1. 2 3 myopia short sightedness myopia is a greek word meaning *close the eye* refractive error i...
TRANSCRIPT

1

2

3
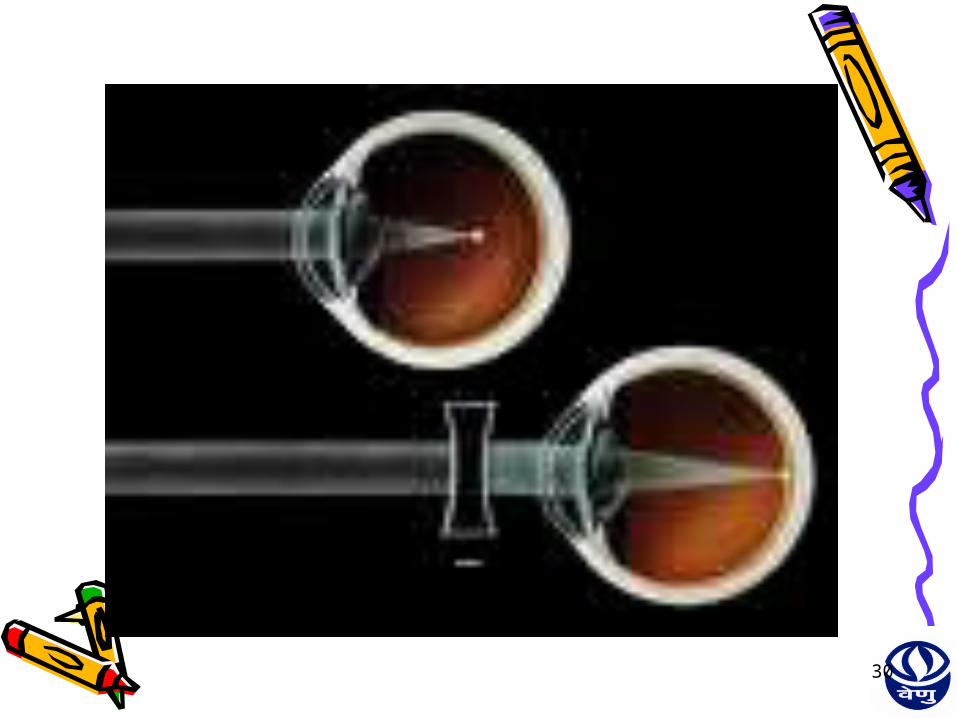
MYOPIA• Short sightedness• Myopia is a greek word meaning *close the eye*• Refractive error I• Parallel rays of light coming from infinity are
focused in front of the retina.• Accommodation is at rest
4
Mechanism of production
• Axial • Curvatural • Positional • Index • Myopia due to excessive accommodation
5
Optics of myopia • Far point is finite (In front of the eye) • Emmetropic eye it is at infinity• Higher the myopia the shorter the distance• Far point is 1mt from the eye ,there is 1D
of myopia• Nodal point is further away from retina
Accommodation need not develop normally resulting in Convergence insufficiencyExophoria
6
TYPES OF CLASSIFICATION
• Clinical Classification
• Degree of Myopia• Age of Onset

7
Clinical Classification• Congenital Myopia• Simple Myopia• Degenerative Myopia• Nocturnal Myopia• Pseudo Myopia• Induced Myopia
8
Degree of Myopia
• Low Myopia(<3D)• Medium
Myopia(3-6D)• High
Myopia(>6D)
9
AGE OF ONSET
• Congenital Myopia• Youth-Onset
Myopia(<20 yrs of age)
• Early Adult-Onset Myopia(20-40 yrs of age)
• Late Adult-Onset Myopia(>40 yrs of age)
10
Congenital myopia Frequently seen in Premature babies Marfan’s syndromeHomocystinuria Increase in axial length Increase inOverall globe sizeSince birth, diagnosed at age 2-3 years If unilateral, as anisometropia, may develop
amblyopia, strabismusUsually 8-10 D, remain constantBilateral- difficulty in distant vision, hold things
very close

11
Associated conditions Convergent squint CataractMicrophthalmosAniridiaMegalocorneaCongenital Separation of retinaManagement Early Correction is desirable Retinoscopy under full cycloplegia Early full correction desirable Poor prognosis
12
• Simple / developmental myopia
Physiological error not associated with any disease of the eye
Etiology :Normal biological variation in development
of eye Inheritence
13
Associated factors
Role of diet
Theory of excessive near work
14
Clinical picture
Rarely present at birth
Rather born hypermetropic, become myopic
Begins at 7-10 years, stabilizing around mid teens
Usually around 5D, never exceeds 8D
15
Symptoms
Poor vision for distanceAsthenopic symptoms develop due to
dissociation between accommodation and convergence
Convergence weakness, exophoria, suppression
Excessive accommodation inducing ciliary spasm and artificially increasing the amount of myopia
Psychological outlook

16
Signs
Large and prominentDeep ACLarge, sluggishly reacting pupilsNormal fundus, rarely crescentUsually doesn't exceed 6-8D
• Retinoscopy under full cycloplegia
17
• Pathological / degenerative / progressive myopia
Rapidly progressive associated with degenerative changes in the eye
EtiologyRapid axial growth of the eyeball outside
the normal biological variations of development
Role of heredityRole of general growth process
18
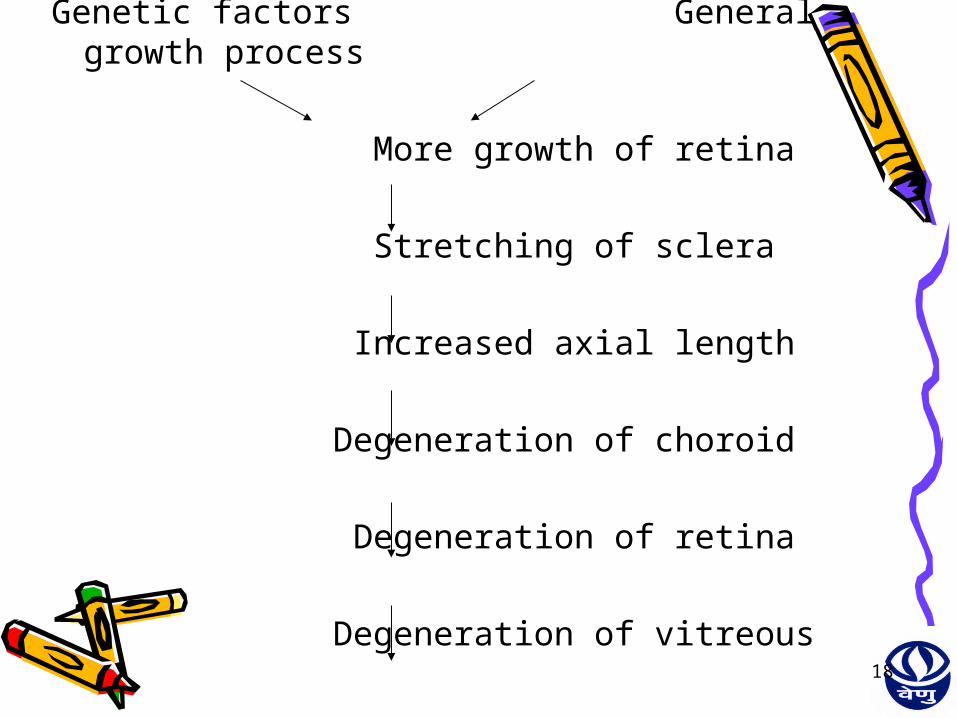
Genetic factors General growth process
More growth of retina
Stretching of sclera Increased axial length
Degeneration of choroid
Degeneration of retina
Degeneration of vitreous

19
Symptoms
Defective vision
Muscae volitantes / floating black opacities
20
Signs
EYE Large, prominent eyes simulating exophthalmos
CORNEA large ANTERIOR CHAMBER deep LENS show opacities at the posterior pole
due to aberration of lenticular metabolism and due to overstretching anterior dislocation may also occur

21
VITEROUS degeneration,viterous liquefication,vitreous detachment present as WEISS REFLEX
SCLERA thinning resulting in formation of STAPHYLOMA
VISUAL FIELD DEFECTS show Contraction and in some ring scotomas present
22
DISC Large in sizeMyopic Crescent on the temporal side of
the discChoroidal CrescentSupertraction of the retina Inverse myopia Myopic crescent situated
nasally and supertraction of the retina temporally
called as INVERSE CRESCENTPeripapillary Atrophy
23
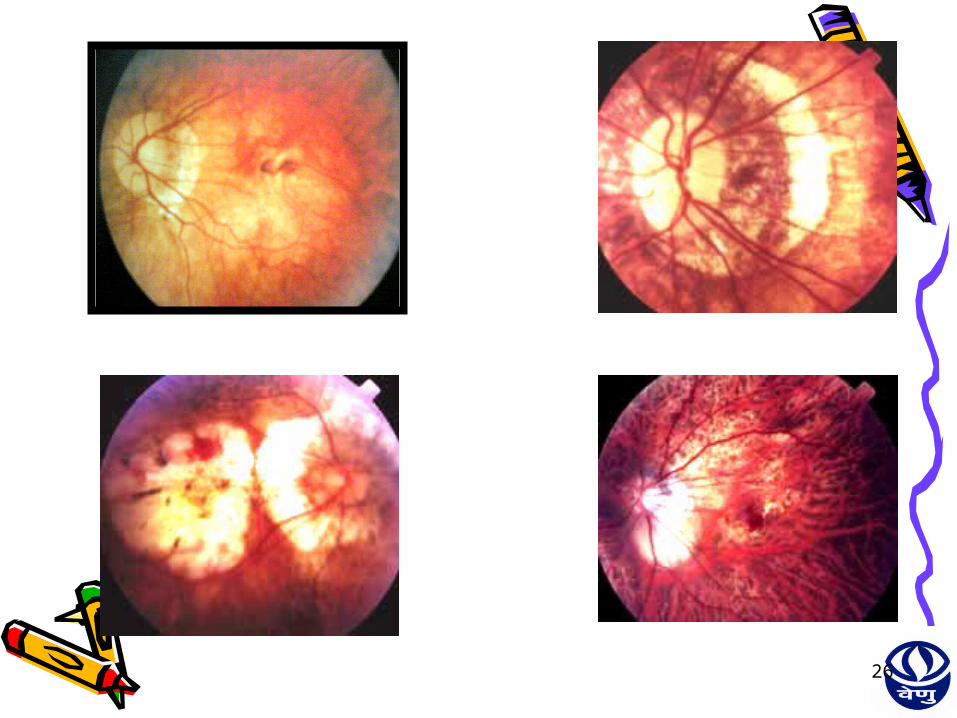
MACULA Foster-Fuchs fleck
RETINAL DETACHMENTPOSTERIOR STAPHYLOMARETINAL HOLES TESSELATED FUNDUS

24

25
26

27
Treatment Optical treatment
Appropriate concave lenses
Minimum acceptance providing maximum vision

28
Guidelines LOW DEGREES OF MYOPIA (Up to -
6D)
IN YOUNG SUBJECTS Defect should never be overcorrected and advised
for constant use to avoid squinting and develop a normal ACCOMMODATION-CONVERGENCE reflex
IN ADULTS Receiving spectacle for the first time,have the ciliary
muscle that are unaccostomed to accommodate efficiently so that lens of slightly lower power(1 or 2 D) may be prescribed for reading,especially if engaged in to any greater extent.Above the age of 40 years,when accommodation fails physiologically, a weaker glass for near work is essential

29
HIGH DEGREES OF MYOPIA
Full correction rarely be tolerated so we attempt to reduce the correction as little as is compatible with comfort for binocular vision. We prescribe the lens with which the greatest visual acuity is obtained without distress
30

31
ADVANTAGES OF SPECTACLESEconomicalAllow incorporation of prism,bifocals,pal
which can be used for the management of esophoria or any accommodative disorders accompanying myopia
Spectacles require less accommodation than contact lens for myopia that likelihood of accommodative asthenopia or near point blur in patients approaching presbyopia may be less
32
DISPENSING SPECTACLES IN HIGH MYOPIA
• High index lens materials• Lighter lens materials• Reduced eyesize of selected frames• Minus lenticular lens designs
33
ADVANTAGES OF CONTACT LENS
• Contact lens provides cosmosis
• Large retinal image size and slightly better visual acuity in severe myopia

34
SURGICAL TREATMENT
EpikeratophakiaRKPRK ISCRPhakic IOL’SLASIK
LASIKLASIKPRKPRK
RKRK
ISCRISCR
Phakic IOL’SPhakic IOL’S

35
Photorefractive Keratectomy
(PRK)• Involves direct laser ablation of corneal stroma
after removal of corneal epithelium mechanically or using a laser beam.
• Done using Excimer laser• MUNNERLYN EQN: depth of ablation
(micrometer)=[diameter of optical zone(mm)]² × 1/3power(Diopter)
• For myopic a large amount of ablation is done in central cornea than in the periphery.
• Give good results for -2D to -6D of myopia

36
LASIKLaser Assisted In situ
Keratomileusis• Method:Anterior flap of cornea is lifted with a keratome and
excimer laser is used to sculpt the stromal bed to change the refractive error of eye
• Corrects 0.5 to 12D of myopia and upto 8D of astigmatism• Guidelines:Age more than 18yrs BCVA better than 6/12 Stable refraction for last 1yr Absence of corneal disease & ectasia• Note:• (1) In no case the residual bed thickness after the ablation
should measure 250microns so as to avoid central corneal ectasia
• (2) Ideally the ablation should be done within 30sec of the preparation of flap

37
LASEKLaser subepithelial
Keratomileusis• Indications:• Low myopia• Irregular astigmatism• LASIK complications in contralateral eye• Thin corneal pachymetry• Predisposition to trauma• Glaucoma suspect
38
• Method:• Simple inexpensive procedure that
involves creation of epithelial flap after exposure to 18% alcohol for 25sec & subsequent replacement of flap after laser ablation

39
RKRadial Keratotomy
• It refers to making deep corneal incisions(initially 16,now down to 4) in the peripheral part of cornea leaving about 4mm central optical zone
• The incisions are made almost down to the level of Descemet’s Membrane
• These incisions on healing flatten the central cornea thereby reducing its refractive power
• For low to moderate degree of myopia(-1.5 to -6D of myopia)
40
Epikeratophakia• For high degree of myopia (upto 20D)• Method:• The epithelium is removed & then a
pocket is fashioned under the edge of the remaining epithelium & into this is inserted the cryolathed donor homograft
• Preserved material can also be used
41
NON CORNEAL INTERVENTIONS
• (A) REMOVAL OF CLEAR LENS• We know that an aphakic eye is strongly hypermetropic • If an eye with an axial myopia of -24D is deprived of its
lens it will become emmetropic without any correcting lens
• Note:• Whenever surgery on clear lens is contemplated the
eye is examined thoroughly for abnormalties like Raised IOP,Vitreous & retinal degeneration etc

42
• (b)Phakic intraocular lenses• An IOL of appropriate power is implanted
inside the eye without touching normal crystalline lens thus without disturbing accomodation
• Method can be used to correct both myopia & hypermetropia
• Phakic IOL types:• PC IOL• Angle supported IOL• Iris claw lens
43
INTRA CORNEAL RING(ICR) IMPLANTATION• ICR implantation into the peripheral
cornea approx.upto 2/3rd of stromal depth can also be considered for correction of myopia
• It results in a vaulting effect that flattens the central cornea decreasing the myopia
• The procedure has the advantage of being reversible

45
ThankThank youyouThankThank youyou