utility of umbilical artery doppler in preterm premature ... · pdf fileutility of umbilical...
TRANSCRIPT
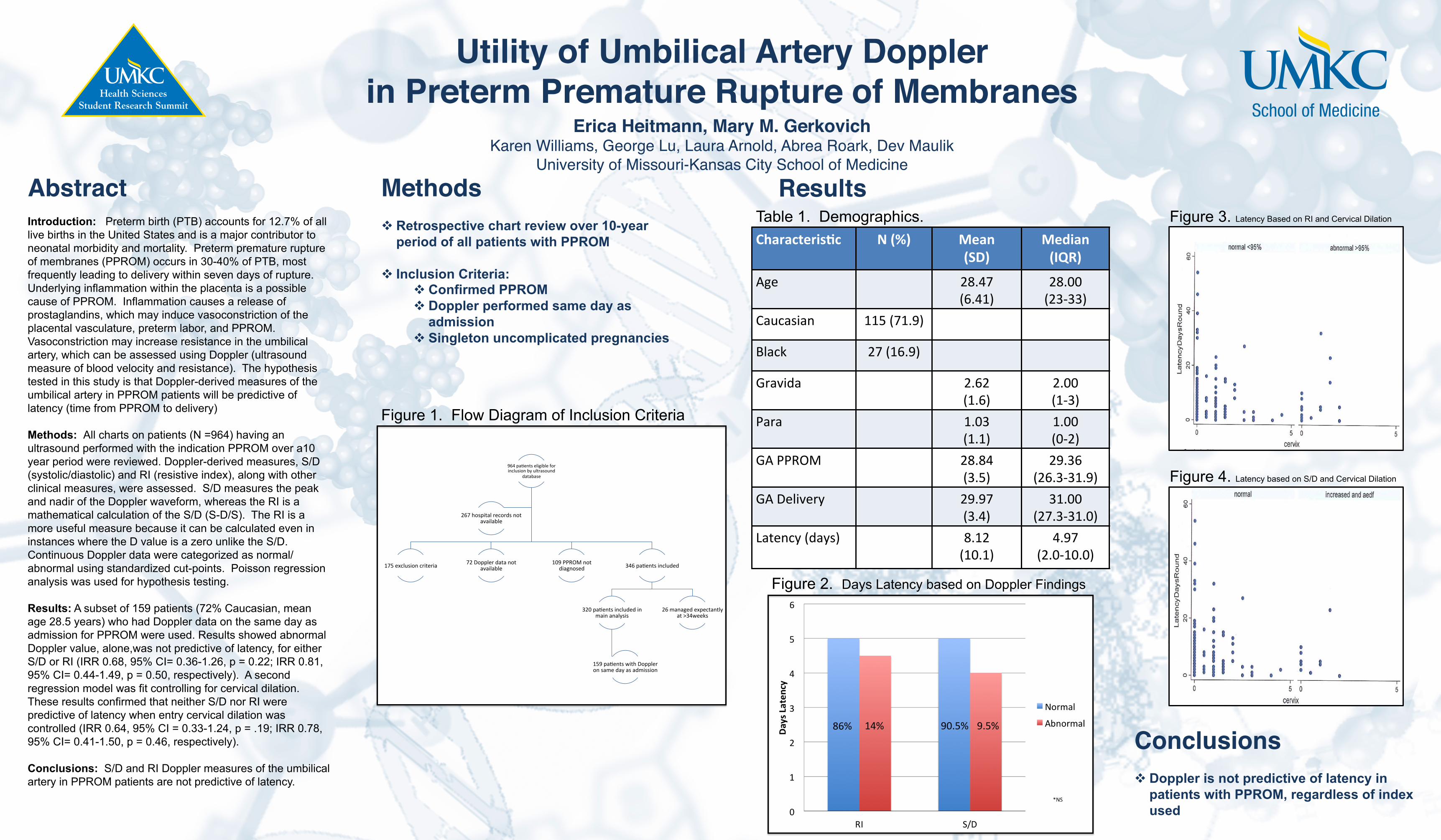
Utility of Umbilical Artery Doppler !in Preterm Premature Rupture of Membranes!
Erica Heitmann, Mary M. Gerkovich !Karen Williams, George Lu, Laura Arnold, Abrea Roark, Dev Maulik!
University of Missouri-Kansas City School of Medicine!!Abstract!
Introduction: Preterm birth (PTB) accounts for 12.7% of all live births in the United States and is a major contributor to neonatal morbidity and mortality. Preterm premature rupture of membranes (PPROM) occurs in 30-40% of PTB, most frequently leading to delivery within seven days of rupture. Underlying inflammation within the placenta is a possible cause of PPROM. Inflammation causes a release of prostaglandins, which may induce vasoconstriction of the placental vasculature, preterm labor, and PPROM. Vasoconstriction may increase resistance in the umbilical artery, which can be assessed using Doppler (ultrasound measure of blood velocity and resistance). The hypothesis tested in this study is that Doppler-derived measures of the umbilical artery in PPROM patients will be predictive of latency (time from PPROM to delivery) Methods: All charts on patients (N =964) having an ultrasound performed with the indication PPROM over a10 year period were reviewed. Doppler-derived measures, S/D (systolic/diastolic) and RI (resistive index), along with other clinical measures, were assessed. S/D measures the peak and nadir of the Doppler waveform, whereas the RI is a mathematical calculation of the S/D (S-D/S). The RI is a more useful measure because it can be calculated even in instances where the D value is a zero unlike the S/D. Continuous Doppler data were categorized as normal/abnormal using standardized cut-points. Poisson regression analysis was used for hypothesis testing. Results: A subset of 159 patients (72% Caucasian, mean age 28.5 years) who had Doppler data on the same day as admission for PPROM were used. Results showed abnormal Doppler value, alone,was not predictive of latency, for either S/D or RI (IRR 0.68, 95% CI= 0.36-1.26, p = 0.22; IRR 0.81, 95% CI= 0.44-1.49, p = 0.50, respectively). A second regression model was fit controlling for cervical dilation. These results confirmed that neither S/D nor RI were predictive of latency when entry cervical dilation was controlled (IRR 0.64, 95% CI = 0.33-1.24, p = .19; IRR 0.78, 95% CI= 0.41-1.50, p = 0.46, respectively). Conclusions: S/D and RI Doppler measures of the umbilical artery in PPROM patients are not predictive of latency.
Methods! v Retrospective chart review over 10-year
period of all patients with PPROM v Inclusion Criteria:
v Confirmed PPROM v Doppler performed same day as
admission v Singleton uncomplicated pregnancies !
Results!!!
Conclusions!!v Doppler is not predictive of latency in
patients with PPROM, regardless of index used
964 pa'ents eligible for inclusion by ultrasound
database
175 exclusion criteria 72 Doppler data not available
109 PPROM not diagnosed 346 pa'ents included
320 pa'ents included in main analysis
159 pa'ents with Doppler on same day as admission
26 managed expectantly at >34weeks
267 hospital records not available
Characteris+c N (%) Mean (SD)
Median (IQR)
Age 28.47 (6.41)
28.00 (23-‐33)
Caucasian 115 (71.9)
Black 27 (16.9)
Gravida 2.62 (1.6)
2.00 (1-‐3)
Para 1.03 (1.1)
1.00 (0-‐2)
GA PPROM 28.84 (3.5)
29.36 (26.3-‐31.9)
GA Delivery 29.97 (3.4)
31.00 (27.3-‐31.0)
Latency (days) 8.12 (10.1)
4.97 (2.0-‐10.0)
Figure 1. Flow Diagram of Inclusion Criteria
Figure 2. Days Latency based on Doppler Findings
Figure 3. Latency Based on RI and Cervical Dilation
Figure 4. Latency based on S/D and Cervical Dilation
Table 1. Demographics.
86% 14% 90.5% 9.5%