- la technique endoscopique - - american academy of …orthodoc.aaos.org/drdidierfontes/biceps -...
TRANSCRIPT

Rupture distale du Biceps brachial
- La technique endoscopique - Didier FONTÈS
Espace Médical Vauban - Paris VIIe
Hôpital Européen Georges Pompidou
SOFEC Paris 2010

Clinical Recall w Less frequent than proximal lesions (3%) w = Avulsion of the radial attachment
(almost no partial lesion of distal tendon)
w Univocal clinical context
92% Males 4th decade 86% dominant elbow Excessive eccentric tension from flexion of the elbow 1,2 ruptures / 100 000 patients / year 43% smokers (over-risk x 7,5) Anabolic steroids consumers Professional sportsmen

Clinical Recall
w Positive diagnosis with comparative clinical exam n Local swelling n Ascension of the muscle n Resisted Flexion-supination
painfull and weak n Superficial dysesthesia (forearm
cutaneous lateral nerve, Bassett & Nunley type syndrom)

Clinical Recall
w Positive diagnosis with comparative clinical exam n Local swelling n Ascension of the muscle n Resisted Flexion-supination
painfull and weak n Superficial dysesthesia (forearm
cutaneous lateral nerve, Bassett & Nunley type syndrom)

Clinical Recall
w Positive diagnosis with comparative clinical exam n Local swelling n Ascension of the muscle n Resisted Flexion-supination
painfull and weak n Superficial dysesthesia (forearm
cutaneous lateral nerve, Bassett & Nunley type syndrom)

Radiographic Diagnosis
FABS
Tendon Distal Normal
FABS View
“T1 weighted”
Flexed elbow Abducted shoulder Supinated forearm w US non reliable for distal
avulsions w MRI with « australian »
FABS incidence n Jeff Hughes (Sydney)
n Diagnosis n Retraction n « Partial » Lesions

Radiographic Diagnosis
w US non reliable for distal avulsions
w MRI with « australian » FABS incidence n Jeff Hughes (Sydney)
n Diagnosis n Retraction n « Partial » Lesions

Radiographic Diagnosis
w US non reliable for distal avulsions
w MRI with « australian » FABS incidence n Jeff Hughes (Sydney)
n Diagnosis n Retraction n « Partial » Lesions

Therapeutic Attitude w Bad functional tolerance
of non operative treatment (weakness in flexion and supination)
w Painfull retracted tendon w Cutaneous adherences w Dysesthesia (Bassett &
Nunley) w Cosmetic disorder
=> Surgery
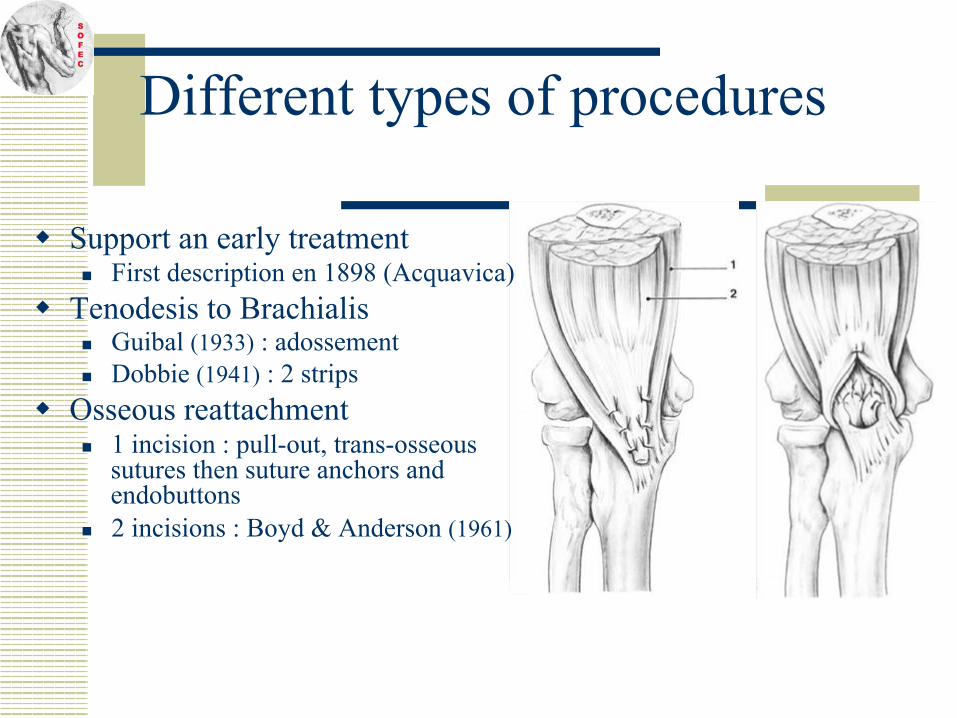
Different types of procedures
w Support an early treatment n First description en 1898 (Acquavica)
w Tenodesis to Brachialis n Guibal (1933) : adossement n Dobbie (1941) : 2 strips
w Osseous reattachment n 1 incision : pull-out, trans-osseous
sutures then suture anchors and endobuttons
n 2 incisions : Boyd & Anderson (1961)

Different types of procedures
w Support an early treatment n First description en 1898 (Acquavica)
w Tenodesis to Brachialis n Guibal (1933) : adossement n Dobbie (1941) : 2 strips
w Osseous reattachment n 1 incision : pull-out, trans-osseous
sutures then suture anchors and endobuttons
n 2 incisions : Boyd & Anderson (1961)

Different types of procedures
w Support an early treatment n First description en 1898 (Acquavica)
w Tenodesis to Brachialis n Guibal (1933) : adossement n Dobbie (1941) : 2 strips
w Osseous reattachment n 1 incision : pull-out, trans-osseous
sutures then suture anchors and endobuttons
n 2 incisions : Boyd & Anderson (1961)

Results of classical treatments
w Non operative management : n Weakness in flexion and supination
(from 30 to 50%) n Decrease of endurance (Cybex) ++
(>60%)
w Brachialis tenodesis : n Flexion weakness (-30% Catonné -
1995) and supination (-50% Klonz-2003) n Rare nervous complications n No heterotopic ossifications n Dissatisfaction of sportsmen

Results of classical treatments
w Trans osseous reattachment n More anatomical (suture anchors) n Best results in strength and
endurance n Neurological Complications
sometimes serious and definitive (5-10%)
n Heterotopic Ossifications and n Synostosis (5-14%) / 2 incisions

Results of classical treatments
w Trans osseous reattachment n More anatomical (suture anchors) n Best results in strength and
endurance n Neurological Complications
sometimes serious and definitive (5-10%)
n Heterotopic Ossifications and n Synostosis (5-14%) / 2 incisions

Results of classical treatments
w Trans osseous reattachment n More anatomical (suture anchors) n Best results in strength and
endurance n Neurological Complications
sometimes serious and definitive (5-10%)
n Heterotopic Ossifications and n Synostosis (5-14%) / 2 incisions

Results of classical treatments
w Trans osseous reattachment n More anatomical (suture anchors) n Best results in strength and
endurance n Neurological Complications
sometimes serious and definitive (5-10%)
n Heterotopic Ossifications and n Synostosis (5-14%) / 2 incisions

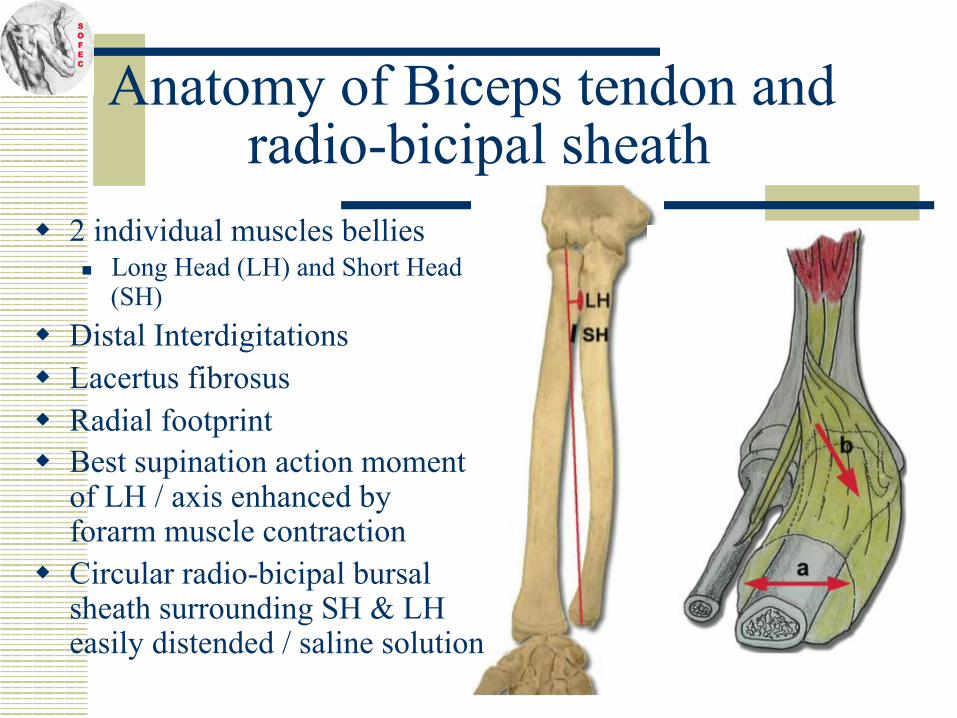
Anatomy of Biceps tendon and radio-bicipal sheath
w 2 individual muscles bellies n Long Head (LH) and Short Head
(SH)
w Distal Interdigitations w Lacertus fibrosus w Radial footprint w Best supination action moment
of LH / axis enhanced by forarm muscle contraction
w Circular radio-bicipal bursal sheath surrounding SH & LH easily distended / saline solution

Anatomy of Biceps tendon and radio-bicipal sheath
w 2 individual muscles bellies n Long Head (LH) and Short Head
(SH)
w Distal Interdigitations w Lacertus fibrosus w Radial footprint w Best supination action moment
of LH / axis enhanced by forarm muscle contraction
w Circular radio-bicipal bursal sheath surrounding SH & LH easily distended / saline solution

Anatomy of Biceps tendon and radio-bicipal sheath
w 2 individual muscles bellies n Long Head (LH) and Short Head
(SH)
w Distal Interdigitations w Lacertus fibrosus w Radial footprint w Best supination action moment
of LH / axis enhanced by forarm muscle contraction
w Circular radio-bicipal bursal sheath surrounding SH & LH easily distended / saline solution

Anatomy of Biceps tendon and radio-bicipal sheath
w 2 individual muscles bellies n Long Head (LH) and Short Head
(SH)
w Distal Interdigitations w Lacertus fibrosus w Radial footprint w Best supination action moment
of LH / axis enhanced by forarm muscle contraction
w Circular radio-bicipal bursal sheath surrounding SH & LH easily distended / saline solution
Anatomy of Biceps tendon and radio-bicipal sheath
w 2 individual muscles bellies n Long Head (LH) and Short Head
(SH)
w Distal Interdigitations w Lacertus fibrosus w Radial footprint w Best supination action moment
of LH / axis enhanced by forarm muscle contraction
w Circular radio-bicipal bursal sheath surrounding SH & LH easily distended / saline solution

Anatomy of Biceps tendon and radio-bicipal sheath
w 2 individual muscles bellies n Long Head (LH) and Short Head
(SH)
w Distal Interdigitations w Lacertus fibrosus w Radial footprint w Best supination action moment
of LH / axis enhanced by forarm muscle contraction
w Circular radio-bicipal bursal sheath surrounding SH & LH easily distended / saline solution

w Forearm cutaneous lateral nerve w Radial Nerve outwards of the
sheath (18 mm)
w Ulnar artery (6 mm) w Median nerve (12 mm) ⇒ «Noble » structures all in the
anterior plan
Anatomical neighborhood of bicipital tendon

w Safe anterior zone
w Well identified sheath as a working space (hematoma)
w Endoscopic magnification optimize operative safeness
Feasibility of an endoscopic approach

Goals of the classical one incision technique
Useless
w Location of the retracted biceps tendon w Vasculo-nervous pedicles control w Opening of the sheath and exposition of
radial tuberosity (retractors ++) w Trans osseous reattachment w Large sinuous anterior incision

Goals of the classical one incision technique
Dangerous
Useless
w Location of the retracted biceps tendon w Vasculo-nervous pedicles control w Opening of the sheath and exposition of
radial tuberosity (retractors ++) w Trans osseous reattachment w Large sinuous anterior incision

Goals of the classical one incision technique
Dangerous
Useless
w Location of the retracted biceps tendon w Vasculo-nervous pedicles control w Opening of the sheath and exposition of
radial tuberosity (retractors ++) w Trans osseous reattachment w Large sinuous anterior incision

Goals of the classical one incision technique
Dangerous
Useless
w Location of the retracted biceps tendon w Vasculo-nervous pedicles control w Opening of the sheath and exposition of
radial tuberosity (retractors ++) w Trans osseous reattachment w Large sinuous anterior incision

References
w S. Sharma (endobutton) n Arthroscopy 2005
w M. Eames, G. Bain (endobutton) n Tech. in Shoulder & Elbow surgery 2006
w Didier Fontès (suture anchors) n J. Traumato du Sport 2007 n Chir. De la Main 2009 n Am. J. Sports Medicine 2009

Our mini-invasive technique
w Supine position, proximal tourniquet
w Short approach in a distal crease (3 cm, rather medial) in the « safe area »
w Superficial dissection just to open the sheath (removing the hematoma and washing to avoid post-op ossifications)

Our endoscopic technique
w Grasping the retracted avulsed tendon inside and pulling down out of the wound
w Refreshing of tendon end
w Control of superficial nerves
w Possibility of reinforcement with the lacertus fibrosus

Our endoscopic technique w Location of the distal tendon
tract(following hematoma) w Introduction of a mini single use
speculum or endoscopic sheath down to tuberosity +/- saline solution
w Endoscopic control (scope 4,5 mm)
w One or 2 suture anchors
Radial tuberosity Anchor fixation

Our endoscopic technique w Removing of speculum and
scope w Tacking the tendon with
sliding knots to pull it down onto the bone
w Immobilization en Flexion 90° + supination (3 weeks)

Our series (from 2000 to 2009)
w 35 Males : (15 prof. Sport) n 5 international Rugby players n 10 carried out high level weigh
training n 1 mountain guide n Age : 31-58 years old
w Early procedure ≤ 3 weeks w Loco regional anesthesia w One day surgery w Use of tourniquet

Our series
w Quasi-normalization of range of
motion, strength and isocinetic tests w Return to preinjury activities (3 months)
at same level (94%) w Satisfying cosmetic aspect w Complications :
n Scar adherences n 1 Transitory radial nerve paralysis n 1 Median nerve paralysis 4 weeks after
procedure (past of anterior interosseous nerve syndrom) : re-intervention (scar ++ of residual lacertus fibrosus)
n 2 heterotopiques ossifications (no clinical consequences)

Our series
w Quasi-normalization of range of
motion, strength and isocinetic tests w Return to preinjury activities (3 months)
at same level (94%) w Satisfying cosmetic aspect w Complications :
n Scar adherences n 1 Transitory radial nerve paralysis n 1 Median nerve paralysis 4 weeks after
procedure (past of anterior interosseous nerve syndrom) : re-intervention (scar ++ of residual lacertus fibrosus)
n 2 heterotopiques ossifications (no clinical consequences)

Our series
w Quasi-normalization of range of
motion, strength and isocinetic tests w Return to preinjury activities (3 months)
at same level (94%) w Satisfying cosmetic aspect w Complications :
n Scar adherences n 1 Transitory radial nerve paralysis n 1 Median nerve paralysis 4 weeks after
procedure (past of anterior interosseous nerve syndrom) : re-intervention (scar ++ of residual lacertus fibrosus)
n 2 heterotopiques ossifications (no clinical consequences)

Our series
w Quasi-normalization of range of
motion, strength and isocinetic tests w Return to preinjury activities (3 months)
at same level (94%) w Satisfying cosmetic aspect w Complications :
n Scar adherences n 1 Transitory radial nerve paralysis n 1 Median nerve paralysis 4 weeks after
procedure (past of anterior interosseous nerve syndrom) : re-intervention (scar ++ of residual lacertus fibrosus)
n 2 heterotopiques ossifications (no clinical consequences)

Our series
w Quasi-normalization of range of
motion, strength and isocinetic tests w Return to preinjury activities (3 months)
at same level (94%) w Satisfying cosmetic aspect w Complications :
n Scar adherences n 1 Transitory radial nerve paralysis n 1 Median nerve paralysis 4 weeks after
procedure (past of anterior interosseous nerve syndrom) : re-intervention (scar ++ of residual lacertus fibrosus)
n 2 heterotopiques ossifications (no clinical consequences)

Conclusion w Reliable for acute lesions w Short learning curve w No necessity of a second approach (≠
endobutton) w Mini invasive procedure in a safe area
distant from neurovascular structures (decreasing risk of complications)
w Raisonnable Alternative to simple Tenodesis when functional , sports or cosmetic demands need an
Anatomical Restitution