0 trust board agenda (public) 1 may 2019...
TRANSCRIPT

GROUP TRUST BOARD MEETING IN PUBLIC1
The next meeting of the group trust board will take place on Wednesday 1 May 2019 at 1.00pm in the boardroom, executive office, 2nd floor, Royal Free Hospital.
Dominic Dodd Chairman
A G E N D A
ITEM LEAD PAPERQUALITY IMPROVEMENT/CPG ITEM
2019/20-01 Palliative care presentation – Ms Sonia Anwar, NCA / NCOR lead and Dr Tamar Ish-horowicz, specialty registrar
Chief medical officer
Verbal
ADMINISTRATIVE ITEMS
2019/20-02 Apologies for absenceTo note apologies for absence – chief nurse
Chairman
2019/20-03 Declaration of interests To note the interests declared. If any member of the board has an interest in any item on the agenda, they must declare it at the meeting, and if necessary withdraw from the meeting
Chairman 1.
2019/20-04 Minutes of meeting held on 27 March 2019To approve the minutes of the last meeting
Chairman 2.
2019/20-05 Matters arising report To note updates on actions arising from previous meetings
Chairman 3.
2019/20-06 Record of items discussed at the confidentialboard meeting on 27 March 2019 To note the report
Chairman 4.
QUALITY, PATIENT SAFETY AND EXPERIENCE
2019/20-07 Patients’ voicesTo note the patients’ voices
Group chief executive
Verbal
2019/20-08 Go see visitsTo provide feedback on visits and note the report
Chief communications officer
5.
2019/20-09 Learning from deaths review reportTo note the report
Chief medical officer
6.
FINANCE AND PERFORMANCE
2019/20-10 Financial performance reportTo discuss the current financial performance of the trust
Chief finance and compliance officer
7.
1 In accordance with the Health & Social Care Act 2012, all Trust Board meetings must be held in public. All decisions which require the board’s collective approval can only be made at a Trust Board (or a Part II meeting held in closed session to discuss confidential matters).

ITEM LEAD PAPER2019/20-11 Operational performance report
To discuss the current operational performance of the trust
Hospital chief executive
8.
GOVERNANCE AND REGULATION: REPORTS FROM BOARD COMMITTEES – DISCUSSION BY EXCEPTION ONLY
2019/20-12 Chair’s and group chief executive’s report To note the report
Chairman/group chief executive
9.
2019/20-13 Audit committee report – 15 March 2019To receive the report from the committee
Committee chair 10.
2019/20-14 Clinical standards and innovation committee report – 10 April 2019 To receive the report from the committee
Committee chair 11.
2019/20-15 Group services and investment committee report – 11 April 2019 To receive the report from the committee
Committee chair 12.
2019/20-16 People committee report – 28 March 2019To receive the report from the committee
Committee chair 13.
2019/20-17 Use of trust seal To note the report
Chief finance and compliance officer
14.
OTHER BUSINESS 2019/20-18 Questions from the public Chairman
2019/20-19 Any other business Chairman
2019/20-20 Date of next meeting – 22 May 2019 Chairman

Page 1 of 1
REGISTER OF INTERESTS OF MEMBERS OF THE BOARD OF DIRECTORS
Executive summary
The trust constitution requires trust board members to declare interests which are relevant
and material to the NHS board of which they are a member. The register of interests is
presented at each board meeting.
The chief medical officer, and Doris Olulode and James Tugendhat, non-executive directors,
have updated their declarations.
Action required/recommendationBoard members are asked to provide an update if they have any changes in interests since the last meeting.
Board members are asked to declare any interests which are relevant to matters on the board agenda.
The board is asked to ratify the register, subject to any further changes made.
Meetings where this report has been discussed previously Not applicable
Board/GEC/LEC/committee goals
GOALS BAF
risks
1. Not applicable
CQC standards impacted Well led
Financial/business implications Not applicable
Equality analysis Not applicable
Compliance impact Compliance with NHS Improvement
(Monitor) code of governance and trust
constitution
Report from Dominic Dodd, chairman Author Alison Macdonald, board secretary
Report to Date of meeting Attachment number
Trust Board 1 May 2019 Paper 1
Paper 1

Version 31 Updated 24/4/19
Declaration of interests – board members are requested to highlight any changes to the register of interests at each board meeting held in public.
REGISTER OF THE INTERESTS OF MEMBERS OF THE TRUST BOARD
Board Member and position
Directorships, including non-executive directorships held in private companies or PLCs (with the exception of those of dormant companies)
Ownership or part-ownership of private companies, business or consultancies likely or possibly seeking to do business with the NHS
Majority or controlling share holdings in organisations likely or possibly seeking to do business with the NHS
A position of authority in a charity or voluntary organisation in the field of health and social care
Any connection with a voluntary or other organisation contracting for NHS services
Research funding/grants that may be received by an individual or their department
Interests in pooled funds that are under separate management (any relevant company included in this fund that has a potential relationship with the Trust must be declared)
Dominic Dodd, Chair
Director of UCLPartners
1
Member of NHSI’s Chairs’ Advisory Group. Unpaid position.
Nil Nil Trustee, The King’s Fund. Unpaid position
Nil Nil
Non-executive directors
Mary Basterfield Non-executive director 8/3/18
Flatberg Ltd (property management)
Chief finance officer, UKTV
Trustee, National Cancer Research Institute and UCL Union.
1 The Company’s constitutional documents have been drafted in accordance with charity law and Charity Commission guidance, so that the Company can apply for charitable status in the
future as and when its Board of Directors considers this appropriate.
Paper 1

Version 31 Updated 24/4/19
Declaration of interests – board members are requested to highlight any changes to the register of interests at each board meeting held in public.
Board Member and position
Directorships, including non-executive directorships held in private companies or PLCs (with the exception of those of dormant companies)
Ownership or part-ownership of private companies, business or consultancies likely or possibly seeking to do business with the NHS
Majority or controlling share holdings in organisations likely or possibly seeking to do business with the NHS
A position of authority in a charity or voluntary organisation in the field of health and social care
Any connection with a voluntary or other organisation contracting for NHS services
Research funding/grants that may be received by an individual or their department
Interests in pooled funds that are under separate management (any relevant company included in this fund that has a potential relationship with the Trust must be declared)
Wanda GoldwagNon-executive director
• Chair of the Office of Legal Complaints (OLC)
• Lay Member QC Appointments Panel
• Advisor SmedvigVenture Capital
• Interim chair, LEASE (Leasehold Advisory Service)
• Chair of independent Financial Services Consumer Panel (wef 1/3/19)
Director, Goldwag Consultancy Ltd
Nil Nil Adopted sister is chief pharmacist of Barnet Enfield and Haringey Mental Health Trust
Nil I have a shareholding via Smedvig Capital in Antidote Technologies Ltd the clinical trial matching platform
Chris Ham Non-execuvtive director
• Non-clinical chair, NHS Assembly
Visiting fellow, King’s Fund Advisor to Carnall Farrar
Doris Olulode Non-executive director
Non-Executive Director, Chartered Institute of Legal Executives (CILEx)Non-Executive Director, Diocese of Chelmsford Multi Academy Trust Lay member, employment tribunal
HR consultancy with South London and the Maudsley NHS Foundation Trust
Paper 1

Version 31 Updated 24/4/19
Declaration of interests – board members are requested to highlight any changes to the register of interests at each board meeting held in public.
Board Member and position
Directorships, including non-executive directorships held in private companies or PLCs (with the exception of those of dormant companies)
Ownership or part-ownership of private companies, business or consultancies likely or possibly seeking to do business with the NHS
Majority or controlling share holdings in organisations likely or possibly seeking to do business with the NHS
A position of authority in a charity or voluntary organisation in the field of health and social care
Any connection with a voluntary or other organisation contracting for NHS services
Research funding/grants that may be received by an individual or their department
Interests in pooled funds that are under separate management (any relevant company included in this fund that has a potential relationship with the Trust must be declared)
Akta Raja Non-executive director
• Director RFL Property Services Company Ltd
• Enhabit Ltd • Passisah Ltd
(dormant) • Geneff Ltd • Thornriver
Management Ltd • Jewelglen Ltd • Ansor Ltd (not
trading) • Amalgamated
Laboratory Solutions Ltd (not trading)
• Selwyn Peters Ltd (not trading)
• Member of PSM Partners LLP
Nil Nil Nil Nil Nil Nil
Paper 1

Version 31 Updated 24/4/19
Declaration of interests – board members are requested to highlight any changes to the register of interests at each board meeting held in public.
Board Member and position
Directorships, including non-executive directorships held in private companies or PLCs (with the exception of those of dormant companies)
Ownership or part-ownership of private companies, business or consultancies likely or possibly seeking to do business with the NHS
Majority or controlling share holdings in organisations likely or possibly seeking to do business with the NHS
A position of authority in a charity or voluntary organisation in the field of health and social care
Any connection with a voluntary or other organisation contracting for NHS services
Research funding/grants that may be received by an individual or their department
Interests in pooled funds that are under separate management (any relevant company included in this fund that has a potential relationship with the Trust must be declared)
Professor Anthony Schapira Non-executive director
Upper Hampstead Walk Residents’ Association. AHV Schapira Ltd
Non-executive director, Ministry of Justice
Nil Nil Parkinson’s Disease Society Research Strategy Group
Nil Medical Research Council, Wellcome Trust, Parkinson’s Disease Society and other charitable sources of research funding
Nil
James TugendhatNon-executive director
Director and managing director, UK, Europe and International Companies: BHFS ONE LIMITED and all its registered subsidiaries BHFS TWO LIMITED
Nil Nil Nil Nil Nil Nil
Paper 1

Version 31 Updated 24/4/19
Declaration of interests – board members are requested to highlight any changes to the register of interests at each board meeting held in public.
Executive directors
Board Member and position
Directorships, including non-executive directorships held in private companies or PLCs (with the exception of those of dormant companies)
Ownership or part-ownership of private companies, business or consultancies likely or possibly seeking to do business with the NHS
Majority or controlling share holdings in organisations likely or possibly seeking to do business with the NHS
A position of authority in a charity or voluntary organisation in the field of health and social care
Any connection with a voluntary or other organisation contracting for NHS services
Research funding/grants that may be received by an individual or their department
Interests in pooled funds that are under separate management (any relevant company included in this fund that has a potential relationship with the Trust must be declared)
Caroline Clarke Group chief executive
Director RFL Property Services Company
Nil Nil Director
Royal Free Charity (1/4/16)
Trustee, Overcoming MS
Trustee, Healthcare Finance Managers Association
Nil Nil
Peter Ridley
Chief finance and
compliance
officer
Director Royal
Free Dispensing
Ltd
Nil Nil Nil Nil Nil Nil
Deborah Sanders Chief nurse
Nil Nil Nil Board member, The Royal Free Hospital Nurses’ Home of Rest Trust
Trustee, Royal Hospital for Neuro-disability
Nil Nil Nil
Kate Slemeck, RFH chief executive
Nil Nil Nil Chair of NHS Elect Advisory Committee Chair of NHS Providers COO Network
Husband works for Canon who provide the trust’s managed print service.
Nil Nil
Paper 1
Version 31 Updated 24/4/19
Declaration of interests – board members are requested to highlight any changes to the register of interests at each board meeting held in public.
Board Member and position
Directorships, including non-executive directorships held in private companies or PLCs (with the exception of those of dormant companies)
State when directorship commenced
Ownership or part-ownership of private companies, business or consultancies likely or possibly seeking to do business with the NHS State when interest acquired
Majority or controlling share holdings in organisations likely or possibly seeking to do business with the NHS State when interest acquired
A position of authority in a charity or voluntary organisation in the field of health and social care
State when position accepted
Any connection with a voluntary or other organisation contracting for NHS services
State when position accepted
Research funding/grants that may be received by an individual or their department
State when funding/grant commenced
Interests in pooled funds that are under separate management (any relevant company included in this fund that has a potential relationship with the Trust must be declared)
State when interest acquired
Chris Streather
Chief medical
officer
Director, RFC
Developments Ltd
Director HSL Ltd
Nil Nil Trustee of
Healthcare
Management
Trust (HMT) a
not for profit
organisation
which provides
care home
facilities and
healthcare in
Lincolnshire and
Swansea.
Unpaid advice to
ZPB on e-
rostering which
will contribute to
a report
commissioned
from them by
Allocate. It
involved two
meetings and
reviewing a
document and
Health Education
England (HEE)
also were
involved. The
trust has a
contract with
Allocate, but not
ZPB, for whom
this work was
done.
Nil Nil
Paper 1

Version 31 Updated 24/4/19
Declaration of interests – board members are requested to highlight any changes to the register of interests at each board meeting held in public.
Board Member and position
Directorships, including non-executive directorships held in private companies or PLCs (with the exception of those of dormant companies)
Ownership or part-ownership of private companies, business or consultancies likely or possibly seeking to do business with the NHS
Majority or controlling share holdings in organisations likely or possibly seeking to do business with the NHS
A position of authority in a charity or voluntary organisation in the field of health and social care
Any connection with a voluntary or other organisation contracting for NHS services
Research funding/grants that may be received by an individual or their department
Interests in pooled funds that are under separate management (any relevant company included in this fund that has a potential relationship with the Trust must be declared)
Non-voting directors
David Grantham
Chief people
officer
Nil Nil Nil Board Member
and Treasurer
London
Healthcare
People
Management
Academy –
March 2013
Chair of NHS
Employers
Medical
Workforce
Forum – August
2010
Board Member Health Education North and East London (HENCEL) – July 2014 Board Member and Treasurer London Streamlining Programme(s) – March 2014
Nil Nil
Emma Kearney
Chief
communications
officer
Director, EK
Consulting Ltd
Nil Nil Nil Nil Nil Nil
Steve Shaw
Chief executive
BH
Nil
Paper 1

Paper 2
1
MINUTES OF THE TRUST BOARD
HELD ON 27 MARCH 2019
Present
Mr D Dodd Ms M Basterfield Ms C Clarke Ms W Goldwag Ms D Olulode Ms A Raja Mr P Ridley Ms D Sanders Ms K Slemeck Mr J Tugendhat
Chairman Non-executive director Group chief executive Non-executive director Non-executive director Non-executive director Chief finance and compliance officer Chief nurse Chief executive, Royal Free Hospital Non-executive director
Invited to attend
Mrs J Dewinter Mr D Grantham Ms E Kearney Ms E McManus Dr S Shaw Miss A Macdonald
Lead governor Chief people officer Chief communications officer Chief transformation officer Chief executive, Barnet Hospital Board secretary (minutes)
Others in attendance
Noelle Skivington Enfield Healthwatch
2018/19-210 QUALITY IMPROVEMENT/CPG ITEM – POINT OF CARE FOUNDATION WORKSHOP?
Action
The chief nurse provided some initial reflections from a workshop facilitated by the Point of Care Foundation which had preceded the formal board meeting. She noted that this had been an important first step in developing thinking about how the trust could really involve patients and users in service development and delivery. There were great examples in the clinical practice group (CPG) work; the issue was how to do this even more effectively and more widely.
Ms Olulode, non-executive director, agreed that it had been a useful session providing a different perspective and raising the question of how the input could be maximised from a range of audiences. She suggested it was important to have a baseline of where patient and user involvement was already taking place.
Ms Goldwag, non-executive director, agreed that patient participation was vital but suggested that it would have been useful to have more time for discussion and debate rather than receiving a presentation.
Ms Basterfield, non-executive director, suggested that there needed to be clarity about the risk appetite for the potential impact of patient empowerment and clinicians would need to be empowered to course correct if there were problems.

Paper 2
2
Ms Raja, non-executive director, said that it would be interesting to know what other trusts were doing on this.
The chief executive, Royal Free Hospital, suggested that there was an issue about how to scale up the CPG programme and making it easier for people to incorporate patient involvement in their work.
Mrs Dewinter, lead governor, said that there was a danger that patient involvement could become tokenistic and that it would be helpful to be clear at every meeting or forum about how patient involvement was being incorporated and what outcome was being sought.
Ms Goldwag, non-executive director, suggested that the trust needed to develop public engagement, particularly if there was the prospect of difficult decisions needing to be taken.
The group chief executive commented that public engagement was one of her key priorities and she would take this forward with the chief communications officer.
Ms Basterfield suggested that in the CPG/QI presentations, presenters could be asked to include information about patient involvement in the course of the project rather than surveys and feedback about the end of it.
Mr Tugendhat, non-executive director, commented that although there was good evidence about the benefits of patients’ involvement in terms of satisfaction and outcomes, there was less of an evidence base for involvement in governance and policy, but this was not to say that this should not be pursued.
Summarising the discussion the chairman noted that the aspiration was to have shared decision making. It was easy for NHS professionals to make assumptions about patients’ views and preferences and it was important in the future to avoid this. Codesign was well developed in CPGs as was patient feedback. This was a good model, which needed to be scaled up. Shared decision making was also needed in the fields of governance and policy making.
2018/19-211 APOLOGIES FOR ABSENCE AND WELCOME
Apologies for absence were received from:
Prof Sir Chris Ham Non-executive director Prof A Schapira Non-executive director Dr C Streather Chief medical officer
The chairman congratulated Dr Chris Streather and Ms Deborah Sanders for their appointment as joint deputy group chief executives, which sent a strong message about the Royal Free group as a clinically led organisation.
2018/19-212 DECLARATION OF INTERESTS
The chairman reminded board members to always have in mind whether they had any actual or potential conflict of interest, particularly if they had a change in circumstances.
There were no changes advised and the report on the register of interests was noted.
Paper 2
3
2018/19-213 MINUTES OF MEETING HELD ON 27 FEBRUARY 2019
The minutes were accepted as an accurate record of the meeting, subject to the following amendment:
2018/19 -207 Questions from the public
Add following as first paragraph of this minute.
The chairman reported that a member of the public had raised a question about the timeliness of the publication of trust board papers on the website. This would be responded to in detail outside the meeting, but it remained the aim to publish papers in a timelier manner
2018/19-214 MATTERS ARISING REPORT
The report was noted.
2018/19-215 RECORD OF ITEMS DISCUSSED AT PART II BOARD MEETING ON 28 NOVEMBER 2018
The report was noted.
2018/19-216 PATIENTS’ VOICES
The chief nurse read out a complaint and compliment from the NHS Choices website, both relating to Chase Farm Hospital
The first related to computer errors which affected the patient’s attendance for appointments. The patient complained that their appointments had been cancelled without notifications and their appointment was deferred by six months. The patient had spent a long time on the telephone trying to sort the matter out. The staff said the problems had been caused by computer errors which the patient did not find reassuring, who also wondered what would happen for patients with a language barrier or who could not communicate their needs well. The patient also commented on the unhealthy foods in the coffee shop.
The compliment was from the parent of a four year old patient at the ear, nose throat department at Chase Farm. They were greeted at the main door on arrival by a friendly staff member who directed them appropriately. On arrival at the children's outpatient waiting area help was on hand to check in using the machines, while there were toys and games for the children. There was little delay and the little boy was seen, assessed and provided with treatment quickly. Staff were kind and patient
The chief executive of Barnet Hospital would present the patients’ stories item next time.
Chief executive, Barnet Hospital
2018/19-217 GO SEE VISITS
The chief communications officer highlighted that new areas had been added to the programme, including areas put forward by members of staff and suggested by the hospital chief executives.
Paper 2
4
The chief people officer reported on his return visit to Olive and Palm wards at Barnet Hospital. Staff welcomed having a second visit as this could be used for feedback and to highlight developments since the last visit. He had fed back on the results of the staff survey. The staff raised recruitment and talked about retention. One of the sisters was relatively new in post and referred to the supportive environment and peer support from other sisters. He had also seen the frailty pathway in action and the emphasis on keeping patients mobile. Junior doctors had been positive about the new electronic patient record. The group chief executive reported on a recent visit to the operating theatres at the Royal Free Hospital.
The board noted the report.
2018/19-218 NATIONAL STAFF SURVEY
The chief people officer highlighted that progress had been made in three areas: the quality of appraisals, relationship with immediate manager and a safe environment. No area had significantly deteriorated but the areas for focus continued to be equality and diversity, staff health and wellbeing and bullying and harassment. He drew the board’s attention to the benchmarking of RFL against other large London trusts and a wider peer group and noted that RFL had one of the lowest rates of bullying and harassment in London – albeit still too high. He also noted that there were signs of improvement on equality. This suggested that the trust was doing the right things but the pace needed to be increased if possible.
Ms Basterfield, non-executive director, noted the low response rate and asked what further the steps the trust could take to address this. The chief people officer responded that paper surveys had been sent out in an attempt to increase the response rate but this had not been successful. He added that the survey had come out at a time when staff were very busy with other priorities. The chief nurse noted that staff still worried that their responses were not confidential, and communication and reassurance was needed on this point. The trust also needed to respond quickly to issues raised in the survey and demonstrate the action being taken. Mr Tugendhat, non-executive director, commented that the low response rate was indicative of the level of staff engagement.
It was noted that the people committee would be having a detailed discussion of the staff survey and would form a view of what further action needed to be taken.
The board noted the report.
2018/19-219 GENDER PAY GAP
The chief people officer noted that there had been a slight reduction in the gender pay gap from 17.68% in 2017 to 15.98% in 2018; some of this was due to better data definitions. The medical workforce remained the area of greatest concern, which was related to structural issues in the consultant workforce and clinical excellence awards (CEAs). This was being addressed in the new CEA process. Ms Goldwag, non-executive director, suggested that it would be helpful to have an aspiration or target to measure progress against over time. The chief finance and compliance officer asked whether it would be helpful to separate out the staff groups as the issues might be different. Mr Tugendhat, non-executive

Paper 2
5
director, said that the people committee would take all the comments and suggestions forward. Interventions could include practical things like staff nurseries and flexible working. This would also need to be done in the context of the people strategy.
The board noted the report.
2018/19-220 FINANCIAL PERFORMANCE REPORT
The chief finance and compliance officer presented this report, noting that there were the same themes as in previous months. As in previous months, the adverse variance predominantly related to the impact of phasing of the financial improvement plan (FIP) income target in equal twelfths in the financial plan whilst delivery was expected in Q4. He noted that the trust was still forecasting that it would miss the 2018/19 financial plan by £1.6m which was the shortfall between the Department of Health funding for the Agenda for Change pay uplift and the actual estimated cost to the trust. The financial improvement plan (FIP) plan of £45m would be delivered, but not enough of the savings were recurrent which increased the pressure going into 2019/20.
The board noted the current financial position of the trust.
2018/19-221 OPERATIONAL PERFORMANCE REPORT
The chief executive of the Royal Free Hospital reported that the cancer target remained challenged and there would be at least 2-3 months before the trust returned to compliance. The current backlog was 103 patients, which was a reduction on the previous month but needed to go lower than this. Because of the high volume of cases, good performance was needed in breast, skin and prostate in order to improve the overall trust position. The cancer clinical practice group (CPG) work would start in April and this should have an impact.
In terms of the referral to treatment time (RTT) target, the major focus was on reducing the number of patients waiting more than 52 weeks and to get as close as possible to zero (excluding ‘pop-ons’) by the end of April. The main challenges were in orthopaedics at Barnet Hospital and plastic surgery at the Royal Free Hospital.
Ms Goldwag, non-executive director, asked whether it would be possible to give patients the option of going to another hospital with a shorter waiting time so they could be treated more quickly. The chief executive of the Royal Free Hospital responded that patients were often reluctant to be treated by a different consultant in the same hospital, let along going to a different hospital and other hospitals were also challenged. However she undertook to pursue this idea further.
She then reported that A&E performance in February had been 83% at trust level but with variation between the sites during the course of the month. The chief executive of Barnet Hospital added that performance at the Royal Free Hospital had improved but Barnet Hospital was challenged. Discussions were currently taking place with Barnet clinical commissioning group about creating an urgent treatment centre adjacent to the Barnet A&E department.
The board noted the current operational performance of the trust.
Chief executive, Royal Free Hospital
Paper 2
6
2018/19-222 CHAIR’S AND CHIEF EXECUTIVE’S REPORT
The group chief executive drew the board’s attention to the section of the report dealing with the Data Security and Protection Toolkit (DSPT) which replaced the information governance (IG) toolkit, and General Data Protection Regulation (GDPR) which was the successor to the Data Protection Act. The group executive committee had received a detailed briefing and training on this and were assured that the trust was meeting the requirements of both regimes.
The board noted the report.
2018/19-223 AUDIT COMMITTEE REPORT – 15 MARCH 2019
The committee chair reported that the committee had received a progress update from the external auditor and the draft head of internal audit opinion which was significant assurance with minor improvements required. The committee had also received a report on the data quality dashboard.
The board noted the report from the committee.
2018/19-224 CLINICAL STANDARDS AND INNOVATION COMMITTEE – 13 MARCH 2019
The board noted the report from the committee.
2018/19-225 GROUP SERVICES AND INVESTMENT COMMITTEE REPORT – 14 MARCH2019
The board noted the report from the committee.
2018/19-226 QUESTIONS FROM THE PUBLIC
Ms Skivington, Enfield Healthwatch, had been pleased to hear about the Point of Care Foundation workshop. She then asked when the new decontamination service would open in Enfield and what communications would take place locally. The response was that the new service would open in the summer and the chief communications officer would share the communications plan with her.
Chief comms officer
2018/19-227 ANY OTHER BUSINESS
There was no other business.
2018/19-228 DATE OF NEXT MEETING
The next trust board meeting would be on 1 May 2019 at 1300 in the boardroom, 2nd floor, Royal Free Hospital.
Agreed as a correct record
Signature …………………………………..date 1 May 2019……………………………. Dominic Dodd, chairman

Paper 3
Page 1 of 2
TRUST BOARD – PUBLIC
ACTION TRACKER AS AT 1 MAY 2019
Ref Open actions – as at 1 May 2019
(Completed actions will remain on the open actions log in a shaded box for reporting at the next meeting and will then be moved to the
closed actions log)
Action Date Target Owner Status
Operational performance report
2018/19-
221
Ms Goldwag, non-executive director, asked whether it would be possible to give
patients the option of going to another hospital with a shorter waiting time so they could
be treated more quickly. The chief executive of the Royal Free Hospital responded that
patients were often reluctant to be treated by a different consultant in the same hospital,
let alone going to a different hospital and other hospitals were also challenged.
However she undertook to pursue this idea further
27/3/19 1/5/19 Chief
executive,
RFH
Open
2018-
19/197
Director of infection prevention and control quarterly report
The group chief executive suggested undertaking a review to try and establish the
reasons for the low take up of the flu vaccine and it was agreed that this would be
included in the July DIPC report.
23/1/19 July
2019
Chief
nurse
Open
2018-
19/203
Well led review action plan
The group chief executive suggested assigning recommendations and actions to the committees, which would monitor progress and report to the board by exception, with a close out report to the board in April 2019. April 2019 update – recommendations have been assigned to committees and actions are being updated with a review to the group executive committee in May 2019. Close out report will be submitted to May board meeting.
23/1/19 22
May
2019
Chief
trans-
formation
officer
Open

Paper 3
Page 2 of 2
Completed actions – as at 1 May 2019
(Completed actions will remain on the open actions log in a shaded box for reporting at the next meeting and will then be moved to the
closed actions log)
2018-
19/165
RFL therapies – smoking cessation project
It was agreed that the people and population health committee would discuss smoking
cessation from both the patient and staff perspective.
May update – was discussed at March meeting.
28/11/18 March
2019
Group
deputy
CEO
Closed

Paper 4
Page 1 of 2
ITEMS DISCUSSED AT THE CONFIDENTIAL BOARD MEETING HELD ON 27 MARCH
2019
Executive summary
Decisions taken at a confidential trust board are reported where appropriate at the next trust
board held in public. Those issues of note and decisions taken at the trust board’s
confidential meeting held on 27 March 2019 are outlined below. The board discussed the
trust’s financial position and performance report, although a detailed discussion also took
place within the public part of the meeting. The following matters were also discussed at the
meeting:
• Referral to treatment time (RTT) update – the trust is currently dealing with data quality issues which are impacting on management of waiting lists and ability to meet the waiting time standards. This is reported to the board every month in the public operational performance report. The board approved the recommendation to pause reporting these figures because of these issues. This is a temporary measure and the trust will begin reporting again when the issue has been resolved. The trust is implementing new, robust methods for measuring RTT data to prevent this happening again. The pause in reporting will not affect waiting times for patients who will be treated according to clinical need and those waiting longest will be seen first.
• Annual plan 2019/20 – the final draft of the annual plan which combined the financial and operational plan was presented and approved by the board. It has been submitted to NHS Improvement from whom feedback is awaited. When the annual plan has been finalised a summary version will be published on the trust’s website.
• EU exit operational readiness: the board received an update on preparations being made by RFL to manage the potential impacts that will be caused by the UK leaving the EU in the event of no deal – this covers medicines and vaccines, medical devices and clinical consumables, non clinical consumables and services, workforce, blood and transplant, data, reciprocal health care and clinical trials. The board was assured that robust arrangements were in place.
• Queen Mary’s House – the board received a verbal update. This issue remains confidential for commercial reasons.
• The board received an update on the Information Commissioner’s Office (ICO) decision notice and the trust’s action plan in response.
Action required
For the board to note.
Meetings where this report has been discussed previously Not applicableMeeting Date Decision
Report to Date of meeting Attachment number
Trust Board 1 May 2019 Paper 4

Paper 4
Page 2 of 2
Board/GEC/LEC/committee goals
GOALS BAF
risks
1. RTT 18 weeks target: 92% G-036
2. Be a digital exemplar(HIMSS level 7) G-040
3. Deliver regulatory undertakings G-021
4. Demonstrable organisation health group governance) G- 42
CQC standards impacted Well led
Financial/business implications Financial/business implications are
articulated where relevant in reports under
consideration by the board.
Equality analysis Equality and diversity implications are
articulated where relevant in reports under
consideration by the board.
Compliance impact Any compliance impacts are articulated
where relevant in reports under consideration
by the board.
Report from D Dodd, chairman Author A Macdonald, board secretary
Paper 5
Page 1 of 5
GO SEE VISITS
Executive summary
This report provides an update on the go see visits programme, which was established in
December 2017. Go See visits continue to be advertised internally and areas which have
been nominated by staff have been incorporated in the programme.
The attached report provides updates on:
• Visits which have taken place since the last board meeting
• Forthcoming visits which have been confirmed
• Forthcoming visits awaiting confirmation
Action required/recommendation The board is asked to note the report.
Meetings where this report has been discussed previously Meeting Date Decision Not applicable
Board goals
GOALS BAF risks
1. Quality Improvement (QI) embedded as our method of transformation
G-031
CQC standards impacted Safe / effective / caring / responsive / well led
Financial/business implications Not applicable
Equality analysis Not applicable
Compliance impact Not applicable
Report from Emma Kearney, chief communications officer
Author Sue Little, executive support manager and Alison Macdonald, board
secretary
Report to Date of meeting Attachment number
Trust Board 1 May 2019 Paper 5
Paper 5
Page 2 of 5
1. Introduction
The board has an established programme of go see visits, which are open to all group
directors, along with site chief executives, non-executive directors and governors. Prior to the
visits, a fact sheet is provided giving some key information about the areas. This includes
information on staffing and where appropriate, patient or client feedback. Visits are not
designed to be inspections, but opportunities to listen to staff and, where appropriate, meet
patients. Non-executives are paired with governors: once the date for a visit is confirmed
governors are invited to attend and the aim is that the same governor accompanies the non-
executive director for the second visit. Feedback is provided both to the area visited and to
the board at each board meeting. Visits are also reported at council of governors meetings.
Since the establishment of the programme in December 2017, more than 100 visits have
taken place, initially to the 40 areas in the original programme which has now been
extended with 70 new areas. The programme covers the three main hospital sites including
support service areas such as porters, domestics and catering and group shared services
and RFL wholly owned subsidiaries. Areas where there are new quality improvement (QI)
projects have also been incorporated. The aim is that all main areas will have been visited
within the next year.
In addition to these go see visits, the new group chief executive is carrying out visits across
all the sites where the trust has services; these are also listed below.
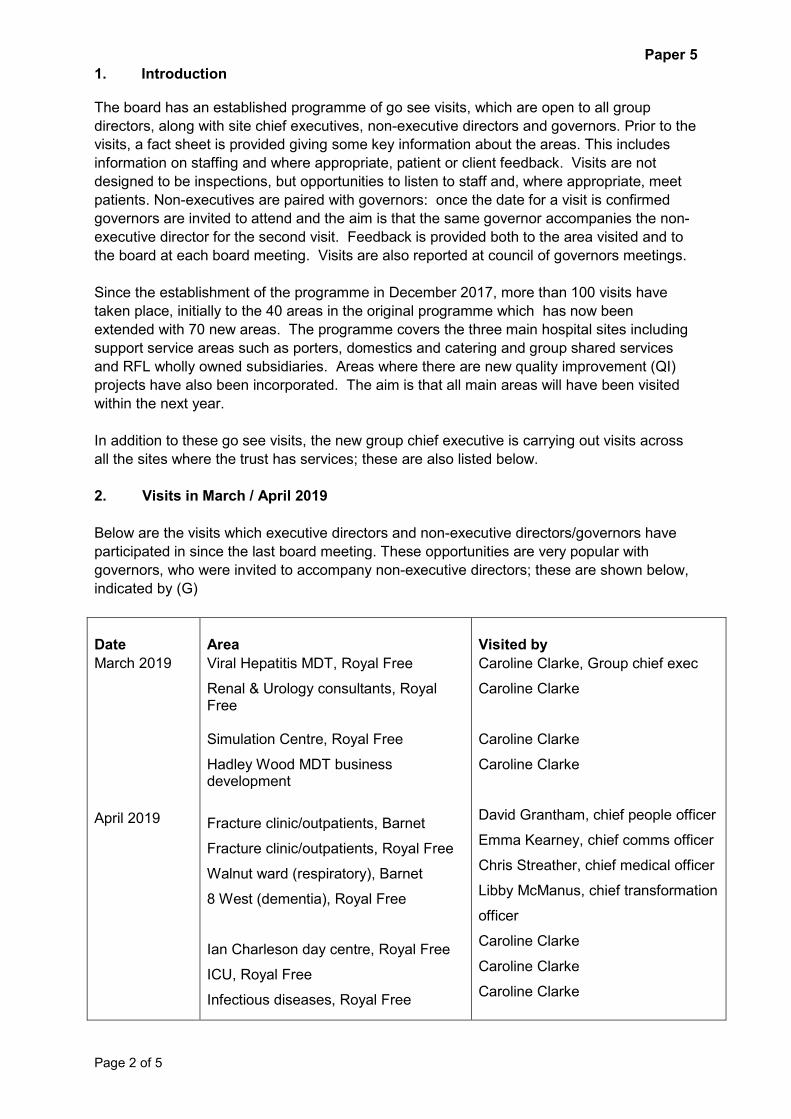
2. Visits in March / April 2019
Below are the visits which executive directors and non-executive directors/governors have
participated in since the last board meeting. These opportunities are very popular with
governors, who were invited to accompany non-executive directors; these are shown below,
indicated by (G)
Date
March 2019
April 2019
Area
Viral Hepatitis MDT, Royal Free
Renal & Urology consultants, Royal Free
Simulation Centre, Royal Free
Hadley Wood MDT business development
Fracture clinic/outpatients, Barnet
Fracture clinic/outpatients, Royal Free
Walnut ward (respiratory), Barnet
8 West (dementia), Royal Free
Ian Charleson day centre, Royal Free
ICU, Royal Free
Infectious diseases, Royal Free
Visited by
Caroline Clarke, Group chief exec
Caroline Clarke
Caroline Clarke
Caroline Clarke
David Grantham, chief people officer
Emma Kearney, chief comms officer
Chris Streather, chief medical officer
Libby McManus, chief transformation
officer
Caroline Clarke
Caroline Clarke
Caroline Clarke
Paper 5
Page 3 of 5
Royal Free Radio, Chase Farm
The Grove building, Royal Free (patient
safety & risk, clinical governance,
performance, group clinical services)
The Grove building, Royal Free
(communications, R&D, workforce)
Urgent care centre, Chase Farm
Enfield Civic Centre, elective access
directorate
Emergency department, Barnet
10 East (renal/acute kidney injury),
Royal Free
10 West (cardiology), Royal Free
7 West (vascular), Royal Free
Caroline Clarke
James Tugendhat, NED, & Judy
Dewinter (G)
Chris Ham, NED, & Ian Bretman (G)
Wanda Goldwag, NED
Chris Ham & Frances Blunden (G)
Mary Basterfield, NED, & Richard
Stock (G)
Doris Olulode, NED, & Anthony
Isaacs (G)
Chris Ham
Chris Ham
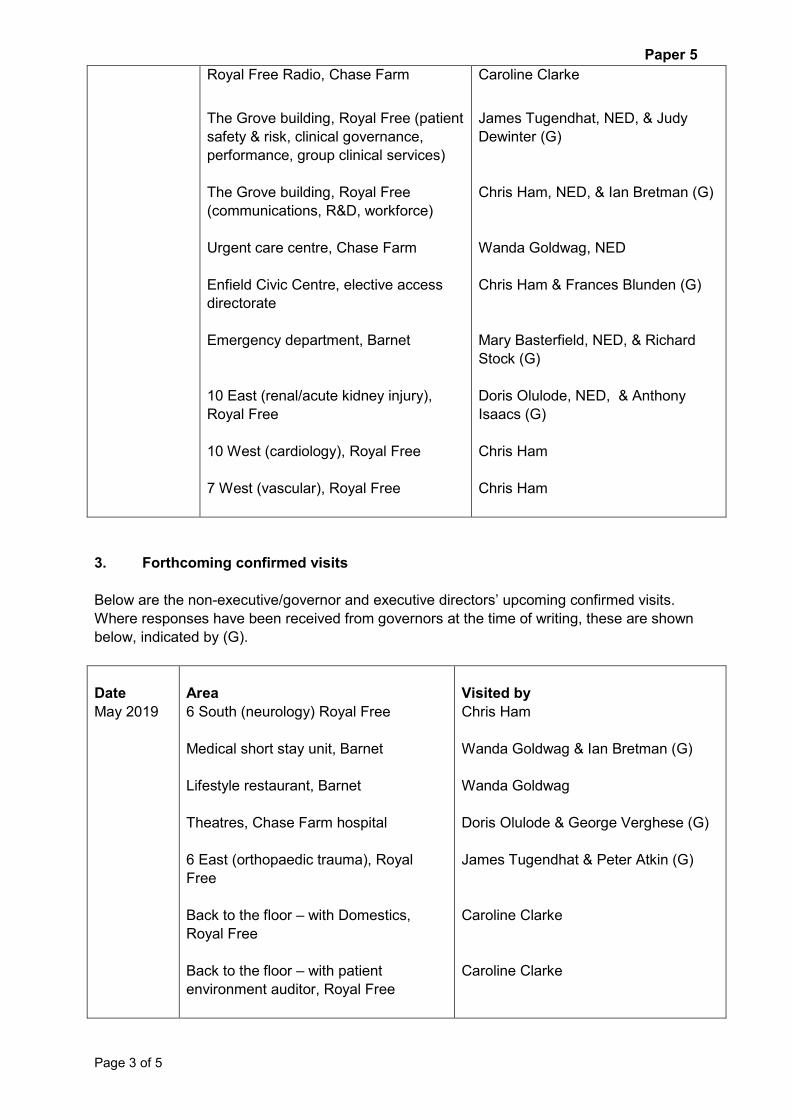
3. Forthcoming confirmed visits
Below are the non-executive/governor and executive directors’ upcoming confirmed visits.
Where responses have been received from governors at the time of writing, these are shown
below, indicated by (G).
Date
May 2019
Area
6 South (neurology) Royal Free
Medical short stay unit, Barnet
Lifestyle restaurant, Barnet
Theatres, Chase Farm hospital
6 East (orthopaedic trauma), Royal
Free
Back to the floor – with Domestics,
Royal Free
Back to the floor – with patient
environment auditor, Royal Free
Visited by
Chris Ham
Wanda Goldwag & Ian Bretman (G)
Wanda Goldwag
Doris Olulode & George Verghese (G)
James Tugendhat & Peter Atkin (G)
Caroline Clarke
Caroline Clarke
Paper 5
Page 4 of 5
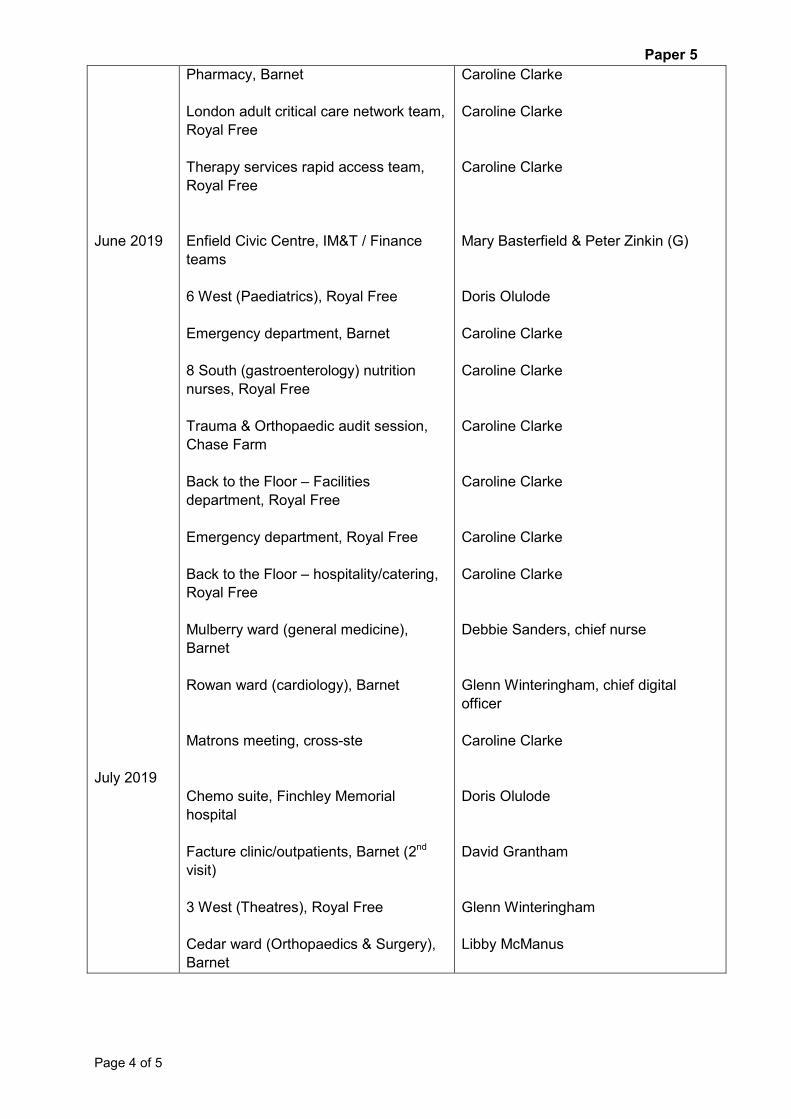
June 2019
July 2019
Pharmacy, Barnet
London adult critical care network team,
Royal Free
Therapy services rapid access team,
Royal Free
Enfield Civic Centre, IM&T / Finance
teams
6 West (Paediatrics), Royal Free
Emergency department, Barnet
8 South (gastroenterology) nutrition
nurses, Royal Free
Trauma & Orthopaedic audit session,
Chase Farm
Back to the Floor – Facilities
department, Royal Free
Emergency department, Royal Free
Back to the Floor – hospitality/catering,
Royal Free
Mulberry ward (general medicine),
Barnet
Rowan ward (cardiology), Barnet
Matrons meeting, cross-ste
Chemo suite, Finchley Memorial
hospital
Facture clinic/outpatients, Barnet (2nd
visit)
3 West (Theatres), Royal Free
Cedar ward (Orthopaedics & Surgery),
Barnet
Caroline Clarke
Caroline Clarke
Caroline Clarke
Mary Basterfield & Peter Zinkin (G)
Doris Olulode
Caroline Clarke
Caroline Clarke
Caroline Clarke
Caroline Clarke
Caroline Clarke
Caroline Clarke
Debbie Sanders, chief nurse
Glenn Winteringham, chief digital
officer
Caroline Clarke
Doris Olulode
David Grantham
Glenn Winteringham
Libby McManus

Paper 5
Page 5 of 5
4. Forthcoming unconfirmed visits
Below are the non-executive and executive directors’ unconfirmed visits. Once dates for non-
executive directors’ have been confirmed, they will then be advertised to governors.
Date
May 2019
June 2019
July 2019
Area
7 North (gynaecology), Royal Free
Facilities department, Estates, Royal
Free
5 North B (Foetal monitoring), Royal
Free
Damson ward (surgical), Barnet
Galaxy ward (paediatrics), Barnet
10 North (HSEP), Royal Free
Discharge lounge, Barnet
Facilities, estates, Barnet
2 North A (planned investigations unit),
Royal Free
10 South (renal, urology, dialysis,
transplant), Royal Free
2 North A (Ambulatory oncology), Royal
Free
Visited by
Chris Ham
Glenn Winteringham
Chris Streather
Peter Ridley, chief finance and
compliance officer
David Grantham
David Grantham
James Tugendhat
Debbie Sanders
David Grantham
Glenn Winteringham
Chris Streather

Paper 6
Page 1 of 9
Learning from deaths 2018/19: Q2
Executive summary
Just over 2,000 patients a year die at RFL, which is approximately 1% of all admissions. On average each month there are 80 deaths at RFH and 90 deaths at BH. We are currently reviewing an average of 15% of our patient deaths and as part of our Quality Accounts we are aiming to increase this to 21% by March 2019.
Data are provided for all information gathered and validated to date, which includes updates for each quarter’s data.
2018/19 Q2 summary:
472 patient deaths 1 stillbirth 42 patient deaths that meet the review criteria 19 patient deaths selected for random review 64 patient deaths listed for review 13.6% of all patient deaths listed for review 45 patient deaths still under review 19 patient deaths reviewed 2 patient deaths considered likely to be avoidable > 50% (Likert 1-3) 2 patients who died who had learning disabilities 0 LD patient deaths considered likely to be avoidable > 50% (Likert 1-3) 2 patient deaths reported as serious incidents
In Q2, there were 2 patient deaths considered likely to be avoidable identified. These were identified as incidents prior to the Learning from deaths (LfD) process and declared as serious incidents.
Action required/recommendation • To note report • To recommend the National return to be published by the Board on Learning from deaths
(LfD)
Meetings where this report has been discussed previously
Meeting Date Decision Clinical standards and innovation committee March 2019 Noted Mortality surveillance group (MSG) March 2019 Accepted
Report to Date of meeting Attachment numberTrust board 1 May 2019 Paper 6

Paper 6
Page 2 of 9
GOALS BAF risks
Zero never events G-001 Continual reduction in avoidable deaths G-002 Zero avoidable infection G-003 Top 3 for research citation G-004 Top 10 for clinical trials participation G-005 Top 10% for education, training and workforce development G-006 CPG pathways embedded, monitored and digitised G-007 £20m cost reduction through CPGs G-008 Quality improvement embedded as our method of transformation G-031
CQC standards impacted
Safe / effective / caring / responsive / well led
Financial/business implications
None
Equality analysis No identified negative impact on equality and diversity
Compliance impact NHS Improvement, CQC, HSE, NHS Resolution, legislation and regulation, commissioners)
Risks • Failure to review all relevant deaths – mitigated by triangulation of data sets from SIRP, stillbirths, and complaints against all trust deaths
• Increased numbers of avoidable deaths identified – provides opportunities for more learning
• Delay of over 4 months to identify deaths 30 days post discharge, could lead to family distress if incidents are identified and duty of candour needs to be completed – mitigated by updating the bereavement literature to inform families
• There are no dedicated resources to manage, provide medical records, or undertake the Learning from deaths (LfD) process, so time delays will probably occur – this process will be fitted into current job roles.
Report from Deborah Sanders, Chief Nursing Officer Robin Woolfson, Medical Director, RFH Mike Greenberg, Medical Director, BH Alan McGlennan, Medical Director, CFH
Author(s) Hester Wain, Deputy Director of Patient Safety and RiskDenis Sellu, Head of Patient Safety and Risk Nino Soutar, Patient safety administrator
Date 28/02/19
Contents 1. Introduction .................................................................................................................... 3
2. Quality Accounts Aims ................................................................................................... 3
3. Learning from deaths (LfD) data summary ..................................................................... 3
4. Learning from deaths (LfD) Quarter 2 of 2018/19 data review ........................................ 5

Paper 6
Page 3 of 9
1. Introduction Hundreds of patients come through our doors on a daily basis, and most patients receive
treatment, get better and are able to return home, or go to other care settings. Sadly and
inevitably, some patients will die here (approximately 1% of all admissions). While most
deaths are unavoidable and would be considered to be “expected”, there will be cases where
sub-optimal care in hospital may have contributed to the patient’s death. We are keen to take
every opportunity to learn lessons to improve the quality of care for future patients and their
families.
This report provides an update on the patient deaths reviewed to date and the learning we
have gained from this process.
2. Quality Accounts Aims
There are two patient safety Quality Accounts aims related to the Learning from deaths (LfD):
• To increase by 10% the percentage of reviews of patient deaths recorded centrally by the
end of March 2019. For 2017/18, 11% of patient deaths were recorded centrally for
review; our aim is to increase this to 21% during 2018/19. Data on the numbers of
patient deaths reviewed during 2018/19 will only be available from October 2018.
• To improve by 5% the sharing of the learning from serious incidents and patient deaths considered likely to be avoidable; as measured by staff survey data, by the end of March 2019. The 2017 NHS staff Survey showed that 68% of RFL staff agreed/strongly agreed that “When errors, near misses or incidents are reported, my organisation takes action to ensure that they do not happen again.” We are working to use more dynamic survey data to show how we can improve this metric.
3. Learning from deaths (LfD) data summary
Please note that because the Learning from deaths (LfD) reviews are a continuing process, the data are dynamic, and there have been updates to the data since the last report.
2017/18 Q1
2017/18 Q2
2017/18 Q3
2017/18 Q4
2018/19 Q1
2018/19 Q2
Number of patient deaths 480 460 554 576 506 472
Number of stillbirths 9 4 4 7 12 1
Number of patient deaths that meet the review criteria
31 39 38 38 62 42
Number of patient deaths selected for random review
5 11 22 24 22 19
Number of patient deaths listed for review
36 51 65 63 85 64
% of all patient deaths listed for review
7.5% 11.1% 11.7% 10.9% 16.8% 13.6%
Number of patient deaths still under review
5 13 13 23 33 45
Number of patient deaths reviewed
31 38 52 40 52 19

Paper 6
Page 4 of 9
2017/18 Q1
2017/18 Q2
2017/18 Q3
2017/18 Q4
2018/19 Q1
2018/19 Q2
Number of patient deaths considered likely to be avoidable > 50% (Likert 1-3)
3 2 4 11 2 2
Number of patients who died who had learning disabilities
2 3 4 5 6 2
Number of LD patient deaths considered likely to be avoidable > 50% (Likert 1-3)
0 0 0 1 0 0
Number of patient deaths reported as serious incidents
4 2 5 12 3 2
Chart 0: The data are presented by quarter. The blue bars show the number of inpatient deaths reviewed, the red bars the number considered likely to be avoidable and the black bars the number declared as serious incidents (which will include the avoidable deaths).
In Q4, 11 patient deaths were identified that were considered likely to be avoidable. It should be noted that we do not yet have enough data to determine a baseline of how many deaths on average are likely to be avoidable. Thus any comparison of the quarterly data at this time may be misleading. However, due to the apparent increase of deaths likely to be avoidable in Q4, these have all been re-reviewed at the Hospital Mortality review groups (MRG) who have agreed that the likert scoring was appropriate and was related to the death of the patient.
Paper 6
Page 5 of 9
4. Learning from deaths (LfD) Quarter 2 of 2018/19 data review
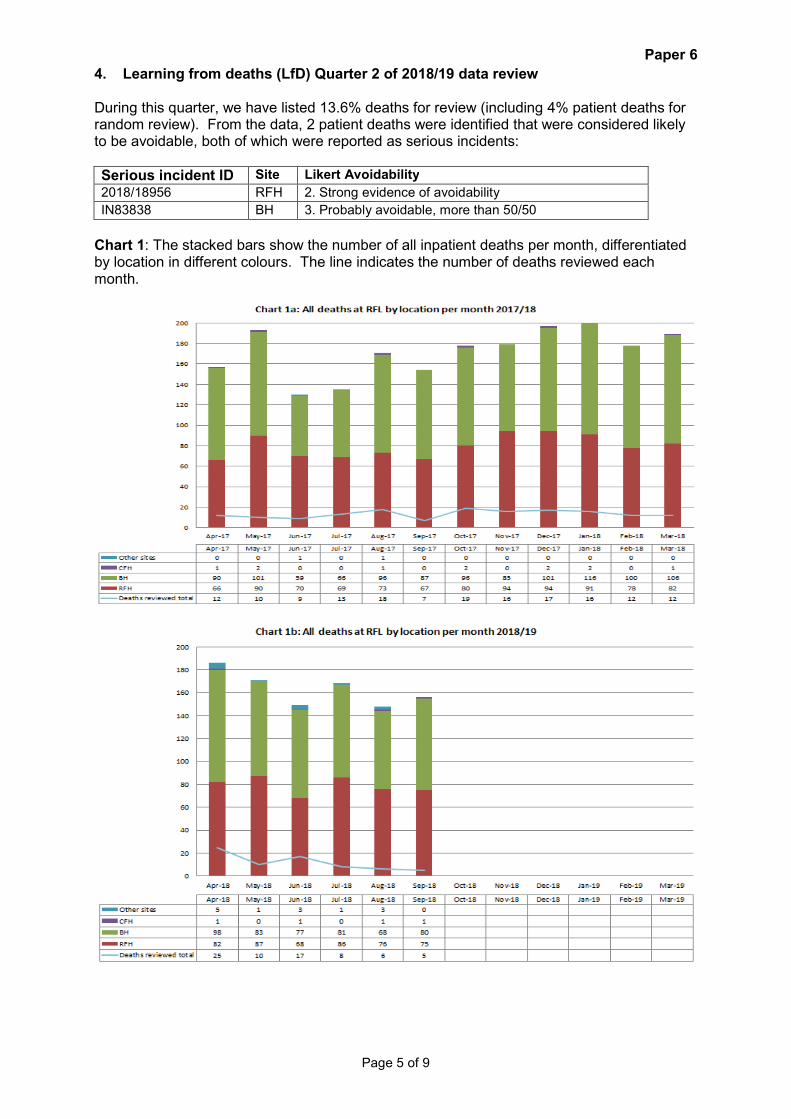
During this quarter, we have listed 13.6% deaths for review (including 4% patient deaths for random review). From the data, 2 patient deaths were identified that were considered likely to be avoidable, both of which were reported as serious incidents:
Serious incident ID Site Likert Avoidability
2018/18956 RFH 2. Strong evidence of avoidability
IN83838 BH 3. Probably avoidable, more than 50/50
Chart 1: The stacked bars show the number of all inpatient deaths per month, differentiated by location in different colours. The line indicates the number of deaths reviewed each month.

Paper 6
Page 6 of 9
Chart 2: The blue bars indicate the total number of deaths reviewed per month, the red bars showing the number that are considered likely to be avoidable. The line indicates the number of inpatient deaths which meet the key criteria for review.
Paper 6
Page 7 of 9
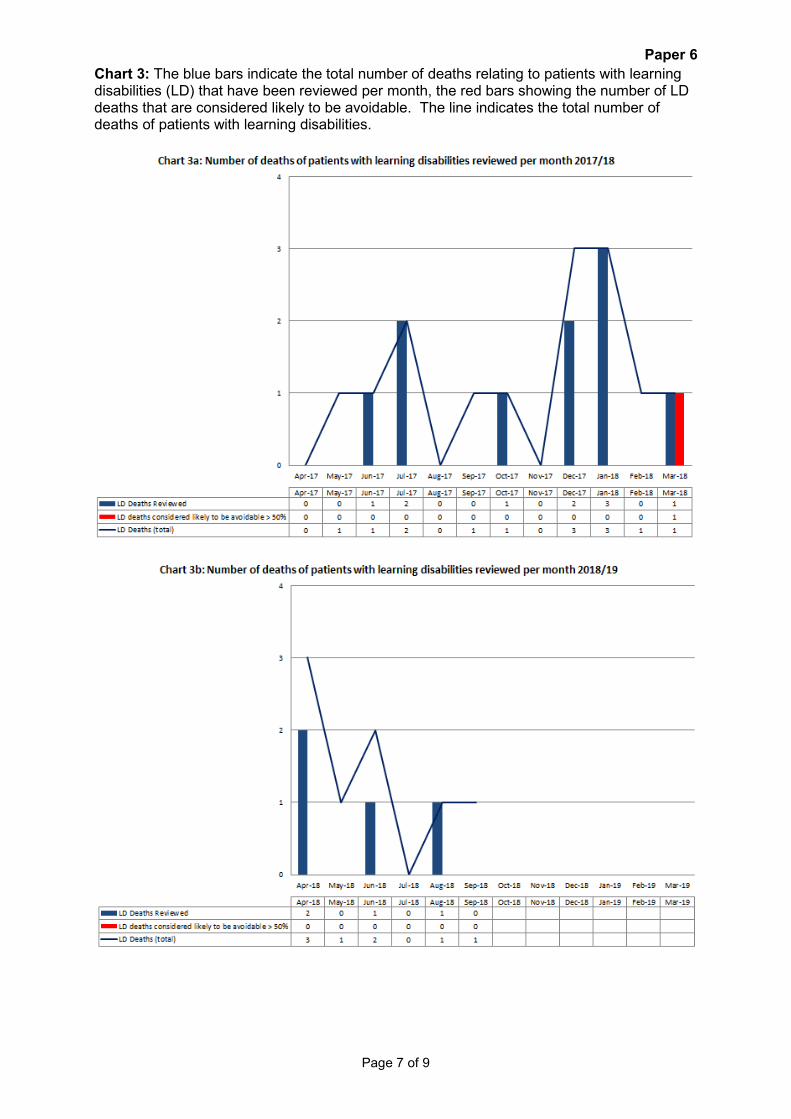
Chart 3: The blue bars indicate the total number of deaths relating to patients with learning disabilities (LD) that have been reviewed per month, the red bars showing the number of LD deaths that are considered likely to be avoidable. The line indicates the total number of deaths of patients with learning disabilities.

Paper 6
Page 8 of 9
Chart 4: The stacked bars indicate the number of inpatient deaths listed for review per month by the different criteria (listed on the right hand side). The line indicates the number which have been reviewed to date.
Paper 6
Page 9 of 9
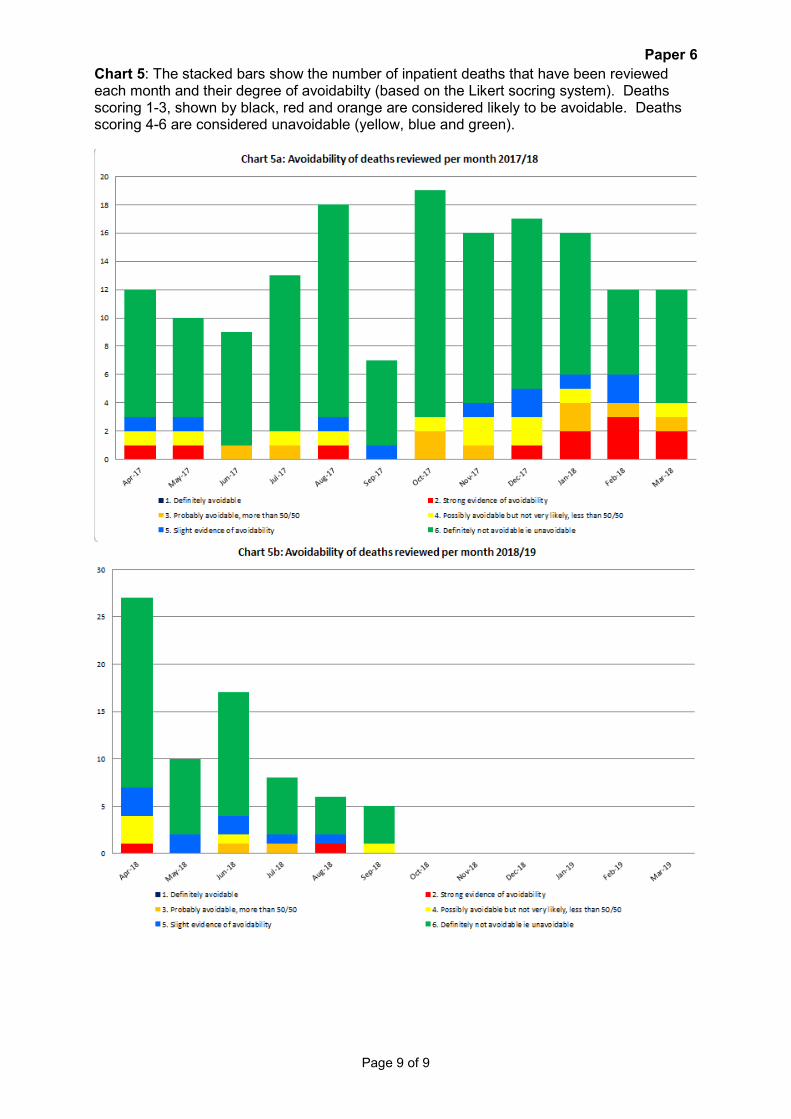
Chart 5: The stacked bars show the number of inpatient deaths that have been reviewed each month and their degree of avoidabilty (based on the Likert socring system). Deaths scoring 1-3, shown by black, red and orange are considered likely to be avoidable. Deaths scoring 4-6 are considered unavoidable (yellow, blue and green).

Page 1 of 1
Financial performance report for month 12 (March 2019)
Executive summary
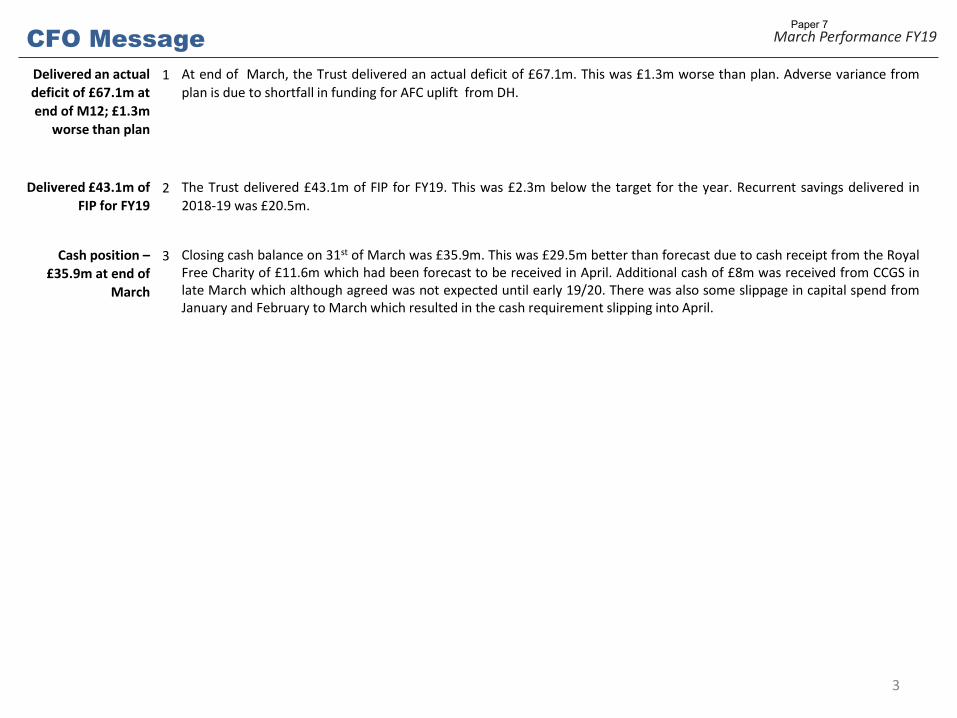
At end of month 12 the trust reported an actual deficit of £67.1m which is £1.3m worse than plan. This is due to shortfall in funding for AFC pay award.
The 2018/19 financial improvement plan (FIP) savings target was £45.4m. The trust delivered savings of £43.1m. This is £2.3m below target.
Closing cash balance on 31st of March was £35.9m. This was £29.5m better than forecast due to cash receipt from the Royal Free Charity of £11.6m which had been forecast to be received in April. Additional cash of £8m was received from clinical commissioning groups (CCGs) in late March which although agreed was not expected until early 2019/20. There was also some slippage in capital spend from January and February to March which resulted in the cash requirement slipping into April.
Action required/recommendation
The board is asked to note the current financial position of the trust.
Meetings where this report has been discussed previously Meeting Date Decision
Board/GEC/LEC/committee goals
GOALS BAF risks
1. Deliver regulatory undertakings G -020
2. Financial performance G- 047
CQC standards impacted Use of resources / Well led
Financial/business implications N/A
Equality analysis No identified negative impact on equality and diversity
Compliance impact NHS Improvement
Report from Peter Ridley, group chief finance and compliance officerAuthor(s) Senior Finance TeamDate 25th April 2019
Report to Date of meeting Attachment number
Trust Board Part I 1 May 2019 Paper 7
Paper 7

The Royal Free London
Finance Report M12 TB Part 1
1
Paper 7

YTD Performance at M12 – Headlines
2
Performance against Plan
In Year Performance - FY19
Agency Spend Vs. Last year
• Fy19 performance against plan - £1.3m adverse due shortfall in AFC funding from DH
FIP Performance
• FY19 FIP delivery of £43.1m - £2.3m below plan
Capital Expenditure
Agency spend £0.3m above ceiling for FY19. Adverse variance against ceiling is predominantly
due to digital strategy
In Month YTD Forecast
Plan Actual Variance Plan Actual Variance
£m £m £m £m £m £m
9.6 11.9 -2.3 84.5 81.0 3.5
Cash Flow forecast
Number Value
£'m Number
Value
£'m % Number % Value
NHS 4,022 £90.62 1,164 £41.51 29% 46%
Non NHS 214,031 £756.11 169,071 £530.78 79% 70%
Total 218,053 £846.74 170,235 £572.30 78% 68%
within 30 days Total
Better Payment Performance Code
Paper 7
CFO Message
Delivered an actual
deficit of £67.1m at
end of M12; £1.3m
worse than plan
1 At end of March, the Trust delivered an actual deficit of £67.1m. This was £1.3m worse than plan. Adverse variance from
plan is due to shortfall in funding for AFC uplift from DH.
Delivered £43.1m of
FIP for FY19 2 The Trust delivered £43.1m of FIP for FY19. This was £2.3m below the target for the year. Recurrent savings delivered in
2018-19 was £20.5m.
Cash position –
£35.9m at end of
March
3 Closing cash balance on 31st of March was £35.9m. This was £29.5m better than forecast due to cash receipt from the Royal Free Charity of £11.6m which had been forecast to be received in April. Additional cash of £8m was received from CCGS in late March which although agreed was not expected until early 19/20. There was also some slippage in capital spend from January and February to March which resulted in the cash requirement slipping into April.
3
March Performance FY19 Paper 7

M12 Overview
4
March Performance FY19
Plan Actual Variance Plan Actual Variance
£ '000s £ '000s £ '000s £ '000s £ '000s £ '000s
NHS Clinical Income 58,767 66,294 7,527 692,406 703,739 11,333
TEDD Income 16,474 14,966 (1,509) 197,682 191,848 (5,834)
Non NHS Clinical Income 3,779 3,060 (720) 40,560 33,780 (6,780)
Other Operating Income 8,381 19,196 10,816 106,146 111,137 4,991
Property Services Income 11,535 11,535 16,807 16,807
Total Income 87,401 115,051 27,650 1,036,793 1,057,311 20,517
Pay (45,527) (47,638) (2,111) (548,539) (543,807) 4,731
Other Pay (Apprentice Levy) (207) (277) (70) (2,413) (2,471) (58)
Non-Pay Expenditure (Excl. TEDD) (23,943) (54,197) (30,254) (302,929) (340,089) (37,160)
Property Services Expenses (73) (1,050) (977) (220) (5,887) (5,666)
TEDD Expenditure (15,930) (9,292) 6,638 (190,715) (177,480) 13,235
Total Operating Expenditure (85,681) (112,455) (26,774) (1,044,815) (1,069,734) (24,918)
SLR 0 0 0 (0) (0) 0
EBITDA 1,720 2,596 876 (8,022) (12,423) (4,401)
Interest, Dividends & Depreciation (4,881) (2,417) 2,464 (57,804) (54,704) 3,100
Profit/Loss Of Disposal Of FA 15 15 6 6
Investment In Joint Ventures 67 67 67 67
Other Gains/Losses (27) (27) (27) (27)
Surplus/Deficit (3,161) 234 3,395 (65,826) (67,080) (1,254)
In Month YTD
Paper 7
Page 1 of 1
OPERATIONAL PERFORMANCE REPORT
Executive summary
This report outlines the latest submitted performance data for the key operational indicators (A&E, cancer & RTT) along with benchmarking information and key risks/mitigations
Action required/recommendation
The board is asked to note the current performance of the trust
Meetings where this report has been discussed previously Meeting Date Decision
Board/GEC/LEC/committee goals
GOALS BAF risks
1. ED access target 95% G-010
2. RTT 18 weeks target: 92% G -036
3. Cancer access 62 days: 85% G- 037
CQC standards impacted Safe / effective / caring / responsive /
well led
Financial/business implications None
Equality analysis No identified negative impact on equality and diversity
Compliance impact NHS constitution standards
Report from Peter Ridley, Chief Finance & Compliance Officer
Author Senita Rani Robinson, Performance Measurement Lead
Report to Date of meeting Attachment number
Trust board 1 May 2019 Paper 8
Paper 8

Royal Free London –operational performance
April 2019
Paper 8

2
Operational performance summary report
Where we are Predictions Key Risks
Cancer – Feb2019
• Performance in February was reported at 74.1%
• The majority of breaches were within the prostate, lung, lower GI and renal tumour sites.
• The largest backlog volumes are in the lower GI (34), prostate (11) & lung (11) tumour sites.
• Un-validated March performance is 75.21%.
• The backlog is currently 121 overall with 34 diagnosed >62 days.
• We have seen 7 consecutive positive outliers in backlog volume compared with previous performance.
• Continued reduction in diagnosed backlog will impact 62 day performance in March.
• Cancer ASI volumes have increased trustwide since the beginning of 2019. This did fall during March but has subsequently increased back to 174. The largest volumes are within Skin and Lower GI tumour sites.
A&E –Mar 2019
• Trustwide performance in March was 86.5%
• BH performance was reported at 81.6%
• RFH performance was reported at 86.6%
• November performance onwards is still being validated due to delay in agreeing the correction workflow. This is being discussed between the Data Quality Team, Information Management and Cerner.
• Predicted increase in attendances during February, as per seasonal adjustment
• A revised system-wide BH improvement plan is being implemented
Paper 8

3
62 Day Cancer – Performance Summary
Current Period February: below 2017/18 performance, trajectory and standard at Trust level
Relative position Feb 2019: 3rd quartile at trust level
% cancer patients waiting < 62 days from GP referral to first treatment
Source: NHS England, Apr 2019
*Please note* Whilst performance has previously been reported on a site-basis in the benchmarking table, this is reported by Business Unit for February and will
continue.
Paper 8

4
In February, 4 out of 16 tumour sites accounted for 41% of the Trust’s total breaches:
● RFH HpB – 3.5 breaches (performance 46.2%)
● RFH Lower GI – 3 breaches (performance 50%)
● RFH Prostate – 3.5 breaches (performance 63.2%)
● BH Lung – 2.5 breaches (performance 37.5%)
62 Day Cancer – Sources of Current Performance
February Performance by Tumour site Observations
Number of excess patient breaches*
* Actual breaches minus breaches that would have been incurred if the tumour site were exactly at 85% standard
41% of total RFL excess breaches
Paper 8

5
62 Day Cancer – Diagnosis and Actions
What is our diagnosis of what is driving current performance and future risks?
What are our action priorities and what is our status on them?
1. Persistent backlog
2. US machine delay for breast service
3. Cancer CPG launch
1. The overall backlog reduced significantly during February and the beginning of March but has now plateaued and is off planned trajectory. Operational managers are managing this in weekly performance meetings and one of the initial CPG aims is to bring the wait for first event (OPA/STT) down to 7 days.
2. The US machine has now been delivered and will provide additional diagnostic capacity. Radiology are currently reviewing their staffing and resource in conjunction with the breast team to ensure it is fully operational.
3. The cancer CPG officially launched on 4th April where tumour site teams met with key support services to identify challenges and actions. The actions captured from this day will inform the start of the pathway work. These will be collated and presented to teams at Cancer Oversight.
Paper 8

6
A&E – Performance Summary
Current Period March: performance is above 2017/18 performance, but below standard & trajectory at Trust level
Relative position Mar 2019: 2nd quartile at trust level
% patients waiting < 4 hours in A&E
*November performance* There were a number of issues following EPR go-live and records are being corrected in Cerner. The position will be updated once the
amendments are made.Source: NHS England, Apr 2019
Paper 8

7
A&E – Barnet Sources of Current Performance
Current Period Performance
Performance against 4 hour standard
DTOC and MOs
Total DTOC and MO bed days – February 2019 DTOC by borough – February 2019
Performance continues to be challenging, however the internal improvement programme continues to progress, focusing on the following areas:• Reducing extended length of stay• Improving Minors flow • Reviewing opportunities to use space differently to
support flow, including development of a UTC• AMU pathways and flow• ED workforce plan & long-term strategy
November performance onwards shown on the graph is the current unvalidated position.
Paper 8

8
A&E – Barnet Diagnosis and Actions
What is our diagnosis of what is driving current performance?
What are our action priorities and what is our status on them?
Capacity & space• Attendances continue to increase; BH ED
is seeing in the region of 340-420 patients per day (department is built for 275).
• Bed occupancy continues at 98-100%.
Flow & discharges• DTOC and MOPs continue• External delays due to pressures within
system partners, (e.g.) D2A Pathway 3 and completion of DSTs
• Volume of discharges and time of day needs to improve
• New AMU pathways not yet embedded
Workforce• Vacancies continue within medical &
nursing workforce
• GPs have been relocated to 3 additional rooms to free up more Minors capacity.
• Scoping of space options for the development of a UTC at BH have commenced and a feasibility study will shortly be developed with CCG
• Bed modelling discussions on-going with system partners to agree long-term plan.
• 21 day+ stranded patients reviews continue; new approach being tested w/c 22 April to reduce delays & improve planning for most complex patients
• Daily DToC & MO meeting being reviewed• Further work to improve discharge training
& education – workshop scheduled in May• New AMU pathways being tested and
refined
• ED workforce plan for 19/20 being developed, to include ANPs/new roles
• eRoster implementation being progressed
Paper 8

9
A&E – Royal Free Sources of Current Performance
Current Period Performance
Performance against 4 hour standard
DTOC and MOs
• A new trajectory has been agreed for 2019/20 which hopes to achieve 90.3% in April 2019.
• The DTOC target was met in February 2019 and patient streaming continues to be stable at 27%.
November performance onwards shown on the graph is the current unvalidated position.
Total DTOC and MO bed days – February 2019 DTOC by borough – February 2019
Paper 8
10
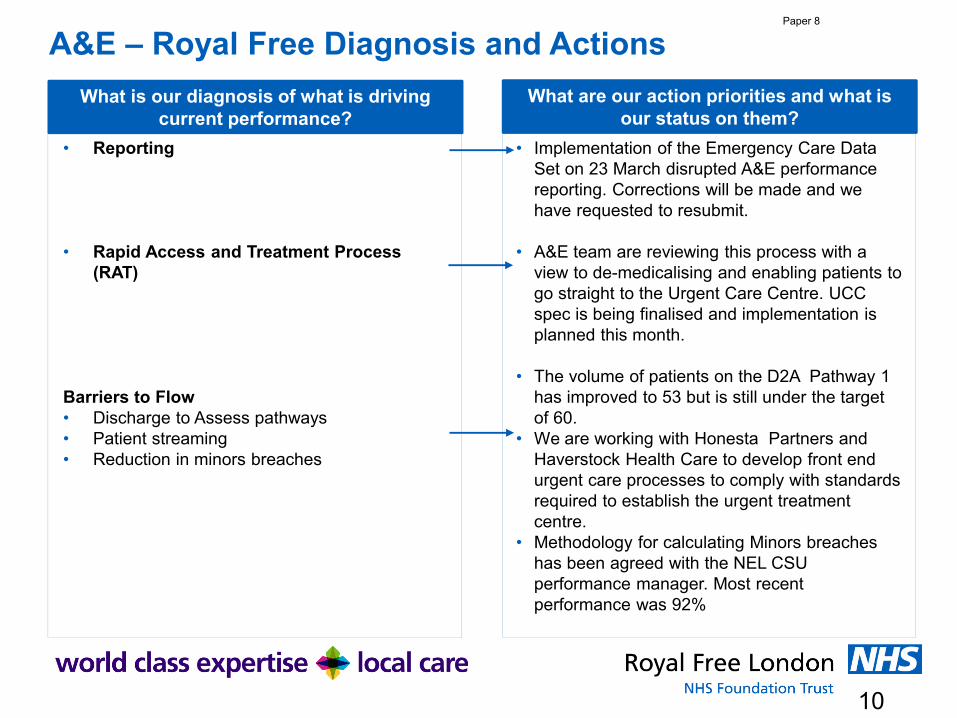
A&E – Royal Free Diagnosis and Actions
What is our diagnosis of what is driving current performance?
What are our action priorities and what is our status on them?
• Reporting
• Rapid Access and Treatment Process (RAT)
Barriers to Flow• Discharge to Assess pathways• Patient streaming• Reduction in minors breaches
• Implementation of the Emergency Care Data Set on 23 March disrupted A&E performance reporting. Corrections will be made and we have requested to resubmit.
• A&E team are reviewing this process with a view to de-medicalising and enabling patients to go straight to the Urgent Care Centre. UCC spec is being finalised and implementation is planned this month.
• The volume of patients on the D2A Pathway 1 has improved to 53 but is still under the target of 60.
• We are working with Honesta Partners and Haverstock Health Care to develop front end urgent care processes to comply with standards required to establish the urgent treatment centre.
• Methodology for calculating Minors breaches has been agreed with the NEL CSU performance manager. Most recent performance was 92%
Paper 8

11
RTT – Diagnosis and Actions
What is our diagnosis of what is driving current performance?
What are our action priorities and what is our status on them?
1. National reporting has now stopped whilst we work through validation of the new PTL.
2. The working version of the PTL (the waiting list) will continue to suffer from ‘pop-on’ long-waiting patients as the validation team uncover genuine patients and add them to the operational view.
3. The full suite of waiting list and performance reports is not yet available to operational and clinical teams to enable them to monitor their performance and act on early warnings.
1. Operational focus of >40 week waiters will remain as is and we will continue to report performance internally. The governance structure will also remain as is to ensure senior oversight and that patients do not wait longer for treatment due to this change.
2. As outlined above, governance including senior oversight of >40 week waiters, the existing meeting structure, clinical harm process and RCA process will continue as normal. As genuine pathways are uncovered operational teams will review quickly and action as appropriate.
3. The outpatients productivity programme has started and we are refreshing our theatres productivity programme. A theatres dashboard is now available. The Luna validation tool has been launched which gives much greater visibility over the validation process and status of the MBI PTL than we have had previously.
Paper 8
Paper 9
1 X:\ Chair and CEO report 1 May 2019
CHAIRMAN’S AND CHIEF EXECUTIVE’S REPORT
Executive summary
This is a combined chairman’s and chief executive’s report containing items of interest / relevance to the board.
Action required
The board is asked to note the report.
Meetings where this report has been discussed previouslyMeeting Date Decision Not applicable
Board/GEC/LEC/committee goals
GOALS
Not applicable
BAF risks
CQC standards impacted Well led
Financial/business implications Not applicable
Equality analysis Not applicable
Compliance impact Not applicable
Report from D Dodd, group chairman and C Clarke, group chief executive Author Alison Macdonald, board secretary
Report to Date of meeting Attachment number
Trust Board 1 May 2019 Paper 9

Paper 9
2 X:\ Chair and CEO report 1 May 2019
CHAIRMAN’S AND CHIEF EXECUTIVE’S REPORT
A RECRUIT DEVELOP AND RETAIN THE BEST TALENT
PLANNED STAFF ENGAGEMENT EVENTS
“What matters to you?” international day Wednesday 5 June 2019
“What matters to you?” is an international initiative originating from NHS Scotland (with support from the Institute of Healthcare Improvement and others). It aims to rebalance the focus of healthcare delivery from ‘What’s the matter with you?’ to ‘What matters to you?’ (WMTY). The first Wednesday of June has become a day when there is international focus on WMTY. This year it is Wednesday 5 June.
RFL first participated actively in June 2017, with a focus on what matters to our patients. This laid foundations for work which in some cases (eg in therapies) has led to national and international recognition for RFL – such as the work presented by Karen Turner to the board in February 2019.
In June 2018 our focus was on what matters to staff. With support from the RFL Charity, events and celebrations were organised on our three main hospital sites and at Enfield Civic Centre. What we did and learned then has laid important foundations for our current Joy in Work initiative as well as generated improvements and momentum across the trust for locally led initiatives and plans (including local staff experience and retention plans and activity).
This year the thematic emphasis will be on what matters to staff, linked to the Joy in Work initiative and outputs of the national staff survey. The focus being on listening locally to what can be done to improve staff satisfaction. Each site will encourage local departments/services to organise activities which best fit the approach they wish to take.
National day for staff networks– Wednesday 8th May 2019
The national day for staff networks is the first ever day recognizing the added value of staff networks. It is an important day because it aims to raise awareness of the support and influence staff networks provide to employees from all communities to share an area of common of interest. The day encourages networks to collaborate in their celebration and work with the trust to foster an inclusive workplace as it provides opportunities to learn and share best practices as well as network and grow. There will be a series of celebratory events involving the trust’s four staff networks – LGBT+ & Friends, disability, BME, and the women’s’ network.
NHS equality, diversity & inclusion week 13-17 May 2019
This year's theme is 'diverse, inclusive, together' and has been chosen to reflect the move across the health and social care sector towards even greater collaboration and integration - as reflected in the publication of the recent NHS Long term Plan.
The RFL events include sessions focussing on career development and disability human stories, which raise awareness of managers and staff around declaration and receiving support for reasonable adjustments.

Paper 9
3 X:\ Chair and CEO report 1 May 2019
RECRUITMENT ROBOT
The Royal Free London (RFL) has been shortlisted for two awards after using a ‘robot’ to help improve the trust’s recruitment process. The robot, known as STU, has helped reduce the average length of time it takes to recruit staff by five days, as well as reducing data error and improving the experience of staff and candidates.
Between January 2018 and January 2019 the RFL recruitment service received 12,487 applications. Additionally, the team handles 3,296 rotational training moves, both for the group’s own trainees and as a lead employer for GP trainees across north London. With ever-increasing pressure to reduce costs and consolidate back office functions, a radical reshaping of recruitment services was needed.
Thanks to the success of the robot, which has reduced delays and backlogs to an absolute minimum, the trust has been shortlisted for a Health Service Journal (HSJ) value award and a Healthcare People Management Association (HPMA) excellence award.
B REDUCE UNWARRANTED VARIATION IN PATIENT CARE AND ACADEMIC EXCELLENCE
HEALTH SERVICE JOURNAL(HSJ) PATIENT SAFETY AWARDS
RFL is a finalist for two awards, as follows
• Deteriorating patients and rapid response systems award – for development of a digitally enabled pathway for Acute Kidney Injury to deliver better, safer patient care (Streams)
• Maternity and midwifery services initiative of the year – keeping mothers and babies together
The final round of judging will take place in May where shortlisted organisations will present their projects to the HSJ’s leading panel of experts and NHS leaders. Winners will be announced in July.
PEARS BUILDING
Works within the ground are now complete and the focus has moved to the construction of the concrete frame, which is emerging from the ground.
This involves casting the upper floors, the stair cores, staircases and lift shafts. The vehicle ramp, providing access to the car park, is near completion. And the external concrete retaining walls are substantially complete and protected against the elements. Brickwork samples have been agreed and an array of samples across all key architectural finishes, fixtures and fittings, are being considered.
Between now and June will see the frame continued to level 5, and a precast concrete feature will provide banding to the individual floor edges. This will then permit work on the brickwork and glazing.

Paper 9
4 X:\ Chair and CEO report 1 May 2019
Design concepts to aid the installation of a future linear accelerator are progressing and these will be signed off by the trust. Discussions are also underway concerning the long-term car parking strategy for the site once the Pears Building opens.
Although a little time has been lost owing to high winds delaying certain works, the project remains on track. As the building progresses, an operational policy is being designed to be put in place before the building is handed over.
Safety of the public and the workforce and minimising the impact on our neighbours remain the highest priorities. The work is constantly monitored to ensure that agreed thresholds of noise, vibration and dust are not exceeded.
C DELIVER WORLD CLASS SUPPORT SERVICES AND NEW SOURCES OF INCOME
Mike Dinan, the commercial finance director is progressing existing plans to grow the trust’s commercial income in areas such as the new property services subsidiary and central decontamination unit and in the trust’s existing range of commercial activities in areas such as the pharmacy manufacturing unit and the pathology joint venture (HSL)
Plans are progressing on the new central decontamination unit at Chalkmill Drive in Enfield. The state of the art unit will open in June and will clean approximately four million instruments and 35,000 scopes for the Royal Free group of hospitals. It is planned to offer this service to other NHS trusts as well as to private hospital providers.
Robert Prince, newly appointed managing director of corporate shared services is actively developing a commercial plan for RFL’s corporate shared services, looking to build a shared service model for the Royal Free group which can be marketed to other organisations. An example would be how to actively make use of the existing investment in robotic process automation (RPA) in areas such as recruitment.
Governance for both developments will be with the group services and investment committee.
D POPULATION HEALTH AND COLLABORATION
INTER-GREAT
The current way the NHS and local authorities manage and deliver health and social care services does not meet the current, and will not meet the future, health and care needs of the aging population. Many areas are looking to develop integrated care systems where health and care partners work much more closely together. The potential gains of this approach; such as better health outcomes and improved patient experience, coupled with reducing demand on health and social care services are essential goals for the local health economy.

Paper 9
5 X:\ Chair and CEO report 1 May 2019
In response to this a simulation event was held in October 2018 bringing together senior leaders from the different organisations within North Central London, and patient/public representatives, to test out through the simulation a potential model for taking forward integrated care across Barnet, Camden, Enfield, Haringey and Islington. It was agreed that further work should take place within the five boroughs.
NCL have invited views on their next steps on the development of integrated care systems. The trust has responded expressing support for this work and enthusiasm to be part of it. Work has started at a borough level on bringing health and care services together to improve care for patients and residents which the Royal Free senior teams are engaged in.
E EXCELLENT OPERATIONAL AND FINANCIAL PERFORMANCE
REFERRAL TO TREATMENT TIME (RTT)
At the board meeting in March 2019 it was agreed to pause reporting the trust’s referral to treatment time (RTT) figures because of the data quality issues previously reported.
RTT is the period of time from when a patient is referred to the trust to when he or she begins their treatment. The standard trusts are required to meet is that 92% of patients should start their treatment within 18 weeks of being referred. The trust identified there was a problem with its RTT data last year and an improvement programme was established to resolve the issue. At all stages the trust has kept local clinical commissioning groups, NHS England and NHS Improvement informed.
The decision to pause reporting the RTT figures is a temporary measure and the trust will begin reporting again when the issue has been resolved. New, robust methods for measuring RTT data are being implemented to prevent this happening again.
The pause in reporting will not affect waiting times for patients, who continue to be the trust’s absolute priority. Patients on the waiting list will be treated according to clinical need and those waiting longest will be seen first.
CHASE FARM HOSPITAL
Generators: It was first reported in August 2018 that the stand-by generator within the energy centre constructed as part of the hospital build was not compliant with the 21 second hospital technical memorandum (HTM) performance requirement.( HTMs provide guidance on healthcare-specific elements of standards, policies and up-to-date established best practice). Whilst a conditional certificate of practical completion was subsequently agreed it is only now possible, following numerous adjustments, changes and black start re-tests to confirm compliance. Full certification is due to be issued.
Diesel Spillage: Following a diesel spillage from the energy centre in in July 2018 that resulted in diesel flowing around, out and under the energy centre, it is advised that expert reports confirming that appropriate remediation works, including removal of contaminated land have been completed. At the time of the spillage all relevant statutory and utility stakeholders were advised and no subsequent notices or claims have been received in relation to downstream contamination.

Paper 9
6 X:\ Chair and CEO report 1 May 2019
Time Capsule: following removal of one of the original 1886 foundations stones during the course of demolition of part of the clocktower a glass time capsule was found which appears to hold numerous scrolls of paper. This was opened on the 24 April 2019 by a professional conservator with BBC London in attendance. Due to the amount of paper desiccation is was not possible to remove the paper scrolls and the time capsule was taken away for removal under laboratory conditions by the conservator. The BBC London could well broadcast a piece on the capsule in the future.
FAMILY AND FRIENDS TEST (FFT)
The NHS friends and family test (FFT) was introduced in 2013 to enable patients to feed back on their care and treatment to enable hospitals and other providers to improve services. It asks patients whether they would recommend hospital wards, A&E departments, maternity services and out-patient clinics to their friends and family if they needed similar care or treatment. The March results are below.
Royal Free London combined data
% likely/extremely likely to recommend March 2019
(range: 0 – 100%)
Number of patient responses
In-patient 86% 832
A&E 84% 3095
Barnet Hospital % likely/extremely likely to recommend March 2019
(range: 0 – 100%)
Number of patient responses
In-patient 85% 267
A&E 79% 1364
Antenatal care 100% 1
Labour and birth 100% 22
Postnatal hospital ward 100% 23
Postnatal community care 100% 7*
Out-patients 85% 72
Chase Farm Hospital % likely/extremely likely to recommend March 2019
(range: 0 – 100%)
Number of patient responses
In-patient 92% 65
Out-patients 96% 157

Paper 9
7 X:\ Chair and CEO report 1 May 2019
Royal Free Hospital % likely/extremely likely to recommend – March 2019
(range: 0 – 100%)
Number of patient responses
In-patient 86% 500
A&E 87% 1731
Antenatal care 100% 1
Labour and birth 100% 34
Postnatal hospital ward 94% 34
Postnatal community care 100% 7*
Out-patients 93% 771
*The postnatal community care question is only reported as a whole trust figure and not split by site.
F STAKEHOLDERS
COUNCIL OF GOVERNORS
Professor Sir Chris Ham, non-executive director, chaired the Chase Farm Hospital local member’ council on 16 April 2019. The chair welcomed Cllr Christine Hamilton the new Enfield Council appointed governor. Items discussed were the performance and challenges faced by Chase Farm Hospital including improving transport access to the hospital. The lessons learnt from the implementation of the electronic patient record system were also discussed. The first medicine for members’ event at Chase Farm Hospital will take place on 30 April 2019. This event will be chaired by Mr George Verghese, staff governor. Over a hundred members have registered for the event; the topic is the new hospital itself.
Barnet Hospital is holding their third local members council on 23 April 2019. Items on this agenda are partnership working, the locally focussed recruitment and retention programme and an update on negotiations with Barnet Council on car parking issues.
G OTHER UPDATES
COMMUNICATIONS BOARD REPORT: FEBRUARY 2019
Media coverage
Positive stories: Digital Health and Nursing Times reported on progress following the launch of our new electronic patient record (EPR). BBC London TV news featured a new laser scanner used in our audiology service. Filming took place with a patient and Mitch

Paper 9
8 X:\ Chair and CEO report 1 May 2019
Chandler, chief audiologist at RFH, was also interviewed. We are the first hospital in the NHS to use the scanner.
Main negative story: The RFL was mentioned in an Observer story about bailiffs being called in to collect the debt of patients not eligible for treatment under the NHS. The table below shows the sentiment of press mentions in March (this does not include coverage of the scaffolding collapse):
March Royal Free Hospital
Barnet Hospital Chase Farm Hospital
Total
Positive 103 0 3 106Neutral 165 14 9 188Negative 42 0 0 42Total 310 14 12 336
Digital communications
Total number of Facebook followers: 7,132 (+379) Number of Posts: 75, reaching 111,938 people
Total number of Twitter followers: 17,483 (+358) Number of Tweets: 165, reaching 300,016 people
Our top Twitter post for March was about the Royal Free Hospital nursing open day. The post received 10,356 impressions and 1,563 total engagements on Twitter.
The second most popular Twitter content was a post following the collapse of scaffolding near the Royal Free Hospital site. The post received 10,302 impressions on Twitter and it was the most popular website content for March with 823 page views.
Internal communications
Freenet 2 – To raise awareness and build excitement about Freenet 2, our new intranet, the key benefits and improvements were highlighted to staff. Key stakeholders received targeted communications to ensure they are engaged and understand they are responsible for migrating existing content over and developing and uploading new content.
Staff survey – Following publication of the 2018 NHS staff survey results, staff were thanked for taking part and areas where the trust has improved, areas where we recognise we can get better and our plans as a trust to improve the experience of our staff were highlighted across all our channels. An infographics page with key headlines and next steps was included in the March issue of Freepress.
Staff experience – Following publication of the staff survey results, communications were shared to increase staff awareness about the work taking place to improve the experience of staff, including articles about staff health and wellbeing events, values and behaviours videos, staff networks day, mental health first aiders training, Joy in Work improvement collaboration and improving our disability declaration.

Paper 9
9 X:\ Chair and CEO report 1 May 2019
NHS ENGLAND’S AND NHS IMPROVEMENT’S FUNDING AND RESOURCE PUBLICATION SUPPORTS DELIVERY OF THE NHS LONG TERM PLAN
On 28 March 2019, NHS England and NHS Improvement published a joint document which sets out the funding pledges and support that will be provided to help the NHS deliver on the priorities outlined in the NHS Long Term Plan. NHS England and NHS Improvement funding and resource 2019/20: supporting ‘The NHS Long Term Plan’ describes how funding, people and resources will be distributed, to transform local health and care systems. It also explains how both organisations will reduce inequalities between patients, both in terms of access to services and outcomes, and how patients will be kept informed, involved and consulted in the development, improvement and delivery of services.
CHIEF MIDWIFE APPOINTED
The first chief midwife, who will become the most senior midwife in England, has been appointed. Professor Jacqueline Dunkley-Bent will be the first to take on the new role, to oversee delivery of a package of measures building on increased safety and support in maternity care as well as promote safer births as part of the NHS Long Term Plan. She will provide professional, strategic and clinical leadership to colleagues working across the country.

FINAL
Audit committee report
Executive summary
To follow is an update from the audit committee meeting held 15 March 2019 on key discussion items and agreed actions.
Also attached are the confirmed minutes of the audit committee meeting held on 18 January 2019 (Annex A)
Action required
The board is asked to note the report.
Meetings where this report has been discussed previously
Meeting Date Decision n/a n/a n/a
Board/GEC/LEC/committee goals
GOALS BAF
risks
Demonstrable organisation health (group governance) G042/044
CQC standards impacted Well led
Financial/business implications Any such implications would be outlined in the report.
Equality analysis No identified negative impact on equality and diversity
Compliance impact Any such implications would be outlined in the report.
Report from Mary Basterfield, non-executive director and chair of audit committeeAuthor Veronica Jackson, group committee administrator Date 17 April 2019
Report to Date of meeting Attachment number
Trust board 1 May 2019 Paper 10

FINAL
SPEAKING UP (WHISTLEBLOWING)
The committee received its regular update on the trust’s speaking up processes. It was pleased to note that staff were continuing to put themselves forward for the role of speaking up champion, taking the total number of champions to over 40. It was noted that had been an increase in the number of speaking up cases reported since the previous meeting and the committee sought assurance that capacity was available to handle those.
DATA QUALITY (DQ)
The committee received its DQ progress update; the DQ strategy had been signed off in January and was being embedded, the governance structure was working well and an annual programme of manual audit in line with the Data Security and Protection Toolkit Standard 1.7 would be undertaken alongside other internal manual audits of patient data. Processes were also in place to ensure there was a structured way of managing change requests to business structures and ensuring they were formally documented. In terms of the outstanding recommendations from the internal audit review on DQ, three had been met and two were partially met with their completion dates having been extended to end April 2019.
The committee was assured that this process of audit and oversight would help to ensure the quality of the data in future and the DQ team had the right skill mix to take that work forward. It appreciated, however, that the DQ processes were still new and so it would take time to get to grips with them fully.
The committee received a live demonstration of the data quality dashboard. It was agreed that a highlight report on the dashboard would go to the next audit committee in May.
INTERNAL AUDIT – KPMG
Progress reportThe committee agreed to defer discussion on the draft internal audit strategic plan (2017-2022) and internal operational plan 2019/20 to the audit committee workshop in May.
Recommendations follow upThe committee noted that since the last meeting there was now a greater number of overdue recommendations. It considered whether the original completion dates set for the recommendations were unrealistic, particularly as some actions were complex, but KPMG was content with the timetabling on the whole. The chief finance and compliance officer assured the committee that the completion dates for all recommendations arising from the internal audit reviews would have been signed off at board director level. The committee reiterated its desire to see the level of overdue actions reduced to zero.
Internal audit reviews KPMG presented the findings from two of its reviews:
1. Data quality (DQ) The committee received the internal audit review on the underlying DQ and level of associated reporting of two of the trust’s performance targets: 4 hour A&E and 2 week cancer referral. KPMG had provided an overall assurance rating of ‘partial assurance with improvements required’ (amber-red) which was in line with management’s anticipated assurance rating. KPMG had recommended that the trust issue greater guidance on clock start and stop times, with training for staff as necessary.

FINAL
2. Business continuity The committee received the internal audit review of the business continuity arrangements in place at the hospital sites and the trust as a whole. KPMG had provided an overall assurance rating of ‘significant assurance with minor improvements required’ (amber-green) which was in line with management’s expectations. The committee noted that there was no significant issue to raise but there was a recommendation raised on ensuring staff were advised of the deadline for completing their business continuity plan templates.
Draft internal audit annual report and Head of internal audit opinion (HoIA opinion) The committee received the draft internal audit annual report and HoIA opinion of the trust for the period 1 April 2018 to 31 March 2019. The full HoIA report would be presented at the audit committee in May.
EXTERNAL AUDIT – PwC
• Progress report The director – PricewaterhouseCoopers (PwC) had discussed the report with the chief finance and compliance officer and the assistant director of finance – financial control in advance of the meeting to address a number of issues including the trust’s designation as a ‘high profile customer’ and the fees for the year end audit. PwC were continuing their focus on the trust’s accounts and accounting standards; the quality report, where it was noted that the council of governors would be asked to agree a local performance indicator at their joint meeting with the board on 26 March; and technical matters.
The chair sought assurance that there was no accounting issue yet to be resolved which could have a material impact on the year-end position. The director – PwC noted there had been a delay in receiving all the information the auditors required, but he was now more assured on a number of matters.
LOCAL COUNTER FRAUD SPECIALIST (LCFS) – RSM
• Progress report The committee noted the key messages arising from RSM’s work undertaken since January which included facilitating bespoke fraud and bribery training with the trust’s overseas visitor’s team and reviewing the first batch of National National Fraud Initiative (NFI) 2018 data matches (payroll and creditor to creditor) released by the Cabinet Office. It was noted that the chief finance and compliance officer and audit committee chair were now required to sign off the trust’s Self Review Tool. In terms of investigations, there had been six new referrals.
• Draft LCFS workplan 2019/20 A copy of the final workplan would go to the audit committee in May as this would allow time for additional detail in respect of the major risks to be included therein. The committee considered the plan needed to also reflect the evolution of the RFL Group; RSM agreed to liaise with the chair on that point prior to issuing the final version.
• Process for the annual assessment of LCFS effectiveness 2018/19 The committee approved the process for the annual assessment of LCFS effectiveness.
GOVERNANCE
• Group BAF The committee noted that the the BAF had been subject to a large number of minor edits,
primarily ensuring mitigations and actions were current.

FINAL
FINANCE
• Annual accounts: 2018/19 timetable and significant accounting issues for 2018/19
The committee received and noted the report.
• Cash flow forecast The committee received the report. However, the chair considered the committee’s ask was for a more forward looking view of the trust’s capital position, i.e. had the forecast captured all sources and applications for the next three years that the trust would need to pay for. She asked that the committee revisit the capital forecast, with a more detailed report, at the May audit committee. It was noted that cash plans were being built into the 2019/20 annual plan, as well as the savings the trust would need to achieve in order to deliver that year’s control total.
• Tender waivers The committee received and noted its regular tender wavers report.
• Losses and special payments The committee received its regular update on the trust’s losses and special payments, the majority of which related to private patient and overseas debt. There was provision for those losses in the trust’s accounts.
• Private patients unit (PPU) The senior manager – PPU was present for this item.
The committee supported the PPU’s ongoing liaison with its referral partner on the recovery of outstanding private patient debt owed to the trust.
The committee was broadly supportive of the proposal to offer credit packages to private patients via a credit provider as this could increase revenue and provide a service to patients while not exposing the trust to additional risk. The chair asked the chief finance and compliance officer and his team to assess the business case and contract, including ownership of risk, and provide a further update at the May meeting.
End

FINAL
1 Public – redacted
Minutes of the Audit Committee
18 January 2019
Present: Ms Mary Basterfield Non-executive director (committee chair) Ms Wanda Goldwag Non-executive director Ms Doris Olulode In attendance:
Non-executive director
Mr Peter Ridley Ms Lubna Dharssi Ms Lisa Marsh Mr Neil Thomas Ms Charlotte Goodrich Mr Kevin Lowe Ms Gemma Higginson (GH) Mr Mark Kidd (MK) Ms Natalie Ware Mr Jim Mansfield Ms Kelly Rank Ms Veronica Jackson
Chief finance and compliance officer Assistant director of finance – financial control Director of financial operations Head of internal audit – KPMG Senior manager – KPMG Director – PricewaterhouseCoopers (PwC) Management consultant - RSM Local counter fraud specialist / assistant manager – RSM Head of workforce – Royal Free Hospital (for item 120/18-19 only) Speaking up guardian (for item 120/18-19 only) Head of data quality - RFL (for item 121/18-19 only – via telephone) Committee administrator (minutes)
ACTION 116/18-19 APOLOGIES FOR ABSENCE Apologies were received from the following:
Members: No apology Attendees: Lynn Pamment - Engagement leader – PricewaterhouseCoopers The chair welcomed Doris Olulode, non-executive director (NED), Mark Kidd, local counter fraud specialist / assistant manager – RSM and Lisa Marsh, director of financial operations to their first meeting of the committee. Akta Raja, NED, would no longer attend the committee. The chair asked that the committee’s thanks to Ms Raja be noted. Mike Dinan, in his new role as commercial operations director, would also no longer attend.
117/18-19 DECLARATIONS OF INTEREST There was no interest declared. 118/18-19 MINUTES OF THE AUDIT COMMITTEE MEETING HELD 9 NOVEMBER 2019 The minutes were agreed as a true record of the meeting. ACTION LOG AND MATTERS ARISING 119/18-19 Review of the action tracker and matters arising. The chair was pleased with the pace at which the actions were bring processed, with the
majority either now closed or agenda items. In respect of the open actions, the following was noted:
Paper 10
FINAL
2 Public – redacted
• 105/18-19 – the target dates for the implementation of the actions arising from the internal audit review on General Data Protection Regulations (GDPR) had been updated and a revised copy of the report sent to the chair. It was agreed that the report would be circulated to the other members and attendees.
• 24/18-19 – the committee was asked to consider whether it required a follow up report in respect of well led. The chief finance and planning officer noted there there were elements arising from both the trust’s informal well led review and the CQC’s recent well led inspection that would need addressed at the audit committee. Emerging issues included the board assurance framework (BAF) and financial governance. The chair asked the chief finance and planning officer to consider those issues that warranted audit committee’s attention and provide a report at the March meeting. It was noted that the draft report from the CQC inspection was expected in February.
• 103/18-19 – KPMG sought clarity on the meaning of this action. The chair
responded that the committee was seeking to get a feel for how efficient the serious incidents (SI) process was considered to be by those staff flagging an SI, e.g. were the steps moving forward as they had hoped / expected. KPMG agreed to provide a one-page update addressing people’s perception of the SI process, and circulate to members and attendees by the end of the month.
There was no matter arising.
VJ PR KPMG
SPEAKING UP 120/18-19 Speaking up The committee welcomed Natalie Ware, head of workforce – Royal Free Hospital (RFH)
and Jim Mansfield, the speaking up guardian to the meeting. They highlighted that good progress was continuing to be made in respect of the trust’s processes around speaking up. There was currently 33 champions, comprising a number of surgeons and the deputy director for patient safety and risk (which helped forge closer links to concerns raised via Datix), plus a representative to cover Enfield Civic Centre. The head of workforce – RFH noted that the aim for the year ahead was to ensure that there was a structured and well managed speaking up process embedded across the trust. She added that the team would continue to address any gaps / hotspots, such as greater liaison with the trust’s BME staff and other such networks, in the aim of recruiting a diverse range of champions which were more reflective of the trust’s staff population. Ms Olulode had been appointed as the trust’s NED lead for speaking up and bullying and harassment (B&H) and she was looking forward to working with the team on those two matters. It was noted that [Redacted] new referrals had come through within the last few weeks, presumably as a result of the CQC inspection and the onset of the new year, but this was indicative of the good reporting culture across the trust. It was noted that few cases were related to B&H. The chair asked whether the team had adequate resources to manage an increased workload; the head of workforce – RFH considered those cases requiring full investigation would provide a challenge but added that this could be helped by having more managers involved in and trained on speaking up etc. She noted that all patient safety related cases were escalated immediately, plus some incidents could be referred to local management for follow up and as such required less resource.
Paper 10
FINAL
3 Public – redacted
The chair closed by noting the good progress made in respect of speaking up. She was pleased to see the champions’ involvement in workshops and other work arising from the trust videos focussing on values and behaviours at work.
ASSURANCE ITEM
121/18-19 Data quality This item was discussed last in the proceedings.
The trust’s head of data quality (DQ) joined the meeting via telephone. The chair started by noting that the current iteration of the report was a great improvement on what had been provided previously, and the strategy for improving DQ was much clearer. The head of DQ provided some context to the overdue recommendations, as highlighted by Ms Olulode, NED, earlier on in proceedings. When she started her role, the team structure was designed to be very data driven, rather than focussed on improving quality, and that had hindered the team’s progress in closing the actions. This was coupled with the team having been overconfident around the speed at which they could address and close the recommendations, plus the lack of a robust DQ strategy at that time. She assured the committee that the recommendations were now being actioned at pace, with oversight by her and the DQ steering group. The committee noted that Electronic Patient Record (EPR) had been implemented at Barnet Hospital and Chase Farm Hospital (CFH), and was due to be rolled out to the RFH. Ms Olulode, NED asked how that squared with a key principle of the DQ strategy for the consolidation of data captured on as fewer systems as possible. The head of DQ responded that there would be a single IT roadmap that would look to bring all IT systems under one place. The chair asked how the team would take assurance that the quality of the data was robust. The head of DQ noted that the DQ dashboards would address this and provide details on the key areas of concern such as recording timeliness etc. There would also be cross matching of data to highlight any inconsistences or inaccuracies. The dashboard was expected to be used by a number of people including the DQ team and operational teams. A full audit programme would also be implemented. The chair asked that reference to GDPR be included in the strategy. She also requested a live demonstration of the DQ dashboard at the next meeting.
KR, PR
INTERNAL AUDIT
122/18-19 Progress report
KPMG provided their regular progress update; they were on track with delivery, with three reviews left to complete by year end. Ms Olulode, NED, asked for background to the data quality recommendations as they were overdue and had been subject to a series of revised deadlines. The chair suggested that that point be addressed when the committee came to discuss the data quality report later on in proceedings [121-18/19].
123/18-19 Follow up recommendations The committee was pleased to note that the overdue recommendations were coming
down, and the chair stressed that the expectation was that all new recommendations be implemented by their due dates.
In terms of the new recommendations, the chair noted that a number were due for completion by end March 2019, which meant that month was overloaded, and asked
Paper 10

FINAL
4 Public – redacted
whether this was a realistic deadline. KPMG responded that they had no sense as yet that the actions were not running to schedule, and they had received a better response from staff so far. They added that a number of clients preferred to close off the previous year’s internal audit business at year–end.
At the chair’s request, the chief finance and planning officer and assistant director of finance – financial control agreed to send a note to all owners of the recommendations reminding them of the completion deadlines.
PR, LD
124/18-19 Internal Audit review – Medicines management: high cost drugs The review covered the overall process for the management of high cost drugs including
value for money. A rating of amber-green (significant assurance with minor improvement opportunities) had been awarded. KPMG highlighted that no significant issue had arisen and they were impressed with the process overall, adding that a reconvening of the high cost drugs panel in 2018 as a formal body had had a positive effect. In terms of recommendations, it was noted that formal definition of what constituted a high cost drug was required.
Ms Goldwag, non-executive director, asked about risks associated with purchasing drugs from outside of the UK post-Brexit. KPMG’s view was that this formed part of a wider system issue, and it was likely that trust’s role would be to simply follow the NHS guidance issued in line with that. [Paragraph redacted].
125/18-19 Internal audit review – Capital accounting and financing The review covered the capital accounting and financing processes and systems in place
across the trust. A rating of amber-green (significant assurance with minor improvement opportunities) had been awarded. KPMG considered that the trust was good at articulating its vision for its capital planning but was not clear on how that would be financed. Therefore, the four recommendations were KPMG’s view of the action that needed to be taken in order for the trust to get the assurance it needed on that.
The group chief finance and planning officer noted that a number of the actions for follow up were tied to the delivery of an operational plan and, therefore, he would liaise with KPMG on whether some of the deadlines could be relaxed.
The chair suggested that this be added as a risk on the Board Assurance Framework (BAF).
PR PR
126/18-19 Internal audit review – Financial controls The review focussed on the adequacy of the trust’s arrangements for accounts receivable,
payroll and general ledger controls. A rating of amber-green (significant assurance with minor improvement opportunities) had been awarded. The position was consistent with previous year’s reviews of the trust’s core controls as part of the year end audit, and on the whole the report presented was positive. It was noted that their testing had shown that a number of payroll amendments and leaver forms were submitted to payroll after the cut-off date. Consequently, KPMG had recommended that the guidance for line managers be updated so it was clear that all such changes must be received by the deadline.
The chair noted that KPMG’s sampling had identified a credit note having been prepared and authorised by the same individual. KPMG responded that this was due to a new member of staff who was not aware of the correct sign off process and had therefore attempted to correct their own invoicing error. KPMG had recommended that as part of the induction process in the accounts payable team, staff were clearly made aware of all the processes where segregation of duties was required.
Paper 10

FINAL
5 Public – redacted
127/18-19 Internal audit review – Retention strategy
The review focussed on the design and governance of the trust’s retention strategy at a group and hospital site level. A rating of amber-green (significant assurance with minor improvement opportunities) had been awarded. KPMG highlighted that there was no significant issue identified, nor any high priority recommendations for follow up, but they did raised two key points for noting. Firstly, there was a lack of consistency in the format and content of the site’s staff experience and retention plans, and secondly, the less formal nature of reporting at a divisional level meant that in some instances progress on actions was not reported upwards to the heads of workforce. Both of those issues were subject to medium priority (amber) recommendations in the report.
The chair asked whether KPMG had identified any good retention initiatives across its NHS client base which the trust could look to replicate. KPMG considered this was not the case, adding that the trust was leading in terms of best practice.
It was agreed that this review would be taken through the local executive committees (LECs).
VJ
EXTERNAL AUDIT 128/18-19 Audit committee’s views on fraud In its external audit plan 2018/19, PwC asked the audit committee for its views on fraud.
The committee was asked to review its proposed response; this was agreed subject to the following updates:
• state that Ms Olulode was the appointed NED for speaking up and B&H; and • clarifying that the committee received updates from local counter fraud at
the meetings it was required to attend as per its agreed annual workplan, not all audit committee meetings.
The director – PwC asked the committee whether there were any specific, key areas they would want external audit’s focus on as part of their year-end audit, adding that it would be helpful to be aware of those ahead of time. It was agreed that this would be discussed at the March committee meeting.
VJ PR, MB
LOCAL COUNTER FRAUD SPECIALIST (LCFS)
129/18-19 Progress report and Notice Fraud December 2018
LCFS had undertaken a local proactive exercise (LPE) in respect of overseas visitors. [Paragraph redacted]. The actions arising from the LPE would be added to the management action tracker, which was currently showing zero outstanding actions. It was noted that the management consultant – RSM and chief finance and compliance officer were in discussion about two planned ‘prevent and deter’ proactive exercises utilising the results from the fraud and bribery risk assessment. The management consultant – RSM noted that a greater number of referrals were being made, and from different areas across the organisation, which was positive in terms of the trust’s reporting culture. An update was provided on a number of cases:
• [Redacted] • [Redacted]
Paper 10

FINAL
6 Public – redacted
• [Redacted] The management consultant – RSM highlighted that 10% of trust staff, as per Counter Fraud Authority’s guidance, were required to complete the online fraud awareness survey but getting the numbers up was challenging. The chief finance and compliance officer agreed to flag this requirement with staff and ask that they participate. In response to a question from the chair, it was noted that RSM has not attended any LEC meetings thus far. RSM were keen to do that and would build that into their 2019/20 workplan.
PR
GOVERNANCE
130/18-19
Group board assurance framework
The committee approved the revised data quality risk (G-022).
The chair highlighted that the recent clinical standards and innovation committee, in reviewing their assigned section of the BAF, had noted a number of risks were without actions and timescales, plus a number of timescales had long passed. The chief finance and compliance officer noted that group executives had been asked to review and update their allocated risks as soon as possible.
131/18-19
Process for the annual review of audit committee effectiveness
The committee approved the process for the annual review of audit committee effectiveness 2018/19.
132/18-19 Clinical standards and innovation committee minutes – 17 September and 15 November 2018
The minutes were noted.
133/18-19 People and population health committee minutes – 27 September 2018
The minutes were noted.
FINANCIAL 134/18-19 Wholly owned subsidiaries(WOS) financial governance The chief finance and compliance officer noted that the report had aimed to address the
changes requested at the previous meeting. The aim was to not overcomplicate the process; as such the group audit committee would review the external audit of WOS in conjunction with the RFL end of year external audit, and recommend the accounts / audit to the trust board. Where appropriate, the managing directors of the WOS would be asked to attend the audit committee to review the results arising out of the external audit work. In addition, all WOS internal audit work would be reported into the audit committee. The committee noted the update but the chair requested some further clarification in respect of the following was needed:
• the process for signing a revenue contract, and • the delegation of authority for revenue contracts
The report would be updated accordingly and presented at the next meeting.
MD, PR
Paper 10

FINAL
7 Public – redacted
There was discussion around the set-up of the trust’s decontamination service [Section redacted].
135/18-19 Cash flow forecast The cash position looked favourable due, in part, to the receipt of funds from the sale of
Parcel B land; this meant the trust would not need to draw down revenue loans until the last quarter of the year. It was noted that the trust board in December had agreed to draw down two capital loans in 2018/19 for the CFH redevelopment. The chief finance and compliance officer assured the committee that NHS Improvement was well sighted on the trust’s financial position.
136/18-19 Tender waivers The committee received and noted its regular tender wavers report. The chief finance and
compliance officer noted that the report showed those waivers below £90k. He was reviewing whether there was a sufficient level of approval for those contracts of lesser value.
137/18-19 Losses and special payments The committee received its regular update on the trust’s losses and special payments, the
majority of which related to bad debts, private patients and overseas debt.
138/18-19 Private patient debt write-off
No update was given. This would be rolled over to the next meeting. LD
ANY OTHER BUSINESS 139/18-19 Production of board and committee papers The report was noted. 140/18-19 Review of the forward planner – to agree agenda items for the next meeting The following would got to the March meeting:
KMPG
• Head of internal audit opinion • Final three internal audit reviews • Internal audit draft annual plan 2019/20 • Regular internal audit recommendations update
FINANCE
• Annual accounts 2018/19 timetable • Accounting for RFLPS and latest position on each of the subsidiaries • Capital funding forecast • Accounting update covering unusual items for 2018/19 year end
GOVERNANCE
• Audit committee annual workplan RSM
• LCFS draft annual plan 2019/20 OTHER
KPMG LD PR RSM PR, KR
Paper 10
FINAL
8 Public – redacted
• Data quality update (now a standing item) The chief finance and compliance officer would bring a paper on Freenet 2 (new trust intranet) financial implications.
PR
141/18-19 PRIVATE MEETING BETWEEN AUDIT COMMITTEE MEMBERS AND AUDITORS AND COUNTER FRAUD OFFICERS
No meeting was required on this occasion.
Date of next meeting: 15 March 2019, 1130 – 1400, group HQ boardroom, first floor, Anne Bryans House, 77 Fleet Road, NW3 1QH
Paper 10

Paper 11
FINAL
Clinical standards and innovation committee (CSIC) report
Executive summary
To follow is an update from the CSIC meeting held 10 April 2019 on key discussion items and agreed actions. This was a shorter meeting with a focussed agenda looking specifically at the National Clinical Audit Outcomes 2018 and the management of serious incidents.
Action required
The committee is asked to note the report.
Meetings where this report has been discussed previously
Meeting Date Decision n/a n/a n/a
Board/GEC/LEC/committee goals
GOALS BAF
risks
Demonstrable organisation health (group governance) G042/044
CQC standards impacted Well led
Financial/business implications N/a
Equality analysis No identified negative impact on equality and diversity
Compliance impact
Report from Dr Chris Streather, chief medical officer Author Veronica Jackson, group committee administrator Date 15 April 2019
Report to Date of meeting Attachment number
Trust board 1 May 2019 Paper 11

Paper 11
FINAL
National Clinical Audit (NCA) Outcomes 2018
The committee noted that there were a number of areas of ‘poor performance’ that required further focus. Many of those, on the whole, related to process issues but there were some indicators that would impact on patient care. The chief medical officer noted that responsibility for the areas of poor performance would be pushed down to the divisional leadership teams as the aim was to move away from a central team overseeing the improvement actions required. The committee agreed with that approach.
It was suggested that the committee may want to be sighted on the priority areas for data quality improvement to ensure that they were the correct ones from a clinical audit / clinical decision-making perspective. The chief medical officer agreed to take this forward.
The chair was keen to ensure the committee did not lose sight of the improvement work arising from the NCA 2018. It was agreed that the associate medical director – clinical performance would be asked to undertake a follow up report on the processes reviewed and benefits identified at divisional level for reporting back up to CSIC.
Serious incidents (SIs)
At its March meeting, the committee requested a review be undertaken of the trust’s current SI governance and management processes, specifically whether there was any way they could be reengineered to work better, help take the burden off staff and improve the trust’s SI position overall. Proposals in respect of the following were provided.
• Management of SIs
It was recommended that the trust’s current open SIs and overdue reports be prioritised for action using a risk stratification process, i.e. low, medium or high risk. In order to manage the quality governance resources more effectively to address the significant number of SIs under investigation, a number of other approaches were also being trialled alongside the re-prioritisation. This included having the safety incident review panels take a more critical approach to determining whether an incident met the SI criteria; reviewing the trust’s incident policy; and improving the investigation report template to give greater focus on timelines and actions rather than detailed narrative.
The committee agreed it was sensible to prioritise SIs as they came in using the risk stratification process, as this would ensure the prioritisation of those incidents that would offer the greatest level of benefit to / learning for the trust. However, it recognised that good clinical input and brevity would be needed to ensure this was effective. In addition, the chair stated he would want to understand at what point the committee could be comfortable that the SI position was at a satisfactory level and was sustainable. He requested a practical definition was required of what ‘satisfactory’ and ‘good’ would look like across all parameters of this work.
The committee also considered it was important to ensure that there was a level of control / management around those incidents not deemed as SIs, and having a culture whereby staff maintained accountability for those.
• Management of unapproved incidents
The committee noted that the site quality governance teams were working hard to reduce the high volume of unapproved incidents on Datix, a large number of which were overdue for approval, but this was challenging, particularly given the 12% increase in incident reporting when compared to the previous year. Therefore, it was proposed that a batch-closure of

Paper 11
FINAL
incidents by the safety informatics and Datix team be undertaken to enable timelier incident management. Mitigations were in place, namely an agreed set of exclusion criteria, to prevent a SI from being missed. The aim was to do the batch closure in three phases and see if there were any concerns raised as the team progressed through each stage.
The committee considered this was a sensible approach but did seek assurance on a number of fronts; that the new process would be maintained in order that the trust did not find itself in the same position later on, that the batch closure method would not lead to a lack of ownership of no / low harm incidents by local staff, and that governance processes were in place to ensure there was minimal risk that an incident could be assigned incorrectly which meant an SI could be missed.
In closing, the committee approved the recommendations outlined in the report, namely:
• Agreed the proposed action for batch closure. • Agreed the exclusion criteria for batch closure. • Agreed the timeframe for batch closure. • Agreed the future process for batch closure. • Agreed that the deputy director – patient safety and risk would keep a log of any
concerns raised at each stage of the process, with a view to looking at making further improvements, as necessary, thereafter.
The chair thanked the deputy director – patient safety and risk and her team for their hard work on reviewing the processes around the management of serious incidents and unapproved incidents.
End.

Paper 12
FINAL
Report from group services and investment committee
Executive summary
To follow is an update from the group services and investment meeting held 11 April 2019 on key discussion items and agreed actions.
Disposal of Queen Mary’s House (QMH) and Plot D The committee supported the full business case (FCB). It recommended that the trust board be asked to approve the FBC at its confidential board meeting on 1 May 2019.
Royal National Throat, Nose and Ear Hospital (RNTNE) The committee approved the proposed course of action for the disposal of residual land on the RNTNE site.
RFL wholly owned subsidiaries (WOSs) o The committee received a report outlining the lessons learned from the setting up of
the trust’s Royal Free Property Services Limited WOS (RFLPSL) and the Royal Free Dispensing Limited WOS (RFLDi) which were now live.
o The committee considered additional information needed to be sought before it could take a decision on whether to create a holding company. This would be discussed again at a future meeting.
o The committee agreed not to activate RFL Decontamination Limited WOS (currently dormant) at this time.
Corporate shared services programme The committee received an update on the current state of and the proposed direction on the consolidation of the trust’s corporate and back office support services. It approved the strategy and direction and asked that it be kept informed of progress.
Financing and leasing decisions, plus capital plan 2019/20 The committee noted the approach taken by the trust in respect of its financing and leasing decisions laid down in the Standing Financial Instructions. It also received the capital plan for 19/20 which had been approved by the trust board.
• Routine reports The committee received routine reports in respect of:
o Pharmacy WOS o RFL property services limited WOS
Report to Date of meeting Attachment number
Trust board 1 May 2019 Paper 12

Paper 12
FINAL
o Decontamination WOS, o Health Services Laboratory – investor perspective o Procurement / Other commercial
• Group goals and Board Assurance Framework (BAF) risks The committee approved its allocated goals and the current risk scores. It also received verbal updates in respect of its goals that were not covered by the items on the agenda. It was agreed that a report on the goal, ‘Chase Farm Hospital deficit eliminated’ would be taken to the May meeting.
Action required
The committee is asked to note the report.
Meetings where this report has been discussed previously
Meeting Date Decision n/a n/a n/a
Board/GEC/LEC/committee goals
GOALS BAF risks
Demonstrable organisation health (group governance) G042/044
CQC standards impacted Well led
Financial/business implications N/a
Equality analysis No identified negative impact on equality and diversity
Compliance impact N/a
Report from Wanda Goldwag, non-executive director and chair – group services and investment committee Author Veronica Jackson, group committee administrator; Alison Macdonald, board secretary Date 17 April 2019

Paper 13
Final
Report from the people committee meeting held 28 March 2019
Executive summary
The chair wanted to ensure the people committee meetings added real value and requested this first meeting consider how it could do that to best shape the ‘people’ agenda. All agreed that there was a lot of good work going on across the trust but the committee should look at identifying the top priorities across the organisation and focus its efforts there.
Following a lengthy discussion, it was clear that there were a number of themes that could accelerate the trust’s quality work and would be the most impactful. Those included bullying and harassment, such as the ‘no bullying no bystanders’ videos and links with the trust’s World Class Care values; the trust’s training and development agenda; diverse interview panels; and staff health and well being.
It was agreed that a brief laying out the agreed key themes for the committee’s focus would be drafted for consideration at a future meeting. The chair would also consider what needed to be reported into the committee in respect of speaking up (whistleblowing).
As the discussion on the committee’s future focus covered a number of reports on the agenda, it was agreed that those concerned would be noted and verbal updates would be given on a select number of reports only.
Verbal updates
Group goals and BAF risks aligned to the committee A decision had yet to be taken on whether the education goal should move from clinical standards and innovation committee to the people committee. If agreed, the deputy director – education would be invited to join the committee.
Smoking cessation presentation The committee noted that the trust was refocussing its efforts on smoking cessation and having a ‘smoke free’ environment, identifying the achievements made previously and areas for further action. Action was also being taken to try and reinvigorate smoking activity across the trust’s other sites as it was predominately on the RFH site. The committee heard about the impact of smoking on the trust, where it was noted that the RFL was seeing over 3,000 patients a year that smoked, and on the patient. The trust was also mindful of the impact of smoking on its workforce, including those staff that smoked themselves. Ultimately, however, there was recognition that smoking was an addiction and should be treated as such.
The committee noted the achievements made thus far; that included the introduction of the national referral system for referrals to community stop smoking services and successful
Report to Date of meeting Attachment number
Trust board 1 May 2019 Paper 13

Paper 13
Final
delivery on the healthy behaviours CQUIN. There were areas for improvement, however, and one of the greatest challenges was enforcing a truly smoke free site. It was agreed that the message that the trust was a smoke free zone needed to be reinforced and patient’s expectations managed.
It was suggested that the Oracle Learning Management system could be used to capture the number of staff that had undertaken the smoking cessation related training - that way the trust could report on the data and map it against demographics etc.
Organisational development and leadership The committee recevied an update in respect of the trust’s organisational development and leadership programme of work. It noted that resourcing within the OD team was under review and that the group executive committee had recently agreed to the centralisation of all courses and conference budgets under the workforce and organisational development team.
Local patient and staff experience and workforce committees The site representatives highlighted the key issues for the committee’s noting.
Reports noted
• Gender pay gap report 2018 • People goals update • Interim workplan implementation plan: emerging priorities and actions • Annual national staff survey 2018 • Bullying and harassment update • Revalidation and maintaining high professional standards issues • Guardian of safe working reports – Q3 2018-19 • Quality account – proposed priorities for 2019/20 • People committee terms of reference
Action required
The board is asked to note the report.
Meetings where this report has been discussed previously Meeting Date Decision n/a n/a n/a
Board/GEC/LEC/committee goals
GOALS BAF risks
Demonstrable organisation health (group governance) G042/044
CQC standards impacted Well led
Financial/business implications N/a
Equality analysis No identified negative impact on equality and diversity
Compliance impact N/a
From from James Tugendhat, non-executive director and chair of the people committee Author Veronica Jackson, group committee administrator Date 18 April 2019

Paper 14
Page 1 of 3 DRAFT
Use of the Royal Free London NHS Foundation Trust seal 2018/19
Executive summary
The trust’s standing orders require an annual report to the board on the use of the trust seal. The report should contain details of the date of sealing, the seal number, and the description of the document. The table below lists the documents to which the seal has been affixed within the last year.
Action required
The board is asked to note the report.
Meetings where this report has been discussed previously This is an annual update that goes to each trust meeting in April. Meeting Date Decision
Board/GEC/LEC/committee goals
GOALS BAF
risks
Demonstrable organisation health (group governance) G042/044 0
CQC standards impacted N/a
Financial/business implications N/a
Equality analysis Any adverse impact on equality and diversity has been remedied or escalated
Compliance impact N/a
Report from Dominic Dodd, chairman and Caroline Clarke group chief executive
Author(s) Alison Macdonald, board secretary
Date 16 April 2019
Report to Date of meeting Attachment number
Trust Board 1 May 2019 Paper 14

Paper 14
Page 2 of 3 DRAFT
Use of the Royal Free London NHS Foundation Trust seal
Date Item no.
Item
01/05/18 490 Royal Free London NHS Foundation Trust and GE Capital Equipment Finance Limited and CFES Limited-Funder’s Direct Agreement.
01/05/18 491 NHS Master Lease Agreement and Conditions of Contract for the lease of goods – CFES Limited and Royal Free London Foundation Trust.
01/06/18 492 Lease of premises at part of Finchley Memorial Hospital, Granville Road, North Finchley, London, N12 0JE for Community Health partnerships Limited and Royal Free London NHS Foundation Trust regarding breast screening service.
25/06/18 493 Royal Free London NHS Foundation Trust and Royal Free Property Services LTD-Project Agreement.
25/06/18 494 Royal Free London NHS Foundation Trust and Property Services Ltd-Strategic Partnership Agreement.
06/07/18 495 Royal Free London NHS Foundation Trust, RFL Property Services Limited and Integrated Health Projects - Novation of building contract relating to a development of the site of the Chase Farm Hospital.
20/07/18 496 Deed of Variation to the Project Agreement dated 12 February 1999 relating to managed technology services between Metier Healthcare Limited and Royal Free London NHS Foundation Trust.
20/07/18 497 Deed of Variation to the Project Agreement between the parties dated 12 February 1999 for the Soft FM Services between Metier Healthcare Limited and Royal Free London NHS Foundation Trust.
16/08/18 498 Section 106 Agreement Under the Town and Country Planning Act 1990 for Unit 2-3 Chalkmill Drive Enfield between the Mayor and Burgesses of the London Borough of Enfield Barclays Nominees (George Yard) Limited.
30/08/18 499 Supplemental Agreement to a Deed of Surrender of Part of Parcel B Chase Farm Hospital.
13/08/18 500 Lease of Substation (Rowland Hill Street) 26/09/18 501 Settlement Agreement between Royal Free London NHS Foundation
Trust and Utility Healthcare Energy Services. 08/10/18 502 Contract of Refurbishment of the Air Handling Units in the plant room,
AHU 71, 72, 73 &74 at the Royal Free between Capri Mechanical Services Ltd and the Royal Free London NHS Foundation Trust.
08/10/18 503 Gene Therapy Lab Modifications-UCL Biobank, contract between Royal Free London NHS Foundation Trust and Logan Construction (South East) Limited.
07/11/18 504 Contract for the Soft Facilities Management Services between the Trust and the contractor at the Chase Farm Hospital Site, Parent Company Guarantee.
16/11/18 505 Deed of Variations Lease for Chalkmill Drive. 17/11/18 506 Deed of Variation of Agreement for lease in respect of 60 Whitfield Street,
London W1. 17/11/18 507 Lease of 60 Whitfield Street, London W1. 21/12/18 508 Transfer of Electrical Substation in the North Side of Lavender Hill,
Enfield. 21/12/18 509 Release of part of the land from a registered change – electricity
substation on the north side of Lavender Hill, Enfield. 05/02/19 510 Mary Rankin- Ground Floor Refurbishment at St Pancras Hospital.

Paper 14
Page 3 of 3 DRAFT
05/02/19 511 Royal Free London NHS Foundation Trust & CBRE Managed Services Ltd - Parent Company Guarantee.
05/02/19 512 Royal Free NHS Foundation Trust and CBRE Managed Services Ltd – Framework Agreement for Hard FM Management Services.
05/03/19 513 Royal Free London NHS Foundation Trust and Telefonica UK Limited – Deed of Variation.
05/03/19 514 JCT Intermediate Building Contract 2016 for Breast Clinic Project, Royal Free London NHS Foundation Trust.
08/03/19 515 Collateral warranty between Edina UK, Royal Free NHS Foundation Trust and EDF Energy Services Ltd.
09/04/19 516 Royal Free London NHS Foundation Trust and WH Smith Hospitals Limited and WH Smith Holdings Limited – Lease for the convenience store.
09/04/19 517 Royal Free London NHS Foundation Trust and WH Smith Hospitals Limited and WH Smith Holdings Limited – Licence for alterations relating to Marks and Spencer retail unit.
09/04/19 518 Royal Free London NHS Foundation Trust and WH Smith Hospitals Limited and WH Smith Holdings Limited – The Marks and Spencer store.
09/04/19 519 Royal Free London NHS Foundation Trust and WH Smith Hospitals Limited and WH Smith Holdings Ltd – Deed of Surrender for the convenience store, RFH.
09/04/19 520 Royal Free London NHS Foundation Trust, RFL Property Services Limited, EDF Energy Customers Limited, IMTECH Low Carbon Solutions Limited – Deed of Novation for the provision of energy and energy management facilities at Chase Farm Hospital.
End