603 Lembah PantaiKuala Lumpur, [email protected]
Author
perso
nal c
opy

Obturation quality of gutta-percha and resin-coated gutta-perchae308
© 2016 Wichtig Publishing
to soften the GP inside the canal, and then a cold spreader is inserted to create sufficient space for accessory points (16, 20). To allow better adaptation of the GP points to the canal walls during the thermoplasticized GP technique, GP points with different tapers, 0.04-0.08, were introduced, which cor-respond to the taper of the rotary nickel-titanium (NiTi) in-struments. Reports in the literature, however, suggest there is no advantage of 0.06 taper GP points over the 0.02 taper (21). Therefore, single cone (SC) obturation of root canals, a noncompaction technique, has recently been revitalized as a result of the introduction of a greater taper master core point (22). The SC technique may, moreover, produce an adequate root canal obturation without the use of more complicated and time-consuming techniques, such as lateral compaction or warm vertical compaction (23). Nevertheless, this tech-nique relies on the original canal tapered circular preparation. Therefore, only small diameter and minimally curved roots are suitable for this technique (24).
There are many obturation materials and techniques that could be used to obturate the root canal space; however, studies that have investigated the root canal obturation qual-ity using resin-coated GP points are sparse. Therefore, the aim of this study was to evaluate and compare the obturation quality of different obturation materials – GP points/AH Plus sealer and resin-coated GP/EndoREZ® sealer – using different obturation techniques (CLC, WLC and SC).
Materials and methods
Tooth collection, storage and selection
Two hundred extracted single-rooted mandibular pre-molar teeth were collected regardless of age and race. The teeth were stored in 0.5% chloramine-T trihydrate solution for 1 week. Ultrasonic scaler (Densply® Cavitron® Bobcat® Pro, USA) was used to remove both calculus deposits and re-sidual periodontal tissues. Throughout this study, the teeth were kept hydrated in distilled water to maintain dentine per-meability. The storage solution was changed regularly every 1 week, and the teeth were stored at 4°C.
A total of 90 of the 200 teeth had a single root canal, which was relatively straight, with a well-developed root and com-pletely formed canal with patent foramen and teeth, with a canal diameter smaller or equal to a size 15 K-File (Colorinox; Dentsply Maillefer) at 4-5 mm from the radiographic apex, and these were used for the purposes of this study. In addi-tion, an attempt was made to standardize the size and shape of the selected teeth (diameters at cervix were 5.0-5.5 mm mesiodistally and 7.5-8.0 mm buccolingually).
Canal preparation
The teeth were decoronated with a sectioning machine (Metkon® Micracut® 125 Low Speed Precision Cutter) at the lev-el of 16 mm from the apex perpendicular to the long axis of the root canal, to relatively standardize the length for all specimens.
The working length was determined by insertion of size 15 K-File (Colorinox; Dentsply Maillefer) into the root ca-nal until it was visible in the apical foramen, and then the working length of each canal was calculated to 1.0 mm short
of that position. All root canals were prepared with the size 15 K-Files (Colorinox; Dentsply Maillefer) and Mtwo® NiTi ro-tary instrument (VDW, München, Germany).
Initially, the size 15 K-File (Colorinox; Dentsply Maillefer) was introduced into each root canal to produce a glide path, and then to complete the root canal preparation, the Mtwo® NiTi rotary instruments were used according to the manufac-turer’s instructions, starting with size 15/0.05 to size 35/0.04, which was used as the master apical file (MAF). All rotary root canal instruments were used to the full working length of the canals, employing a cyclical in-out brushing motion. After each instrument, the canal was irrigated with 2.0 mL of 5.25% so-dium hypochlorite (NaOCl) delivered using Ultradent® 5-mL syringe (Ultradent Products Inc., USA) with a 27-gauge needle (Ultradent). The apical patency was established throughout the preparation by passing a size 10 K-File 1.0 mm beyond the apical foramen. Once root canal preparation was completed, each ca-nal was then irrigated in the following sequence: 3.0 mL 5.25% NaOCl, 3.0 mL 18% ethylenediaminetetraacetic acid (EDTA) to remove the smear layer and finally 3.0 mL distilled water to en-sure complete removal of the irrigation solutions from the root canal. Each irrigation solution was used for 1 minute.
Each specimen was then dried with a paper point (VDW, München, Germany) prior to the application of the obtura-tion materials.
Canal obturation
A total of 90 mandibular premolar teeth were randomly divided into 2 main groups (2 × 45 canals): the GP group and the ER group. A total of 45 canals in each group was randomly divided into 3 subgroups (n = 15) according to different obtu-ration techniques (CLC, WLC and SC).
CLC technique
CLC of GP
An ISO-standardized GP point size 35/0.02 (VDW, München, Germany) which fitted to the working length was chosen as the master cone. AH Plus sealer was placed into the canal using a paper point. The master cone was then placed to working length. A size 25 finger spreader (VDW, München, Germany) was advanced to within 1 mm of the working length, rotated and removed. Then, a GP accessory point size 25/0.02 (VDW, München, Germany) was placed into the prepared space. This was repeated until the spreader could not be inserted 2-3 mm into the canal. The excesses of the GP points were removed with a heat plugger standard BeeFill® 2in1 device (VDW, München, Germany). Following this, the GP in the coronal por-tion was vertically compacted using a root canal plugger, size 4.
CLC of ER
An ISO-standardized ER master cone size 35/0.02 (Ultra-dent) was chosen as a master cone. The ER sealer (Ultradent) was applied in the canal according to the manufacturer’s in-structions, by inserting the delivery NaviTip (Ultradent) into the root canal to within 2-4 mm short of the apex. The tip was withdrawn slowly while expressing ER sealer coronally to the
Author
perso
nal c
opy
Al-Afifi et al e309
© 2016 Wichtig Publishing
canal orifice. A paper point, size 35, was then inserted to the working length and smeared onto the canal walls to remove ex-cess sealer from the canal. Then the paper point was removed. The same steps were followed as described in the section “CLC of GP” to obturate the canals, except that the ER accessory point size 25/0.02 (Ultradent) was used instead of a GP point.
WLC technique
WLC of GP
An ISO-standardized GP point size 35/0.02 (VDW, München, Germany) which fitted to the working length was chosen as the master cone. AH Plus sealer was placed into the canal using a paper point. The master cone was then placed to the working length. A heat plugger standard BeeFill® 2in1 device was then introduced 2.0 mm short of the working length at 100°C (the lowest power setting). Next, the cold spreader was inserted 1 mm short of the working length, rotated and removed. Then, the first GP accessory point size 25/0.02 was inserted into the prepared space. This was repeated until the cold spreader could not be inserted 2-3 mm into the canal. The excess of the GP points was removed with a heat plugger standard BeeFill® 2in1 device. Next, the GP in the coronal portion was vertically compacted using a root canal plugger, size 4.
WLC of ER
An ISO-standardized ER point size 35/0.02 (Ultradent) which fitted to the working length was chosen as a master cone. The ER sealer (Ultradent) was then applied in the canal according to the manufacturer’s instructions as described in the section “CLC of ER.” The master cone was inserted to the working length. A heat plugger standard BeeFill® 2in1 device was then introduced 2.0 mm short of the working length at 100°C. Next, the cold spreader was inserted 1 mm short of the working length, rotated and removed. The first ER acces-sory point size 25/0.02 was inserted into the prepared space. This was repeated until the cold spreader could not be in-serted 2-3 mm into the canal. The same steps were followed as described in the section “WLC of GP.”
SC technique
SC of GP
AH Plus sealer was placed into the canal using a paper point. A standardized GP master cone size 35/0.04 (VDW, München, Germany) was placed to the working length, and GP accessory points size 25/0.02 were inserted passively into the canal. The excess of the GP points was removed with a heat plugger standard BeeFill® 2in1 device (VDW, München, Germany). Next, the GP in the coronal portion was vertically compacted using a root canal plugger, size 4.
SC of ER
A skinny syringe with a NaviTip was inserted 2-4 mm short of the apex, and ER sealer was introduced slowly while withdrawing the NaviTip from the canal space. A paper point
was inserted into the canal to remove excess sealer. An ER master cone size 35/0.04 was placed to the working length, and ER accessory points 25/.02 were placed passively in the root canal. The excess of the ER Points was removed with a heat plugger standard BeeFill® 2in1 device. Next, the ER Points in the coronal portion were vertically compacted using a root canal plugger, size 4.
In each GP and ER group, following the obturation tech-nique, the access cavities of the specimens were restored with IRM (Dentsply Caulk, Milford, USA). Additionally, in the ER group, prior to placement of IRM, the coronal surface was light cured for 40 seconds to produce an immediate coronal seal, as recommended by the manufacturer.
All specimens were then kept in an incubator (Memmert, Germany) at 37°C in 100% humidity for 1 week, to allow com-plete setting of the sealer.
Sectioning of specimens
First, each specimen was fixed in a plastic cuvette using baseplate wax, and then embedded in epoxy resin. The ep-oxy resin was allowed to set for 24 hours. Next, the speci-mens were ground from the root tip with a grinding machine (METASERV® 2000 GRINDER POLISHER) until obturation ma-terial was visible.
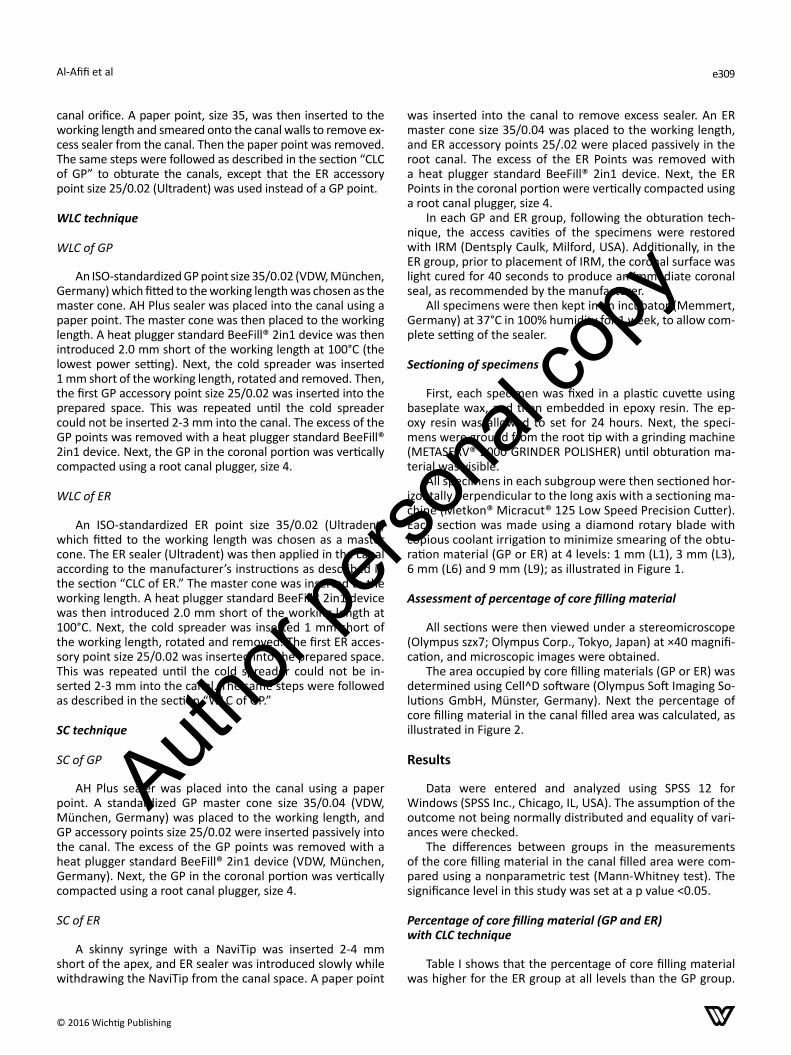
All specimens in each subgroup were then sectioned hor-izontally perpendicular to the long axis with a sectioning ma-chine (Metkon® Micracut® 125 Low Speed Precision Cutter). Each section was made using a diamond rotary blade with copious coolant irrigation to minimize smearing of the obtu-ration material (GP or ER) at 4 levels: 1 mm (L1), 3 mm (L3), 6 mm (L6) and 9 mm (L9); as illustrated in Figure 1.
Assessment of percentage of core filling material
All sections were then viewed under a stereomicroscope (Olympus szx7; Olympus Corp., Tokyo, Japan) at ×40 magnifi-cation, and microscopic images were obtained.
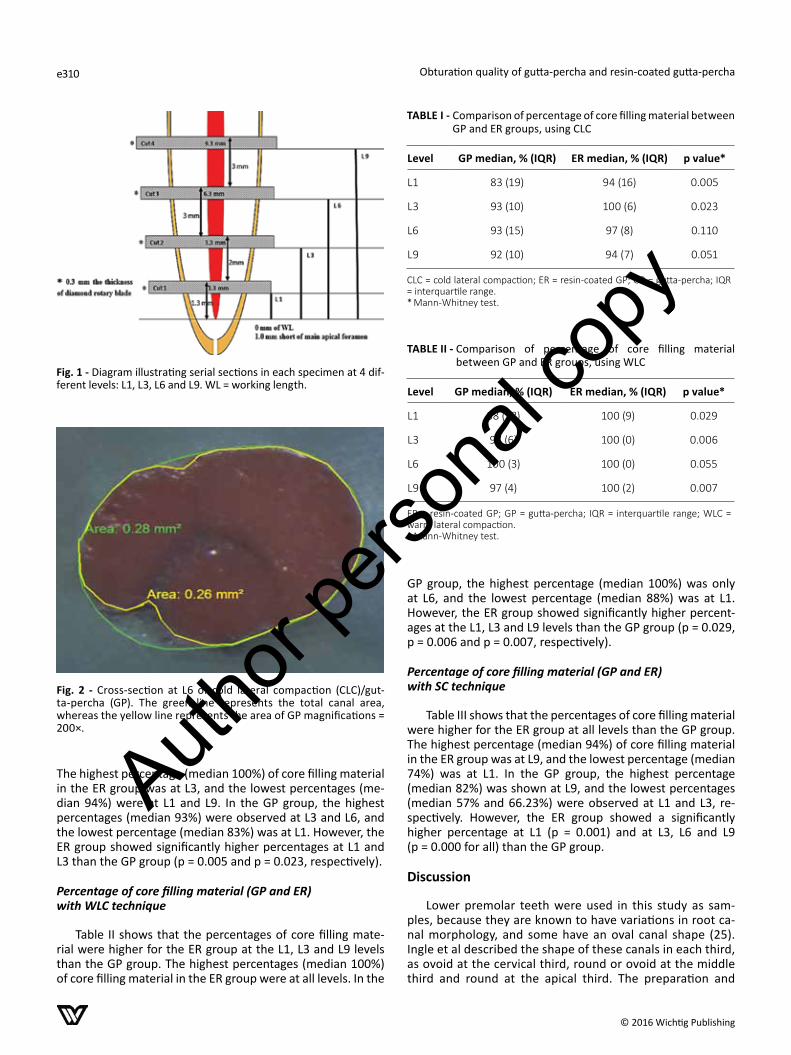
The area occupied by core filling materials (GP or ER) was determined using Cell^D software (Olympus Soft Imaging So-lutions GmbH, Münster, Germany). Next the percentage of core filling material in the canal filled area was calculated, as illustrated in Figure 2.
Results
Data were entered and analyzed using SPSS 12 for Windows (SPSS Inc., Chicago, IL, USA). The assumption of the outcome not being normally distributed and equality of vari-ances were checked.
The differences between groups in the measurements of the core filling material in the canal filled area were com-pared using a nonparametric test (Mann-Whitney test). The significance level in this study was set at a p value <0.05.
Percentage of core filling material (GP and ER) with CLC technique
Table I shows that the percentage of core filling material was higher for the ER group at all levels than the GP group.
Author
perso
nal c
opy
Obturation quality of gutta-percha and resin-coated gutta-perchae310
© 2016 Wichtig Publishing
The highest percentage (median 100%) of core filling material in the ER group was at L3, and the lowest percentages (me-dian 94%) were at L1 and L9. In the GP group, the highest percentages (median 93%) were observed at L3 and L6, and the lowest percentage (median 83%) was at L1. However, the ER group showed significantly higher percentages at L1 and L3 than the GP group (p = 0.005 and p = 0.023, respectively).
Percentage of core filling material (GP and ER) with WLC technique
Table II shows that the percentages of core filling mate-rial were higher for the ER group at the L1, L3 and L9 levels than the GP group. The highest percentages (median 100%) of core filling material in the ER group were at all levels. In the
GP group, the highest percentage (median 100%) was only at L6, and the lowest percentage (median 88%) was at L1. However, the ER group showed significantly higher percent-ages at the L1, L3 and L9 levels than the GP group (p = 0.029, p = 0.006 and p = 0.007, respectively).
Percentage of core filling material (GP and ER) with SC technique
Table III shows that the percentages of core filling material were higher for the ER group at all levels than the GP group. The highest percentage (median 94%) of core filling material in the ER group was at L9, and the lowest percentage (median 74%) was at L1. In the GP group, the highest percentage (median 82%) was shown at L9, and the lowest percentages (median 57% and 66.23%) were observed at L1 and L3, re-spectively. However, the ER group showed a significantly higher percentage at L1 (p = 0.001) and at L3, L6 and L9 (p = 0.000 for all) than the GP group.
Discussion
Lower premolar teeth were used in this study as sam-ples, because they are known to have variations in root ca-nal morphology, and some have an oval canal shape (25). Ingle et al described the shape of these canals in each third, as ovoid at the cervical third, round or ovoid at the middle third and round at the apical third. The preparation and
Fig. 1 - Diagram illustrating serial sections in each specimen at 4 dif-ferent levels: L1, L3, L6 and L9. WL = working length.
Fig. 2 - Cross-section at L6 of cold lateral compaction (CLC)/gut-ta-percha (GP). The green line represents the total canal area, whereas the yellow line represents the area of GP magnifications = 200×.
TABLE I - Comparison of percentage of core filling material between GP and ER groups, using CLC
Level GP median, % (IQR) ER median, % (IQR) p value*
L1 83 (19) 94 (16) 0.005
L3 93 (10) 100 (6) 0.023
L6 93 (15) 97 (8) 0.110
L9 92 (10) 94 (7) 0.051
CLC = cold lateral compaction; ER = resin-coated GP; GP = gutta-percha; IQR = interquartile range.* Mann-Whitney test.
TABLE II - Comparison of percentage of core filling material between GP and ER groups, using WLC
Level GP median, % (IQR) ER median, % (IQR) p value*
L1 88 (18) 100 (9) 0.029
L3 97 (6) 100 (0) 0.006
L6 100 (3) 100 (0) 0.055
L9 97 (4) 100 (2) 0.007
ER = resin-coated GP; GP = gutta-percha; IQR = interquartile range; WLC = warm lateral compaction.* Mann-Whitney test.
Author
perso
nal c
opy

Al-Afifi et al e311
© 2016 Wichtig Publishing
obturation of these canals have been considered to pose a challenge (25).
For many years, dye leakage studies have been the most commonly used method to evaluate the quality of root canal fillings. However, the reliability of those results has been ques-tioned (26). This is due to the fact that the dye penetration may be hindered by entrapped air and may not be visible because the dye can lose its color when in contact with some root filling materials (24, 27). In general, good obturation should consist of a large amount of core material and minimal amount of sealer (28). This is because the sealer will be dissolved with time, thus creating spaces, which can act as a venue for a potential leak-age area (25). Consequently, the percentage of GP-filled canal area has been used as a measure of obturation quality (29). A high percentage of core filling material with a low percent-age of sealer plus voids indicates good obturation quality (27). Therefore, a cross-sectioning method was used in this study to evaluate the quality of 2 different materials (GP and ER) for each obturation technique.
The aim of root canal obturation is to provide a complete filling of the canal in all dimensions (3). A variety of mate-rials and techniques have been developed to improve the sealing quality and reinforcing effect of root canal obturation (30). With the CLC technique, it has been shown that the api-cal seal is best produced when the spreader can be placed close to the working length (31). The spreader’s shape and its depth of penetration are considered to be important fac-tors in producing a more homogenous root canal filling (32). In the current study, however, with the CLC technique, the percentage of ER core filling material was significantly higher than the percentage of GP core filling material, at L1 and L3 (p < 0.05). This might be due to the fact that with this tech-nique, it was apparent that the depth of spreader penetra-tion in the ER group was better than that in the GP group. This result is in agreement with a study performed by Nielsen and Baumgartner (33), who evaluated spreader penetration with Resilon® (a resin-based material) and GP using CLC. They found that spreader penetration was better with Resilon® than with GP. Improved penetration of a spreader may allow better placement of accessory points into the canals even to the apical third of the canal area, as observed in the ER group in this present study. However, there has not been an earlier study to investigate spreader penetration using the ER Points, thus no direct comparison can be made.
With the WLC technique, the percentage of core filling material in the ER group at the L1, L3 and L9 levels was high-er than that in the GP group, with a significant difference for L1, L3 and L9 (p < 0.05). This might be associated with better plasticity and flow rate of the softened core filling material of the ER group compared with that of the GP group. This result was in agreement with that in a study performed by Epley et al (3), who evaluated obturation of lateral canals and found that the penetration of filling material was a function of the viscoelastic properties of the filling material. Moreover, Gurgel-Filho et al (34), who assessed the ability of different GP brands to fill simulated lateral canals, sug-gested that the brand of GP point had an influence on the length of filling within lateral canals. The flow rate capacity was affected directly by the variation in the amounts of zinc oxide and GP in the products. Higher amounts of GP in the composition of some commercial brands demonstrated a better ability to fill simulated accessory canals, wide canals and other anatomical irregularities (35). GP is a natural poly-mer that undergoes an industrial process prior to its use in the patient. This may influence its thermoplasticity behav-ior (3). However, one should take into consideration the fact that the thermal properties of the ER Points have yet to be determined.
The SC technique was included in the present study based on the information mentioned by the manufacturer of ER to the effect that SC is the preferred technique. They mentioned that in large canals, additional ER point size 25/0.02 may be inserted as a “harpoon.” No “condensation” is necessary. With the SC technique, the ER group showed a higher percentage of core filling material than the GP group, with a statistically significant difference at all levels (p < 0.05). This might be due to the monoblock formation in the ER group. The monoblock concept refers to “the creation of a solid, bonded, continuous material from one dentine wall of the canal to the other” (36). Another research finding showed that a monoblock in ER ob-turation materials is created by deep penetration of the sealer into dentinal tubules and a chemical bond between ER sealer and ER Points (37).
Conclusions
Under the experimental conditions of the present study, the ER group was superior to the GP group in maximizing the percentage of core filling material occupying the canal area. Based on the different obturation techniques, the following conclusions can be reached:
1. CLC technique: the ER group was better than the GP group for maximizing the amount of filling core material at all levels, with a statistically significant difference at the 1- and 3-mm levels.
2. WLC technique: the ER group was better than the GP group for maximizing the amount of core filling material at L1, L3 and L9, with a statistically significant difference at the 1-, 3- and 9-mm levels.
3. SC technique: the ER group was better than the GP group for maximizing the amount of core filling ma-terial, with a statistically significant difference at all levels.
TABLE III - Comparison of percentage of core filling material between GP and ER groups, using SC
Level GP median, % (IQR) ER median, % (IQR) p value*
L1 57 (22) 74 (17) 0.001
L3 66.23 (14) 90 (6) 0.000
L6 78 (14) 91 (8) 0.000
L9 82 (6) 94 (3) 0.000
ER = resin-coated GP; GP = gutta-percha; IQR = interquartile range; SC = single cone.* Mann-Whitney test.
Author
perso
nal c
opy

Obturation quality of gutta-percha and resin-coated gutta-perchae312
© 2016 Wichtig Publishing
In conclusion, we can obviously note that with the SC tech-nique, the amount of core filling material was higher than in the GP group. Therefore, if dental practitioners want to use a simple and fastest obturation technique (i.e., SC), they can select resin-coated GP/EndoREZ® sealer to obturate the root canal space. However, in this study, the SC technique was performed with a gentle “harpooning” motion using a greater tapered point with passive insertion of additional accessory points.
AcknowledgementThe authors would like to express their appreciation and deepest gratitude to the Faculty of Dentistry, University of Malay (postgradu-ate research grant no. PS 169/2010B) for their support during all steps of this project.
DisclosuresFinancial support: A postgraduate research grant (PPP) from the Faculty of Dentistry, University of Malay (grant no. PS 169/2010B) was received by Nashwan A. Al-Afifi and Mariam Abdullah.Conflict of interest: There are no conflicts.
References1. Kuçi A, Alaçam T, Yavaş O, Ergul-Ulger Z, Kayaoglu G. Sealer
penetration into dentinal tubules in the presence or absence of smear layer: a confocal laser scanning microscopic study. J Endod. 2014;40(10):1627-1631.
2. Onay EO, Ungor M, Ozdemir BH. In vivo evaluation of the bio-compatibility of a new resin-based obturation system. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 2007;104(3): e60-e66.
3. Epley SR, Fleischman J, Hartwell G, Cicalese C. Completeness of root canal obturations: epiphany techniques versus gutta-percha techniques. J Endod. 2006;32(6):541-544.
4. Hammad M, Qualtrough A, Silikas N. Evaluation of root canal obturation: a three-dimensional in vitro study. J Endod. 2009; 35(4):541-544.
5. Monteiro J, de Ataide IN, Chalakkal P, Chandra PK. In vitro resis-tance to fracture of roots obturated with Resilon or gutta-percha. J Endod. 2011;37(6):828-831.
6. Prado M, de Assis DF, Gomes BP, Simão RA. Effect of disinfec-tant solutions on the surface free energy and wettability of filling material. J Endod. 2011;37(7):980-982.
7. Tuncer K, Aysun ST, Selçuk Gökyay S. Correlation between sealer penetration into dentinal tubules and bond strength of two new calcium silicate-based and an epoxy resin-based, endodontic sealer. J Adhes Sci Technol. 2014;28(7): 702-710.
8. Mohammadi Z, Shalavi S. Clinical applications of glass ionomers in endodontics: a review. Int Dent J. 2012;62(5): 244-250.
9. Stiegemeier D, Baumgartner JC, Ferracane J. Comparison of push-out bond strengths of Resilon with three different seal-ers. J Endod. 2010;36(2):318-321.
10. Kim YK, Grandini S, Ames JM, et al. Critical review on meth-acrylate resin-based root canal sealers. J Endod. 2010;36(3): 383-399.
11. Shanahan DJ, Duncan HF. Root canal filling using Resilon: a review. Br Dent J. 2011;211(2):81-88.
12. Drukteinis S, Peciuliene V, Maneliene R, Bendinskaite R. In vitro study of microbial leakage in roots filled with EndoREZ sealer/
EndoREZ Points and AH Plus sealer/conventional gutta-percha points. Stomatologija. 2009;11(1):21-25.
13. de Sousa Menezes M, Queiroz EC, Soares PV, Faria-e-Silva AL, Soares CJ, Martins LR. Fiber post etching with hydrogen per-oxide: effect of concentration and application time. J Endod. 2011;37(3):398-402.
14. Gençoğlu N. Comparison of 6 different gutta-percha tech-niques: Part II: Thermafil, JS Quick-Fill, Soft Core, Microseal, System B, and lateral condensation. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 2003;96(1):91-95.
15. Hale R, Gatti R, Glickman GN, Opperman LA. Comparative analysis of carrier-based obturation and lateral compaction: a retrospective clinical outcomes study. Int J Dent. 2012;2012: 954675.
16. Wesselink P. Root filling technques. In: Bergenholtz G, Hörsted-Bindslev P, Reit C, eds. Textbook of endodontology. 2nd ed. Chichester, UK: Wiley-Blackwell. 2009;219-233.
17. Wu MK, Bud MG, Wesselink PR. The quality of single cone and laterally compacted gutta-percha fillings in small and curved root canals as evidenced by bidirectional radiographs and fluid transport measurements. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 2009;108(6):946-951.
18. Gilhooly RMP, Hayes SJ, Bryant ST, Dummer PM. Comparison of lateral condensation and thermomechanically compacted warm alpha-phase gutta-percha with a single cone for obtu-rating curved root canals. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 2001;91(1):89-94.
19. Ulusoy Öİ, Yılmazoğlu MZ, Görgül G. Effect of several ther-moplastic canal filling techniques on surface temperature rise on roots with simulated internal resorption cavities: an infrared thermographic analysis. Int Endod J. 2015;48(2): 171-176.
20. Ingle John I, Newton Carl W, West John D, et al. Obturation of the radicular space. In: Ingle JI, Bakland LK, eds. Endodontics. 5th ed. Hamilton, ON: PMPH/BC Decker. 2002;571-667.
21. Al-Hadlaq SM, Al-Rabiah AA. In vitro evaluation of three tech-niques to obturate 0.06 taper canal preparations. Aust Endod J. 2005;31(2):63-65.
22. Royer K, Liu XJ, Zhu Q, Malmstrom H, Ren YF. Apical and root canal space sealing abilities of resin and glass ionomer-based root canal obturation systems. Chin J Dent Res. 2013;16(1): 47-53.
23. Pitout E, Oberholzer T. Leakage of teeth root-filled with Gut-taFlow and a single GP cone compared to lateral condensa-tion and warm vertical condensation. South African Dental Journal. 2009;64(3):104-108.
24. Topçuoğlu HS, Demirbuga S, Tuncay Ö, Arslan H, Kesim B, Yaşa B. The bond strength of endodontic sealers to root den-tine exposed to different gutta-percha solvents. Int Endod J. 2014;47(12):1100-1106.
25. Rodrigues A, Bonetti-Filho I, Faria G, Andolfatto C, Camargo Vilella Berbert FL, Kuga MC. Percentage of gutta-percha in me-sial canals of mandibular molars obturated by lateral compac-tion or single cone techniques. Microsc Res Tech. 2012;75(9): 1229-1232.
26. De Deus G, Murad CF, Reis CM, Gurgel-Filho E, Coutinho Filho T. Analysis of the sealing ability of different obturation tech-niques in oval-shaped canals: a study using a bacterial leakage model. Braz Oral Res. 2006;20(1):64-69.
27. Kierklo A, Tabor Z, Pawińska M, Jaworska M. A microcomputed tomography-based comparison of root canal filling quality fol-lowing different instrumentation and obturation techniques. Med Princ Pract. 2015;24(1):84-91.
28. Taşdemir T, Er K, Yildirim T, et al. Comparison of the seal-ing ability of three filling techniques in canals shaped with two different rotary systems: a bacterial leakage study. Oral
Author
perso
nal c
opy
Al-Afifi et al e313
© 2016 Wichtig Publishing
Surg Oral Med Oral Pathol Oral Radiol Endod. 2009;108(3): e129-e134.
29. Wolf M, Küpper K, Reimann S, Bourauel C, Frentzen M. 3D analyses of interface voids in root canals filled with different sealer materials in combination with warm gutta-percha tech-nique. Clin Oral Investig. 2014;18(1):155-161.
30. Shaheen N, Farag AM, Alhadainy HA, Darrag AM. Fracture resistance of endodontically treated roots using different preparation–obturation combinations. Tanta Dental Journal. 2013;10(2):97-102.
31. Chang J, Baek S-H, Lee I-B. Rheological characterization of thermoplasticized injectable gutta percha and resilon. Jour-nal of Korean Academy of Conservative Dentistry. 2011;36(5): 377-384.
32. Beer R, Baumann M, Kielbassa A. Filling the root canal. In: Pocket atlas of endodontics. 1st ed. New York: Thieme Medical. 2006;176-189.
33. Nielsen BA, Baumgartner JC. Spreader penetration dur-ing lateral compaction of resilon and gutta-percha. J Endod. 2006;32(1):52-54.
34. Gurgel-Filho ED, Feitosa JP, Gomes BP, Ferraz CC, Souza-Filho FJ, Teixeira FB. Assessment of different gutta-percha brands during the filling of simulated lateral canals. Int Endod J. 2006;39(2): 113-118.
35. Ghorpade RR., Aglawe PS, Phakatkar HG. Experimental and FEA based modal analysis of scaled up dental pin (plugger): a case study in endodontics. International Journal of Research in Advent Technology. 2013;1(5):270-280.
36. Garg N, Kapoor R. Obturation of root canal system. In: Garg N, Garg A, eds. Textbook of endodontics. 2nd ed. New Delhi: Jaypee Brothers Medical. 2010;265-300.
37. Silva LAB, Barnett F, Pumarola-Suñé J, Cañadas PS, Nelson-Filho P, Silva RA. Sealapex Xpress and RealSeal XT feature tissue com-patibility in vivo. J Endod. 2014;40(9):1424-1428.
Author
perso
nal c
opy