update on the pathogenesis of rheumatoid...
TRANSCRIPT

Update on the Pathogenesis of Rheumatoid Arthritis
Professor Ernest ChoyHead of Rheumatology and Translational Research
Institute of Infection and ImmunityDirector of Arthritis Research UK and Health and Care
Research Wales CREATE Centre
1

C
H
R
O
N
I
C
I
N
F
L
A
M
M
A
T
I
O
N
TNFα
IL1
IL15
IL18
IL6
IL20
IL32
IL33
RANKL
GM-CSF
IL10
IL1Ra
IL18BP
sIL1R
sTNFR
IL27
IL35
TGFβ
Cytokines promote inflammatory synovitis
Firestein GS, et al, eds. Kelley’s Textbook of Rheumatology. 8th ed. Philadelphia: Saunders Elsevier; 2009:376.
B cell
Endothelial
cell
Tissue
cell
Mast cell
Neutrophil
Synoviocytes
Cell contact, co-stimulation
Macrophage
IL17
IL22
IL-17, IL-22
IFNγ
IL-12, IL-23
chemokines, ECM,
co-stimulation
Th1/Th17
DC
2

Cytokines are implicated in each phase of RA pathogenesis
3
Cellular
recruitment
Immunologic
activation and
organization
Cellular
retention and
survival
Tissue
response
McInnes IB, Liew FY. Nat Clin Pract Rheumatol. 2005;1:31-39; 2. Schett G, et al. Arthritis Rheum. 2008;58:2936-2948.
Adapted and reprinted by permission from Macmillan Publishers Ltd: Nat Clin Pract Rheumatol. 2005.

PsA and RA were originally treated as the same disease• Not until the 1950s were the typical features of PsA described1
• Before Moll and Wright produced the first classification of PsA, disease descriptions included:2
• Arthritis confined to the DIP joints with psoriasis
• Atypical arthritis with atypical psoriasis
• Arthritis following prolonged, uncontrollable psoriasis
• Coincident psoriasis and RA – there being no distinct entity
• Classification criteria have evolved to address the difficulty in PsA diagnosis1,3
• Still, joint involvement in psoriasis/PsA is often treated in the same way as RA, with drugs known to be ineffective against some PsA symptoms4
AS, ankylosing spondylitis;
RA, rheumatoid arthritis; DIP, distal interphalangeal.
1. Moll J and Wright V. Semin Arthritis Rheum 1973;3:55–78; 2. Wright V. Arthritis &
Rheumatology 1978;21:619–33; 3. Helliwell P, et al. Ann Rheum Dis 2005;64(Suppl II):ii3–ii8.
doi: 10.1136/ard.2004.032318; 4. Kingsley G, et al. Rheumatology (Oxford) 2012;51:1368–377.
4

α chain
β chain
Gregersen PK, et al. Arthritis Rheum 1987;30:1205–13.
DR type Sequence Association
70 71 72 73 74
DR4 -W4 Q K R A A Positive
-W14 Q R R A A Positive
-W15 Q R R A A Positive
DR1 Q R R A A Positive
DR4 -W10 D E R A A Negative
-W13 Q K R A A Negative
HLA-DR associations with
rheumatoid arthritis defined by DR
β1 sequence position 70–74
Q=glutamine; K=lysine; R=arginine; A=alanine
D=aspartic acid; E=glutamic acid
Class II genes account for about 30% of genetic susceptibility to RA
5
HLA-DR=human leukocyte antigen D-related.

Current RA genetic risk loci from GWAS
6
McAllister Open Access Rheumatol. 2011; 3: 31–46.

Citrullination is a process of protein modification
7
Van Venrooij WJ, et al. Arthritis Res. 2000;2:249-51 PAD, peptidyl arginine deiminase

16
PAD expression in the lung
8
Luigli EB, et al. Arthritis Res Ther 2015;17:9

Citrullination improved peptide binding to come HLA class II alleles and leads to T-cell activation
9
Adapted from Hill JA, et al. J Immunol 2003; 171:538–41.

20
ACPA and RF precede RA
Adapted from 1. Nielen MM, et al. Arthritis Rheum 2004;50:380–6. 2. Rantapaa-Dahlqvist S, et al. Arthritis Rheum 2003;48:2741–9.

Immune response develops Pathologic inflammatory response
Genetic and environmental factors
Synovial inflammation
Humoral
immunity
Complications
comorbidities
Joint destruction
Time
ACPA=anti-citrullinated protein antibodies; mφ=macrophage; MHC=major histocompatibility complex; RF=rheumatoid
factor; TCR=T-cell receptor.
Adapted from Klareskog, et al. Lancet 2009;373:659–72.
ACPA
RF
Evolution of rheumatoid arthritis
mφ
Immune
complexes
Activated
macrophages
T cell
B cell
Activated
T cell
mφ
Activated
B cells
TCR
MHC II
11

Prognostic value of ACPA in patients with recent-onset RA
12
Kroot EJ, et al. Arthritis Rheum 2000;43:1831–5. Schellekens GA, et al. Arthritis Rheum 2000;43:155–63.

ACPA or CCP?
13
1. Van Gaalen FA, et al. Ann Rheum Dis 2005;64:1510–2. 2. van Steendam K, et al. Rheumatology (Oxford). 2001;50:830–7.

1
Several epitopes are recognised by ACPAs
14
Ioan-Facsinay, et al. Ann Rheum Dis. 2011;70:188–93; Wagner CA, et al. Ann Rheum Dis 2015;74:579–86.

Poor prognostic factors in RA
15
Smolen JS, et al. Ann Rheum Dis 2013;3:529–35.

ACPAs form immune complexes to activate macrophages
16
Adapted from Nimmerjahn F and Ravetch JV. Nat Rev Immunol 2008;8;34–47

Percentage of early RA with erosions by serology
Katchamart W et al. Rheumatol Int. 2015,35:1693-1699
17

Percentage of early RA with erosions by serology after 1 year
18
Katchamart W et al. Rheumatol Int. 2015,35:1693-1699

23
19
Reproduced from: Kleyer A, et al. Ann Rheum Dis. 2014;73:854–60
Changes in cortical bone structure

ACPA and osteoclast differentiation
20
Adapted from Harre U, et al. J Clin Invest 2012;122:1791–802.

24
Interaction between ACPA and RF in RA-mediated bone loss
21
Adapted from Hecht C, et al. Ann Rheum Dis 2015;74:2151–6.

19
Moving from citrullination to ACPA
22
Adapted from Klareskog L, et al. Annu Rev Immunol 2008;26:651–75.

23
Demoruelle MK et al Arthritis Rheumatol; 2017; 69:1165-75
Sputum ACPAs and NETs in FDRs of RA patients

Sputum ACPAs and NETs in FDRs of RA patients
24
Demoruelle MK et al Arthritis Rheumatol; 2017; 69:1165-75

Porphyrymonas gingivalis citrullinatesbacterial and human proteins• This organism and several other common infectious
agents have been suggested to trigger RA
• Generally via molecular mimicry
Wegner N, et al. Arthritis Rheum 2010;62:2662–72.
25

18
Classification and disease duration
26Adapted from van Steenbergen HW, et al. Arthritis Rheum. 203;65:2219–32. Raza K, et al. Ann Rheum
Dis. 2012;71:1921–3. Willemze A, et al. Nat Rev Rheumatol 2012;8:144–52.

The cells and cytokines involved in the pathogenesis of psoriasis, PsA, and RA
Coates LC, et al. Semin Arthritis Rheum. 2016;46(3):291-304.
27
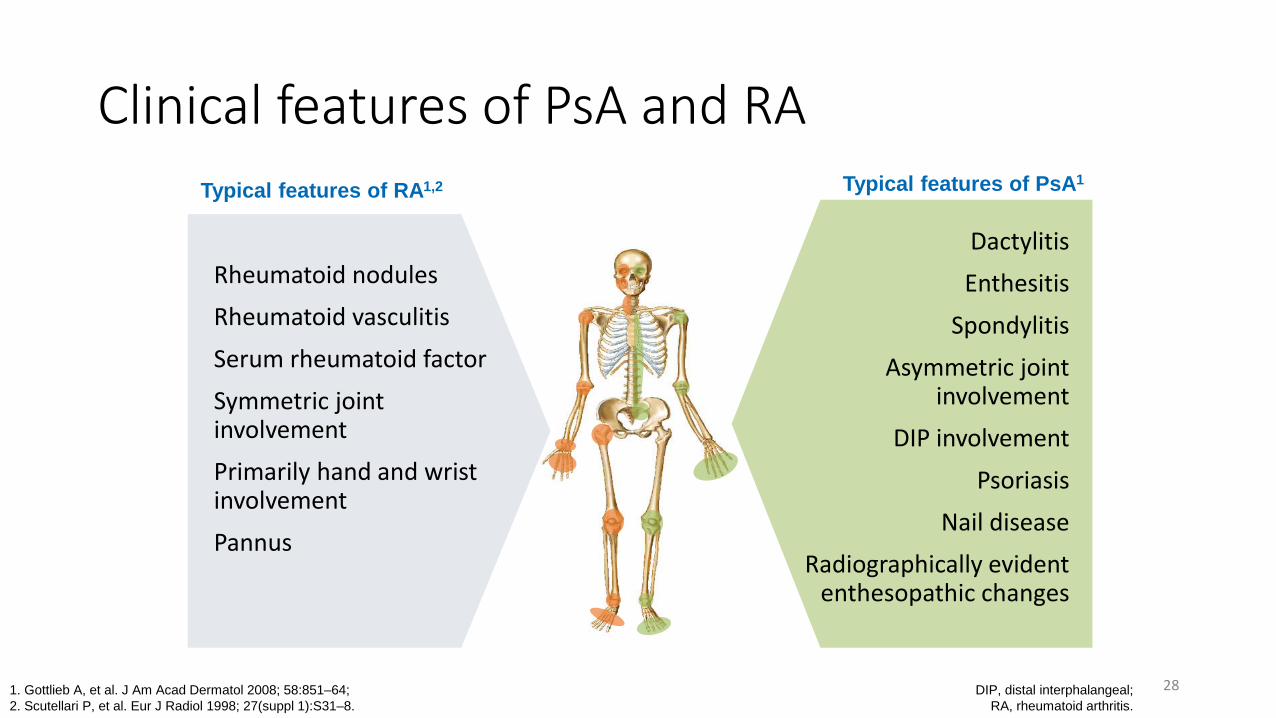
Clinical features of PsA and RA
DIP, distal interphalangeal;
RA, rheumatoid arthritis.
1. Gottlieb A, et al. J Am Acad Dermatol 2008; 58:851–64;
2. Scutellari P, et al. Eur J Radiol 1998; 27(suppl 1):S31–8.
Dactylitis
Enthesitis
Spondylitis
Asymmetric joint involvement
DIP involvement
Psoriasis
Nail disease
Radiographically evident enthesopathic changes
Rheumatoid nodules
Rheumatoid vasculitis
Serum rheumatoid factor
Symmetric joint involvement
Primarily hand and wrist involvement
Pannus
Typical features of PsA1Typical features of RA1,2
28

Genomic analysis highlights differences between PsA and RA
OR, odds ratio; RA, rheumatoid arthritis,
SNP, single nucleotide polymorphism.
1. Belasco J, et al. Arthritis Rheumatol 2015;67(4):934–44;
2. Bowes J, et al. Ann Rheum Dis 2012;71:1350–354.
OR plots for eight SNPs demonstrating evidence for association to PsAsusceptibility, highlighting the opposing direction of effectsfor REL, PLCL2 and KIF5A.
29

MHC-1-opathy versusautoimmunity
30ERAP, endoplasmic reticulum aminopeptidase; IL, interleukin;
MHC, major immunohistocompatibility complex.
Feature MHC-I-opathy Autoimmune disease
Sex No femalepredominance Femalepredominance
Age of onset Generally young Wide agerange
Eye disease Anterior or posterior uveitis, orboth
Can includescleritis
Injury Linked to tissue-specific injury No link
Barrierfunction perturbation
Skin, mouth, gut Absent
Course without therapy Waxing and waning Progressive
Genetics MHC-1, ERAP1/2, IL-23/IL-17 axis MHC-II
Gut involvement Clinical or subclinical gutdisease iscommon
No link to gut disease(except coeliac disease)
Therapy Respond to anticytokine therapy, but not B-cell depletion
May respond to anticytokine therapy and B-celldepletion
Joint disease Sites of mechanical stress(entheses and lower limbs)
Polyarticular and synovial
Underpinning theory Danger as immunologicaldriver Self versus non-self discrimination
Comparison of the features of MHC-1-opathies and autoimmune diseases
.
McGonagle D, et al. Nat Rev Rheum 2015;11:731–740.

Differentiation of RA and the diffuse inflammation in PsA
• Early in RA joint disease localisation is to the synovium• Synovium the primary target organ
• In early PsA the inflammatory changes have a widespread distribution• Appear to relate to patterns of joint
stressing around ligaments, adjacent bone and soft tissues
• As opposed to a specific antigen territory
DIP, distal interphalangeal;
RA, rheumatoid arthritis.McGonagle D, et al. PLoS Medicine 2006;3(8):1242–248.
PsA: DIP joint with extensive inflammatory
changes in all tissues
31

The physiology of entheses‒ the enthesis organ (more than an insertion)• Neighbouring tissues are also involved in the dissipation of stress1
• Periosteal and sesamoid fibrocartilage, bone, soft tissues, synovium
• Widespread stress dissipation may explain the diffuse tissue swelling observed in SpAs2
SpA, spondyloarthropathy.
1. Benjamin M, et al. Arthritis & Rheumatism 2004;50:3306–313;
2. Eshed I, et al. Ann Rheum Dis 2007; 66(12):1553-559 ;
3. McGonagle D, et al. Arthritis Rheum 2007;56(8):2482–491;
4. McGonagle D. http://enthesis.info/anatomy/synovio-entheseal_complex.html (Accessed Aug 2016).
• The synovio-entheseal complex (SEC) can form part of the enthesis organ3
• Damage to the enthesis by micro-damage or other mechanisms can lead to inflammation of the SEC due to their close association3
32

Model for how enthesitis leads to joint and bone damage
SEC, synovio-entheseal complex.
1. McGonagle D. http://enthesis.info/damage/fibrocartilage_microdamage.html (accessed Oct 2016); 2. McGonagle D.
http://enthesis.info/damage/microscopic_inflammation_in_normal_insertions.html (accessed Oct 2016);3. McGonagle D, et al. Lancet 1998;352(9134):1137–140;
4. McGonagle D, et al. PLoS Medicine 2006;3(8):1242–248; 5. Tan A, McGonagle D. Imaging of psoriatic arthritis in Atlas of PsA. 2005. Mease & Helliwell, ed.
Progression
Mechanical stressing can lead to micro-
damage and micro-inflammation
at normal entheses1,2
Diffuse inflammation occurs across all structures of the
entheseal organ and SEC4
In psoriasis/PsA patients, a dysregulated inflammatory
response occurs at the enthesis3
Enthesitis
Cytokines/growth factor
Primary enthesitis
Osteolysis occurs from persistent inflammation5
33

IL-23 induces spondyloarthropathy by acting on ROR-γt+ CD3+CD4−CD8− entheseal resident T cells
Sherlock JP et al. Nat Med. 2012 Jul 1;18(7):1069-76.
34

IL-23 drives entheseal-resident T cells in the pathogenesis of spondyloarthritis
Lories RJ and McInnes IB Nat Med 2012;18:1018-9
35

Kirkham B et al. Immunology. 2014 Feb;141(2):133-42.
36

Cytokine targets in inflammatory arthritisRA PsA AS
TNF +++ +++ +++
IL-6 +++ +1 - 2
IL-17 +3 +++ +++
IL12/23 - 4 +++ +5
JAK +++ +++ +6
37
+++: approved treatment or positive phase III trial++: not approved but positive phase III trial+: not approved but limited efficacy from phase II or III clinical trials-: negative clinical trial
1. Mease PJ, et al. Arthritis Rheum 2016;68:2163–73. 2. Sieper J, et al. Ann Rheum Dis 2014;73:95–100. 3. Rheumatol Ther. 2017;4:475-488.
4. Smolen J, et al. Ann Rheum Dis. 2017;76:831-839. 5. Poddubnyy D, et al. Ann Rheum Dis. 2014;73:817-23. 6. van der Heijde D, et al. Ann Rheum Dis 2017;0:1–8

Regulation of autoantibody activity by the IL-23-Th17 axis determines the onset of autoimmune disease
38
Collagen induced arthritis
WT
IL-23-/-
Pfeifle R et al. Nat Immunol 2017;18:104-113

Regulation of autoantibody activity by the IL-23-Th17 axis determines the onset of autoimmune disease
39
Pfeifle R et al. Nat Immunol 2017;18:104-113
TNF
B cells
T cellsIL-6
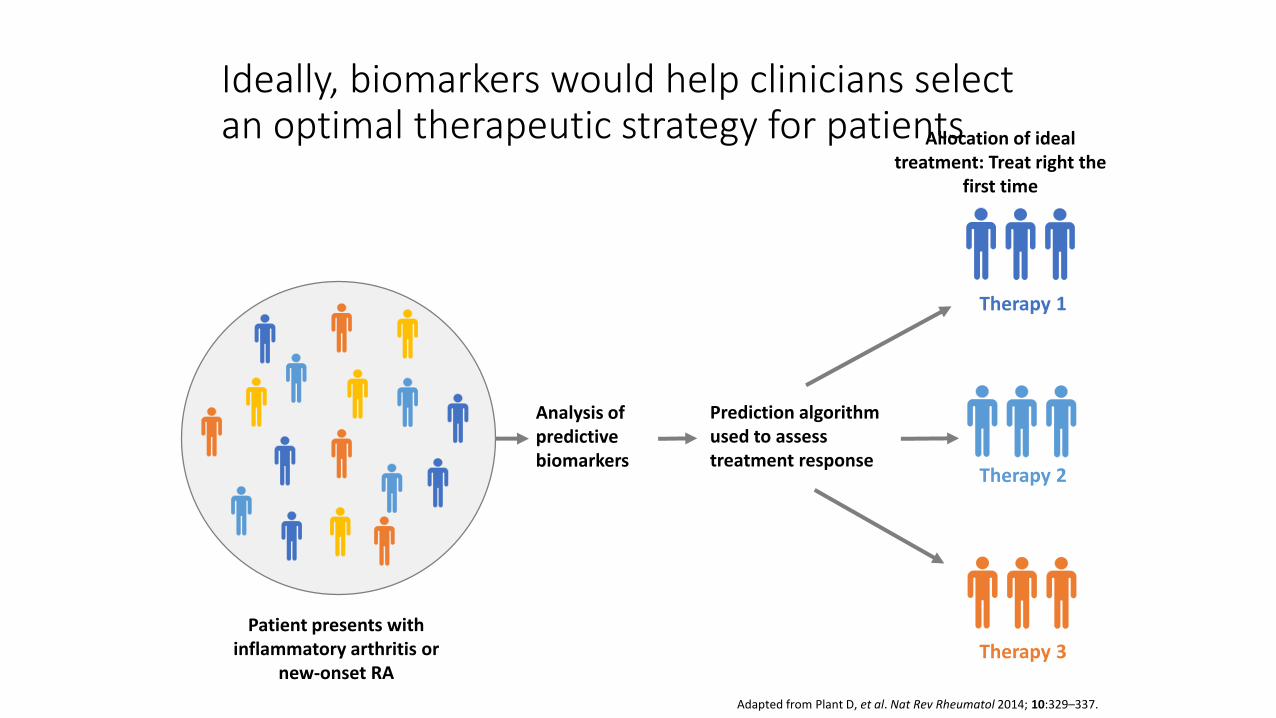
Ideally, biomarkers would help clinicians select an optimal therapeutic strategy for patients
Adapted from Plant D, et al. Nat Rev Rheumatol 2014; 10:329–337.
Analysis of predictive biomarkers
Prediction algorithm used to assess treatment response
Therapy 1
Therapy 2
Therapy 3
Patient presents with inflammatory arthritis or
new-onset RA
Allocation of ideal treatment: Treat right the
first time
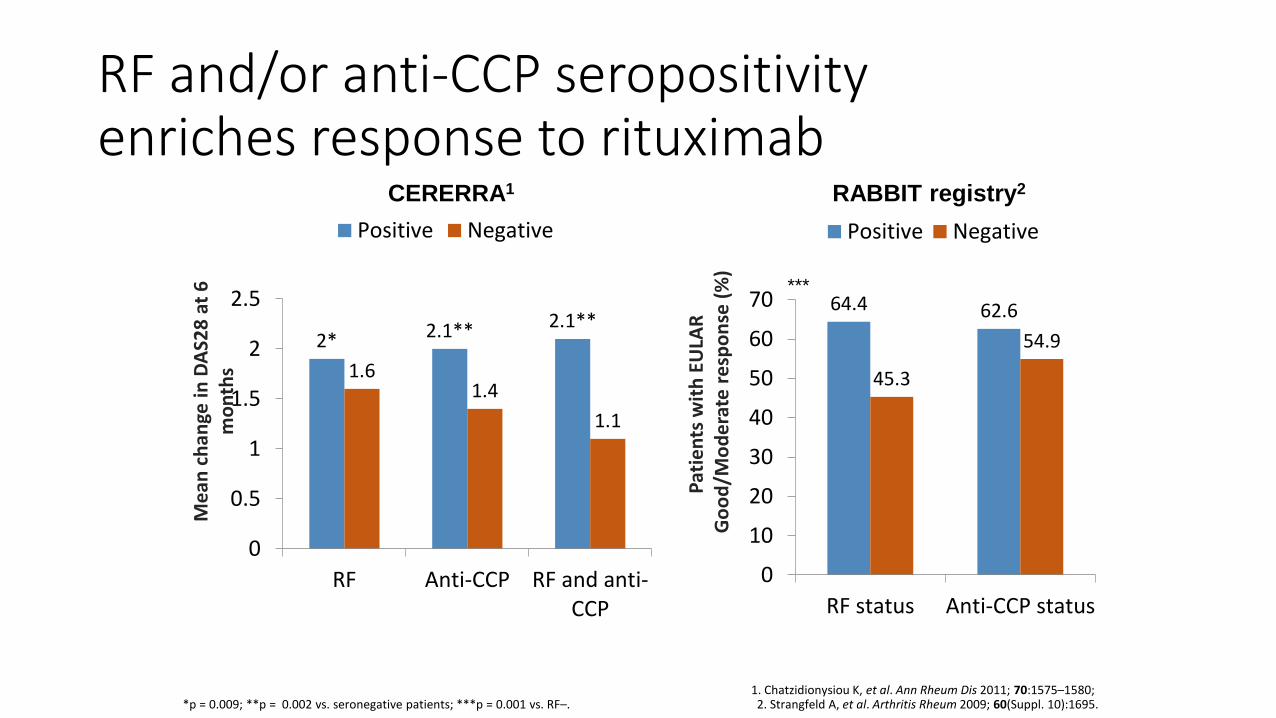
RF and/or anti-CCP seropositivity enriches response to rituximab
*p = 0.009; **p = 0.002 vs. seronegative patients; ***p = 0.001 vs. RF–.1. Chatzidionysiou K, et al. Ann Rheum Dis 2011; 70:1575–1580; 2. Strangfeld A, et al. Arthritis Rheum 2009; 60(Suppl. 10):1695.
64.4 62.6
45.3
54.9
0
10
20
30
40
50
60
70
RF status Anti-CCP status
Positive Negative
2* 2.1** 2.1**
1.61.4
1.1
0
0.5
1
1.5
2
2.5
RF Anti-CCP RF and anti-CCP
Positive Negative
Me
an c
han
ge in
DA
S28
at
6
mo
nth
s
Pat
ien
ts w
ith
EU
LAR
G
oo
d/M
od
era
te r
esp
on
se (
%)
***
CERERRA1 RABBIT registry2

Boolean remission to abatacept inbiologic-naïve RA patients at 6 months (ACTION study)
Error bars represent 95% CI. Alten R, et al. Arthritis Rheumatol 2015; 67(Suppl. 10); Abstract 551
0
3
6
9
12
15
18
RF (+)(n=318)
RF (-)(n=128)
Anti-CCP (+)(n=287)
Anti-CCP (-)(n=141)
RF (+) andanti-CCP (+)
(n=243)
RF (-) andanti-CCP (-)
(n=100)
RF (+) oranti-CCP (+)
(n=362)
Pat
ien
ts (
%)p=0.008 p=0.096 p=0.013 p=0.025

Dennis et al. Arthritis Research & Therapy 2014, 16:R90
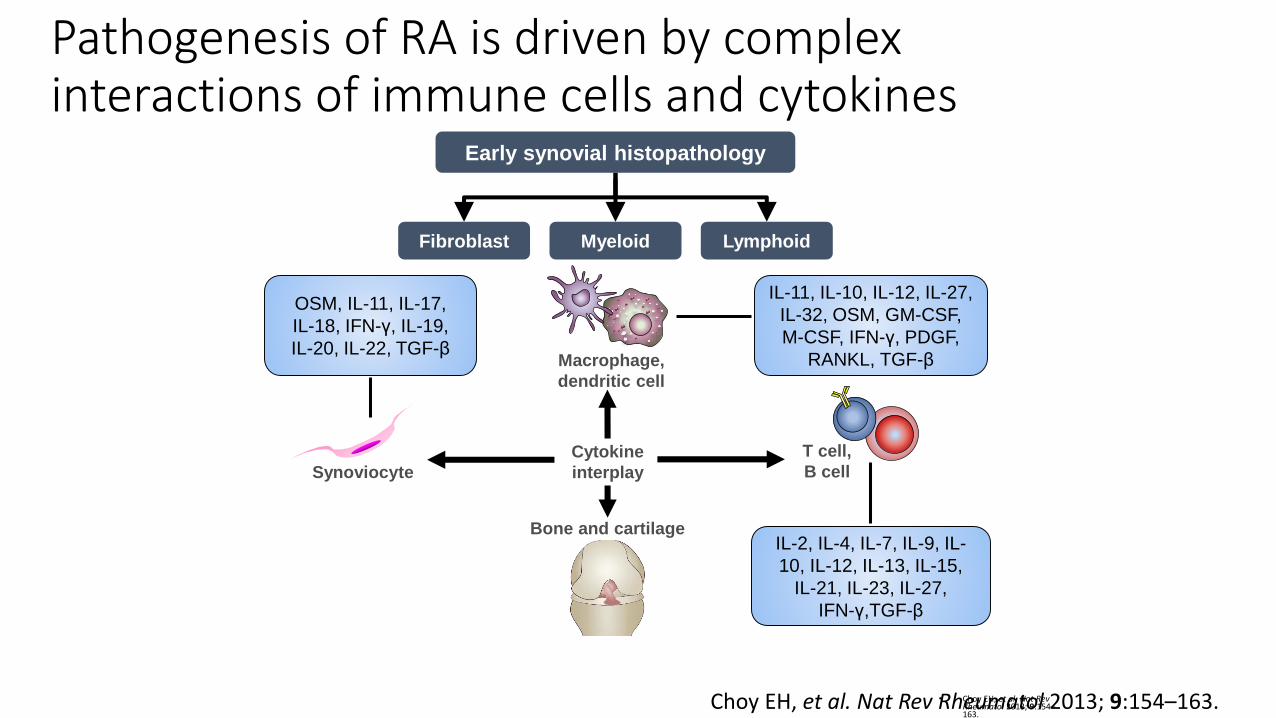
Pathogenesis of RA is driven by complex interactions of immune cells and cytokines
• Choy EH, et al. Nat Rev Rheumatol 2013; 9:154–163.
Cytokine
interplay
Bone and cartilage
T cell,
B cell
Macrophage,
dendritic cell
Synoviocyte
Early synovial histopathology
Fibroblast Myeloid Lymphoid
IL-11, IL-10, IL-12, IL-27,
IL-32, OSM, GM-CSF,
M-CSF, IFN-γ, PDGF,
RANKL, TGF-β
OSM, IL-11, IL-17,
IL-18, IFN-γ, IL-19,
IL-20, IL-22, TGF-β
IL-2, IL-4, IL-7, IL-9, IL-
10, IL-12, IL-13, IL-15,
IL-21, IL-23, IL-27,
IFN-γ,TGF-β
Choy EH, et al. Nat Rev Rheumatol 2013; 9:154–163.

Conclusion• Pathogenesis of RA and PsA are different
• Different cytokines have different pathogenic roles in inflammatory rheumatic diseases
• Cytokines have different roles during different stages of inflammatory arthritis
• In RA, immune activation as evident by ACPA serpositivity, is present before symptoms
• In HLA-DR4 positive individual, citrullinated peptide are more potent antigens
• Infection can leads to development and amplification of ACPA response leading to disease
• RA are heterogenous: ACPA +ve and ACPA-ve diseases may be fundamentally different and associated with difference in response to rituximab and abatacept
46