vol. 28, no. 2. pp. 163-174 nurse staffing and ... · nurse staffing and healthcare outcomes 165 us...
TRANSCRIPT
Advances tn Nursing ScienceVol. 28, No. 2. pp. 163-174© 2005 Uppincotl Williams &. VPiikins. Inc.
Nurse Staffing and •Healthcare OutcomesA Systematic Review of theInternational Research Evidence
Annette J. Lankshear, PhD; Trevor A. SheUion, DSc; •:Alan Maynard, BPhil
The relationship between quality of care and the cost of the nursing workforce is of concern topolicymakers. Ihis study assesses the evidence for a relationship between the nursing work-force and patient outcomes in the acute sector through a systematic review of internationalresearch produced since 1990 involving actite hospitals and adjusting for case mix. Twenty-two large studies of variable quality were included. They strongly suggest that higher nursestaffing and richer skill mix (especially of registered nurses) are associated with improved pa-tient outcomes, although the effeet size cannot lie estimated reliably. The association appearsto show diminishing marginal ixrturns. Key words; fiiiitire to resme, mortality, outcomes,quality nursing care, research metbods, skill mix, staffing, systematic retiew, ivorkforce
BACKGROUTO)
Healthcare systems are struggling to con-trol costs and improve the quality and safetyof care. Given that a high proportion ofhealthcare expenditure is on staffing, par-ticularly nursing, there is considerable inter-est in seeing how this resource contributesto patient outcomes. In some parts of theworld, greater investment iti qualified nursesis part of a strategy to improve quality of care,whereas in other areas policymakers are seek-ing to substitute qualified nursing workforce
From the l^partment of Healtb Sciences, Universityof York. York, Enghind.
Tbe autlvirs acknowledge the support of tlje fi>llow-ing wbo contributed to searcbing for, and analysis of,the [Hipers tn the wview: Karen Smith. HSc; CatherineHewitt. MSc; Professor .Martin Hland. PhD. This reviewwas carried out on hebalf of the Chief Nursing Officerof England and funded by the Department of Healtbi'olicy Researcb Program and tije NIIS Service Delii'eryand Organisation (SDO) R&D Program.
Corresponding autimr Annette J Lankshear. PhD. De-partment of Health Sciences, Uniivrsity of York. See-bobm Rownttve Building, Heslington Road, York YOlO4LG, England (e-maii: [email protected]).
numbers with less expensive assistive staif.There is cotisiderable research capable of in-forming this debate but it is often selectivelyquoted to support arguments. In tliis article,we report on a systematic review of the in-ternational research on tbe relationsbip be-tween the nursing workforce (level and skillmix) and patient outcomes (including mor-tality, failure-to-rescue, and complications) inthe acute sector and consider its relevance forpolicy.
METHODS ,
We carried out a systematic review of theliterature' and a policy analysis and con-ducted interviews with key researchers in thefield in both the United States and the UnitedKingdom. .
Search strategy
The aim was to retrieve research on nursestaffing and healthcare outcomes publishedsince 1990. We searched a combination ofelectronic databases, Internet, and organiza-tional Web sites, and contacted researchers
163
164 ADVANCES IN NURSING SCIENCH/APRIL-JLINE 2005
and other experts. The following electronicdatabases were searched in March 2004 from1990: Medline, C:inahl, EMBASE, PsycINFO,HMIC (including DH Data, King's Fund, andHELMIS), SICiLE, Coclirane Library, BritisbNursing Index, ;md NLM Gateway Web ofKnowledge. Relevant "grey" literature wasidentified (ie, produced by government, aca-demics, or business in print and electronic for-mats, but not controlled by commercial pub-lishers) by searching organizational Web sitessuch as the American Ntirses Association,Agency for Healthcare Research and Qual-ity; Australian Resource Centre for HealthcareInnovations, Audit Commission, UK Depart-ment of Health, International Association ofHealth Policy, Royal College of Nursing andWorid Healtb Organization.
Multiple terms are used internationally todescribe qualified nurses and nursing sui>port staff, so synonyms were retrieved byidentifying key authors, selecting their arti-cles using agreed criteria, and acquiring themto check their search terms and strategies.Search terms were adjusted to take into ac-count tbose listed in the thesaurus of Chedatabases searched. MeSH terms were usedwhere possible. •';
Inclusion and exclusion criteria
We included empirical research, publishedsince 1990 in any language, on the rela-tionship between nurse staffing and one ormore of the following patient outcomes:mortality rate, complication rate (pneumo-nia, urinary tract infections, nosocomial itifec-tions, wound infections), failure-to-rescue, in-cidence of adverse events (falls, medicationerrors), length of stay, or patient satisfaction.Observational studies were included if theyhad adjusted for case mix and hospital char-acteristics. Purely qualitative studies were ex-cluded, as were those undertaken in a singleward or unit.
Study quality and assessment
For each relevant study, data were ex-tracted systematically using a predesigned ta-
ble to describe the type and feature of theworkforce, the setting, the outc<>me(s), themethods used, the results found, tbe qualityof the studies, and tbe limitations. One re-viewer abstracted each study and a samplewas checked.
Analysis '
Studies report different outcomes and usedifferent measures of staffing and ways ofsummarizing the association between staffingand outcome. Because of the heterogeneity,we were not able to conduct a formal meta-analysis of the results.' Instead, we carried outa more qualitative synthesis to explore pat-terns in the data and possible explanationsfor inconsistencies such as study design, anal-ysis, context, and setting." To aid analysis andcomparison, we attempted to impose a com-mon measure of staffing level/skill mix. Some.studies use hotirs per patient clay (HPPD) asa staffing measure '*—the average total num-ber of patients in hospital divided by the to-tal number of nursing hours of staff on duty.Where this includes only productive hours, itmay be termed worked hours per patient day(WHPPD). We converted tbe results of studiestbat did not use HPPD to a common currencyof converted hours per patient day (CHPPD)where possible.
Another commonly used measure is theNurse-to-patient ratio—the number of pa-tients for wbom one nurse has direct respon-sibility at any one time. This ratio may re-late to RNs alone or to RNs and LPN/I,VNs,together known as "licensed nurses."Figuresseldom include unlicensed assistive person-nel. To convert a nurse-to-patient ratio tohours per patient day, tbe number of patientsassigned to an RN is converted to a 24-hourday, so a 1:4 ratio becomes 24/4 = 6 CHPPD.Full-time equit'alentsAhc number of futi-ximeemployees, may or may not include staff onmaternity/sick leave and may include clini-cal nurse specialists and managers without di-rect responsibility for patient care. One FTEis approximately equal to 2080 hours paid or1920 worked after allowing for 4 weeks" an-nual leave. We have used the lower figure for

Nurse Staffing and Healthcare Outcomes 165
US studies, so the conversion is as follows:CHPPD = (FTEs X 1920)/(patient census x365).
RESULTS
A total of 8644 nonduplicate referenceswere downloaded. The title and abstractswere then scanned for relevance and iden-tified for retrieval using preagreed criteria.Four hundred twenty-two references were se-lected, retrieved, and recorded. After the ap-plication of the inclusion and exclusion cri-teria, 61 studies were identified, 38 of wliichdealt with acute general hospitals. Of these,22 studies were multisite and attempted to ad-just for case mix."'"' "'
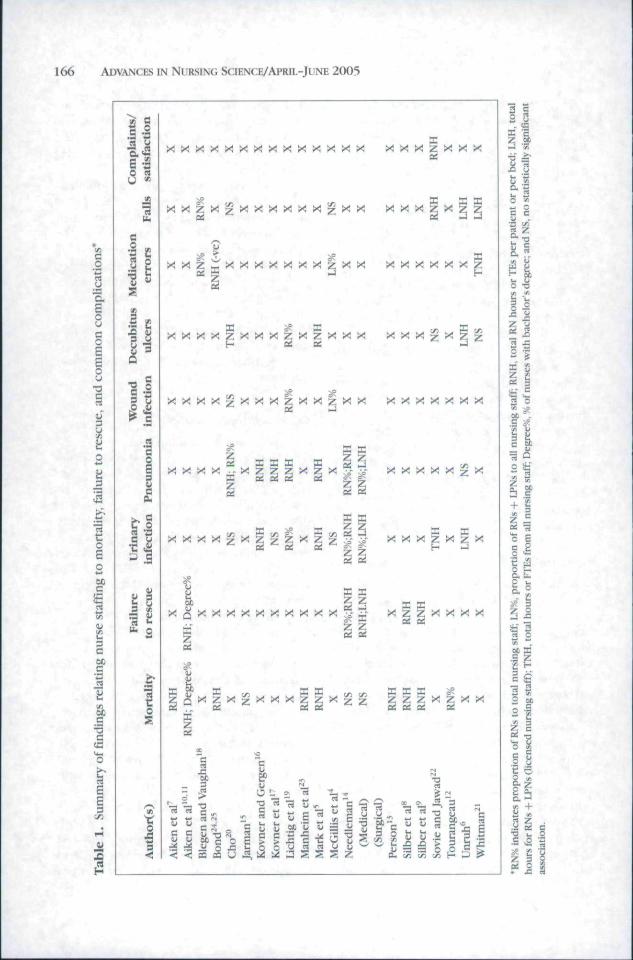
Their results are summarized in Table 1as 20 sets of studies because 4 articles arere/subana!yses of 2 studies. "*"-^'^'* Table 2shows the mean and range of staffmg levelsin those large studies that have used mea-surements that can be expressed as CHPPD(column 5) although these should be treatedwith caution. Column 6 records the main as-sociations between RN staffing and patientoutcomes.
Longitudinal studies
Mark et aP analyzed data submitted by 422hospitals (in 11 US states) to the HealthcareCost and Utilization Project National Inpa-tient Sample. In-hospital mortality, decubitusulcers, pneumonia, and urinary tract infec-tions were examined against staffing data sub-mitted to the American Hospitals Association(AHA) database. Hospital characteristics wereadjusted for technology, market data, and cal-endar year. Patient risk adjustment was car-ried out by means of Mcdstat's Disease Stagingmethodology and complications-of-care soft-ware. The longitudinal design took accountof unknown variables by comparing hospitalswith their own performance in previous yearsand allowing for "feedback effects" (such ashigli monality in 1 year leading to increasedstaffmg in the next). The authors found thatan increase in RN staffing levels was associ-
ated with reduced rates of pneumonia, uri-nary tract infections decubitus ulcers, andmortality'. Interestingly, the size of the effectdecreased the greater the base level of staffing(Table 2).
In the only other risk-adjusted longitudi-nal study, Unruh explored the effect of RNand LPN staffing in 211 Pennsylvania hospi-tals from 1991 to 1997 to determine whetherthere was a correlation with complicationrates.** During the 7 years, Mediqual-basedpatient acuity-adjusted nurse staffing levelsfell, with a mean 33 licensed nurses per1000 adjusted patient days (CHPPD =: 6.9).Hospitals with higlier RN and LPN (licensednurse) staffing had lower incidences of atelec-tasis, decubitus ulcers, falls, and urinary tractinfections.
Cross-sectional studiesSome of the most influential work in the
field has been carried out in the Universityof Pennsylvania. The 1988 study of Aikenet al reported a lower 30-day case mix ad-justed mortality rates in 39 Magnet hospitalsthan in a matched sample of 195 non-Magnethospitals.^ The RN staffmg was 1.6 per pa-tient (CHPPD = 8.4) in Magnet hospitals asopposed to 1.2 for controls (CHPPD - 6.3)although the authors attributed this to differ-ences in organizational culture.
Silber et al," using data from 73,737 pa-tients in 147 hospitals in 1991 and 1992,found that after adjusting for case mix andother factors, liigher ratios of nurses perbed were associated with both lower mor-tality and lower failure-to-rescue (mortalityamongst patients who developed complica-tions). In a later study, using a data set con-sisting of all Medicare patients having gen-eral or orthopedic surgery between 1991 and1994, they again found that hospitals withhigher RN/bed ratios were consistently associ-ated with reduced death and failure-to-rescue
Aiken et al'" analyzed 3()-day mortality andfailure-to-rescue (defined here as 30-day mor-tality among rates patients with complications
166 ADVANCES IN NURSING SCIENCE/APRIL-JUNE 2005
X X X "Z X X X
X X x z x
X X X X X X
xxxxzxxx x xxx X X X
XXXX^XXXZXX^XX X X X X X X X
X Z X -^^ ^ X X X X X
e f i o i
X X , . un wiX Z Z X X

Nurse Staffing and Healthcare Outcomes 167
re
a.
.3
c 5
^
-r t-
II
— r.- —r-i d rf
Tlu£
radj
i
ua u
62c
1;>
C
Dni
o
CL.
£
u
helo
™

168 ADVANCES IN NURSING SCIENCE/APRIL-JUNE 2005
plus deaths without a recorded compli-cation) in 232,342 patients who had un-dergone common general, orthopedic, andvascular surgical procedures in 168 acute hos-pitals. Nurse staffmg data and nursing out-comes were derived from a survey of 50% ofRNs registered and working in Pennsylvaniain 1999. They reported a significant inverserelationship hetween nurse staffing and bothmortality and failure-torescue, after control-ling thoroughly for hospital and patient char-acteristics. However, hecause of the way thestaffing data were collected, the nursing staffratios derived at a hospital level may not ap-ply to the units from which the patient datawere collected. The methodology has sincebeen repeated in England, Scotland, Canada,and Germany, and results are expectedimminently.
Aiken et a! later reanalyzed these data andalso found that after adjusting for patient char-acteristics, hospital structural characteristics,and tbe spiffing levels, the odds of mortal-ity and failure-to-rescue after surgery were re-duced in settings with a higher proportionof nurses educated to at least a baccalaure-ate degree (odds ratio = 0.95; 95% confidenceinterval ICI], 0.91-0.99)." As before, we donot know the educational level of the actualnurses who cared for the patients in the study.
Tourangeau et al investigated the effectsof nursing-related variables on risk-adjusted30-day mortality rates for hospitalized pa-tients with a diagnosis of acute myocar-dial infarction, stroke, pneumonia, or septi-caemia, using data from nearly 4000 nursesand 46,94! patients discharged from 75 hospi-tals in Ontario.'^ After adjusting for case mixand patient care need, they found tbat a richerskill mix of RNs was associated with lower30<lay mortality whereas the total amount ofnurse staffing was not. Overall, a 10% increasein the proportion of RNs across all hospitaltypes was associated with a 0.5% point reduc-tion in mortality.
The study of 200,000 acute myocardial in-farction patients in over 4(K)0 US hospitals'^used a sophisticated series of statistical mod-els on the Cooperative Cardiovascular Project
data set (collected from patient charts bytrained reviewers) for case mix and hospitalcharacteristics adjustment. They foxmd thatmortality for patients treated in high RN (lowLPN) environments was lower than that forpatients treated in low RN (high LPN) envi-ronments. However, as with the Pennsylvaniastudies, the staffing data related to the wholehospital, nither than the unit in which the pa-tients were nursed.
Needleman et al used administrative datafor 799 hospitals in 11 US states (represent-ing 26% of all LIS hospitals) to examine the re-lationship between the amount of care pro-vided hy nurses at tbe hospital and variousnurse-sensitive patient outcomes.'* Amongmedical patients, a higher proportion of careprovided by registered nurses and/or moreRN hours per day correlated with a reduc-tion in urinary tract infections, pneumonia,length of stay, upper gastn>intestinai bleed-ing, shock, and failure-to-rescue (using a re-stricted set of complications). Among surgicalpatients, a bigbcr proportion of RN hours andhigher numbers of licensed nurse (RN -I- LPN)hours was strongly associated with a lower(iulure-to-rescue rate and more weakly, butstill significantly, with lower rates of pneumonia and urinary tract infections. They foundno association with mortality.
Canadian Nursing Staff Mix Outcomesstudy of McGiliis et al examined the associa-tion between RNs, registered practical nurses(RPNs), and unlicensed staff and a range ofpatient outcomes in 19 Canadian teachinghospitals. ** The study used hierarchical mod-eling and hoth staffing and patient outcomesdata were collected at ward or unit level. Theyfound that the lower the proportion of RN andRPNs on tbe unit and the less experiencedthe nurses, the higher the nimiher of medica-tion errors and wound infections. They alsofound a positive association between the proportion of regulated staff (RNs and RPNs) ontbe unit and patient activities of daily livingand social functioning, which disappeared at6-week follow-up.
Jarman analyzed the records of 8 mil-lion patients discharged from English public

Nurse Staffing and Healtbcare Outcomes 169
hospitals during 1991-1995.''' Inpatient mor-tality was inversely related to the number ofhospital doctors per hospital bed, the ratio ofdoctors to population, and a high percentageof lower gnide nursing assistants. This study,although similar in design to those describedabove from North America, suffers from thelack of good case mix data held routinely bythe UK National Health Service.
Kovner and (iergen examined the relation-ship between nurse staffing levels and a ningeof postsurgical adverse events sensitive tonursing care in 506 US hospitals in 1993. 'Using Medicare risk-adjustment and control-ling for hospital characteristics, they reporteda negative correlation between RN FTEs peradjusted inpatient day and urinary tract itifec-tion, pneumonia, thrombosis, and pulmonarycompromise. However, when they repeatedthe analysis, using data in 530-570 hospitalsfor 1990 to 1996, they found a statisticallysignificant association only for pneumonia.''Ihc study was unusual in also examin-ing doctor hotirs, uncovering a positiveassociation between resident/intern HPPDand all adverse events except urinary tractinfections.
Blegen and Vaughan studied 39 medical,surgical units and intensive care units in 11hospitals, all of which routinely submitted ad-verse event data to the Institute for QualityHealthcare.'** Using case-mix-adjusted datafrom 1993 to 1995, they found a significantinverse relationship between the proportionof RNs and medication administration errorsand patient tails. As tbe RN proportion var-ied from 50%i to 85%, the rate of medicationerrors decreased but above this, the effectdisappeared.
Lichtig et al and Knauf et al reportedthe results of the American Nursing Associa-tion's''^"*' study in 3 US states, examiningthe outcomes related to all nursing staff perpatient day, which ranged from 6.95 HPPDin New York in 1992 to 10.18 HPPD in(California in 1994, with RN percentages rang-ing from 56.7 to 77.3, respectively. Theyfound that, for California and New York, pres-sure ulcers, pneumonia, urinary tract infec-
tion, and postoperative infections were in-versely significantly related to RN skill-mixand, to a lesser extent, higher nursing hoursper acuity-adjusted patient day. The authorsreported that the Massachusetts data weresignificantly poorer and no significant rela-tionship emerged.-'' Cho et al in their studyof 124,204 patients in 232 Californian hos-pitals also fotmd that as RN hours and RNproportion increased, the rate of pneutnoniadropped, but not pressure ulcers, UTIs, orwound infections.^"
Whitman et al examined staffing and out-comes in 1999 in 95 patient care units across10 hospitals in the Eastern United States.^'Data for central tine infection rates came frommonthly surveillance and pressure ulcer datafrom a monthly systemwide, prevalence studyconducted on all units. Medication errors andfalls data were retrieved from hospital riskmanagement reports. No statistical relation-ship was found between .staffing, pressure ul-cer rates, and rates of central line Infection. Incardiac intermediate care units, higher hoursworked per patient day was associated withfewer falls. Medication error rates were higherin ecu and noncardiac intermediate unitswhen staffing levels were lower. Tbe mean forhours worked per patient day (including theunit secretary and manager) in this study wassaid to be low (4 WHPPD for medical and sur-gical; 8.4-8.9 for intermediate care).
Sovie and Jawad^^ investigated both theimpact of restructuring on the organizationand delivery of patient care and that of nurs-ing structure and processes on the incidenceof falls, nosocomial infections, pressure ul-cers, and urinary tract infections. Examiningdata from 29 university hospitals more than2 years, they found that that increased RNhours worked per patient per day was asso-ciated with lower fall rates although thesewere "minimal" when the levels reached 6RN HPPD. Higher patient satisfaction levelswere seen when RN hours worked per pa-tient day increased from 4-4.5 to the 5-6hour range. Lower urinary tract infection rateswere also associated with an overall rise innurse staffing niunhers.
170 ADVANCES IN NURSING SCIENCE/APRIL-JUNE 2005
Manheim et a!, using Health Care Financ-ing Administration (HCFA) data from 1987 in3796 hospitals, found that as the percentageof board-certified doctors and the percentageor number of RNs per adjusted adtnission in-creased, so the mortality rates decreased.^^Bond et al studied full-time staffing ratios peroccupied bed, using HCFA and AHA data from1992 in 3762 US hospitals, and found a neg-ative correlation between tbe mortality rateand the number of RNs and a positive relation-sbip with LPNs per occupied bed." * Using thesame data in a subset of 1116 bospitals. Bondet a! also explored medication errors from thenational clinical pharmacy services databasesurvey. '' Tbey found that as the number ofRNs and the ratio of RNs to LPN/LVNs in-creased so did the number of medication er-rors altbougb tbese calculations did not allowtor the number of drugs administered.^''
DISCUSSION
This systematic review of research on therelationship between nursing staffing and pa-tient outcomes in general acute settings iden-tified 61 studies, 38 of which dealt with acutegeneral hospitals and were published since1990. Many of these studies were of poor qual-it>', using data from only 1 unit or hospital orfailing to control for case mix variations. The22 studies discussed in this article were themost robust but are still of variable method-ological quality using a range of designs andsettings and measuring a variety of differentstaffing inputs and patient outcomes. Here wediscuss the pattern of results and how thesemight be affected by study design and quality.
Ideally, one would look for rigorous ran-domized trials or qtiasi-experimental meth-ods accompanied by rich qualitative organiza-tional research to evaluate whether and howchanges in the level of the nurse staffing influ-ences patient outcomes. We did not find anysuch research. The majority of the research iscross-sectional, relying on the analysis of datafrom groups of hospitals or large public ad-ministrative data sets to identiiy correlationsbetween one measure (eg, ntu-se staffing) and
a second measure (eg, mortality). Althoughthese studies are likely to be generalizablebecause of the size and representative na-ture of the patient data analyzed, they hadweaknesses.
Accuracy and completenessof staffing data
Many studies obtained staffing data fromthe AHA, which do not distinguish betweenRNs involved in direct care and those em-ployed by the hospital in indirect or man-agement roles. The distribution of RN rolesin hospitals with similar AHA-recorded RNstaffing levels may be different with someproviding more direct patient care. Moreover,the AHA staffing data reflect paid hours andso overestimate productive hours. Finally, inmany of the studies, the data on staffingis taken from the hospital as a wbole'^'^rather than accurately reflecting the staffingon the units/wards from which patient datawere collected.^ This may result in (prob-ably random) error in the measurement ofnurse staffing and a reduction in the estimatedeffect.
Ad|ustnient for confounding
Most of the large cross-sectional studies ad-just t<)r case mix hy using data derived fromadministrative systems such as Mediqual orMedstat's disease staging. This is better thanthe rather poorer data Jarman acquired fromthe English NHS,''' but not as good as thoseobtainahle from clinical databases such as thatcollected as part of the C^ooperative Cardio-vascular Project.'^ The importance of adjust-ment is illustrated by results presented in thestudy of Aiken et al in surgical patients.'" Tlieunadjusted odds ratio of dj'ing of a unit in-crease in the number of patients cared for pernurse was 1.14; after adjusting for patient casemix, it was 1.09 and fell further after adjust-ment for hospital characteristics to 1.07 (95%Cl: 1.03-1.12). Not only does this show howconfounding can result in an overestimationof the effect of staffing but also shows that theeffect size is sufficiently small as to be due to

Nurse Staffing and Healthcare Outcomes 171
residual confounding. However, studies withbetter case mix adjustment such as Person'^and Toiirangeau'^ also showed significant as-sociations between nurse staffing level andmortality. Therefore, it is unlikely that thereported associations are entirely due toconfounding.
Studies also varied in their adjustment forhospital characteristics (eg, rural/urban, own-ership, mergers, and capacity utilization, tech-nology, teaching status, patient volume). OnlyMcGillis* used a multilevel modelling ap-proach for analyzing such hierarchical data.One major weakness in most of the studies isthe omission of data about doctors. It is pos-sible, for example, that hospitals with higherlevels of nursing staff also have more andbetter qualified doctors. In the United King-dom, for example, Jarman found that doc-tors were the most important professionalgroup associated with reductions in mortal-ity. Although most North American studiestook hospital teaching status into account,only a few looked at doctors specifically andthey found that the numher of residents/interns,"' the level of training of doctors,"^"and numher^ or percentage of board-certifiedsuhspecialists-^ contributed to explainingvariations in patient outcomes. However, theyall found that the effect of nurse staffing wasover and above any association with medi-cal staffing. Thus, although the estimates ofthe effect size of nurse input may be wrong,the effect itself is unlikely lo be due to thisomission.
In the ahsence of experimental research,which would be less susceptible to confound-ing tban observational studies, the most ro-bust design is longitudinal. If the effect ofnurse staffing is real, patient outcomes shouldchange in relation to variations in nursestaffing over time. Because hospitals can actas their own controls over time in longitudinalstudies, attribution of causality is also easier.We identified 2 longitudinal studies both ofwhich found that increases in RN input overtime was correlated with reductions in the in-patient mortality rate^ and patient complica-tions (UTIs, pressure ulcers, and falls).
Despite the variability in the quality of thestudies, there is a consistent pattern of results.Nine large acute studies foimd a significant in-verse relationship between RN staffing levelsand mortality rates (Table 1)5.7-10.12,13.23.24
Four studies also found negative associationsbetween nurse staffing and failure to rescue(variably defined).*^- '*'' Only Jarman'"^ inthe United Kingdom failed to find a signif-icant correlation between nursing numbersand any measure of mortality (including fail-ure to rescue), although he did establish a pos-itive relationship between low-grade nursesand mortality.
The pattern of association between thenursing worktbrce and complications isslightly less consistent. Seven of 8 studiesshowed a positive association between RNor LN hours or RN proportion and pneumo-j^ja 5.14.16.17.19.20.22 - j^g ^^^^^^ ^ f ^H the stud-
ies that examined the fol!owing outcomesalso found a link between nurse staffing andurinary tract infections,'''*'- '*-' ' ' ' decubi-tus ulcers,'*'''^-^'' fa!ls.* '« '' ^ and woundinfections."*' It is possible that this reflectsthe poorer reporting of patient complicationsother than death and pneumonia. There doesnot appear to be anything distinctive aboutthe studies that did not find a relationshipwith these complications and they all foundassociations with at least some outcomes.
The possibility of publication bias has tohe considered, especially with regard to thesmaller studies, where there may be a ten-dency to publish selectively those studies thatfound a significant positive association. How-ever, tbe estimates of association do not varyby study size and so this is unlikely to beimportant.'
Skill mixIt appears from many of the studies that
the relationship between nurse staffing andpatient outcomes is associated more withRN staffing levels and the proportion of RNsin the total staff mix. In acute settings, to-tal staffing and LPN staffing tend not todemonstrate a link with improved outcomes.

172 ADVANCES IN NURSING SCIENCE/APRIL-JUNE 2005
Needleman et al'^ found that high num-bers of licensed practical/vocational nurses(LPN/I,VNs) in the United States correlatedwith higher levels of complications. Unnihpointed out that this may be due to the ten-dency to use LPNs to replace RNs and so theirnumbers tend to be higher where RNs arelower.'' In Canada, McGillis found that a mix-ture of RNs and aides gave better outcomesthan when second-level practical nurses wereincluded in the staffing mix.* Tliis was alsofound in a UK prospective study using directobservation of nursing activity which foundthat the quality of nursing care improvedas the ratio of qualified and fLirther trainedstaff to patients increased and with increasinggrade mix.-~
Causal mechanisms
The results of our review are consistentwith, but extend, the findings of previousreviews.-""^' There is a tendency amongstsome authors to interpret the relationsbip ascausal. Although this is more convincing inthe longitudinal studies, other factors may beoperating in cross-sectional studies such asnurses being attracted to hospitiils with bet-ter outcomes or nurses favoring jobs in "bet-ter" areas. Ho^vever, tbe weight of evidencefrom different studies hy time and place andmethod is strongly suggestive.
Fundamental nursing care is often referredto as "basic" ft>r much of what nurses doappears deceptively simple. However, it isduring these "basic" tasks that a complexinteraction occurs—nurses assess patients'physical and psychological .status and patientstalk to, and receive information from, nurses.Tbis can be important in detecting early signsof clinical deterioration•^•^ or complications.^^If the nursing resource is stretched because ofcontextual factors (geograpbical disposition,decreased skill mix, increased patient depen-dency, and unit activity) then the ability toprovide proactive care, cope with the unpre-dictable, and maintain flexibility can be ad-versely affected. "* Where RN ratios are lower,much of the frontline care may be given hy
less qualified and less empowered staff Inaddition, noting deterioration does not of it-self improve outcomes and, having decidedthat an intervention is needed, a nurse mayneed to persuade medical staff to attend thepatient. This requires nurses to be able topresent the case logically and confidently;prompt attendance by medical staff is morelikely if the doctor called has respiect for thenurse.
This may also explain why the Englishstudy'^ (and others that did not meet our en-try criteria) found less evidence for an asso-ciation between nurse st:iffing and mortalitythan those in North America. In the UnitedStates, there is more emphasis on forma! as-sessment ofthe patient s condition by nurses.Nurses are often expected to undertake a fullphysical assessment ofthe patients for whomthey are responsible at the commencement ofeach shift, including where appropriate, aus-cultation ofthe chest, not routinely practicedin the United Kingdom. The US hospitals alsodo not generally have the 24-hour cover byonsite doctors, as is tbe case in most acute fa-cilities in the United Kingdom, a luxury thatmay diminish with the introduction ofthe Eu-ropean Working Time Directive and the con-sequent reduction in hours worked by juniormedical staff.
Interestingly, 2 studies reported tbat the re-lationship between increasing nursing levelsand improved outcomes tailed off at higherRN levels'* or percentage'^ (see Table 2). Sucha curvilinear relationship indicating diminish-ing marginal returns to increased RN levelsand skill mix has more face validity than thelinear relationship as.sumed in most studiesand is of considerable policy importance. Athigher RN levels, these staff probably increas-ingly carry out tbe work that could he equallywell done by less qualified staff.
In the United States, the Californian Depart-ment of Health Services has set absolute min-imum ratios for licensed nurses (RNs and li-censed vocational nurses) at 1:6 (4 CHPPD),day and night f()r medical and surgical ar-eas, altbough the introduction ofthe 1:5 (4.8CHPPD) ratio has recently been postponed to

Nurse Staffing and Healthcare Outcomes 173
2008." In Australia, the state of Victoria hasrecommended that RN ratios should be 1:4/5(4.8-6 CHPPD) for day shifts in general med-ical and surgery, depending on the type ofhospital. However, the research evidence pre-sented here does not support a precise rec-ommendation on staffing levels, and the evi-dence of diminishing returns implies that thecost-effectiveness of using nurse staffing as aquality improvement lever must fall as levelsincrease. More research is needed to investi-gate the resource implications alongside theimpact on patient outcomes.
The fmdings of this review are particularlyrelevant to countries such as England thathave low levels of RN staffing relative to theratios reported here (around 1:10; 2.4 CHPPDin 1999y Proposals to dilute the skill mix bythe introduction of assistive personnel^*' maybe a false economy as the savings of reduc-ing the RN staffing mix may he more thanoffset hy the costs associated with complica-tions and adverse events. McCue et al, analyz-ing longitudinal data from 1990 to 1995. con-cluded that although hospitals experiencedincreased operating costs when they raisedRN staffing levels, there was no significantimpact on profit margins. "^ Sovie and Jawadfound that when the percentages of RNs rosefrom 40-50 to 60-70, costs per discharge fellby 3%--
Future research to estimate these relation-ships needs now to move up a level and ide-
ally should be large, longitudinal, and, wherepossible, experimental. Both staffing data andpatient outcomes should be gathered at wardor departmental level. Because these data arestructured in a hierarchical way, multilevelmodeling techniques should be used.
Associated qualitative organizational re-search is important to try and imj rove ourunderstanding ofthe causal mechanisms andelucidate what it is about the nursing workprocesses that affect patient outcomes, andhow this varies by skill mix and experience.We must now move beyond the correlationalstudies in which the attribution of causality isdifficult and wliich treat the nursing processas a black box.'Future research needs to elu-cidate the mechanisms through which nurs-ing care affects outcomes, be more tbeoreti-cally based, ^ and also consider the resourceimplications. '••
CONCLUSIONS
Overall, there is accumulating evidence ofa relationship between nurse staffing, espe-cially higher skill mix. and patient outcomes.However, the estimates of the nurse st:iffingeffects are likely to be unreliable. Tbere isemerging evidence of a curvilinear relation-ship that suggests that the cost-effcctivenessof using RN levels as a quality improvementtool will gradually become less cost-effective.
REFERENCES
1. Centre for Reviews and Dissemination. UndertakingSystematic Ret'iews of Researcb on Effectiveness.York, Pa: University of York; 2<H)1. CRD Report Nu,4.
2. Mays N, Roberts E, Poppay J. Synthesising researchevidence. In; Fulop N, Allen P. Clarke A, Black N,ed-s. Studying Organization and Delivery of HealthServices: Research Methods. London; Routledge;2000:188-220.
3. McCiillis HL. Doran D. Baker GR, ct al. The Impactof Nursing Staff Mix Models and OrganisationalChange Strategies on Patient. System, and NurseOutcomes. Toronto, Oniario, Canada; University ofToronto; 2001.
4. McGillis H, Doran D, Pink G. Nurse staffing models,nursinft hours, and patient safety outcomes. J NursAdmin. 2O()4;.^4:4l-4'>.
5. Mark BA, Harless iiW, McCue M, Xu Y A longitudinalexamination of hospital registered nurse staffmg andquality of care. HSR. 2OO4;39:279-3OI.
6. Unruh I.. Licensed nurse staffing and adverse eventsm hospiiais. Med Care. 2(K)5;41;t42-152.
7. Aiken LH, Smith HL, Lake ET. Lower medicaremortality umong a set of hospitals known Ibrgood nursing care. Med Care. I994;i2;771-787.
8. Silber JH. Rosenbaum P. Ross R. (Tomparing the con-tributions of groups of predictors: whieh outcomes
174 ADVANCES IN NURSING SctENCE/APRa-JUNE 2005
var>' with hospital rather than patient cliaracteristics.JASA. 1995;90:7-18.
9. SUber JH, Kennedy SK, EvenShoshan O, et al.Anesthesiologisi direction and patient outcomes.Anestheslolog}-. 2000:9.'^: 152-163.
10. Aiken LH. Clarke SP Sloane DM. Sochalski J, Sil-ber JH. Hospital nurse staffing and patient monal-ity, nurse burnout, and job dissatistaction. JAMA.2(M)2;288:I987-1993.
11. Aiken LH. Clarke SP Cheung RB. Sloane DM, SUberJH. Educational levels of bospital nurses and surgicalpatient mortdlity. JAMA. 2OO3;29{t:l6]7-l623.
12. Tourangeau AE. Giovannetti P. Tu JV. Wood M.Nursing-related determinants of 30-day mortality' forhospitalized patients. CanJ Nurs Res. 2002:33:71-88.
13. Person SD, Allison JJ. Kiefe Cl, et al. Nurse staffingand mortality' tor medicare patients with acute my-(Kardial infarction. MedCare. 2(K)4;42;4-12.
14. Needleman J, Buerbaus R Mattke S, Stewart M,Zelevinsk>' K. Nurse-staffing levels and tbe quality ofcare in bospitals. A'E/Af. 2OO2;.-;46:1715-1722.
15. Jarman B. (iault S. Alves B. et al. T-xplaining differ-ences in English bospital death rates using routinelycollected dala. HMJ 1999:318:1515-1520.
16. Kovner C, (iergen PJ. Nurse staffing levels and ad-verse events following surgery in U.S. bospitals. Im-age J Nurs Scb. 1998;30;315-.121.
17. Kovner C. Jones C, Zban C, Gergen R IJasu J. Nursestaffing and post surgical adverse events; an analysisof administrative data from a sample of U.S. hospitals:1990-1996. H.SR. 2002;37:611-629,
18. Blegen MA, Vaugbn T. A multisite study of nursestaffing and patient occurrences. Nurs Econ.1998:16:196-203.
19. Uditig I,K. Knauf RA, MUbolIand DK. Some impactsof nursing on acute care outcomes./OiV4. 1999;29;25-33.
20. Cho SH. Ketefian S, Barkauskas VH. Smitb DG. Tbeeffects of ntirse staffing on adverse events, morbidity,mortality, ajid medical costs. Nurs Res. 2OO3;52;71-79.
21. Whitman GR. Tbe impact of staffmg on patientoutcomes acmss specialty units. / Nurs Admin.2(X)2;32:633-639.
22. Sovie MD. Jawad AE Hospital restructuring and its im-pact on outcomes: nursing .staff regulations are pre-mature.y/V«rsy*^m. 2(H)l;3l:588-600.
23. Manbeim LM, FeinglassJ, Sbortell SM. Hugbes EF. Re-gional variation in medicare hospital mortality. In-ifulry. 1992:29:55-66.
24. Bond CA, Raebl CL. Pitterle ME, Franke T Healtb-care professional staffmg, bospital cbaracteristics.
and bospital monality rates. Pbartnacotberapy.1999;19:13O-I38.
25. Bond CA. Raehl CL, Eranke T Medication errors inUnited States hospitals. Pbannacotberapy. 2OO1;21:1023-1036.
26. Knauf RA, Uebtig LK. Rison-McCoy R. Singer AD,Wozniak LAI. Implementing Nursing's Report Card:A Study ofRN .Staffing, length of Stay and PatientOutcomes. Wasbington, DC: American Nurses Pub-lishing; 1997.
27. Carr-HiU R. Tbe impact of nursing grade on tbequality and outcome of nursing care. Healtb Econ.l995;4;57-72.
28. Hickam DH, Severance S. Eeldstein A. et al. IJte Ef-fect of Health Care Working Conditions on Pa-tient .Safety: Rockville. Md: Agency for HealthcareResearch and gualit>; 20()^.
29. Scbultz MA. van Ser\elkn G. A critical reviewof researcb on hospital mortalit)' among medical-surgical and acute myocardial inlarction patients.Nurs Health Sci. 2000:2; 103-112.
30. Carr-Hill R, Currie L, Dixon P Skillmix in SecondaryCare: SDO Scoping Exercise. York. Pa; University ofYork. Centre Ibr Healtb Economics: 2003.
31. Biichan J, Da! Poz M. Skill mix in tbe bealth care worii-tbrce: reviewing tbe evidence. Bull World Healtb Or-gan. 2OO2;8O:575-58O.
32. Franklin C. Mathew J. Developing strategies to pre-vent inhospital cardiac arrest: analyzing responses ofphysicians and nurses in the boiirs before the event.Crit Care Med. 1994;.22:2i4-247.
33. Naugbton C, Prowroznyk A, Feneck R Reasons forprolonged hospital stays following hean sui^er>. HrJ Nurs. 1999:8:1085-1087.
34. BaU C. McEUigot M. Realising tbe potential of criticalCite tmrscs. Intensive Crit Care Nurs. 2003;19;226-2.38.
35. Rapaport L. State eases nurse staffing law until 2008ISacramento Bee online]. AvaUable at; bttp;//www..sacbee.com/content/news/medical/story/11326042p-1224O753c.btml. Accessed March 1, 2005.
36. Workforce Development Confederations' standingconference. A Proposal to Develop a NationalFramework for .Assistant Practitioners andAdvanced Practitioners. Greater Manchester.England: Workforce Development Confederation;2003.
37. MeCue M, Mark BA. Hariess DW. Nurse staffing, qual-ity, and financial performance. J Health Care Fi-nance. 2(H)3;29;54-76,
38. Sidani S. Doran DM, Mitchell PH. A tbeory-driven ap-proach to evaluating quality of nursing care. J NursScbolarsh. 2004;.36:60-65.
