© 2014 kaufman, hall & associates, inc. all rights reserved. insurance exchanges – public...
TRANSCRIPT
© 2014 Kaufman, Hall & Associates, Inc. All rights reserved.
Insurance Exchanges – Public & Private Implications for Hospitals
GSMC| 2014 Fall Conference and Annual MeetingYoung Harris, GA| October 2, 2014

GSMC 2014 Fall Conference & Annual Meeting 2
Meeting Agenda• Introductions• Private exchanges
– What are private exchanges and how do they work?– Private exchange adoption outlook– Implications for hospitals and health systems
• Public exchange update– National– Georgia
• Narrow network prospects and implications• Summary implications• Questions
GSMC 2014 Fall Conference & Annual Meeting 3
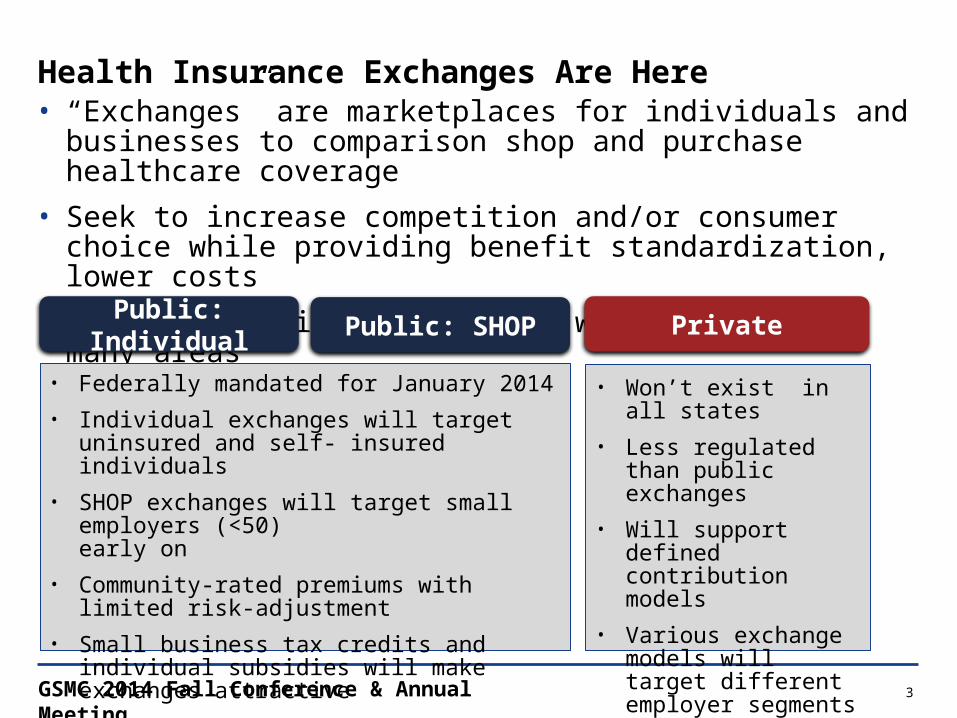
Health Insurance Exchanges Are Here• “Exchanges” are marketplaces for individuals and businesses to
comparison shop and purchase healthcare coverage• Seek to increase competition and/or consumer choice while providing
benefit standardization, lower costs• Public and private exchanges will co-exist in many areas
Public: Individual Public: SHOP Private
• Federally mandated for January 2014 • Individual exchanges will target uninsured and self-
insured individuals • SHOP exchanges will target small employers (<50)
early on• Community-rated premiums with limited risk-
adjustment • Small business tax credits and individual subsidies
will make exchanges attractive
• Won’t exist in all states• Less regulated than
public exchanges• Will support defined
contribution models• Various exchange models
will target different employer segments

GSMC 2014 Fall Conference & Annual Meeting 4
Private Exchanges – What Are They And How Do They Work?

GSMC 2014 Fall Conference & Annual Meeting 5
Private Exchanges – What Are They?As the commercial insurance market continues to move from defined benefit to
defined contribution plans, employers will seek new benefit models to maximize or cap the value of their healthcare benefit subsidies
Private Exchange Sponsors
Defined ContributionDefined Benefit
Private exchanges will support this market shift by offering a broader choice of plan and coverage options sponsored by a variety of organizations

GSMC 2014 Fall Conference & Annual Meeting 6
Private Exchange Adoption Outlook

GSMC 2014 Fall Conference & Annual Meeting 7
Private Exchange Activity Occurs Across a Range of Employer Sizes
Small to Midsize Employers
Large Employers
Midsize to Large Employers
Liazon Forges Partnerships with National Brokers
Mercer Announces 2014 Private Exchange Participants
Walgreens Joins AON Hewitt Private Exchange
BAN/USI have 150 US offices; Liazon exchange
includes 2,000 employers
33 mostly midsize companies across range of industries will
enroll 75K employees
160K Walgreen’s employees will enroll in 2014; total AON 2014 enrollment will be 600K
Note: 600K AON enrollees includes employees and dependents across 18 employers, an increase of 15 employers vs. the 3 employers enrolled in 2013. Sources: Shutan, B: “BAN Partners with Liazon,” Health Insurance Exchange News, Sept 17, 2013. “USI Helps Clients Manage Employee Benefits Through Launch of Private Insurance Exchange,” Fort Mill Times, Oct 17, 2013. McCann, D: “Midsize Companies Move to Private Health Exchanges,” CFO.com, Oct 15, 2013. Armstrong D, “Walgreen Joins in Exodus of Workers to Private Exchanges,” Bloomberg, 18 Sept, 2013. “Private Exchanges Woo More Employers, But Real Traction Won’t Begin Until 2015,” Inside Health Insurance Exchanges, Aug 15, 2013.

GSMC 2014 Fall Conference & Annual Meeting 8
2014 Enrollment Amongst Select Major Private Exchange Operators Has Reached 1.2 Million Commercial Lives
Exchange Operator
# of 2014 Enrollees
# of 2014 Employers
# of Enrollees per Employer
600,000 18 33,333
400,000 14 28,571
100,000 2,400 42
75,000 33 2,273
46,500 3 15,500
Total 1,221,500 2,468 495
Private exchange operators are quickly growing their enrollee bases and appealing to employers of all sizes
Source: Company press releases and investor conference calls.

GSMC 2014 Fall Conference & Annual Meeting 9
Early Adopters Include Many Household Names with Outsized Representation by the Retail and Restaurant Industries

GSMC 2014 Fall Conference & Annual Meeting 10
Drivers That Could Impact Commercial Shift to Private Exchanges
Driver Influence Factors Shift Impact
“Me Too” Effect Secondary wave of “fast followers” will emerge if initial wave of employers demonstrates success
↑Rising Administrative Costs Employers continue to look for ways to lower
administrative expenses of employee benefitsDelivery Cost Favorable insurer network contracts will increase plan
participation and pressure on employers to shiftCadillac Tax Some employers may use private exchanges to avoid
the excise tax stipulated to begin in 2018Exchange Plan Options and Premiums
Plan designs and premiums must be as good or better than current group coverage ↔
Paternalism Employers can be paternalistic and resistant to significant changes in employee benefit design ↓Union and Public Sector Collectively bargained cohorts and public sector employers typically are slower to change
Source: “Sizing Up The Healthcare Exchanges - Big Long-Term Opportunity,” Credit Suisse, Sept 26, 2013.

GSMC 2014 Fall Conference & Annual Meeting 11
Implications for Hospitals and Health Systems
GSMC 2014 Fall Conference & Annual Meeting 12
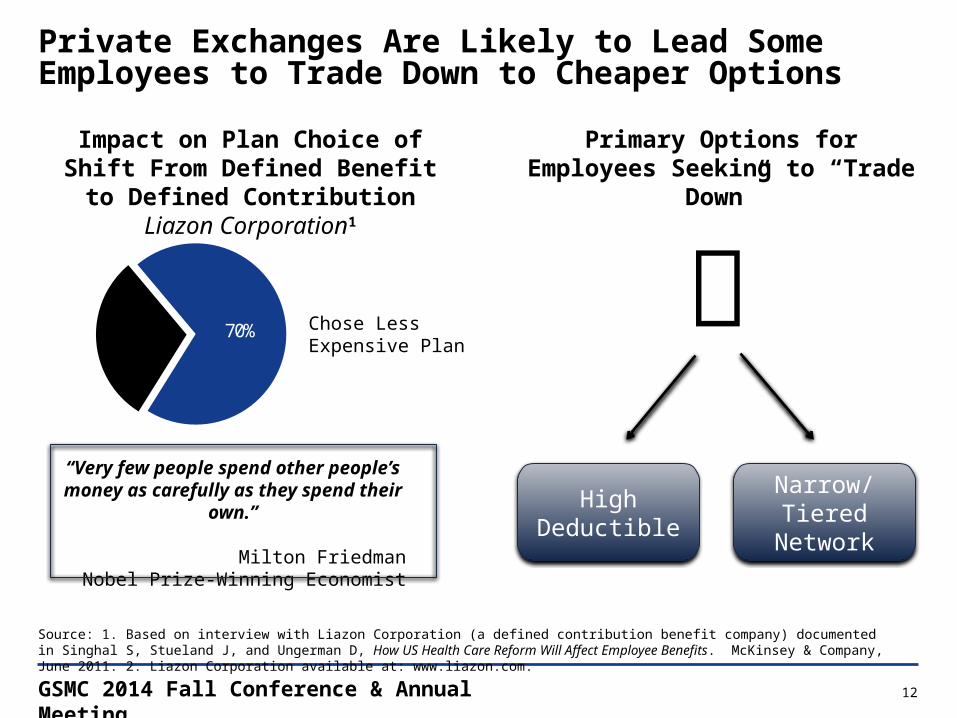
Private Exchanges Are Likely to Lead Some Employees to Trade Down to Cheaper Options
Source: 1. Based on interview with Liazon Corporation (a defined contribution benefit company) documented in Singhal S, Stueland J, and Ungerman D, How US Health Care Reform Will Affect Employee Benefits. McKinsey & Company, June 2011. 2. Liazon Corporation available at: www.liazon.com.
Chose Less Expensive Plan
Primary Options for Employees Seeking to “Trade Down”
High Deductible
Narrow/ Tiered Network
Impact on Plan Choice of Shift From Defined Benefit to Defined Contribution
Liazon Corporation1
70%
“Very few people spend other people’s money as carefully as they spend their own.”
Milton FriedmanNobel Prize-Winning Economist
GSMC 2014 Fall Conference & Annual Meeting 13
Sears and Darden Among the Major Employers to Pioneer the Private Exchange Concept
Source: 1. Enrollment Results Show Aon Hewitt’s Corporate Exchange Empowers Employees to Become More Astute Health Care Consumers. Aon Hewitt, March 18, 2013. www.aon.com. 2. Mathews A.W. Big Firms Overhaul Health Coverage. The Wall Street Journal, Sept 26, 2012. online.wsj.com.
Sears and Darden Private Exchange
• Sears and Darden chose a defined benefit/ private exchange healthcare benefit model for 2013
• More than 100,000 active employees of Sears, Darden, and other employers were given a company credit to purchase benefits via an exchange sponsored by Aon Hewitt
• Aon Hewitt decision support tools and benefits advisors facilitated employee plan decisions

GSMC 2014 Fall Conference & Annual Meeting 14
Many Participants Shifted to CDHPs in the First Year of the Sears and Darden Private Exchange
Sears and Darden found that choice of plans changed when employees were presented with expanded plan options and control over employer subsidy
Source: Mathews A.W. To Save, Workers Take on Health-Cost Risk. The Wall Street Journal, Mar 17 2013. online.wsj.com.
2012 2013
70%
47%
18%
14%
12%
39%
Consumer-Directed Health PlanHMOPPO
Distribution of Sears and Darden Employee Health Benefits by Type of Plan

GSMC 2014 Fall Conference & Annual Meeting 15
Transparency Tools Are a Key Catalyst for High Deductible Impact
• Growth in high deductible plans has prompted payers and employers to develop price transparency tools revealing cost and quality data to members
• Informed patients are likely to choose the “low-cost/high-quality” providers when faced with increased cost sharing
• Providers in competitive markets are at risk of revenue and market share erosion as payers and patients become aware of reimbursement variance
• Improving cost structure and competing on value is the only viable long-term option
Select Companies Offering Transparency Tools
GSMC 2014 Fall Conference & Annual Meeting 16
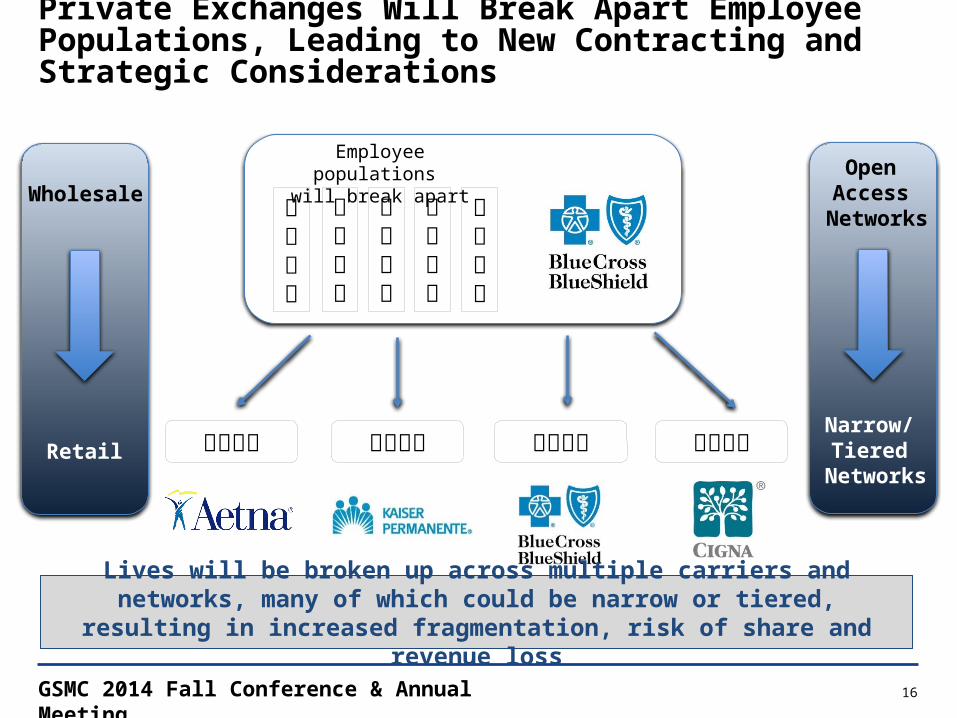
Private Exchanges Will Break Apart Employee Populations, Leading to New Contracting and Strategic Considerations
Employee populations will break apart
Lives will be broken up across multiple carriers and networks, many of which could be narrow or tiered, resulting in increased fragmentation, risk of share and revenue loss
Open Access
Networks
Narrow/ Tiered
Networks
Wholesale
Retail
GSMC 2014 Fall Conference & Annual Meeting 17
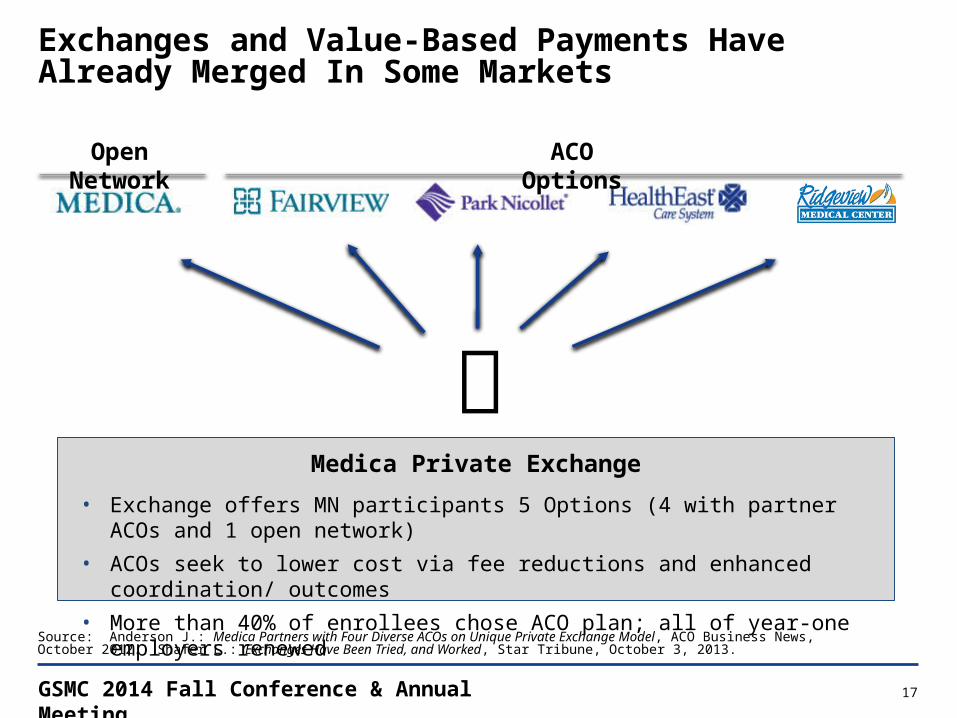
Exchanges and Value-Based Payments Have Already Merged In Some Markets
Medica Private Exchange
• Exchange offers MN participants 5 Options (4 with partner ACOs and 1 open network)• ACOs seek to lower cost via fee reductions and enhanced coordination/ outcomes• More than 40% of enrollees chose ACO plan; all of year-one employers renewed
Open Network ACO Options
Source: Anderson J.: Medica Partners with Four Diverse ACOs on Unique Private Exchange Model, ACO Business News, October 2012. Shafer L.: Exchanges Have Been Tried, and Worked, Star Tribune, October 3, 2013.

GSMC 2014 Fall Conference & Annual Meeting 18
Today’s Model Emerging Models
Implications
Expected to decline over time
Likely near-term model of choice
Expected to increase over time as narrow/tiered networks mature
Risk of Share Loss
Price Pressure
Bad Debt
Use Rate Pressure
Private Exchanges
Limited Threat Significant Threat
Open Access PPO High Deductible Narrow/Tiered
Private Exchanges Will Accelerate the Transition to Emerging Payment Models and Create New Strategic/ Financial Challenges

GSMC 2014 Fall Conference & Annual Meeting 19
Public Exchange Update

GSMC 2014 Fall Conference & Annual Meeting 20
Public Exchange Update and Analysis – National

GSMC 2014 Fall Conference & Annual Meeting 21
Public Exchange Enrollment Surpassed both Incremental and Cumulative Administration Targets for March
Notes: (1) HHS definition of enrollment (those who have “selected a plan”) (2) March data includes Special Enrollment Period through 19 April 2014 (3)Percentage of HHS enrollment target. Sources: ASPE, Health Insurance Marketplace Enrollment Reports, 13 Nov 2013, 11 Dec 2013, 13 Jan 2014, 12 Feb 2014, 11 Mar 2014, and 1 May 2014. Tavenner M, Projected Monthly Enrollment Targets for Health Insurance Marketplaces in 2014, 5 Sept 2013.
Public Exchange Enrollment
• National public exchange enrollment increased to 8.0M during the initial enrollment period
• Administration 2014 enrollment goal was 7.1M
% Target3 21% 65%30%
Cumulative U.S. Public Exchange Enrollment1
Thousands
Oct Nov Dec Jan Feb Mar106 364
2,153
3,300 4,242
8,020
75% 75% 113%
2

GSMC 2014 Fall Conference & Annual Meeting 22
The Vast Majority of Those Enrolled Nationally Chose Silver and Bronze Plans
Plan Choice Trends• 85% of those enrolled nationally
chose cheaper Bronze or Silver plans• Silver plans (eligible for cost-sharing
subsidies) are the most popular and account for 65% of all enrollment
National Plan Selection by Metal Level Initial Enrollment Period1
20%
65%9%
5%
2% Silver
Bronze
Gold
Platinum
Cat. (2%)2
Notes: (1) Includes additional special enrollment period activity through 19 April 2014. (2) Catastrophic plan. Source: ASPE, Health Insurance Marketplace Enrollment Report, 1 May 2014.

GSMC 2014 Fall Conference & Annual Meeting 23
Initial National Public Exchange Enrollment Skews Older Than Administration Targets
National6%
28%
17%
23%
25%
55 - 64
45 - 54
35 - 44
18 - 34
<18
National Exchange Age DistributionInitial Enrollment Period1
• Enrolling young and healthy people is critical to a stable risk pool• Age 18-34 enrollment lags the 39% administration target• How enrollment compares to health plan expectations will dictate plan profitability• The “3Rs” will mitigate premium changes in the near to medium term
Note: (1) Includes additional special enrollment period activity through 19 April 2014. Source: ASPE, Health Insurance Marketplace Enrollment Report, 1 May 2014.
Well below national HHS 18-34 target of 39%

GSMC 2014 Fall Conference & Annual Meeting 24
Despite Recent Improvements, the Previously Uninsured Represent Only About Half of the National Enrollment
Notes: McKinsey data from 11/25 to 1/10 survey, Feb 4 to Feb 13 survey, and April 7 to April 16 survey; Broker/consultant estimates from 1/17 WSJ article. Sources: Weaver C and Mathews A, Exchange See Little Progress on Uninsured, WSJ, 17 Jan, 2014; Demko P, 27% of 2014 Individual Market Enrollees Previously Lacked Coverage, Study Says, Modern Healthcare, March 2014: Hamel L, Rao M, Levitt L, Claxton G, Cox C, Pollitz K, Brodie M, Survey of Non-Group Health Insurance Enrollees, Kaiser Family Foundation, 19 June, 2014..
% of Public Exchange Enrollment by UninsuredNational Surveys
Nov 25 - Jan 10McKinsey
Feb 4 - Feb 13McKinsey
April 7 - April 16 McKinsey
June 19 Kaiser
11%
27% 26%
57%
• McKinsey surveys suggest that a majority of those enrolled nationally previously had individual or employer coverage
• Broker/ consultant data from mid-January found that 33% were previously uninsured• Kaiser Family Foundation Survey of small sampling suggests that 57% were previously uninsured
GSMC 2014 Fall Conference & Annual Meeting 25
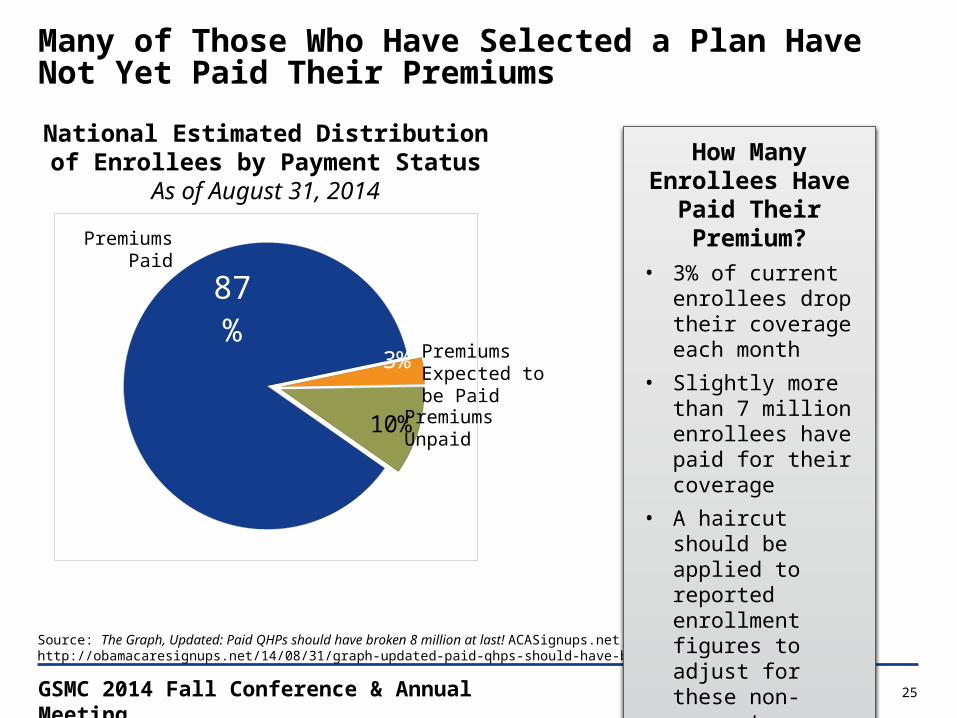
Many of Those Who Have Selected a Plan Have Not Yet Paid Their Premiums
Source: The Graph, Updated: Paid QHPs should have broken 8 million at last! ACASignups.net, August 31, 2014, http://obamacaresignups.net/14/08/31/graph-updated-paid-qhps-should-have-broken-8-million-last-92m-total
How Many Enrollees Have Paid Their
Premium?• 3% of current
enrollees drop their coverage each month
• Slightly more than 7 million enrollees have paid for their coverage
• A haircut should be applied to reported enrollment figures to adjust for these non-payments
National Estimated Distribution of Enrollees by Payment Status
As of August 31, 2014
87%
3%
10%PremiumsUnpaid
Premiums Paid
Premiums Expected to be Paid

GSMC 2014 Fall Conference & Annual Meeting 26
Public Exchange Update and Analysis – Georgia

GSMC 2014 Fall Conference & Annual Meeting 27
Georgia Is One of 28 Federally Facilitated Exchanges
Source: Kaiser Family Foundation, www.statehealthfacts.org. State Decisions For Creating Health Insurance Exchanges as of Oct. 2013.
177

GSMC 2014 Fall Conference & Annual Meeting 28
Public Exchange Enrollment in Georgia Surpassed Administration Targets
Notes: (1) HHS definition of enrollment (those who have “selected a plan”) (2) March data includes Special Enrollment Period through 19 April 2014 (3)Percentage of HHS enrollment target. Sources: ASPE, Health Insurance Marketplace Enrollment Reports, 13 Nov 2013, 11 Dec 2013, 13 Jan 2014, 12 Feb 2014, 11 Mar 2014, and 1 May 2014. Tavenner M, Projected Monthly Enrollment Targets for Health Insurance Marketplaces in 2014, 5 Sept 2013.
Public Exchange Enrollment
• GA public exchange enrollment increased to 316,543
• Full year HHS target was 204,000
• Enrollment in GA reached 155% of HHS initial enrollment target% Target3 10% 61%20%
Cumulative Georgia Enrollment1
Oct Nov Dec Jan Feb Mar1,390 6,859
58,611
101,276 139,371
316,543
80% 85% 155%
2
GSMC 2014 Fall Conference & Annual Meeting 29
CA TX NC GA IL WA OH TN IN AZ LA UT CT OK
MD KS NV AR NH MTMA RI DE AK DC HI
-
50,000
100,000
150,000
200,000
250,000
300,000
350,000
400,000
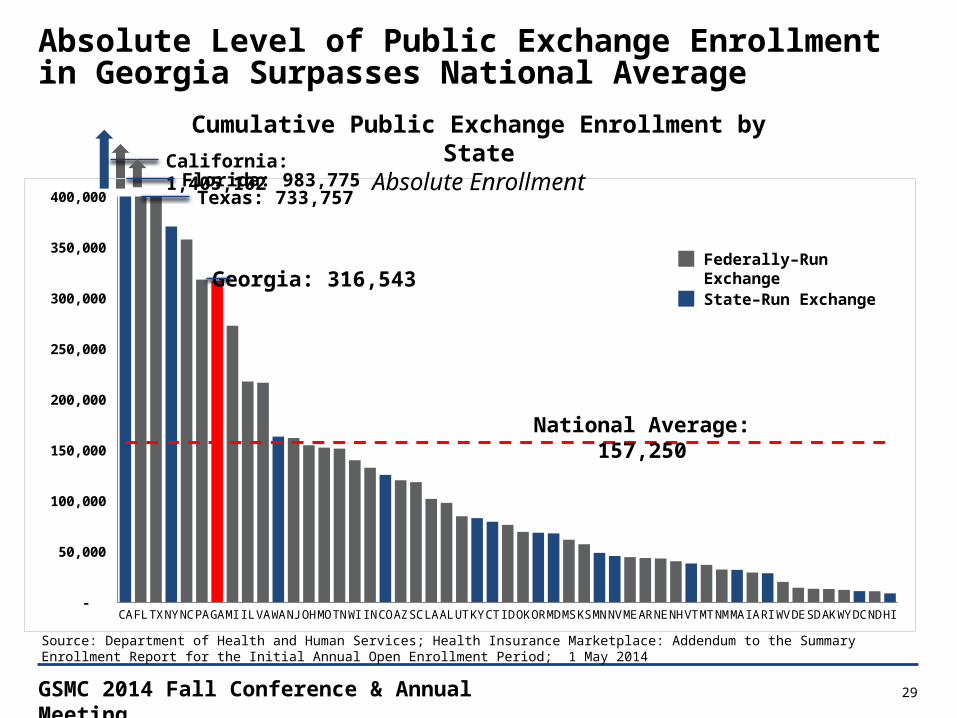
Cumulative Public Exchange Enrollment by StateAbsolute Enrollment
Florida: 983,775
Absolute Level of Public Exchange Enrollment in Georgia Surpasses National Average
Federally–Run Exchange
State–Run Exchange
Source: Department of Health and Human Services; Health Insurance Marketplace: Addendum to the Summary Enrollment Report for the Initial Annual Open Enrollment Period; 1 May 2014
Georgia: 316,543
National Average: 157,250
California: 1,405,102
Texas: 733,757

GSMC 2014 Fall Conference & Annual Meeting 30
CT NH ME NC DE NY NJ PA UTMO TN MT LA CA NE IN HI
AR OKMN SD AK
MDNM OR MA
0%
50%
100%
150%
200%
250%
Georgia Also Surpasses National Averages as a Percentage of HHS Targets
Federally–Run Exchange
State–Run ExchangeGeorgia: 155%
National Average: 113%
Cumulative Public Exchange Enrollment by State% of HHS Targets
Source: Department of Health and Human Services; Health Insurance Marketplace: Addendum to the Summary Enrollment Report for the Initial Annual Open Enrollment Period; 1 May 2014

GSMC 2014 Fall Conference & Annual Meeting 31
20%
65%9%
5%2%
Bronze and Silver Plans Make Up 82% of Public Exchange Enrollment in Georgia
• Plan selection in Georgia skews toward low cost Silver and Bronze plans but slightly less so than the national average
Georgia
11%71%
7%
10%2%
Gold
Cat. (2%) 2 Silver
Bronze
Gold
Platinum
Cat. (2%)
Note: (1) Includes additional special enrollment period activity through 19 April 2014. (2) Catastrophic plan Source: ASPE, Health Insurance Marketplace Enrollment Report, 1 May 2014.
Plan Selection by Metal Level Initial Annual Open Enrollment Period1
National
Silver
Bronze
Platinum

GSMC 2014 Fall Conference & Annual Meeting 32
Age Distribution of Georgia and National Enrollment Are Similar
Georgia National5% 6%
32% 28%
20%17%
23%23%
21%25%
55 – 64
45 – 54
35 – 44
18 – 34
<18
• Georgia has a slightly lower percentage of enrollees between the ages of 55 and 64 than the national average
• 32% of Georgia enrollees are in the pivotal 18–34 cohort, which is slightly higher than the national average (28%) and well below the administration target (39%)
Note: (1) Includes additional special enrollment period activity through 19 April 2014. Source: ASPE, Health Insurance Marketplace Enrollment Report, 1 May 2014.
Exchange Age DistributionInitial Enrollment Period1

GSMC 2014 Fall Conference & Annual Meeting 33
Georgia Bronze Premiums Are Slightly Higher than the National Average
WY AK MS CT VT NJ ME DE IN SD WI NH NC ND WV CA NY AR SC GA LA RI WA OH FL MTAvg. AL MO NE VA CO PA ID NV MI NM AZ IA TX OR DC IL UT KS MD TN OK MN$0
$50
$100
$150
$200
$250
$300
$350
$400
$450
$265
Monthly Premium of Lowest Cost Individual Bronze Plan in State1
National Avg: $249
Note: 1) Age weighting for all states is based on expected age distribution in the Marketplaces, estimated by the RAND Corporation.Source: APSE Issue Brief, Health Insurance Marketplace Premiums for 2014, Health and Human Services, avail able at: aspe.hhs.gov (accessed Oct 1, 2013).
$144
$425

GSMC 2014 Fall Conference & Annual Meeting 34
Georgia’s Five Individual Market Plans Puts the State Toward the Middle of the Pack
Source: Avalere Health, Analysis on Health Plan Offerings on the Federally-Facilitated Marketplace, 3 Oct 2013.
Insurer Competition by StateIndividual Market

GSMC 2014 Fall Conference & Annual Meeting 35
Georgia Health Insurance Exchange Participants – Blue Cross Blue Shield of Georgia Plans are Available State Wide
Georgia Public Individual Exchange Participants
Georgia Public SHOP Exchange Participants
Source: Miller, A.: UnitedHealthcare to be fourth company to offer insurance in State Exchange next year, The Augusta Chronicle, July 14, 2014

GSMC 2014 Fall Conference & Annual Meeting 36
Drivers That Could Impact Commercial Shift and Employer “Dumping” to Public Exchanges
Driver Influence Factors Shift Impact
Firm Size Small firms are more likely to choose SHOP exchanges or dump to HIX
↑Subsidy/ Tax Credits Subsidy and tax credit availability will stimulate exchange uptake
Delivery Cost Favorable insurer network contracts will increase plan participation and pressure on employers to shift
Wages/ Part-Time Workforce/ Retirees
Low-wage geographies will have greater subsidy availability; part-time employees and pre-65 retirees more apt to shift
Exchange Implementation and Promotion
Good communication, promotion, and receptivity will stimulate enrollment ↔
Timing Uptake could initially be slow but increase over time once the market settles out, particularly if the “me too” effect takes hold
Recruitment and Retention
Higher skilled/ wage employers who prioritize recruitment and retention may not be willing to shift to public exchanges
↓Exchange Plan Options and Premiums Fewer plan options and higher premiums will delay uptake
Penalties Employer responsibility penalties a key deterrent for larger employers; fear among some that penalties could be increased in the future
GSMC 2014 Fall Conference & Annual Meeting 37
Public Exchange Analysis Summary Observations• Georgia is one of 28 Federally-Facilitated Exchanges• Georgia enrollment of 316,543 far exceeded the HHS projection of
204,000• Of the 50 States, Georgia was ranked 7th in enrollment• Georgia was one of 24 States that exceeded the HHS enrollment goals• Leaner and less expensive silver (71%) and bronze (11%) plans are
currently the most popular in Georgia which could result in collection challenges for providers
• 32% of Georgia enrollees are in the pivotal 18–34 cohort, which is slightly higher than the national average (28%) and well below the administration target (39%)
• Average Bronze Premiums were slightly higher than the National Average
• There was a decent selection of plans available in GeorgiaSource: Medicaid & CHIP: April 2014 Monthly Applications, Eligibility Determinations and Enrollment Report, June 4, 2014
GSMC 2014 Fall Conference & Annual Meeting 38
Narrow Network Considerations

GSMC 2014 Fall Conference & Annual Meeting 39
0%
20%
40%
60%
80%
100%
120%
72%
2014 Limited Network Percentage of Plan Offerings By StateFederal Exchange States
Note: Limited network defined as EPO and HMO plans. Survey results exclude the 49% of respondents who indicated that they “did not know” their exchange contract network plan design.Source: Health Insurance Marketplace Premiums for 2014 Databook (Information Current as of Sept 18, 2013); MHA member survey.
Limited Network Penetration
• Network adequacy regulations, hospital competition, spare capacity will influence prevalence
• 72% of plans offered on Georgia’s exchange were narrow network plans
Limited Networks Will Have a Significant Presence on the Georgia Public Exchange

GSMC 2014 Fall Conference & Annual Meeting 40
Commercial Market Share by Service Area
PSA SSA PSA + SSA0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
100%
52%
29%46%
23%
6%
18%
25%
65%
36%
Other CompetitorsCompetitor 1Client
Mar
ket S
hare
Tot. Discharges
Tot. Discharges
Tot. Discharges
Conceptual Illustration
GSMC 2014 Fall Conference & Annual Meeting 41
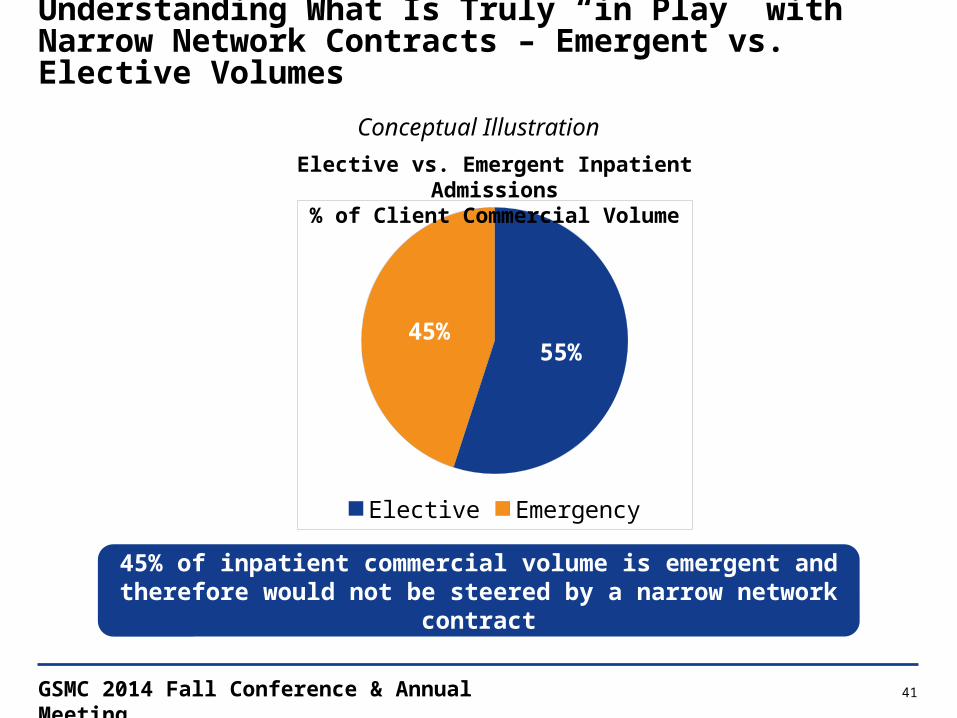
Understanding What Is Truly “in Play” with Narrow Network Contracts – Emergent vs. Elective Volumes
45% of inpatient commercial volume is emergent and therefore would not be steered by a narrow network contract
55%45%
Elective Emergency
Elective vs. Emergent Inpatient Admissions% of Client Commercial Volume
Conceptual Illustration
GSMC 2014 Fall Conference & Annual Meeting 42
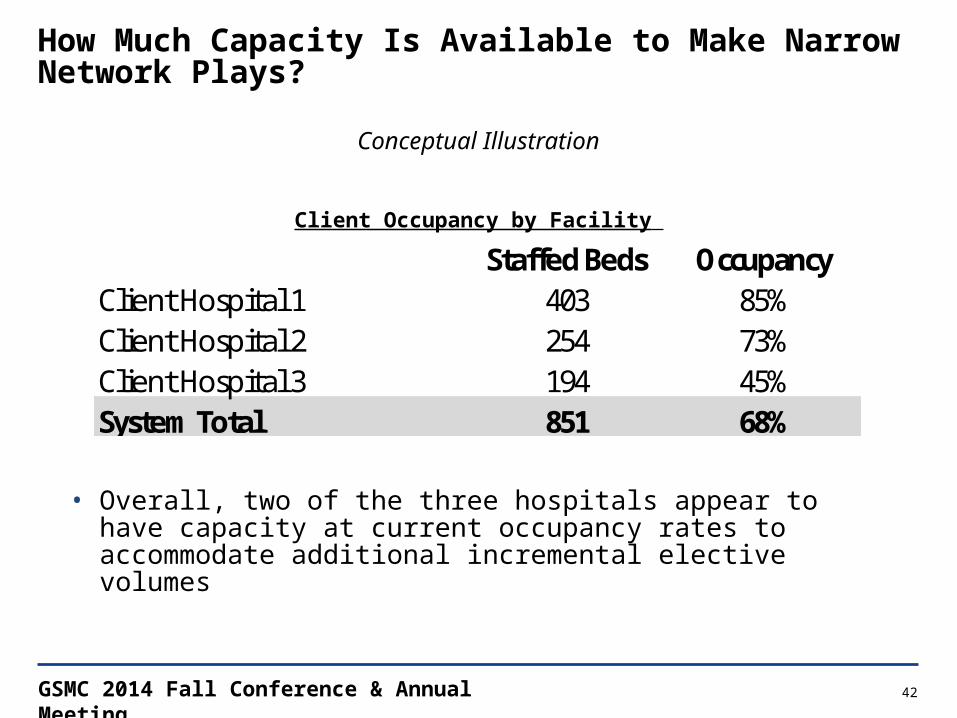
How Much Capacity Is Available to Make Narrow Network Plays?
Client Occupancy by Facility
Staffed Beds OccupancyClient Hospital 1 403 85%Client Hospital 2 254 73%Client Hospital 3 194 45%System Total 851 68%
• Overall, two of the three hospitals appear to have capacity at current occupancy rates to accommodate additional incremental elective volumes
Conceptual Illustration

GSMC 2014 Fall Conference & Annual Meeting 43
Key Considerations for Narrow Network ParticipationKey Consideration Steps:
1. Evaluate market share of local competitors to quantify if additional share can be gained • How much volume is potentially at risk if you do not participate?
2. Based on available market share, evaluate elective vs. emergent split – how much elective volume can you expect to gain?
3. Does the organization have the capacity to handle the additional volume?
4. What discounts will be required to participate in narrow networks and are individuals likely to choose narrow networks?
In pursuing a narrow network contract, is it worth discounting rates to obtain additional volume, and if so, by how much?
GSMC 2014 Fall Conference & Annual Meeting 44
Summary Implications

GSMC 2014 Fall Conference & Annual Meeting 45
What is the optimal way to balance these threats and opportunities?
Balancing New Revenue Opportunities and Cannibalizing the Existing Commercial Business
Uninsured Exchange
Commercial
Exchange
New Rev. Lost Rev.

GSMC 2014 Fall Conference & Annual Meeting 46
Summary Implications• Exchanges will catalyze the shift of purchasing healthcare benefits from
the wholesale to the retail channel• This channel shift will change the behavioral economics of plan
purchasing decisions and increase the prevalence of high deductible and narrow network plans
• Value-based reimbursement will increase over the long-term as pricing and cost pressures grow, which will require improved cross-continuum care coordination
• Competing on value and improving cost structure are the only viable long-term options for continued growth
GSMC 2014 Fall Conference & Annual Meeting 47
How Do You Prepare for the Increasing Shift to Public and Private Exchanges?Kaufman Hall believes that operational and financial success with healthcare exchanges requires an integrated planning framework
• Strategic Planning: A Health Insurance Exchange Strategy will be necessary to compete in the changing market environment. New reimbursement and contract models, in addition to FFS, will be used for exchange-based products, most likely requiring providers to assess and acquire new strategies and tactics
• Financial Planning: Many health systems and providers are in the early stages or have not yet begun to plan for how health insurance exchanges will impact their current and future patient populations and revenue base. A thorough analysis and plan to quantify the implications and potential financial impact should be completed
• Tactical Planning: New skills and capabilities will certainly be required for financial and operational success when working with health insurance exchanges. Developing the right tactical plan, resources, and investments while taking into consideration specific opportunities, priorities, risks, and benefits will be necessary
Exchanges are expanding; make sure your organization is prepared

GSMC 2014 Fall Conference & Annual Meeting 48
Discussion/ Questions
GSMC 2014 Fall Conference & Annual Meeting 49
COMPREHENSIVE SOFTWARE SUITE
Over 1,400 software licenses are in place
nationwide. The ENUFF Software Suite uses
corporate finance principles to directly support the
financial management cycle
CAPITAL ALLOCATIONKaufman Hall helps
organizations design and implement capital allocation
processes which provide consistent and rigorous
methodologies to guide the capital decision-making
process
MERGERS, ACQUISITIONS, AND DIVESTITURES
Kaufman Hall has advised on hundreds of M&A-related
engagements including analyzing, structuring,
negotiating and executing mergers, acquisitions,
divestitures, joint ventures, strategic partnerships and
affiliations
FINANCIAL AND CAPITAL PLANNING
Introduced concept of strategic financial planning to
healthcare field in 1983. Kaufman Hall has prepared
financial and capital plans for over 800 hospitals and
healthcare systems
STRATEGIC SERVICES
Kaufman Hall provides a broad range of strategy-
related services to support organizational management
and decision making. Kaufman Hall pioneered the
development of the integrated strategic financial
plan
CAPITAL MARKETS
Since 1985, Kaufman Hall has acted as financial advisor to more than 1050 healthcare debt transactions. Total debt and swaps issued on behalf of our clients exceeds $105
billion and $50 billion, respectively
Kaufman Hall Services at a Glance

GSMC 2014 Fall Conference & Annual Meeting 50
Kalani Redmayne, Assistant Vice PresidentKalani Redmayne is an Assistant Vice President at Kaufman Hall and a member of the firm’s Strategy practice. In this role, she provides strategic planning advisory services for a wide range of clients, including healthcare systems, academic medical centers, and community hospitals. Ms. Redmayne’s responsibilities focus on payer-provider strategies, alternative reimbursement methodologies, health plan and service operations, healthcare reform, payer relations and product development.
Ms. Redmayne has more than 20 years of experience in the healthcare industry. Prior to joining Kaufman Hall, Ms. Redmayne was Vice President of Product Development and Management for UnitedHealthcare, Inc., where she focused on Medicare Advantage, Medicare Supplement, Prescription Drug Plans and UnitedHealthcare’s private exchange products. During her 15 year tenure with UnitedHealthcare, Inc, Ms. Redmayne held other senior positions in Sales Operations, Sales and Marketing, and Marketing Operations. Before UnitedHealthcare, she spent five years as a sales executive with Downey Community Hospital/HealthFirst Medical Group.
Contact Ms. Redmayne at 310.227.8988 or [email protected]

GSMC 2014 Fall Conference & Annual Meeting 51
Qualifi cati ons, Assumpti ons and Limiti ng Conditi ons (v.12.08.06):This Report is not intended for general circulati on or publicati on, nor is it to be used, reproduced, quoted or distributed for any purpose other than those that may be set forth herein without the prior writt en consent of Kaufman, Hall & Associates, Inc. (“Kaufman Hall”).All informati on, analysis and conclusions contained in this Report are provided “as-is/where-is” and “with all faults and defects”. Informati on furnished by others, upon which all or porti ons of this report are based, is believed to reliable but has not been verifi ed by Kaufman Hall. No warranty is given as to the accuracy of such informati on. Public informati on and industry and stati sti cal data, including without limitati on, data are from sources Kaufman Hall deems to be reliable; however, neither Kaufman Hall nor any third party sourced make any representati on or warranty to you, whether express or implied, or arising by trade usage, course of dealing, or otherwise. This disclaimer includes, without limitati on, any implied warranti es of merchantability or fi tness for a parti cular purpose (whether in respect of the data or the accuracy, ti meliness or completeness of any informati on or conclusions contained in or obtained from, through, or in connecti on with this report), any warranti es of non-infringement or any implied indemniti es.The fi ndings contained in this report may contain predicti ons based on current data and historical trends. Any such predicti ons are subject to inherent risks and uncertainti es. In parti cular, actual results could be impacted by future events which cannot be predicted or controlled, including, without limitati on, changes in business strategies, the development of future products and services, changes in market and industry conditi ons, the outcome of conti ngencies, changes in management, changes in law or regulati ons. Kaufman Hall accepts no responsibility for actual results or future events.The opinions expressed in this report are valid only for the purpose stated herein and as of the date of this report.All decisions in connecti on with the implementati on or use of advice or recommendati ons contained in this report are the sole responsibility of the client.In no event will Kaufman Hall or any third party sourced by Kaufman Hall be liable to you for damages of any type arising out of the delivery or use of this Report or any of the data contained herein, whether known or unknown, foreseeable or unforeseeable.
5202 Old Orchard Road, Suite N700, Skokie, Illinois 60077847.441.8780 phone | 847.965.3511 fax
www.kaufmanhall.com
© 2014 Kaufman, Hall & Associates, Inc. All rights reserved.