+ diabetes maureen mcqueeney, pharmd, bcps, bcacp, cde
TRANSCRIPT

+
Diabetes
Maureen McQueeney, PharmD, BCPS, BCACP, CDE

+Learning Objectives
Describe each class of diabetic agents in detail including the following: efficacy, indications, advantages, adverse effects, contraindications and drug interactions.
Be familiar with how the oral and injectable agents compare in terms of their effect on weight, the lipid profile, cost, HbA1c reduction and fasting plasma reduction.
Demonstrate proper technique in preparing an insulin dose including the specific sequence of steps in mixing insulins where appropriate.
Describe medications that may cause hypo/hyperglycemia and potential drug interactions

Pathophysiology of DM
Glucagon
BG
BG

Pathophysiology of DM
Glucagon
BG
BG, but feedback is that there is no glucose to tissue
Little or no insulin secreted from pancreas
Insulin not working at
tissue receptors

+
Insulin from β-cells
Blood glucose homeostasis
Ingestion of food
Pancreas
-cells -cells
Glucagon from α-cells
Glucose production by liver
Glucose uptake by adipose
and muscle tissue
Release of gut hormones (Incretins:
GLP-1 and GIP)Glucose-dependent
Glucose-dependent
GI Tract
Merck Medicus. Accessed April10, 2008. For educational purposes only.
DPP-IV
Pathophysiology of DM5
In type 2 DM--- GLP-1and GIP with loss of effect

+
Diabetes Medications
6

+Patient Case #1
HPI: H.G is a 45 year old obese female who comes to your clinic for a follow-up on her blood results and to start a medication for her Type 2 DM. She refuses to start insulin at this point.
PMH: Type 2 diabetes (recently diagnosed) Hypertension x 2 years, hyperlipidemia
Medications: lisinopril 20 mg daily, hydrochlorothiazide 25 mg daily, aspirin 81 mg daily
7

+Patient Case #1
SH: Alcohol: (-), (-) Smoking
All: NKDA
PE: BP: 122/72, HR 77 Height: 5’5’’, Weight: 210 lbs, BMI: 35
Labs: FPG: 210 mg/dL; PPG: 200 mg/dL; HbA1c: 8.0%; Scr: 1.01; LFTs: WNLs
8

+Patient Case #1
Which of the following medications is the most appropriate initial medication for this patient?
Before we answer----lets talk about the options!!!!
9

+Biguanides1
Medications Metformin (Glucophage ®) Metformin ER (Glucophage XR ®, Fortamet ER
®)
Mechanism of action ↓ hepatic glucose production ↑ insulin sensitivity
Effects ↓ A1c by 1.5% ↓ FPG
10

+Biguanides1
Side effects Weight loss Transient N/V/D Lactic acidosis
Contraindications/Precaution Males w/SCr ≥ 1.5; females w/SCr ≥ 1.4 Caution in pts over 80 years of age
Additional comments May have positive effect on lipid profile ER formulation may be associated with less GI effects May be taken with food to decrease GI effects
11

+Sulfonylureas1
Medications Glipizide (Glucotrol ®) Glipizide ER (Glucotrol XL ®) Glyburide (Micronase ®, Diabeta ®) Glimepride (Amaryl ®)
Mechanism of action ↑ pancreatic beta cell insulin secretion in a glucose
independent manner
12

+Sulfonylureas1
Effects ↓ A1c by 1.5% ↓ FPG and PPG (mixed effect)
Side effects Hypoglycemia Weight gain
Additional comments Glyburide should not be used in CrCl < 50 ml/min Glipizide should be taken 30 minutes before meals Other agents should be taken with meals
13

+Short-Acting Secretagogues1
Medications Repaglinide (Prandin ®) Nateglinide (Starlix ®)
Mechanism of action ↑ pancreatic insulin secretion in a glucose-
dependent manner
Effects ↓ A1c by 0.6 – 1.5% ↓ PPG
14

+Short-Acting Secretagogues1
Side effects Weight gain Hypoglycemia
Additional comments Repaglinide more effective Less hypoglycemia than sulfonylureas Take before or with meals
Repaglinide: immediately before or with meals Nateglinide:1-30 minutes prior to meals
15
+Glucagon-Like Peptide 1 Agonists1,2
Medication Exenatide (Byetta ®) Liraglutide (Victoza®) Exenatide extended-release (Bydureon®)
Mechanism of action ↑ glucose-dependent insulin secretion ↓ glucagon secretion ↓ gastric emptying ↑ satiety
Effects ↓ A1c by 0.5 – 1.0% ↓ PPG
16

+Glucagon-Like Peptide 1 Agonists1,2
Side effects N/V/D Weight loss Headache Pancreatitis Hypoglycemia
Additional comments Subcutaneous injection Use with sulfonylureas: ↓ sulfonylurea dose by 50%
due to risk of hypoglycemia Take up to 60 minutes prior to morning and evening
meals
17

+Amylin Agonists1,3
Medication Pramlintide (Symlin ®)
Mechanism of action ↓ gastric emptying ↓ glucagon production ↑ satiety
Effects ↓ A1c by 0.5 – 0.7% ↓ PPG
18

+Amylin Agonists1,3
Side effects Nausea Anorexia Weight loss Hypoglycemia
Additional comments Subcutaneous injection Use with insulin: ↓ meal time insulin by 50% due to
risk of hypoglycemia Used in type 1 and 2 DM
19

+Dipeptidyl Peptidase 4 (DPP-4) Inhibitors4-6
Medications Sitagliptin (Januvia ®) Saxagliptin (Onglyza ®) Linagliptin (Tradjenta®)
Mechanism of action ↓ metabolism of incretin hormones
Effects ↓ A1c by 0.62 – 0.85% ↓ PPG
20

+DPP-4 Inhibitors4-6
Side effects Nasopharyngitis URI Headache Abdominal pain N/D Hypersensitivity Pancreatitis (with sitagliptin)
Additional comments Use with sulfonylureas: ↓ sulfonylurea dose by 50%
due to risk of hypoglycemia
21

+DPP-4 Inhibitors4-6
Renal adjustment Sitagliptin
CrCl< 50 ml/min: 50 mg daily CrCl< 30 ml/min: 25 mg daily
Saxagliptin CrCl< 50 ml/min: 2.5 mg daily
Drug Interactions Saxagliptin is a CYP 3A4 substrate
Caution with strong 3A4 inhibitors
22

+Back to Patient Case #1
HPI: HG is a 45 year old obese female who comes to your clinic for a follow-up on her blood results and start a medication for her Type 2 DM. She refuses to start insulin at this point.
PMH: Type 2 diabetes (recently diagnosed) Hypertension x 2 years, Hyperlipidemia
Medications: lisinopril 20 mg daily, hydrochlorothiazide 25 mg daily, aspirin 81 mg daily
23

+Back to Patient Case #1
SH: Alcohol: (-), (-) Smoking
All: NKDA
PE: BP: 122/72, HR: 77 Height: 5’5’’, Weight: 210 lbs, BMI: 35
Labs: FPG: 210 mg/dL; PPG: 200 mg/dL; HbA1c: 8.0%; Scr: 1.01; LFTs: WNLs
24

+Back to Patient Case #1
Which of the following medications is the most appropriate initial medication for this patient?
A. Glipizide
B. Sitagliptin
C. Pioglitazone
D. Metformin
25

+Patient Case #2
RE is a 75 year old female who was referred to you by her PCP for help with DM management. She was recently diagnosed with Type 2 DM. She has a history of CAD, hyperlipidemia, depression and HTN.
Her current medications include: aspirin 81mg daily, Diovan 320 mg daily, Plavix 75 mg, ranitidine 150mg PO BID, NTG PRN, metoprololsuccinate 50 mg daily, Crestor 40 mg daily, Cymbalta 90 mg daily
26

+Patient Case #2
Allergies/intolerances: ACEIs - cough
Vital signs: BP: 123/61, HR: 62, wt: 135 lbs, ht: 5’5”,
Labs: A1c 7.9%, Scr 1.43, LFTs: WNLs, CrCl: 31 ml/min
Social pearls Patient has Medicare Part D and is very concerned
about reaching her the “donut hole”
27

+Patient Case #2
Which of the following is most appropriate initial treatment for this patients DM?
A. Glyburide 2.5 mg PO BID
B. Metformin 500 mg PO BID
C. Saxagliptin 5 mg daily
D. Glipizide 2.5 mg PO BID
28

+Insulin Therapy
29

+Insulin Therapy
Medications Aspart (Novolog ®) Lispro (Humalog ®) Glulisine (Apidra ®) Regular (Humulin R ®, Novolin R ®) NPH (Humulin N ®, Novolin N ®) Glargine (Lantus ®) Detemir (Levemir ®)
30

+Insulin TherapyMedication (continued)
Humalog Mix 75/25 ® 75% lispro protamine/25% lispro
Humalog Mix 50/50 ® 50% lispro protamine/50% lispro
Novolog Mix 70/30 ® 70% aspart protamine/30% aspart
Humulin Mix 70/30 ® and Novolin Mix 70/30 ® 70% NPH/30% regular
Humulin Mix 50/50 ® 50% NPH/50% regular
31

+Insulin Therapy7
32

+Insulin Therapy1
Mechanism of Action Exogenous administration of insulin
Side effects Hypoglycemia Weight gain
Additional comments Subcutaneous injection Most effective treatment Positive effect on HDL and TGs Glargine and detemir cannot be mixed
33

+Insulin Regimens8
Nonphysiologic Insulin regimen
34

+Insulin Regimens8
Physiologic insulin regimen
35

+Initiation of Insulin per ADA Guidelines10 36

37

+Insulin Titration11-12
Treat-to-Target algorithm
.
38

+Sliding Scale Insulin13,14
Advantages Convenient and simple to initiate Patient involvement in his/her therapy Can be used to supplement scheduled insulin doses
Disadvantages Not supported by clinical literature Treats hyperglycemia instead of preventing it Lag time to onset of insulin Poor glycemic control Patient adherence and competency required
Not recommended in outpatient setting per ADA
39

+Adjusting Insulin Therapy15
Type Injection Time Affected BG reading
Rapid or Short-acting
Before Breakfast Before Lunch
Before Lunch Before Supper
Before Supper 2-3 hrs after supper or bedtime
Intermediate-acting or mixed
insulin
Before Breakfast Before Supper
Before Supper/Bedtime
Before Breakfast (next morning)
Long-acting Before Bedtime Throughout the day
40

+ Converting Between Types of Insulin18-20
Types of Insulin Recommendation
NPH to detemir Convert unit-per-unitGive detemir once daily or BID
NPH to glargine NPH once daily: unit-per-unit give once dailyNPH twice daily: added total NPH dose and reduce by 20% give once daily
Detemir or glargine to NPH
Convert unit-per-unitGive NPH at bedtime or BID
Detemir to glargine or glargine to detemir
Concert unit-per-unitGive once daily or BID if necessary
41

+Converting Between Types of Insulin Regimens21
Regular to Rapid Total up daily dose then split between meals
One basal injection → Add rapid-acting insulin at largest meal Give 10% of total daily dose as rapid-acting analog at
largest meal Reduce basal dose by 10% Can give additional insulin injections before all meals if
necessary
42

+Converting Between Types of Insulin Regimens21
One basal injection → Two premix injections Divide total daily dose in half
Give pre-breakfast and pre-supper premix insulin The largest meal requires a larger proportion of
insulin Reduce total dose by 20% if recurrent hypoglycemia
One premix injection → 2 premix injections Divide TDD in half
Give before breakfast and dinner Reduce total dose by 20% if recurrent hypoglycemia
43

+Conversion Example
Convert to physiologic regimen using Lantus and Humalog insulin
Insulin AM PM
NPH 8 12
Regular 6 10
44

+Conversion Example
What should the total Lantus® dose be? A. 20 units B. 18 units C. 16 units D. 14 units
What should the Humalog® dose be? A. 5 units before breakfast, lunch and dinner B. 5 units before breakfast and lunch and 6 units before
dinner C. 8 units before breakfast and dinner D. 6 units before breakfast and 10 units before dinner
45

+
Treatment Strategies
46

+Contributions of FPG and PPG to Overall A1C
22
Post-Prandial
Fasting
Diabetes Care. 2003;26:881-885.47

+

+AACE Treatment Guidelines23
Monotherapy: HbA1c 6-7% Options: metformin, TZDs, secretagogues, DPP-4 inhibitors, alpha-
glucosidase inhibitors Monitor and titrate every 2-3 months Consider combination therapy if goals not met after 2-3 months
Combination therapy: HbA1c 6-7%
Initiation/intensify combination therapy: A1c 8-10%
Initiate/intensify insulin: A1c > 10%
Consider basal-bolus insulin therapy: A1c > 8.5%
49

+Patient Case #3
HPI: AT is a 64 year old female with a history of Type 2 DM. She is reporting to clinic for evaluation of DM control.
PMH: Type 2 DM since 2005, hyperlipidemia, depression and GERD
Medications: metformin 1000 mg PO BID, glyburide 10mg PO BID, omeprazole 20 mg daily, Lipitor 20 mg daily
50

+Patient Case #3
Allergies: NKDA
SH: (+) smoking: 1 ppd, occ ETOH
Vital signs: BP: 149/58, HR: 60, Height: 63.5 in, Weight: 138 lbs
BG per glucometer: FBG: 80s-110s, PPG: 200-220s
51

+Patient Case #3
Labs: A1c: 7.3% Scr: 0.71
LFTs: WNLs Total cholesterol: 138
Triglycerides 121 HDL: 31
LDL: 83
Social pearls Patient refuses to start insulin therapy at this point
despite extensive education regarding the benefits of insulin therapy. She is fearful of the injection and potential for weight gain.
52

+Patient Case #3 Which of the following treatment recommendations
would be the most appropriate for this patient? A. Sitagliptin 100 mg daily
B. Byetta 10 mcg SC before breakfast and dinner
C. Nateglinide 60mg PO TID
D. Pioglitazone 30 mg PO daily
53

+Patient Case #4 GR is a 57 year obese male with a PMH
history of Type 2 DM, hyperlipidemia and HTN who reports to the clinic for a follow up on his DM management and to discuss weight loss options.
Medications: metformin 850 mg PO TID, simvastatin 80 mg QHS, lisinopril 80 mg daily, diltiazem ER 360 mg daily, nefazodone 300mg PO BID
Allergies: NKDA
54
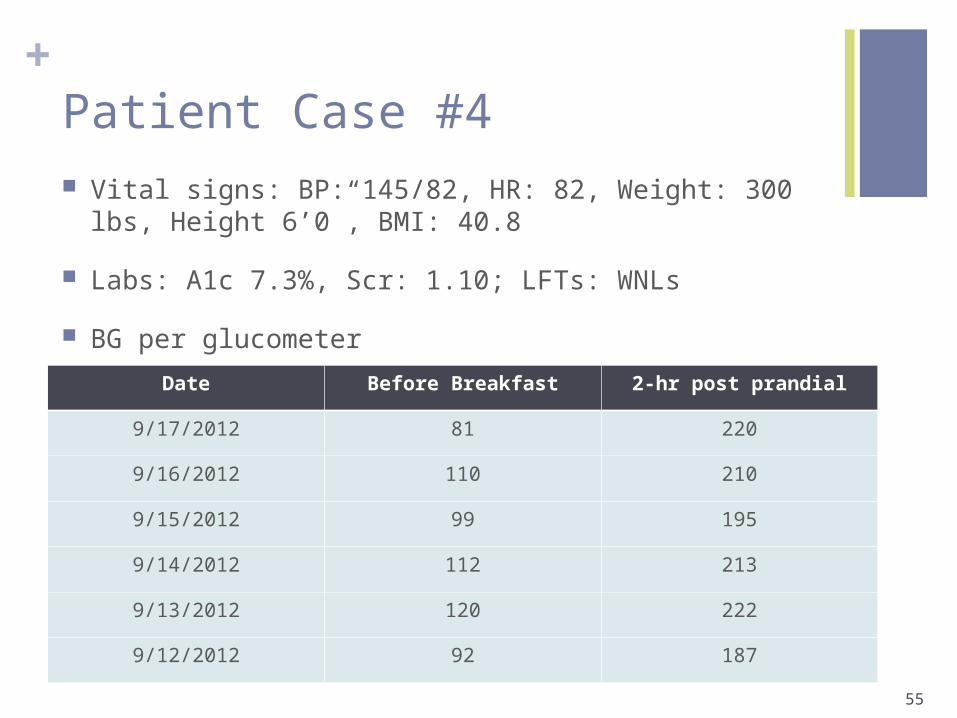
+Patient Case #4 Vital signs: BP: 145/82, HR: 82, Weight: 300 lbs, Height
6’0”, BMI: 40.8
Labs: A1c 7.3%, Scr: 1.10; LFTs: WNLs
BG per glucometer
55
Date Before Breakfast 2-hr post prandial
9/17/2012 81 220
9/16/2012 110 210
9/15/2012 99 195
9/14/2012 112 213
9/13/2012 120 222
9/12/2012 92 187

+Patient Case #4 Which of the following is most appropriate
recommendation for management of GRs DM?
A. Byetta 5 mcg SC BID
B. Saxagliptin 5 mg PO daily
C. Humalog 4 units before largest meal
D. Lantus 10 units QHS
56
+Patient Case #5
EM is a 54 year old male who was recently started on Lantus insulin. You were asked to make a recommendation regarding his diabetes regimen. He is currently taking metformin 1000mg PO BID, glyburide 10 mg PO BID and Lantus 38 units at bedtime (increased from 30 units last week), simvastatin 80mg QHS and lisinopril 20 mg daily
57

+Patient Case #5
BG per patient glucometer
58
Date Before Breakfast Bedtime
9/17/2012 267
9/16/2012 227 248
9/15/2012 215
9/14/2012 302
9/13/2012 274
9/12/2012 168

+Patient Case #5
SH: (+) smoking: 1 ppd, occ ETOH
Vital signs: BP: 130/58, HR: 60, Height: 67 in, Weight: 255 lbs
Fasting Lipid panelTotal Cholesterol: 148 Triglycerides: 289HDL: 30 LDL: 65
Labs: A1c: 9.5%; Scr 1.13 mg/dL
59

+Patient Case #5
What is the most appropriate recommendation for this patients DM treatment?
A. Increase Lantus insulin to 40 units
B. Add Humalog 4 units before his biggest meal
C. Increase Lantus insulin to 46 units
D. Increase Lantus insulin to 44 units and add Humalog 4 units before breakfast and dinner
60
+Patient Case # 6
EM comes back to the clinic after several visits and his current diabetes regimen includes: metformin 1000mg PO BID, Lantus insulin 60 units QHS.
Most recent labs A1c: 7.3% SCr: 1.13 mg/dL FPG 80-110s
61
+Patient Case #6
What would be the most appropriate recommendation at this time?
A) Increase Lantus to 65 units
B) Add Januvia 100 mg daily
C) Advise patient to test BS before meals and at bedtime
D) Add 10 units of Regular insulin before breakfast
62
+Patient Case #6
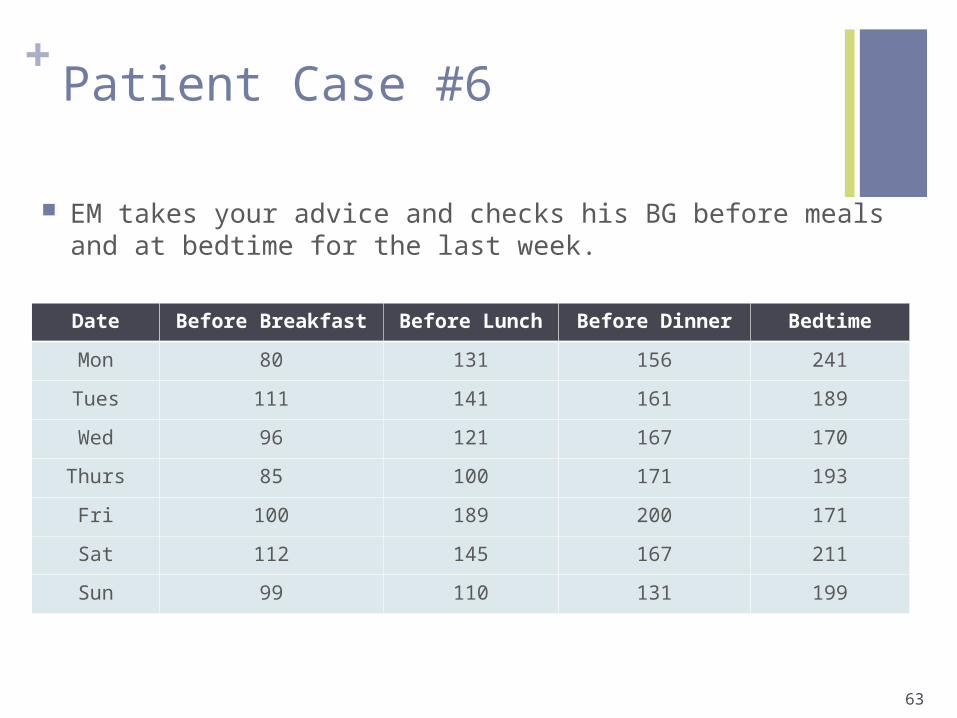
EM takes your advice and checks his BG before meals and at bedtime for the last week.
63
Date Before Breakfast Before Lunch Before Dinner Bedtime
Mon 80 131 156 241
Tues 111 141 161 189
Wed 96 121 167 170
Thurs 85 100 171 193
Fri 100 189 200 171
Sat 112 145 167 211
Sun 99 110 131 199

+Patient Case #6
What would be the most appropriate recommendation for EM at this time?
Add Humalog 4 units before breakfast
Add Apidra 4 units before lunch
Add Novolog 4 units before dinner
64

+
Insulin Administration

+
ADMINISTRATION OF INSULIN Preparation of insulin using vial and syringe:
Hands and injection should be cleaned Remove the cap on the insulin vial and sterilize the top
with an alcohol swab If using NPH or mixed insulin roll gently between hands Do not shake vigorously
Draw air into the syringe that is equal to the amount of insulin to be injected and push that air into the vial
Draw up amount of insulin to be given Air bubbles not dangerous Can cause less dose to be injected

+
ADMINISTRATION OF INSULIN Preparation of insulin by insulin pen device
Hands and injection site should be cleaned Wipe the rubber seal on the pen body with an
alcohol swab If using NPH or mixed insulin roll the pen gently
between handsDo not shake
Prime the pen by dialing to 2 units of insulin (do this with every use)
Select the required dose by turning the dial until it reached the desired dose

+
ADMINISTRATION OF INSULIN Subcutaneous technique
Lightly grasp a fold of skin (“pinch an inch”) Inject at a 90° angle Release the skin fold Push the plunger down Wait at least 5 seconds after complete depression of
plunger If painful, blood or clear fluid is seen after withdrawing
the needle, apply pressure for 5-10 seconds without rubbing

+ADMINISTRATION OF INSULIN
Rate of absorption: abdomen > arms > thighs > buttocks area

+
MIXING OF INSULIN
Column 1_____________________ _Column 2
Humalog NPH
Novolog Glargine
Regular Detemir
Apidra

+QUESTIONS?
71

+References
1. Nathan DM, Buse JB, Davidson MB, et al. Medical management of hyperglycemia in type 2 diabetes: a consensus algorithm for the initiation and adjustment of therapy. Diabetes Care 2008;31:1-11.
2. Byetta [package insert]. San Diego (NC): Amylin Pharmaceuticals, Inc and Eli Lilly and Company; 2007.
3. Symlin [package insert]. San Diego (NC): Amylin Pharmaceuticals, Inc; 2005.4. Covey DF, Rodgers PT. New therapeutics options for improving glycemic
control in patients with type 2 diabetes mellitus.5. Januvia [package insert]. Whitehouse Station (NJ): MERCK & CO., INC.;2008 6. Onglyza [package insert]. Princeton (NJ): Bristol-Myers Squibb; 20097. Lexi-Comp Online™, Hudson, Ohio: Lexi-Comp, Inc.; 2008; November 2, 2008. 8. DeWitt DE, Dugdale DC. Using new insulin strategies in the outpatient
treatment of diabetes. JAMA 2003;289(17):2254-2264.9. Dipiro JT, Wells BG, Schwinghammer TL, Hamilton CW. Pharmacotherapy
handbook. 6th ed. New York: McGraw-Hill, 2006.10. Nathan DM, Buse JB, Davidson MB, et al. Medical management of
hyperglycemia in type 2 diabetes: a consensus algorithm for the initiation and adjustment of therapy. Diabetes Care 2008;31(12):1–11. Nathan DM, Buse JB, Davidson MB, et al. Medical management of hyperglycemia in type 2 diabetes: a consensus algorithm for the initiation and adjustment of therapy. Diabetes Care 2008;31(12):1–11.
72

+References
11. Riddle MC, Rosenstock J, and Gerich J. The Treat-to-target trial: randomized addition of glargine or human NPH insulin to oral therapy of type 2 diabetic patients. Diabetes Care 2003;26(11):3080-3086.
12. Unger Jeff. Management of Type 1 Diabetes. Prim Care Clin Office Pract. 2007; 34: 791-808.
13. Umpierrez GE, Palacio A, Smiley D. Sliding scale insulin use: myth or insanity? The American Journal of Medicine 2007; 120: 563-567.
14. Hirsch IB, Farkas-Hirsch R. Sliding scale or sliding scare: it’s all sliding nonsense. Diabetes Spectrum 2001; 14(2): 79-81.
15. Carlise BA, Kroon LA, Koda-Kimble MA. Diabetes mellitus. In: Koda-Kimble MA, Young LY, Kradjan WA, Guglielmo BJ, editors. Applied therapeutics: the clinical use of drugs. 8th edition. Philadelphia, PA: Lippincott Williams & Wilkins; 2005.
16. Garber A, Wahlen J, Wahl T, et al. Attainment of glycaemic goals in type 2 diabetes with once-, twice-, or thrice-daily dosing with biphasic insulin aspart 70/30 (the 1-2-3). Diabetes Obes Metab. 2006; 8(1): 58-66.
17. Raskin P, Allen E, Hollander P, et al. Initiating insulin therapy in type 2 diabetes: a comparison of biphasic and basal insulin analogs. Diabetes Care. 2005;28(2):260-265.
18. Levemir [package insert]. Princeton (NJ): Novo Nordisk Inc;200719 Lantus [package inser]. Bridgewater (NJ): Sanofi-Aventis U.S. LLC; 200720. U.S. Food and Drug Administration. Information regarding storage and switching between
products in an emergency. http://www.fda.gov/Drugs/EmergencyPreparedness/ucm085213.htm (accessed October 10, 2009).
21. Hirsch IB, et al. A real-world approach to insulin therapy in primary care practice. Clinical Diabetes 2005; 23: 78-86.
73

+References
22. Monnier L, Lapinski H, Colette C. Contributions of fasting and postprandial plasma glucose increments to the overall diurnal hyperglycemia of type 2 diabetic patients: variations with increasing levels of HbA1c. Diabetes Care. 2003; 26: 881-885.
23. Rodbard HW, Blonde L, Braithwaite SS, et al. American association of clinical endocrinologists medical guidelines for clinical practice for the management of diabetes mellitus. Endocr Pract 2007;13 (supp 1):s3-68.
24. Grundy SM, Cleeman JI, Merz CN, Brewer HB Jr, Clark LT, Hunninghake DB,Pasternak RC, Smith
SC Jr, Stone NJ. Implications of recent clinical trials for theNational Cholesterol Education Program
Adult Treatment Panel III guidelines. Circulation 2004 Jul 13;110(2):227-39.25. Cholesterol-lowering agents. Pharmacist's Letter/Prescriber's Letter
2006;22(8):220802.

+Questions