上海市第六人民医院 shanghai sixth people’s hospital shankai yin prof dept of...
TRANSCRIPT

上海市第六人民医院Shanghai Sixth People’s Hospital
Shankai Yin Prof Dept of Otolaryngology, the sixth hospital affilia
ted to Shanghai jiaotong university Otolaryngology institute at Shanghai jiaotong u
niversity
Facial Nerve Disease

上海市第六人民医院Shanghai Sixth People’s Hospital
Anatomy
Facial nerve is a mixed nerve, having a motor root and a sensory root.
Motor root supplies all the mimetic muscles of the face which develop from the 2nd brachial arch.
上海市第六人民医院Shanghai Sixth People’s Hospital
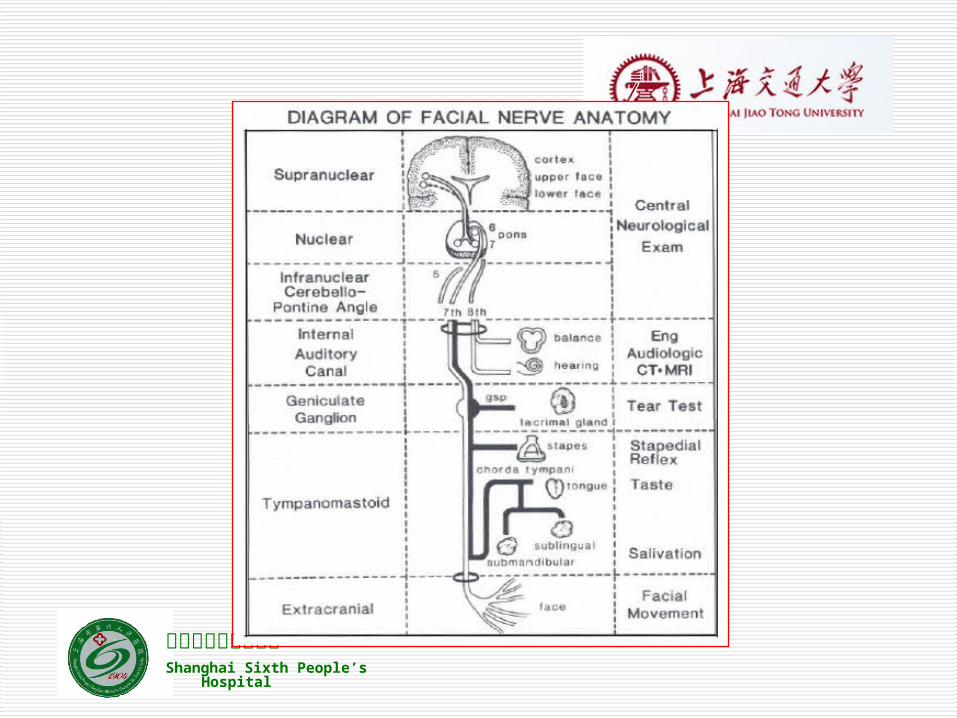
Sensory root “nerve of Wrisberg” carries taste fibers from the anterior 2/3 of the tongue and general sensation from the concha and retroauricular skin.
Also it carries secretomotor fibers to the lacrimal, submandibular and sublingual glands as well as those in the nose and palate.

上海市第六人民医院Shanghai Sixth People’s Hospital
Anatomy: Parts
Intracranial part
Intratemporal part
Extracranial part

上海市第六人民医院Shanghai Sixth People’s Hospital
Course of the Facial Nerve
Intracranial Arises at the pontomedullary junction and c
ourses with CNVIII to the internal acoustic meatus
12mm

上海市第六人民医院Shanghai Sixth People’s Hospital
Intratemporal Meatal
Anterior to the superior vestibular nerve and superior to the cochlear nerve – 10mm
Labyrinthe segment Passes through narrowest part of fallopian canal - 12mm Narrowest part of facial nerve. The most susceptible to compres
sion secondary to edema. Tympanic segment
From geniculate ganglion to pyramidal turn – 11mm Mastoid segment
Exits the stylomastoid foramen – 13mm

上海市第六人民医院Shanghai Sixth People’s Hospital
Extracranial From stylomastoid foramen to pesanserinus

上海市第六人民医院Shanghai Sixth People’s Hospital
Anatomy: Branches
Greater superficial petrosal nerve Nerve to stapedius Chorda tympani Comunicating branch Posterior auricular nerve Muscular branches Peripheral branches: “Pes anserinus”

上海市第六人民医院Shanghai Sixth People’s Hospital
3-D t bone

上海市第六人民医院Shanghai Sixth People’s Hospital
Presentation
Functional and cosmetic problems Upper lid fails to drop down and close Lower lid loses tone and sags downward
May evert leading to ectropion Produces lagophthalmos and consequent
corneal exposure. Interruption of the tear film Leads to drying of cornea
Ocular discomfort Corneal ulcers Infection Perforation

上海市第六人民医院Shanghai Sixth People’s Hospital
Upper motor neurone (UMN) can wrinkle their forehead (unless bilateral les
ion) sagging of the face seen with lower motor neu
rone palsies is not as prominent. Lower motor neurone (LMN)
can't wrinkle their forehead

上海市第六人民医院Shanghai Sixth People’s Hospital

上海市第六人民医院Shanghai Sixth People’s Hospital
House-Brackmann Facial NerveGrading Scale
I NormalII Normal tone and symmetry at rest. Slight weakness on close inspection
Good to moderate movement of forehead. Complete eye closure with minimum effort. Slight asymmetry of mouth with movement
III Normal tone and symmetry at rest. Obvious but not disfiguring facial asymmetry. Synkinesis may be noticeable but not severe .+/- hemifacial spasm or contracture. Slight to moderate movement of foreheadComplete eye closure with effort. Slight weakness of mouth with maximum effort.
IV Normal tone and symmetry at rest. Asymmetry is disfiguring or results in obvious facial weakness. No perceptible forehead movement. Incomplete eye closure. Asymmetrical motion of mouth with maximum effort
V Asymmetrical facial appearance at rest. Slight, barely noticeable movement. No forehead movement. Incomplete eye closure. Asymmetrical motion of mouth with maximum effort.

上海市第六人民医院Shanghai Sixth People’s Hospital
Degree of Lesion
Sunderland classification 1° Partial block: Neuropraxia 2° Loss of axons: axonotemesis 3° Injury to the endoneurium: neurotemesis 4° Injury to the perineurium: partial transection 5°Injury to the epineurium: complete
transection

上海市第六人民医院Shanghai Sixth People’s Hospital

上海市第六人民医院Shanghai Sixth People’s Hospital
Diagnosis
History Presentation Hearing test Vestibular function MRI / CT Topognostic - Where is the lesion? Qualitative -Degree of the lesion

上海市第六人民医院Shanghai Sixth People’s Hospital
Schirmer’s tear test Stapedius reflex Taste test Submandibular salivary flow test
Topodiagnostic Diagnosis
上海市第六人民医院Shanghai Sixth People’s Hospital

上海市第六人民医院Shanghai Sixth People’s Hospital
Qualitative Diagnosis
Nerve Excitability Test: NET Maximum stimulation Test: MST Electroneurography: ENoG Electromyography: EMG
上海市第六人民医院Shanghai Sixth People’s Hospital
Bell’s Palsy
60-70% cases Pathophysiology – Impaired “axoplasmic” flow from ede
ma of facial nerve within fallopian canal Rapid onset and evolution < 48 hours May be associated with acute neuropathies of cranial nerv
es V- X Pain or numbness affecting ear, mid-face, tongue and tast
e disturbances Recurrences are more likely (2.5x) in patients with family h
istory, immunodeficiency or diabetes

上海市第六人民医院Shanghai Sixth People’s Hospital
Pathophysiology
Main cause of Bell's palsy is latent herpes viruses (herpes simplex virus type 1 and herpes zoster virus), which are reactivated from cranial nerve ganglia.
Polymerase chain reaction techniques have isolated herpes virus DNA from the facial nerve during acute palsy.

上海市第六人民医院Shanghai Sixth People’s Hospital
Oral antivirals - Acyclovir - 10mg/kg (500mg) q8hrs x 7 days
Corticosteroid taper 1mg / kg / day for 10 days Eye protection - lacrilube Follow progression with serial exams Facial nerve decompression
Progression to > 90% degeneration on ENOG Performed before irreversible injury to the endoneurial
tubules occurs (two weeks), will allow for axonal regeneration to occur
Treatment

上海市第六人民医院Shanghai Sixth People’s Hospital
Herpes Zoster Oticus(Ramsay Hunt syndrome)
10-15% of acute facial palsy cases Lesions may involve the external ear, the skin of E
AC or soft palate Associated symptoms – hearing loss, dysacusis an
d vertigo Additional involvement of CN V, IX and X and cervi
cal branches 2, 3 and 4 Pathogenesis – Neural injury due to edema at poi
nt between the meatal foramen and the geniculate fossa in the labyrinthe segment

上海市第六人民医院Shanghai Sixth People’s Hospital

上海市第六人民医院Shanghai Sixth People’s Hospital
Thanks !