what will be presented today - reach counseling...treating trauma and traumatic grief in children...
TRANSCRIPT
WHAT WILL BE PRESENTED TODAY
How to challenge our viewpoints and perspectives to be
more trauma focused
Tools we can use to become more trauma informed and
effective
Resources we can use to help support our teens
THE ABC’S TO BEING TRAUMA INFORMED
Awareness
knowledge or perception of a situation or
fact.
Belief
an acceptance that a statement is true or
that something exists
Capacity
the ability or power to do, experience, or
understand something
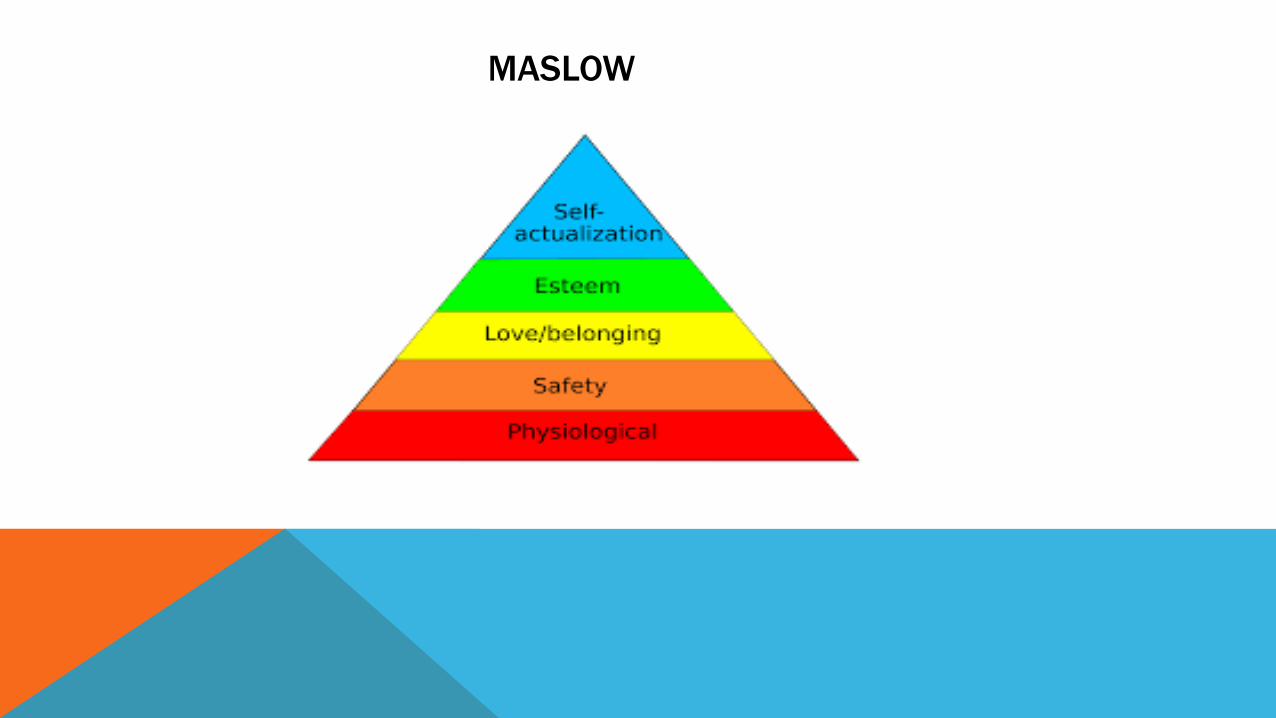
MASLOW
MASLOWS HIERARCHY OF NEEDS
1) Physiological needs: the person who is starving and dehydrated wants nothing more than water and food.
2) Once this need is satisfied, s/he desires safety and security – somewhere to live without being threatened or
harassed.
3) Once safety is achieved, s/he wants to obtain a sense of belonging, of being accepted and loved, and also seeks
healthy relationships.
4) After the above goals are satisfied, the next need, according to Maslow, is to develop a sense of self – esteem.
5) The final need, Maslow informs us, is to achieve the highly elusive state of self-actualization. By self-
actualization, he meant creatively reaching one’s potential and finding meaning and purpose in life. Maslow
also states that this need is only satisfied by individuals extremely rarely.
WHAT DO PEOPLE TAKE FOR GRANTED WHEN THEIR NEEDS ARE MET?
THE EFFECTS OF CHILDHOOD TRAUMA ON OUR ABILITY TO
ASCEND MASLOW’S PYRAMID OF NEEDS:
The Effects Of Childhood Trauma On Our Ability To Ascend Maslow’s Pyramid Of Needs:
Childhood trauma can drastically impinge upon our ability to reach these goals. For example:
– a highly neglectful parent may not feed his/her child properly, meaning that that child’s physiological needs are
not met
– a child who lives with a parent who abuses him/her, or lives in a household in which domestic violence exists will
live in an atmosphere of fear and, therefore, will not have his/her needs for safety and security met
– the child who is rejected by his/her patents will not have his/her need to belong satisfied nor is s/he likely to
develop a solid sense of self-esteem
FAULTY TRAUMA ASSUMPTIONS
-Teens are grateful for help
-You are the reason for their actions or lack of
-Your approach to them is non threatening
-They have the ability at this time to process or take in information given
-Tools given are able to be useful outside of your safe environment
EVERYONE HAS EM……
What are some experiences that have formed your beliefs?
What are some ways these beliefs affect how we see others?
How are these ideas changed if we see things from a survival perspective?
THE EFFECTS OF TOXIC STRESS AND TRAUMA ON
DEVELOPMENT AND WELL‐BEING It may be harder to forge a trusting relationship, because the young person has not experienced adults as
consistently safe.
Parents and teachers may describe the youth as easily upset, easily provoked, or highly reactive.
The youth may display what others consider inappropriate emotions and behavior.
The young person may be triggered by traumatic reminders.
The youth may be diagnosed as hyperactive, or oppositional, or conduct disordered.
The teen may appear inattentive, but he is actually hyper- attentive to “danger signals” of which adults are not
aware.
common post-traumatic presentation is dissociation. This may be reported as “lying” – which actually represents a
confabulated reality produced to replace actual events difficult to recall - or “zoning out” – which has proven
adaptive during traumatic moments.

ACTING OUT
What if we see behaviors as the sign that a person might be dealing with trauma?
OUR INTERACTIONS CAN BE HEALING . . . OR CAN
RE‐TRAUMATIZE Many who have experienced trauma have a harder time distinguishing between healthy and unhealthy
relationships. Therefore, the issue of trust and betrayed trust will be a major, on-going issue.
Relationships worthy of trust are the foundation of progress.
We have been taught healthy things whether we knew it or not. We often can expect healthy behaviors without
realizing these are not things they have ever seen or understand
Appropriate boundaries are key underpinnings of relationships. Because traumatized youth have so little
experience with trust, breaking their trust or not following through on a perceived commitment can cause great
harm.
Think about the possibility of past adversity as an underlying problem when you are up against something you don’t
understand. If you cannot understand why someone does or doesn’t do something that seems to be common
sense, be curious and ask “What happened?”
USEFUL TOOLS TO INCREASE OUR KNOWLEDGE
NATIONAL CHILD TRAUMATIC STRESS NETWORK
http://www.nctsn.org/sites/default/files/assets/pdfs/tips_for_finding_help.pdf
ITS OK TO SAY WE ARE
NOT EQUIPPED AND
REACH FOR HELP.
Why is it important for us to know our limitations when it
comes to trauma ?
So we can have the
capacity
to do something about it!
TF CBT
NATIONAL CERTIFICATION
Tfcbt.org
Master’s degree & licensure
Completion of TF-CBT Web Training (http://tfcbt.musc.edu/)
Minimum 2 days live training with approved trainer or developer
Follow up consultation/supervision for 6-12 months
3 completed cases
Use of standardized instrument to assess progress
Passing TF-CBT knowledge test.
WHAT IS TF-CBT?
A structured individual and parent trauma-focused model for children and adolescents (3-18 years old) who have
experienced one or more traumatic events and are experiencing symptoms as a result.
Includes initial skills-based components followed by more trauma-specific components with gradual exposure
integrated into each component.
CORE VALUES -CRAFTS
Components Based
Respectful of cultural values
Adaptable and Flexible
Family Focused
Therapeutic relationship is central
Self-efficacy is central
EVIDENCE BASE
TF-CBT is the most researched and most supported of all current treatments for childhood Posttraumatic Stress
Disorder (PTSD) and child trauma, with seven completed randomized controlled trials (RCT), three open (non-
controlled) studies, and four ongoing RCTs. (www.nctsn.org)
Evidence base is strong when done in sequence.
A TF-CBT THERAPIST…
Has knowledge about child/adolescent trauma & development.
Has trauma-specific assessment skills
Is able to be directive as well as to inhabit a teacher role in session
Has child and adult therapy skills
Has resolved personal trauma issues
Guards against colluding with avoidance
Seeks consultation with others experienced in using the model
Is able to resist chasing of COWs
PRACTICE COMPONENTS
Assessment
Conceptualization
Psychoeducation & Parent Education
Relaxation
Affect Regulation
Cognitive Coping
Trauma Narrative
In vivo exposure
Conjoint Sessions
Enhancing Future Safety
CAREGIVER INVOLVEMENT
Caregiver engagement is essential
1:1 – Parallel child’s progress through components.
Green light parent:
Believes child
Stays child-focused
Is positive and supportive of child
Protects child

GRADUAL EXPOSURE
The process through which children and parents undergo incremental desensitization to trauma reminders → relief
from emotional/physiological distress upon re-exposure.
This is what makes it Trauma-Focused
This does NOT refer to the gradual telling of a child’s trauma story.
As the child progresses through the model, therapist encourages parent and child to implement skills with
increasing specificity of reminders of the abuse until the details are recounted in narrative compenent.
PSYCHOEDUCATION
Handouts providing trauma specific info (i.e. sexual abuse, witness to DV)
Common reactions to stress and trauma
Common parent reactions to child trauma
Neurobiology of trauma
Fight, flight, freeze
Triggers
A Terrible Thing Happened Holmes et al (2000)
PARENTING
Generic Parenting skills and trauma-specific skills.
Validate parents’ concerns and take them seriously.
Functional Analysis of behaviors: what is the goal of the behaviors? (escape, attention, control?)
GE: Help parents understand the impact of the traumatic experience on themselves and the child – frame child’s
behavior as due to trauma, rather than being “bad.”
RELAXATION
Goal: Decrease physiological reactivity and/or learn mindfulness.
Peaceful Piggy Meditation or Moody Cow Meditates (McLean)
Breathing
Progressive Muscle Relaxation
Guided Imagery
https://www.youtube.com/watch?v=_mZbzDOpylA (Sesame Street: Belly Breathe)
http://amysmartgirls.com/short-film-just-breathe-helps-kids-deal-with-emotions/
AFFECT REGULATION
Goal: To improve identification and expression of feelings
“How might a child feel when they experience abuse?”
Focus on recognizing emotional triggers and regulating emotion, not on the description of the experiences
themselves
If trauma reminders are a main cause of dysregulation, they may not improve significantly till after the narrative.
COGNITIVE COPING
Goal: To change inaccurate and unhelpful thoughts to accurate and helpful thoughts; and to link thoughts and
feelings to behaviors.
MINIMAL MASTERY
When to move on to next component?
1 skill used 1 time, away from therapist
TRAUMA NARRATIVE
Goals:
To expose the child to distress of trauma memories in measurable doses – desensitization
To integrate and make meaning out of the trauma.
Not: a forensic interview, or a tell all
Is: a therapist guided process
HOW DO WE KNOW WHEN WE’RE “DONE”?
Measuring Desensitization
Decreased refusal/avoidance
Affective changes
0-10 rating drop by ½
Increase in trauma details
Willingness to write about other traumas
Willingness to share with witness
“This is boring…”
COGNITIVE PROCESSING
Guide child to add thoughts and feelings at key points
Guide child to change euphemistic language
Guide child to correct distortions about fault, blame and responsibility
Identify themes and make meaning of them
CONJOINT SESSIONS
Goal:
Have the child share the full trauma narrative with caregiver
Have the caregiver witness the telling, give praise, believe and cheerlead.
Always prepare the caregiver.
Witness must be an adult
ENHANCING FUTURE SAFETY
Goals:
Increase child’s safety skills
Address safety with caregiver
Should occur after narrative component so child will not blame self for not preventing the trauma, but we can move
this up if there are urgent safety concerns not being addressed by skill building in PRAC components.
Assertiveness skills
Ask parent/child to bring in topics (i.e. internet, dating)
Protective skills
ENDING TF-CBT
Post test of PTSD assessment & share results
“Graduation” party
Maintenance sessions if needed
WHAT ARE TRAUMA FOCUSED ASPECTS THAT YOU CAN SEE IN
THIS CASE DESCIPTION
GENERAL RESOURCES
http://depts.washington.edu/hcsats/PDF/TF-%20CBT/pages/psychoeducation.html (many good handouts
applicable to all components)
http://learn.nctsn.org/mod/pcast/view.php?id=9497&mode=4&hook=I (ADHD vs. Trauma Symptoms podcast)
www.nctsn.org
https://www.pinterest.com/cami0416/
Treating Trauma and Traumatic Grief in Children and Adolescents & Trauma Focused CBT for Children and
Adolescents: Treatment Applications, both by Judith A. Cohen , Anthony P. Mannarino , Esther Deblinger
OTHER GREAT COMMUNITY RESOURCES
NAMI: YOUTH AND FAMILY PROGRAM
COORDINATOR Megan Mc Lachlin
REMEMBER
• When we are trauma informed, we shift from a stance of “What’s wrong with you?” to “What happened to
you?”
• When we are trauma informed we are respectful and minimize the possibility of triggering their reactivity.
• When we are trauma informed we understand what is about us and what is not about us. When we do not
interpret mistrust, reactivity, or anger as personally directed, we can respond with empathy rather than
defensiveness.
• When we are trauma informed we learn to “hold” others’ pain in a supportive way rather than to “own” it.
• When we work with youth who have endured unbearable lives, we often find that in sharp contrast to them
being “damaged” or “broken,” they are sensitized and fully committed to making others’ lives better.