what is the extent of safety and efficiency of drug desensitization on patients with allergic...
TRANSCRIPT
What is the Extent of Safety and Efficiency of Drug Desensitization on
Patients with Allergic Reactions?
Cindy Law
Dr. Mary Lee-Wong
What are Allergies?
An abnormal sensitivity to an allergen that is inhaled, eaten, or touched
An overreaction of a hypersensitive immune system
Misidentification of a harmless substance as harmful
Common Types of Allergies
Allergic rhinitis Food Medication Insect stings Latex chemical
Allergies and the Immune System
B-lymphocytes &T-lymphocytes
Lymphocytes identifies a foreign invader
Foreign antigens cause production of antibodies
5 types of immunoglobulins
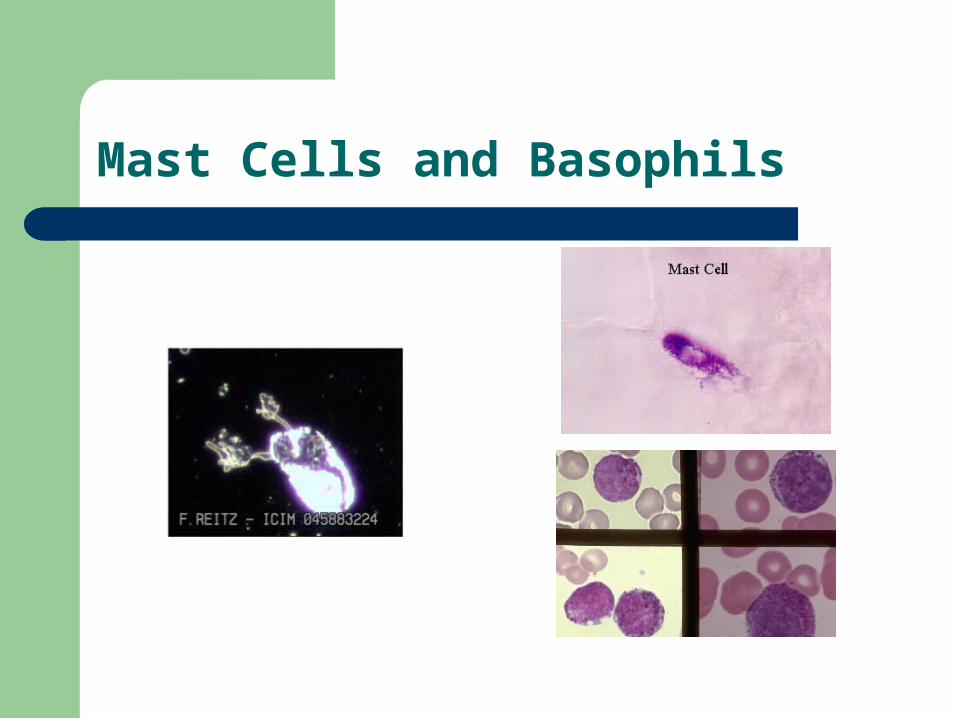
Mast Cells and Basophils
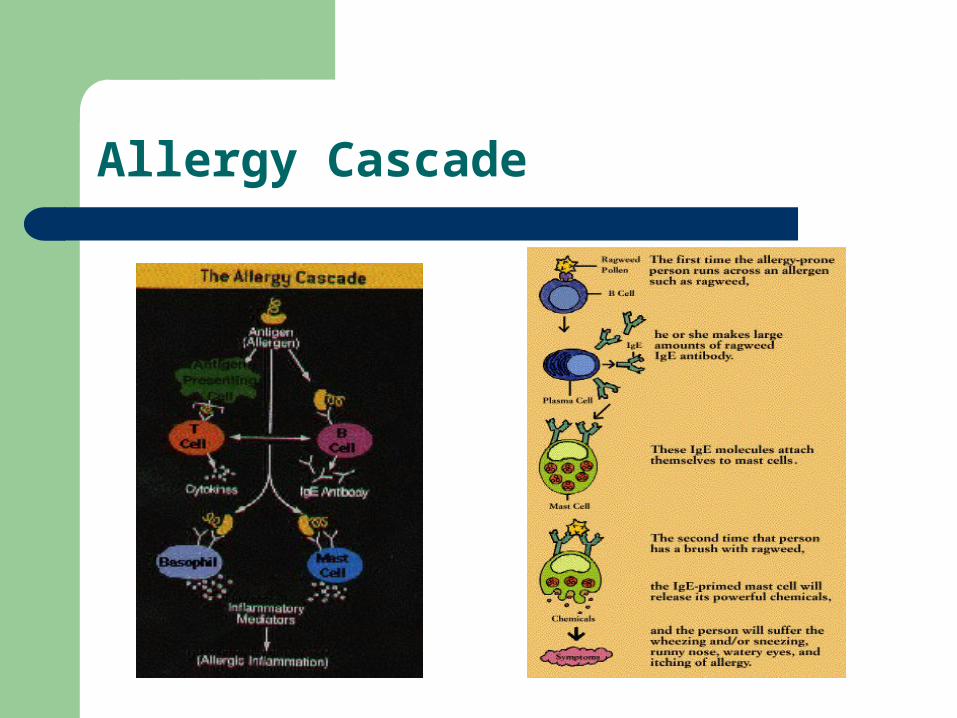
Allergy Cascade
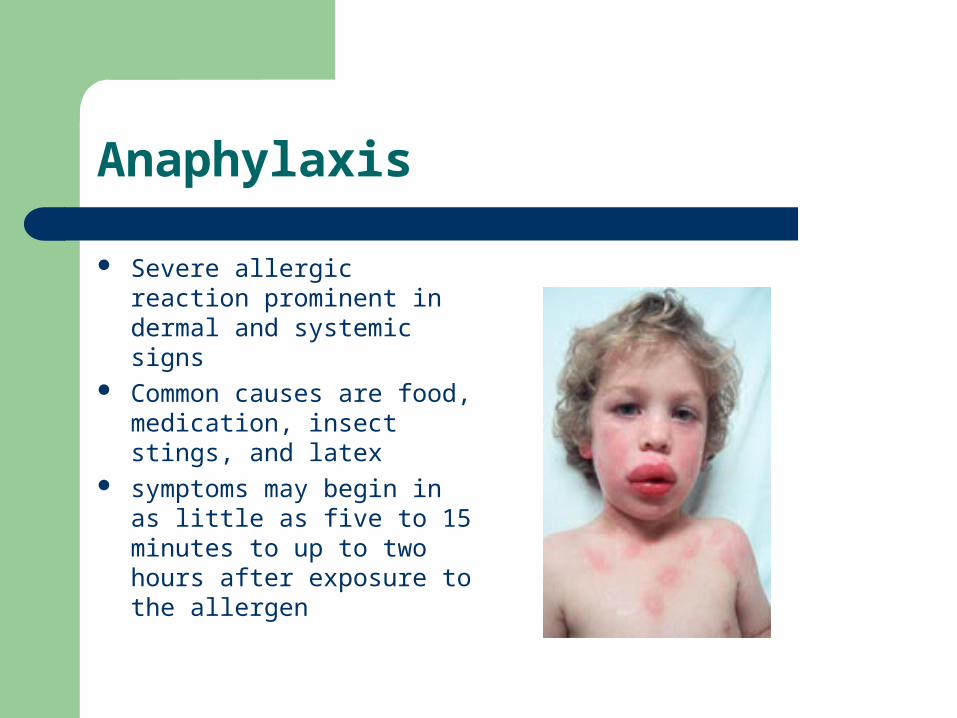
Anaphylaxis
Severe allergic reaction prominent in dermal and systemic signs
Common causes are food, medication, insect stings, and latex
symptoms may begin in as little as five to 15 minutes to up to two hours after exposure to the allergen
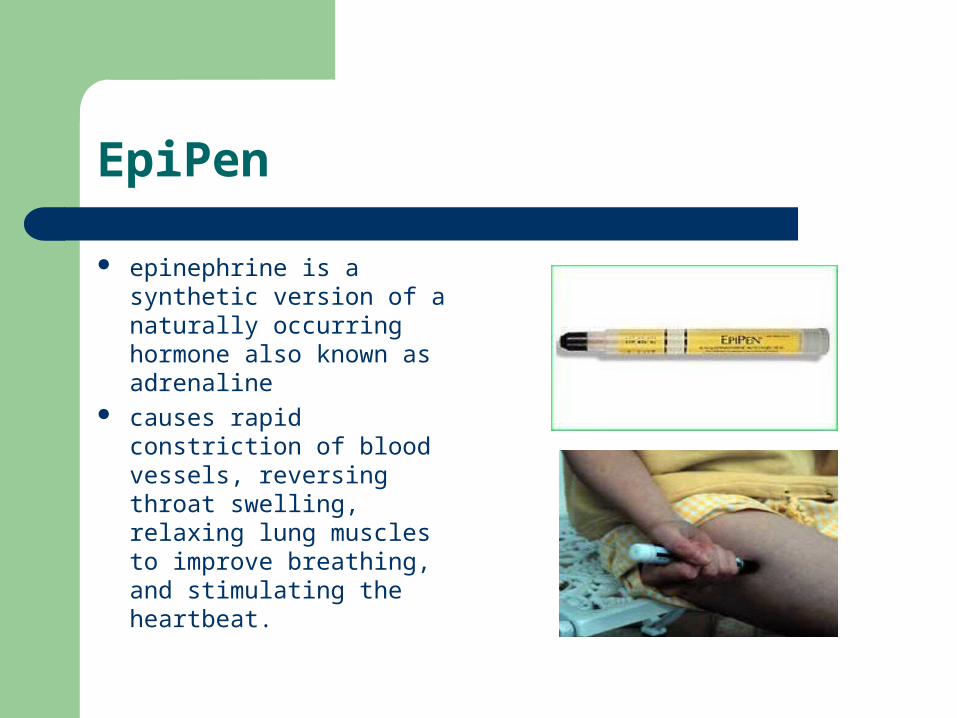
EpiPen
epinephrine is a synthetic version of a naturally occurring hormone also known as adrenaline
causes rapid constriction of blood vessels, reversing throat swelling, relaxing lung muscles to improve breathing, and stimulating the heartbeat.
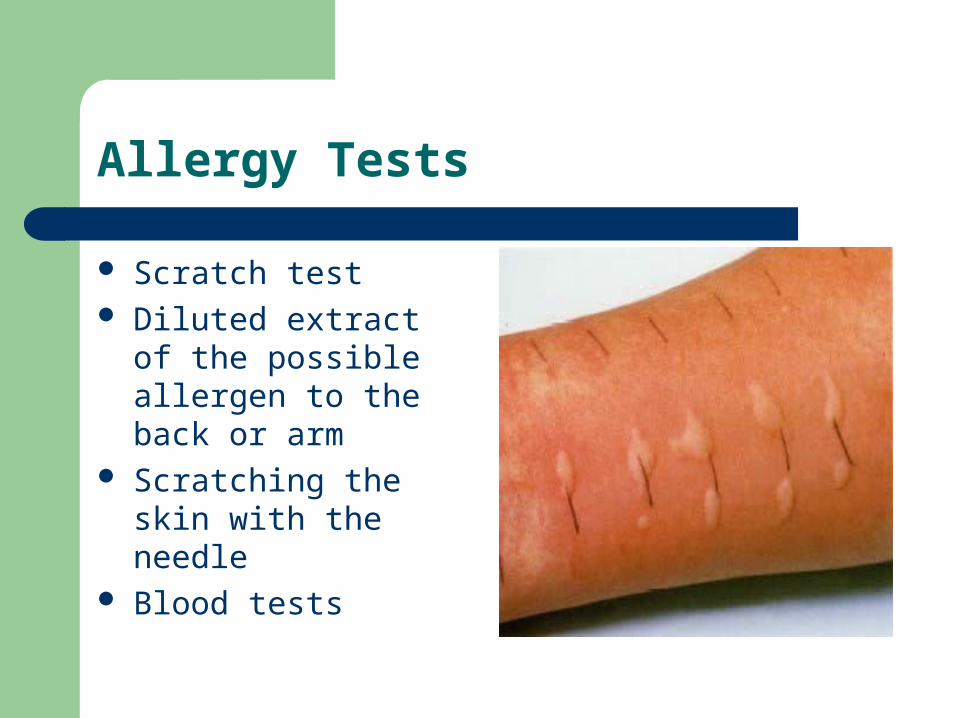
Allergy Tests
Scratch test Diluted extract of the
possible allergen to the back or arm
Scratching the skin with the needle
Blood tests
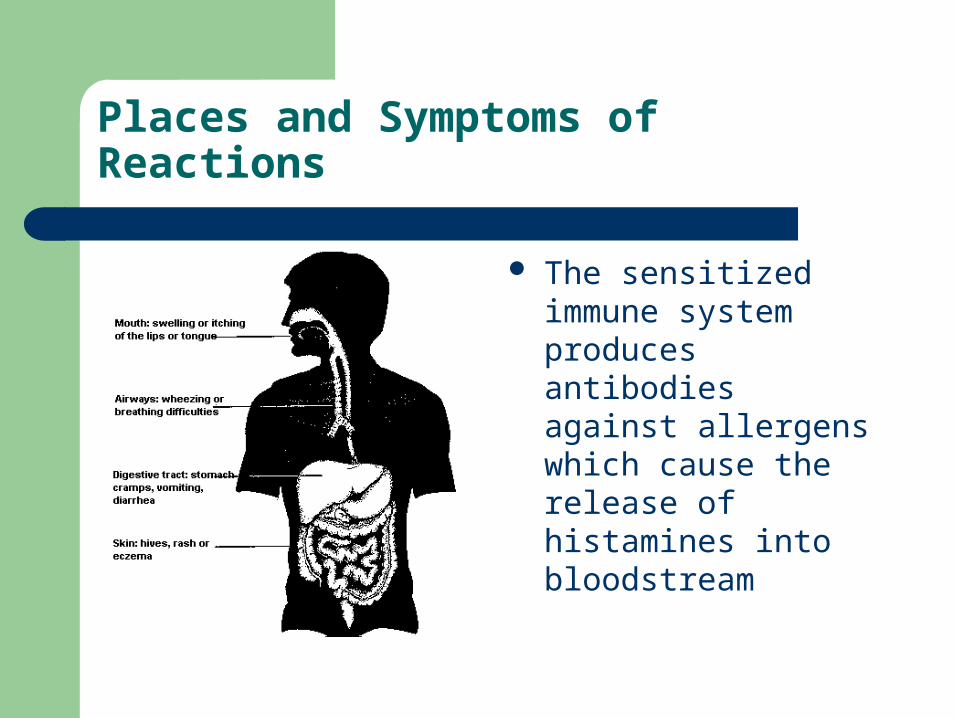
Places and Symptoms of Reactions
The sensitized immune system produces antibodies against allergens which cause the release of histamines into bloodstream
Treatments
Avoidance Medication Immunotheraphy The injections help the immune system to
produce fewer IgE antibodies, while also stimulating the production of a blocking antibody IgG
Drug Desensitization
Drug Desensitization allows safe delivery of an antibiotic to a patient which has an IgE medicated sensitivity to the drug by administering it in small doses until a full therapeutic dose is clinically tolerated
The procedure entails risk of acute allergic reactions, including death
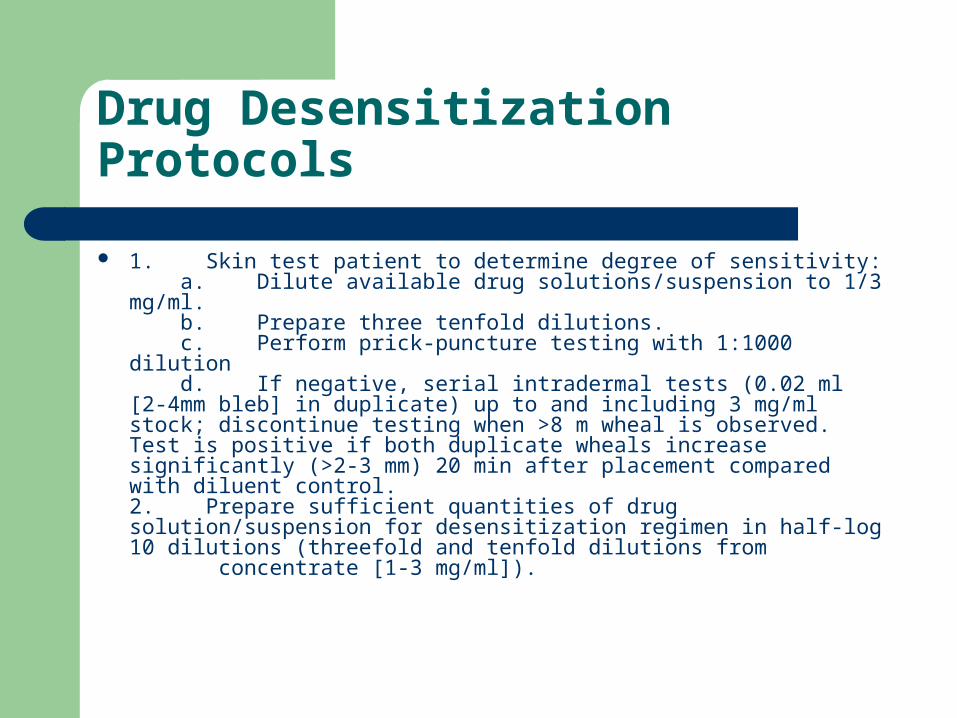
Drug Desensitization Protocols
1. Skin test patient to determine degree of sensitivity: a. Dilute available drug solutions/suspension to 1/3 mg/ml. b. Prepare three tenfold dilutions. c. Perform prick-puncture testing with 1:1000 dilution d. If negative, serial intradermal tests (0.02 ml [2-4mm bleb] in duplicate) up to and including 3 mg/ml stock; discontinue testing when >8 m wheal is observed. Test is positive if both duplicate wheals increase significantly (>2-3 mm) 20 min after placement compared with diluent control.2. Prepare sufficient quantities of drug solution/suspension for desensitization regimen in half-log 10 dilutions (threefold and tenfold dilutions from concentrate [1-3 mg/ml]).
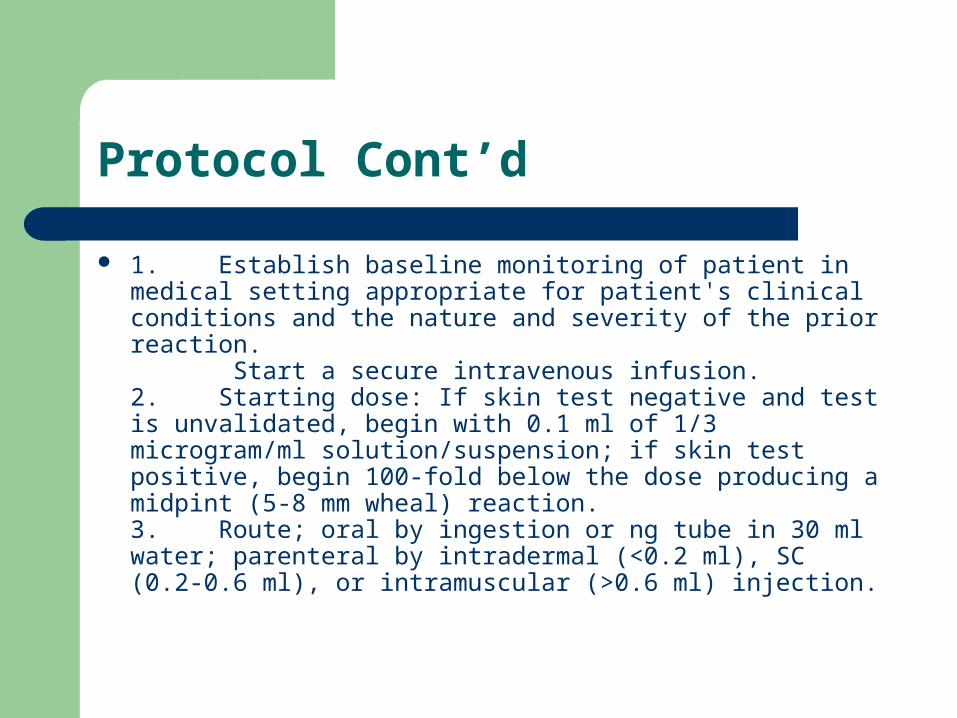
Protocol Cont’d
1. Establish baseline monitoring of patient in medical setting appropriate for patient's clinical conditions and the nature and severity of the prior reaction. Start a secure intravenous infusion.2. Starting dose: If skin test negative and test is unvalidated, begin with 0.1 ml of 1/3 microgram/ml solution/suspension; if skin test positive, begin 100-fold below the dose producing a midpint (5-8 mm wheal) reaction.3. Route; oral by ingestion or ng tube in 30 ml water; parenteral by intradermal (<0.2 ml), SC (0.2-0.6 ml), or intramuscular (>0.6 ml) injection.
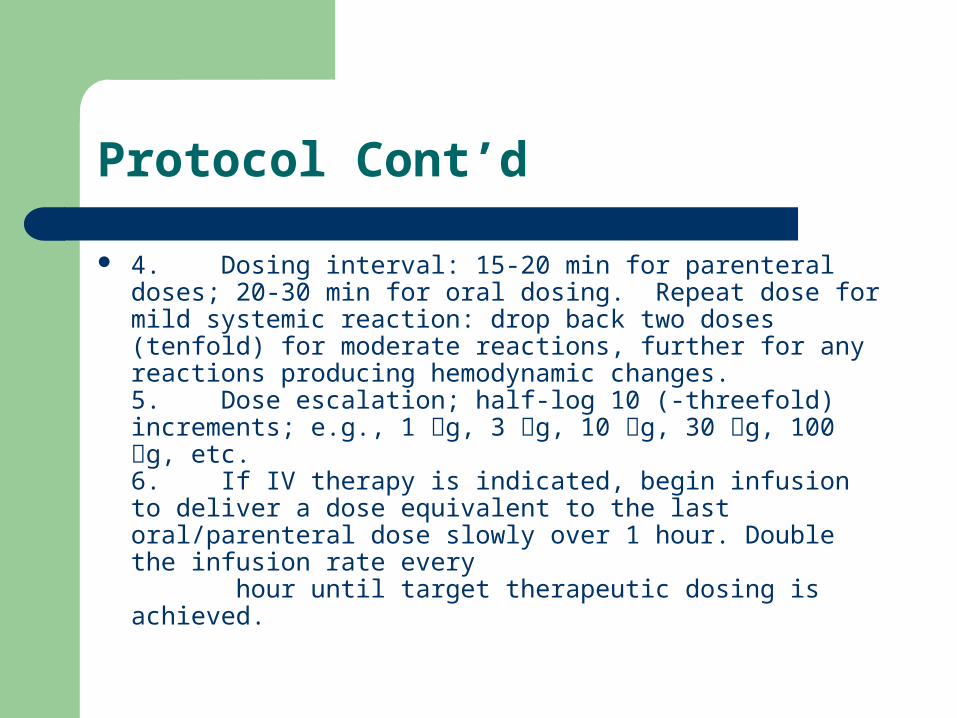
Protocol Cont’d
4. Dosing interval: 15-20 min for parenteral doses; 20-30 min for oral dosing. Repeat dose for mild systemic reaction: drop back two doses (tenfold) for moderate reactions, further for any reactions producing hemodynamic changes.5. Dose escalation; half-log 10 (-threefold) increments; e.g., 1 g, 3 g, 10 g, 30 g, 100 g, etc.6. If IV therapy is indicated, begin infusion to deliver a dose equivalent to the last oral/parenteral dose slowly over 1 hour. Double the infusion rate every hour until target therapeutic dosing is achieved.
Penicillin Drug Desensitization
Background: – A 32 year old female is pregnant and is
diagnosed with syphilis – Penicillin is the ideal antibiotic to treating – The mother is allergic to penicillin – Her obstetric history included one vaginal delivery
at term and four subsequent spontaneous abortions at 12 to 16 weeks.
Bibliography
.Sullivan TJ. Drug Allergy. In: Midleton E, Jr. ed. Allergy, principles, and practice. 4th ed. St. Louis: CV Mobsby Co, 1993: 1725-1746
.Ohman JL, Jr. Clinical and immunologic responses to immunotherapy. In: Lockey RF, Bukantz SC, eds. Allergen immunotheraPY. New York: Marcel Decker, Inc, 1991: 209-232
.Yunginger JW. Insect Allergy. In: Midleton E, Jr, ed. Allergy, principles, and practice. 4th ed. St. Louis: CV Mobsby Co, 1993: 1511-1514
.Patterson R, De Swarte RD, Greenberger PA, et al. Drug Allergy and protocols for mangement of drug allegies. N Engl Reg Allergy Proc 1986; 7: 325.
.In: The extra pharmacopoeia. 29th ed. London: The Pharmaceutical Press, 1989, 1189-1195
.Monaghan MS, Glasco G, et al. Safe administration of iron dextran to patient who reacted to the test dose. South Med J 1994: 87(10): 1010-1012
.Fishbane S, Ungureanu VD, Maesaka JK, et al. The Safety if intravenous iron dextran in hemodialysis patients. Am J Kidney Dis 1996: 28(4): 529-534
.Novey HS, Pahl M, Haydik Y, Vaziri ND, Immunologic studies of anaphylaxis to iron destran in patients on renal dialysis. Ann Allergy 1994; 72(3): 224-228
.Patterson R, De Swarte RD, Greenberger PA, et al. Drug Allergy and protocols for managements to drug allergies. Allergy Proc (Spanish edition) 1995;9(2):13
.Bridges KR, Bunn HF. Anemias with distributed iron metabolism. In: Isselbacher KJ, Braunwald E, Wilson JD, et al, eds. Harrison’s. Principles of internal medicine. 13th ed. McGraw-Hill, 1994; 1721-1723
.Patterson R, De Swarte RD, Greenberger PA, et al. Drug Allergy and protocols for managements to drug Allergies. N Engl Reg Allergy Proc 1986; 7: 325-342
.Sullivan TJ, Yecies LD, Shats GS, et al. Desensitization of patients allergic to penicillin using orally administered beta-lactam antibiotics. J Allergy Clin Immunol 1982; 69:275-282
.Stark BJ, Earl HS, Gross GN, et al. Acute and chronic desensitization of penicillin. J Aallergy Clin Immunol 1987; 79: 523-532
Special Thanks to:
Harlem Children Society Dr. Sat Dr.Mary Lee-Wong Beth Israel Medical Center