updated beers criteria for potentially inappropriate · pdf fileupdated beers criteria for...
TRANSCRIPT


Updated Beers Criteria for Potentially Inappropriate
Medication Use in Older Adults
Dr. Janice Hoffman, PharmD, CGP, FASCP
Dr. Sam Shimomura, PharmD, CGP, FASHP
Western University of Health Sciences
College of Pharmacy
October 2016

Disclosure
Dr. Janice Hoffman has no conflict of interest to disclose.
Dr. Sam Shimomura has no conflict of interest to disclose.

Pharmacist Learning Objectives
• Describe the physiological changes that occur in aging and how that may affect pharmacokinetics
• State at least three principles to consider when prescribing or recommending drug therapy for older adults
• Apply Beer’s Criteria to patient cases

• Identify the key physiological changes that occur in aging.
• List three characteristics of medications that meet the Beer’s
Criteria.
• Identify from patient cases at list 3 medications that are
potentially not appropriate in the elderly according to Beer’s
Criteria.
Pharmacy Technician Learning Objectives

Physiological changes with aging

Pharmacotherapy in elderly is complicated by multi-factorial issues
◦ Age related physiologic changes
◦ Presence of multiple chronic disease states
◦ Cognitive changes
◦ Physical disabilities
◦ Patients desire vs.
ability to comply to recommended medications
Pharmacotherapy

Increased prevalence of disease
Difficulty in differentiating often subtle adverse effects from the disease
Drug-Disease Interaction or Exacerbation
◦ Anticholinergic drugs
◦ BPH
◦ Constipation
◦ Alzheimer’s Disease
◦ Confusion
◦ Benzodiazepines
◦ Depression
◦ Dementia
◦ Gait
Change in Disease States
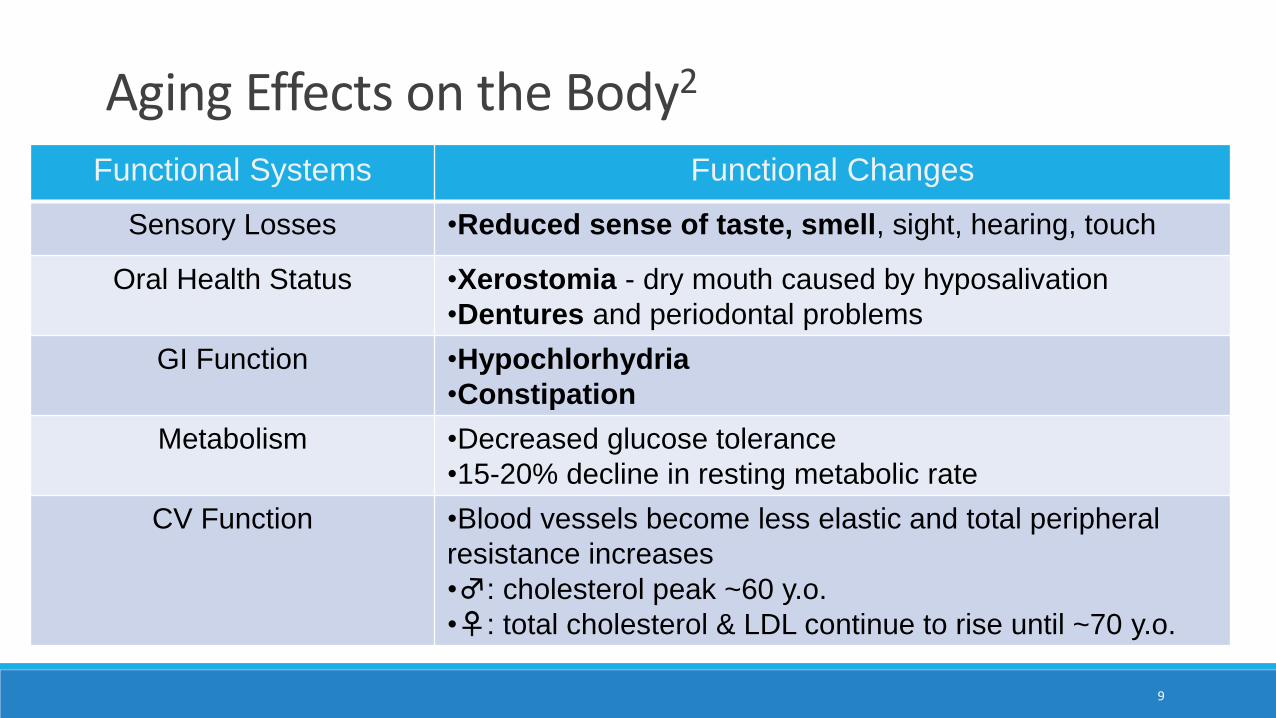
Aging Effects on the Body2
Functional Systems Functional Changes
Sensory Losses •Reduced sense of taste, smell, sight, hearing, touch
Oral Health Status •Xerostomia - dry mouth caused by hyposalivation
•Dentures and periodontal problems
GI Function •Hypochlorhydria
•Constipation
Metabolism •Decreased glucose tolerance
•15-20% decline in resting metabolic rate
CV Function •Blood vessels become less elastic and total peripheral
resistance increases
•♂: cholesterol peak ~60 y.o.
•♀: total cholesterol & LDL continue to rise until ~70 y.o.
9

If Sally is 97 years old woman who is not eating well which of the following changes from aging may be contributing?
A. Increase in drooling or hypersalivation to accommodate dentures
B. Blood vessels become more elastic causing weakening in the legs
C. Loss in sensory functions (smell, taste and sight)
D. Increased gastric motility causing her to feel “full” faster
Question # 1

Most oral drugs are absorbed via passive diffusion
◦ No major changes in bioavailability of drug due to age-related physiologic changes
Decreased first-pass effect
(e.g. Morphine, propranolol)
results in :◦ increased bioavailability
◦ higher plasma concentrations
Changes in Absorption1

skin hydration
surface lipids
peripheral circulation
keratinization
Outcome: Possible absorption from a transdermal patch
Transdermal Absorption1

gastric emptying rate
intestinal motility
intestinal blood flow and surface area
gastric acid output - gastric pH
Outcome:
◦ No significant change in quantity absorbed
◦ Time to onset or peak may be delayed
GI Absorption1

muscle mass
peripheral circulation
connective tissue
Outcome: possible Intramuscular absorption
IM absorption1

Physiologic Changes
◦ in total body water
◦ Volume of distribution of hydrophilic drugs is
◦ in lean body mass (Scr will be )
◦ in body fat
◦ Volume of distribution of lipophilic drugs is
◦ in albumin
Distribution1

serum albumin
protein affinity binding
alpha 1- acid glycoprotein
Outcome: Increased free fraction of highly protein-bound medications
Protein Binding Changes1

We find out that Sally our 97 years old patient is not eating well due to her Depression. Which of the following physiologic complications may occur?
A. Increase in body fat will lead to larger distribution of hydrophilic drugs
B. Decrease in albumin will lead to more free drug and more adverse effects
C. Decrease stomach acid will lead to more drug being absorbed
D. Increased absorption from a transdermal patch
Question # 2

Liver is the major organ for metabolism :
Aging leads to:
◦ hepatic mass
◦ hepatic blood flow
Decreased phase-I metabolism (oxidation)
◦ clearance half life of drug Side effects
◦ (e.g.. Diazepam, theophylline, quinidine, alprazolam)
Phase II metabolism (conjugative)
◦ Less affected by age (e.g.. Lorazepam, oxazepam)
CYP 450 activity – limited changes
Metabolism2

Aging and CYP Activity2
Decreased Decreased or Unchanged
Increased
CYP 1A2CYP 2C19
CYP 2ACYP 2C9CYP 3A4
CYP 2D6
19Cusack. Am Geriatr Pharmacother 2004: 2:274: 302

Other metabolic Influences2
Factor Result
Smoking Enzyme Induction
Alcohol Enzyme Induction
Drugs Enzyme Induction/Inhibition
Diet Variable
Malnutrition Enzyme Inhibition if severe
Frailty Enzyme Inhibition
20

Physiologic Changes
◦ Renal blood flow
◦ GFR – creatinine clearance (CrCl)
◦ Tubular secretion function
◦ Stable serum creatinine due to muscle mass
Outcome:
CrCl by 50% between age 25 - 85 despite maintained SCr of 1.0 mg/dL.
Renal Excretion1

Clinical Effects:
◦ half life of renally excreted drugs
◦ concentration of renally excreted drugs
Significant for narrow therapeutic index
◦ Aminoglycosides
◦ Anticoagulants
Primary goal: prevent toxicity
Clinical Application of Renal Changes1

We also find out that our 97 year old patient smokes a pack of cigarettes daily and drinks 2 glasses of wine with dinner every night. How will these lifestyle choices affect her medications? Select the BEST answer
A. Decrease renal elimination of her medications
B. Contribute to liver enzyme Induction increasing hepatic elimination of her medications
C. Enhance topical absorption of transdermal patches increasing adverse effects
D. Decreased GI pH ( more acidic) increasing oral absorption of her medications
Question # 3

Alterations in sensitivity to drugs with age
◦ Receptor sensitivity to:
◦ benzodiazepine, warfarin, opioids
◦ side effects
◦ Receptor sensitivity to beta-blockers
◦ Baroreceptor sensitivity
◦Orthostatic hypotension with
◦ vasodilators, tricyclic antidepressants, antihypertensives
◦ Outcome: FALL risk1
Pharmacodynamics

•Receptor changes
• in number of some receptors (β receptors)
•Altered reserve capacity
•Homeostatic changes
•Increased sensitivity to drug therapeutic & adverse effects
•Increased co-morbid diseases
•Increased drug interactions from polypharmacy1
Etiology for Altered Pharmacodynamics

• Antipsychotic agents - risk of Tardive Dyskinesia and psuedoparkinsonism (receptor sensitivity)
• sensitivity to anticholinergics increased side effects
• sensitivity to warfarin risk of bleeding
• renin and aldosterone levels response to ACE-I
• NSAID, ACE-I, K+ sparing diuretics risk of hyperkalemia1
Pharmacodynamics – Outcomes

“ The genes you are born with are the genes you die with”B. Williams USC
No apparent changes during adult lifespan
◦ Possible decreased in CYP 3A4 and CYP 2A6
◦ Fast and slow metabolizers (ethnicity)
◦ N-acetyltransferase activity
◦ Slow acetylators (autosomal recessive)1
Pharmacogenomic Issues

Clinical response =
PK + PD + Individual variance ???(Brad Williams USC professor)
Applying these principles to patients ……


Dr. Mark Howard Beers with a team from Harvard, looked atprescriptions and case files for 850 residents of nursing homesaround Boston.
Researcher’s found that sedatives, antidepressants andantipsychotic drugs often caused confusion or even physicaltremors in patients.
The teams finding were published in The Journal of theAmerican Medical Association in 1988.
Beers Criteria History

This Boston study led to establish a list of drugs with knownside effects on elderly.
◦ In the year 1991,this list of drugs was published known asBeers Criteria.
◦ Consist of Potentially Inappropriate Medications (PIM) for use in older adults
Beer’s Criteria History

Incorporated new evidence on currently listed PIMs andevidence from new medications or conditions not addressed inthe 2012 update.
Incorporated 2 new areas of evidence on drug-druginteractions and dose adjustments based on kidneyfunction for select medications.
Grade the strength and quality of each PIM statement basedon level of evidence and strength of recommendation.6
2012 AGS Beers update used the following criteria:

Improve care of older adults
By reducing their exposure to Potentially InappropriateMedications (PIM).
Provide the evidence to support the PIM8
Goal of 2015 AGS Beers Criteria

Exclusion
• Age less than 65
• Hospice & Palliative care
Inclusion
• Age 65 and older
• Intended for use in ambulatory, acute, and institutionalized setting of care in the United States.
Beers Criteria
Modified Delphi method was used to systematically review and grade the evidence.

Renal Adjustment for drug
• Previously marked as “avoid”
Drug-Drug Interactions
Effects of drug-drug
interactions
Clarification of drugs from
2012 list
New ADDED changes in 2015 update

Table 2 Beer’s Potentially Inappropriate Medication(PIM) in Elderly : 2015 update
Additions to Table 2 PIM Deletions to Table 2 PIM
PPI’s for duration > 8 weeks Anti-arrhythmic drugs (Class 1a,1c, III
except amiodarone) as first-line
treatment for atrial fibrillation
Desmopressin Trimethobenazmide
*Independent of Diagnoses or Condition10

Table 3 Beer’s in Elderly : 2015 update
(Drug-drug and Drug-Disease Interactions)
37
Medication ADDED to Table 3 REMOVED
Falls and fractures- Opioids Chronic Constipation- Entire criterion
Insomnia- Armodafinil & Modafinil Lower urinary tract- Inhaled anticholinergic
drugs
Dementia or cognitive impairment-
Eszopiclone & Zaleplon
Delirium- Antipsychotics
10

Table 5: Potentially clinically important Drug-Drug Interactions
that should be avoided in older adults 10
Object
Drug and
Class
Interacting
drug and
class
Risk
Rationale
Recommendation Quality of
Evidence
Strength of
recommendation
Antidepressant
(i.e., TCAs and
SSRIs)
≥2 other
CNS-active
drugs
Increased
risk of falls
Avoid total of ≥3
CNS-active drugs Moderate Strong
Antipsychotic
≥2 other
CNS-active
drugs
Increased
risk of falls
Avoid total of ≥3
CNS-active drugs Moderate Strong
Hypnotics ≥2 other
CNS-active
drugs
Increased
risk of falls
Avoid total of ≥3
CNS-active drugs High Strong
39

Table 5: Potentially clinically important Drug-Drug Interactions that
should be avoided in older adults10
Object
Drug and
Class
Interacting
drug and
class
Risk
Rationale
Recommendation Quality of
Evidence
Strength of
recommendation
Corticosteroids
(po/iv)
NSAIDs
Increased
risk of
peptic
ulcer/GI
bleeding
Avoid; if not
possible provide
GI protection Moderate Strong
Lithium ACEIs
Increased
risk of
toxicity
Avoid, monitor
lithium conc. Moderate Strong
Warfarin Amiodarone
Increased
risk of
bleeding
Avoid when
possible;
Monitor INR
Moderate Strong
40

Table 6: Non-Anti-Infective medications to AVOID or dose REDUCE in
impaired kidney function in > 65 years10
Medication
Class/
Medication
Creatinine
Clearance
(ml/min)
Rationale Recommendation Quality
of
Evidence
Strength of
Recommendation
Cardiovascular/Hemostasis
Amiloride <30 ↑Potassium
↓ Sodium
Avoid Moderate Strong
Apixaban <25 ↑ bleeding Avoid Moderate Strong
Dabigatran <30 ↑ bleeding Avoid Moderate Strong
Edoxaban
30-50 ↑ bleeding Reduce dose
Moderate Strong<30 or
>95
Avoid
41

Table 6: Non-Anti-Infective medications to AVOID or dose REDUCE in
impaired kidney function in > 65 years 10 (cont. 2)
Medication
Class/
Medication
Creatinine
Clearance
(ml/min)
Rationale Recommendation Quality of
Evidence
Strength of
Recommendation
Cardiovascular/Hemostasis
Enoxaparin <30 ↑ bleeding Reduce dose Moderate Strong
Fondaparinux <30 ↑ bleeding Avoid Moderate Strong
Rivaroxaban 30-50 ↑ bleeding Reduce dose Moderate Strong
Spironolactone <30 ↑Potassium Avoid Moderate Strong
Triamterene <30 ↑ Potassium
↓ SodiumAvoid Moderate Strong
42

Table 6: Non-Anti-Infective medications to AVOID or dose REDUCE in impaired
kidney function in > 65 years 10 (cont. 3)
Medication Creatinine
Clearance
(ml/min)
Rationale Recommendation Quality
of
Evidence
Strength of
Recommendation
Central Nervous System and Analgesics
Duloxetine <30 GI adverse
effects
Avoid Moderate Weak
Gabapentin <60 CNS adverse
effects
dose Moderate Strong
Levetiracetam ≤80 CNS adverse
effects
dose Moderate Strong
Pregabalin <60 CNS adverse
effects
dose Moderate Strong
Tramadol <30 CNS adverse
effects
Immediate
release: dose
ER: Avoid
Low Weak
43

Which of the following medications according to the Beer’s Criteria Update 2015 should be absolutely be AVOIDED in an elderly patient with a CrCl < 30 ml/min due to risk of complications?
A. Spironolactone due to risk of decreased potassium
B. Apixaban due to increased risk of bleeding as
C. Tramadol ER due to risk of increased CNS side effects
D. Risperdone due to increased risk of Tardive Dyskinesia
Question #4

Stakeholders and Star Ratings
In 2007 star rating were created by CMS to help beneficiaries select insurance plans
◦ Plans were rated based on HEDIS scores, CMS Outcome scores and CMS data
◦ A 5-point scale - 5 = excellent and one was poor
CMS met with 15 pharmacy associations, pharmacy benefit management companies and pharmacy chains in 2013
◦ Outcomes: If health plans collaborate with community improved star ratings
45

Active Learning: Case Studies
Please work in groups of MAX 6 people
Refer to separate sheets on table
46
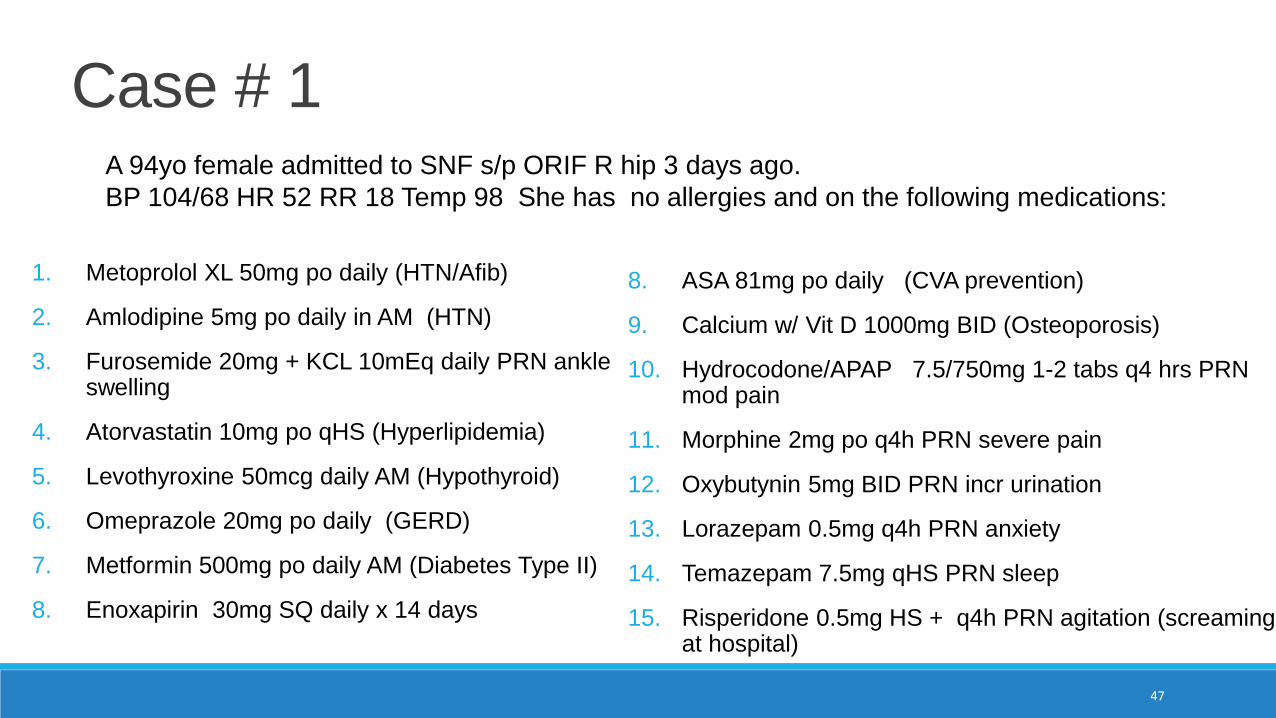
Case # 1
1. Metoprolol XL 50mg po daily (HTN/Afib)
2. Amlodipine 5mg po daily in AM (HTN)
3. Furosemide 20mg + KCL 10mEq daily PRN ankle swelling
4. Atorvastatin 10mg po qHS (Hyperlipidemia)
5. Levothyroxine 50mcg daily AM (Hypothyroid)
6. Omeprazole 20mg po daily (GERD)
7. Metformin 500mg po daily AM (Diabetes Type II)
8. Enoxapirin 30mg SQ daily x 14 days
8. ASA 81mg po daily (CVA prevention)
9. Calcium w/ Vit D 1000mg BID (Osteoporosis)
10. Hydrocodone/APAP 7.5/750mg 1-2 tabs q4 hrs PRN mod pain
11. Morphine 2mg po q4h PRN severe pain
12. Oxybutynin 5mg BID PRN incr urination
13. Lorazepam 0.5mg q4h PRN anxiety
14. Temazepam 7.5mg qHS PRN sleep
15. Risperidone 0.5mg HS + q4h PRN agitation (screaming at hospital)
47
A 94yo female admitted to SNF s/p ORIF R hip 3 days ago.
BP 104/68 HR 52 RR 18 Temp 98 She has no allergies and on the following medications:

Which of the following medications that is on the Beer’s Criteria can easily be discontinued?
A. Metoprolol XL
B. Omeprazole
C. Metformin
D. Risperidone PRN
Question #5
Case #1 Target #1
1. What meds could would be considered Potentially Inappropriate Medications according to the Beer’s Criteria ?
49

Case #1 Target #2
2. What labs should be monitored ?
50

Case #1 Target #3
3. What potential drug-drug interactions exist in her medication regimen?

Case #1 Target #4
4. What ADR would you be concerned about?
52

Case #1
5. How should Antipsychotics be used in SNF ? What are their risks vs. their benefits?

References
54
1. Cusack. Am Geriatr Pharmacother 2004: 2:274: 3022. O’Mahoney&Woodhouse. Pharmacol Ther 1994;61:279-2873. Resnik B, Pacala JT. 2012 Beers Criteria. J AM Geriatr Soc; 2012; 60:612-613 DOI 10.1111/j.1532-5415.2012.03921.4. Beers, MH. Explicit criteria for determining potentially inappropriate medication use by the elderly. An update. Arch Intern
Med 1997; 157: 1531-15365. Fick DM, Cooper JW, Wade WE et al. Updating the Beers Criteria for Poteintally Inappropriate Medication Use in Older
Adults: Results of consensus panel of experts. Arch Intern Med 2003; 163: 2716-27246. The American Geriatrics Society 2012 Beers Criteria Update Expert Panel. AGS updates Beers Criteria for potentially
inappropriate medication use in older adults. J AM Geriatr Soc; 2012; 60: 616-631 7. Steinmen, MA, Beizer, JL, DuBeau, CE, et al. How to Use the American Geriatrics Society 2015 Beers Criteria-a Guide for
Patients, Clinicians, Health Systems, and Payors. J AM Geriatr Soc; 2015; 63: e1-e78. The American Geriatrics Society 2015 Beers Criteria Update Expert Panel. American Geriatrics Society 2015 Updated Beers
Criteria for Potentially Inappropriate Medication Use in Older Adults. J AM Geriatr Soc; 2015; 63: 22227-2246 9. McCormick WC. American Geriatrics Society response to letter to the editor from Marc S. Berger “Misuse of Beers Criteria”
July 2014. J. Am Geriatr. 2014; 62(12): 2466-246710. 2015 AGS Beers Criteria and Evidence Tables. http://geriatricscareonline.org/toc/american-geriatrics-society-updated-
beers-criteria-for-potentially-inappropriate-medication-use-in-older-adults/CL001 Published 2015 Accessed 6.20.201611. Hanlon JT, et al. Alternative medications for medications in the use of high-risk medications in the elderly and potentially
harmful drug-disease interactions in the elderly quality measures. J Amer Geriatr Soc 2015;63:e8-e18

AcknowledgementsThank you to
◦ Aida Oganesyan, PharmD
◦ Brad Williams PharmD
◦ Azin Keyvani, PharmD Candidate 2017
◦ Mariam Khachatryan, PharmD
55

1. Write down the course code. Space has been provided in the daily program-at-a-glance sections of your program book.
2. To claim credit: Go to www.cshp.org/cpe before December 1, 2016.
Session Code: