wound care medicine - inosteo.org annual... · acute versus chronic wounds ......
TRANSCRIPT
Wound Care MedicineGaston Dana D.O.
Financial Disclosures
• Siemens Healthcare
• Toshiba Medical Systems Inc.
• Philips Healthcare
• Carestream Health
• GE Healthcare
• Shimadzu Corporation
• Global Health Corporation
• Microsoft
• Apple
• Intel
• Verizon
• Ultra-Solution
• Healthcare Navigation Inc.
• Puppy Chow
• Cat’s Meow
Financial Disclosures
None!
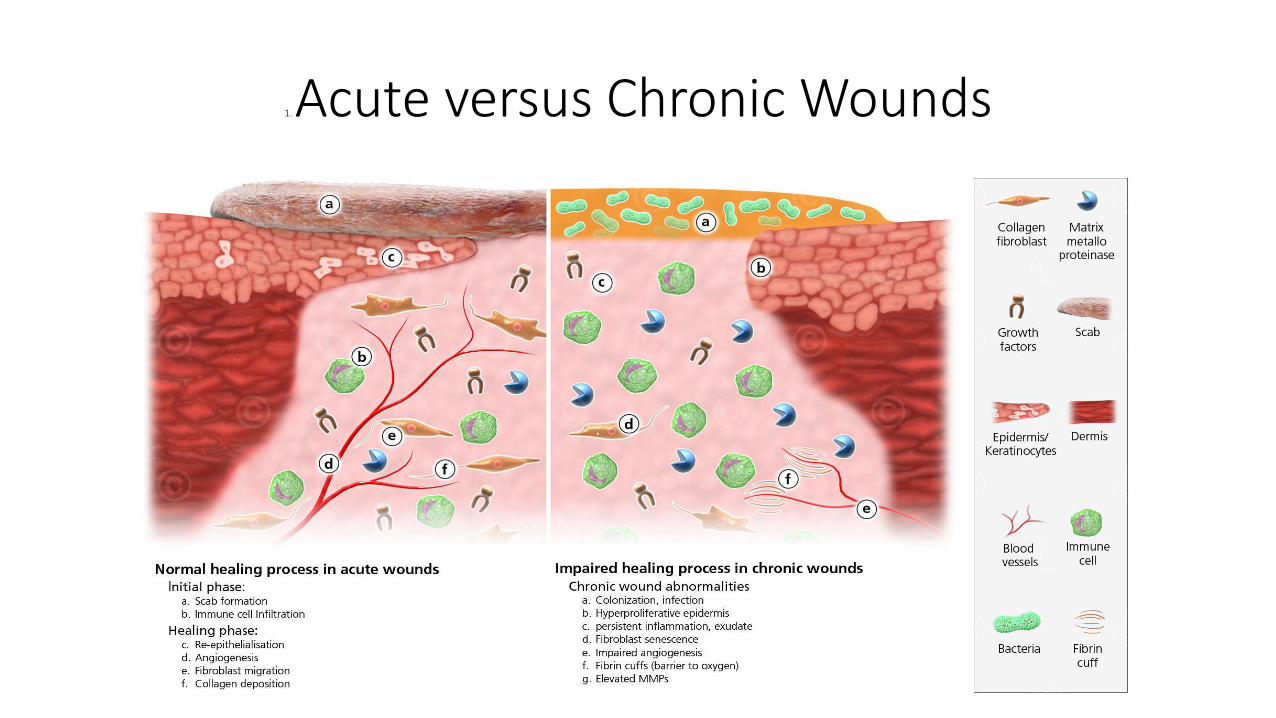
1. Acute versus Chronic Wounds
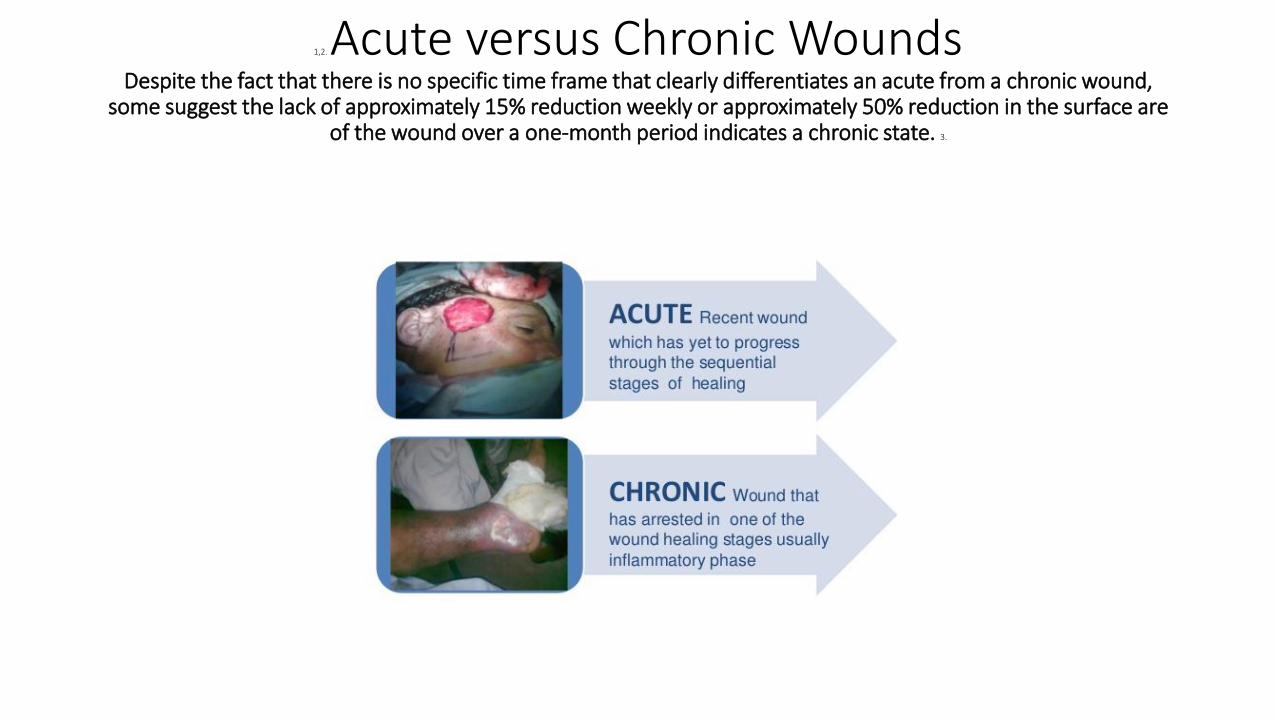
1,2. Acute versus Chronic WoundsDespite the fact that there is no specific time frame that clearly differentiates an acute from a chronic wound,
some suggest the lack of approximately 15% reduction weekly or approximately 50% reduction in the surface are of the wound over a one-month period indicates a chronic state. 3.
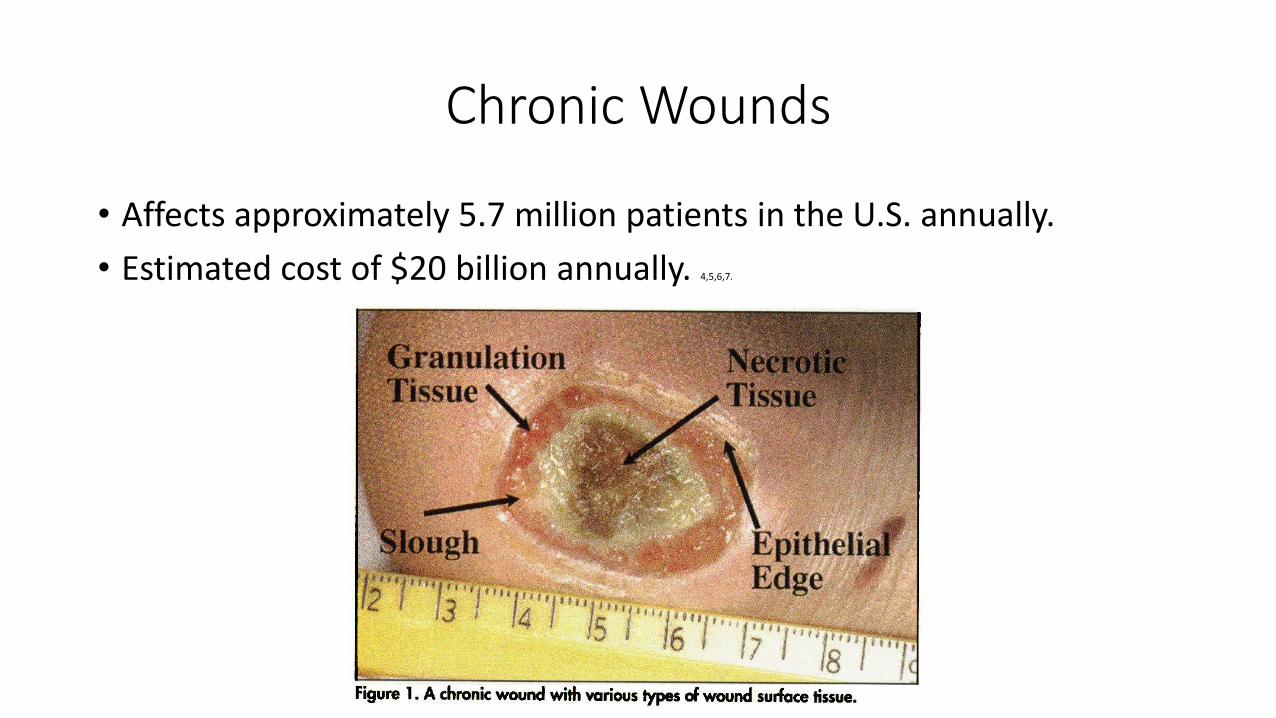
Chronic Wounds
• Affects approximately 5.7 million patients in the U.S. annually.
• Estimated cost of $20 billion annually. 4,5,6,7.
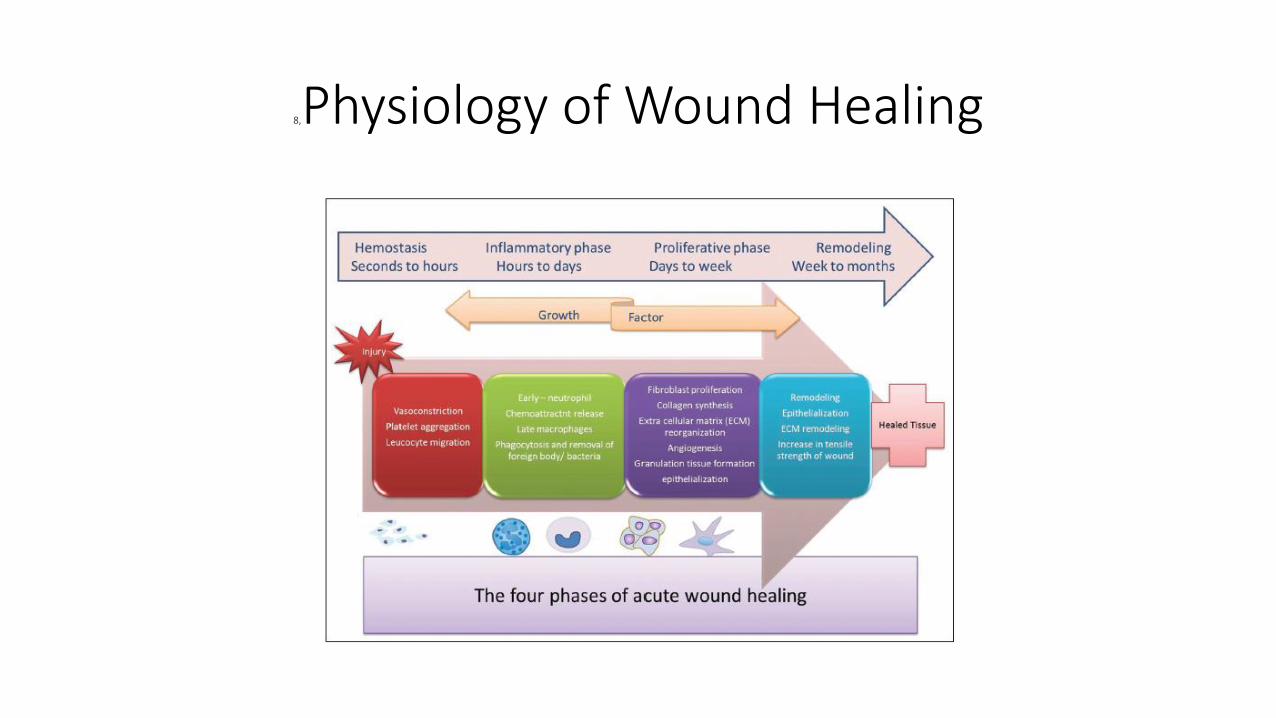
8,Physiology of Wound Healing
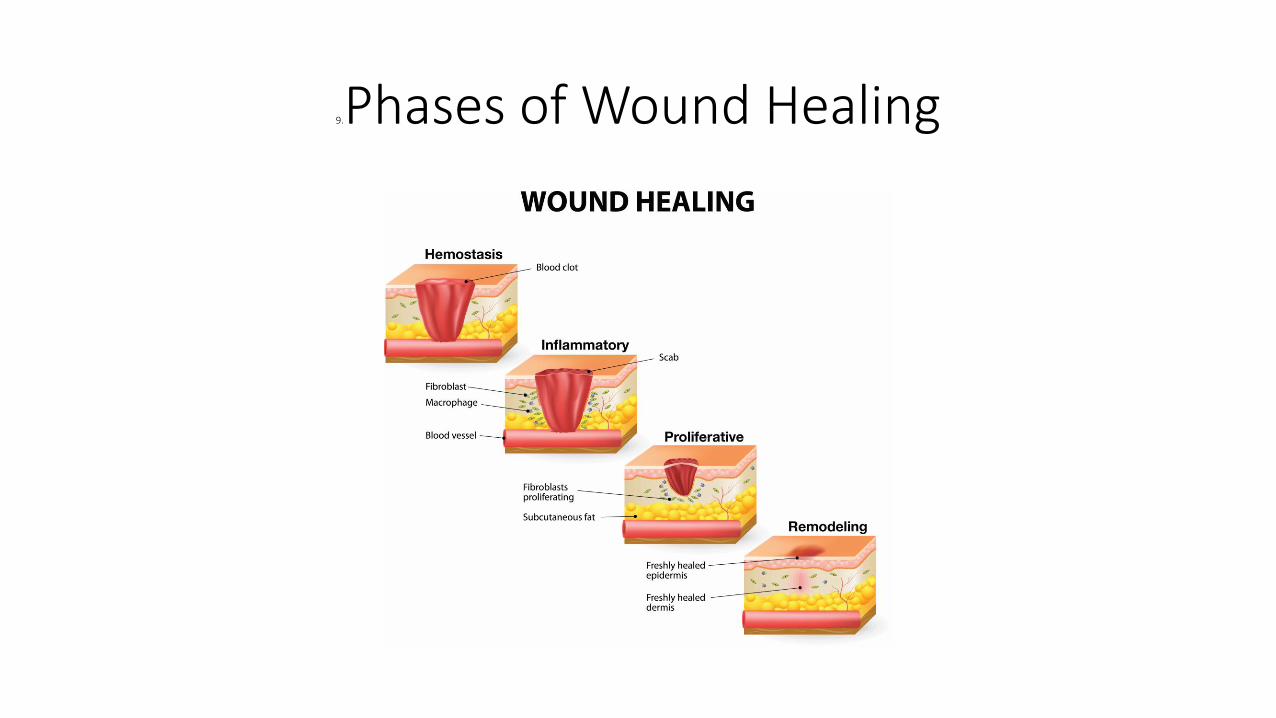
9.Phases of Wound Healing
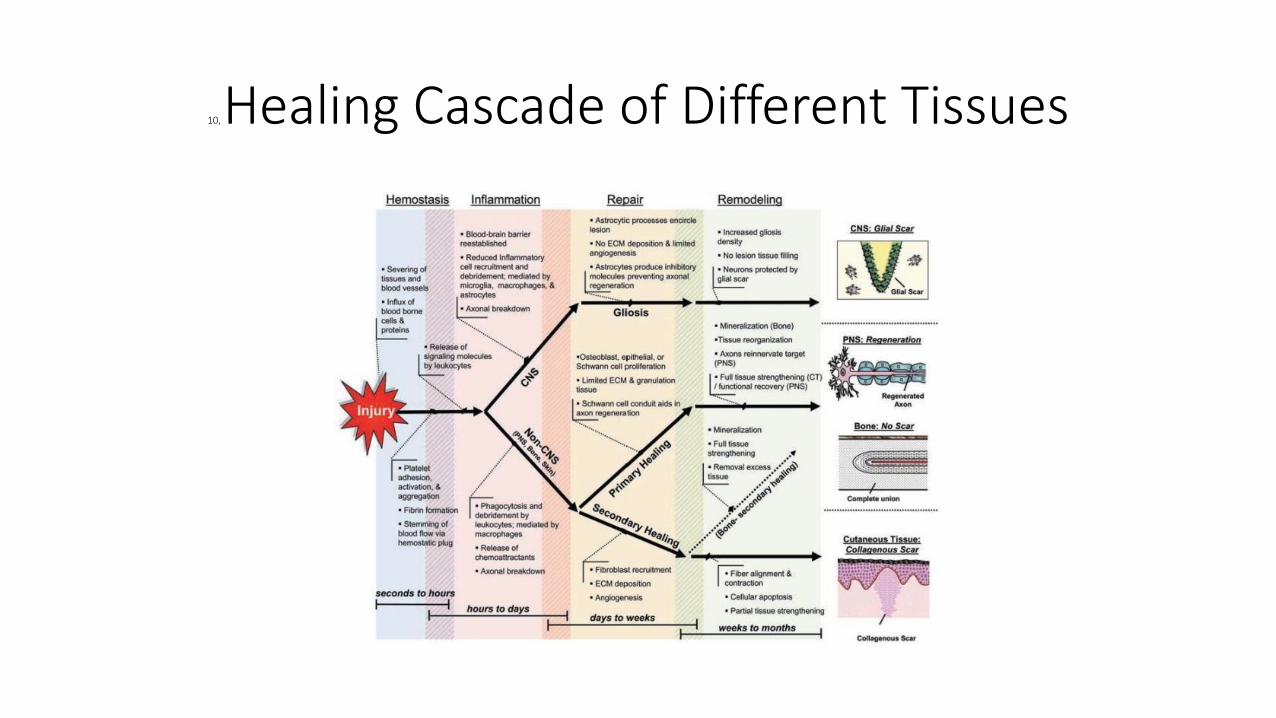
10, Healing Cascade of Different Tissues
Common Problems in Wound Healing
• Infection
• Cellular hypoxia
• Systemic disease
• Malnutrition
• Chronic venous insufficiency
• Malignancy
• Inadequate offloading.
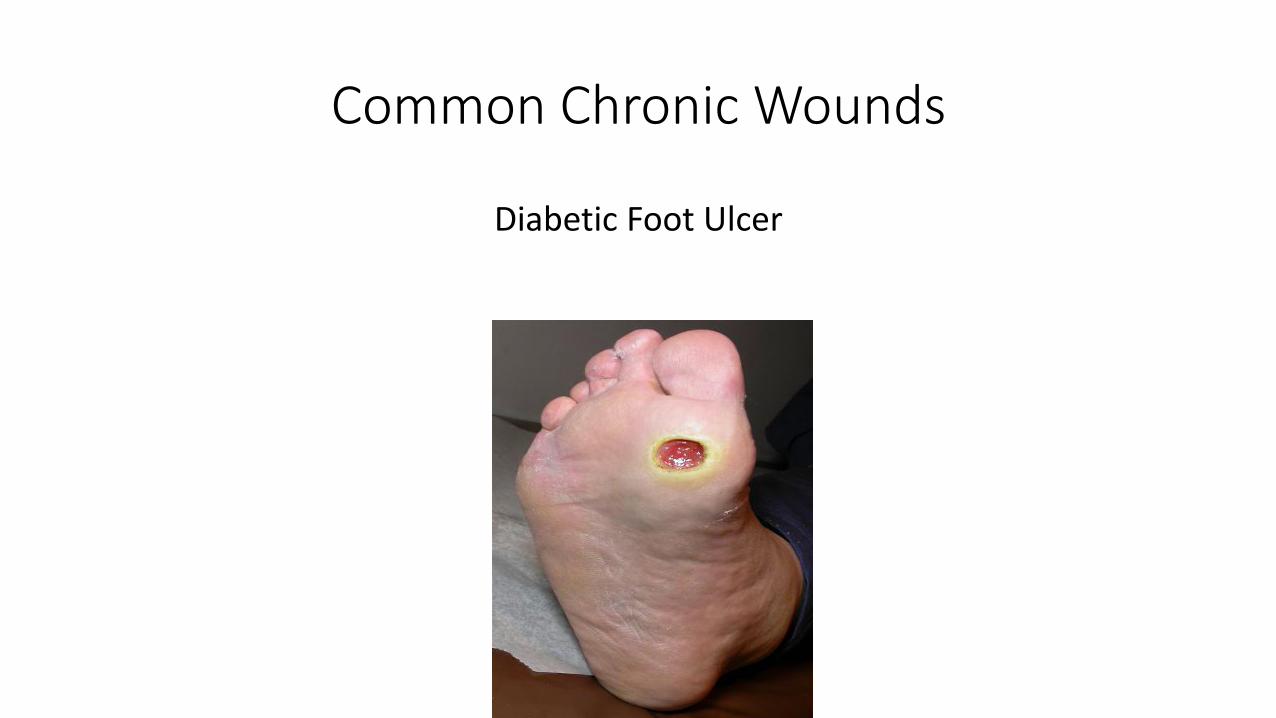
Common Chronic Wounds
Diabetic Foot Ulcer
ADA
• Approximately 340 million people in the world with DM.
• 1 in 4 will develop a diabetic foot ulcer (DFU) in their lifetime.
• Approximately 900,000 DFU each year in the U.S.
• 73,000 amputations each year in the U.S.
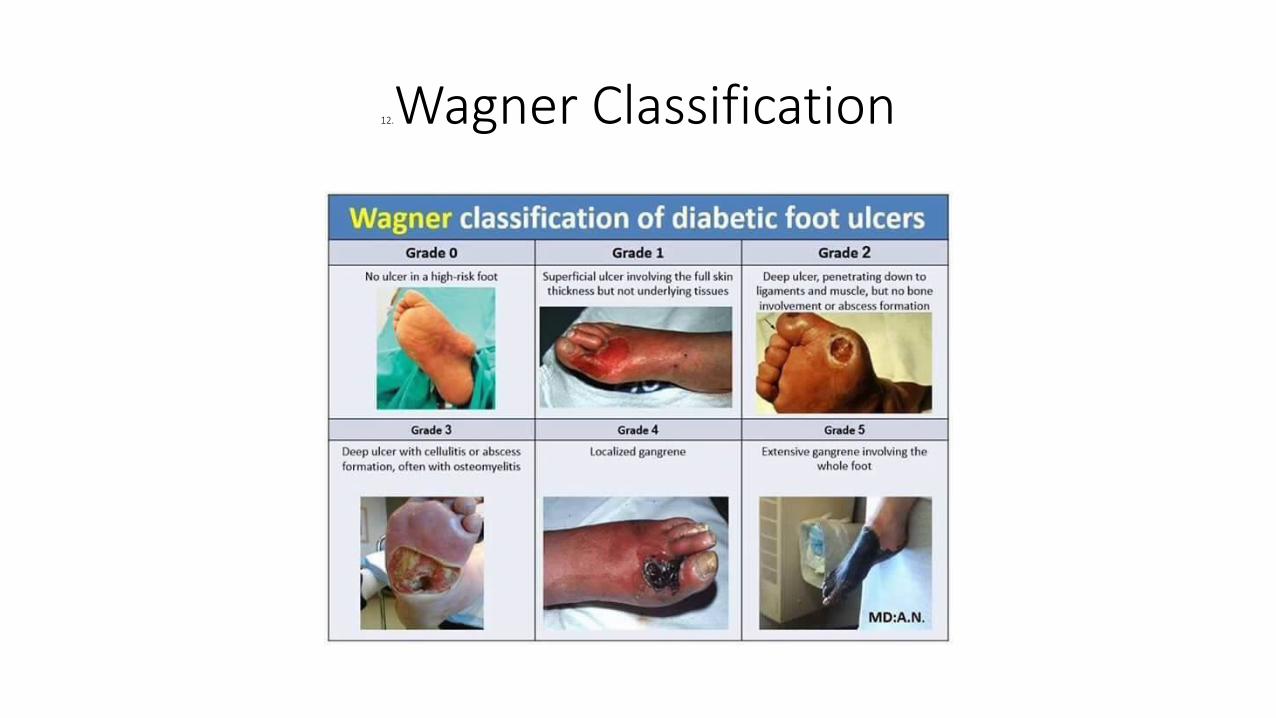
12.Wagner Classification
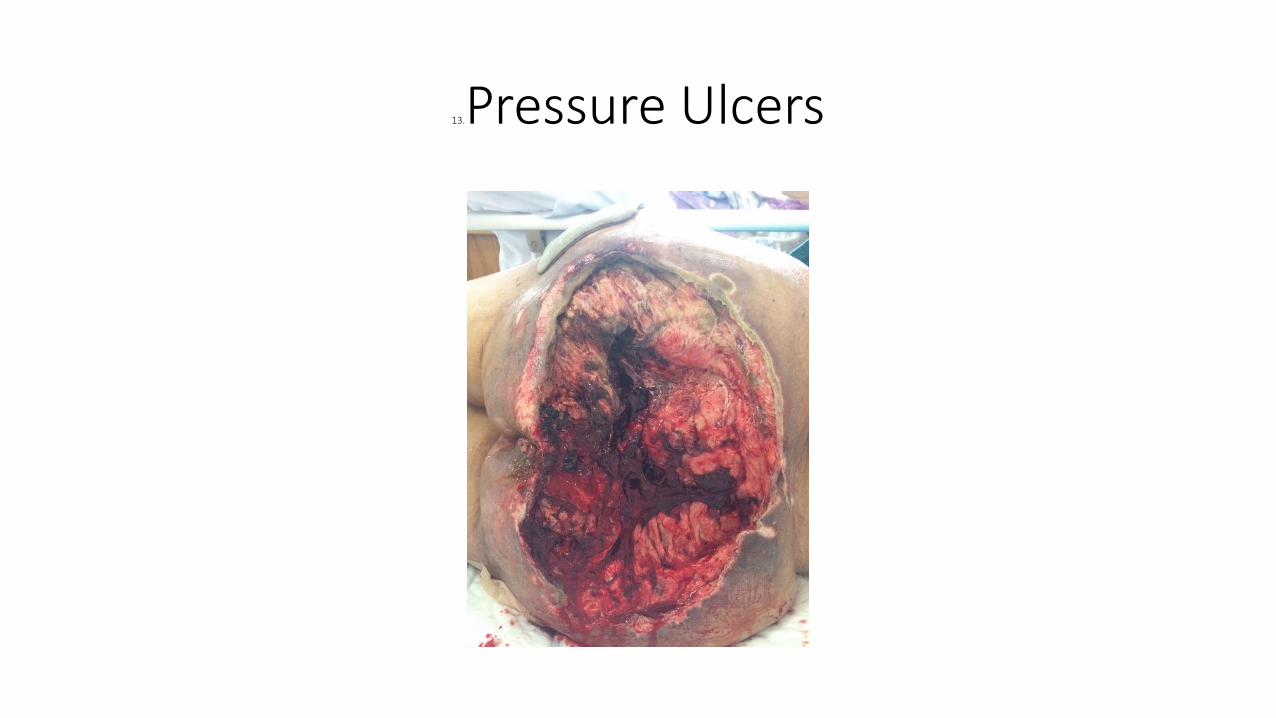
13.Pressure Ulcers
Pressure Ulcers
• Each year, 2.5 million Americans develop pressure ulcers. 14.
• Annual cost = 3 billion dollars. 15.
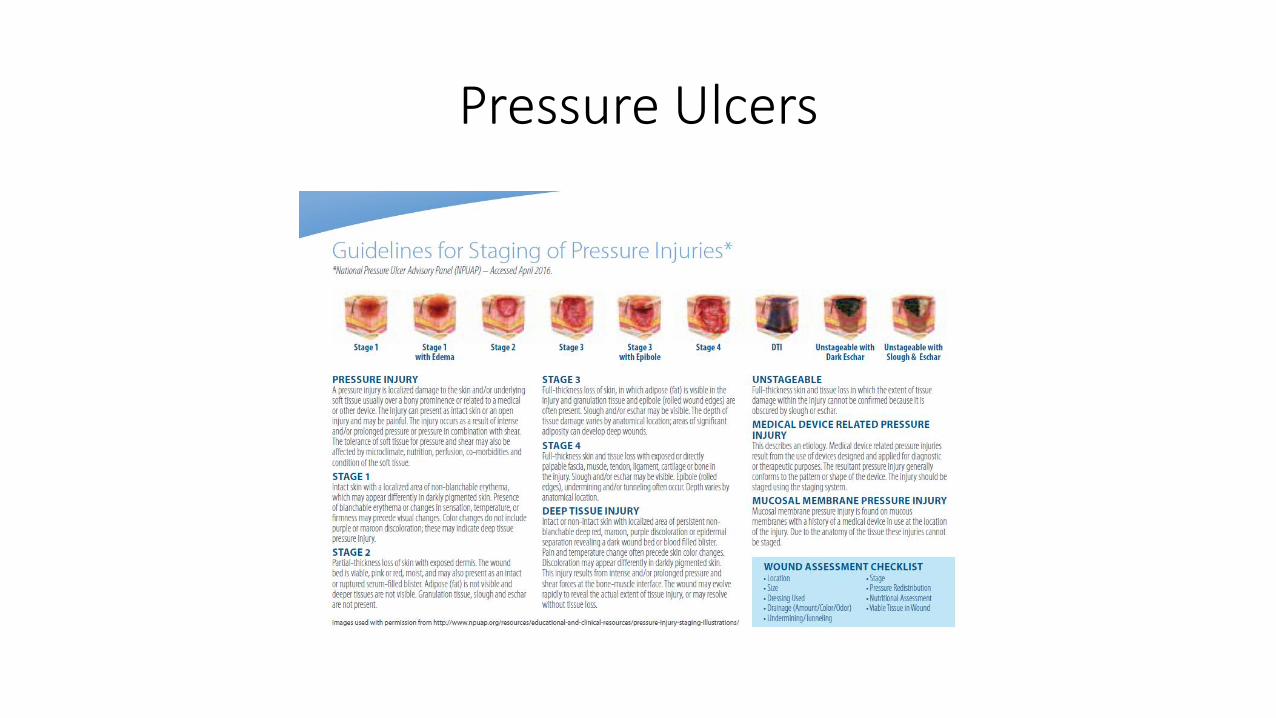
Pressure Ulcers
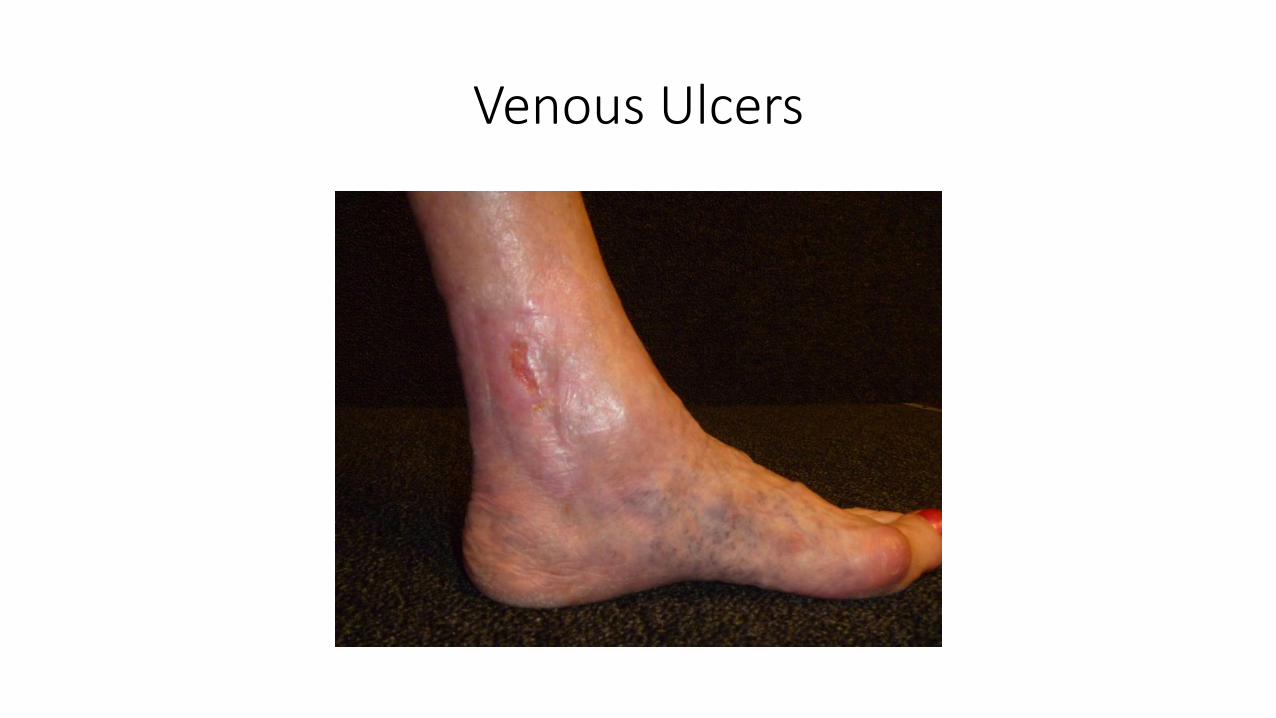
Venous Ulcers
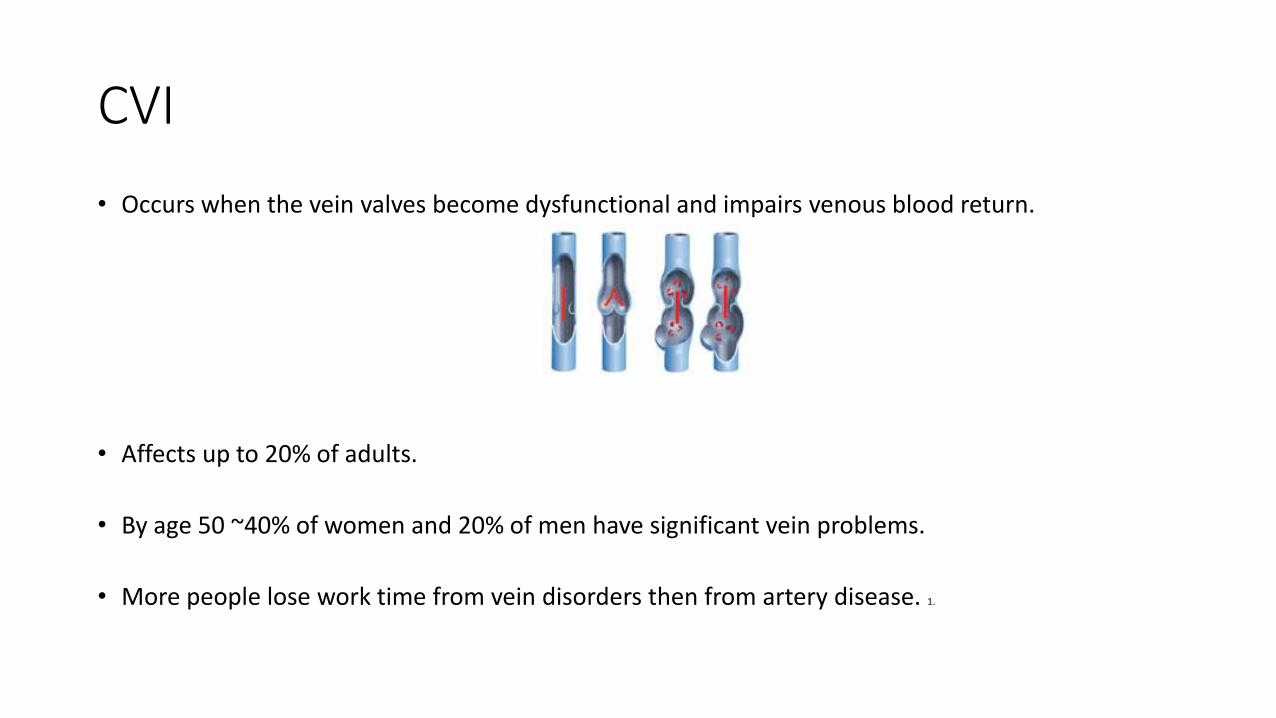
CVI
• Occurs when the vein valves become dysfunctional and impairs venous blood return.
• Affects up to 20% of adults.
• By age 50 ~40% of women and 20% of men have significant vein problems.
• More people lose work time from vein disorders then from artery disease. 1.
RISK FACTORS• Advancing age
• Family history of venous disease
• Ligamentous laxity (eg, hernia, flat fleet)
• Prolonged standing
• Increased body mass index
• Smoking
• Sedentary lifestyle
• Lower extremity trauma
• Prior venous thrombosis (superficial or deep)
• Arteriovenous shunt
• Hereditary conditions
• High estrogen states
• Pregnancy 2.
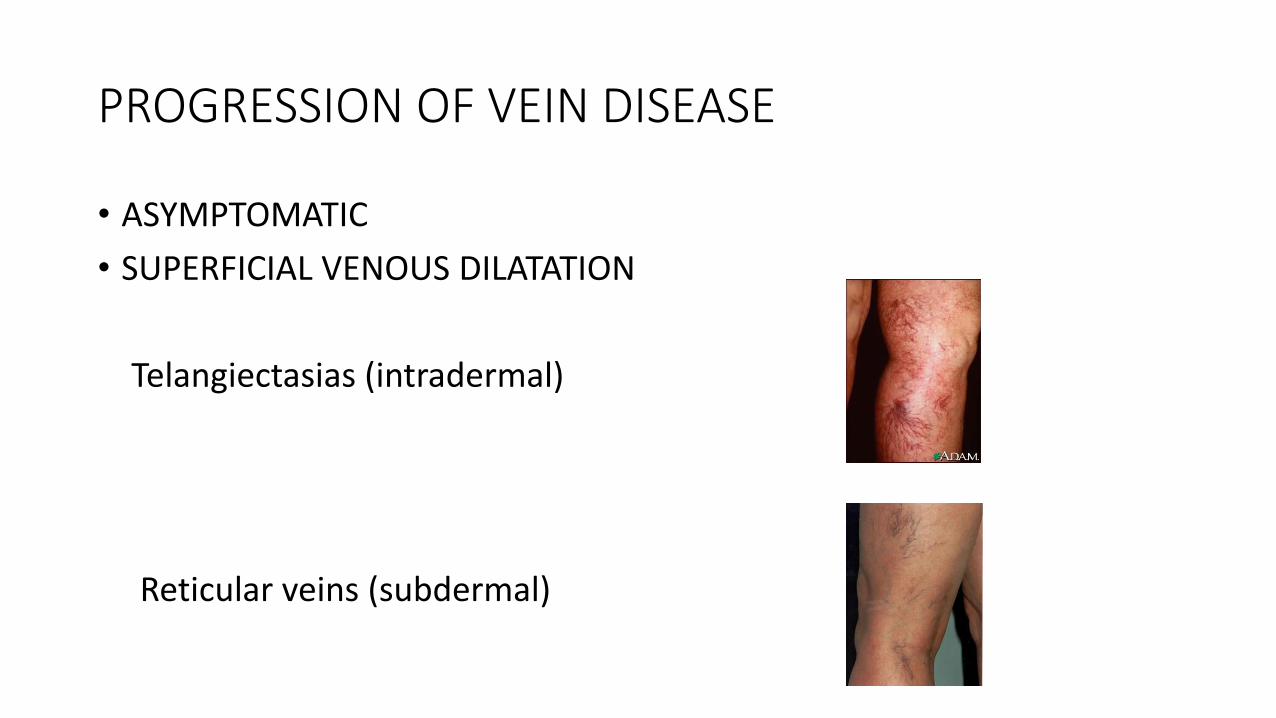
PROGRESSION OF VEIN DISEASE
• ASYMPTOMATIC
• SUPERFICIAL VENOUS DILATATION
Telangiectasias (intradermal)
Reticular veins (subdermal)
PROGRESSION OF VEIN DISEASE
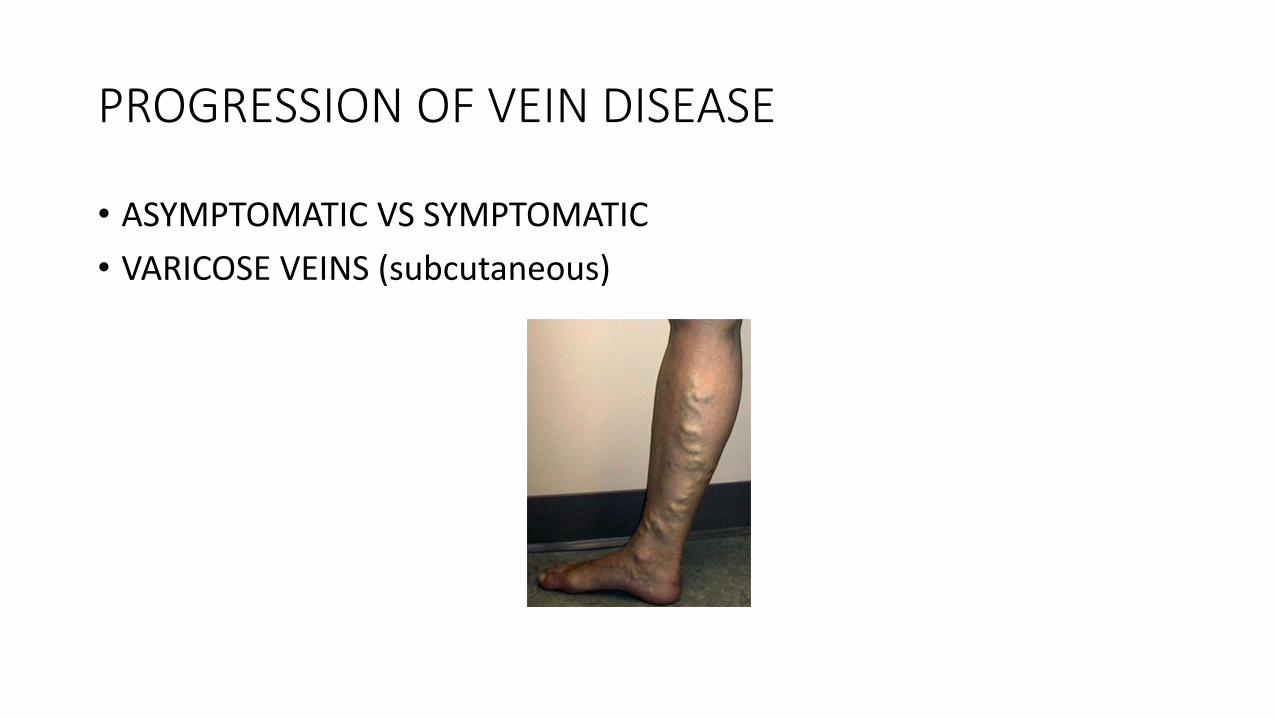
• ASYMPTOMATIC VS SYMPTOMATIC
• VARICOSE VEINS (subcutaneous)
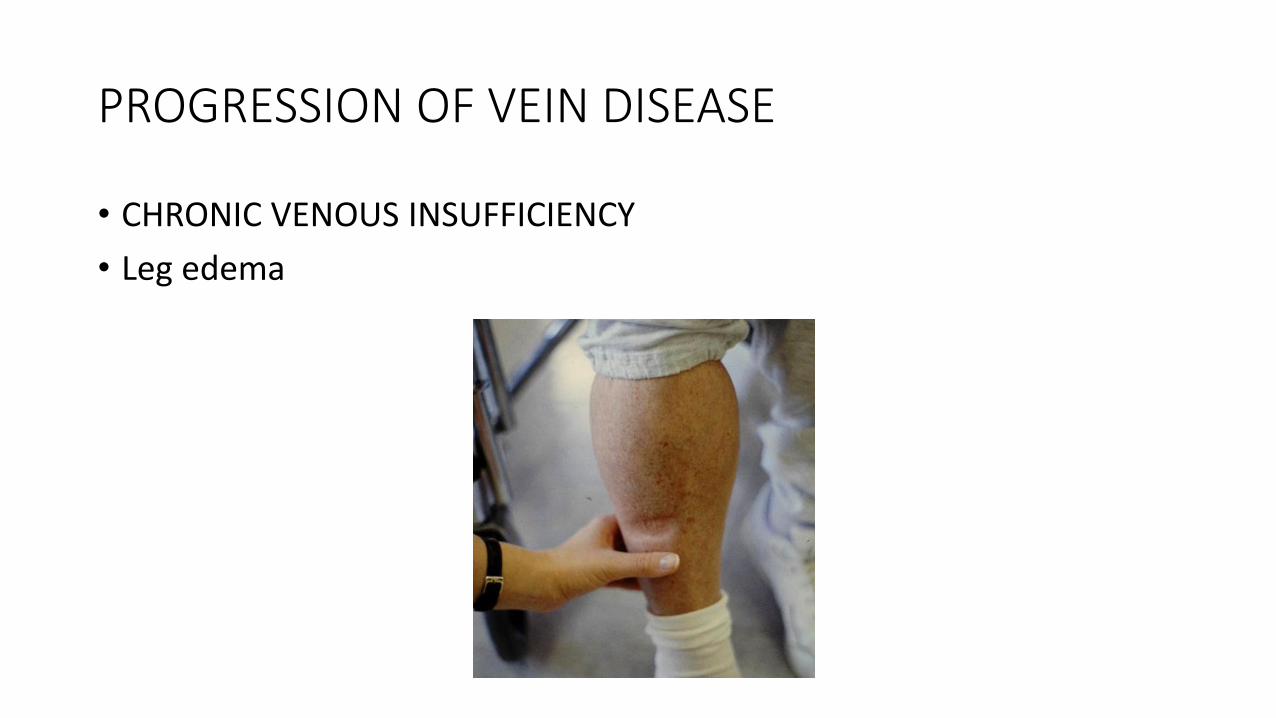
PROGRESSION OF VEIN DISEASE
• CHRONIC VENOUS INSUFFICIENCY
• Leg edema
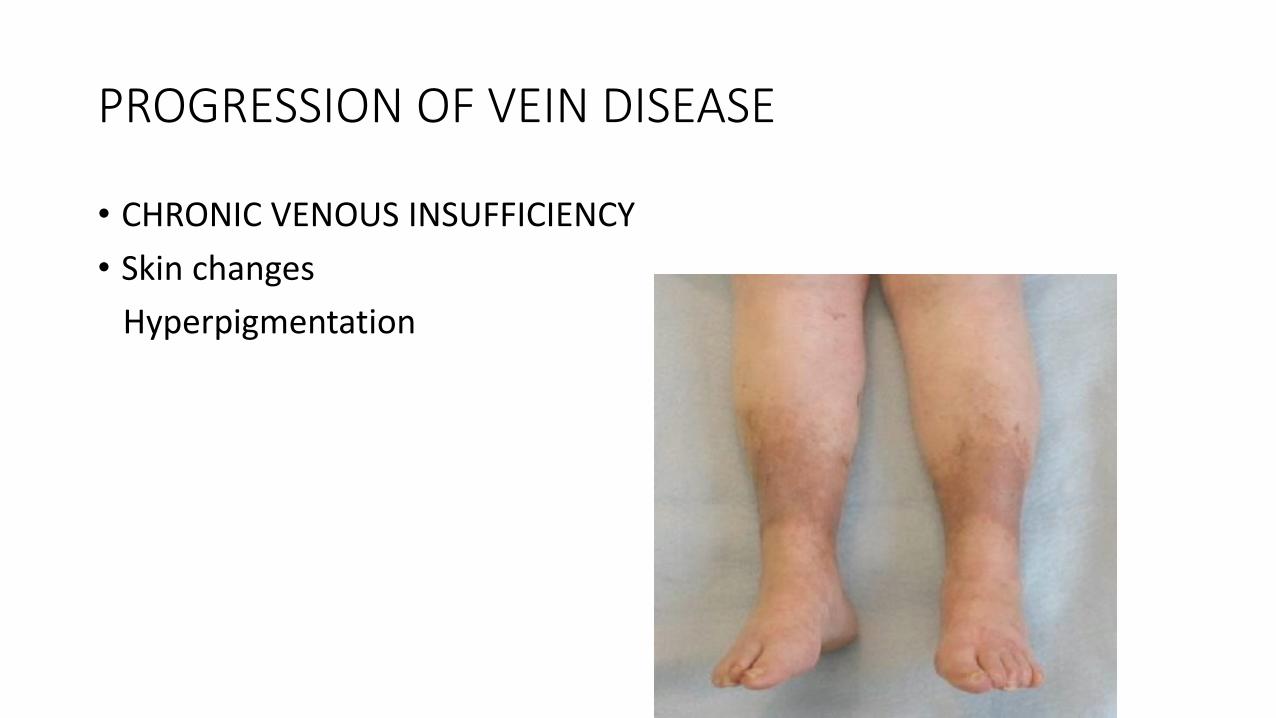
PROGRESSION OF VEIN DISEASE
• CHRONIC VENOUS INSUFFICIENCY
• Skin changes
Hyperpigmentation
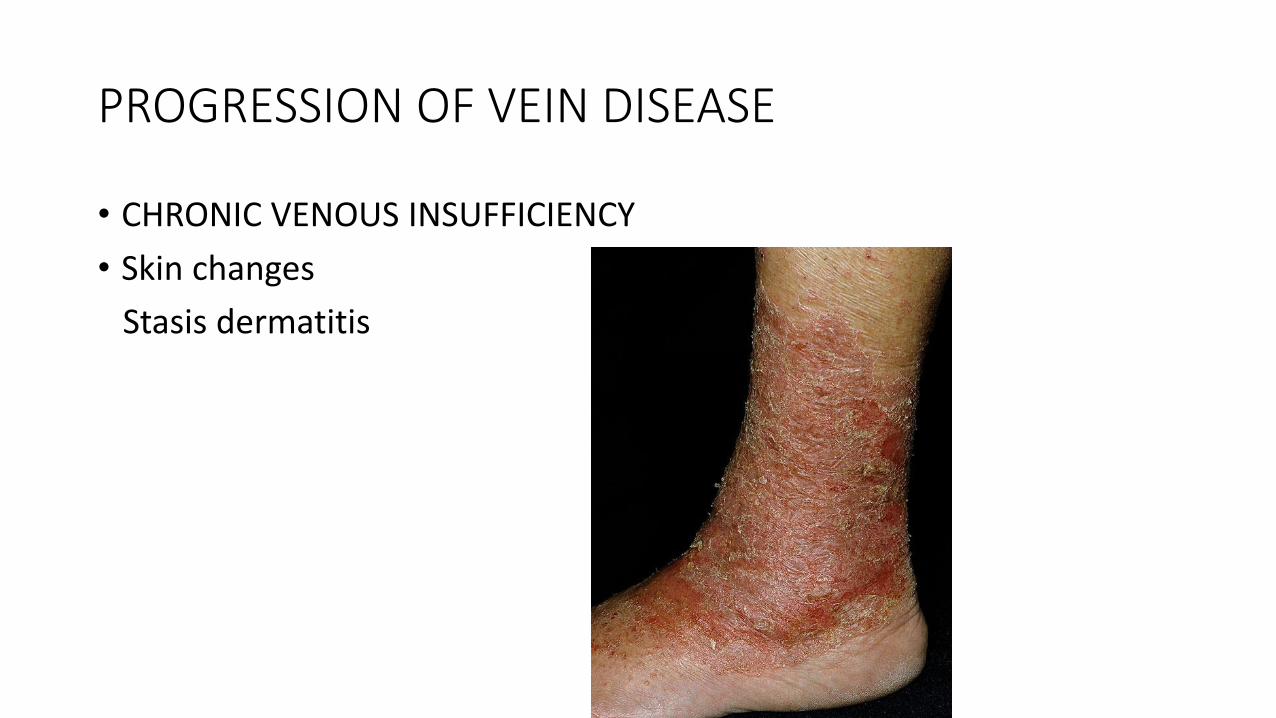
PROGRESSION OF VEIN DISEASE
• CHRONIC VENOUS INSUFFICIENCY
• Skin changes
Stasis dermatitis
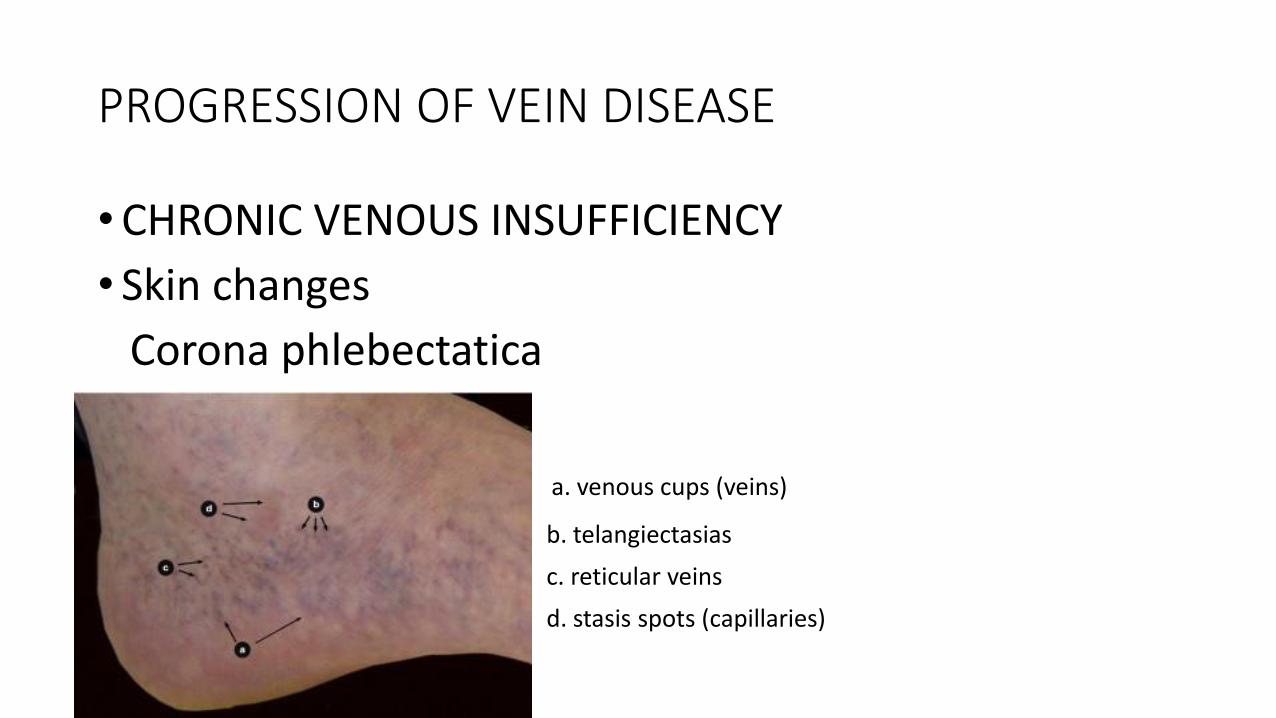
PROGRESSION OF VEIN DISEASE
•CHRONIC VENOUS INSUFFICIENCY
• Skin changes
Corona phlebectatica
a. venous cups (veins)
b. telangiectasias
c. reticular veins
d. stasis spots (capillaries)
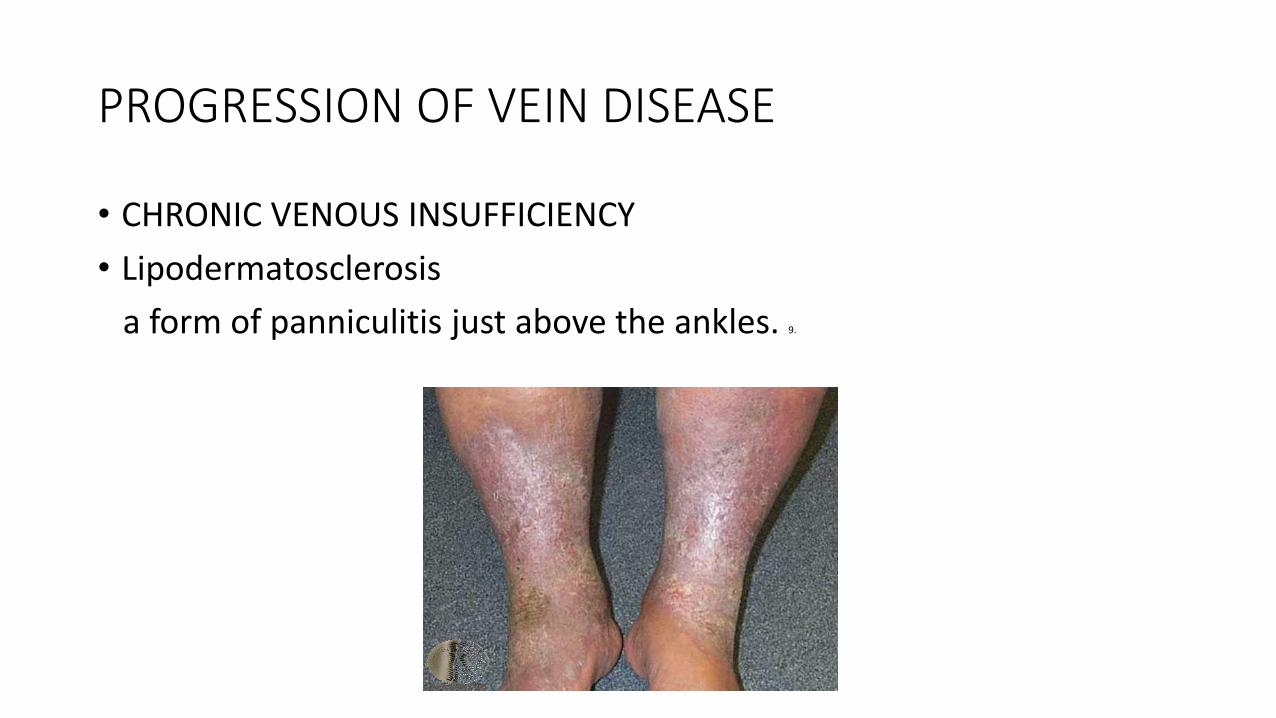
PROGRESSION OF VEIN DISEASE
• CHRONIC VENOUS INSUFFICIENCY
• Lipodermatosclerosis
a form of panniculitis just above the ankles. 9.
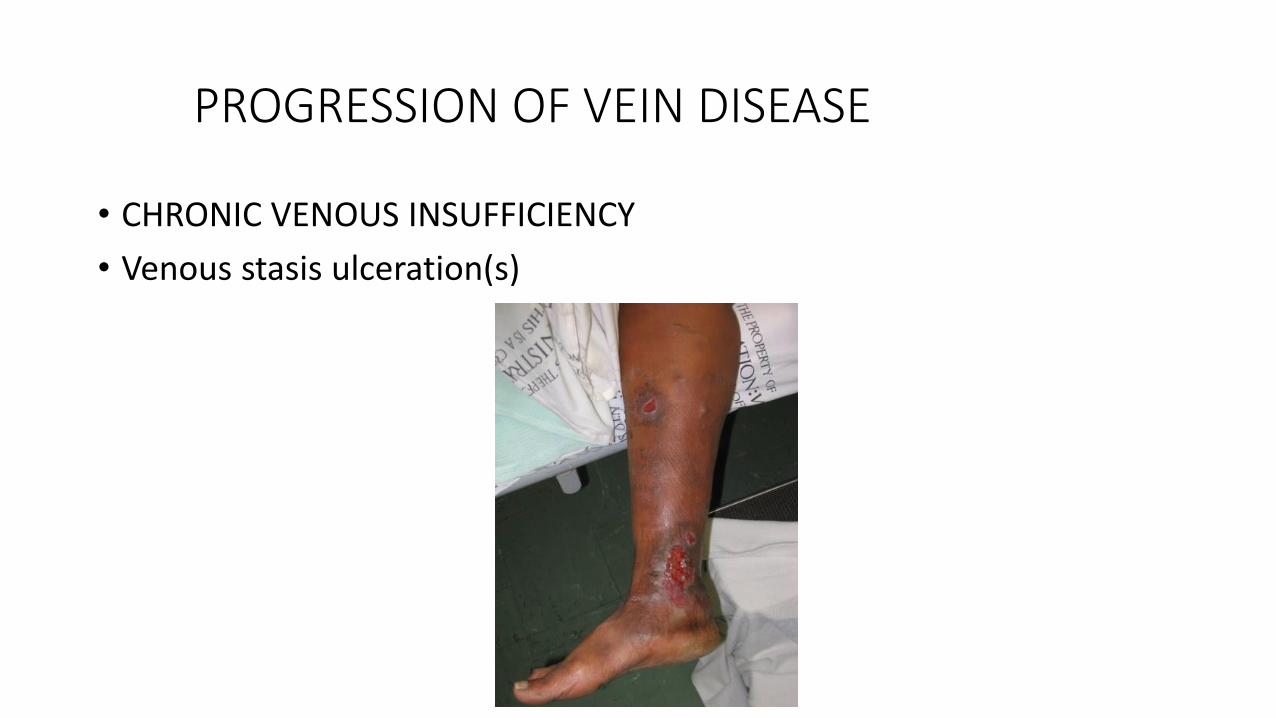
PROGRESSION OF VEIN DISEASE
• CHRONIC VENOUS INSUFFICIENCY
• Venous stasis ulceration(s)

EVALUATION
CHARACTERISTICS VENOUS ARTERIAL
APPEARANCE Irregular, dark pigmentation,
sometimes fibrotic, granulation,
usually shallow.
Irregular, smooth edge, minimum to
no granulation, usually deep with a
punched out appearance.
LOCATION Distal lower leg, medial malleolus. Distal lower leg/feet/toes, lateral
malleolus, anterior tibial area.
PEDAL PULSES Usually present. May be diminished or absent.
PAIN May be present. Usually improves
with leg elevation.
Usually painful especially with leg
elevation.
DRAINAGE Moderate to large. Minimal to none.
TEMPERATURE May be increased. May be decreased.
SKIN CHANGES Flaking, dry, hyperpigmented. Thin, shiny, hairless, yellow nails. 3.
EVALUATION
• VENOUS DOPPLER ULTRASOUND
Evaluate for deep and superficial venous
thrombosis.
Evaluate for incompetent veins with
significant reflux disease.
Evaluate for incompetent perforating
veins and tributaries.
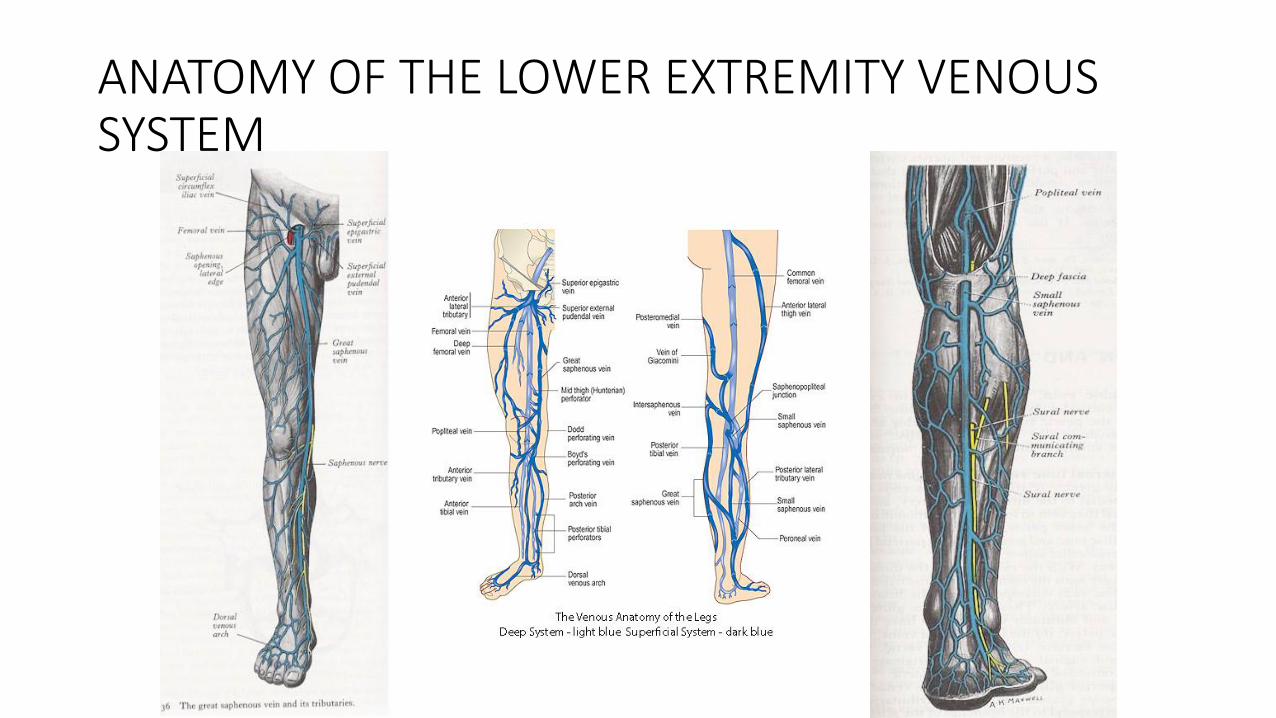
ANATOMY OF THE LOWER EXTREMITY VENOUS SYSTEM
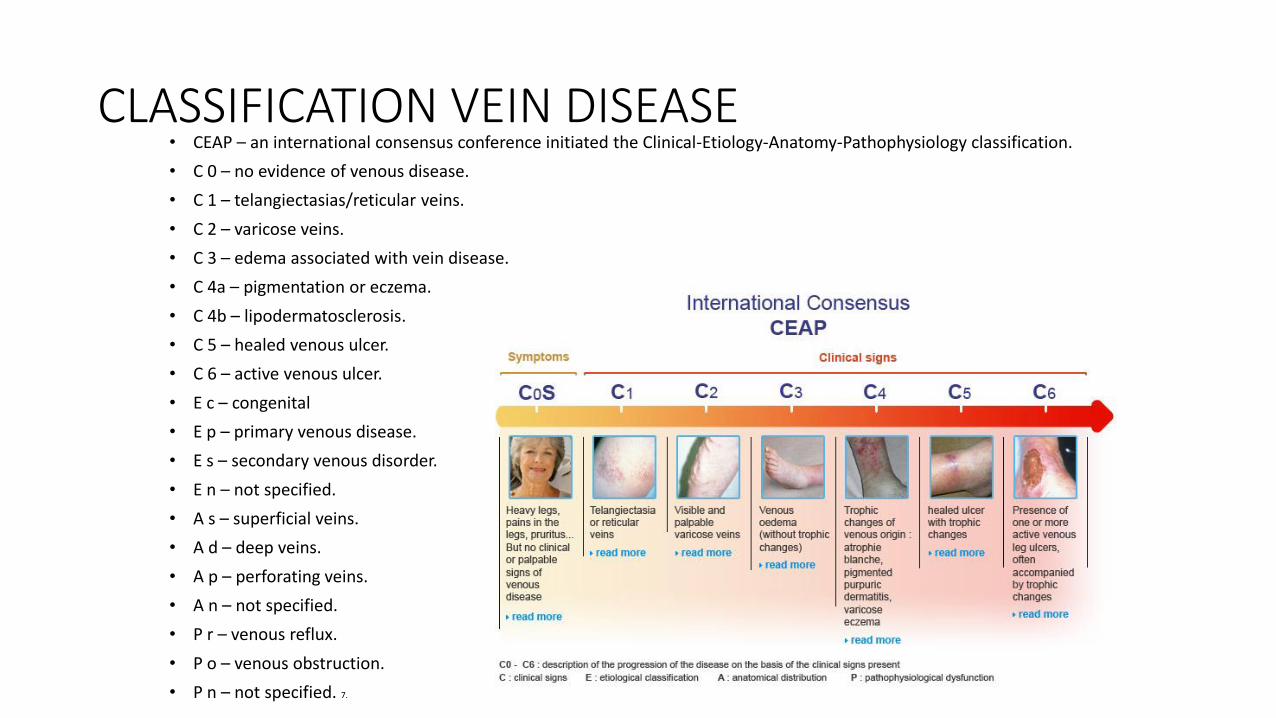
CLASSIFICATION VEIN DISEASE• CEAP – an international consensus conference initiated the Clinical-Etiology-Anatomy-Pathophysiology classification.
• C 0 – no evidence of venous disease.
• C 1 – telangiectasias/reticular veins.
• C 2 – varicose veins.
• C 3 – edema associated with vein disease.
• C 4a – pigmentation or eczema.
• C 4b – lipodermatosclerosis.
• C 5 – healed venous ulcer.
• C 6 – active venous ulcer.
• E c – congenital
• E p – primary venous disease.
• E s – secondary venous disorder.
• E n – not specified.
• A s – superficial veins.
• A d – deep veins.
• A p – perforating veins.
• A n – not specified.
• P r – venous reflux.
• P o – venous obstruction.
• P n – not specified. 7.
MANAGEMENT OF CVI
• LEG ELEVATION – heart level for 30 minutes 3-4 times daily improves micro-circulation reduces edema, and promotes healing of venous ulcers.4.
• EXERCISE – daily walking and simple ankle flexion exercises.

MANAGEMENT OF CVI – COMPRESSION THERAPY
• Compression bandages – elastic or non-elastic with single or multi-layers.

MANAGEMENT OF CVI – COMPRESSION STOCKINGS

MANAGEMENT OF CVI
• PNEUMATIC COMPRESSION THERAPY
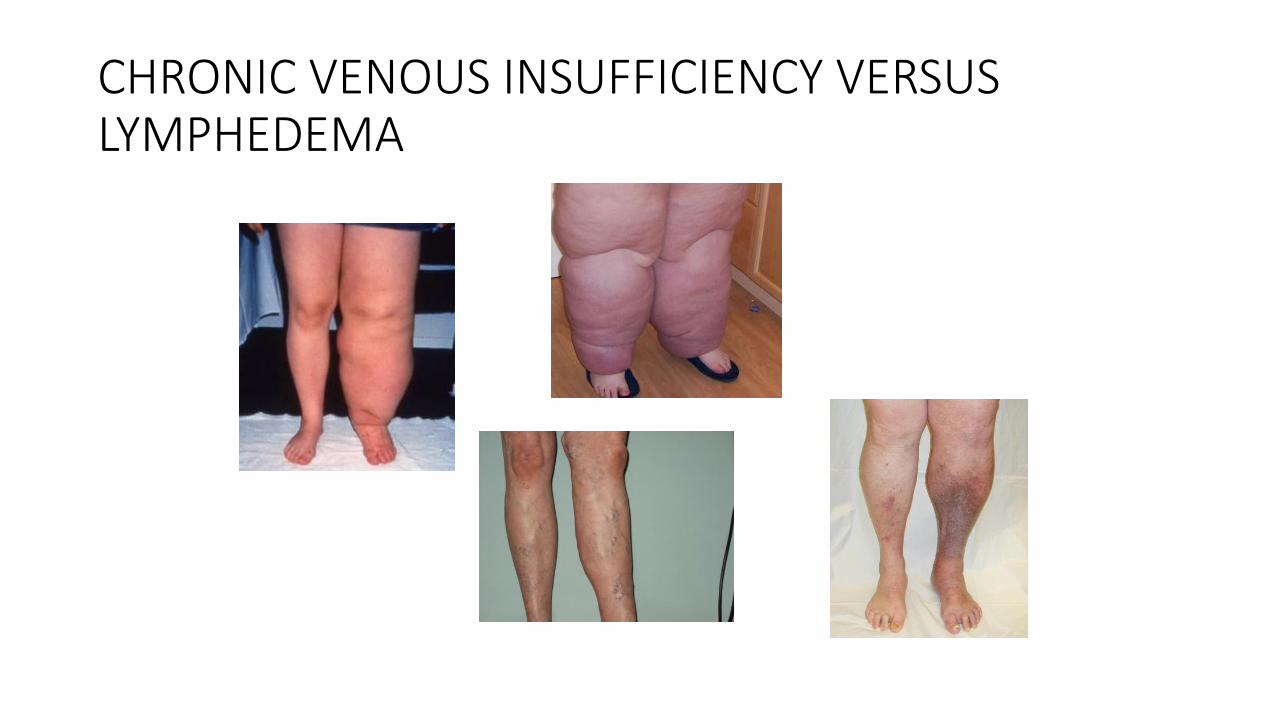
CHRONIC VENOUS INSUFFICIENCY VERSUS LYMPHEDEMA
MANAGEMENT OF CVI – VENOUS STASIS ULCERS
• Surgical debridement – used to remove devitalized tissue.
• Enzymatic agents – used to break down necrotic tissue (e.g. Santyl).
• Growth factors – synthesized by many cell types such as platelets, neutrophils, and epithelial cells (e.g. Regranex).
• Bioengineered tissue – used for a variety of non-healing ulcers (e.g. Apligraf, Dermagraft).
• Skin grafting – an option for non-healing ulcers. 4.
MANAGEMENT OF CVI – VENOUS STASIS ULCERS
• Dressings – depend upon the ulcer characteristics, frequency of dressing changes, and cost.
-Occlusive dressings may be fully occlusive (impermeable to gases and liquids) or semi-impermeable (impermeable to liquids and partially permeable to gases and water vapor).
It stimulates collagen synthesis, angiogenesis, and speeds reepithelialization.
-Low adherent gauze dressings – frequent changes but inexpensive.
-Hydrogels and alginate dressings are highly absorbent to handle heavily exudative ulcers, while hydrocolloids can help with wound debridement and skin protection.
-Silver can be incorporated if the ulcer is infected. 4.
MANAGEMENT OF CVI – ABLATION THERAPY
• Indications – patients with persistent signs/symptoms of venous disease after a minimum of 3 months of medical therapy (e.g. compression) and documented reflux (e.g. >0.5 seconds of reflux GSV).
• Absolute contraindications – acute DVT or phlebitis and pregnancy. 5,6.
• Radiofrequency versus laser endovenous ablation therapy.
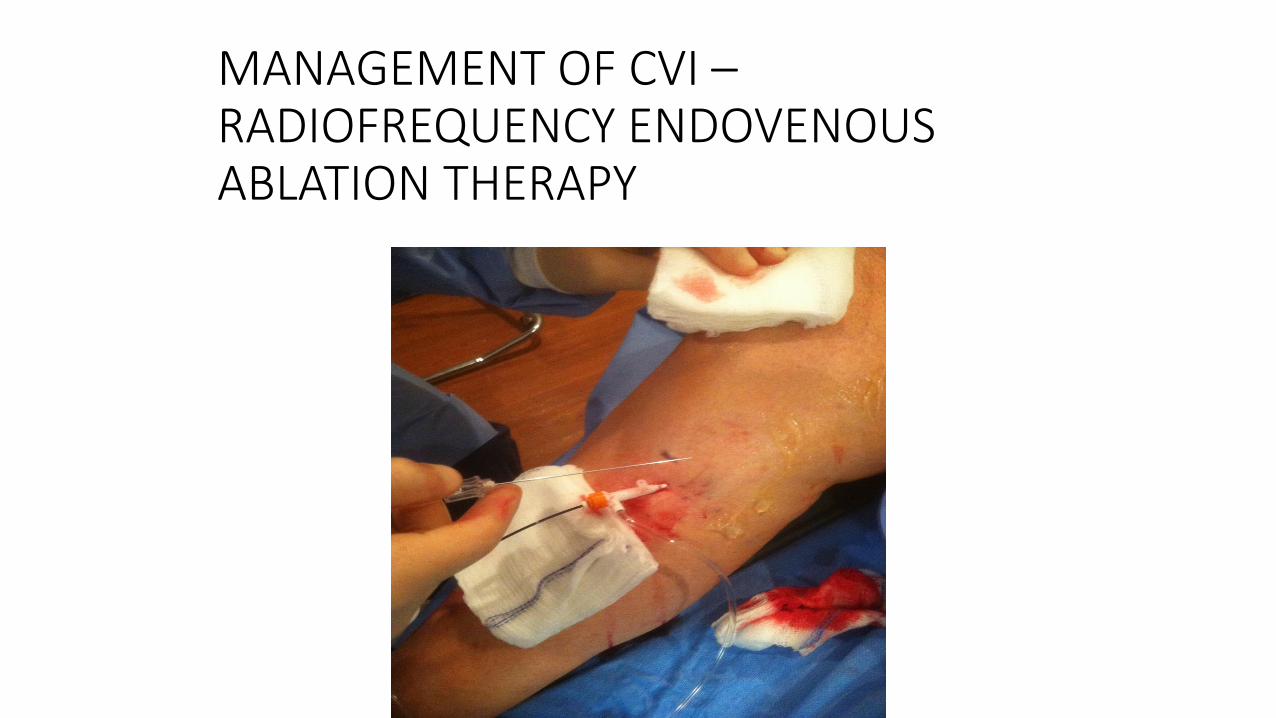
MANAGEMENT OF CVI – RADIOFREQUENCY ENDOVENOUS ABLATION THERAPY
• Radiofrequency devices – generate a high frequency alternating current for which the energy heats the adjacent vein walls to the probe which alters the protein structure of the vein effecting its closure. 5.
• Superficial veins include – Great Saphenous Vein, Small Saphenous Vein, Anterior Accessory Saphenous Vein and incompetent perforator veins.
MANAGEMENT OF CVI –RADIOFREQUENCY ENDOVENOUS ABLATION THERAPY
MANAGEMENT OF CVI – RADIOFREQUENCY ENDOVENOUS ABLATION THERAPY
MANAGEMENT OF CVI – RADIOFREQUENCY ENDOVENOUS ABLATION THERAPY
MANAGEMENT OF CVI – RADIOFREQUENCY ENDOVENOUS ABLATION THERAPY
MANAGEMENT OF CVI –RADIOFREQUENCY ENDOVENOUS ABLATION THERAPY

MANAGEMENT OF CVI –RADIOFREQUENCY ENDOVENOUS ABLATION THERAPY
BEFORE AFTER
MANAGEMENT OF CVI – ENDOVENOUS LASER ABLATION THERAPY
• Lasers emit a single, coherent wavelength of light. Laser therapy of venous structures is based upon the concept of selective photothermolysis (ie, selective thermal confinement of light induced damage). Vein wall injury is mediated directly by absorption of photon energy by the vein wall and indirectly by thermal convection from steam bubbles, and from heated blood.
• Superficial veins include – Great Saphenous Vein, Small Saphenous Vein, incompetent perforator veins, telangiectasias and reticular veins. 6.
MANAGEMENT OF CVI – MECHANICAL ABLATION
• Physical destruction of a vein with its partial or complete removal.
- Vein ligation/stripping
- Stab phlebectomy
- Powered phlebectomy
- Open or endoscopic perforator ligation.
MANAGEMENT OF CVI - SCLEROTHERAPY
• Chemical irritants injected to close unwanted veins. Preparations include liquid and foam. It is used primarily in the treatment of telangiectasias, reticular veins, and small varicose veins.
• These substances cause endothelial damage by their actions as either osmotic or detergent agents. Osmotic agents achieve their effect by dehydrating endothelial cells through osmosis. Detergents are surface active agents which damage the endothelium by interfering with cell membrane lipids. 8.
MANAGEMENT OF CVI - SCLEROTHERAPY
• DETERGENT AGENTS
- Sodium tetradecyl sulfate
- Polidocanol
• OSMOTIC AGENTS
- Hypertonic saline
- Glycerin
Chronic Wound Evaluation
• History and Physical.
• Wound culture and biopsy for pathology.
• Labs – ? CMP, CBC, Pre-albumin, A1c, sed rate, CRP.
• Vascular - ? Arterial dopplers, complete venous duplex US lower extremities.
• Radiologic – Xrays, MRI, bone scan.
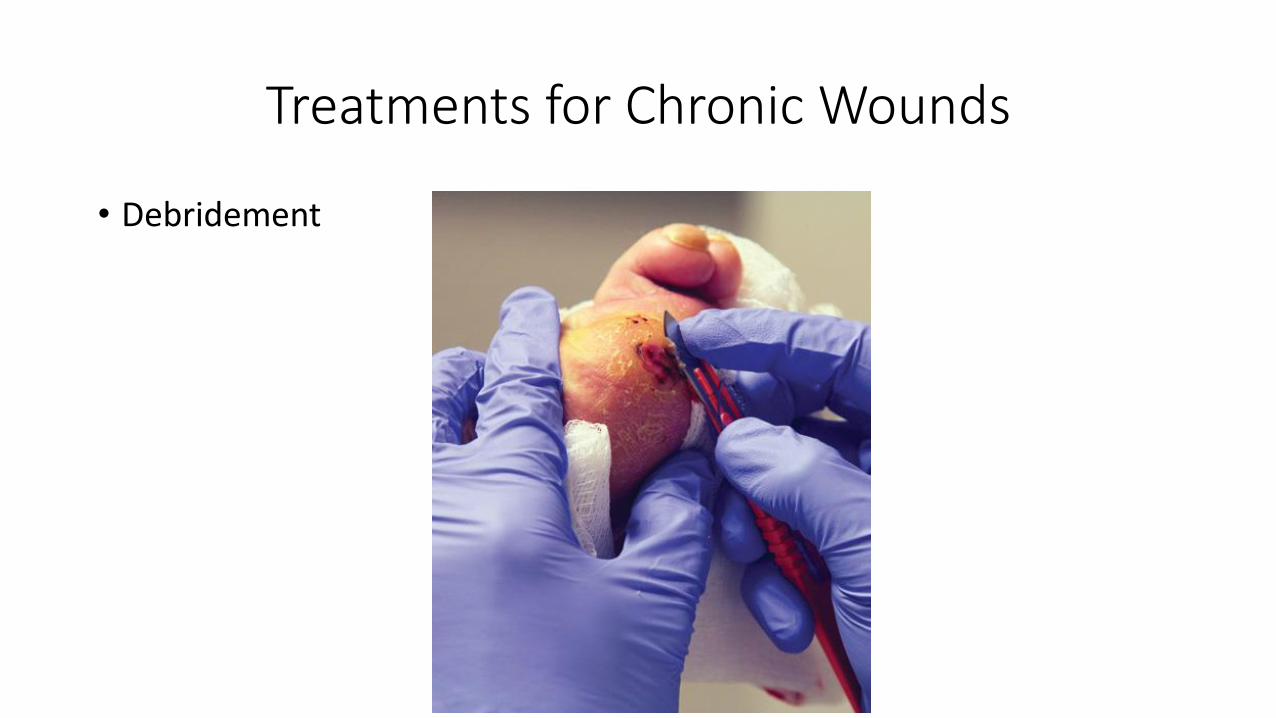
Treatments for Chronic Wounds
• Debridement

Treatments for Chronic Wounds
• Offloading if indicated.
• Total contact cast?
Treatments for Chronic Wounds
• Wound care dressings – Hydrocolloid, hydrogel, alginate, and collagen.
Treatments for Chronic Wounds
• Skin substitutes.
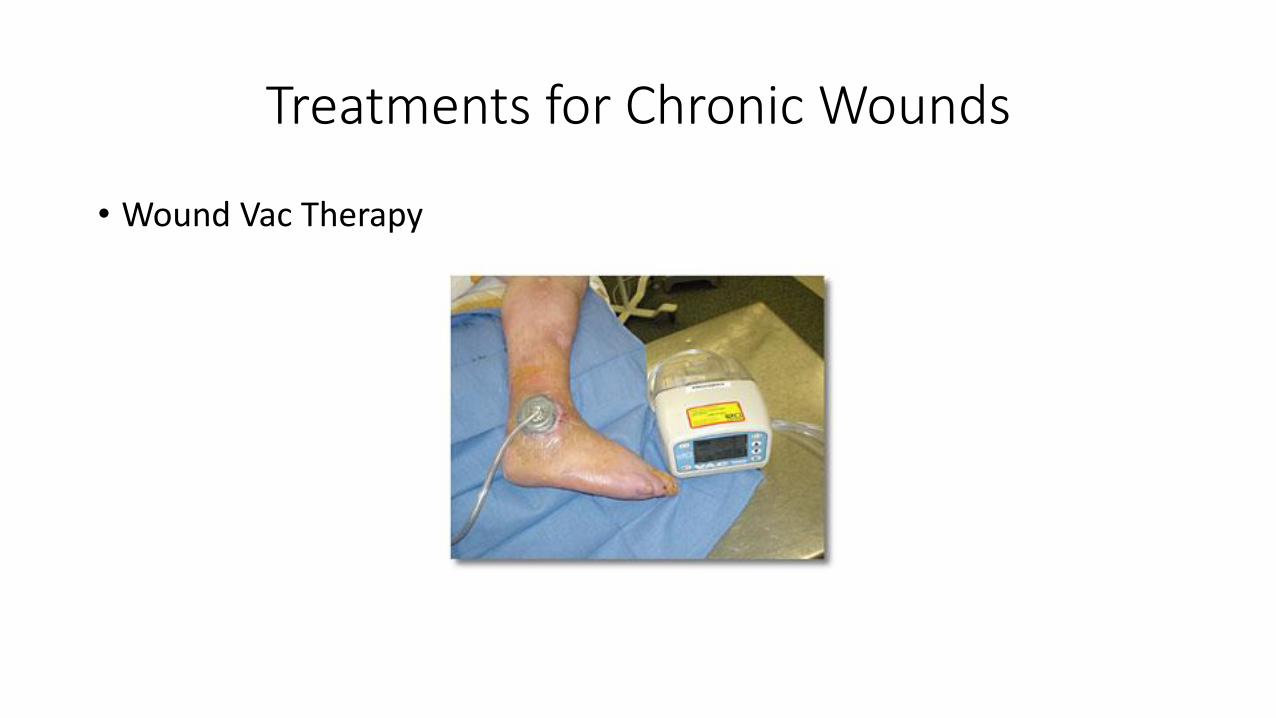
Treatments for Chronic Wounds
• Wound Vac Therapy
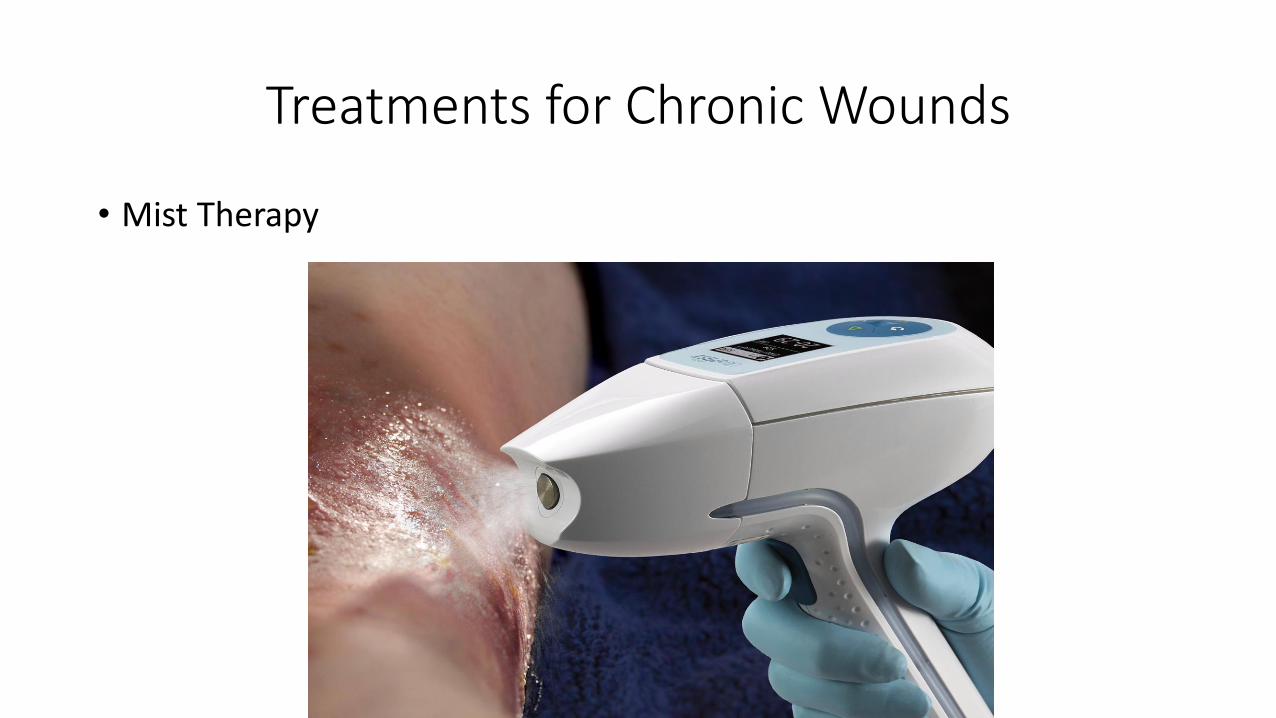
Treatments for Chronic Wounds
• Mist Therapy
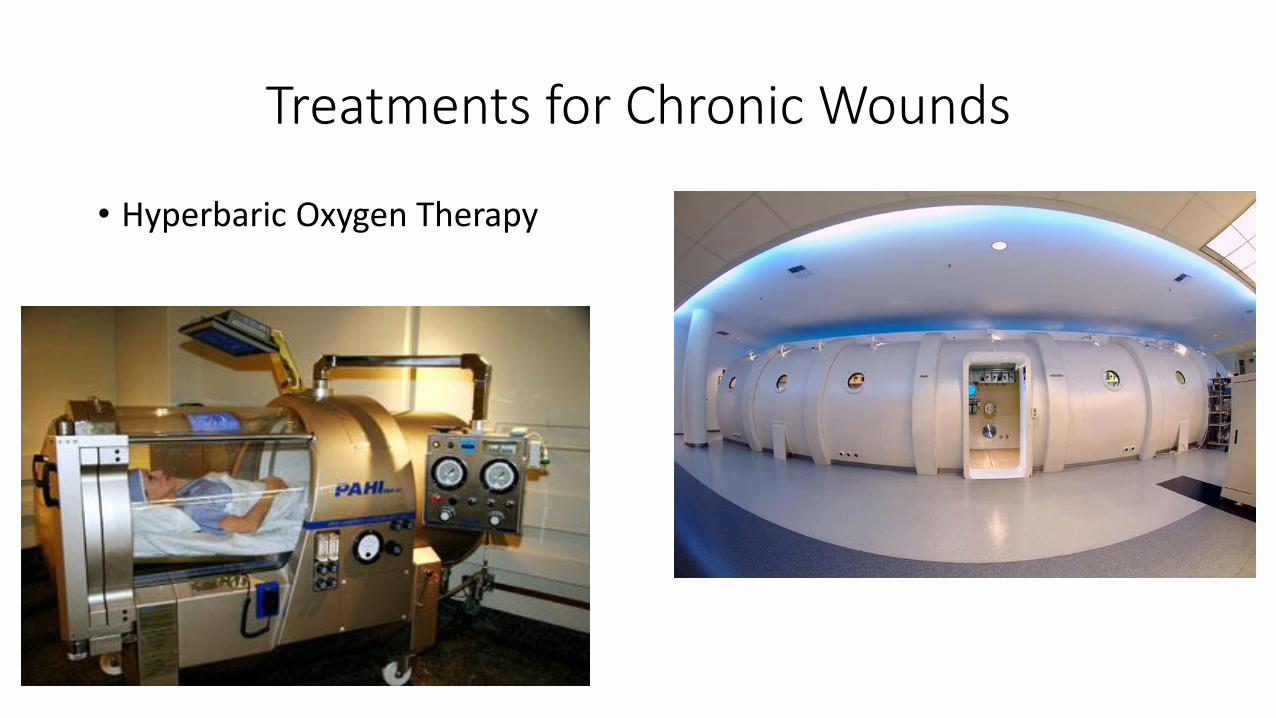
Treatments for Chronic Wounds
• Hyperbaric Oxygen Therapy
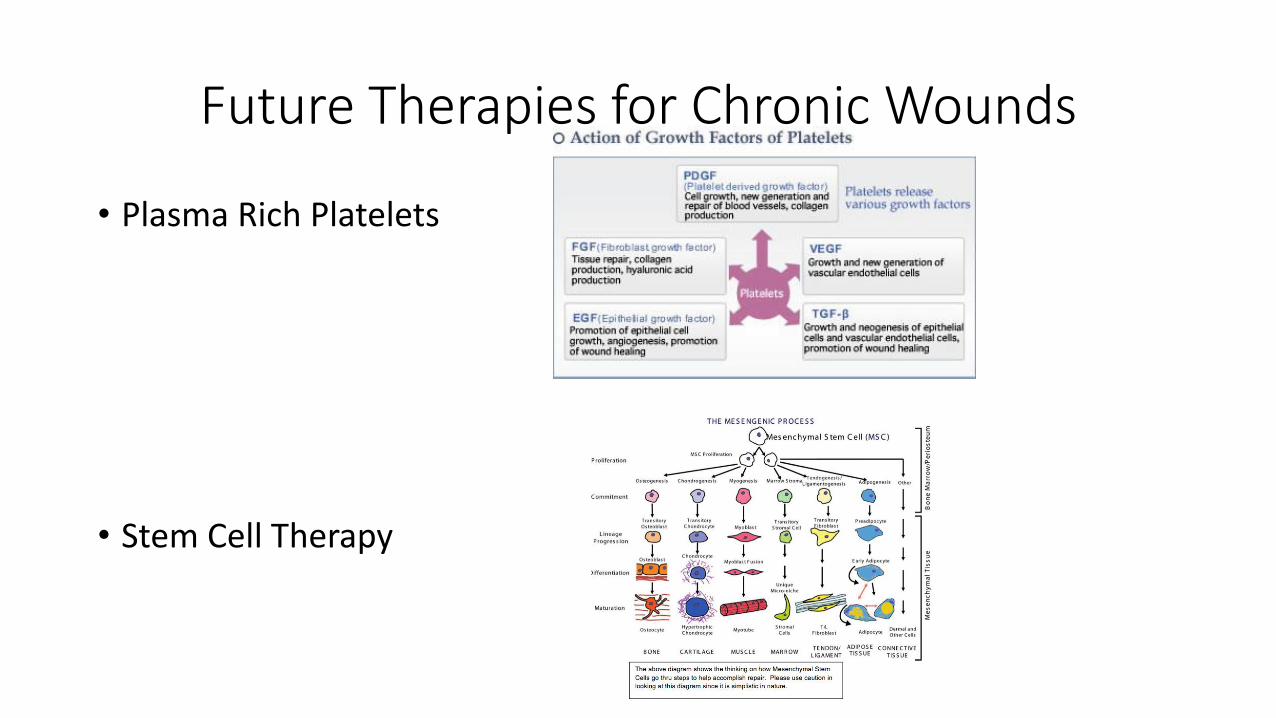
Future Therapies for Chronic Wounds
• Plasma Rich Platelets
• Stem Cell Therapy
REFERENCES
1, Medicalgraphics.de2. Sheehan P, Jones P, Giurini JM. Percent change in wound area of diabetic foot ulcers over a 4-week period is a robust predictor of complete healing in a 12-week prospective trial. Plast reconstr Surg 2006;117:239S.3. Overview of treatment of chronic wounds. Evans, K. Kim, Paul. Up To date. Copyright 2017.4. Chronic Wounds. Torre, J, Molnar, JA. Medscape. Updated 2017.5. Branski LK, Gauglitz GG, Herndon DN. A review of gene and stem cell therapy in cutaneous wound healing. Burns. 2008 July 4.6. Frykberg RG, Banks J. Challenges in the Treatment of Chronic Wounds. Adv. Wound Care. 2015 Sept 1. 7. Healio.com8. Parjournal.net.9. Sheldhealthcare.com.10. Herryyudha.blogspot.com.11. Homehealthconwordpress.com.12. Twitter.com13. Picquery.com.14. U.S. Dept of Health and Human Services. Presenting Pressure Ulcers in the Hospital. 2014.15. National Institute of Health.16. SaiSei-Iryou.com.17 Stemcellorthopedic.com.18. National Pressure Ullcer Advisory Panel.19. Alguire PC, Scovell S. Overview and management of lower extremity chronic venous disease. 2012. Up To Date.
