· web viewmodels of change in care homes . final. report . december . 201. 4. written by . liz...
TRANSCRIPT

Models of change in care homes
Final report
December 2014
Written by Liz Burtney, Danni Teahan, Davina Figgett, Paul Buchanan and Karen StevensPublished by Thomas Pocklington Trust
i

Models of change in care homes Published by Skills for Care, West Gate, 6 Grace Street, Leeds LS1 2RP www.skillsforcare.org.uk© Skills for Care 2014Copies of this work may be made for non-commercial distribution to aid social care workforce development. Any other copying requires the permission of Skills for Care.Skills for Care is the employer-led strategic body for workforce development in social care for adults in England. It is part of the sector skills council, Skills for Care and Development.
ii

Table of contents
List of abbreviations......................................................................................................... ivAcknowledgements...........................................................................................................viExecutive summary.........................................................................................................vii1. Background and research approach......................................................................12. What is the ‘traditional’ model of care?.................................................................43. What does future care look like?..........................................................................114. How can we make the shift?..................................................................................145. Models of change in care homes..........................................................................186. Characteristics of positive culture care homes...................................................287. Benefits of the changes that have been made....................................................538. What do staff need to know and understand about visual impairment to be
able to offer person-centred care and assess person centred risks?...............579. Conclusions and learning for others....................................................................6010. References..............................................................................................................65
iii

List of abbreviations
ACP Advanced care planning
ADASS Association of Directors of Adult Social Services
BIS Department for Business, Innovation & Skills
CAF Common Assessment Framework
CQC Care Quality Commission
DOLS Deprivation of Liberty Safeguards
ECM Every Child Matters
ED Electronic documentation
EPaCCS Electronic Palliative Care Co-ordination systems
ELCQuA End of Life Care Quality Assessment
FaNs Community Friends and Neighbours
FRS Flexible Response Service
GIRFEC Getting it Right for Every Child
HSCIC Health and Social Care Information Centre
HTS Holding the Space
ILC UK International Longevity Centre, UK
IRISS The Institute for Research and Innovation in Social Services
JRF Joseph Rowntree Foundation
NCHR & D The National Care Homes Research and Development Forum
NDTI The National Development Team for Inclusion
NEoLCP National End of Life Care Programme
NHS National Health Service
NHS NIHR National Institute for Health Research
NICE National Institute for Health and Care Excellence
NSA National Skills Academy
POWR The Principles of Workforce Redesign
RCN Royal College of Nursing
REA Research evidence assessment
iv

SAB Safeguarding Adults Board
SCIE Social Care Institute for Excellence
SfC Skills for Care
SIRCC Scottish Institute for Residential Child Care
UNCRC United Nations Convention on the Rights of the Child
v

Acknowledgements
The Thomas Pocklington Trust funded this research and the authors would like to thank Pamela Lacy for her support in conducting the REA.
In addition, the authors would like to acknowledge the following for their help and support at different stages of the work:
George Coxon Skills for Care Area Managers Skills for Care Area Officers
The authors would also like to give special thanks to the following organisations for participating in the qualitative stage of the research, all of whom have been extremely helpful and generous with their time:
Aylsham Manor, Aylsham Wren Hall, Nottingham Sefton Hall, Dawlish Tendring Meadows, Essex Greenwich Gardens, Derby
vi
Executive summary
Introduction This report was commissioned by the Thomas Pocklington Trust (TPT) to investigate models of change which could improve the quality of care provided by care homes in the UK. The rapid evidence assessment (REA) therefore set out to identify published models of change and their impact on the quality of care. In addition, the REA sought to identify key characteristics for successful change in care homes, in order to extract learning for others. Finally, the REA touched on the information needed to offer person-centred care to people with visual impairment. The work comprised a rapid evidence assessment plus primary research with 5 care homes.
Drivers for changeTraditionally care has been described as task focused, inflexible, lacking a sense of purpose and institutionalised. Policy, the quality improvement agenda, changes to regulation and registration, and current public perception of care were all identified as drivers for change. The model of future care highlighted by some authors, and to a large degree exhibited by those care homes involved in the consultation, includes a focus on relationships, quality of care, flexibility and engagement. Older people themselves have identified characteristics which are important for care as being continued freedom of movement and ability to continue with individual routines, a positive environment and a sense of belonging to a community rather than residing in a home.
Making the shiftThere is a lack of evidence examining models of change in care homes, and even less information available on the effectiveness of change. However, management literature would suggest that different levels of change could occur, e.g. developmental, transitional and transformational. Various theories have been formulated to conceptualise change and could be applied to care homes, however, we did not identify literature that discussed change in care homes at this theoretical level. Literature identified was more likely to talk about the practical aspects of change, for example, tools to help with change or characteristics of change facilitation.
vii
Models of change in care homesIn terms of models which care homes could adopt to change culture and service delivery, the REA identified: The Butterfly Service, a programme specifically aimed at homes working with people
with dementia. The Eden Alternative, aimed at eliminating boredom, loneliness and helplessness for
care home residents. Social pedagogy, drawing on European experiences to improving relationship-based
care. My Home Life, a UK based model of care underpinned by evidence and growing in
popularity. Dignity in care, less of a model per se but a policy focusing on transforming services. The Devon Kitemark, has been based on evidence and shared between local care
home providers in the area to drive up quality. 360 Forward, a programme allowing care homes to benchmark current services, agree
change and review progress.
‘Ingredients’ for change in care homes From the literature, a number of characteristics were identified that appear to be associated with change within an organisation: Person-centred and relationship-based care A positive organisational culture of care Well trained staff Joint decision-making and participation Strong leadership and supportive management A positive physical environment.
These characteristics were also discussed in the consultation with managers and staff. Participants in the consultation process particularly highlighted the need for strong leadership and participation from staff and residents as key to introducing and sustaining change.
The impact of changeThe evidence of impact, either positive or negative, was very limited. However some formal evaluation did indicate positive outcomes for residents’ physical and mental health, as well as improvements in staff satisfaction borne out through a reduction in staff turnover. Anecdotal evidence from the literature and our consultation with care homes summarised below, gives some insight into the potential benefits of change, although these should be treated with caution.
viii
Potential benefits for residents included: flexibility greater choice a more creative and stimulating environment a sense of purpose something to look forward to in their day scope for individual focused approaches.
Potential benefits for families included: a sense of trust and confidence in the care being delivered which allowed them to
concentrate on other aspects of their lives.
Potential benefits for staff included: job satisfaction autonomy increased career and development opportunities a more positive working environment increased confidence improved staff morale
Potential benefits for employers included: more stability in the workforce improved reputation locally.
Transferrable learningFrom the REA there was limited information on the theory and impact of models of change specific to residential care. However, the consultation did identify some examples of models of change that are being implemented in the sector. There is a need to ensure that current models continue to extend and that practice is reviewed. There is also a need to continue to plan evaluations and share findings with other providers.
Beyond models of change themselves, and focusing on characteristics that can facilitate change, transferable learning did emerge across a number of themes, and is described below.
Care homes will have to consider the implications of new regulations, policy and commissioning processes within a local context. However, there is every indication that the drive to deliver person-centred care will continue and failure to review their existing practice in line with these external changes is likely to impact on the quality of care provided within care homes.
ix

The importance of involving stakeholders (e.g. staff, residents, family members) when introducing and sustaining change was evident. In particular the consultation illustrated the need to involve staff through effective communication, joint working to identify and understand the need for change and teamwork to introduce and maintain change. While the literature focuses mostly on processes rather than impact, there was some evidence that when staff are involved they feel more supported and valued. This has potential benefits for staff satisfaction and staff recruitment and retention. Care homes considering change should ensure that high levels of engagement are in place to ensure sucess.
Strong leadership was a consistent theme throughout the research. Without this, the process of change faces more challenges and may not be driven through or sustained. This was a clear message from the consultation, where the need for a champion at the top of the organisation, someone with a clear vision reflecting local market needs was highlighted. Care home owners should ensure that managers and leaders are supported developed and committed to the change process, and that resources are available to make change happen.
There was evidence from the REA and the consultation that improvement in the physical environment is a practical move toward change that can positively impact on care homes. Care homes considering changes could use existing tools to audit the current environment, taking on board views from staff, residents and families. This would help identify where changes could be made now or in the future to encourage a ‘homely’ atmosphere and facilitate person-centred attention to detail.
Care homes wishing to make changes should seek out learning from others but there is more work needed to consider how best to make the connections between innovators and good practice and employers who are ready to make changes. More information is needed on the impact of person-centred care in care homes on organisational delivery, management, staff, residents and families. In addition, some work to examine the cost benefit implications or the social return on investment or social value of change might help care home owners and managers consider the case for differing models of change depending on their needs.
x
1. Background and research approach
1.1 Purpose of this research This report was commissioned by the Thomas Pocklington Trust (TPT) to investigate the scope for improving the quality of care provided by care homes in the UK and focused on the following questions (see Appendix 1 for further details): What are the key characteristics of ‘good practice’ in care homes? What models of change have been applied in care homes? To what extent have these models of change been effective in improving predefined
outcomes? What key learning can be extracted from the evidence to inform thinking of
stakeholders? What do staff need to know and understand about visual impairment to be able to offer
person-centred care and assess person-centred risks?1
Given the breadth of the questions a rapid evidence assessment (REA) was undertaken between July and October 2014. This was based on: Secondary or review level evidence from international and national literature Primary level evidence from the UK on effective practice and characteristics of good
practice Identified published and grey literature from a range of online sources.
In addition to the REA, the research involved primary research with frontline practitioners and managers in 5 care homes which will be referred to as the ‘consultation’. This focused on their experiences and extractable learning for others.
1.2 Methodology for the rapid evidence assessment
Identification of evidence Agreed search terms reflected the breadth of the key REA questions and were categorised into risk management and relationships, outcomes, characteristics of success and effectiveness (see Appendix 2 for more detail). International systematic reviews and literature reviews, primary studies from the UK, and, where appropriate, opinion papers published in the English language during or after 2000, were considered for inclusion in the REA. Reports on medical interventions and medication management were excluded.
1 The researchers investigated whether there was any literature that suggests the effective models of change vary, depending on the characteristics of older people, including sensory deprivation.
1

Quality assessment The REA-approach identified papers were checked for relevance and, if they were a review or a primary study on effectiveness, were assessed for quality (see Appendix 2 for further detail). However, while attention has been paid to the quality and applicability of the research selected for inclusion, there remain some limitations to the REA, described below.
Inclusion in the report The REA incorporated a broad range of search terms and areas for consideration (see Appendix 2 for the key terms used). Following critical quality assessment, key findings were extracted and synthesised by topic for potential inclusion. However, in areas where findings from the synthesised evidence were inconclusive, weak or lacked transferability across to the residential care setting for older adults, the decision was made not to include them in this report. The purpose of this report is to clearly focus on what we can learn from other settings so papers where direct learning was absent were excluded.
Strengths and limitations of the REA The methods used were transparent, systematic in approach and replicable. The approach design included a critical appraisal of the strength and quality of the evidence. The consultation with staff and managers in care homes added to this evidence base and sought to both highlight similarities with the body of evidence and act as a sense check for the findings from the REA.
However, the reader should note that reflecting the rapid approach adopted, this REA does not provide detailed descriptions of all aspects of care but rather focuses on effective or promising approaches that might have transferable lessons for others.
Authors have noted that rapid evidence assessments have some limitations and challenges (Thomas et al. 2013). The timescale and resources available for the research meant a pragmatic approach was adopted to scope out the literature using comprehensive searching but the REA does not claim to present an exhaustive analysis of all aspects of the culture of care.
Furthermore, there was an absence of robust evidence of the effectiveness of approaches. This was noted by other authors (Szczepura et al. 2008) and while there has been some additional research since then, the evidence base remains limited.
It is important to note that much of the literature concentrates on describing and discussing needs and/or flaws in the services rather than documenting the evidence on effectiveness of approaches to address some of the concerns raised. Where limited evidence was available one of the major challenges was identifying the essential ‘ingredients’ of the models and translating these to residential care settings and client groups.
2

A further challenge for the care sector is achieving the balance between quality care and bottom-line efficiencies. The focus on measurable outcomes as an indication of effectiveness does not necessarily reflect the complex care within residential settings that require softer, more qualitative measures.
1.3 Methodology for the primary research The primary research with care homes was included to complement the findings from the REA. The purpose of the study was to hear more about the views and experiences of front line staff and managers who had been through a process of change in a care home setting.
Care homes were identified through various routes: findings from the REA – a number of approaches were identified through online
searching feedback from Skills for Care locality managers who were able to identify a range of
care homes who had undergone change or were renowned for having a positive culture of care
input from specialists working in the care home sector.
Selection of the care homes to be included was a joint process between Skills for Care and TPT. From shortlist of 20 care homes, five were selected on the basis of the approach to change, approach to care delivery and organisational size.
Once selected, the care homes were individually approached and recruited. Staff and managers were sent a participant information sheet which explained the purpose of the study and gave information about Skills for Care. In total 10 managers and 10 staff were interviewed.
The interviews were conducted by Skills for Care staff. Managers were interviewed separately and frontline staff in pairs. Full consent was attained before each interview. Interviews were recorded and analysed for inclusion in the report. A separate technical report is available for this stage of the work. This is referred to as the ‘consultation’ in this report.
3
2. What is the ‘traditional’ model of care?
OverviewThe perception of current care provision is ‘traditional’ care which is task-focused and not person-centred. How far this perception reflects reality is not documented but it is fair to say that policy is constantly driving for person-centred care, choice, and flexibility as far as possible. However, this is in the face of budgetary constraints, which mean that commissioners and service providers have to think differently about how services are sustained and improved.
New regulations coming into place are another consideration for service providers and commissioners with a strong focus on leadership and effective care. However, regulation as well as helping to strengthen services can be a barrier to care homes in terms of processes and on-going audit trails.
Public perception of care homes could be improved as it is often seen as a ‘last option’; a negative choice rather than a positive move in a care journey. The sector is acutely aware of the poor perception of care, often fuelled by media stories, and there is work underway to focus on the positive aspects of care delivery.
2.1 Current care provisionBefore we consider models of change in care homes it is worth focusing on current care provision, or the perception of it as evidence in this area is limited.
Some authors refer to this as ‘traditional’ or ‘task focused’ care delivery and there is some agreement in the literature that key elements of this include the following characteristics: task focus regular routine where the time of day rules timing of care activities fostered reliance rather than rehabilitation lack of meaningful activities lack of homely environment no connection with previous life or interests.Source: Demos 2014, Szcepura 2010
2.2 What are the drivers for change?
Policy direction One of the main drivers for change is recent policy, the key elements of which include: personalisation of care supported through the introduction of individual budgets
4

independence, choice and control with a focus on remaining at home for as long as possible by supporting carers and promoting preventative action
holistic care and support facilitated through the integration of health and social care quality improvement in the delivery of care and quality of life for service users, through
delivery of compassionate care and improving the culture of care.
These have been made clear through a number of policy documents, for example, Making sure health and social care services work together (DH 2013a), Helping carers to stay healthy (DH 2013b), Treating patients and services users with respect, dignity and compassion (DH 2013c), Helping people make informed choices about health and social care (DH 2013d), and Improving quality of life for people with long term conditions (DH 2013e).
The Care Act and economic climateThe Care Act is the latest policy development and the first major reform of social care law for over 60 years. It reflects the policy goals outlined above and in addition sets out new funding patterns, the rights of informal carers and highlights the need for better information and advice than is currently available. This is particularly relevant with the increase in people funding their own care and support; often referred to as self-funders.
The full impact of the shift in policy needs to be considered in the current financial climate, which is feeling strain from both austerity cuts and an increase in service demands. According to ADASS, since 2010/11 councils have had to make service reductions of £725million (ADASS 2014 budget surveys 2011 to 2014 in Demos 2014). In real terms the spend on adult social care has fallen by 12% (National Audit Office, 2010/11 to 2012/13 and ADASS budget survey, 2013/14) when the demand for support has increased by 14% (ADASS 2014).
There is real concern among Directors of Social Services that this gap will increase and become unsustainable, as indicated by the new president of ADASS who points out that financial burdens will flow from the Care Act and while changes are welcome; ‘Directors are increasingly concerned about the impact on countless vulnerable people who will fail to receive, or not be able to afford, the social care services they need and deserve’. (ADASS 20142)
Poorer outcomes 2 Quoted in ADASS, ‘Social care services “unsustainable”– ADASS’, press release, Association of Directors of Adult
Social Services, 2 Jul 2014. Click on this link for more information www.adass.org.uk/social-care-services-unsustainable-
adass/ (accessed 4 Jul 2014)
5

In terms of outcomes, there is evidence to suggest that residents of care homes do not fare as well as other older people. For example, residents in nursing homes may experience; lower quality of life than community dwelling elders (Karakaya et al 2009), they may suffer from increased depressive symptoms, decreased comfort and reduced engagement in meaningful activities (Degenholtz et al 2008) and there is evidence to suggest declines in physical and psychological health are not uncommon (Scocco et al 2006).
2.3 What does this mean for care homes? It is unclear from the Care Act just what changes care homes will face as pressure is placed on commissioners and regulators to deliver on the Care Act while facing budgetary cuts. However this, along with other policy drivers, set up a number of challenges for care home providers.
These are set out in recent reports from Demos (2014) and ILC UK (2012) both of which focused on the future of care homes and point out the major challenges this sector faces in the next few years: Funding: cuts in budgets, combined with changes in administration and an increase in
self funders make the market a different place to operate in. Market shaping: the impact of austerity is still rolling out but there are concerns that
economies of scale are pushing commissioners toward larger providers. Split in care provision: as more affluent citizens can afford to pay for care, there are
concerns that the market will split into luxury provision for those who can afford it and more basic provision for those with fewer resources.
Workforce issues: this will be discussed in detail below but, in summary, pay, progression and the recruitment and retention of a high quality workforce is a challenge for care homes.
Public perception/Media portrayal: recent programmes highlighting abuse and violence in care homes have been incredibly damaging for the reputation of care homes among the public. Care homes are often viewed as ‘a last resort’, as discussed below.
Policy presumptions: policy assumes care at home is the best option for older people and therefore aims to keep older people at home as long as possible; feeding the view that care homes are a last resort.
Population demographics: as the population demographics change and people are encouraged to live at home for longer, the demands on care homes will increase as more complex care will be required to meet the needs of an older population who may be living with various health issues.
Integration: as there is an ongoing move to integration of health and social care, and pressure to minimise hospital admissions, care homes are an alternative for nursing care.
6
Engagement: engagement across a number of fronts including residents, families and friends, the community and engagement with new technologies.
Summary of current care The perception of current care provision is a ‘traditional’ model, which is task-focused and not person-centred. How far this perception reflects reality is not documented but it is fair to say that policy is constantly driving for person-centred care, choice, and flexibility as far as possible. However, this is in the face of budgetary constraints meaning commissioners and service providers have to think differently about how services are sustained and improved.
2.4 Changes in registration and regulation Changes in the management of the Care Quality Commission have resulted in proposed changes to the registration regulation and actual changes in the standards around which care delivery will be monitored and inspected. The planned registration regulation for care aims to: introduce fundamental standards below which no provider should fall make regulations more effective and improve enforcement against them become outcomes-focused reduce the burden on business.
The timeline for introducing these measures is set out in the following sequence: The Duty of Candour will be introduced for NHS bodies only in October 2014. The fit and proper persons requirement will be introduced for NHS bodies only in
October 2014. The fundamental standards will be introduced for all providers in April 2015. The Duty of Candour and fit and proper persons requirements will be extended to all
CQC-registered providers from April 2015.
Inspection processesThe new inspection regime for services that are registered focuses on delivery of care that is safe, effective, caring, responsive and well-led. Leadership is perhaps the most significant and important change for care homes. The standards will be enforced through registration, intelligence monitoring, expert inspections and feedback from the public. In addition, inspection ratings have been introduced to reflect ‘outstanding’, ‘good’, ‘requires improvement’ and ‘inadequate’ standards of care.
Regulation as a barrier?While regulation may be a driver for improvement, there is some evidence that it is also a barrier. BIS (2013) reviewed the impact and experiences of regulatory enforcement on adult care homes. They found that while the sector recognises the importance of independent assessment for public confidence, and the role of the regulator in this context,
7
there were concerns expressed over the way in which regulations are enforced and how commissioning roles are exercised.
The sector also expressed concerns over the focus on paperwork at the expense of care. Both in terms of diversity required for different organisations and duplication of effort required to meet the requirements.
This view was supported by research commissioned by the Joseph Rowntree Foundation (Warrington et al. 2013), which identified more than 100 separate items of paperwork that must be completed regularly in care homes to respond to commissioning and regulatory requirements. However, the authors note the absence of a shared view of what should be valued in care across the paperwork identified. Staff involved in the research felt that the demands to complete paperwork had no bearing on the assessment of quality of care in residential care and that they were judged on the quality of paperwork not care delivered. There was a real sense that paperwork cannot measure the quality of interaction between care staff and residents but offers false assurances in this regard.
Summary The new regulations coming into place are another consideration for service providers and commissioners with a strong focus on leadership and effective care. However, regulation as well as helping to strengthen services can be a barrier to care homes in terms of processes and on-going audit trails.
2.5 Current public perception of care It is incredibly important to understand the policy context when thinking about change and why care homes should, and do, change their approach. It is a particular challenge as the common public perception is that care homes are the ‘last resort’, to be used once all other care options have been exhausted. This is influenced by several factors: the media portrayal of the care sector, the political drive to keep people ‘in their own homes’ for as long as possible and the perceived poor pay and conditions dominating the adult social care sector.
Public perception There is limited literature in this area but what there is indicates that the public view the choice to move to a care home as a negative, reactive decision rather than a positive proactive one and therefore to view care homes as the ‘last resort’ (Abbott et al 2000, NDTI 2009). Residential care expanded in the 1980s in response to the privatisation agenda and while care homes will be based on a similar vision and set of values, there is no central thread holding them together and public perception is very different compared with other community based organisations e.g. hospices.
In a recent survey (Demos 2014), the general public were asked to use words associated with care homes. The most commonly cited ones included boredom, loneliness, illness,
8

isolation, abuse, uncaring. While there were positives as well (e.g. safety, friendships, comfort, modern, fun etc.) the overwhelming picture was one of negativity.
In the same survey, members of the public who said they would not move into residential care in later life gave the following reasons for their response:
loss of independence (69%) risk of neglect or abuse (54%) wouldn’t be like home (48%) poor quality care (42%) no desire to be surrounded by people who are old or disabled (42%) would have to sell house (33%) lose contact with friends, family and community (31%). Source: Demos 2014
These findings of negativity and fear have been found in other studies with the general public. For example, 70% of UK adults said they would be scared to move into a care home in the future (Quince 2013).
Reasons for the negative imageThere are a number of reasons that this negative image exists including the recent and on-going media portrayal of care homes highlighting abuse and neglect. For example, the Winterbourne View scandal over which four staff members were arrested following undercover filming by a former nurse. It is interesting to note that while statistics indicate that 2% of residents in care homes suffered abuse at the hands of a staff member, which all agree is unacceptable, this remains lower than abuse by friends and family (HSCIC 2014).
Finally, there is evidence of inconsistent care across the sector as illustrated through CQC inspections, which indicate that from the latest inspections using new parameters, 43 out of 107 required improvement, and 6 were under enforcement action3. This is supported by findings from inspections carried out in 2012/13 where 1 in 5 nursing homes revealed safety concerns and 10% of inspections in care homes without nursing uncovered problems with safeguarding, safety and staffing (CQC 2013).
Redressing the balance Within the sector, there is a desire to improve public perception through initiatives such as the National Care Home Open Day. This involves care homes linking together to present care homes in positive and proactive light and make lasting connections between local communities and care homes. The approach is supported by the Department of Health, CQC, National Association for Providers of Activities for Older People and SCIE. 3 http://www.cqc.org.uk/search/services/care-homes?f[0]=im_field_inspection_rating%3A4392&f[1]=im_field_status%3A3683 accessed 26 August 2014
9

A further initiative is the Social Care Commitment where employers and employees enter into a voluntary agreement to improve the quality of care and support services and public confidence in these services. Employers commit to recruit staff who care, provide thorough induction training, help
staff develop skills, make sure staff understand quality and safety standards, take responsibility for how staff work, supervise staff properly, support staff to put their commitment into practice every day.
Employees commit to work responsibly, uphold dignity, work co-operatively, communicate effectively, protect privacy, continue to learn, treat people fairly.
An initiative that sets out to engage in conversation with the public directly about care homes is ‘The Big Conversation’. This is a public project led by My Home Life which aims to raise public awareness about what makes a good life in care homes now, what could make them better and how might we get there. The vision is to open a dialogue about quality improvement, engage the public in better understanding of care homes and offer a creative way to meet requirements around user and carer involvement.
Finally, Skills for Care operate an annual award scheme, The Accolades, to highlight excellence in workplace development in the adult social care sector.
Summary The public perception of care homes could be improved as it is often seen as a ‘last option’, a negative choice rather than a positive move in a care journey. The sector is acutely aware of the poor perception of care, often fuelled by media stories, and there is work underway to focus on the positive aspects of care delivery.
10

3. What does future care look like?
OverviewTraditional care has been described as task focused, inflexible, lacking a sense of purpose and institutionalised. Policy, the quality improvement agenda, changes to regulation and registration and current public perception of care have all been identified as drivers for change. The model of future care highlighted by some authors, and to a large degree exhibited by those care homes involved in the consultation, includes a focus on relationships, quality of care, flexibility and engagement. Indeed older people themselves have identified characteristics which are important for care as being continued freedom of movement and ability to continue with individual routines, a positive environment and a sense of belonging to a community rather than residing in a home.
3.1 Key elements to attitude and approach Traditionally, people have been expected to fit into existing services with little control over the provider and flexibility of the service (Dowling et al 2006). However, based on policy, quality improvement and emerging research in the area, there is a move to person-centred and relationship-based care (Brown Wilson 2009, Dowling et al. 2006). This shift requires change across a number of areas including funding mechanisms, organisational culture, staff attitudes, strategic targets and working with others and some argue much more difficult to implement that promote through policy (Dowling et al. 2006).
3.2 Institution-directed care v. resident-centred care Musselbrook (2013) summarises this in her paper by demonstrating where services have been (or in some cases still are) task-focused and how these should look in the future if the personalisation agenda is to be fully realised. She argues that past and some present services are expert/provider-centred, inflexible (‘one size fits all’), based on a needs and deficit model, protective and risk averse, foster dependency and are inputs and outputs focused. Future services should be person-centred, flexible, outcome-focused, strengths and assets based, facilitate individual decision making and individual responsibility. This is echoed through the philosophy of person-centred and relationship-based care described in section 6.0 below. It can be summarised by an extract from the Pioneer Network which is a US network supporting care homes to embrace culture change.
They suggest that in an institution-directed care culture: Staff provide standardised "treatments" based upon medical diagnosis. Schedules and routines are designed by the institution and staff, and residents must
comply. Work is task-oriented and staff rotates assignments. As long as staff know how to perform a task, they can perform it "on any patient" in the
home.
11
Decision making is centralized. There is a hospital environment. Structured activities are available when the activity director is on duty. There is a sense of isolation and loneliness.
In a resident-centred care culture: Staff enter into a caregiving relationship-based upon individualized care needs,
personal desires and with a focus on ability. Elders and staff design schedules that reflect their personal needs and desires. Work is relationship-centred, and staff have consistent assignments. Staff bring their personal knowledge of elders into the caregiving process. Decision making is as close to the elder as possible. The environment reflects the comforts of home. Spontaneous activities are available around the clock. There is a sense of community and belonging.
In her think piece, Musselbrook (2013) goes on to highlight the importance of shifting from ‘expert’ cultures to an assets based approach, to focus on workforce development, consider how to reallocate resources, develop support planning and brokerage and consider new working roles (e.g. generic workers or hybrid roles).
3.3 From older people’s perspective As potential service users, it is important to consider the views of older people themselves when thinking about residential care for the future. Demos (2014) asked older people who currently do not live in a care home what would be important for them, as they grew older, regardless of where they might live. Respondents identified the following quality of life traits: freedom to have own rhythms and routines and choice of what to do and when support to maintain social networks a sense of belonging to a community of people with similar tastes and interests access to a range of leisure activities within and outside the house continued freedom of movement an environment surrounded by familiar things a connection to the outside world through technology and the internet the ability to manage own finances help with some aspects of daily life retention of dignity. Source: Demos 2014, NDTI 2009, Davies and Nolan 2008 in Milne 2011
3.4 SummaryDemands for future care provision focus on resident-centred care where staff enter into more of a relationship with residents to understand their backgrounds, existing interests,
12

preferences and care needs. In reality, older people are asking for a high standard of care in terms of staffing etc. but, in addition, they are interested to see a more individual approach to care and some retention of independence and continued access to the wider community as part of this.
13

4. How can we make the shift?
OverviewThere is a lack of evidence from care homes, which look at models of change, and even less information available on the effectiveness of change. However, management literature would suggest that different levels of change could occur; e.g. developmental, transitional and transformational. Various theories have been formulated to conceptualise change and could be applied to care homes, however, we did not identify literature that discussed change in care homes at this theoretical level. Literature identified was more likely to talk about the practical aspects of change, for example, tools to help with change or characteristics of change facilitation. These included strong leadership, innovative people, employee and stakeholder involvement and participation in change.
Having looked at current care and the potential for future care, a number of questions remain: How do we get there? What are effective models of change? What are characteristics of facilitators for change? This section begins to address some of these questions but it is worth stating that there is a lack of published research based in care homes, and in particular care homes without nursing.
There are even further restrictions when it comes to identifying evidence of effectiveness of transformational change or models of change. Therefore the following section highlights more generic approaches to change in adult social care and models of care which are being delivered but currently not tested or evaluated in the hope that future work will be able to address some of these shortcomings in the evidence base.
4.1 Organisational change management According to Anderson and Ackerman Anderson (2010) there are three types of change that can occur in organisations: Developmental change: improvements to current approach to improve processes or
methods used. Transitional change: replaces old processes with new e.g. new services or technology. Transformational change: whole systems change that can involve developmental and
transitional change.
In adult social care, there is talk of transformational change although there is less evidence to support this and more indication that transitional or developmental change is more likely.
14

Managing changeThe way in which change is managed can be described in many ways but one of the most influential perspectives within ‘planned approaches’ is that of Lewin (1952 in Elrod ll and Tippett 2002) who argued that organisational change involved 3 stages: unfreezing current approaches, moving to new behaviour and refreezing of new behaviour (sometimes called Bridge’s Transition Model).
This has been largely superseded by the ‘emergent approach’ (or Kotter’s Eight Steps to Change) which describes change as so rapid that it can’t be managed in this respect and is a process of learning where the organisation responds to internal and external changes. Common themes include the development of a vision, establishing a sense of urgency to change, strong leadership, implementation and supporting structures, good communication of change, embedding changes in culture and processes, and reflection on gains (Barnard and Stoll 2010). The underpinning assumption in this approach is that managers have a depth of understanding of the organisation, its structure, the people and culture.
Finally the whole systems approach, which states that change requires collective action on the part of many key individuals from different perspectives, has gained popularity. Not simply the sum of its parts, whole systems change focuses on identifying the components of a system and understanding how each link and contribute to the whole.
Organisational readiness for change In order for change to be introduced there must be organisational readiness for change, characterised by motivation, resources, positive staff attitude and supportive organisational culture (Austin and Claassen 20008). Examples of tools to measure ‘readiness’ include ‘Organisational Readiness for Change’ and ‘Audit of Readiness’.
One of the biggest challenges managers face is individual resistance to change based on fear of the unknown, loss of control or face, fear of demotion and the need for security (Austin and Claassen 2008). There are different schools of thought in this area including application of the Five Stages of ‘Grief’ model (Kubler-Ross Five Stage model which includes denial, anger, bargaining, depression and acceptance), the technology adoption curve and the ‘Prosci Model” based on awareness, desire, knowledge, ability and reinforcement. Regardless, all agree on the importance of a proactive strategy to support staff through the changes required. Strategies include education, participation, facilitation, negotiation and coercion, each useful in different situations.
Another potential challenge for change is current management or leadership. In order for change to occur, leaders must be viewed as transformational, able to stimulate an environment of learning and risk as well as a supportive environment for staff (Austin and
15

Claassen 2008). This REA also identified the importance of Rogers’ work (1995) which identified five characteristics in the context of sustaining and diffusing innovation: relative advantage, compatibility with current practice, complexity of change, trial-ability or change in stages, observed and positive outcomes associated with change.
Beyond implementation, managers need to pay attention to sustainability, as it is easy to slip back into old habits. However, there is relatively little research in this area but what little there is suggests the need to have strong leadership, supportive policies and environments, good organisational fit with the new belief system, shared norms among the workforce, and commitment from individuals.
Summary There is a lack of care home specific literature available which looks at organisational change and the impact on quality of care. However, general change management literature would indicate that there are various types and stages of change which could be applied to different situations. For example, planned approaches to change require some prior thought and preparation to introduce and sustain change. Emergent processes are more rapid and often happen when organisations are required to respond to change. Dealing with change requires understanding of the organisation, of staff and strong leadership to drive the change through. 4.2 Organisational change in care homes We did not identify any specific literature which considered organisational change in care homes at this theoretical level, i.e. consideration of a planned approach to change, measurement of the impact of planned changes etc. However, more generally in adult social care there has been some work to identify processes and actions that have been most effective in bringing about change and sustaining improvement in social care services.
In 2005 the Local Government Association stated that organisations that had achieved transformative change shared the following characteristics: a well-developed and embedded culture of change that positively valued difference,
and that learned from failure a record of organisational innovation innovative people-management and strategic and transformative approaches to human
resource management.
Fauth and Mahdon 2007 conducted a knowledge review in this area and identified three action points for organisations to consider when embarking on change to improve services: strong leadership that propels change and improvements employee involvement and participation in change
16
stakeholder involvement and participation.Some of these points were reflected in the consultation with managers. While none described the desire for transformational change at the outset, many talked about the importance of leadership, staff involvement and shared practice as integral to their process of change.
Practical tools to help with changeWhile there was little literature on the theory of change, some practical tools to help with change were identified. For example, The Principles of Workforce Redesign (POWR), published by Skills for Care (2008), is based on organisational change theory.
The guide for employers outlines seven principles for social care organisations to adhere to in order to manage transformation of services: Take a whole systems view of organisational changes. Recognise how people, organisations and partnerships respond differently to change. Nurture champions, leaders and innovators. Engage people in the processes—acknowledge and value their experience. Be aware of the way adults learn. Change minds and change systems. Develop workforce strategies that support transformation and recognise the shape of
resources available in the local community. Source: Skills for Care 2007 (currently being revised).
Finally there are tools to help with organisational change in long-term care. For example, ‘Implementing Change in Long-Term Care: A practical guide to transformation’ (author?) an American guide which outlines current thinking around person-centred care, culture change, leadership models, team development, staff education and preparing for change.
SummaryWithin adult social care, and the care home sector specifically, there is little published work around theoretical approaches to change. However, some characteristics begin to emerge around readiness for change and some tools relating to practical guidance and change management are available for care homes.
17

5. Models of change in care homes
Models of change in care homesIn terms of models which care homes could adopt to change culture and service delivery, the REA identified: The ‘Butterfly Service’, specifically aimed at homes working with people with dementia. The ‘Eden Alternative’, aimed at eliminating boredom, loneliness and helplessness for
care home residents. ‘Social pedagogy’, drawing on European experiences to improving relationship-based
care. ‘My Home Life’, a UK based model of care underpinned by evidence and growing in
popularity. ‘Dignity in care’, less of a model per se but policy focusing on transforming services. The ‘Devon Kitemark’, based on evidence and shared between local care home
providers in the area to drive up quality. ‘360 Forward’, allowing care homes to benchmark current services, agree change and
review progress.
Moving from the theory of change to identified change models, this section sets out the key approaches that were identified in the REA. In total we have identified and will describe 7 approaches to change in care homes. The models are predominantly linked to person-centred care.
Again it is worth stating from the outset that evidence is limited and there is little published evidence in this area, a finding supported by others (e.g. Szczepura et al. 2008). This is also the case for the models of change included. There is limited formal evaluation, but what is available is presented alongside feedback from those involved in promoting the model.
5.1 Butterfly Service A model of care that is being adopted in the UK and Ireland in a move away from the traditional ‘institutional’ type care is the Butterfly Service model, developed and delivered by Dementia Care Matters4. Currently focused on people with dementia, it outlines principles that support a person-centred approach to care. The five key elements are strong leadership, appropriate physical environment, emotionally intelligent staff, power sharing and purposeful activities.
4www.dementiacarematters.com last accessed 1 Sept 201418
Organisations are encouraged to improve the culture of care by undertaking a one year strategy project, supported through a range of steps including a review of current service provision, management strategy, leadership training, workforce development, consultancy, team leader modelling and unannounced audit visits. Organisations are encouraged to start from the premise that ‘feelings matter most’ and consider removing divisions in care home between ‘them’ and ‘us’ e.g. uniforms, staff only signs etc., and think of the setting as a ‘home’ or ‘community’ not as a workplace. Homes are also encouraged to think about evidence of physical and emotional freedom, feelings are foremost, meaningful activities, positive mealtime experiences and person-centred planning.
Sheard (2014) outlined a series of questions to assess readiness for change for organisations considering the Butterfly Service (see Table 1). Table 1: Readiness for organisational change
Design Will the home adopt a household model, breaking up the home into houses with separate front doors and combined living/dining rooms?
Environment Is the home going to be given permission to fill the houses up with the ‘stuff of life’ rather than marketing a hotel model of care?
Family like culture
Will the home remove all ‘them and us’ features of institutionalisation?
Specialism Will the home see that people living with different points of dementia need different skilled approaches?
Matching Will the home agree to group people in houses based on where people are in their level of dementia?
Emotional intelligence
Will the home recruit, train and appraise staff on this as the primary competence?
Leaders Will the home appoint on values and leadership rather than seniority or nursing skill alone?
Attached staff Will the home match individual staff to a specific house recognising the people’s different skills so that this brings out the best in staff?
Nursing Will the home demonstrate its value in nurses, agree to modernise their role and adapt a personalised way of providing nursing care?
Decentralisation
Will the home create housekeepers rather than central domestic services and remove centralised dining?
Home for life Will the home promote a home for life not house for life agreement with families?
Intimacy Will the home take a balance approach to wellbeing while meeting non-restrictive safeguarding processes?
Quality Will the home accept as its primary qualitative methodology the lived experience of people?
Source Sheard 2014
19
Evaluation of the Butterfly Service There are currently no formal evaluations available of the approach. However, Dementia Care Matters have confirmed that they have anecdotal evidence to indicate some positive impacts include a reduction in staff sickness rates, safeguarding alerts, medication usage and falls as well as an increase in staff retention and residents’ weight.
5.2 The Eden Alternative Originating in the US, the Eden Alternative is now established in the UK. The mission of the Eden Alternative is to ‘improve the wellbeing of Elders and their care partners by transforming the communities in which they live and work’. The vision is to eliminate loneliness, boredom and helplessness by working within 10 principles of: Reducing loneliness, boredom and helplessness. Creating a community where life revolves around close and continuing contact with
nature and others. Loving companionship as an antidote to loneliness. Creating opportunity to give as well as receive care. Embracing variety and spontaneity by creating an environment in which unexpected
and unpredictable interactions can take place. Filling daily life with opportunities that are meaningful. Reassessing the role of medicines. De-emphasising top-down bureaucratic authority and replacing with shared decision
making. Recognising that creating person-centred communities is a never-ending process. Supporting strong leadership.
The model is supported by training courses for a minimum of 10% of care home staff, regardless of their position / role. The learning focuses on the ten principles and takes a personalised approach to exploring participants’ experiences of loneliness, boredom and helplessness to change their mind-set for delivery of care and priorities. Participants are provided with tools to cascade the learning in their organisations and supported through review days, help with rollout, peer support events etc. After around a year, the home is assessed to ensure change in care delivery has changed. The approach is also being adapted to work with domiciliary care staff.
Evaluation of the Eden Alternative There have been a small number of studies evaluating the Eden Alternative although none have been conducted in the UK. Studies from the US have reported mixed results depending on the focus of the evaluation. Positive results were found when looking at depression scores for residents and family satisfaction whereas there was little evidence to support increased cognition of functional status of residents (Mueller 2008).
20

Anecdotal evidence from the UK suggests that care homes that have been validated as Eden Alternative care homes have seen a positive impact. For example, an increase among residents in appetite, community participation both in the home and with the wider community, stable sleeping patterns, and organisations have seen an increase in staff retention. Decreases in falls, stress levels (both among residents and staff), use of (?) medication, and staff absenteeism have also been noted.
The work has been endorsed by the Deputy Director of Nursing at the Department of Health as fitting with policy and the organisation is working with the National Skills Academy and the Centre of Excellence for Practice Development to endorse the training.
5.3 Social pedagogic approach Social pedagogy was developed in Europe and provides a unifying concept of work with people in many formal or informal institutional settings. The approach can be understood as a process of nurturing whereby the residents are treated as equal, and their ideas and beliefs are valued. It is an approach to practise rather than a method. The aim of the approach is to provide wellbeing and happiness, promote holistic learning over the lifespan, resident empowerment and positive experiences.
The focus is on staff becoming ‘risk competent’ that is knowledgeable and skilled in assessing risk in order to promote empowerment (Eichsteller and Holthoff 2009). Other principles of social pedagogy include: a focus on the resident as a whole person a foundation on the rights and understanding that this is not limited to procedural
matters or legislated requirements the practitioner seeing herself/himself as a person in a relationship with the resident residents and staff are seen as inhabiting the same life space, not as existing in
separate hierarchical domains sharing in many aspects of daily lives and activities an emphasis on team work and on valuing the contribution of others the centrality of relationship and, allied to this, the importance of listening and
communicating.Source: Petrie et al. 2006
Pedagogic practice is a holistic process that creates balance between: the professional (theory and concepts, reflective practitioner – the head) the personal (using one’s personality, positive attitude, building personal relationships
but keeping the ‘private’ out – the heart) the practical (using certain methods and creative activities – the hands).Source: ThemPra Social Pedagogy
21

Social pedagogy in the UK In the UK the approach is mainly used with people with learning disabilities and residential care services for looked after and accommodated young people. However, further afield, social pedagogues use the approach across the lifespan and there is one example of a care home in Aberdeen that takes a social pedagogic approach to working with residents.
Evaluation of social pedagogyEvaluation of the approach has mainly focused on children’s services in the UK and recent findings (Cameron 2011, 2012) indicate that while there were some cultural difficulties in introducing social pedagogues into an existing situation, there were positive outcomes for residents. This is difficult to interpret as the pedagogues were employed to fit with existing staff rather than transformation of the service to embrace this approach.
5.4 My Home LifeOriginally sponsored by Age UK, City University and the Joseph Rowntree Foundation it has subsequently attracted funding from local authorities and City Bridge Trust. It is based on evidence that looked at quality of life in care homes and identified eight themes to underpin the vision outlined in 2 below.
22

Table 2: My Home Life themesGrouping Theme QuestionsPersonalisation Maintaining
identityDoes the home give priority to residents’ backgrounds and histories?How is this information used to improve their care?
Creating community
Is the home linked with local community organisations?
Sharing decision making
How are residents, relatives and friends encouraged to participate with the home?Is there a choice of meaningful activities for residents and how often do these take place?How can residents and their relatives express their views and preferences about the way the home is run?
Navigation Managing transitions
How are new residents welcomed and encouraged to participate in the life of the home?
Improving health and healthcare
How does the home ensure access to appropriate health care services?
Supporting good end of life
How does the home deal with dying, death and bereavement for residents, relatives and staff?
Transformation Keeping the workforce fit for purpose
What is the resident to staff ratio?What training programmes are in place for staff?
Promoting positive culture
What makes the home ‘special’?In what ways is it a ‘home from home’?
Source: My Home Life website, Help the Aged 2007, Owen et al. 2012
The themes are supported by a series of video clips, newsletters and resources for care home managers to use in their journey to improving quality of care based on the evidence available. In addition, there is a leadership programme which is delivered over a 12-month period and sets out to help managers engage with evidence-based, relationship-centred practice.
23

Evaluation of My Home LifeThe most recent evaluation of the approach (NDTI 2014) worked with Essex County Council to take a relationship-based approach to commissioning and procurement of care as well as delivery of care. Findings indicate that care home managers are pivotal to embed the approach and where this occurs, there were signs of staff empowerment and changes in emphasis from task-orientated to relationship-focused care. The ‘no blame’ culture has enabled staff to build on success and in some homes, the approach has led to staff describing more balanced, creative approach to risk.
Granville et al (2014) in an evaluation of My Home Life noted positive changes for both care home managers and residents as depicted below:
FOR CARE HOME MANAGERSFrom ToHaving little confidence in their own values and beliefs
Being able to challenge and share decision-making
Having an unequal partnership with stakeholders e.g. NHS
Able to operate as an equal partner
Feeling isolated and lonely Part of a supportive network of peersBehaving as if powerless Behaving like a leader
FOR OLDER PEOPLEFrom ToCare is about task with people Care is about building good relationshipsNo risk-taking is allowed Risk is well managedIsolated from the community Part of the communityProprietor’s home The older person’s homeNot being able to continue the things that give life meaning
Getting support needed to continue doing the important things
5.5 Dignity in care Dignity is a major policy theme that encourages a cultural shift to ensure care is person, not task focused. According to Age UK, dignified care means having a positive attitude to ageing and working together with older people, families, carers and advocates to shape care around an individual’s needs5. The concept of dignity embraces modesty, protects self-respect, helps retain a sense of control and maintains good communication and good relationships (Edith Cowan University 2006, Thompson and Chochinov 2008, Gerry 2011). Delivery of dignified care relies on staff attitudes, kind and professional behaviour, compassion and strong relationships (Chochinov 2007).
5 http://www.ageuk.org.uk/home-and-care/improving-dignity-in-care-consultation/ last accessed 2 Sept 2014 24

In 2012 the Independent Commission on Dignity in Care (collaboration between the NHS Confederation, Local Government Association and Age UK) published the report of their investigations “Delivering Dignity” (2012) and outlined steps to improve dignified care. The next step is to work up a comprehensive implementation plan with three priorities: Transforming culture and practice in hospitals and care homes. Empowering older people, their families and communities. Identifying the good work already happening and driving it through the system.It is not clear when this implementation plan will be published.
Dignity therapyOne specific approach “Dignity therapy” is a brief intervention designed to address legacy needs among patients at the end of life, something often faced in care homes. By offering recorded therapy sessions which encourage patients to talk about their lives and what matters most to them, individuals have a written record of their thoughts to share with family and friends. It is not historical, rather focused on thoughts, ideas and events that hold particular meaning.
Evaluation of dignity therapyFindings from a randomised controlled trial suggested that while the intervention did not mitigate outright distress e.g. depression, desire for death; there were significant self-reported benefits in terms of patient experiences e.g. improved quality of life, sense of dignity etc. (Chochinov et al. 2011). In the UK, a smaller scale study reported that participants felt their life was more meaningful and their sense of purpose was heightened. It could be argued that the social interaction, which came as part of research participation, was an important contributor to the findings. Indeed other studies have shown that social relationships and feeling valued are important aspects of dignity in care homes.
5.6 Devon Care Providers Dementia Quality Kite Mark Not so much a model of change but an area-led approach to improve quality of care in care homes, in this instance focused on people living with dementia. The network was initiated in 2012 by a small number of care home owners with the view of driving up quality based on best evidence and a humanistic approach to care delivery based on relationship-based ideology (e.g. the work of Carl Rogers, Anthony Robbins etc.). The model is based on peer review where homes hoping to achieve the kite mark are visited by other care home owners/managers who conduct an ‘appreciative inquiry’ and provide feedback on different aspects of care, including the environment and atmosphere.
The peer review programme focuses on person-centred care planning, managing challenging behaviour, safeguarding, medical care, basic care, fall prevention and end of life care. This is supported by master class training which to date has covered leadership and management, staff development and living well with dementia. The programme is focused on improving outcomes in the following areas: creating environments that balance being safe with a good quality of life and having fun
25
optimising stability in care and reducing hospital admissions supporting a positive, loyal, skilled and enthused workforce strong leadership improving the media image of care homes high standards of care according to regulations.
Evaluation of the Kite MarkThere has been no formal evaluation of the approach to date although feedback form those involved would suggest that the approach has a positive impact on organisations, staff and service users.
5.7 360 Standard Framework - overview360 Standard Framework is an evidence-based approach to change and quality improvement in care homes. It is based on the views of service users and patients, families and staff, findings from research into what a good experience of health and social care looks like for most people, expert professional opinion, the views of campaigning services and the experience of the authors. The approach promotes Relationships Activated Care, which considers quality of care from the perspective of residents, staff and relatives (see Table 3 below). Table 3: Relationships Activated Care; quality of care perspectiveResidents:
Receive person-centred care to acceptable standards.Occupy time meaningfully.Able to influence preferences of food and drink.Able to express spiritual needs.Able to resolve concerns and complaints.
Staff:Find work fulfilling.Have time to deliver good care.Are equipped to do the job properly.Feel valued as a staff member.
Relatives:Feel a welcoming ambience of the homes.Observe effective communication between the resident, staff, mangers and relatives.Are fully informed on events affecting resident’s wellbeing.Are able to raise concerns and complaints on behalf of the resident without fear of retaliation.Are welcome to contribute to the care of a family member and community of the home.
26

The 360 Standard Framework allows managers to analyse evidence of current performance against the framework and their measures of achievement. This in turn enables them to plan and deliver quality improvement initiatives, associated learning, and develop practice on a continuum on a daily basis.
Organisations are supported through the change process through a set of tools for undertaking the diagnostic assessment of performance against the 360 SF, guidance and support for managers, learning programmes and management programmes. The process is managed through an e-learning system which offers the ability to project manage actions according to timescales.
In addition to offering a process of change for care homes, the authors have developed, and are piloting, specialist nursing roles and enhanced care home workers in order to offer a career pathway for health and social care staff working in care homes.
Evaluation of 360 Framework While the approach is evidence-based, there is currently no formal evaluation of the approach. However, the process is accredited by the RCN and endorsed by a number of national organisations and agencies including the NICE, SCIE, and College of Occupational Therapists among others.
Summary A number of key threads have emerged across all models of change considered including: Strong leadership and supportive management Relationship-based care Nurturing a ‘home’ not a house or care home Joint decision-making and involvement from stakeholders – not a ‘them and us’
approach Well trained staff Meaningful activities and positive engagement.
These ‘ingredients’ are explored in more detail individually in section 6 below.
27
6. Characteristics associated with change in care homes
OverviewFrom the literature a number of characteristics were identified that were linked to a more positive culture of care. These included person-centred and relationship-based care, a focus on organisational culture, a strong and supported workforce, a positive physical environment, joint decision making, links with the community and strong leadership. These characteristics were also identified as part of the consultation process, with participants particularly highlighting the need for strong leadership and participation from staff and residents as being key to introducing and maintaining change.
As stated above, from the models of care examined a number of consistent themes emerged as important characteristics for change in care homes: Person-centred and relationship-based care A positive organisational culture of care Well trained staff Joint decision-making and participation Strong leadership and supportive management A positive physical environment.
While the evidence of effectiveness is limited from these approaches, there was evidence from the broader rapid evidence assessment, which reinforced the significance of these characteristics. To try and dig a bit deeper, and provide more evidence of impact, this section looks at each of these characteristics in turn highlighting key points and any evidence of impact.
28
6.1 Person-centred and relationship-based care
What is person-centred care? Person-centred care remains central to current social care policy with the emphasis on transforming care, placing individuals at the heart of care planning and ensuring independence, choice and control. For the Department of Health (2010) this means putting individuals and their families at the centre of care planning and decision-making, to ensure personal preferences, needs and values are met.
‘Perhaps, most significantly, this [person-centred care] involves doing things ‘with people’ rather than ‘to them” (Musselbrook 2013).
This really reflects the model of future care set out in section 3.0 above and was a key term in our consultations. While staff didn’t always use the term person-centred care, the principles and desire to ensure that residents were at the heart of the service was evident. This was clear in the language used where the focus was building a home for residents rather than a workplace for staff.
[The care home is]… ‘their home and you are entering their home and you have to have that respect for them.’ (Staff participant)
Reflective practice and a deeper understanding of the individuals in order to guarantee person-centred care and the best outcome for residents was clear throughout the consultation.
‘We find out what they like and don't like, how they like to be addressed and spoken to. Anything we do is to help them feel at home.’ (Staff participant)
‘The 4-lounge set up helps to build relationships because everyone knows each other better.’ (Manager)
‘[We need to]…step back and look at the way they react and respond. Everybody is an individual and reacts in different ways and we have to assess responses.’ (Staff participant)
‘We nurture people’s emotional intelligence…we need to understand why people act in the way that they do.’ (Staff participant)
Elements of person-centred care From the REA a number of elements of person-centred care and working were identified: Putting the person at the heart of work and treated with dignity, compassion and
kindness. 29

The development of a relationship between staff and the individual, which involves shared decision-making, individual choice and control.
Attention to the whole person including spirituality, sexuality and cultural preferences. Good communication, including ensuring residents have access to appropriate
information (and advocacy if appropriate). ‘Living and breathing’ a culture of personalisation which means embracing
empowerment and inclusion. Positive risk taking and the creation of a defensible trail of shared decision-making and
robust systems of quality assurance. Joined-up working across multidisciplinary teams and between organisations with a
shared purpose and methods for working from outset. Strong leadership and management that discriminates between good and mediocre
practice. A skilled and competent workforce who are committed to understanding individual
needs and delivering a personalised service. Investment in recruitment and training for staff to ensure they have the values, attitude,
skills and knowledge to deal with the specific challenges posed. Provision of emotional support for staff working in challenging environments, through
good team working, supervision, debriefing and counselling. Systems for learning and reflection established.Sources: Kennedy 2014, Help the Aged 2007, Dowling et al. 2007, Mansell 2007 Glyn et al 2008, Neill et al. 2009, SCIE 2009, Froggatt et al. 2009, Department of Health 2010, Beresford et al 2011, Manley et al 2014
Introducing a person-centred approachThe Department of Health (2010a6) suggests that the best way to introduce a person-centred approach is to create ‘one page profiles’ and to utilise person-centred approaches in reviews and support planning. One-page profiles can, they argue, be particularly useful for people who have communication difficulties because they can enable them to express their desires and needs in a way that enables them to be supported how they want to be.
However, the literature highlights that working in a person-centred way is more than simply creating a plan. Quality of life can only be improved if the staff implementing the approach are properly trained and supported (Froggatt et al. 2009), and good quality plans tend to be equated with higher levels of engagement in meaningful activities (Adams et al., 2006). This approach was well substantiated in the consultation with care homes where all described the effort that went into ensuring a range of activities on offer, reflecting personal choice, past interests and, in some instances, employment.However, Robertson et al. (2005) also concluded that person-centred working appears to work better for some people than others, because their specific needs tend to dictate the type of plan they receive (if they receive one at all).
6 Department of Health (2010a) Personalisation through Person-Centred Planning. London: Department of Health
30

There are numerous tools for care homes to help with person-centred and relationship-based care which do not require the transformational change outlined in section 4.0 above. For example, NHS Institute has been working with a small number of care homes on two projects to improve relationships inside the care home (‘Care Homes Wellbeing’) and with external partners (‘Care Homes Connect’). Over a nine-month period they have worked in co-production with staff, residents and relatives to develop a programme to empower staff to make changes, improve safety and internal systems, improve efficiency and staff skills and knowledge. Evidence suggests that there have been some positive impact of the approaches. As a result of this work, downloadable guides are available for care homes to use7. The table below highlights some key guidance for employers.
Table 4: Key areas for managers’ consideration when moving to person-centred care
Does your service respond to identified local need or will changes need to be made?
Given the size and facilities of the care home, are there opportunities to diversify and is this possible financially?
Does your Statement of Purpose clearly describe services in personalised ways?
Do your residents have access to advocacy services and information needed to make decisions which reflect their needs and are culturally sensitive?
Is the culture and practice in your home enabling and open to change and not paternalistic?
Is your complaints procedure clear, easy to understand and responsive?
Commissioning practices will change as Local Authorities may move away from the use of block contracts with providers in an attempt to fund other service arrangements. How will this affect what you do?
Are staff aware that control should be with residents and are they supported to work in this way?
Is your care home able to think about risk, not linked to regulation, but to individuals and take a positive-risk taking approach?
Source: SCIE (2009) Granville et al 2014
Relationship-based care in comparison with person-centred careSome authors have argued (Brown Wilson 2009) that relationship-based care takes
7 www.institute.nhs.uk/care_homes/_programme/an_overview.html31

person-centred care to the next level. As well as being individually focused, the real emphasis in relationship-based care is on the relationship between staff, between staff and residents, and between residents (Dowling et al. 2007, Brown Wilson 2009). The focus shifts from personal and responsive relationships between residents, staff and, to a lesser extent, families to one of a reciprocal relationship taking into account the communal nature of living in a care home. An understanding of how ‘we all’ fit into the community. As with others, relationships in this context are built on trust, consistency, shared understanding of significance of all members of the care home, warmth, respect and a caring attitude (Brown Wilson 2009, Mansell 2007, 2010, Carr 2010, Wallcraft 2011, Ofsted 2011, Camble 2012). A number of specific models have been identified which aim to promote a relationship-based approach to care to develop a positive environment for living.
The Butterfly Service, My Home Life, social pedagogy and dignity therapy can all be described as relationship-based care as they focus on breaking down barriers in care homes, promoting a shared approach to life and creating a positive, trusting environment for staff, residents families and carers (see section 5 for more detail).
Barriers to the development and delivery of person-centred and relationship-based care have been highlighted: an underdeveloped and unsupported workforce continuing institutionalisation and organisational bureaucratisation with an on-going
emphasis on negative risk often framed in health and safety terms social care practice focused on what residents can’t do rather than what they can lack of appropriate support to make full advantage of person-centred care and
planning.Source Beresford et al. 2011
Evidence of impactWhilst these concepts are firmly rooted in government policy, translation into practice appears to be slower. The scale of change required to shift from service-focused delivery, where outputs (such as the number of people using the service) are measured, to an individual-focused approach, where experiences and quality of care are central, is challenging for many care homes although, as demonstrated in section 4.0 above, achievable. However, there is also a lag with the development of the evidence base. As described earlier, there is limited evidence available which evaluates the impact of person-centred care on outcomes for service users.
In their systematic review, Li and Porock (2014) concluded that evidence regarding the effects of person-centred practice focusing on residents’ outcomes is not well established or synthesized. They found some limited evidence that person-centred care had beneficial effects on residents’ psychological wellbeing and benefits when applied to dementia care in particular.
32

Summary Person-centred care and relationship-based care are closely linked. Both focus on placing individuals and families at the heart of care planning and decision-making. Person-centred care requires attention to the whole person, facilitated by better relationships between staff and residents, but also between staff, for better outcomes all round. Fostering a culture of flexibility, positive risk taking and communication are all facets in their own right, but also form the backbone of person-centred care. While the evidence base is currently underdeveloped, emerging evidence would indicate strength in this approach resulting positive outcomes for service users and staff.
33

6.2 Organisational culture
What is organisational culture? Austin and Claassen (2008) argue that understanding organisational culture is fundamental to organisational change. Doherty et al (2013) and others (Kirkley et al 2011, Westrum 2004) suggest the concept of ‘organisational culture’ has been increasingly recognised as a level for inducing improvement in quality and performance in health care systems. However, writers in the area argue that there is no single or correct definition of organisational culture (Bellot 2011, Mannion et al. 2008) and that is subject to change. This makes it more difficult to grasp, understand, introduce and measure. Whether or not this causes any problems on the ground is unknown as others argue that for people running organisations, culture is likely to be self-evident and doesn't require explanation (Kirkley et al 2011).
Nonetheless, a wide-ranging set of theories and opinions have been set out over the last 30 years which explore the characteristics of organisational culture. It can be as simple as ‘the way we do things round here’ (Balogun and Hayley 2004). Or more complex as the approach proposed by Hawkins (1997 referenced in Doherty et al 2013) that comprises five levels. These include organisational policies and procedures, behaviour, organisational mind-set, emotional grounds and motivation. Schein (2004) presents a refined version of this approach which outlines the importance of: artefacts: dress code, mission statement, annual reports etc. values: ideologies and charters assumptions: thought processes, feelings, behaviour.
Martin and Meyerson (in Wilson 2001) argue that there are three major perspectives which can sum up different cultures: Integration perspective: organisation-wide consensus on one type of culture and
conflict could result in dysfunction. Three main types suggested are ‘club’ or ‘clan’ culture, ‘hierarchy’ culture and ‘competitive’ culture (Austin and Claassen 2008).
Differentiation perspective: culture that exists in the boundaries of sub-culture that can co-exist in conflict or harmony.
Fragmentation perspective: no organisation-wide culture or sub-cultures and people are influenced by events or issues.
These classifications may be useful for those considering culture change in order to assess current position and future vision.
Culture of care in social careIn social care, the culture of care is receiving more attention now than ever. The Care Quality Commission (CQC) openly talks of the need for regulation to support a culture of quality, safety and openness. Indeed one of the top ten changes they have stated in their
34

recent publication A fresh start for the regulation and inspection of adult social care (CQC 2014) is to “focus on leadership, governance and culture, with a different approach for larger and smaller providers”.
Recent reviews (Department of Health 2012a) have also stated the importance of culture focusing on a ‘culture of compassionate care’ supported by leadership, training and collaborative working. In addition, the recent review of Winterbourne View Hospital (Department of Health, 2012b) stated that ‘dysfunctional and malignant culture of care’ was one of the factors that contributed to criminal actions against vulnerable adults.
Characteristics of positive cultureIn a recent think piece Sheard (2014) suggests that in order to transform organisations and achieve a national culture of compassion, we need to first understand what ‘good care looks, sounds and feels like for people living and working together’ (pp329). He typified four different models of care: 1. Old culture / traditional: emotionless organisations where staff are detached, emotions
are suppressed and the focus is on task-based care.2. Confused service: Service exposed to new beliefs in person-centred care with no
implementation so still task-based but now a philosophy based on hierarchy of needs and person-centred care. This can lead to staff stress and burnout as working across two models of care.
3. Creative service: introduced some new cultural approaches but mixed with old culture actions. No clarity that lack of training and lack of person-centred approach to staff teams is defeating the purpose of the new approach. The approach is likely to involve attached staff, person-centred beliefs, philosophy of care based on emotions but confused task-based care.
4. Congruent service: this is an emotion-led organisation which has grasped the concept and is implementing training to support beliefs and action compatible to people living and working together.
The last of these typologies is the ultimate goal for culture change and some factors that help attain this type of culture are outlined in Table 5 below. Some of the characteristics identified reflect facilitators of culture change more widely as described in Table 5 below.
35

Table 5: Elements of facilitators to promote culture change
Strong leadership, senior management support and commitment and organisation-wide awareness and commitment to change
NHS NIHR 2009
Hernandez et al 2013
Hardacre et al. 2011
IRISS 2012
SfC 2014
Kennedy 2014
Understanding of current organisational culture and clear lines of communication around what is expected and ‘normal’ for the workplace
SfC 2014
IRISS 2012
Ongoing organisational learning and development with support for staff
NHS NIHR 2009
SfC 2014
Rondeau and Wagar 2006
Hernandez et al. 2013
Dowling et al. 2006
Kennedy 2014
Support for innovation and positive risk taking
NHS NIHR 2009
SfC 2008
Hardacre et al 2011
IRISS 2012
A clear vision IRISS 2012
Hernandez et al 2013
Involvement of stakeholders Deutschman 2001
Shaping our Lives, National Centre for Independent Living and University of Leeds Centre for Disability Studies (2007)
Hardacre et al. 2011
Hernandez et al. 2013
Dowling et al. 2006
36
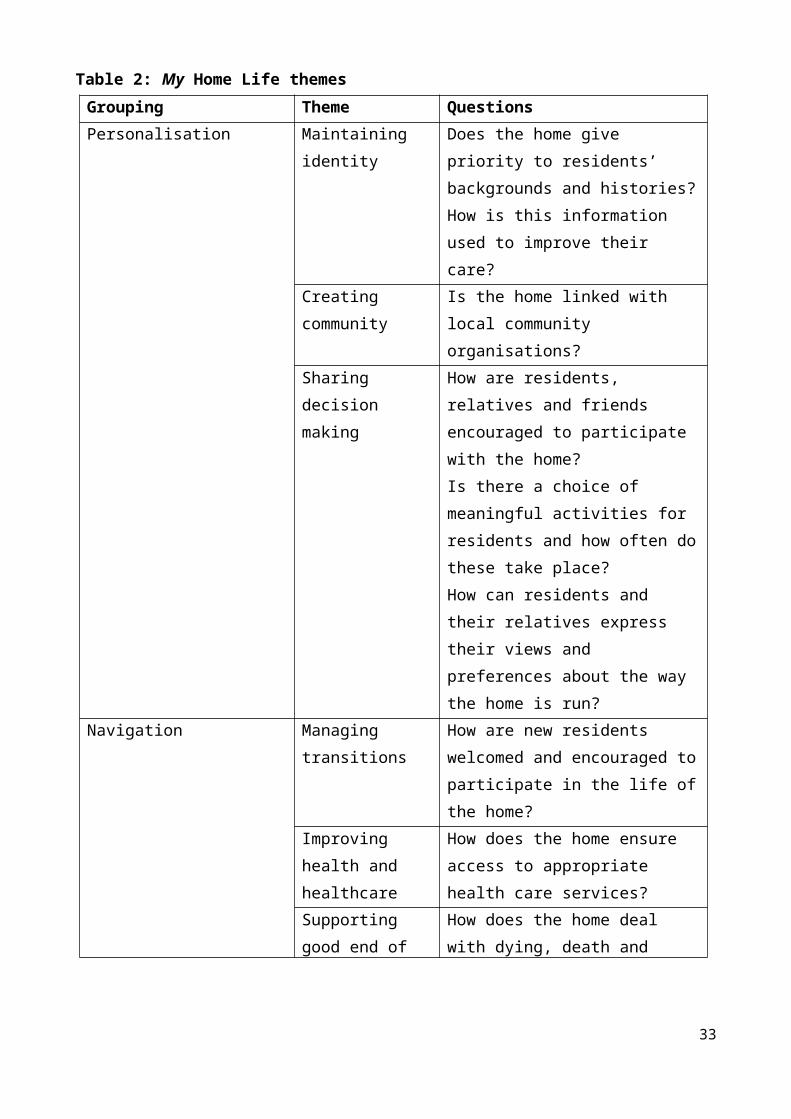
Tools to help with culture change in social care A number of tools exist to help assess culture but often they have not been subjected to evaluation (Bellot 2011). There is no ideal instrument but two of the most rigorous are the Organisational Culture Assessment instrument and the Organisational Culture Inventory according to Bellot (2011). These are generic tools which can be applied to different organisational types for example; the Organisational Culture Invention has been used in health care settings.
In the social care sector tools are emerging to help organisations think about culture change and how to manage the change process. Skills for Care (2014) have produced the “Culture for care: your toolkit”. Based on evidence and feedback from employers the toolkit outlines what a more positive culture looks and feels like. It also highlights the potential benefits of a more positive culture, and provides guidance to help employers move toward this goal.
The impact of organisational culture While policy and guidance point out the importance of culture, there is only weak evidence to link culture to positive outcomes for residents (Kirkley et al 2011). Three evidence reviews identified focused on culture change in care homes (Hill et al 2010, Andre et al. 2013, Shier et al 2014).
Hill et al. found that regardless of the culture change model, all embraced the same core belief that by transforming institutions into communities, residents and staff will thrive. They focused on physical and psychosocial health outcomes for residents and found that while the evidence for improved physical health outcomes was mixed, there were clear benefits to outcomes like depression, helplessness and wellbeing. However they also state that the evidence in this area is underdeveloped and more is needed to fully determine the extent of the impact of culture change on care homes.
Andre et al. identified 10 studies for their review and concluded that work culture was linked to the quality of care in nursing homes. In particular, leadership style, supportive management, increased empowerment and participation are all linked to organisational culture.
Shier et al. identified 36 studies for inclusion in their review and concluded that culture change in nursing homes is an evolving field but that the current evidence does not give sufficient information for selecting interventions or approach based on expected outcomes. More work is needed to determine the impact of change on quality.
One large-scale study from the US is worth including as they found nursing homes that had undergone culture change toward more person-centred care had better quality with few health-related issues (Grabowski et al. 2014b).
37

Summary Organisational change and culture change are increasingly attracting attention as a possible way to drive through improvement in care homes. For example, the CQC have included culture of care as part of their new inspection agenda. While various theories of general organisational culture are available, there is little care home specific information and very little work has been carried out to look at culture of care and outcomes. What exists supports culture change to transform institutions into communities where residents and staff are fully involved. Again there are overlaps with person-centred and relationship-based care in terms of the approach and facilitators. Culture change is supported by strong leadership, clear understanding of existing culture, commitment to change, support for innovation and a clear vision of direction of travel.
38

6.3 Skilled and positive workforce who are fully supported
Having the right staff in place, good staff communication, effective learning and development for staff are at the heart of any change in care homes especially when considering change within the organisation.
This was reflected in the consultation where communication in particular was seen as a lynchpin of successful change management. The managers involved described a range of approaches to two-way transfer of information including staff meetings, open door policies, hands on managers etc. Managers talked about the importance of communication and the significance it played in the management of the home.
‘I don’t put any changes in place without telling staff, I like to sit down and talk to them and explain why.’ (Manager)
Without this firm foundation in place, staff can experience stress and burnout. Stress and burn out have been identified as a particular issue for staff in residential care settings. In particular, those working with groups whose behaviour can be described as unpredictable or challenging (Burtney et al. 2014).
Wild et al. (2010), in their evidence review would support this and highlight the importance of providing support through a time of change as this has the potential to increase both stress levels and staff burnout. They also found that change often requires new roles that can compound the situation if the correct support is not in place.
Support for staffWhile personal attributes can provide staff with resilience to absorb stress, there are techniques and supports that can be put in place to reduce the effects of stress and burnout. Various responses to staff stress and burnout have been documented including organisational approaches (e.g. a positive working environment and culture, good policies.), team level (e.g. peer support, good leadership and management, supervision) and individual (e.g. self care, education and training; especially around communication skills and understanding residents behaviour). (Burtney et al 2014).
These approaches are being realised in practice. Through the consultation, staff and managers described a range of opportunities on offer, focusing on induction for new staff to explain the philosophy of the care home, the role of staff and person-centred care. Depending on the care home, other training focused on the needs of residents, e.g. dementia training, peer to peer learning and shadowing to learn practical aspects of individual care.
‘[The owner] is committed to valuing the staff and supporting the staff to understand the culture.’ (Staff participant)
39
Managers and staff also placed a strong emphasis on the ‘team’, mutual understanding and good support structures.
‘We just support each other. We're like a close knit family...I just know if there's something wrong with one of my staff members when I see them & they know I'll be here for them when they're ready to talk.’ (Staff participant)
‘We focus on developing relationships with staff – we ask staff how they feel and they say they feel taken care of when they start working here and throughout…nurturing staff is vital if we want them to nurture residents.’ (Manager)
Schwartz Center Rounds approach to reducing stress‘Schwartz Center Rounds©’ are a practical tool that health and care providers can use to improve their organisational culture and support for staff. Supported by the Point of Care Foundation, the approach has now been implemented in 70 organisations across the UK. While this has been predominantly across health settings, there is potential for care settings to use the approach. The ‘Rounds’ bring together staff in a multidisciplinary forum to discuss non-clinical, social and emotional aspects of caring.
Evidence of impact As this is a recent concept in the UK, the evidence is limited. However, Goodrich (2012) conducted some work in hospitals to determine if the approach had transferred from the US to the UK. She concluded they were perceived as a source of support, and that the approach had the potential to translate into benefits for patients, team working and organisational culture.
Staff attitude and values While it is important to support staff already in post, there has been an increase of emphasis on recruitment of new staff through policy and recent practice development in social care. For some time, children’s services have adopted a ‘value-based recruitment’ (VBR) approach whereby in addition to skills and experiences, job applicants are interviewed to assess ‘value fit’ with the organisation.
The reason for a focus on values is that everyone brings their own personal attributes, ambitions and reasons for wanting to work in their role. They cannot be treated as ‘empty vessels’ into which formal processes and organisational values can be transferred (Felce et al. 2002a, 2002b). Instead, employers need to consider how staff values, along with the setting (physical environment) and formal (policies and procedures) and informal (staff views and relationships) organisational culture combine to determine the outcome for people who need care and support.
40

Characteristics and values might be specific to individual job roles but there are some pointers from the research evidence which highlights core values for staff working in the care sector.
Staff should have the ability to: empathise rather than sympathise with people they are caring for show willingness to undertake a range of activities relevant to the individuals they care
for actively choose to work in their role which can indicate a level of job commitment have a strong sense of wanting to make a difference have behavioural and cognitive strategies for coping with difficult caring situations e.g.
death be clear of personal and professional boundaries. Sources:, Kennedy 2014, Bates et al. 2012 reported in Burtney et al 2014, Pitt 2011, Brown Wilson 2007, Ablett and Jones 2007
Managers in the consultation also reflected on the need to have staff with the right values and attitude. Some described the need to ensure new recruits understand and accept the ethos and culture of the organisation. Others talked about the challenges faced when new values are established as part of the change process, which do not sit comfortably with staff values.
VBR in adult social care The National Skills Academy, in partnership with Skills for Care and McIntyre, have developed a toolkit to help social care employers recruit using VBR. It focuses on organisational and personal value match with the aim of increasing the likelihood of ‘right first time’ appointments. The toolkit brings together: the ‘Leadership Qualities Framework for Adult Social Care’ which sets out what good
behaviour looks like at every level of the social care workforce example job adverts which promote social care values and give guidance for
employers when preparing their own online personality profiling questionnaire and resultant profile to give a basic profile of a
candidate’s value-base.
As well as employers considering the value match between staff and organisation, there is an increasing emphasis on encouraging potential recruits to consider their suitability for a career in social care. ‘A Question of Care’, a new video based resource, helps potential recruits understand what social care is really about. It enables people to assess suitability in terms of the values and attitudes that are regarded as important in the sector. Another tool, the Skills for Care etool, also sets out different job roles and expectations for potential recruits to encourage them to think carefully before entering the social care workforce.
Evidence of impact41

Within residential care there is limited evidence on value-based recruitment. Skills for Care (Goode 2014) conducted a pilot of the approach which yielded positive results. In particular, employers have found that inclusion of this approach has led to a more robust recruitment process. In addition, many of those involved in the pilot are reviewing recruitment practices to reflect this new practice.
One review of care in other residential settings did find some limited evidence of positive impact on staff and organisations when VBR was used in terms of staff retention, satisfaction and delivery of care (Burtney et al 2014).
Summary In summary, good recruitment and support for staff is a key theme for sustaining change. There was some available literature on the importance of securing the right staff in the first place, support for staff on an on-going basis to help with the stresses of work, and the need for strong communication about any planned changes, learning and development to support change and engagement with staff to ensure smooth transitions.
42
6.4 Stakeholder involvement Service user involvement, shared decision-making, and user participation are all ways of ensuring the voice of residents is evident both in their own care but potentially in the broader provision of care in a home. Policy states the need to involvement stakeholders (Department of Health 2007, 2008b) and charges organisations with developing systems of effective engagement supported by skill and trained staff and within a culture of strong and committed leadership.
The literature also reflects the importance of engagement with service users to ensure care changes according to needs (Davies 2001, Innes et al. 2006, Help the Aged 2007). Falkner (2012) in a review of the literature specifically highlights risk assessments and decision-making about risks as key points for engagement. Others support his argument that it would be impossible to deliver person-centred care without shared decision-making and a rethink of the power relationship between residents and providers (Dowling et al. 2006).
However a recent study (NDTI 2009) indicated that the voice of older people who need care and support is largely absent and they found evidence that family and professionals speak for them. They concluded that we need a deeper understanding from older peoples’ perspective of what needs to change in order for them to have a good life, rather than relying on view of others about what constitutes a high quality service. This view was supported by others (Worden and Challis 2008) who found only 16% of care homes in their study of care homes (182 responses, 118 copies of care plan documentation) specifically asked for a resident’s signature or agreement.
Again the lack of users’ voice was noted in the commissioning process (Schehrer and Sexton 2010). The authors concluded that credible user involvement in service commissioning is far from being achieved and that skills, knowledge and practice of commissioners are limited in his area.
Models of involving stakeholders There are different approaches to involving stakeholders in decision-making. For example, Help the Aged (2007) have identified four main models of decision-making in care homes in their literature review: 1. Authoritative: externally imposed by policy or determined by corporate function. 2. Given: a set of taken-for-granted decisions, which define culture of the home.3. Negotiated: largely individualistic decisions resulting in interaction between various
stakeholders. 4. Reflexive: autonomous decisions made by individuals through a process of self-
deliberation.
43

Certainly the last two models of operating outlined above sit better with person-centred and relationship-based care described above.
Effective engagement Working within a framework of effective consultation and engagement, the literature offers some facilitators for effective engagement: an agreed framework for involvement jargon free and accessible language awareness of the external pressures and context for strategic decision-making decisions based on needs assessment of users and significant others ongoing monitoring and evaluation to gather intelligence and feed into the needs
assessment openness and transparency about budget availability with service users identification of decision-making points in the cycle as there will be more than one
opportunity to involve service users good understanding of service users concerns and fears a review process and allow time for organisational learning.Sources: Schehrer and Sexton (2010), Dowling et al 2006
Of interest, there is a website (Care Opinion part of Patient Opinion) which offers everyone the right to share experiences of the social services they use. The site endeavours to make sure the comments get back to the right person and participants have the opportunity to see to services respond to comments (www.careopinion.org.uk).
Co-production as an approach Some social care employers have moved towards co-production as a way of increasing involvement, sharing decisions and shifting the power balance. This more involved approach moves beyond listening to the voice of residents and treating people as passive recipients of services. Rather it involves residents in collaborative relationships with more empowered frontline staff able to share power and accept user expertise.
Needham (2012) argues that co-production can have the power to transform thinking about power distribution, partnerships and outcomes. However, success in co-production is reliant on trained staff able to recognise the benefits of co-production and support positive risk-taking and new commissioning, financial and regulatory structures to embed the approach.
Co-production in practice Perhaps an example of co-production at a practical level can be illustrated through the Oomph Wellness initiative (www.oomph-wellness.org). Based on co-production of classes with older people, the emphasis is on fun, participation and engagement. This social enterprise organisation has documented some impact of the work and claims to have 81%
44

improvement in social interaction, 75% improvement in mental stimulation, 67% improvement in mobility and 28% reduction in falls. Currently they work in over 750 care homes in England.
Advanced Care Planning (ACP) is a good example of co-production focusing on end of life care. It is defined as ‘a voluntary process of discussion and review to help an individual who has capacity to anticipate how their condition may affect them in the future, and, if they wish, set on record: choices about their care and treatment and/or advance decisions to refuse a treatment in specific circumstances’ (NEoLCP 2011). It relies on relationship-based care and good training and support for staff. The approach is being increasingly used in care homes with some evidence of improved satisfaction in care delivered, improved mental health, and increased confidence in staff (Stobbart-Rowlands et al. 2012, Detering et al. 2010, NEoLCP 2010b, Clifford et al. 2007).
Co-production was very evident in the care homes we visited. There was clear involvement of staff, residents and families in both developing individual care plans and more generally the running of the care home to various degrees.
‘Everyone is involved in developing the service including residents and families, for example, the change from wearing uniform to no uniform. Discussed and agreed by everyone. This has made the home more open and feels more like a home not a hospital.’ (Staff participant)
‘We try to make residents feel as important as possible, for example we do quite a bit of fund raising and we meet with residents and families to decide what to spend the money on.’ (Manager)
Evidence of impact There is some evidence that if implemented properly, co-production can deliver: value for money social capital improvement in service delivery potential physical, social and health benefits for residents.Sources: Oomph Wellness 2014, Needham 2012
Involvement of the wider community There have been recent moves to foster community engagement beyond the care home itself. For example, the National Care Home Open Day is supported by the Department of Health, CQC, National Association for Providers of Activities for Older People and SCIE. This is an attempt to present care homes in positive and proactive light and make lasting connections between local communities and care homes. However, there is little evidence available of the impact of wider community engagement in relation to care homes.
45

Another example of active engagement with the community is the work of My Home Life. In Essex, they have developed a community association (My Home Life Essex Community Association) that promotes links locally through advice, support, volunteering and befriending schemes. As part of this work they are piloting three approaches: The ‘Community Visitor’ ‘Community Friends and Neighbours’ (FaNs) ‘The Big Conversation’.
FaNs encourages individuals, local groups, schools, colleges, and businesses to take an active interest in the wellbeing of people living in care homes in the local area. It is a three year programme funded by Essex County Council and is a collaborative effort of members not an organisation. FaNs do not join a specific organisation but are asked to take on a role to build up and keep going with support from the scheme.
The Community Visitor aims to recruit community volunteers to visit a care home once a week for a couple of hours to befriend members of the care home community, act as critical friends and informal advocates and witness the evolving culture of the care homes. There is evidence to suggest that this helped reduce isolation, encourage involvement and increase choice among residents. Staff also felt more supported and community visitors felt that benefits were evident (Tanner 2014).
Finally, The Big Conversation which sets out to engage in conversation with the public directly about care homes. This project, led by My Home Life, aims to raise public awareness about what make a good life in care homes now, what could make them better, and how might we get there. The vision is to open a dialogue about quality improvement, engage the public in better understanding of care homes and offer a creative way to meet requirements around user and carer involvement.
Summary In summary, working together to improve care through involving management, staff, residents and families would appear to have some limited support from available evidence. There are different levels of engagement, at an individual level for care planning and advance care planning, at a community level to help with the running of the care home and to feed into decision making at this more strategic level, and with the community to ensure a sense of wider participation.
46

6.5 Strong leadershipRecent policy and research has identified leadership as important in changing culture within social care organisations (e.g.HM Government 2012, Skills for Care 2011, Department of Health 2008, 2010, Dowling et al. 2006, Brown Wilson 2007, Szczepura et al. 2008, Wild et al. 2010, Hardacre et al. 2011, Castle and Decker 2011, Owen et al. 2012, NSA 2012, Keating et al. 2013, Kennedy 2014).
Strong leadership was also identified as a key theme from the consultations. Both staff and managers were clear that change would not happen without strong leadership.
‘Leadership is very important to know that they will listen, but also be firm.’ (Staff participant)
‘Staff did find it hard…but I developed a level of resilience because I firmly believed that this is how things needed to be. If I caved in at every obstacle I came to I would never have achieved anything…staff realised that they were either going to be on board and changes were going to happen or that changes would happen without them.’ (Manager)
What is leadership? While there has been growing interest in leadership in social care, little is written on what exactly this looks like (Owen et al. 2012). Some suggest there are distinct styles of leadership. For example, transformation leadership when whole systems changes are being made, transitional leadership for stepped change, and situational leadership that changes depending on the circumstances (Lynch et al 2011).
Lynch et al. (2011) set out four sets of leadership behaviours which can be adapted for different situations. These are based on high and low supporting behaviours (e.g. listening, providing feedback and encouraging) and high and low directing behaviours (task-related behaviours e.g. demonstrating, instructing and monitoring): High directing / low supporting: ‘directing’ as leader defines roles and gives
instructions High directing / high supporting: ‘coaching’ as leader giving direction but two way
communication Low directing / high supporting: ‘supporting’ as locus of control for daily decisions
lies with worker Low directing / low supporting: ‘delegating’ as workers have a high degree of
autonomy.
Others argue that leadership is conceptually driven and there are very few theories that emerge from empirical research (Tamkin et al. 2010). Tamkin et al. (2010) conducted a major piece of research with leaders in six major organisations to find out more about what leadership meant in practice. They identified three ‘big ideas’:
47
Thinking and acting systematically is central to leadership: outstanding leaders understand and consistently act in the knowledge that reaction follows action. Management and leadership follow seamlessly and they attend to the current and the future.
People are the route to performance: time given to others builds social capital within and between people. Outstanding leaders understand that outcomes such as quality are achieved by engaging with others, entrusting them, growing them and creating conditions of trust and passing power.
Outstanding leaders understand they achieve through their impact on others: personal ego does not feature and they are aware of the need to use themselves with care and respect, with full self-awareness and reflection.
Leadership in social careThe NSA joined with The Work Foundation to focus on what the Tamkin report meant for social care (Pearson et al. 2011). The authors compared social care to the original private sector study and found commonality around creating a positive vision, environment and relationship, empowering people where possible, promoting excellence and communication, appreciation of strengths and good systems.
However there was some difference particularly as social care leaders have a vision that extends beyond their own organisation, their passion was described as ‘almost tangible’ and a much stronger sense to inspire others with the same passion was noted. The authors highlighted social care leaders did not appear as confident as those in the private sector and there was an absence of the notion of team spirit and collective achievement, something more pertinent perhaps in private sector, that have a focus on encouraging self-sufficiency in teams. Pearson et al. concluded that ‘the key to building outstanding leadership in social care is to enhance its existing strengths around inspiring a passion for purpose, developing people, relationships and networks, and working in collaboration to deliver the highest quality of care’ (Pearson et al. 2011, p11).
Owen et al. (2012) also did some work to identify attributes of good leadership in care homes. Leaders will be supported from the top of the organisation and be transformational managers who are able to: get the right staff in place to help with change help staff to engage with their work support staff and role modelling develop an environment conducive to relationship-based care work in partnership with external organisations.
They also identified nine outcomes of good leadership in the care home sector: a confident and resilient manager a confident, stable and committed workforce
48

greater engagement with external bodies and communities a reflective, questioning workforce taking initiative and ownership care home that positively welcomes complaints a vibrant community of older people greater spontaneity and responsiveness greater emphasis on positive risk-taking supporting greater community inclusion.
From the consultation managers and staff described characteristics of good leadership. For managers this was the need to bring staff along with change leaders as part of a smooth transition process. Staff described the importance of access to managers and leaders. They highlighted the importance of an open door policy, where management was available to discuss issues and help with any issues or concerns staff might have.
Obstacles to good leadership in social careObstacles to good leadership have been identified in the social care literature. These centre around the challenging relationship between care homes and regulation, and includes difficulties in supporting positive risk-taking and managing tensions with the safeguarding agenda. The lack of clear support from owners or the provider organisation for managers may also be a challenge (Owen et al. 2012, Help the Aged 2007) and can lead to a sense of isolation. This may be increased by the lack of recognition of positive moves but blame culture when things go wrong also hamper change (Wild et al. 2010).
Support for leadership in social careThe NSA strategy (NSA 2013) built upon this research and developed the Leadership Strategy (‘Leadership Starts with Me). This strategy sets out values, principles and qualities upon which strong leadership in social care should be set (see Table 6). The strategy supports the notion that leadership needs to happen at all levels across an organisation and is not the domain of managers.
49
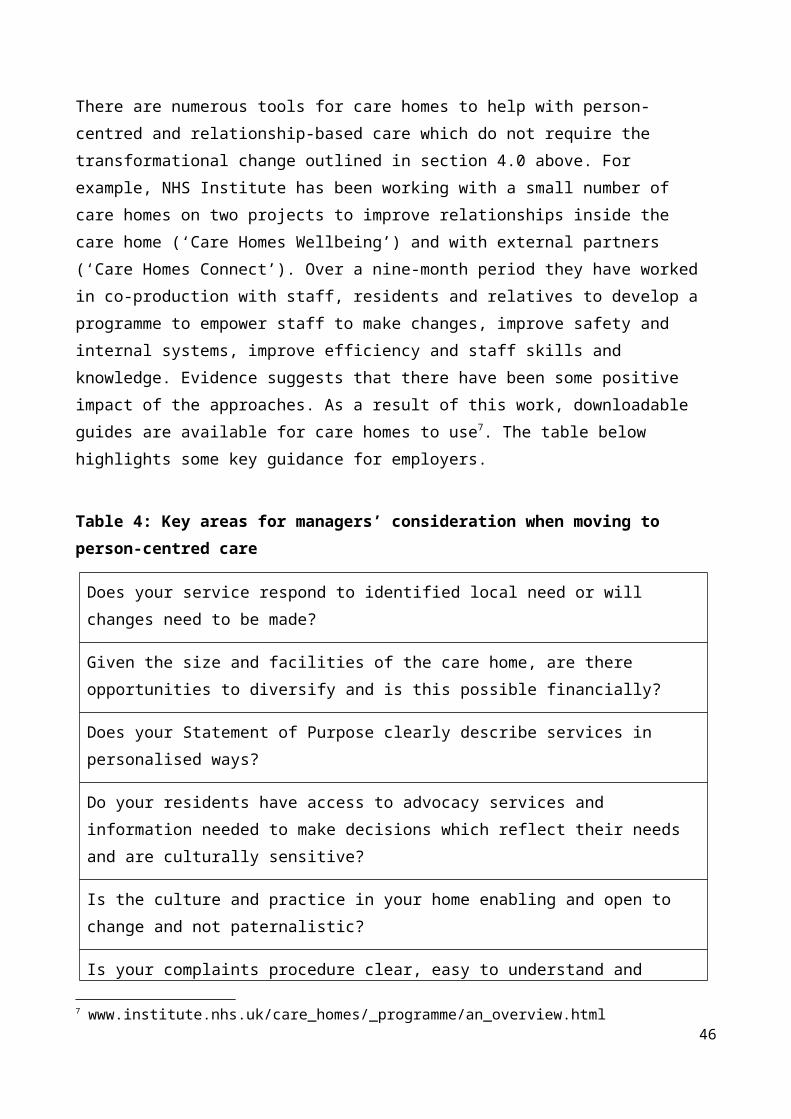
Table 6: Leadership starts with me (NSA 2013)
Values Principles QualitiesIntegrity Social purpose Demonstrating personal
qualitiesDignity Co-production Managing servicesCompassion Innovation Creating the vision and
delivering the strategySupport Improvement Improving servicesGrowth Integration Working with othersPrinciples Risk and Responsibly Setting direction
This again is reflected in the Leadership Qualities Framework (NSA 2013) which takes each of the qualities outlined above and talks about what leadership looks like for each of the dimensions for front-line workers, front line leadership, operational leaderships and strategic leadership. This work is supported by case studies, an app for smart phones, online discussion forums, events and online video clips in order to maximise the impact of the strategy.
Other initiatives, for example My Home Life, have a strong leadership element built into the programme and evaluation has provided evidence for leadership in improving the environment, and improving and supporting transformation among other outcomes.
SummaryStrong leadership was identified through policy, literature on organisational cultural change and while there was limited evidence specifically linked to social care, there is a developing body of tools to help support leadership in social care. For example, a recent report based on findings from the private sector highlighted strong leadership as the ability to create a positive vision, environment and relationship, empower people where possible, promote excellence and communication, appreciate strengths and good systems. This was applied to social care and extended to include the strong sense that social care leaders have to inspire others. Others working to deliver models of change in care homes have incorporated leadership skills into their approach as a central pillar.
50
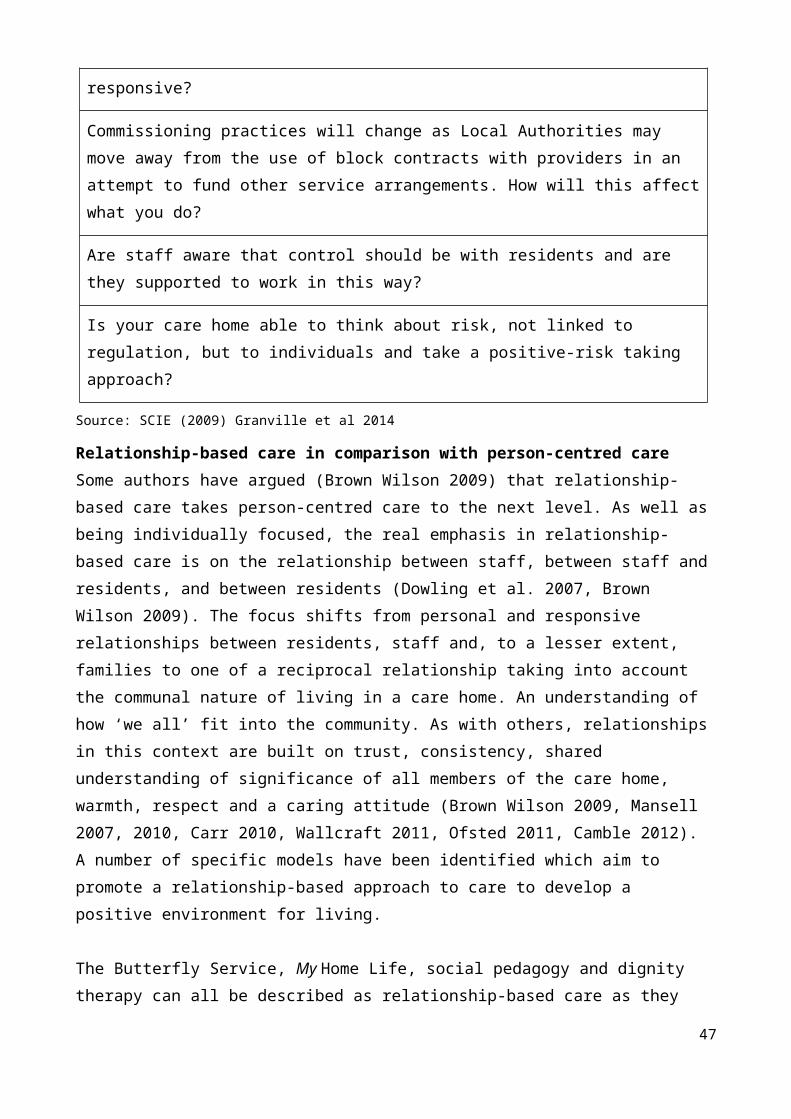
6.6 Positive physical environment The importance of the physical environment has been reflected above and in policy (Department of Health 2008). Characteristics to improve experience of care for residents, families and staff, were identified in the literature (see Table 7).
Table 7: Characteristics of a positive environment
Characteristic Description
Homeliness Patients wanted to feel ‘at home’ in the setting and some studies reported personalising space with their belongings to make it feel more like home.
Single rooms Research suggests some patients and family members prefer single rooms for privacy, more control etc. while others preferred distraction of a busy ward but prior discussion to establish preference is key.
Proximity to family
An important aspect was proximity for family and friends to visit and maintain that closeness of relationships.
Space for social interaction
Some patients were keen to remain socially active as long as possible, to use lounges and dining areas and engage in mutual support. However, choice is the key as not everyone will want to interact.
Facilities for families
Having adequate space to accommodate families overnight as well as administer medical tasks, have care discussions, etc. is important for staff and families alike.
Spiritual places Often an important aspect for older people, the need for a place to worship or meditate was felt to be beneficial to the levels of satisfaction expressed by patients and families.
Sources: Brereton et al. 2011, Rigby et al. 2010, Waller et al. 2008, 2011, Brown Wilson 2007
The theme of a positive environment was reflected in our consultations where we heard of care homes taking decisive action and working with residents and families to make care homes more ‘homely’. At one extreme, a care home had reformatted their environment to move from one large lounge to four more comfortable and ‘homely’ lounges. They had also built a ‘street’ inside with a sweet shop, post office and green grocer. Others had given each resident their own address and doorknockers to make it less institutionalised. Other examples include personal furniture, subtle colour scheme, personal effects etc. to increase the warmth of the home. In addition, participants were able to describe changes
51

they had made for people with visual impairment including themed corridors, plain carpets, adapted flats etc.
Evidence of impact There is some limited evidence that a high quality physical environment can impact on care experiences and outcomes for residents (Waller et al. 2011, Parker et al. 2004) although more evidence is required to form more conclusive answers.
Summary Characteristics of a positive environment to support improvement in care quality and change in culture and care delivery have been highlighted in the evidence. However, there is limited published research evidence on the effectiveness or impact of changing the physical environment. Characteristics include homeliness, proximity to family, contact with the natural world, facilitates for family interactions, option for single rooms and attention to colour and décor.
52

7. Benefits of the changes that have been made
OverviewThe evidence of impact was very limited although some formal evaluation did indicate positive outcomes for residents’ physical and mental health, as well as improvements in staff satisfaction borne out through a reduction in staff turnover. More anecdotal evidence and consultation with care homes themselves, while it should be treated with caution, gives some insight into the potential benefits of change.
Benefits for residents included flexibility, greater choice, a more creative and stimulating environment, a sense of purpose, something to look forward to in their day and scope for individual focused approaches. For families benefits included a sense of trust and confidence in the care that was being delivered allowing them to concentrate on other things.
Benefits for staff included job satisfaction, autonomy increased career and development opportunities, a more positive working environment, increased confidence and improved staff morale. Organisations were also likely to benefit through more stability in the workforce as well as improved reputation locally.
7.1 The impact of change The models of change identified through this research had some limited information available on the impact of change. The data is weak however, as much is based on anecdotal evidence rather than formal evaluations of the approach and should be treated with caution. Nonetheless, some of the key themes that emerged were substantiated through our discussions with care homes and are presented below.
From the published and grey literature, it would appear that a new approach to care delivery focused on the individual and relationships has the potential to improve outcomes for residents and staff alike. For example, through the ‘Butterfly Service’ residents were found to have an increase in weight, a reduction in medication usage and falls. Staff also benefitted through a reduction in sickness and the organisation seemed better at retaining staff.
With the Eden Alternative, limited published evidence indicates the benefits include an improvement in depression scores for residents, an improvement in family satisfaction and, anecdotally, improved physical and mental health for residents was supported. The social pedagogic approach is well established in Europe and in the UK is more widely used in children’s services compared to adult’s services. Again positive outcomes for
53

residents were described but it isn’t possible to consider the outcomes for staff as they were trained to behave in this way so no change had taken place.
A formal evaluation of My Home Life described the benefits to staff and managers in terms of improvements in staff empowerment, changes in delivery of care and the positive impact of a ‘no-blame’ culture in terms of a more balanced and creative approach to risk.
The consultation with care homes really highlighted the benefits of change and while the sample is clearly small, and therefore should be read with caution, the responses were consistent across all five care homes and can give some insight into the potential for quality improvement if culture change is taken seriously. Participants reflected on the benefits of culture change focusing on benefits for residents, families, staff and the organisation itself.
7.2 Benefits for residents Benefits for residents included flexibility, greater choice, a more creative and stimulating environment, a sense of purpose, something to look forward to in their day and scope for individual focused approaches.
‘The biggest impact on residents is us being focused on the individual … we have replaced things by working around people and bringing things to them … we are flexible in how do things.’ (Staff participant)
‘One of the biggest changes was to encourage staff to walk and accompany people, get out and about and feel better for being out in the garden. Do things with people and be flexible …. It’s a lot more relaxed.’ (Staff participant)
One manager also described the benefits to families who previously might have been the main carer but were now able to take a step back and be confident that their relative was being well looked after and give them some time back for their own life.
‘Trust is there – that things will be deal with straight away.’ (Manager)
7.3 Benefits for staff Benefits for staff included job satisfaction, autonomy, increased career and development opportunities, a more positive working environment, increased confidence and improved staff morale.
‘It's totally different, and I struggled with it to start with, but I couldn't go back to the old ways now.’ (Staff participant)
54

‘I have seen staff really develop confidence and feel good about themselves.’ (Staff participant)
‘Stress levels [amongst staff] have really gone down, sickness has dropped and the atmosphere is calmer and more relaxed.’ (Staff participant)
‘It just feels right. It's so natural now for us to work like this and I can't understand why anyone else doesn't do it like this and why we didn't do it before.’ (Staff participant)
‘Staff look happier, appear friendlier when they come to the door and their body language is completely different.’ (Manager)
‘Staff are more confident in how they approach the care and are more relaxed and willing to ask for help.’ (Manager)
There was some recognition of the challenges however, that staff face in maintaining change.
‘You need to sustain staff. To start with it might be hard as staff can be set in their own ways. Now we accept things and know that they work well for the team.’ (Staff participant)
‘Change isn’t always easy, in fact it can be very difficult and uncomfortable but it’s worth doing.’ (Staff participant)
‘It’s about the team sticking together and creating what we want to create because it's very easy for staff to flick back into being task orientated. There are times when you have to pull a member of staff out of a lounge to say 'do you know what you've just said?' and usually it's a genuine mistake and they feel awful, but you have to constantly reinforce it.’ (Staff participant)
7.4 Benefits for organisations Broader benefits for the organisation were important as well.
‘[The organisation gets a] good name, proud to work here, very good feedback from families and residents, nice atmosphere when you walk through the door.’ (Staff participant)
‘I am feeling more confident with being a leader – more confident in myself and more supported by my team.’ (Manager)
55
7.5 Sustaining change Managers reflected on the need to sustain successful changes and this happens through a number of routes starting with staff recruitment.
‘To embed the culture? When we’re recruiting people, from day one, staff have to accept out ethos and culture.’ (Manager)
‘We recruit for values but this means that it is hard as there are never enough of the right people available for this work … and we are strict so if someone is not working in the right way they don’t stay.’ (Manager)
‘There are practical considerations for people who don’t fit into the process for whatever reason – you need to be able to cope with the exceptions to the rules.’ (Manager)
Once recruited, managers make a clear effort to promote the culture of care to new staff. One manager runs staff induction days so new members of staff get to hear the messages from the top and interact with the manager from the start. The manager has also set up meetings with new staff to hear their views and makes herself available for informal chats with all staff. Others described on-going supervision sessions which have all of the benefits of allowing people to discuss the practical aspects of their job in a positive environment.
The reality for some managers was that to maintain the changes, staff had to rise to the challenge or leave the care home. Some managers described the difficulties some experienced staff had with the more flexible approach to care and in some circumstances the only way to move forward was to recruit new staff members.
Others highlighted the need to work with commissioners to make sure they are on board with the process and are clear on their objectives and what they are trying to achieve through the change process.
7.6 Summary There is some limited formal evaluation to support change from traditional to the more person-centred approaches to care identified in through the REA. More support was gained through the consultation with organisation who had been through a process of change. Managers and staff were able to identify benefits for the organisation, staff, residents and families alike. Sustainability was a key issue for managers and some facilitators to maintaining change were identified through the consultation.
56

8. What do staff need to know and understand about visual impairment to be able to offer person-centred care and assess person centred risks?8
Overview
There is useful information available on the issues facing undetected sight loss among older people in care homes. In addition, there are some pointers in the literature to help with skills identification and key considerations for staff working in care homes. What appears to be missing is insight as to how sight loss is included in person-centred and relationship based care, or how models of change have incorporated this aspect of care planning. Feedback from the consultation supported detecting sight loss as one aspect of person-centred care and there were examples of changes that had been made to support an older person with detected sight loss.
This REA focused on the key question “What do staff need to know and understand about sight loss to be able to offer person-centred care and assess person-centred risks within the context of models of change?” There was no specific literature which addressed this point directly reflecting the limited available evidence on models of change in care homes more generally.
Some literature did identify particular issues for older people with sight loss including more difficulty in: accessing information, in communicating, with mobility and transport. In addition, there appears to be more potential to develop mental health issues and experience social isolation (Hodges and Douglas 2007, Dreer et al 2007, RNIB 2014). Specifically the RNIB (2014) did find some evidence that people with sight loss were involved in examples of poor treatment, and that indeed they found it more difficult to complain compared to other residents.
Watson and Bamford (2012) reviewed the literature around undetected sight loss in care homes and highlighted the key issues as: the lack of one specific pathway to sight testing in care homes lack of priority given to eye health with few specific mentions of sight loss in regulation
and policy lack of awareness of sight loss among key stakeholders eye health is often overlooked as a general health indicator 8 The researchers investigated whether there was any literature that suggests the effective models of change vary, depending on the characteristics of older people, including sensory deprivation.
57

limited time and organisational practices for informal sight checking while training materials are available, there is limited delivery due to restricted time,
staff turnover and other barriers.
They called for more research into the barriers to good health practices for care home workers, managers and providers to help tailor existing resources. No further work was identified which picked up on this call. However we did identify a small number of studies that offer some insight into potential areas for skills development among care staff to help build knowledge around sight loss. In particular, do staff have the ability to: recognise a deterioration in vision assess the individuals skills to navigate in a new or strange environment sensitively offer help when it is needed recognise emotional and mental health issues associated with visual impairment deal with emotional aspects of visual impairment be empathetic and have respect for individuality?Sources: Watkinson et al 2003, Sinoo et al 2012, NICE 2013, RNIB 2014
8.1 Existing supportThis is not an exhaustive list but gives a flavour of the work in care homes to help support residents with sight loss. In particular, the work of the Thomas Pocklington Trust has a strong theme of promoting the issue of sight loss in care homes, demonstrated through research, practice and guidance. “Seeing it from their side: A guide to recognising and supporting sight loss in your care homes” (RNIB 2010) is just one product from the RNIB which can help support staff recognise what they need to understand about sight loss and how to identify sight loss in service users.
Other organisations have worked with stakeholders and produced specific guidance for care homes .e.g. My Home Life has produced a guide for care homes which focuses on the quality of life for residents with sight loss. The booklet points out the signs of sight loss, experiences of people with sight loss, action steps for staff to take and top tips for staff supporting residents with sight loss.
Some support is available and at a national policy level, NICE states that older people in care homes should be cared for by people who recognise needs that occur because of sight or hearing problems and record these as part of their care plan (NICE 2013). The Vision 2020 Adult Sight Loss Pathway (2013) also helps set the agenda as it highlights the principles of best practice for service providers which include early intervention, rehabilitation, intervention to maximise function vision care assessments. Elements of the framework could be accessed by care homes, particularly around early intervention and rehabilitation.
58

8.2 Current practice Moving beyond the literature, we did speak to care homes about how sight loss was included as part of their service delivery and person-centred care. At one level, there were some examples of where adjustments had been made to the offer of care for people with visual impairment; this was the outcome of a person-centred process. Whether the issue had been sight, hearing loss or other physical considerations, was secondary. The process was to focus on the individual needs of residents and adapt accordingly rather than separate out people with visual impairment for special treatment.
In a way, this is supported by a small scale study which identified three aspects of care that inform decisions around care offered to people with visual impairment (Charles and Manthorpe 2009). First: independent living skills; personal care, social contact, physical ability etc. Second: emotional impact; adjustment to sight loss and support to adapt. Third: risk; the deterioration of sight brings with this obvious risk in terms of physical safety. The authors argue that these areas that are used in specialist assessment for people with visual impairment might well be shared by older people regardless of visual impairment. Indeed this could well be the case as the areas highlighted fall into line with current policy which is around maintaining independence and quality of life and reflects ‘typical’ areas covered in assessments and care planning for example, personal care, communication, mental health and wellbeing, meals and nutrition, activities of daily living, mobility, risks, relationships and social activities. The authors conclude by reflecting on the challenges and unanswered questions around potential inequity for older visually impaired people and the need for more evidence to determine the impact of different definitions used among staff, potential ambiguity in the assessment process and practice.
8.3 Summary The impact of undetected sight loss is clear in terms of quality of life for residents, but if and how this is incorporated into person-centred planning within a care home setting requires more attention. There is currently no available evidence on the extent to which this is included or the action taken as a result.
59

9. Conclusions and learning for others
This section provides an overview of the main points from the REA and work with care homes, extracting where possible, learning for others. However, it should be noted that one defining feature of this REA was the lack of evidence of effectiveness both in terms of models of change and the subsequent impact of characteristics identified that can help with change and care improvement.
9.1 Current delivery of careThe perception of current care provision is ‘traditional’ care which is task-focused and not person-centred. How far this perception reflects reality is not documented but it is fair to say that policy is constantly driving for person-centred care, choice and flexibility as far as possible. However, this is in the face of budgetary constraints which means that commissioners and service providers have to think differently about how services are sustained and improved.
New regulations coming into place are another consideration for service providers and commissioners with a strong focus on leadership and effective care. However, regulation as well as helping to strengthen services can be a barrier to care homes in terms of processes and on-going audit trails.
Public perception of care homes could be improved as it is often seen as a ‘last option’, a negative choice rather than a positive move in a care journey. The sector is acutely aware of the poor perception of care, often fuelled by media stories, and there is work underway to focus on the positive aspects of care delivery.
Care homes need to consider the implications of policy, new regulation and public demands in the context of their local care home needs and demands and within current commissioning processes. However, there is every indication that the drive to deliver person-centred care will continue and failure to review existing practice in line with these external changes is likely to have implications for the care homes themselves.
9.2 Organisational change in care homes There is a lack of care home specific literature available which looks at organisational change and the impact on quality of care. However, general change management literature would indicate that there are various types and stages of change which could be applied to different situations. For example, planned approaches to change require some prior thought and preparation to introduce and sustain change. Emergent processes are more rapid and often happen when organisations are required to respond to change.
60

Dealing with change requires understanding of the organisation, of staff and strong leadership to drive the change through. Within adult social care and the care home sector specifically there is little published work around theoretical approaches to change. While this is the case, there are some processes and tools which are recognised and used in adult social care to help with change management, and are based on change management theory.
9.3 Models of change in care homesIn terms of models which care homes could adopt to change culture and service delivery, the REA identified the: ‘Butterfly Service’, a programme specifically aimed at homes working with people with
dementia. The ‘Eden Alternative’ aimed at eliminating boredom, loneliness and helplessness for
care home residents. ‘Social pedagogy’ drawing on European experiences to improving relationship-based
care. ‘My Home Life’ which is a UK based model of care underpinned by evidence and
growing in popularity. ‘Dignity in care’ which is less of a model per se but policy focusing on transforming
services. ‘Devon Kitemark’ which has been based on evidence and shared between local care
home providers in the area to drive up quality. ‘360 Forward’ which allows care homes to benchmark current services, agrees change
and reviews progress.
While there is limited information on the theory and impact of models of change specific to adult social care and in particular residential care, there are good examples which are happening in practice. There is a need to ensure that current models continue to extend and review practice and share findings from evaluation with other care home providers. Employers wishing to make changes should seek out learning from others but there is more work needed to consider how best to make the connections between innovators and good practice and employers who are ready to make changes.
9.4 ‘Ingredients’ for successful change Based on these models, our work with care homes and findings from the REA more generally a number of themes emerged as important for moving care forward and changing the culture of care delivery. These included: Person-centred and relationship-based care A positive organisational culture of care Well supported staff
61
Joint decision-making and participation Strong leadership and supportive management A positive physical environment.
Person-centred and relationship-based care Person-centred care and relationship-based care are closely linked and focus on putting individuals and families at the heart of care planning and decision-making. Person-centred care requires attention to the whole person, facilitated by better relationships both between staff and residents but also the literature emphasises the importance of staff relationships for better outcomes all round. Fostering a culture of flexibility, positive risk taking and communication are all facets in their own right, but also form the back-bone of person-centred care. While the evidence base is currently underdeveloped, emerging evidence would indicate strength in this approach and positive outcomes for service users and staff. There are various supports for employers when considering the shift to person-centred care and models of care to help them with the transition.
More information is needed on the impact of person-centred care in care homes on organisational delivery, management, staff, residents and families. In addition, some work to examine the cost benefit implications or the social return on investment or social value might help care home owners and managers consider the case for differing models of change depending on their needs.
Organisational culture Organisational culture is increasingly attracting attention as a possible way to drive through improvement in care homes. For example, the CQC have included culture of care as part of their new inspection agenda. While various theories of general organisational culture are available, there is little care home specific information and very little work has been carried out to look at culture of care and outcomes. What exists supports culture change to transform institutions into communities where residents and staff are fully involved. Again there are overlaps with person-centred and relationship-based care in terms of the approach and facilitators. Culture change is supported by strong leadership, clear understanding of existing culture, commitment to change, support for innovation and a clear vision of direction of travel.
Staff supportSupport for staff is a key theme for introducing change. There was some available literature on the importance of securing the right staff in the first place, support for staff on an on-going basis to help with the stresses of work, and the need for strong communication about any planned changes, learning and development to support change and engagement with staff to ensure smooth transitions.
62

Working together to improve care through involving management, staff, residents and families would appear to have some limited support from available evidence. There are different levels of engagement, at an individual level for care planning and advance care planning, at a community level to help with the running of the care home and to feed into decision making at this more strategic level, with the community to ensure a sense of wider participation.
Care homes should consider a values-based approach to recruitment to ensure staff are suited to the organisation and the job. Beyond this, managers should remember good communication, good support and staff empowerment have potential to promote change in an organisation.
Joint decision-making Demands for future care provision focus on resident-centred care where staff enter into more of relationship with residents to understand their backgrounds, existing interests, preferences and care needs. In reality, older people are asking for a high standard of care in terms of staffing etc. but in addition, they are interested to see a more individual approach to care and some retention of independence and continued access to the wider community as part of this.
A key learning point for introducing changes was the need to involve stakeholders and to ensure effective communication channels. Again limited information on the impact was available but the evidence that does exist would suggest that people are more likely to demand this in future, staff are more supported and valued when engaged and there are potential benefits for the organisation in terms of staff satisfaction and retention. Care homes considering change should assess current systems for engagement and identify potential for higher levels of engagement in order to begin the process of changing care homes together.
Strong leadershipStrong leadership was identified as central to organisational cultural change through the REA and the consultation. While there was limited evidence specifically linked to social care, there is a developing body of tools to help support leadership in social care. For example, a recent report based on findings from the private sector highlighted strong leadership as the ability to create a positive vision, environment and relationship, empower people where possible, promote excellence and communication, appreciate strengths and good systems. This was applied to social care and extended to include the strong sense
63
that social care leaders have to inspire others. Others working to deliver models of change in care homes have incorporated leadership skills into their approach as a central pillar.
Strong leadership again was a theme that was consistent through our REA. Without leadership, the process of change faces more challenges and may not be instigated or sustained. However, the importance of leaders working with rather than dictating to staff and other stakeholders was highlighted. In addition, care homeowners should ensure that managers and leaders are supported and developed to ensure commitment to the change process, and resources available to make change happen.
Positive environment Characteristics of a positive environment to support improvement in care quality and change in culture and care delivery have been highlighted in the evidence. However, there is limited published research evidence on the effectiveness or impact of changing the physical environment. Characteristics include homeliness, proximity to family, contact with the natural world, facilitates for family interactions, option for single rooms and attention to colour and décor.
There is some support in the literature and from the work carried out with care homes that the physical environment can make a difference and changes to small, as well as larger aspects, can have a positive impact. One positive step for care homes considering change would be to audit the current environment, taking on board views from staff, residents and families, using existing audit tools etc. to identify where changes could be made now or in the future to encourage a ‘homely’ atmosphere and facilitate person-centred attention to detail.
One final theme that was identified through the consultation was the need to think about change rather than reacting to a set of circumstances. Reflect on the process, share the learning and above all, stop if it isn’t working.
64

10. References
Abbott, S., Fisk, M., & Forward, L. (2000). Social and democratic participation in residential settings for older people Ageing and Society (Vol. 10, pp. 327–340).
Academy, N.S. (2013). Leadership starts with me: The why, what and how of leadership in adult social care. London: NSA.
Adams, L., Beadle-Brown, J., & Mansell, J. (2006). Individual planning: An exploration of the link between quality of plan and quality of life British Journal of Learning Disabilities (Vol. 34, pp. 68–76).
ADASS West Midlands, Joint Improvement Partnership & NHS West Midlands (2011). A positive approach to risk and personalisation: Developed by ADASS West Midlands joint improvement partnership NHS West Midlands: A framework: NHS West Midlands.
Alzheimer’s Society (2011). Guidelines for care: Person-centred care of people with dementia living in care homes (Vol. January): Alzheimer’s Society.
André, B., Sjøvold, E., Rannestad, T., & Ringdal, G.I. (2014). The impact of work culture on quality of care in nursing homes — a review study Scandinavian Journal of Caring Sciences (Vol. 28, pp. 449–457.p. 443 Charts).
Austin, M., & Claassen, J. (2008). Impact of organizational change on organizational culture: Implications for introducing evidence-based practice Journal of Evidence-Based Social Work (Vol. 5, pp. 321–359).
Balogun, J., & Hailey, V. (2004). Exploring strategic change. London: Prentice Hall.Bartlett, R., & McKeefry, D. (2009). People with dementia and sight loss: A scoping study
of models of care. London: Thomas Pocklington Trust.Battilana, J. & Casciaro, T. (2012). Change agents, networks, and institutions: A
contingency theory of organizational change Academy of Management Journal (Vol. 55, pp. 381-398).
Beadle-Brown, J., Hutchinson, A., & Whelton, B. (2008). A better life: The implementation and effect of person-centred active support in the avenues trust Tizard Learning Disability Review (Vol. 13, pp. 15 – 24).
Bellot, J. (2011). Defining and assessing organisational culture Nursing Forum (Vol. 46, pp. 29–37).
Beresford, P., Fleming, J., Glynn, M., Bewley, C., Croft, S., Branfield, F., & Postle, K. (2011). Transforming social care: Sustaining person-centred support (Vol. May). York: Joseph Rowntree Foundation.
Berkhout, A., Boumans, N., Mur, I., & Nijhuis, F. (2009). Conditions for successfully implementing resident-oriented care in nursing homes Scandinavian Journal of Caring Sciences (Vol. 23, pp. 298–308): Wiley Blackwell.
Bernard, B. (2004). Kurt Lewin and the planned approach to change: A re-appraisal Journal of Management Studies (Vol. 41, pp. 6): Sage Publications.
65

Royal National Institute for the Blind (2014). How common is sight loss? How does sight loss affect people’s lives? (Vol. March): UK Vision Strategy.
Bowers, B., Nolet, K., Roberts, T., and Esmond, S. Implementing change in long-term care: A practical guide to transformation: University Wisconsin–Madison, School of Nursing.
Boyle, D., Slay, J., & Stephens, L. (2013). Public services inside out. London: NESTA.Brereton, L., Gardiner, C., Gott, M., Ingleton, C., Barnes, S., & Carroll, C. (2011). The
hospital environment for end of life care of older people and their families: An integrative review Journal of Advanced Nursing (Vol. 68, pp. 981–993).
British Geriatrics Society (2011). Quest for quality: British geriatrics society joint working party inquiry into the quality of healthcare support for older people in care homes: A call for leadership, partnership and quality improvement (Vol. June). London: British Geriatrics Society.
Brown Wilson, C. (2009). Developing community in care homes through a relationship-centred approach Health and Social Care in the Community, (Vol. 17, pp. 177–186).
Brown Wilson, C., Swarbrick, C., Pilling, M., & Keady, J. (2012). The senses in practice: Enhancing the quality of care for residents with dementia in care homes Journal of Advanced Nursing (Vol. 69, pp. 77–90).
Brune, K. (2011). Culture change in long term care services: Edengreenhouse-aging in the community Educational Gerontology (Vol. 37, pp. 506–525): Taylor & Francis.
Burtney, L., Figgett, D., Fullerton, D., Buchanan, P., Stevens, K., & Cooper-Ueki, M. (2014). Learning for care homes from alternative residential care settings: Report In April (Ed.): Joseph Rowntree Foundation
Burton, J. (2008). Care homes: Caring and homely? But how? Journal of Care Services Management (Vol. 2, pp. 227–238).
Burton, J. (2012). Behind the facade, beneath the surface: Where registered managers need to look and what they need to know Journal of Care Services Management (Vol. 6, pp. 63–68).
Camble, A. (2012). Personcentred support of people who exhibit challenging behaviour Learning Disability Practice (Vol. 15, pp. 18–20): RCN Publishing Company.
Carnaby, S., Roberts, B., Lang, J., & Nielsen, P. (2010). A flexible response: Person-centred support and social inclusion for people with learning disabilities and challenging behaviour British Journal of Learning Disabilities (Vol. 39, pp. 29–45).
Castle, N., & Decker, F. (2011). Top management leadership style and quality of care in nursing homes Gerontologist (Vol. 51, pp. 630–642).
Charles, N., & Manthorpe, J. (2009). An exploratory qualitative study of equity and the social care needs of visually impaired older people in England British Journal of Visual Impairment (Vol. 27, pp. 97–109).
College of Occupational Therapists (2007). Activity provision: Benchmarking good practice in care homes. London: College of Occupational Therapists
Care Commission (2009). Promoting nutrition in care homes for older people. In January (Ed.): Scottish Commission for the Regulation of Care
66
Care Quality Commission (2012). Learning disability services inspection programme: National overview. Newcastle: Care Quality Commission.
Care Quality Commission (2012). The state of health care and adult social care in England: An overview of key themes in care in 2011/12 (Vol. November). London: The Stationery Office.
Care Quality Commission (2013). The state of health care and adult social care in England (Vol. November). London: CQC.
Care Quality Commission (2014). A fresh start for the regulation and inspection of adult social care. London: Care Quality Commission.
Corazzini, K., Twersky, J., White, H., Hunt, S.R., Buhr, G.T., McConnell, E.S., . Colon-Emeric, C. (2012). Implementing culture change in nursing homes: An adaptive leadership framework Gerontologist (Vol. 52, pp. 510–510).
Coulter, A., Roberts, S., & Dixon, A. (2013). Delivering better services for people with long-term conditions. London: The Kings Fund.
Crocker, T., Young, J., Forster, A., Brown, L., Ozer, S., & Greenwood, D. (2013). The effect of physical rehabilitation on activities of daily living in older residents of long-term care facilities: Systematic review with meta-analysis. Age & Ageing (Vol. 42, pp. 682–688).
Davies, S., Goodman, C., Bunn, F., Victor, C., Dickinson, A., Iliffe, S., Gage, H.,Martin, W. & Froggatt, K. (2011). A systematic review of integrated working between care
homes and health care services BMC Health Services Research (Vol. 11, pp. 320).Davies, S., & Nolan, M. (2008). Excellence in dementia care: Research into practice In M.
a. B. Downs, B. (Ed.), Attending to relationships in dementia care (pp. 438–454). London: Open University Press.
Department for Business Innovation and Skills (2013). Focus on enforcement regulatory reviews: Review of the adult care homes sector (Vol. October). London: BIS.
Department of Health (2001). Valuing people: A new strategy for learning disability for the 21st century (Vol. March). London: Department of Health.
Department of Health (2005). Independence, well-being and choice: Our vision for the future of social care for adults in England (Vol. March). London: Department of Health.
Department of Health (2007). Our NHS, our future London: Department of Health Department of Health (2008). End of life care strategy: Promoting high quality care for all
adults at the end of life (Vol. July ): Department of Health.Department of Health (2008a). End of life care strategy: Promoting high quality care for
adults at the end of their life. London: Department of Health.Department of Health (2008b). High quality care for all. London: Department of Health Department of Health (2009). Living well with dementia in a care home (Vol. December):
RCN Publishing.Department of Health (2010). ‘Nothing ventured, nothing gained’: Risk guidance for people
with dementia (November). London: Department of Health.Department of Health (2010). Putting people first (February): Department of Health.
67
Department of Health (2010a). Personalisation through person-centred planning (March). London: Department of Health.
Department of Health (2010b). Vision for adult social care. London: Department of Health.Department of Health (2011). Better care at home and in care homes: Contract inserts
(July). London: Department of Health.Department of Health (2012a). Compassion in practice - nursing, midwifery and care staff.
Our vision and strategy London: Department of Health.Department of Health (2012b). Transforming care: A national response to winterbourne
view hospital: Department of Health.Department of Health (2014). Requirement for registration with the care quality
commission (Vol. July). London: Department of Health.Deutschman, M. (2001). Redefining quality and excellence in the nursing home culture
Journal of Gerontological Nursing (Vol. 27, pp. 28–36).Dixon, D. (2003). Successfully surviving culture change Journal of Social Work in Long-
Term Care (Vol. 2, pp.423–438).Doherty, R., Loughrey, C., & Higgins, P. (2013). Organisational culture: A review of the
literature. Belfast: Department of HealthDowling, S., Manthorpe, J., & Cowley, S. (2006). Person-centred planning in social care. A
scoping review. York: Joseph Rowntree Foundation.Dowling, S., Manthorpe, J., & Cowley, S. (2007). Working on person-centred planning:
From amber to green light? Journal of Intellectual Disabilities (Vol. 11, pp. 65–82). England: SAGE Publications.
Dreer, L., McGwin, G., Scilley, K., Meek, G.C., Dyer, A., Seker, D., & Owsley, C. (2007). Development of a nursing home vision-targeted health-related quality of life questionnaire for older adults Aging & Mental Health (Vol. 11, pp. 722–733).
Drumm, M. (2012). Culture change in the public sector. Glasgow: IRISS.Edvardsson, D., Winblad, B., & Sandman, P. (2008). Person-centred care of people with
severe Alzheimer's disease: Current status and ways forward The Lancet Neurology (Vol. 7, pp. 362–367).
Elliot, A. (2010). Occupancy and revenue gains from culture change in nursing homes: A win-win innovation for a new age of long-term care Seniors Housing and Care Journal (Vol. 18, pp. 61–76).
Ellmers, T., Arber, S., Luff, R., Eyers, I., & Young, E. (2013). Factors affecting residents' sleep in care homes Nursing Older People (Vol. 25, pp. 29–32): RCN Publishing Company.
European Centre for Social Welfare Policy and Research (2010). Measuring progress: Indicators for care homes. In October (Ed.). Vienna: European Centre for Social Welfare Policy and Research.
Evans C., G.C. (2009). Changing practice in dementia care for people in care homes towards the end of life Dementia: the International Journal of Social Research and Practice (pp. pp.424–431).
68
Evans, S., Hills, S., & Grimshaw, L. (2010). Sustainable systems of social care (Vol. October): SCIE.
Faulkner, A. (2012). Care homes: Risks and relationships. How can approaches to risk in care homes support good relationships and quality of life? (Vol. February). York: Joseph Rowntree Foundation.
Finlay, W., Walton, C., & Antaki, C. (2008). Promoting choice and control in residential services for people with learning disabilities Disability & Society (Vol. 23, pp. 349–360): Disability & Society.
Gage, C. (2014). Vibrant communities: The care homes of the future Journal of Dementia Care, (Vol. 22, pp. 22–25. ).
Glynn, M., Beresford, P., Bewley, C., Branfield, F., Butt, J., Croft, S., Turner, M. (2008). Person-centred support: What service users and practitioners say (July ). York Joseph Rowntree.
Goode, J. (2014). Value based recruitment toolkit: Evaluation of 12 month pilot (. August). Leeds: Skills for Care.
Goodrich, J. (2012). Supporting hospital staff to provide compassionate care: Do Schwartz center rounds work in English hospitals? Journal of the Royal Society of Medicine (Vol. 105, pp. 117–122).
Grabowski, D., Elliot, A., Leitzell, B., Cohen, L., & Zimmerman, S. (2014b). Who are the innovators? Nursing homes implementing culture change The Gerontologist (Vol. 54, pp. 565–575).
Grabowski, D., O’Malley, J., Afendulis, C., Caudry, D., Elliot, A., & Zimmerman, S. (2014a). Culture change and nursing home quality of care The Gerontologist (Vol. 54, pp. 535–545): Oxford University Press.
Gage, H., Knibb, W., Evans, J., Williams, P., Rickman, N. & Bryan, K. (2009). Why are some care homes better than others? An empirical study of the factors associated with quality of care for older people in residential homes in Surrey, England Health and Social Care in the Community (Vol. 16, pp. 599–609).
Hall, S., Goddard, C., Opio, D., Speck, P. & Higginson, I. (2012). Feasibility, acceptability and potential effectiveness of dignity therapy for older people in care homes: A phase ii randomized controlled trial of a brief palliative care psychotherapy Palliative Medicine (Vol. 26, pp. 703–712).
Hanley, J. and Marsland, D. (2014). Unhappy anniversary? The journal of adult protection (Vol. 16 pp. 104–112).
Hanson, J., & Percival, J. (2005). The housing and support needs of visually impaired adults living in England today British Journal of Visual Impairment (Vol. 23, pp. 102–107).
Hays, R., Clarkson, P., Tucker, S., & Challis, D. (2012). Healthcare support services for care home residents. Nursing Older People (Vol. 24, pp. 26–30).
Help the Aged (2007). My home life: Quality of life in care homes: A review of the literature: Help the Aged
69

Hernandez, S., Conrad, D., Marcus-Smith, M., Reed, P., & Watts, C. (2013). Patient-centred innovation in health care organizations: A conceptual framework and case study application Health Care Management Review (Vol. 38, pp. 166–175).
Hill, N., Kolanowski, A., Milone-Nuzzo, P., & Yevchak, A. (2011). Culture change models and resident health outcomes in long-term care Journal of Nursing Scholarship (Vol. 43, pp. 30–40).
HM Government, H. (2012). Caring for our future. London: HM Government.Hockley, J., Watson, J., Oxenham, D., & Murray, S. (2010). The integrated implementation
of two end-of-life care tools in nursing care homes in the UK: An in-depth evaluation Palliative Medicine (Vol. 24, pp. 828–838).
Hodges, L., & Douglas, G. (2007). Hearing and sight loss: A review of the issues affecting older peopleLondon: Thomas Pocklington Trust
Holroyd-Leduc, J., Lorenzetti, D., Straus, S., Sykes, L., & Quan, H. (2011). The impact of the electronic medical record on structure, process, and outcomes within primary care: A systematic review of the evidence Journal of the American Medical Informatics Association (Vol. 18, pp. 732–737).
Hoolahan, S. (2012). ISF in action: Personalising block contracts - a research report (Vol. March ): The Centre for Welfare Reform.
Hughes, J., Chester, H., & Challis, D. (2009). Recruitment and retention of a social care workforce for older people Manchester: PSSRU.
Hurtley, R., & Duff, A. (2012). Achieving excellence in person-centred living Nursing and Residential Care (Vol. 14, pp. 99–100).
Iles, V., & Sutherland, K. (2001). Managing change in the NHS: Organisational change: National Coordinating Centre for the Service Delivery and Organisation (NCCSDO).
Innes, A., Macherson, S., & McCabe, L. (2006). Promoting person-centred care at the front line. York: Joseph Rowntree Foundation.
Joseph Rowntree Foundation (2010). Residential care home workforce development: The rhetoric and reality of meeting older residents’ future care needs (May ). York: Joseph Rowntree Foundation.
Jie Jin, W., Mitchell, P., Cumming, R., & Smith, W. (2003). Visual impairment and nursing home placement in older Australians: The Blue Mountains eye study Ophthalmic Epidemiology (Vol. 10, p. 3).
Katz, R., & Richard, F. (2010). A vision for the future: New care delivery models can play a vital role in building tomorrow's eldercare workforce. Generations - Journal of the American Society on Aging (Vol. 34, pp. 82–88): American Society on Aging.
Keating, M., Long, J., and Wright, J. (2013). Leading culture change to improve dementia care Nursing Times (pp. 16-18).
Kelly, F., Innes, A., Dincarslan, O. (2011). Improving care home design for people with dementia Journal of Care Services Management (Vol. 5, pp. pp.147-155.).
Kennedy, J. (2014). John Kennedy’s care home inquiry. York: Joseph Rowntree Foundation.
70

Kinley, J., Froggatt, K. and Bennett, M. (2013). The effect of policy on end-of-life care practice within nursing care homes: A systematic review Palliative Medicine (Vol. 27, pp. 209–220).
Kirkley, C., Bamford, C., Poole, M., Arksey, H., Hughes, J., & Bond, J. (2011). The impact of organisational culture on the delivery of person-centred care in services providing respite care and short breaks for people with dementia Health and Social Care in the Community (Vol. 19, pp. 438–448).
Knocker, S. (2013). Home from home Nursing Standard (Vol. 27, pp. 20–21).Langley, A., Smallman, C., Ttsoukas, H., & Van De Ven, A. (2013). Managing change with
a time-tested organic model Academy of Management Journal (Vol. 56, pp. 1–13): Academy of Management
Lawrence, V., & Banerjee, S. (2010). Improving care in care homes: A qualitative evaluation of the Croydon care home support team Aging & Mental Health (Vol. 14, pp. 416–424).
Lepore, M. (2014). Focus groups: A powerful lever for culture change Long-Term Living: For the Continuing Care Professional. (Vol. 60, pp. p30–31.).
Li, J &Porock, D. (2014). Resident outcomes of person-centred care in long-term care. . A narrative review the interventional research International Journal of Nursing Studies (Vol. 51, pp. 1395–1415).
Lopez, S. (2014). Culture change and shit work: Empowering and overpowering the frail elderly in long-term care. In March (Ed.), American Behavioral Scientist (Vol. 58, pp. 435–452): Sage Publications
Lynch, B., McCormack, B., & McCance, T. (2011). Development of a model of situational leadership in residential care for older people. Journal of Nursing Management (Vol. 19, pp. 1058–1069.
Manley, K., O'Keefe, H., Jackson, C., Pearce, J., & Smith, S. (2014). A shared purpose framework to deliver person-centred, safe and effective care: Organisational transformation using practice development methodology International Practice Development Journal (Vol. 4, pp. 1–31).
Mannion, R., Davies, H., Konteh, F., Jung, T., Scott, T., Bower, P., McMurray, R. (2008). Measuring and assessing organisational culture in the nhs (June). York: York Management School.
Mansah, M., Coulon, L., Brown, P., Reynolds, H., & Kissiwaa, S. (2014). Tailoring dementia care mapping and reflective practice to empower assistants in nursing to provide quality care for residents with dementia Australian Journal of Advanced Nursing (Vol. 31, pp. 34–44).
Mansell, J. (2007). Services for people with learning disabilities and challenging behaviour or mental health needs (October). London: Department of Health.
Mansell, J. (2010). Raising our sights: Services for adults with profound intellectual and multiple disabilities (March): Department of Health.
Mason, M. (2012 ). Care home sweet home: Care home of the future: International Longevity Centre UK
71

Milne, A. (2011). Living with dementia in a care home: Capturing the experiences of residents Quality in Ageing and Older Adults, (Vol. 12, pp. 76–85).
Moiden, N. (2002). Leadership in the elderly care home sector Nursing Management - UK (Vol. 9, pp. 24 –25).
Moore, J. (2013). Independent living in care homes for older people Quality in Ageing and Older Adults (Vol. 13, pp. 156–159).
Mueller, C. (2008). Research in culture change in nursing homes Nurses involvement in culture change.
Musselbrook, K. (2013). Imagining the future: Workforce (Vol. December). Glasgow: IRISS.
National Development Team for Inclusion (2009). Finding out what determines 'a good life' for older people in care homes. York: Joseph Rowntree Foundation.
National Development Team for Inclusion (2014). Commissioning relationship-centred care in Essex: An evaluation. York: Joseph Rowntree Foundation.
Neill, M., Allen, J., Woodhead, N., Sanderson, H., Reid, S., & Erwin, L. (2009). A positive approach to risk requires person-centred thinking Tizard Learning Disability Review (Vol. 14, pp. 17–24).
Newton, M., & Sanderson, A. (2013). The effect of visual impairment on patients' falls risk Nursing Older People (Vol. 25, pp. 16–21).
Nolan, M., Davies, S., Brown, J., Keady, J., & Nolan, J. (2002). Longitudinal study of the effectiveness of educational preparation to meet the needs of older people and carers: The ageing project. Sheffield: University of Sheffield.
Nolan, M., Davies, S., Brown, J., Keady, J., & Nolan, J. (2004). Beyond 'person-centred' care: A new vision for gerontological nursing Journal of Clinical Nursing (Vol. 13, pp. 45–53).
Nolan, R., Brown, J., Davies, S., Nolan, J. and Keady, J. (2006). The senses framework: Improving care for older people through a relationship-centred approach. Getting research into practice (GRIP): University of Sheffield.
Northern Ireland Assembly (2010). Arrangements for ensuring the quality of care in homes for older people (December ). Belfast: Northern Ireland Assembly
Owen, T., Meyer, J., Cornell, M., Dudman, P., Ferreira, Z., Hamilton, S., Wallis, J. (2012). My home life: Promoting quality of life in care homes. Joseph Rowntree Foundation.
Packer, T. (2000). Does person-centred care exist? Journal of Dementia Care (Vol. 8, pp. 19–21).
Parker, C., Barnes, S., Mckee, K., Morgan, K., Torrington, J., & Tregenza, P. (2004). Quality of life and building design in residential and nursing homes for older people Ageing and Society (Vol. 24, pp. 941–962).
Pearson, G., Tamkin, P., Blazey, L. and Zheltoukhova, K. (2011). Outstanding leadership in social care (Vol. February). London: National Skills Academy for Social Care.
Perrin, T. (2005). Let's stir up the outdated activity culture in care homes Journal of Dementia Care (Vol. 13, pp. 26–27).
72

Practice, L.D. (2009). Quality of life in care homes Learning Disability Practice (Vol. 12, pp. 13–13): RCN Publishing Company.
Quince, C. (2001). Low expectations: Attitudes on choice, care and community for people with dementia in care homes (Vol. February). London: Alzheimer's Society
Rahman, A.S., J. (2007). The nursing home culture-change movement: Recent past, present, and future directions for research. The Gerontologist (Vol. 48, pp. 142–148).
Reilly, S., Abendstern, A., Hughes, J., Challis, D., and Venables, D. (2005). Care homes for older people with dementia in the north west of England (Vol. May): PSSRU.
Riazi, A., Bradshaw, S., & Playford, D. (2012). Quality of life in the care home: A qualitative study of the perspectives of residents with multiple sclerosis Disability & Rehabilitation (Vol. 34, pp. 2095).
Rigby, J., Payne, S., & Froggatt, K. (2010). What evidence is there about the specific environmental needs of older people who are near the end of life and are cared for in hospices or similar institutions? A literature review. Palliative Medicine (Vol. 24, pp. 268–285).
Robertson, J., Emerson, E., Hatton, C., Elliott, J., McIntosh, B., Swift, P., Krijnen-Kemp, E.Towers, C. Romeo, R., Knapp, M., Sanderson, H. Routledge, M., Oakes, P. & Joyce, T. (2005). The impact of person centred planning. Lancaster: Institute for Health Research, Lancaster University.
Rondeau, K., & Wagar, T. (2006). Nurse and resident satisfaction long term care organisations: Do high involvement approaches matter Journal of Nursing Management (Vol. 14, pp. 244–250).
Royal National Institute of Blind People (2010). Seeing it from their side: A guide to recognising and supporting sight loss in your care home (September): RNIB.
Royal National Institute of Blind People. (2014). Evidence-based review: Older people (February): RNIB.
Ryan, T., Gardiner, C., Bellamy, G., Gott, M., & Ingleton, C. (2012). Barriers and facilitators to the receipt of palliative care for people with dementia: The views of medical and nursing staff. Palliative Medicine (Vol. 26, pp. 879–886): Sage Publications.
Sanderson, H., Thompson, J., & Kilbane, J. (2006). The emergence of person-centred planning as evidence-based practice Journal of Integrated Care (Vol. 14, pp. 18–25 ).
Schehrer, S., & Sexton, S. (2010). Involving users in commissioning local services (Vol. May ). York Joseph Rowntree Foundation
Schehrer, S., & Sexton, S. (2010). Involving users in commissioning local services. York: Joseph Rowntree Foundation.
Schein, E.H. (2004). Organisational culture and leadership San Francisco: Jossey-Bass.SCIE (2009). Research briefing 31: Co-production: An emerging evidence base for adult
social care transformation. (March). London: SCIE.SCIE (2012). Safeguarding and quality in commissioning care homes. London: SCIE.
73

The Scottish Government (2007). National care standards: Care homes for older people (Vol. November ). Edinburgh: The Scottish Government.
Seymour, J., Kumar, A. and Froggatt, K. (2011). Do nursing homes for older people have the support they need to provide end-of-life care? A mixed methods enquiry in England. Palliative Medicine (Vol. 25, pp. 125–138).
Shaping our Lives, National Centre for Independent Living and University of Leeds Centre for Disability Studies (2007). Developing social care: Service users driving culture change London: SCIE.
Sheard, D. (2014). Achieving culture change: A whole organisation approach Nursing and Residential Care (Vol. 16).
Shier, V., Khodyakov, D., Cohen, L., Zimmerman, S., & Saliba, D. (2014). What does the evidence really say about culture change in nursing homes? . Gerontologist (Vol. 54 pp. S6-S16).
Silver, S. (2010). A guide for managers Napa.Sinclair, A.J. (2012). Good clinical practice guidelines for care home residents with
diabetes Diabetic Medicine (Vol. 28, pp. 772–777).Sinoo, M., Kort, H., & Duijnstee, M. (2012). Visual functioning in nursing home residents:
Information in client records Journal of Clinical Nursing (Vol. 21, pp. 1913–1921).Skills for Care (2008). Principles of workforce redesign (October). Leeds: Skills for Care.Skills for Care (2011). Capable, confident, skilled: A workforce development strategy for
people working, supporting and caring in adult social care Leeds: Skills for Care Skills for Care and Skills for Health (2012). Developing end of life care practice: A guide to
workforce development to support social care and health workers to apply the common core principles and competences for end of life care. . Leeds: Skills for Care.
Sullivan Restock, D. (2013). Changing the culture of long-term care Planning (Vol. 79, p. 39).
Szczepura, A., Clay, D., Hyde, J., Nelson, S., & Wild, D. (2008). Models for providing improved care in residential care homes: A thematic literature review: University of York
Szczepura, A., Clay, D., Hyde, J., Nelson, S., & Wild, D. (2008). Models for providing improved care in residential care homes: A thematic literature review: Annotated bibliography University of Warwick
Szczepura, A., Clay, D., Nelson, S., & Wild, D. (2008). Improving care in residential care homes: A literature review (Vol. October). York Joseph Rowntree Foundation
Tadd, W., Woods, R., O’Neill, M., Windle, G., Read, S., Seddon, D,. Hall, C. & Bayer, T. (2010). Promoting excellence in all care homes (July): Cardiff University.
Tamkin, P., Pearson, G., Hirsh, W., & Constable, S. (2010). Exceeding expectation: The principles of outstanding leadership. London: The Work Foundation.
Tanner, C., & B., M. (2014). We’ll meet again - don’t know where, don’t know when" supporting community visiting in Essex care homes. In February (Ed.): University of Essex.
74

Tanner, C., & Brett, B. (2014). Improving quality of life in care homes through community visiting (June). York: Joseph Rowntree Foundation.
Thomas Pocklington Trust (2003 ). Meeting the needs of older people with visual impairment: Social care or social exclusion? (October ). London: Thomas Pocklington Trust
Thomas Pocklington Trust (2013). How can care homes “look out” for eye health? London: Thomas Pocklington Trust.
Thomas Pocklington Trust (2013). Loneliness, social isolation and sight loss: Proposal for a literature review for the Thomas Pocklington Trust (Vol. March). London: Thomas Pocklington Trust.
Thomas Pocklington Trust (2013). Raising awareness of sight loss in care homes: Briefing for research and development team meeting Thomas Pocklington Trust.
Thomas Pocklington Trust (2014). How older people define wellbeing – a synthesis of the evidence: Thomas Pocklington Trust.
Thomas Pocklington Trust (2014). Mapping training for care homes: Providers of visual awareness training for care homes. London: Thomas Pocklington Trust.
Thomas Pocklington Trust (2014). Producing accessible materials (chapter 6): Thomas Pocklington Trust.
Thomas Pocklington Trust (2014). Sight tests at home. London: Thomas Pocklington Trust.
Tilly, J., & Reed, R. (2004). Evidence on interventions to improve quality of care for residents with dementia in nursing and assisted living facilities: The Alzheimer's Association.
Vabø, M. (2012). Norwegian home care in transition - heading for accountability, off-loading responsibilities. In May (Ed.), Health & Social Care in the Community (Vol. 20, pp. 283–291): Wiley Blackwell.
Van Beek, A.P.A., & Gerritsen, D.L. (2010). The relationship between organizational culture of nursing staff and quality of care for residents with dementia: Questionnaire surveys and systematic observations in nursing homes International Journal of Nursing Studies (Vol. 47, pp. 1274–1282).
National Voices Prioritising person-centred care: Summarising evidence from systematic reviews: National Voices.
Wallcraft, J., & Sweeney, A. (2011). Adults services report 47: User involvement in adult safeguarding (September ). London SCIE.
Waller, S., Dewar, S., Masterson, A., & Finn, H. (2008). Improving environments for care at end of life. London: The King's Fund.
Waller, S., & Finn, H. (2011). Improving the patient experience: Environments for care at end of life. London: The King's Fund.
Ward, G., Awang, D., Campion, C., Dring, P., & Bryce, C. (2009). Improving outcomes for people with sight loss: Identifying the continuing professional development needs of occupational therapists (Vol. September ): Thomas Pocklington Trust
75

Warrington, J., Afridi, A., & Foreman, W. (2013). Is excessive paperwork in care homes undermining care for older people? . York: Joseph Rowntree Foundation.
Watkinson, S., & Scott, E. (2004). Managing the care of patients who have visual impairment Nursing Times (Vol. 6 June ): Nursing Times.
Oomph Wellness (2014). Oomph! Impact report Q3 2014: Oomph Wellness.Wenborn, J. (2013). Providing activity for people with dementia in care homes: A cluster
randomised controlled trial International Journal of Geriatric Psychiatry (Vol. 28, pp. pp.1296–1304).
West, S.K., Friedman, D., Munoz, B., Roche, K.B., Park, W., Deremeik, J., German, P. (2003). A randomized trial of visual impairment interventions for nursing home residents: Study design, baseline characteristics and visual loss Ophthalmic Epidemiology (Vol. 10, pp. 193–209).
Westrum, R. (2004). A typology of organisational cultures Quality Safety Health Care (Vol. 13, pp. 22–27).
Wild, D., Nelson, S., & Szczepura, A. (2010). A ‘home for life’ in residential homes for older people in England: Exploring the enhancers and inhibitors. In May (Ed.), Housing Care and Support (Vol. 13, pp. 26–35).
Willis, M. (2005). Defining vision. In July (Ed.), Community Care (Vol. 1580, pp. 32–33): Community Care.
Wise, C., Jeffrey, A., Green, L., Cohen, G., & Koster, C. (2011). Journey toward a patient-centered medical home: Readiness for change in primary care practices The Millbank Quarterly (Vol. 89, pp. 399–424).
Worden, A., Challis, D. (2008). Care planning systems in care homes for older people Quality in Ageing (Vol. 9, pp. 28–38): Pier Professional
Yalden, J., McCormack, B., O'Connor, M., & Hardy, S. (2013). Transforming end of life care using practice development: An arts-informed approach in residential aged care. In November (Ed.), International Practice Development Journal (Vol. 3, pp. 1–18).
76