연세대학교 원주의과대학 원주기독병원 감염내과 · 2016-09-06 · – a boy who...
TRANSCRIPT

수술부위 감염관리
연세대학교 원주의과대학 원주기독병원 감염내과
김 영 근

SENIC study Study on the Efficacy of Nosocomial Infection Control
0%
10%
20%
30%
Relative change in NI in a 5 year period (1970-1975)
-31% -35% -35%
-27% -32%
-40%
-30%
-20%
-10%
With infection control
14% 9%
19%
26%
18%
Without infection control
LRTI SSI UTI BSI Total
Haley RW et al. Am J Epidemiol 1985;121(2):182-205
50%

• Operating room: little better than kitchen table
• Nearly half of people died from blood poisoning
after op. 1-2 days after op. the op wound
became red and inflamedfeverdied
• Louis Pasteur’s paper
– A boy who had broken his leg
OP. after wash his and his assistant’s hand, patient’s wound
with Carbolic acid after 4 days there were no sign of fever and
blood poisoning. After six weeks the boy was able to work
Joseph Lister (1827-1912)

• Mortality after amputation
Joseph Lister
Year Total Death Mortality rate(%)
1864-1866(before)
1867-1869(after)
35
40
16
6
46
15
현대 수술실에서의 감염관리/소독제의
사용의 기초
수술부위 창상감염 (Surgical Site Infection)
-
• 수술부위 감염: 전체 병원감염 중 2-3위 (약 20%)
• 수술환자 중 병원감염의 38%는 수술부위감염
• 수술의 약 2%에서 발생
• 수술부위감염 발생시 문제점 – 입원 기간의 연장: 6.5일 (US), 20.4일 (Korea)
– 추가 의료비용 발생: 최소추정 추가비용 3,317,812원
– 의료분쟁: 병원감염 관련 의료분쟁의 68%는 수술로 인한 것임
– 사망률 증가: 감염이 있는 경우 2배 증가
• 적극적인 감염관리 활동을 통해 약 35%까지 예방 가능

수술부위 감염 (SENIC 연구, 1970 vs 1975)
감염발생 감시를 기초로 한 관리
집도의에게 감염률 보고
20% 감소
+ 역량 있는 감염관리의사의 활동
35% 감소

수술부위 감염
• Infection occurs within 30 days
after the operation
• Within 1 year if implant is in
place and the infection appears to
be related to the operation
7
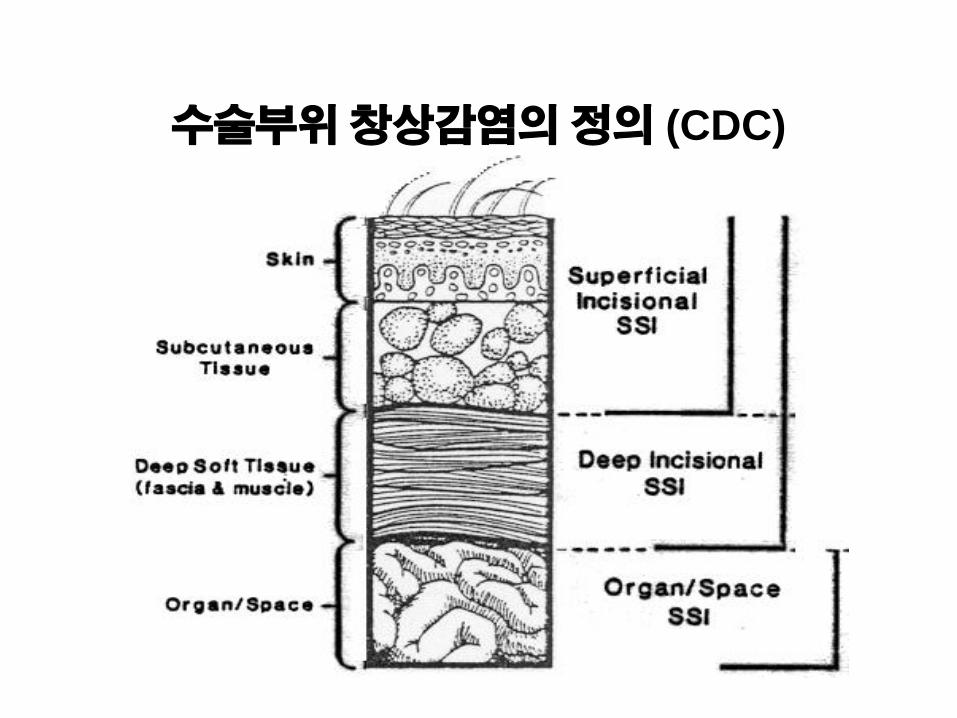
수술부위 창상감염의 정의 (CDC)

발병기전

Source of Pathogens
Endogenous flora
• Patient’s skin • Mucous
membranes • Hollow viscera
Exogenous sources
• surgical personnel
• operating room environment
• all tools, instruments, and materials

수술부위 창상감염의 주요 원인균
Pathogen Percent of Infections
Staphylococcus aureus
Coagulase-negative staphylococci
Enterococci
Escherichia coli
Pseudomonas aeruginosa
Enterobacter spp.
Proteus mirabilis
Klebsiella pneumoniae
Other streptococcal spp.
Candida albicans
Group D Streptococci
Bacteroides fragilis
Other gram-positive aerobes
20
14
12
8
8
7
3
3
3
2
2
2
2
NNIS, January 1990 to March 1996 (n=17,671)

Risk of SSI
Reduce the inoculum of bacteria at the surgical site
Surgical Site Preparation
Antibiotic Prophylaxis Strategies
Optimize the microenvironment of the surgical site
Enhance the physiology of the host (host defenses)
Strategies to prevent SSI
Dose of bacterial contamination x virulence
Resistance of the host patient

Risk and Prevention
– Patient-related (intrinsic)
– Pre-operative
– Operative

Patient-related factors
• Age
• Nutritional status
• Diabetes
• Smoking
• Obesity
• Coexistent infections at a remote body site
• Colonization with microorganisms
• Altered immune response
• Length of preoperative stay
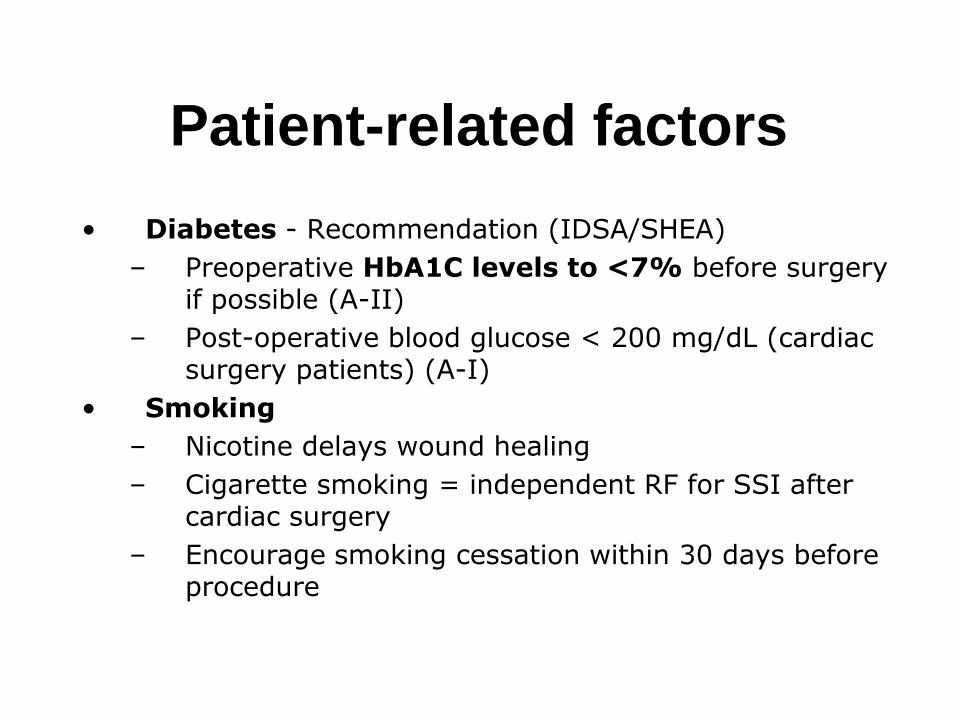
Patient-related factors
• Diabetes - Recommendation (IDSA/SHEA)
– Preoperative HbA1C levels to <7% before surgery if possible (A-II)
– Post-operative blood glucose < 200 mg/dL (cardiac surgery patients) (A-I)
• Smoking
– Nicotine delays wound healing
– Cigarette smoking = independent RF for SSI after cardiac surgery
– Encourage smoking cessation within 30 days before procedure

Operation-relative
• Preoperative issue
– Duration of surgical scrub
– Skin antisepsis
– Preoperative shaving
– Preoperative skin prep
– Antimicrobial prophylaxis
• Intraoperative issue
– Duration of operation
– Operating room ventilation
– Inadequate sterilization of
instruments
– Foreign material in the
surgical site
– Surgical drains
– Surgical technique
• Poor hemostasis
• Failure to obliterate dead space
• Tissue trauma

Preoperative showering
• Advise patients to shower or have a bath (or help patients to shower, bath or bed bath)
• Using soap
• The day before, or on the day of, surgery

Hair removal
• Hair removal
– Increase the rate of SSI
• If hair has to be removed
– Use electric clippers with a single-use head on the day of surgery
– Do not use razors for hair removal
x

Theatre wear
• Patient
– Give patients specific theatre wear
– Consider also the patient’s comfort and dignity
• Staff
– All staff should wear specific non-sterile
theatre wear in all areas where
operations are undertaken

Staff leaving the operating area
• Staff wearing non-sterile theatre
wear should keep their
movements in and out of the
operating area to a minimum

Nasal decontamination
• Do not use nasal decontamination with topical antimicrobial agents aimed at eliminating S. aureus routinely

Mechanical bowel
preparation
• Do not use mechanical bowel
preparation routinely

Hand jewellery, artificial
nails and nail polish
• should remove hand jewellery before operations
• should remove artificial nails and nail polish before operations

Antimicrobial prophylaxis for surgery
• Clean surgery involving the placement of a prosthesis or implant
• Clean-contaminated surgery
• Contaminated surgery

Antimicrobial prophylaxis for surgery
• Surgical wound classification
• Timing
• Re-dosing

Surgical Wound Classification
창상 분류 원인균 감염원 감염률 예
Class I
청결 (clean)
그람
양성균
수술실, 의료진, 환자 피부
1-2% 갑상선수술, 헤르니아 꿰멤술, 유방암수술
Class II
청결오염
(clean-contaminated)
혼합균 장관 내 집락균 2-4% 계획되어진 대장수술, 위십이지장 수술, 담도수술, 제왕절개술
Class III
오염 (contaminated)
혼합균
전반적인 집락균
7-10% 위 또는 장 천공
Open cardiac massage
Class IV
불결 (Dirty)
혼합균 이미 존재하는 병원균
10-40% 복강 내 농양, 괴사된 장 절제술
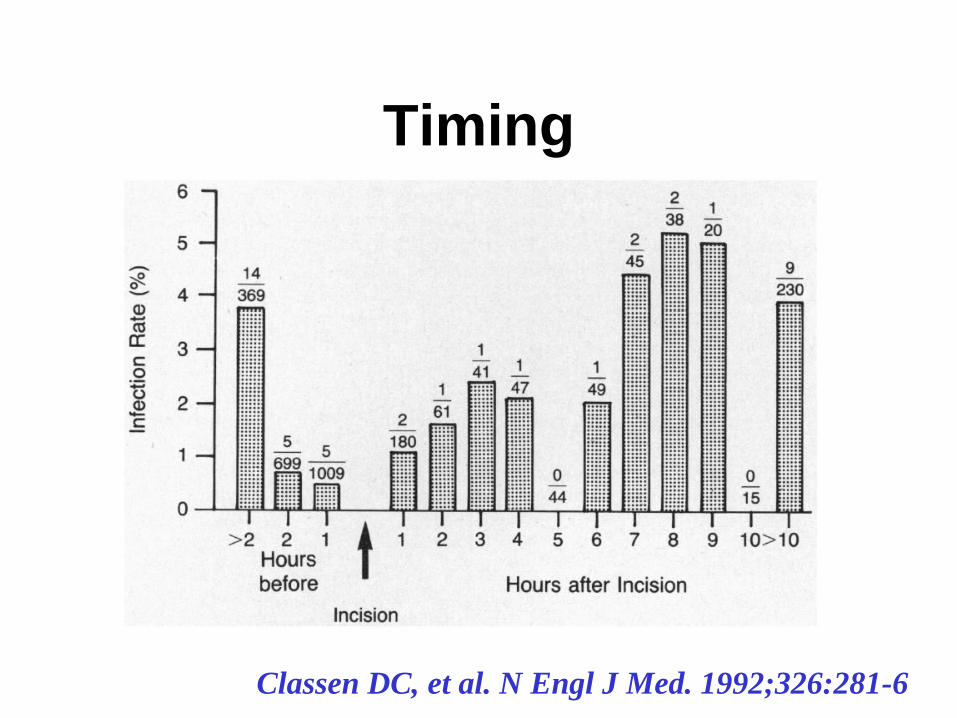
Timing
Classen DC, et al. N Engl J Med. 1992;326:281-6

Re-dosing during surgery
2013 Surgical Prophylaxis. ASHP, IDSA, SHEA, SIS. Am J Health-Syst Pharm. 2013; 70:195-283

Antimicrobial prophylaxis
• Duration of prophylaxis (A-I)
– Stop prophylaxis
• within 24 hours after the procedure
• within 48 hours after cardiac surgery
– To:
• Decrease selection of antibiotic resistance
• Contain costs
• Limit adverse events
Bratzler et al Arch Surg 2005, 140:174-82
Harbarth S et al. Circulation 2000;101:2916–2921

Skin preparation and scrub
Surgical Scrub 3-5분이면 충분
Prepare the skin at the surgical site immediately before
incision using an antiseptic (aqueous or alcohol-based)
preparation: povidone-iodine or chlorhexidine are
most suitable

Incise drapes
• Do not use non-iodophor-impregnated incise drapes routinely for surgery

Incise drapes
• Use an iodophor-impregnated drape unless the patient has an iodine allergy if an incise drape is required

Diathermy
• Do not use diathermy for surgical incision to reduce the risk of surgical site infection

Wound irrigation and
intracavity lavage
• Do not use wound irrigation to reduce the risk of surgical site infection
• Do not use intracavity lavage to reduce the risk of surgical site infection
34

Operation room environment
• Ventilation
– Positive pressure
– 15 air changes of fillered air/hour
– Ultraclean air (laminar flow) – THR, TKR
• Tacky mats – no effect
• Microbiologic sampling
– No recommended
• Appropriate sterilization for surgical instruments

Surgeon Skill and Technique
• Excellent surgical technique
reduces the risk of SSI (A-III)
수술부위 창상감염의 예방
• 수술 전 처치
– 감염의 조절, 당뇨의 조절, 금연
– 피부준비 • 필요한 경우만 수술직전에 삭모(Electric clipper사용)
• 소독제 도포
– 수술 전 입원기간의 단축
– 올바른 Surgical Scrub (3-5분)
– 적절한 예방적 항생제 사용

수술부위 창상감염의 예방
• 수술 중 처치
– 수술 중 사람의 움직임을 줄인다.
– 외과적 무균술: 수술기구, 수술팀복장
– 세심한 술기: Debridement, Irrigation,
Bleeding control, FB removal
– Preserve Oxygenation and Perfusion

수술부위 창상감염의 예방
• 수술 후 처치
– 절개부위는 24~48시간정도 멸균 드레싱으로 보호
– 드레싱 교환 전. 후 손 씻기
– 드레싱 교환 시 무균법 준수
– 수술부위의 세밀한 관찰
– 배농관: 밀폐배농관 사용, 주 수술부위와 떨어진 곳에 삽입, 가능하면 빨리 제거

SSI SURVEILLANCE

Active surveillance
Courtesy: Astagneau, SFHH 2007

Risk Stratification
1) intrinsic degree of microbial
contamination of the surgical site
2) duration of an operation
3) markers for host susceptibility

Risk Stratification
SENIC Project
• abdominal operation
• lasting >2 hours
• wound classification
of contaminated or
dirty/infected
• patient having >3
discharge diagnoses
NNIS Risk Index (0-3)
• American Society of
Anesthesiologists (ASA)
Physical Status
Classification of >2
• either contaminated or
dirty/infected wound
classification
• length of operation > T
hours (75th percentile)
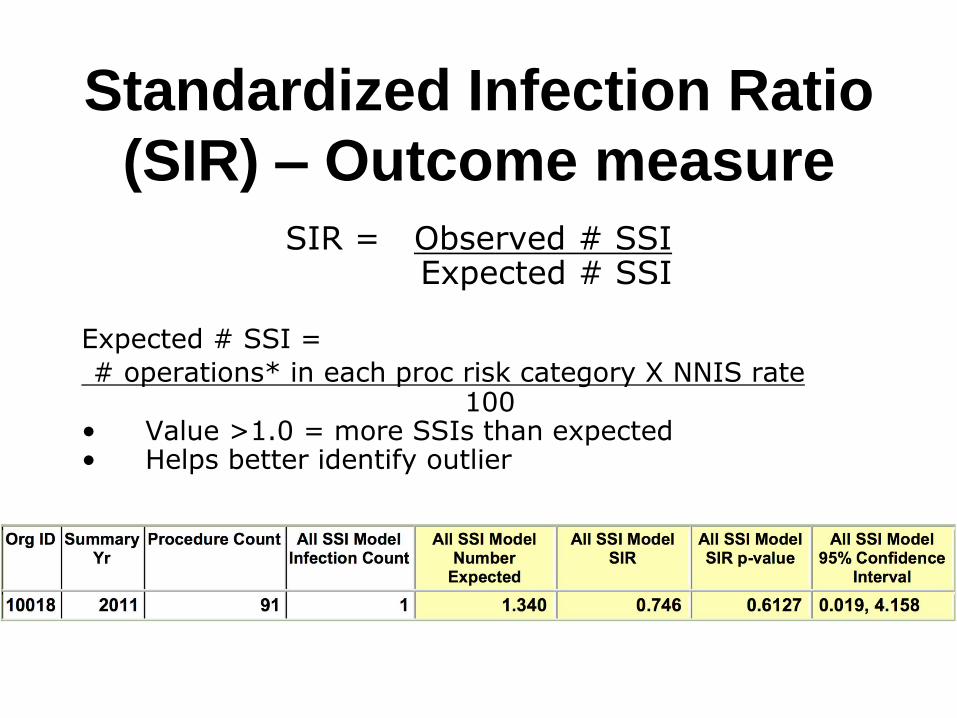
Standardized Infection Ratio
(SIR) – Outcome measure
SIR = Observed # SSI Expected # SSI
Expected # SSI =
# operations* in each proc risk category X NNIS rate 100 • Value >1.0 = more SSIs than expected • Helps better identify outlier
Surveillance Methods
• Inpatient
• Postdischarge
• Outpatient

Inpatient SSI Surveillance
• Direct observation – Surgeon
– Trained nurse surveyor
– Infection control personnel
• Indirect observation – Infection control personnel
– Review of laboratory reports, patient records
– Discussions with primary care providers

Postdischarge SSI
Surveillance
• direct examination of patients’ wounds
during follow-up visits to either surgery
clinics or physicians’ offices
• review of medical records of surgery clinic
patients
• patient surveys by mail or telephone
• surgeon surveys by mail or telephone

Outpatient SSI Surveillance
• Direct and indirect methods

Reference
• Guideline for Prevention of Surgical Site Infection, 1999. Centers for Disease Control and Prevention (CDC) Hospital Infection Control Practices Advisory Committee. (Am J Infect Control. 1999 Apr;27(2):97-132) - http://www.cdc.gov/hicpac/pdf/SSIguidelines.pdf
• Surgical site infections: prevention and treatment. NICE guidelines [CG74] Published date: October 2008 - http://www.nice.org.uk/guidance/cg74)
50
감사합니다