urgencies & emergencies medications - official … handouts/january 2015... · urgencies &...
TRANSCRIPT
12/29/14
1
CARDIOVASCULAR URGENCIES & EMERGENCIES
Steven Ganzberg, DMD, MS Director of Anesthesiology,
Century City Outpatient Surgery Center Clinical Professor of Anesthesiology,
UCLA School of Dentistry [email protected]
MEDICATIONS Disclaimer:
Specific Required Medications May Vary Among States Use Only Those Medications With Which You Are Familiar
Cardiovascular Emergency Medications
• Dysrythmias • Ventricular
• Amiodarone 150 mg Vials** • Cardiac Lidocaine 1%/2% Syringes??
• Supraventricular • Esmolol 10mg/ml**; 10ml Vial • Diltiazem 5mg/ml; 5ml Vial • Adenosine 3mg/ml; 2ml Vial
Cardiovascular Emergency Medications
• Bradycardia • Atropine** 0.4mg/ml or 1mg/10ml Syringe • Glycopyrrolate 0.2mg/ml
• Tachycardia • Esmolol 10mg/ml** • Metoprolol 1mg/ml ? • Labetalol 5mg/ml ?
Cardiovascular Emergency Medications • Hypertension
• Beta Blockers • Esmolol 10mg/ml** • Metoprolol 1mg/ml • Labetolol 5mg/ml**
• Vasodilating Agents • Nitroglycerin SL 0.3/0.4 mg/dose**
• IV 5mg/ml?? • Hydralazine 20mg/ml • Nicardipine 2.5mg/ml • Enalaprilat 1.25mg/ml
Cardiovascular Emergency Medications • Hypotension
• Ephedrine 50 mg/ml** • Requires 1:10 Dilution to 5 mg/ml • Both α and β Effects
• Phenylephrine 10 mg/ml** • Requires “Double 1:10” Dilution to 100 mcg/ml • Primarily α Effect
• Epinephrine 1:1000 (Multiple Vials)** • Cardiac Arrest/Anaphylactic Shock (Bronchospasm)
• Dopamine 40 mg/ml (Dilution & Infusion)? • Vasopressin 40 U (For Pulselessness)?

12/29/14
2
Cardiovascular Emergency (Medications)
• AED? • Manual Defibrillator? • Cardioverter? • Transcutaneous Pacer?
General Principles For Sedated Patients If Persistent CV Urgency/Emergency • If Patient Is Conscious, Ask Them How They Feel • If Very Sedated, Consider Making Them Less Sedated
• If Not Conscious, Consider Making Them Conscious • Evaluate Multiple Indicators
REVIEW OF THE ELECTROCARDIOGRAM Electrical
Conduction System
✷
Cardiac Pacemakers • SA Node 60 -100 BPM • AV Node 40 - 60 BPM • Ventricular 20 - 40 BPM
LEAD PLACEMENT

12/29/14
3
Lead + ― • I LA RA • II LL RA • III LL LA • aVL LA LL/RA • aVR RA LL/LA • aVF RF LA/RA
Anterior
Basics of the EKG
Heart Rate • Normal 60-100 BPM • Bradycardia = HR < 60 • Tachycardia = HR > 100 • Physiologic Bradycardia • Relative Bradycardia

12/29/14
4
ECG Interpretation • Rate • Rhythm • Axis • Hypertrophy • Infarction
Rhythm
• Identify Basic Rhythm • Abnormal Waveforms • Pauses • Premature Beats • Irregularity
Rhythm • ü P Before Each QRS & QRS After Each P • ü PR Intervals • ü QRS Interval • ü PVCs
SINUS RHYTHM
SELECTED RHYTHM EMERGENCIES
Too Slow Irregular Rhythms Too Fast Wide Complexes

12/29/14
5
SELECTED RHYTHM EMERGENCIES
Too Slow Irregular Rhythms Too Fast Wide Complexes
What About Bradycardia? • Physiologic Bradycardia/Reflex Bradycardia/↑ Age • Hypoxia/Hypercarbia • Drug Induced:
• Beta Blockade/Ca++ Channel Blockade/Excess Digoxin /α2’s /Li++
• Opioid Effect • Anesthetic Overdose
• Primary Conduction Defect (MI?) • Sick Sinus Syndrome • Junctional Rhythm • 2nd and 3rd Degree Heart Block
• Decompensation/20% Acute MI, Esp. Inferior Wall • Pharyngeal and Oculocardiac Reflexes • Hypothyroidism/SLE/Collagen Vascular Disease
Respiratory Arrhythmia • Increase in heart rate during inspiration • Exaggerated in children, young adults and athletes • Decreases with age
• Usually asymptomatic, no treatment or referral • Can be non-respiratory
• Both in normal or diseased heart • Referral may be necessary if not clearly respiratory, history of heart disease
IF YOU DROP BEATS, YOU END UP WITH A BRADYCARDIA

12/29/14
6
2nd & 3rd Degree Heart Blocks Bradycardia What is the Cause AND
Is It Hemodynamically Significant??? • If Symptomatic
• Atropine 0.5 – 1mg • 3mg Full Adult Vagolytic Dose • No Help In 2nd Degree, Type II or 3rd Degree Heart Blocks
• Glycopyrrolate? • 0.1 - 0.2 mg Initially
• Ephedrine? • Consider If Both BP and HR Low
• For Select Heart Blocks (Discussed Later) • Dopamine? Epinephrine? Transcutaneous Pacing??
SELECTED RHYTHM EMERGENCIES
Too Slow Irregular Rhythms Too Fast Wide Complexes
What About Sinus Tachycardia? • Hypoxia/Hypercarbia • Surgical Stimulation/Inadequate Local Anesthesia • Intravascular Epinephrine Injection From LA • Severe Pre-operative Anxiety • Full Bladder • Hypotension/Hypovolemia (Reflex Tachycardia) • Medication Related: Pre-Operative & Intraoperative
• Albuterol • Ketamine/High Concentrations of Potent Inhaled Anesthetics • Amphetamines, Atomoxetine, Tricyclic Antidepressants, SNRIs • Rebound From Beta Blocker/Clonidine
• Anemia • Decreased Cardiac Output (e.g., CHF/MI/PE) • Hyperthyroidism/Hypermetabolic State/Pheo.

12/29/14
7
OTHER TACHYCARDIAS Primary Conduction Defects
Supraventricular Dysrythmias
Supraventricular Dysrythmias Why, Why, Why ?? • Primary Conduction Abnormality • Sympathetic Nervous System Activation
• Hypoxia/Hypercarbia • Atrial Volume Overload
Supraventricular Dysrythmias
• Treat Underlying Cause If Possible • Treat Rate Before Rhythm!!
• Vagal Stimulation? • Beta Blockers Acceptable First Line Treatment in All Supraventricluar Dysrythmias • Esmolol 10mg/ml
• Rule of Thumb → 1mg Decreases Heart Rate 1 Beat/Min (e.g. 10mg Decreases 10 Beats/Min)
• Exception: CHF → Consider Amiodarone
• Other Beta Blockers? Calcium Channel Blockers? • Adenosine??? Cardioversion???
What is the Cause AND Is It Hemodynamically Significant???
Early Cardioversion Should Be Considered • For All Primary Tachyarrythmias With Serious Signs & Symptoms
• Because.... • Antiarrhythmics Are Also Proarrythmics • If Impaired Myocardial Function, Antiarrythmics
Decrease Cardiac Function • Arrive At a Specific Diagnosis

12/29/14
8
SELECTED RHYTHM EMERGENCIES
Too Slow Irregular Rhythms Too Fast Wide Complexes
Irregular Rhythm • Narrow Complex or Wide Complex? • Regularly Irregular or Irregularly Irregular? • Is My Patient Hemodynamically Stable?
Irregular Rhythms – Narrow QRS • Primary Conduction Defects
• Sick Sinus Syndrome • Pre-Atrial Contractions (PACs) • Atrial Fibrillation • 2nd and 3rd Degree Heart Block
Irregular Rhythms – Wide QRS • Pre-Ventricular Contractions (PVCs) • PACs With RBBB

12/29/14
9
SICK SINUS SYNDROME
Treatment?
PRE-ATRIAL CONTRACTIONS:
PACs

12/29/14
10
So What About PACs • Can be Caused By:
• Anxiety/Caffeine • Excessive Alcohol • Sympathetic Stimulation/Drugs • Cardiac Disease/MVP • Congenital
• Treatment: • Usually Benign Without Hemodynamic
Significance
ATRIAL FIBRILLATION IRREGULARLY, IRREGULAR
Atrial Fibrillation • Epidemiology
• 1% Incidence; 2.2 Million Americans • 160,000 New Cases Per Year • Double Mortality Risk vs. Normal Sinus Rhythm • 5-Fold Increase in Stroke Risk: Cause in 20%
• Pathophysiology • Uncoordinated Atrial Rhythm • Four Types:
• Lone, Paroxysmal, Persistent, Permanent • Irregularly, Irregular Ventricular Rhythm • Possible Embolus with Conversion to Normal Sinus Rhythm
• Treatment • Control Ventricular Response To Prevent A-Fib with RVR • Anticoagulation (Prevents Mural Thrombus) • Cardioversion • Ablation
Atrial Fibrillation With RVR • Control Rate, Then Rhythm
• Beta Blockers • Esmolol, 0.5mg/kg and titrate • Metoprolol, Titrate 2.5mg q10 – 15 minutes
• Calcium Channel Blockers • Diltiazem, 5mg q10 – 15 min
• Amiodarone in CHF → ED Titration? • Caution!! Cardioversion - Unless Onset Less Than 48 Hours (and you really want to) • Risk of Pulmonary Embolus/Stroke
HEART BLOCKS Another Irregular Rhythm
2nd & 3rd Degree Heart Blocks

12/29/14
11
Electrical Conduction System
✷
10 AV Block + Wenckebach
Electrical Conduction System
✷
20 AV Block, Type 2
& 30 Block
Questions: Heart Blocks • Is My Patient Hemodynamically Stable? • Onset?
• Before Case On Placement of ECG • During Case → Must Ask: Is This Presentation of MI?
• 10 AV Block → Minimal Issues • 20 Type I – Wenckebach
• Vagally Mediated During Case? • If Pre-op, Cardio Consult?
• 20 Type II and 3rd Degree → ED Evaluation • Is This Initial Presentation of Intraoperative MI?
PRE-VENTRICULAR CONTRACTIONS - PVCs
Yet Another Irregular Rhythm

12/29/14
12
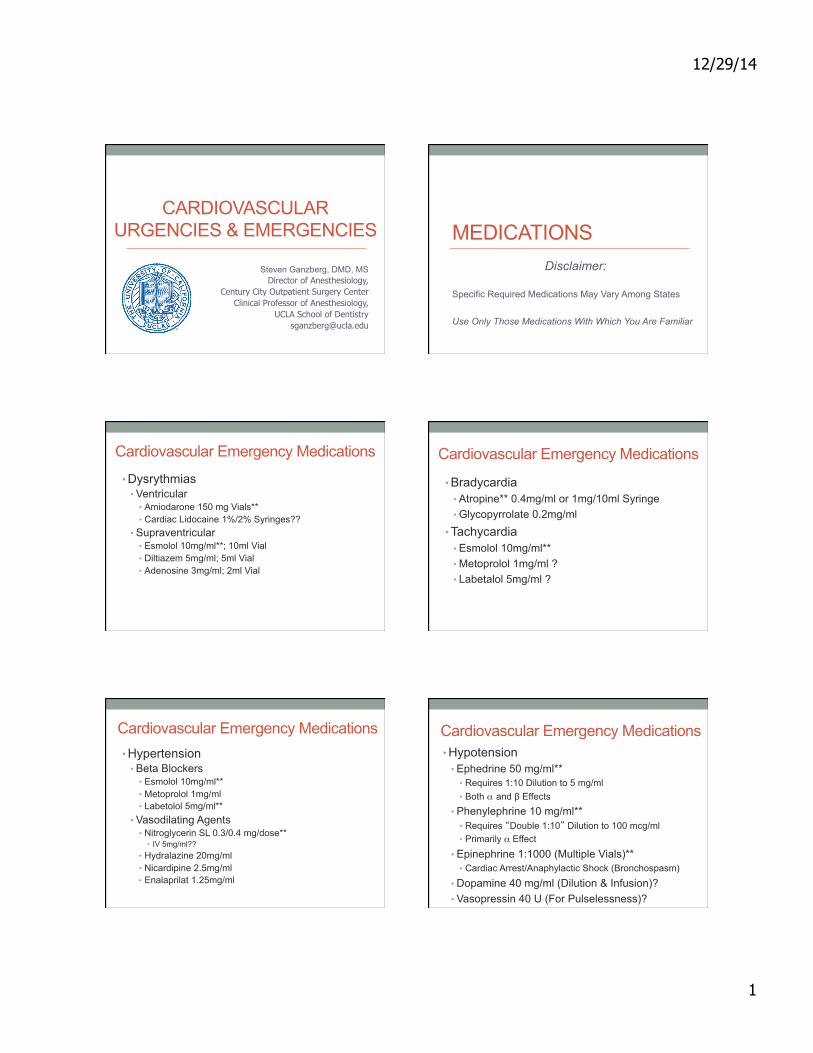
PVCs
SELECTED RHYTHM EMERGENCIES
Too Slow Irregular Rhythms Too Fast Wide Complexes
12/29/14
13
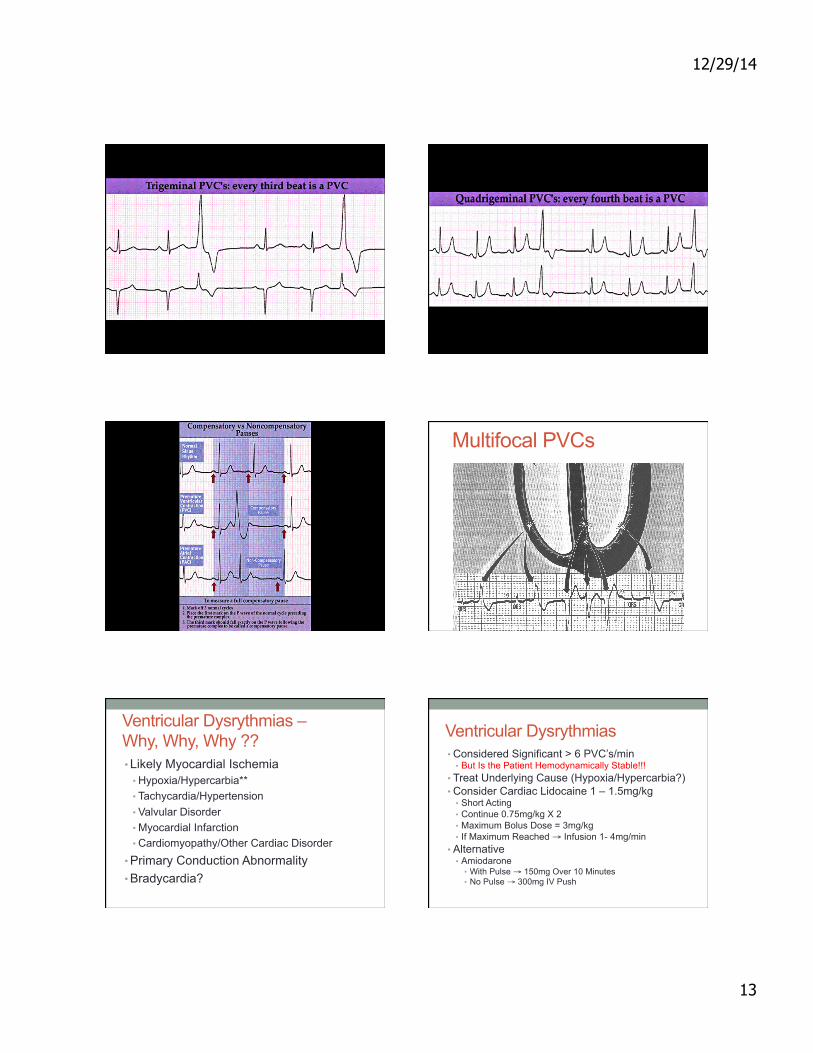
Multifocal PVCs
Ventricular Dysrythmias – Why, Why, Why ?? • Likely Myocardial Ischemia
• Hypoxia/Hypercarbia** • Tachycardia/Hypertension • Valvular Disorder • Myocardial Infarction • Cardiomyopathy/Other Cardiac Disorder
• Primary Conduction Abnormality • Bradycardia?
Ventricular Dysrythmias • Considered Significant > 6 PVC’s/min
• But Is the Patient Hemodynamically Stable!!! • Treat Underlying Cause (Hypoxia/Hypercarbia?) • Consider Cardiac Lidocaine 1 – 1.5mg/kg
• Short Acting • Continue 0.75mg/kg X 2 • Maximum Bolus Dose = 3mg/kg • If Maximum Reached → Infusion 1- 4mg/min
• Alternative • Amiodarone
• With Pulse → 150mg Over 10 Minutes • No Pulse → 300mg IV Push

12/29/14
14
CAN YOU HAVE A P WAVE BEFORE A WIDE COMPLEX QRS????
RIGHT/LEFT BUNDLE BRANCH BLOCK
Another Wide Complex Rhythm
Yes!!
Electrical Conduction System - RBBB
✷
Electrical Conduction System - LBBB
✷
LBBB WPW Wolf-Parkinson-White

12/29/14
15
Fusion activation of the ventricles
AP
Sinus beat Hybrid
QRS shape
Accessory Pathway with Ventricular Preexcitation- WPW
Varying Degrees of Ventricular Preexcitation
AND……….. THE ULTIMATE VENTRICULAR RHYTHM

12/29/14
16
LASTLY, WHAT ABOUT MI? CHEST PAIN Is It Angina Pectoris Or
Myocardial Infarction???? Or Something Else???
Chest Pain - Angina Pectoris • Increased O2 Demand Relative To Supply • Usually Exertional • Angina Pectoris Usually Resolves in Minutes With Rest or After Sublingual Nitroglycerin (NTG)
• Types of Angina • Stable Angina • Unstable Angina • Vasospastic (Prinzmetal’s) Angina
Chest Pain - Acute MI • Decreased O2 Supply to Myocardium • Chest Pain at Rest • Chest Pain Lasts Longer Than Angina • Crushing CP, Sense of ‘Impending Doom’ • ↓ CO -Lightheadedness, Diaphoretic, Nausea, SOB, Weakness, Cool Skin
• Ashen, Gray Color, Cyanosis, Arrhythmias • No Response to NTG

12/29/14
17
Under Sedation/GA?? • Evidence of Myocardial Ischemia?
• Downgoing ST Segment
Under Sedation/GA?? • Evidence of Myocardial Infarction?
• Elevated ST Segment
Under Sedation/GA?? • Onset of New Major Cardiac Dysrhytmias?
• Heart Blocks, Especially Advanced • PVCs • Runs of V-Tach • Unexplained Sinus Tachycardia OR Bradycadia • Pulseless Rhythms
Chest Pain - Treatment • If + History of Angina & Pain Typical • Position to Comfort • Vital Signs • Yes → NTG 0.3 - 0.4mg Q 5 Min Sublingual Spray or Tablet X 2 to Decrease O2 Demand • Caution: Phosphodiesterase 5 Inhibitors
• Supplemental O2 • Resolution → ?? Continue Treatment • No Resolution → Activate EMS, Possible MI • NTG Again, BLS If Needed
Chest Pain - Treatment • No Hx of Angina or Atypical Chest Pain • BLS, Vital Signs, Loosen Clothing • Activate EMS - Assume MI • Consider Trendelenberg if ↓ BP • Treatment
• Morphine (N2O/O2?)
• Oxygen – How Much??? • Nitroglycerin sublingual (BP > 90 mmHg) • Aspirin – 160 - 325mg Chewable
• If Sedation/GA → Wake Up Patient

12/29/14
18
THANK YOU Questions????