visceral larva migrans presenting as acute abdomen in a child
TRANSCRIPT
www.elsevier.com/locate/jpedsurg
Visceral larva migrans presenting as acute abdomenin a child
Mustafa Inana,*, Nermin Sakrub, Ulfet Vatanseverc, Selcuk Bilgid
aDepartment of Pediatric Surgery, Faculty of Medicine, University of Trakya, 22030 Edirne, TurkeybDepartment of Microbiology and Clinical Biology, Faculty of Medicine, University of Trakya, 22030 Edirne, TurkeycDepartment of Paediatrics, Faculty of Medicine, University of Trakya, 22030 Edirne, TurkeydDepartment of Pathology, Faculty of Medicine, University of Trakya, 22030 Edirne, Turkey
0022-3468/$ – see front matter D 2006
doi:10.1016/j.jpedsurg.2005.11.081
* Corresponding author. Trakya U
Cerrahisi AD, 22030, Edirne-Turkey. Te
+90 505 527 13 89; fax: +90 284 235 7
E-mail address: mustafainan@trakya
Index words:Visceral larva migrans;
Toxocariasis;
Acute abdomen;
Toxocara canis
Abstract An unusual presentation of visceral larva migrans observed in a patient is reported. A 5-year-
old boy suffering fever, abdominal pain, tenderness, and rigidity in the right lower and upper quadrant of
the abdomen was operated on, with the false diagnosis of acute abdomen, and exploratory surgery was
carried out. The pathological examination of the liver biopsy revealed eosinophil-rich necrotizing
granulomatous inflammation with Toxocara spp larva. The diagnosis was also confirmed by serologic
results. Clinicians should remember that toxocaral visceral larva migrans may rarely mimic an acute
abdomen and cause unnecessary operations.
D 2006 Elsevier Inc. All rights reserved.
Toxocara canis and T cati are distributed worldwide, and
the degree of host damage and the concomitant elicitation of
signs and symptoms vary with regard to which tissue has
been invaded: the liver, lungs, or central nervous system [1].
Human toxocariasis is manifested as 3 distinct entities. The
first is visceral larva migrans (VLM), with typical presen-
tation of fever, pulmonary manifestations, and hepatomeg-
aly. The second one is ocular toxocariasis, and the last one is
covert toxocariasis [2].
To our knowledge, acute abdomen table during the
toxocaral VLM syndrome has not been published in the
English literature [1-7]. We would like to report a patient
who had toxocaral VLM mimicking acute appendicitis and
discuss its clinical features.
Elsevier Inc. All rights reserved.
niversitesi Tip Fakqltesi, Cocuk
l.: +90 284 235 7641 1094, GSM:
6 52.
.edu.tr (M. Inan).
1. Case report
A 5-year-old boy presented to the emergency department
(ED) with a primary complaint of abdominal pain and fever
for a 2-day duration. Initially, the pain was dull, constant,
and perceived in the midepigastrium. The pain did not
respond to a dose of acetaminophen taken 2 days earlier at
the onset of his pain. Over the course of 24 hours, the pain
became sharp and colicky and had localized to the right
lower quadrant. The worsening pain was associated with 2
episodes of nonbloody, nonmucous diarrhea and anorexia.
His history was significant for upper airway infection over
the last week. He had been given antibiotic (unknown name)
and metimazol (antipyretic) and had experienced urticaria
after 4 days. He was admitted to another hospital and was
diagnosed to have lower airway infection and urticaria due
to metimizol. He had been given acetaminophen, claritro-
mycin, corticosteroids, and antihistaminics, which partially
improved his symptoms. He was transported to our ED
Journal of Pediatric Surgery (2006) 41, E7–E9
M. Inan et al.E8
because of high white blood cell count, fever, and
abdominal pain indicating acute abdomen. There was no
surgical history. There was no history of pica, association
with cats or dogs, and recent traveling. The family history
was not significant.
At the first examination, the blood pressure was 90/60
mm Hg, the pulse was 132 beats per minute, and the
temperature was 398C axillary (40.58C rectally). The
abdominal examination was significant for mild midepigas-
tric tenderness, and profound tenderness in the vicinity of
McBurney point and right upper quadrant. The patient had
moderate rebound and guarding exclusively in the right
lower quadrant. The examinations of other systems were
normal. Laboratory evaluation disclosed a white blood cell
count of 42,000 cells per mm3 with 50% neutrophils, 10%
lymphocytes, and 40% eosinophils. The hemoglobin level
was 12.3 g/dL. The results of electrolyte studies, liver
function tests, and serum lipase measurements were all
normal. Erythrocyte sedimentation rate was 36 mm/h
(1-12 mm/h) and C-reactive protein was 4.6 mg/dL
(1-10 mg/dL). The urinalysis demonstrated a specific
gravity of 1.025 and was positive for acetone. Radiography
of the chest was normal, but abdominal radiographs showed
paucity intestinal gas and mass effect on the upper and
lower right side of the abdomen with 2 little air-fluid levels
on the right fossa ilaca. The ultrasound examination of the
abdomen revealed hepatomegaly and locular fluid collection
neighboring to the right psoas muscle and kidney.
Parasitic diseases (ascariasis, trichinosis, toxocariasis,
strongyloidiasis, and hook worm infections) or a drug
allergy was considered in this case because the eosinophil
count was markedly elevated and hepatomegaly was found.
However, the presumptive diagnosis of acute abdomen was
entertained based on the progression of the patient’s
symptoms, his abdominal examination, and elevated white
blood cell count. A stool specimen for ova and parasite
examination was also sent to the laboratory. The patient was
observed in the ED for a total of 12 hours. His pain did not
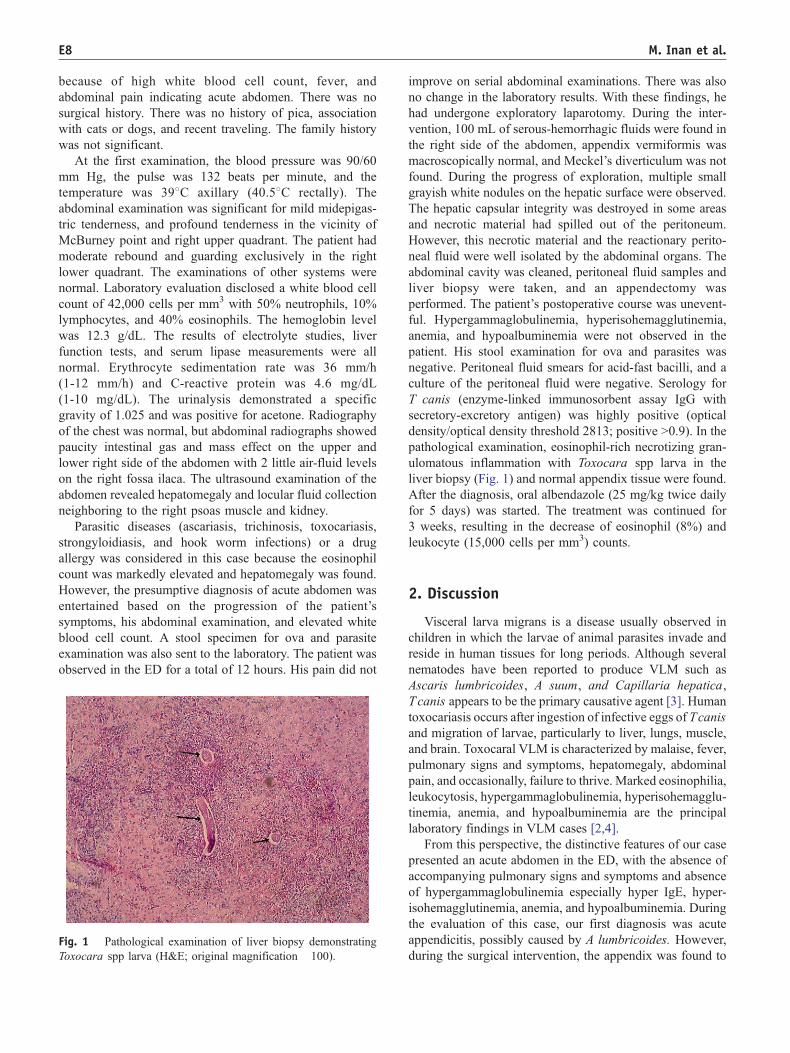
Fig. 1 Pathological examination of liver biopsy demonstrating
Toxocara spp larva (H&E; original magnification �100).
improve on serial abdominal examinations. There was also
no change in the laboratory results. With these findings, he
had undergone exploratory laparotomy. During the inter-
vention, 100 mL of serous-hemorrhagic fluids were found in
the right side of the abdomen, appendix vermiformis was
macroscopically normal, and Meckel’s diverticulum was not
found. During the progress of exploration, multiple small
grayish white nodules on the hepatic surface were observed.
The hepatic capsular integrity was destroyed in some areas
and necrotic material had spilled out of the peritoneum.
However, this necrotic material and the reactionary perito-
neal fluid were well isolated by the abdominal organs. The
abdominal cavity was cleaned, peritoneal fluid samples and
liver biopsy were taken, and an appendectomy was
performed. The patient’s postoperative course was unevent-
ful. Hypergammaglobulinemia, hyperisohemagglutinemia,
anemia, and hypoalbuminemia were not observed in the
patient. His stool examination for ova and parasites was
negative. Peritoneal fluid smears for acid-fast bacilli, and a
culture of the peritoneal fluid were negative. Serology for
T canis (enzyme-linked immunosorbent assay IgG with
secretory-excretory antigen) was highly positive (optical
density/optical density threshold 2813; positive N0.9). In the
pathological examination, eosinophil-rich necrotizing gran-
ulomatous inflammation with Toxocara spp larva in the
liver biopsy (Fig. 1) and normal appendix tissue were found.
After the diagnosis, oral albendazole (25 mg/kg twice daily
for 5 days) was started. The treatment was continued for
3 weeks, resulting in the decrease of eosinophil (8%) and
leukocyte (15,000 cells per mm3) counts.
2. Discussion
Visceral larva migrans is a disease usually observed in
children in which the larvae of animal parasites invade and
reside in human tissues for long periods. Although several
nematodes have been reported to produce VLM such as
Ascaris lumbricoides, A suum, and Capillaria hepatica,
Tcanis appears to be the primary causative agent [3]. Human
toxocariasis occurs after ingestion of infective eggs of Tcanis
and migration of larvae, particularly to liver, lungs, muscle,
and brain. Toxocaral VLM is characterized by malaise, fever,
pulmonary signs and symptoms, hepatomegaly, abdominal
pain, and occasionally, failure to thrive. Marked eosinophilia,
leukocytosis, hypergammaglobulinemia, hyperisohemagglu-
tinemia, anemia, and hypoalbuminemia are the principal
laboratory findings in VLM cases [2,4].
From this perspective, the distinctive features of our case
presented an acute abdomen in the ED, with the absence of
accompanying pulmonary signs and symptoms and absence
of hypergammaglobulinemia especially hyper IgE, hyper-
isohemagglutinemia, anemia, and hypoalbuminemia. During
the evaluation of this case, our first diagnosis was acute
appendicitis, possibly caused by A lumbricoides. However,
during the surgical intervention, the appendix was found to

Acute abdomen: visceral larva migrans E9
be normal; on further exploration, an eosinophil-rich
necrotizing granulomatous inflammation with Toxocara
spp larva was found on the liver surface. This result con-
firmed our definitive diagnosis of VLM due to toxocariasis.
The capsular tension of necrotic inflammation into the
liver tissue and reactionary peritoneal fluid may have caused
his abdominal clinical features. However, we thought that
our patient could be in parasitic infestation in the
preoperative period; his persistent pain in the right lower
abdominal quadrant and continued fever made surgery a
logical and necessary step.
Our case demonstrated that the diagnosis of toxocaral
VLM can be difficult without surgical intervention because
its clinical picture mimics an acute appendicitis, and if liver
abscesses are encountered during abdominal exploration in
such a patient, biopsy should be considered. In addition,
once the diagnosis is established, antihelmintics treatment
should be started as soon as possible [2,3,6]. The present
case report suggests that we are still not fully aware of the
potential gastrointestinal presentations and complications of
T canis infection.
Acknowledgments
The authors thank Metin Korkmaz, MD, and his
colleagues in the Department of Parasitology, Faculty of
Medicine, Ege University for serologic tests of the patient.
References
[1] Despommier D. Toxocariasis: clinical aspects, epidemiology, medical
ecology, and molecular aspects. Clin Microbiol Rev 2003;16:265-72.
[2] Markell EK, John DT, Krotoski WA. Sings and symptoms of parasitic
disease. In: Markell EK, John DT, Krotoski WA, editors. Markell and
Voge’s medical parasitology. Philadelphia7 WB Saunders; 1999.
p. 403 -23.
[3] Taylor MR, Keane CT, O’Connor P, et al. The expanded spectrum of
toxocaral disease. Lancet 1988;26:692 -5.
[4] Gayotto LDC, Da Silva LC. Ascariasis, visceral larva migrans,
capillariasis, strongyloidiasis, and pentastomiasis. In: McIntyre N,
Benhamou JP, Bircher J, et al, editors. Oxford textbook of clinical
hepatology, vol. 1. Oxford7 Oxford Medical Publications; 1991.
p. 730 -9.
[5] Zinkham WH. Visceral larva migrans. Am J Dis Child 1978;132:
627 -33.
[6] Worley G, Green JA, Frothingham TE, et al. Toxocara canis infection:
clinical and epidemiological associations with seropositivity in
kindergarten children. J Infect Dis 1984;149:591 -7.
[7] Fenoy S, Cuellar C, Guillen JL. Serological evidence of toxocariasis in
patients from Spain with a clinical suspicion of visceral larva migrans.
J Helminthol 1997;71:9 -12.