1) for intravesicle therapy: a) mitomycin c instillation dose is 40mg for 2 hour b) oncotice bcg...
TRANSCRIPT
1) For intravesicle therapy:
A) Mitomycin C instillation dose is 40mg for 2 hour
B) Oncotice BCG instillation dose is 81mg for 2hours
C) ImmuCyst BCG instillation dose is 12.5mg for 1 hours
D) ImmuCyst BCG instillation dose is 81mg for 2hours
E) Oncotice BCG instillation dose is 12.5mg for 1 hour
MCQ

2) BCG treatment:A) Lamm’s protocol use 28 doses BCG over a period of 3 years
B) SWOG trial protocol uses maintenance BCG for 1 year only
C) BCG maintenance drop out rate is as high as 84% according to SWOG trial
D) There is good evidence to suggest that Immuncyst BCG is more effective than Oncotice BCG
E )In superficial bladder cancer BCG reduces progression but not recurrence, whereas mitomycin C reduces recurrence but not progression

3) BCG toxicity :
A) EORTC and CUETO suggest reduced dose BCG reduces the incidence of severe systemic toxicity compared to standard dose BCG
B) BCG can be administered in patients with macroscopic haematuria
C) Patient with microscopic haematuria is a contraindication for BCG instillation
D) Presence of leukocyte or asymptomatic bacteriuria is not a contraindication for BCG application
E) Patient with symptomatic UTI can have BCG provided prophylactic antibiotic is given
4) Long term (e.g. 15 years) outcome after BCG for patient with high risk non-muscle invasive bladder cancer. Which of the following is the best answer?
A) ~50% progression rate B) ~27% alive with intact bladder C) 1/3 die of cancer progression D) 1/3 develop recurrence in upper tract / prostate E) All of the above

1) For intravesicle therapy:
A) Mitomycin C instillation dose is 40mg for 2 hour -F
B) Oncotice BCG instillation dose is 81mg for 2hours -F
C) ImmuCyst BCG instillation dose is 12.5mg for 1 hours-F
D) ImmuCyst BCG instillation dose is 81mg for 2hours-T
E) Oncotice BCG instillation dose is 12.5mg for 1 hour-F

2) BCG treatment:A) Lamm’s protocol use 28 doses BCG over a period of 3 years-F (27 doses over
3 yrs)
B) SWOG trial protocol uses maintenance BCG for 1 year only-F (used Lamm’s)
C) BCG maintenance drop out rate is as high as 84% according to SWOG trial-T
D) There is good evidence to suggest that Immuncyst BCG is more effective-F than Oncotice BCG
E )In superficial bladder cancer BCG reduces progression but not recurrence, whereas mitomycin C reduces recurrence but not progression -F

3) BCG toxicity :
A) EORTC and CUETO suggest reduced dose BCG reduces the incidence of severe systemic toxicity compared to standard dose BCG –F (CUETO- fewer patients have toxicity but incident of severe systemic toxicity was similar. EORTC- no difference in toxicity)
B) BCG can be administered in patients with macroscopic haematuria -F
C) Patient with microscopic haematuria is a contraindication for BCG-F instillation
D) Presence of leukocyte or asymptomatic bacteriuria is not a contraindication for BCG application -T
E) Patient with symptomatic UTI can have BCG provided prophylactic antibiotic is given -F

4) Long term (e.g. 15 years) outcome after BCG for patient with high risk non-muscle invasive bladder cancer. Which of the following is the best answer?
A) ~50% progression rate B) ~27% alive with intact bladder C) 1/3 die of cancer progression D) 1/3 develop recurrence in upper tract / prostate E) All of the above –Best answer (MSKCC –cookson J
urol 1997)

Viva Question-EAU guideline 2013 –
intravesical therapy

Viva Question-EAU guideline 2013

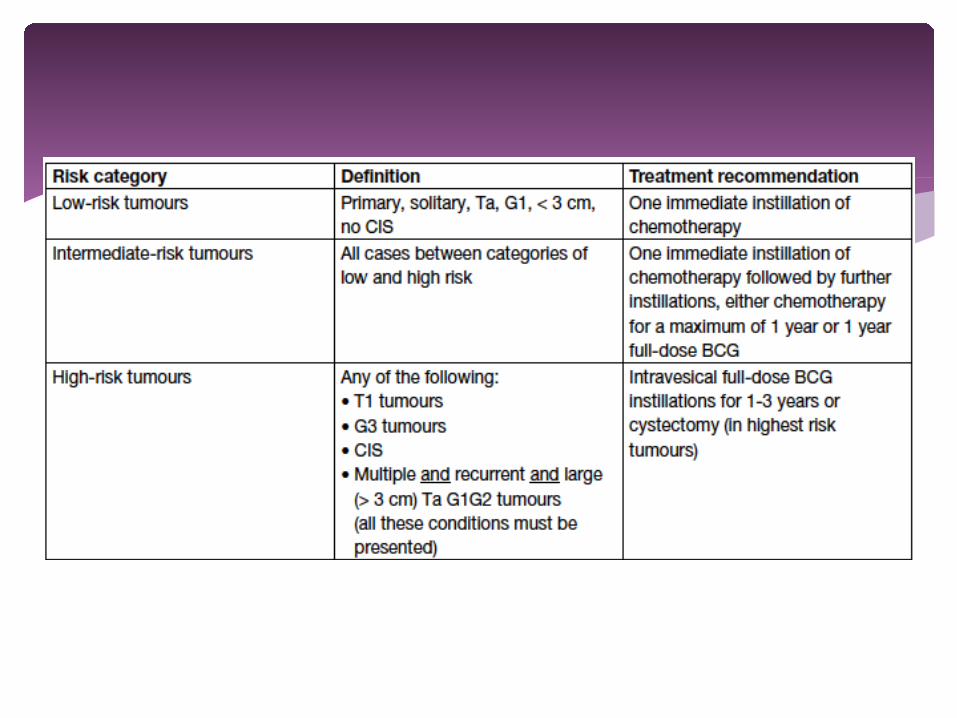
Low risk: Single dose, immediate post op intravesicle instillation of
chemotherapy, no difference between agents (standard treatment)
Absolute recurrence reduction 11.7% (RR 39%) Sylvester 2004 Meta-analysis
To maximised efficacy immediate instillation is recommended – all single instillation studies administered within 24 hrs
Finnbladder group (Kassinen 2002)- suggested by delaying instillation overnight the risk of recurrence is increased by two fold

MITOMYCIN Mechanism of acion - Antitumour antibiotic – DNA
alkylating agent, causes cross links to complementary DNA strands – inhibits DNA synthesis
Dose - 40mg in 40ml sterile water Side effects – skin rash, storage LUTS, bladder
calcifications, myelosupression Evidence – meta-analysis of 7 RCTs, 1476 pts, 36.7% of
pts with one post op dose MMC had recurrence compared to 48.4% treated with TURBT alone (decrease of 39% in odds of recurrence) (Sylvester J Urol 2004).
Mitomycin

Contraindications Bladder perforation Bleeding requires irrigation Previous allergy

Intermediate Risk One immediate installation of chemotherapy Further intravesicle therapy
BCG or chemotherapy (Optimum schedule not defined)
For no more than 1 year Choice between BCG and mitomycin C for 1
year Mitomycin – only prevent recurrence not
progression BCG- more efficacious than Mitomycin for
recurrence, reduce progression BUT more toxic

High risk BCG reduce recurrence and superior to MMC
(meta-analysis Shelley BJUI 2004; Bohle J Urol 2003)
BCG reduce progression (meta-analysis Sylvester J urol 2002- 4% absolute risk
reduction for progression; 27% RR reduction)
BCG maintenance is required to achieve effect(Bohle urology 2004, J urol 2003 at least 1 year of maintenance BCG is required to obtain superiority of BCG over MMC for prevention of recurrence or progression)

Microwave-induced hyperthermia Electromotive drug administration (EMDA)
Considered as experimental treatment, as studies are small and evidence is limited
Methods to improve efficacy of intravesicle chemo

What type/ dose of BCG do you use, what advice do you give and how do
you treat complications
Two BCG preparations licensed in the UK ImmuCyst (Cambridge)
BCG Connaught 81mg dose (contains 0.4-3.7x107 CFU/ml BCG Connaught)
OncoTICE (Organon) BCG-TICE 12.5mg (contains 0.4-1.6x107 CFU/ml BCG TICE)
Mechanism – poorly understood, probably immune response leads to cytokine production
What type/ dose of BCG do you use, what advice do you give and how do you treat complications

Both reconstituted with 50mls saline to make a 53ml volume preparation
Catheter then inserted Ideally full bladder on catheterisation to wash out any lubricant Instill BCG slowly via gravity Pt should retain the fluid for as long as possible up to 2 hours For first 15min, should lie prone, then allowed to get up After 2hrs Patient can void in a seated position Care should be taken with voiding for the next 4 hours Void whilst sitting Bleach toilet and leave for 15min Condoms should be used within a week of treatment

BCG – absolute contraindications: During first 2 weeks after TUR Macroscopic Haematuria After traumatic catheterisation In patient with symptomatic UTI
* WCC or asymptomatic bacteriuria or microscopic haematuria are not contraindication. Prophylactic antibiotic is not required
* BCG should be used with caution in immunocompromised patients

1st year X6 (induction) X3 (at 3/12) X3 (at 6/12) X3 (at 12/12)
2nd year X3 (at 18/12) X3 (at 24/12)
3rd year X3 (at 30/12) X3 (at 36/12)
Total= 27 doses
Lamm’s Protocol used in SWOG &EORTC
BCG complications
Local Cystitis Haematuria Prostatitis Orchitis
Treatment Analgesia +/-Postpone BCG Culture Antibiotic Restart BCG
Systemic BCG sepsis
Treatments If a systemic BCG infection occurs,
an Infectious Diseases consultation should be sought.
BCG should be permanently discontinued
Mulitiple agents anti-tuberculosis therapy should be initiated promptly. Commonly, this will comprise
Isoniazid, Rifampicin, Ethambutol Pyrazinamide

Non specific Symptoms (Malaise, fever, Rash, arthralgia/ arthritis) Anti-histamines or NSAIDs
BCG complications


1/3 dose and full dose BCG- no difference in toxicity
Intermediate-risk patient if BCG is used- should be treated with full dose for 1 year
High-risk patient should have full dose 3 years BCG to reduce recurrence compared with full dose 1 year BCG. However, there is no benefit in terms of progressions or deaths using 3 years or 1 year protocol.
Final EORTC-GU cancers Group randomized study -European Urology 2013

When do you consider radical treatment in superficial
bladder cancer
Highest risk: G3T1 with concurrent Bladder CIS Multiple and /or large (>3cm) G3T1 recurrent G3T1 G3T1 with CIS in prostatic urethra Micropapillary variant of urothelial ca
High risk disease unable to tolerate BCG consider immediate cystectomy because:
TURBT staging accuracy: For T1 disease 27-51% of patients being upstaged to muscle invasive disease at cystectomy
5 years risk of Disease Progression can be as high as 45% Retrospective study shows high risk non muscle invasive disease
undergo early cystectomy has a high survival rate
When do you consider radical treatment in superficial bladder cancer

Fail BCG BCG refractory tumour
1. If high grade, non muscle invasive tumour present at 3 months
2. If CIS is present at both 3 and 6 months3. If high grade tumour appears during BCG therapy
BCG recurrence1. Recurrence of high grade (G3) tumour after
completion of maintenance BCG, despite initial response
Others

Intravesicle Interferon α and BCG Intravesicle Gemcitabine Thermochemotherapy Electromotive drug therapy (EMDA) Intravesicle Taxane chemo agent Intravesicle Mitomycin C and gemcitabine Photodynamic therapy Sequential therapy- Sequential BCG and EMDA MMC
(Small studies with some promising results but insufficient to formulate definitive recommendation)
(D Yates European Urology 2012)
Alternatives to cystectomy after BCG failure