villanueva poster final
TRANSCRIPT
QUICK DESIGN GUIDE (--THIS SECTION DOES NOT PRINT--)
This PowerPoint 2007 template produces a 42”x90” professional poster. You can use it to create your research poster and save valuable time placing titles, subtitles, text, and graphics. We provide a series of online tutorials that will guide you through the poster design process and answer your poster production questions. To view our template tutorials, go online to PosterPresentations.com and click on HELP DESK. When you are ready to print your poster, go online to PosterPresentations.com.
Need Assistance? Call us at 1.866.649.3004
Object Placeholders
Using the placeholders To add text, click inside a placeholder on the poster and type or paste your text. To move a placeholder, click it once (to select it). Place your cursor on its frame, and your cursor will change to this symbol . Click once and drag it to a new location where you can resize it. Section Header placeholder Click and drag this preformatted section header placeholder to the poster area to add another section header. Use section headers to separate topics or concepts within your presentation. Text placeholder Move this preformatted text placeholder to the poster to add a new body of text. Picture placeholder Move this graphic placeholder onto your poster, size it first, and then click it to add a picture to the poster.
For questions please email: [email protected]
QUICK TIPS (--THIS SECTION DOES NOT PRINT--)
This PowerPoint template requires basic PowerPoint (version 2007 or newer) skills. Below is a list of commonly asked questions specific to this template. If you are using an older version of PowerPoint some template features may not work
properly.
Template FAQs
Verifying the quality of your graphics Go to the VIEW menu and click on ZOOM to set your preferred magnification. This template is at 100% the size of the final poster. All text and graphics will be printed at 100% their size. To see what your poster will look like when printed, set the zoom to 100% and evaluate the quality of all your graphics before you submit your poster for printing. Modifying the layout This template has four different column layouts. Right-click your mouse on the background and click on LAYOUT to see the layout options. The columns in the provided layouts are fixed and cannot be moved but advanced users can modify any layout by going to VIEW and then SLIDE MASTER. Importing text and graphics from external sources TEXT: Paste or type your text into a pre-existing placeholder or drag in a new placeholder from the left side of the template. Move it anywhere as needed. PHOTOS: Drag in a picture placeholder, size it first, click in it and insert a photo from the menu. TABLES: You can copy and paste a table from an external document onto this poster template. To adjust the way the text fits within the cells of a table that has been pasted, right-click on the table, click FORMAT SHAPE then click on TEXT BOX and change the INTERNAL MARGIN values to 0.25. Modifying the color scheme To change the color scheme of this template go to the DESIGN menu and click on COLORS. You can choose from the provided color combinations or create your own.
© 2013 PosterPresenta/ons.com 2117 Fourth Street , Unit C Berkeley CA 94710 [email protected]
Student discounts are available on our Facebook page. Go to PosterPresentations.com and click on the FB icon
• In hospitalized newborn aged 0 -12 months, is oral sucrose safe and effective when used in procedural pain management?
INTRODUCTION & STATEMENT OF THE PROBLEM • Approximately 7-10% of neonates are born preterm and many full term
neonates are admitted into the NICU for surgical and medical management of disease process.
• Other methods of pain relief, including nonnutritive sucking (NNS) and skin-to-skin should be considered in combination with sucrose to reduce or eliminate the pain significantly in this population.
Georgetown University
TECHNOLOGICAL AND MEDICAL ADVANCES
IMPROVED OUTCOMES
INCREASE PAINFUL PROCEDURES
• With the considerable adverse effects of medications that are used to treat pain especially in the neonates focus has shifted on the utilization of SUCROSE, a safer, more easily acquired and cost effective pain management in this age group.
PICOT QUESTION
LEVEL I: 4 SYSTEMATIC
REVIEWS
LEVEL II: 5 WELL
DESIGNED RANDOMIZED
CONTROL TRIALS
LEVEL III: 1 PROTOCOL; 7 SUPPLEMENTAL
REFERENCE ARTICLES
Preterm and full term neonates in NICU Infants 1 month to 1 year for routine clinic visit, pediatric ward and PICU admission Utilization of oral sucrose commonly knows as “sweet ease” for pain management Compare the results of the outcomes of standard care with and without the intervention Decreased pain during venipuncture, heel lance or any other pain or discomfort inducing procedures that cause a break in the skin Entire duration of the procedure
SEARCH ST!TEGY & RESULTS
PURPOSE
• To explore the efficacy and safety of oral sucrose when used in procedural pain management for preterm, full term neonates and infants.
• To generate guidelines on the use of oral sucrose for procedural management that are based on best current evidence
2. LINK problem intervention and outcomes
3. SYNTHESIZE best evidence
4. DESIGN practice change
5. IMPLEMENT AND EVALUATE change in practice
6. INTEGRATE AND MAINTAIN
change in practice
• Include stakeholders • Collect internal data
about current practice
• Compare internal data with external data
• Identify problem
• Use standardized classification systems and language
• Identify potential interventions and activities
• Select outcomes indicators
• Search research literature related to major variables
• Critique and weigh evidence
• Synthesize best evidence
• Assess feasibility, benefits, and risk
• Define proposed change
• Identify needed resources
• Plan implementation process
• Define outcomes
• Pilot study demonstration
• Evaluate process and outcome
• Decide to adapt, adopt, or reject practice change
• Communicate recommended change to stakeholders
• Present staff in-service education on change in practice
• Integrate into standards of practice
• Monitor process and outcomes
1. ASSESS need for change in practice
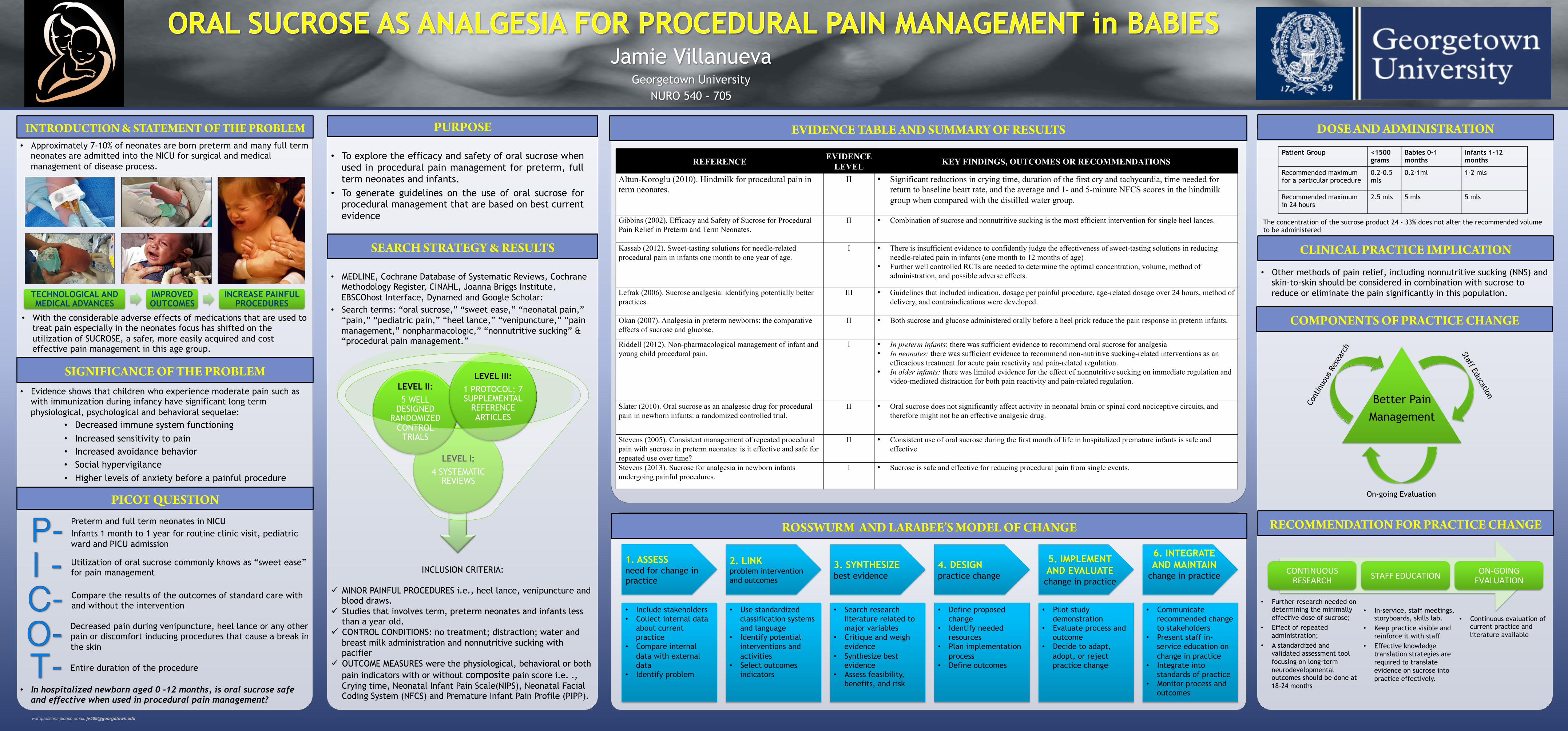
EVIDENCE TABLE AND SUMMARY OF RESULTS
ROSSWURM AND LA!BEE’S MODEL OF CHANGE
Jamie Villanueva Georgetown University
NURO 540 - 705
SIGNIFICANCE OF THE PROBLEM • Evidence shows that children who experience moderate pain such as
with immunization during infancy have significant long term physiological, psychological and behavioral sequelae:
• Decreased immune system functioning • Increased sensitivity to pain • Increased avoidance behavior • Social hypervigilance • Higher levels of anxiety before a painful procedure
• MEDLINE, Cochrane Database of Systematic Reviews, Cochrane Methodology Register, CINAHL, Joanna Briggs Institute, EBSCOhost Interface, Dynamed and Google Scholar:
• Search terms: “oral sucrose,” “sweet ease,” “neonatal pain,” “pain,” “pediatric pain,” “heel lance,” “venipuncture,” “pain management,” nonpharmacologic,” “nonnutritive sucking” & “procedural pain management.”
REFERENCE EVIDENCE LEVEL KEY FINDINGS, OUTCOMES OR RECOMMENDATIONS
Altun-Koroglu (2010). Hindmilk for procedural pain in term neonates.
II • Significant reductions in crying time, duration of the first cry and tachycardia, time needed for return to baseline heart rate, and the average and 1- and 5-minute NFCS scores in the hindmilk group when compared with the distilled water group.
Gibbins (2002). Efficacy and Safety of Sucrose for Procedural Pain Relief in Preterm and Term Neonates.
II • Combination of sucrose and nonnutritive sucking is the most efficient intervention for single heel lances.
Kassab (2012). Sweet-tasting solutions for needle-related procedural pain in infants one month to one year of age.
I • There is insufficient evidence to confidently judge the effectiveness of sweet-tasting solutions in reducing needle-related pain in infants (one month to 12 months of age)
• Further well controlled RCTs are needed to determine the optimal concentration, volume, method of administration, and possible adverse effects.
Lefrak (2006). Sucrose analgesia: identifying potentially better practices.
III • Guidelines that included indication, dosage per painful procedure, age-related dosage over 24 hours, method of delivery, and contraindications were developed.
Okan (2007). Analgesia in preterm newborns: the comparative effects of sucrose and glucose.
II • Both sucrose and glucose administered orally before a heel prick reduce the pain response in preterm infants.
Riddell (2012). Non-pharmacological management of infant and young child procedural pain.
I • In preterm infants: there was sufficient evidence to recommend oral sucrose for analgesia • In neonates: there was sufficient evidence to recommend non-nutritive sucking-related interventions as an
efficacious treatment for acute pain reactivity and pain-related regulation. • In older infants: there was limited evidence for the effect of nonnutritive sucking on immediate regulation and
video-mediated distraction for both pain reactivity and pain-related regulation.
Slater (2010). Oral sucrose as an analgesic drug for procedural pain in newborn infants: a randomized controlled trial.
II • Oral sucrose does not significantly affect activity in neonatal brain or spinal cord nociceptive circuits, and therefore might not be an effective analgesic drug.
Stevens (2005). Consistent management of repeated procedural pain with sucrose in preterm neonates: is it effective and safe for repeated use over time?
II • Consistent use of oral sucrose during the first month of life in hospitalized premature infants is safe and effective
Stevens (2013). Sucrose for analgesia in newborn infants undergoing painful procedures.
I • Sucrose is safe and effective for reducing procedural pain from single events.
INCLUSION CRITERIA:
ü MINOR PAINFUL PROCEDURES i.e., heel lance, venipuncture and blood draws.
ü Studies that involves term, preterm neonates and infants less than a year old.
ü CONTROL CONDITIONS: no treatment; distraction; water and breast milk administration and nonnutritive sucking with pacifier
ü OUTCOME MEASURES were the physiological, behavioral or both pain indicators with or without composite pain score i.e. ., Crying time, Neonatal Infant Pain Scale(NIPS), Neonatal Facial Coding System (NFCS) and Premature Infant Pain Profile (PIPP).
Patient Group <1500 grams
Babies 0-1 months
Infants 1-12 months
Recommended maximum for a particular procedure
0.2-0.5 mls
0.2-1ml 1-2 mls
Recommended maximum in 24 hours
2.5 mls 5 mls 5 mls
Better Pain
Management
On-going Evaluation
RECOMMENDATION FOR P!CTICE CHANGE
COMPONENTS OF P!CTICE CHANGE
CLINICAL P!CTICE IMPLICATION
DOSE AND ADMINIST!TION
CONTINUOUS RESEARCH STAFF EDUCATION ON-‐GOING
EVALUATION
• Further research needed on determining the minimally effective dose of sucrose;
• Effect of repeated administration;
• A standardized and validated assessment tool focusing on long-term neurodevelopmental outcomes should be done at 18-24 months
• Continuous evaluation of current practice and literature available
• In-service, staff meetings, storyboards, skills lab.
• Keep practice visible and reinforce it with staff
• Effective knowledge translation strategies are required to translate evidence on sucrose into practice effectively.
The concentration of the sucrose product 24 - 33% does not alter the recommended volume to be administered