update on liposuction: laser-assisted liposuction versus tumescent liposuction
TRANSCRIPT
COSMETIC DERMATOLOGY (JF SOBANKO, SECTION EDITOR)
Update on Liposuction: Laser-Assisted Liposuction VersusTumescent Liposuction
Christie G. Regula & Naomi Lawrence
Published online: 23 March 2014# Springer Science+Business Media New York 2014
Abstract Tumescent liposuction has become an increasinglypopular cosmetic procedure since its inception nearly 30 yearsago. Laser lipolysis has more recently been studied as analternative method of body contouring. We discuss the effica-cy and safety of laser lipolysis in comparison to tumescentliposuction. Ultimately, while laser lipolysis is effective forlocalized fat reduction, data is lacking to show its superiorityto tumescent liposuction.
Keywords Laser lipolysis . Laser-assisted liposuction .
Tumescent liposuction . Nd:YAG laser . Body contouring
Introduction
Liposuction is one of the most common cosmetic proceduresperformed in the USA. It should be viewed not as “weightloss” surgery but as body contouring, for it is best in removinglocalized adiposities resistant to overall weight loss.Liposuction under local anesthesia was developed in 1987.Even though tumescent anesthesia liposuction has an excel-lent safety and efficacy record, different technologies havebeen applied over the years in an effort to further improve theprocedure. This article focuses on laser-assisted lipolysis andits comparison to tumescent liposuction. Although there arenumerous studies examining the efficacy of laser-assistedlipolysis, the majority are nonblinded pilot studies with lowlevels of evidence.
Traditional Liposuction
Liposuction was first introduced in 1921 by the French sur-geon Dujarrier. The early methods of curettage were replacedby cannula liposuction in the mid-1970s [1]. In 1987, derma-tologist Jeffrey Klein reported his development of tumescentanesthesia which completely revolutionized the field of lipo-suction [2]. The infiltration of this dilute lidocaine and epi-nephrine solution allowed for the procedure to be performedunder local anesthesia, eliminating the need for general anes-thesia and hospitalization [3]. The inclusion of epinephrine isresponsible for decreased blood loss, and it has been demon-strated that the hematocrit in aspirated fat is minimal [4, 5]—1–3 % whole blood in the aspirate of tumescent liposuctioncompared to 40 % in that under general anesthesia.
Safety of Tumescent Liposuction
The earliest report establishing the safety of the tumescentliposuction technique compiled data on 9,478 dermatologytreated patients and was published in 1988 by Hanke andBernstein ([6], grade A). Seven years later, a larger cohort of15,336 patients with 44,014 body areas treated with liposuc-tion were reported ([7], grade A). Sixty-six dermatologicsurgeons responded to a survey to report their safety data.There were no serious complications reported, such as death,embolism (pulmonary or fat), hypovolemic shock, perforationof the peritoneum or thorax, or thrombophlebitis. No bloodtransfusions or admissions to the hospital were needed in thesecases. Further reports from dermatologic surgeons concerningtumescent liposuction’s safety have been consistent in theircomplication rates, with overall complication rates at 0.068–0.14 % and minor complication rates of 0.57 % ([8, 9], gradeA) without any deaths occurring in these reports. This is incontrast to complication rates found outside the dermatologic
C. G. Regula (*) :N. LawrenceDivision of Dermatology, Cooper Medical School of RowanUniversity, 10000 Sagemore Drive, Suite 10103, MarltonNJ 08043, USAe-mail: [email protected]
N. Lawrencee-mail: [email protected]
Curr Derm Rep (2014) 3:127–134DOI 10.1007/s13671-014-0074-1
literature, in which the fatality rate among 496,245 procedureswas 19.1/100,000 ([10], grade B). Instances of serious com-plication occurred in cases when large volumes of fat wereremoved with liposuction under general anesthesia. Coldironreported 10 years of Florida and 6 years of Alabamaoffice-based surgery safety data ([11••], grade A). Intotal, there were ten deaths associated with liposuction.All were performed under general anesthesia, and nonewere performed by dermatologists. Infection rates arelow for tumescent liposuction. Superficial infections, es-pecially around injection sites, are most common [12]. Therehave been rare reports of deeper, delayed infections withatypical mycobacterium [12] as well as necrotizing fasciitis[13, 14]. Overall, tumescent liposuction is a procedure with awell-established safety record.
Background of Laser Lipolysis
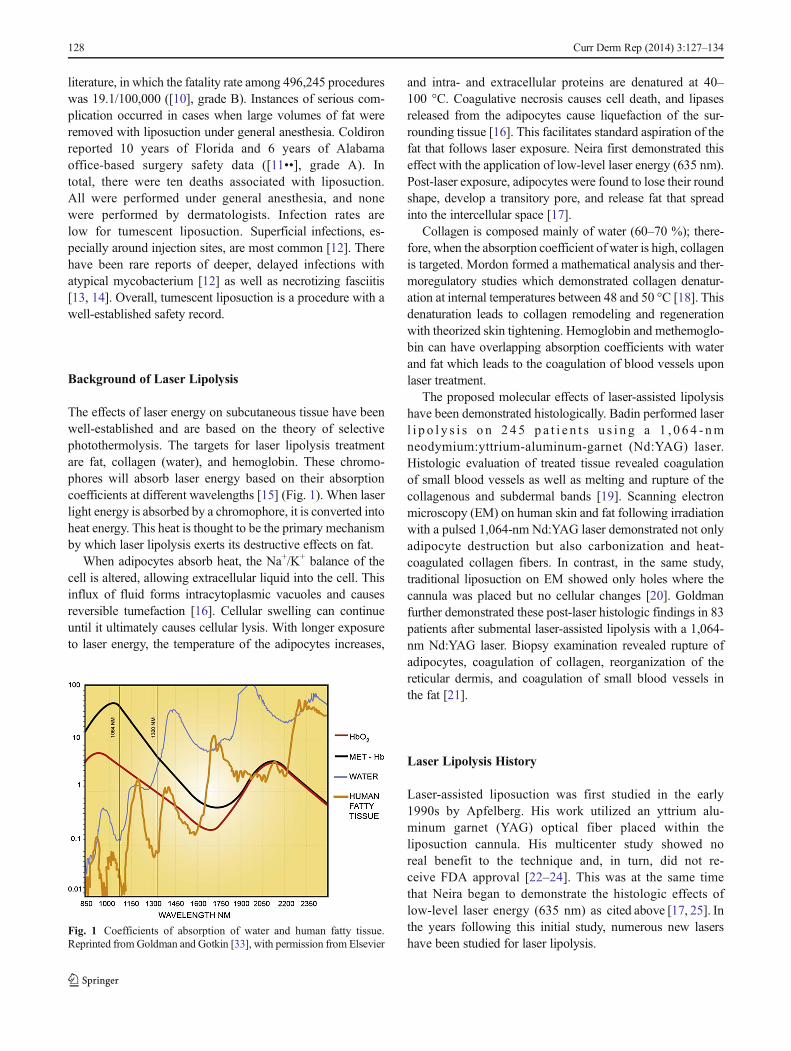
The effects of laser energy on subcutaneous tissue have beenwell-established and are based on the theory of selectivephotothermolysis. The targets for laser lipolysis treatmentare fat, collagen (water), and hemoglobin. These chromo-phores will absorb laser energy based on their absorptioncoefficients at different wavelengths [15] (Fig. 1). When laserlight energy is absorbed by a chromophore, it is converted intoheat energy. This heat is thought to be the primary mechanismby which laser lipolysis exerts its destructive effects on fat.
When adipocytes absorb heat, the Na+/K+ balance of thecell is altered, allowing extracellular liquid into the cell. Thisinflux of fluid forms intracytoplasmic vacuoles and causesreversible tumefaction [16]. Cellular swelling can continueuntil it ultimately causes cellular lysis. With longer exposureto laser energy, the temperature of the adipocytes increases,
and intra- and extracellular proteins are denatured at 40–100 °C. Coagulative necrosis causes cell death, and lipasesreleased from the adipocytes cause liquefaction of the sur-rounding tissue [16]. This facilitates standard aspiration of thefat that follows laser exposure. Neira first demonstrated thiseffect with the application of low-level laser energy (635 nm).Post-laser exposure, adipocytes were found to lose their roundshape, develop a transitory pore, and release fat that spreadinto the intercellular space [17].
Collagen is composed mainly of water (60–70 %); there-fore, when the absorption coefficient of water is high, collagenis targeted. Mordon formed a mathematical analysis and ther-moregulatory studies which demonstrated collagen denatur-ation at internal temperatures between 48 and 50 °C [18]. Thisdenaturation leads to collagen remodeling and regenerationwith theorized skin tightening. Hemoglobin and methemoglo-bin can have overlapping absorption coefficients with waterand fat which leads to the coagulation of blood vessels uponlaser treatment.
The proposed molecular effects of laser-assisted lipolysishave been demonstrated histologically. Badin performed laserl i p o l y s i s o n 245 p a t i e n t s u s i n g a 1 , 0 6 4 - nmneodymium:yttrium-aluminum-garnet (Nd:YAG) laser.Histologic evaluation of treated tissue revealed coagulationof small blood vessels as well as melting and rupture of thecollagenous and subdermal bands [19]. Scanning electronmicroscopy (EM) on human skin and fat following irradiationwith a pulsed 1,064-nm Nd:YAG laser demonstrated not onlyadipocyte destruction but also carbonization and heat-coagulated collagen fibers. In contrast, in the same study,traditional liposuction on EM showed only holes where thecannula was placed but no cellular changes [20]. Goldmanfurther demonstrated these post-laser histologic findings in 83patients after submental laser-assisted lipolysis with a 1,064-nm Nd:YAG laser. Biopsy examination revealed rupture ofadipocytes, coagulation of collagen, reorganization of thereticular dermis, and coagulation of small blood vessels inthe fat [21].
Laser Lipolysis History
Laser-assisted liposuction was first studied in the early1990s by Apfelberg. His work utilized an yttrium alu-minum garnet (YAG) optical fiber placed within theliposuction cannula. His multicenter study showed noreal benefit to the technique and, in turn, did not re-ceive FDA approval [22–24]. This was at the same timethat Neira began to demonstrate the histologic effects oflow-level laser energy (635 nm) as cited above [17, 25]. Inthe years following this initial study, numerous new lasershave been studied for laser lipolysis.
Fig. 1 Coefficients of absorption of water and human fatty tissue.Reprinted fromGoldman and Gotkin [33], with permission from Elsevier
128 Curr Derm Rep (2014) 3:127–134

1,064 nm Nd:YAG
In the early 2000s, Blugerman, Schavelzon, and Goldmanperformed studies with a 1,064-nm Nd:YAG laser, conductedby means of an optical fiber, within a 1-mm introducer can-nula, in direct contact with adipose tissue [26]. This work, ascited above, demonstrated changes on the cellular level thatserved as a basis for further laser studies. Badin confirmedthese findings by showing adipocyte rupture, coagulation ofblood vessels, and remodeling of collagen [19, 16]. Kim andGeronemus studied the use of a 1,064-nm Nd:YAG laser witha 300-μm fiber for the treatment of focal areas of fat less than100 cm3 without fat aspiration. Twenty-nine patients complet-ed the study. Self-assessment evaluations reported an im-provement of 37 % at the 3-month follow-up. Baseline andfollow-up MRIs demonstrated an average of 17 % reductionin fat volume ([27], grade B). Goldman further substantiatedthe use of the 1,064-nm Nd:YAG laser for the treatment oflocalized fat in his study of 82 subjects. He treated thesubmental area with a 300-μm fiber followed by a negative-pressure suction cannula and produced results similar to thoseof traditional liposuction ([21], grade C). These studies, inaddition to the well-established histological effects of laserlipolysis, prompted FDA approval of the first laser lipolysisdevice—a 6-W Nd:YAG laser (manufactured by DEKA anddistributed by Cyanosure, Westford, MA). Following this,many other studies substantiated the effectiveness of the1,064-nm Nd:YAG laser for localized fat reduction.
Sun et al. reported on 35 cases of localized fat reduction withthe 1,064-nm Nd:YAG laser. Good cosmetic outcomes wereobtained from treatment of the face, neck, mental region, upperarm, and abdomen ([28], grade C). This laser has also been usedeffectively for the treatment of gynecomastia. Rho et al. per-formed unilateral treatment on five patients. At 8 weeks post-treatment, chest circumference was significantly reduced—onaverage by approximately 1 cm (29], grade C). The use of the1,064-nm Nd:YAG laser for fat removal of the upper arms hasalso been described [30]. In a 20-patient study, Dudelzak et al.showed fat reduction of, on average, 0.75 cm per arm circum-ference and overall skin tightening at 6 months post-treatment.Further, in this study, one arm of each patient was treated withlaser lipolysis alone while the other was followed by suctionaspiration. Results of treatment were the same regardless ofwhether or not suction was used. There are, however, inherentflaws and inconsistencies with circumference measurements,and this makes them problematic for use as study endpoints.
The 1,064-nm Nd:YAG laser has also been used in com-bination with autologous fat transfer for the improvement ofcellulite. Goldman and colleagues treated 52 women withCurri grade III to IV cellulite (mainly of the hips, buttocks,and thighs). At 6 months, patients had a subjective improve-ment in skin texture and quality. The majority of patients(84.6 %) rated the results of their treatment as good or
excellent ([31], grade C). Following approval of the 1,064-nm Nd:YAG, two other FDA-approved lasers followed in thenext several years—a sequentially firing 1,064-nm/1,320-nmNd:YAG and a 980-nm diode laser (Table 1).
1,064 nm/1,320 nm Nd:YAG
The sequentially firing 1,064-nm/1,320-nm Nd:YAG laser wasfirst clinically studied in 2009 [32]. These twowavelengths havedistinct effects on adipose tissue. At 1,320 nm, the coefficient ofabsorption for water and fat is much higher than that of hemo-globin. This leads to an increased absorption of laser energy byfat with less scatter and, therefore, increased heating of theadipocytes. In contrast, at 1,064 nm, hemoglobin has a highercoefficient of absorption than water. This leads to a slower andmore generalized heating of the fat and coagulation effects onblood vessels [33]. The sequential firing of the two wave-lengths takes advantage of the benefits of each absorp-tion coefficient. Further, the combination laser is equippedwith an accelerometer microchip-equipped handpiece. Thisaccelerometer decreases the energy output of the laser,and the movement of the handpiece slows or stops to preventoverheating of the fat and subsequent burns [34].
DiBernardo and Reyes conducted the first study to evaluatethe effects of the 1,064-nm/1,320-nm Nd:YAG laser on skintightening and shrinkage. In this study, five patients weretreated for focal abdominal adiposities with dermal tattoomarkings placed in four quadrants. Surface area measure-ments between the tattoos were taken pre- and post-treatment. At 3 months post-op, there was an average areareduction, or skin shrinkage, of 17 %. Further, skin tighteningwas measured by an elasticity device using a suction cupprobe. Compared to baseline, skin elasticity was improvedby 26 % at 3 months ([32], grade C). Another pilot study wasconducted by McBean and Katz for the use of this laser inlipolysis and skin tightening. Twenty patients were enrolled
Table 1 FDA-approved laser lipolysis devices
Trade name Manufacturer Wavelength (nm) Laser type
SmoothLipo Eleme 920 Diode
SlimLipo Palomar 924/975 Diode
Lipotherme Osyris 980 Diode
Smartlipo Cynosure 1,064 Nd:YAG
Smartlipo-MPX Cynosure 1,064, 1,320 Nd:YAG
LipoLite Syneron 1,064 Nd:YAG
CoolLipo CoolTouch 1,320 Nd:YAG
ProLipo Sciton 1,064 Nd:YAG
ProLipo Plus Sciton 1,064, 1,319 Nd:YAG
SmartLipo Triplex Cynosure 1,064, 1,320, 1,440 Nd:YAG
Accusculpt Lutronic 1,444 Nd:YAG
Curr Derm Rep (2014) 3:127–134 129

for the treatment of local adiposities. At 1 month follow-up,independent observers found 76–100 % improvement in adi-posities in 85 % of subjects and 51–75 % improvement in15 % of subjects. India ink tattooing was also used to demar-cate and measure the treatment area. Post-treatment, themapped area was found to decrease, on average, by 18 %.Post-treatment biopsies were also performed demonstratingincreased new collagen production on hematoxylin and eosinstaining and increasedmyofibroblasts on electronmicroscopy.Both of these findings signify connective tissue remodeling([34], grade C). It is important to note that India ink tattooingand measurement thereof has not been validated as a tool tomeasure surface area and is inherently dependent on theamount of fat extracted from under the skin.
Woodhall and colleagues published a report on three separatepilot studies of the 1,064-nm/1,320-nmNd:YAG laser [35]. Thefirst demonstrated the efficacy of the 1,064-nm/1,320-nmNd:YAG laser for the lipolysis of localized areas, including thearms, abdomen, flanks, and thighs. Eighteen female patientsparticipated in the study and at 3 months reported 80 % overallfat reduction and 75 % improvement of skin laxity ([35], gradeB). The two other pilot studies were split-treatment studies—onecomparing outcomes of a 1,064-nm/1,320-nm Nd:YAG-treatedarm to tumescent liposuction and the other comparing a 1,064-nm/1,320-nm Nd:YAG laser to a 1,320-nm Nd:YAG laser. Nosignificant improvement in fat reduction or skin laxity was notedbetween the three treatments ([35], grade B).
980 nm Diode
In early 2007, Mordon and colleagues first evaluated thehistologic effects of a 980-nm diode laser for lipolysis of freshcadaver thighs [36]. As previously mentioned, these findingsincluded cytoplasmic retraction, disruption of cell mem-branes, heat-coagulated collagen fibers, coagulated bloodcells, and carbonization of fat tissues. These findings weresimilar to those found with the 1,064-nm Nd:YAG lasersuggesting that heat (48–50 °C), and not a particular wave-length, is responsible for lipolysis and skin tightening [36].Diode lasers have the advantage of high power outputs andcontinuous emission operation. This allows for more heat tobe produced more quickly in the tissues [37].
Reynaud et al. reported a retrospective analysis on the safetyand efficacy of 534 laser lipolysis procedures using a 980-nmdiode laser ([37], grade C). The areas treated included the hips,inner thighs, abdomen, knees, flanks, buttocks, chin, arms, andback. There was no scarring, infection, burns, hypopigmentation,bruising, swelling, or edema noted. No objective clinical analysiswas performed; rather, patients subjectively reported their satis-faction. Fifty-eight percent of patients were found to be verysatisfied, 22 % satisfied, and 18 % less satisfied with the proce-dure ([37], grade C). The use of the 980-nm diode laser was also
found to be effective in the treatment of gynecomastia with amean chest circumference reduction of 14.1 cm at 6 months([38], grade B). Leclère and colleagues recently reported over5 years of data on 674 lipolysis procedures with the 980-nmlaser. Areas treated included the arms, thighs, sides, back, calves,buttocks, abdomen, breasts, chin/jowl, knees, and hips.Ultrasound measurements of fat thickness were reduced in allareas at 3 months. The areas with the greatest reduction were thebuttocks (44 %) and abdomen (40–57 %). Mean patient satis-faction scores ranged from 6/10 to 9.5/10 depending on the areatreated. Treatment of the abdomen and arms resulted in thelowest patient satisfaction scores while treatment of the breastshad the highest patient satisfaction scores ([39•], grade B).
Other Wavelengths
Over the past several years, further studies have been conduct-ed on alternative wavelengths for laser lipolysis. In a study ofminipigs, a 1,440-nm Nd:YAG laser was shown to have agreater lipolytic effect in vivo than a 1,064-nm Nd:YAG laser[40]. This laser is thought to be more efficacious and safer thanthe 1,064- and 1,320-nm Nd:YAG lasers due to its higheraffinity to fat and water. It has also shown effective skintightening in guinea pigs 3 months after treatment—evidencedby histologic sampling which showed increased dermal thick-ness, collagen organization, fibroblast proliferation, intensityof elastic fibers, and mucopolysaccharides [41•].Holcomb and colleagues published a retrospective re-view of 478 patients who underwent laser-assisted facialcontouring of the mid and lower face. A micropulsed 1,444-nm Nd:YAG laser was used with varied subjective improve-ments (modest to subtle to very apparent) ([42], grade C).
Other lasers, aimed to more directly target adipose tissue,have also been studied for lipolysis. This includes a dualcontinuous-wave 924-nm/975-nm diode laser. This technologyis based on a clear peak in adipose absorption at 924 nm and apeak in water absorption at 975 nm. In turn, fat is more directlylysed, while energy absorption by water/collagen aims to tightenskin. Weiss and Beasley reported on 19 patients treated with thislaser for adiposities of varied sites including the submentalregion, neck and jowls, abdomen, arms, thighs, and flanks. At3 months, a quartile assessment was completed by the investi-gators. Reduction of unwanted fat was deemed “good” in 27 %of subjects and “excellent” in 73 % of subjects. Improvement ofskin laxity was observed to be “good” in 36 % of patients and“excellent” in 64 % of subjects ([43], grade B). In two separatestudies, Leclère and Moren-Moraga have reported effectivelipolysis of the knees and ankles with the 924-nm/975-nm diodelaser. In each study, 29 of 30 patients treated would recommendthe treatment ([44, 45], grade C).
Most recently, Licata et al. reported their experience with anew 1,540-nm diode laser. This wavelength has a deeper
130 Curr Derm Rep (2014) 3:127–134

penetration and is preferentially absorbed by fat rather thanwater found in the dermis or interstitial fluid. In turn, adipo-cytes are heated to a temperature several times higher than thatof the surrounding tissue, and this is believed to lead to moreeffective lipolysis [46•]. In this study of 230 patients, treatmentareas included the abdomen, thighs, trochanteric region, flanks,neck, arms, breasts, hips, and knees. Good fat reduction andskin tightening were noted. Subjective patient satisfaction wasalso reported with 66 % of patients being “very satisfied” withthe outcome and 28 % being “satisfied” ([46•], grade C).
Safety of Laser-Assisted Lipolysis
Laser-assisted lipolysis is a relatively new technology. Still,numerous studies exist that have established its safety. Chiaand Theodorou published the largest of such report to date([47•], grade B). Over a period of 22 months, 1,000 consec-utive cases were performed in 581 patients using a 1,064-nmand/or 1,320-nm Nd:YAG laser. Of these patients, 545had multiple procedures done. Treated areas includedthe neck, triceps, male breasts, midback, flanks, axilla,abdomen, mons pubis, thighs, pre-sacrum, and knees.The average number of areas treated was 1.8. Overall,there were a total of three burns, two infections, one hema-toma, and one seroma. The burn and hematoma complicationsoccurred within the first 25 patients and may suggest thesecomplications were due to operator inexperience. There wasone case of cellulitis in the triceps region and one infection inthe abdominal area which both resolved with antibiotics. Atotal of 73 touch-up procedures were needed (7.3 %) ([47•],grade B).
A previous study reported 537 consecutive laser li-polysis procedures performed with the 1,064-nmNd:YAG laser ([48], grade B). Complications occurredin five instances, one local infection and four skin burnsfor a complication rate of 0.93 %. Nineteen touch-upprocedures were needed (3.5 %) [48]. Cutaneous burnsare the most concerning complication unique to laser-assisted lipolysis. The rate of burns is operator-dependent.The goal internal temperature for adequate lipolysis is be-tween 48 and 50 °C. External temperatures of the treated areashould remain between 38 and 41 °C to minimize burns [15].Longer-wavelength lasers may pose higher risk of burns dueto their increased absorption by fat and water and moreaggressive localized heating [49].
Laser Lipolysis Compared to Tumescent Liposuction
Proposed benefits of laser lipolysis over tumescent liposuctioninclude superior skin tightening, less blood loss, post-operative pain and ecchymoses, and less physical strain on
the operator. There are, however, few studies directly compar-ing these two methods.
Prado and colleagues completed a prospective, randomizeddouble-blind controlled trial examining the use of a 1,064-nmNd:YAG-assisted lipolysis and suction-assisted lipoplasty in asplit-body manner with a follow-up of 6–11 months [50].Treatment areas were the submental, posterior axillary,subscapular, lumbar, arms, medial thighs, trochanter, medialknees, ankles, and abdomen. Patients rated post-operativepain on a 10-point visual analog scale for each method.Overall, laser-assisted lipolysis was less painful than suction-assisted lipoplasty (6 vs. 6.7). While this was statisticallysignificant, one has to question if this difference in pain scoreis really clinically significant. Otherwise, there was no differ-ence in patient satisfaction, post-operative ecchymoses, timeto recovery, or edema. Clinical outcomes were scored by ablinded physician and based on contour deformity, asymme-try, malposition, distortion, and scar. There was no significantdifference in these measures between the two methods ([50],grade B).
In a small study, DiBernardo treated ten female patientswith abdominal adiposity and mild to moderate skin laxity tocompare the skin tightening and shrinkage effects of laserlipolysis and suction liposuction [51]. India ink tattoos wereplaced to demarcate the four quadrants of their abdomen. Thequadrants were randomized to receive laser-assisted lipolysiswith a 1,064-nm/1,320-nm Nd:YAG laser or liposuctionalone. The areas were evaluated for skin shrinkage by areameasurements and skin tightening by an elasticity device at 1and 3 months post-treatment. At 3 months, they found a 54 %improvement in skin area shrinkage on the laser-assisted sidecompared to liposuction alone. There was no significant dif-ference between skin stiffness between the two treatments([51], grade C). While this difference in skin area shrinkagewas found to be statistically significant, one has to ask if it istruly clinically significant. Again, this method of surface areameasurement has not been validated. Furthermore, it is notpossible to obtain isolated measurements for each side of theabdomen as treatment of one side can affect the skin tightnessof the other side.
Goldman and colleagues reported a study of 28 patientstreated for upper arm adiposity [52]. Fourteen patients re-ceived laser-assisted lipolysis with a 1,064-nm Nd:YAG laser,and 14 received treatment with tumescent liposuction alone.The laser-assisted group had significantly improved arm
Table 2 Common flaws found in laser-assisted lipolysis studies
• Retrospective design
• Lack of internal control to gold standard (tumescent liposuction)
• Subjective patient-reported outcomes
• Unblinded physician evaluators
• Nonvalidated measuring systems
Curr Derm Rep (2014) 3:127–134 131

circumference and subjectively improved skin tightening at3 months compared to tumescent liposuction ([52], grade C).Ideally, such results would be duplicated in a split-arm studyto internally control the amount of superficial, suctionableadiposity that patients have.
Laser lipolysis is thought to be less traumatic due to itssmall-caliber cannula (1 mm) and liquefaction of fat by thelaser before suctioning [21]. This method also touts lessbleeding than suction liposuction due to laser coagulation ofsmall blood vessels [21]. Tumescent liposuction itself has verylittle whole blood in its aspirate compared to that of liposuc-tion under general anesthesia (1–3 vs. 40 %) ([53], grade B).This reduction in blood loss is due to the vasoconstrictiveeffects of epinephrine in the tumescent solution. Prado andcolleagues evaluated the lipocrit counts (packed red bloodcells in the infranatant) between the 1,064-nm Nd:YAGlaser-assisted lipolysis and tumescent anesthesia in theirsplit-body study ([50], grade B). Laser-assisted lipolysis re-sulted in lower lipocrit (14.9 %±3.3) than did tumescentliposuction (22.5 %±2.7).
In order to examine the clinical relevance of the hypothe-sized decrease in blood loss, Przylipiak and colleagues studiedthe effects of internal 1,064-nm Nd:YAG laser-assisted lipo-suction versus tumescent liposuction on laboratory analysis[54••]. Fifty-four patients were included in the study. Pre- andpost-surgery blood examinations were performed (7–10 daysbefore surgery and 24 h after surgery). Treatment areas in-cluded the abdomen, flanks, and inner or outer thighs.Aspirate volumes ranged from 700 to 3,500 mL of fat. Therewas no statistically significant difference in pre- and post-treatment platelet counts between the two methods. It mustbe kept in mind that major surgery results in a tendency toincrease the production of reactive platelets. So, from thisstudy, we can only determine that the surgical platelet reduc-tion and reaction of platelets are neutral in both treatments([54••], grade B). Neutrophils were higher, and lymphocyteswere lower after surgery in both treatment groups with nostatistical difference between the two ([54••], grade B). Theseresults suggest that there is no significant difference in bloodloss between the two treatments; however, a study evaluatinghemoglobin and hematocrit values may offer more practicalconclusions.
Head-to-head studies proving the consistent superiority oflaser-assisted lipolysis to tumescent liposuction are lacking.Most studies to date have grade B or C evidence. Laser-assisted lipolysis certainly has its disadvantages as well. Thetechnique is less time-efficient than tumescent liposuction dueto the slow movement of the laser needed to cause lipolysis[50]. In addition, no device uses laser alone. All devicesrequire that liposuction follow the laser lipolysis. The neededequipment is expensive (usually greater than $100,000) andrepresents a large investment to make without sound evidencefor clinical superiority.
Conclusion
Obesity is a growing epidemic in the USA. Although manyindividuals struggle with their weight, liposuction is not aweight loss procedure. It is people with disproportionate adi-posity that benefit from fat removal. Tumescent liposuction hasbeen established as a safe and effective method for the treat-ment of focal adiposity. The negative aspects of traditionaltumescent liposuction technique are that it is invasive and theprocedure itself is physically demanding and time-consumingfor the physician. For a new technique to replace this well-established procedure, that technique would have to either benoninvasive, produce dramatically better results, or be signif-icantly easier and less time-consuming. There is now nearly15 years of data concerning laser-assisted lipolysis. Most ofthese are small studies with numerous limitations (Table 2).First, by nature of the technique, the performing physician isunblinded. Second, there is also an inherent bias in the appli-cation of this technology as the studies are generally performedby physicians who have already purchased the equipment.Third, objective assessment of results is difficult to obtain asmeasurements of fat are difficult to standardize. Many studiesrelied on subjective, unblinded reporting of results. Not onlyhas laser-assisted lipolysis not been proven superior to tumes-cent liposuction, but it also is an invasive procedure as itrequires introduction into the subcutis and follow-up liposuc-tion. With the study and approval of cryolipolysis and ultra-sound devices for fat reduction, the potential of bodycontouring with noninvasive techniques seems greater.
Compliance with Ethics Guidelines
Conflict of Interest CG Regula declares no conflicts of interest.N Lawrence declares no conflicts of interest.
Human and Animal Rights and Informed Consent This article doesnot contain any studies with human or animal subjects performed by anyof the authors.
References
Papers of particular interest, published recently, have beenhighlighted as:• Of importance•• Of major importance
1. Flynn TC, Coleman 2nd WP, Field LM, Klein JA, HankeCW. History of liposuction. Dermatol Surg. 2000;26(6):515–20.
2. Klein JA. The tumescent technique for liposuction surgery. Am JCosmet Surg. 1987;4:263–7.
132 Curr Derm Rep (2014) 3:127–134
3. Klein JA. Anesthesia for liposuction in dermatologic surgery. JDermatol Surg Oncol. 1988;14:1124–32.
4. Klein JA. The tumescent technique. Anesthesia and modified lipo-suction technique. Dermatol Clin. 1990;8:425–37.
5. Lillis PJ. Liposuction surgery under local anesthesia: limited bloodloss and minimal lidocaine absorption. J Dermatol Surg Oncol.1998;14:1145–8.
6. Berstein G, Hanke CW. Safety of liposuction: a review of 9478cases performed by dermatologists. J Dermatol Surg Oncol.1988;14(10):1112–4.
7. Hanke CW, Berstein G, Bullock S. Safety of tumescent liposuctionin 15,336 patients. National survey results. Dermatol Surg.1995;21(5):459–62.
8. Housman TS, Lawrence N, Mellen BG, George MN, Filippo JA,Cerveny KA, et al. The safety of liposuction: results of a nationalsurvey. Dermatol Surg. 2002;28(11):971–8.
9. Hanke W, Cox SE, Kuznets N, Coleman 3rd WP. Tumescentliposuction report performance measurement initiative: nationalsurvey results. Dermatol Surg. 2004;30(7):967–77.
10. Grazer FM, de Jong RH. Fatal outcomes from liposuction: censussurvey of cosmetic surgeons. Plast Reconstr Surg. 2000;105(1):436–46.
11.•• Starling 3rd J, Thosani MK, Coldiron BM. Determining the safetyof office-based surgery: what 10 years of Florida data and 6 years ofAlabama data reveal. Dermatol Surg. 2012;38(2):171–7. Review ofsafety data revealing ten deaths associated with liposuction. Allwere performed under general anesthesia, and none were per-formed by dermatologists.
12. Hanke CW, Coleman 3rd WP, Lillis PJ, Narins RS, BueningJA, Rosemark J, et al. Infusion rates and levels ofpremedication in tumescent liposuction. Dermatol Surg.1997;23(12):1131–4.
13. BeesonWH, Slama TG, Beeler RT, Rachel JD, Picerno NA. GroupA streptococcal fasciitis after submental tumescent liposuction.Arch Facial Plast Surg. 2001;3(4):277–9.
14. Nagelvoort RW, Hulstaert PF, KonM, Schuurman AH. Necrotisingfasciitis and myositis as serious complications after liposuction.Ned Tijdschr Geneeskd. 2002;146(50):2430–5.
15. McBean JC, Katz BE. Laser lipolysis: an update. J Clin AesthetDermatol. 2011;4(7):25–34.
16. Badin AZ, Gondek LB, Garcia MJ, Valle LC, Flizikowski FB, deNoronha L. Analysis of laser lipolysis effects on human tissuesamples obtained from liposuction. Aesthet Plast Surg.2005;29(4):281–6.
17. Neira R, Arroyave J, Ramirez H, Ortiz CL, Solarte E,Sequeda F, et al. Fat liquefaction: effect of low-level laserenergy on adipose tissue. Plast Reconstr Surg. 2002;110(3):912–22.
18. Mordon SR, Wassmer B, Reynaud JP, Zemmouri J.Mathematical modeling of laser lipolysis. Biomed EngOnline. 2008;7:10.
19. Badin AZ, Moraes LM, Gondek L, Chiaratti MG, Canta L. Laserlipolysis: flaccidity under control. Aesthet Plast Surg. 2002;26(5):335–9.
20. Ichikawa K, Miyasaka M, Tanaka R, Tanino R, Mizukami K,Wakaki M. Histologic evaluation of the pulsed Nd:YAG laser forlaser lipolysis. Lasers Surg Med. 2005;36(1):43–6.
21. Goldman A. Submental Nd:Yag laser-assisted liposuction. LasersSurg Med. 2006;38(3):181–4.
22. Apfelberg DB. Results of multicenter study of laser-assisted lipo-suction. Clin Plast Surg. 1996;23(4):713–9.
23. Apfelberg DB, Rosenthal S, Hunstad JP, Achauer B, Fodor PB.Progress report on multicenter study of laser-assisted liposuction.Aesthet Plast Surg. 1994;18(3):259–64.
24. Apfelberg D. Laser-assisted liposuction may benefit surgeons, pa-tients. Clin Laser Mon. 1992;10(12):193–4.
25. Neira R, Ortiz-Neira C. Low-level laser-assisted liposculpture: clin-ical report of 700 cases. Aesthet Surg J. 2002;22(5):451–5.
26. Goldman AG, Schavelzon D, Blugerman G. Liposuction usingneodymium-yttrium-garnet laser. Plast Reconstr Surg. 2003;111:2497.
27. Kim KH, Geronemus RG. Laser lipolysis using a novel 1,064 nmNd:YAG laser. Dermatol Surg. 2006;32(2):241–8.
28. Sun Y,Wu SF, Yan S, Shi HY, ChenD, ChenY. Laser lipolysis usedto treat localized adiposis: a preliminary report on experience withAsian patients. Aesthet Plast Surg. 2009;33(5):701–5.
29. Rho YK, KimBJ, KimMN, KangKS, Han HJ. Laser lipolysis withpulsed 1064 nm Nd:YAG laser for the treatment of gynecomastia.Int J Dermatol. 2009;48(12):1353–9.
30. Dudelzak J, Hussain M, Goldberg DJ. Laser lipolysis of the arm,with and without suction aspiration: clinical and histologic changes.J Cosmet Laser Ther. 2009;11(2):70–3.
31. Goldman A, Gotkin RH, Sarnoff DA, Prati C, Rossato F. Cellulite:a new treatment approach combining subdermal Nd: YAG laserlipolysis and autologous fat transplantation. Aesthet Surg J.2008;28(6):656–62.
32. DiBernardo BE, Reyes J. Evaluation of skin tightening after laser-assisted liposuction. Aesthet Surg J. 2009;29(5):400–7.
33. Goldman A, Gotkin RH. Laser-assisted liposuction. Clin PlastSurg. 2009;36:241–53.
34. McBean JC, Katz BE. A pilot study of the efficacy of a 1,064 and 1,320 nm sequentially firing Nd:YAG laser devicefor lipolysis and skin tightening. Lasers Surg Med. 2009;41(10):779–84.
35. Woodhall KE, Saluja R, Khoury J, Goldman MP. A comparison ofthree separate clinical studies evaluating the safety and efficacy oflaser-assisted lipolysis using 1,064, 1,320 nm, and a combined 1,064/1,320 nm multiplex device. Lasers Surg Med. 2009;41(10):774–8.
36. Mordon S, Eymard-Maurin AF, Wassmer B, Ringot J. Histologicevaluation of laser lipolysis: pulsed 1064-nm Nd:YAG laser versuscw 980-nm diode laser. Aesthet Surg J. 2007;27(3):263–8.
37. Reynaud JP, Skibinski M, Wassmer B, Rochon P, Mordon S.Lipolysis using a 980-nm diode laser: a retrospective analysis of534 procedures. Aesthet Plast Surg. 2009;33(1):28–36.
38. Trelles MA, Mordon SR, Bonanad E, Moreno Moraga J,Heckmann A, Unglaub F, et al. Laser-assisted lipolysis in thetreatment of gynecomastia: a prospective study in 28 patients.Lasers Med Sci. 2013;28(2):375–82.
39.• Leclère FM, Trelles M, Moreno-Moraga J, Servell P, Unglaub F,Mordon SR. 980-nm laser lipolysis (LAL): about 674 procedures in359 patients. J Cosmet Laser Ther. 2012;14(2):67–73. A report on674 laser lipolysis procedures with a 980-nm diode laser. Fatreduction was observed on ultrasound at 3 months with the greatestreduction in the abdomen and buttocks.
40. Tark KC, Jung JE, Song SY. Superior lipolytic effect of the 1,444 nm Nd:YAG laser: comparison with the 1,064 nm Nd:YAGlaser. Lasers Surg Med. 2009;41(10):721–7.
41.• Kim JH, Min KH, Heo CY, Baek RM, Park HJ, Youn SW, et al.Histological evaluation of dermal tissue remodeling with the 1444-nm neodymium:yttrium-aluminum-garnet laser in in vivo model. JDermatol. 2013;40(9):706–10. Histologic examination of guineapig tissue treated with a novel 1444-nm Nd:YAG laser showedincreased dermal thickness, collagen organization, fibroblast pro-liferation, intensity of elastic fibers, and mucopolysaccharides.
42. Holcomb JD, Turk J, Baek SJ, Rousso DE. Laser-assisted facialcontouring using a thermally confined 1444-nm Nd-YAG laser: anew paradigm for facial sculpting and rejuvenation. Facial PlastSurg. 2011;27(4):315–30.
43. Weiss RA, Beasley K. Laser-assisted liposuction using a novelblend of lipid- and water-selective wavelengths. Lasers Surg Med.2009;41(10):760–6.
Curr Derm Rep (2014) 3:127–134 133

44. Leclère FM, Moreno-Moraga J, Mordon S, Servell P, Unglaub F,Kolb F, et al. Laser-assisted lipolysis for cankle remodeling: aprospective study in 30 patients. Lasers Med Sci. 2014;29(1):131–6.
45. Moreno-Moraga J, Trelles MA, Mordon S, Unglaub F, Bravo E,Royo de La Torre J, et al. Laser-assisted lipolysis for knee remod-eling: a prospective study in 30 patients. J Cosmet Laser Ther.2012;14(2):59–66.
46.• Licata G, Agostini T, Fanelli G, Grassetti L, Marcianò A, RovattiPP, et al. Lipolysis using a new 1540-nm diode laser: a retrospectiveanalysis of 230 consecutive procedures. J Cosmet Laser Ther.2013;15(4):184–92. A study of 230 patients treated with a novel1,540-nm diode laser. Subjective reporting of fat reduction and skintightening as well patient satisfaction.
47.• Chia CT, Theodorou SJ. 1,000 consecutive cases of laser-assistedliposuction and suction-assisted lipectomy managed with local an-esthesia. Aesthet Plast Surg. 2012;36(4):795–802. Largest report todate of safety data for laser-assisted lipolysis (1,064- and/or 1,320-nm Nd:YAG). Of 1,000 cases, three burns, two infections, onehematoma, and one seroma were noted.
48. Katz B, McBean J. Laser-assisted lipolysis: a report on complica-tions. J Cosmet Laser Ther. 2008;10(4):231–3.
49. Mordon S, Plot E. Laser lipolysis versus traditional liposuction forfat removal. Expert Rev Med Devices. 2009;6(6):677–88.
50. Prado A, Andrades P, Danilla S, Leniz P, Castillo P, Gaete F. Aprospective, randomized, double-blind, controlled clinical trialcomparing laser-assisted lipoplasty with suction-assisted lipoplasty.Plast Reconstr Surg. 2006;118(4):1032–45.
51. DiBernardo BE. Randomized, blinded split abdomen study evalu-ating skin shrinkage and skin tightening in laser-assisted liposuctionversus liposuction control. Aesthet Surg J. 2010;30(4):593–602.
52. Goldman A, Wollina U, de Mundstock EC. Evaluation of tissuetightening by the subdermal Nd:YAG laser-assisted liposuctionversus liposuction alone. J Cutan Aesthet Surg. 2011;4(2):122–8.
53. Lillis PJ. Liposuction surgery under local anesthesia. Limited bloodloss and minimal lidocaine absorption. J Dermatol Surg Oncol.1988;14:1145–8.
54.•• Przylipiak AF, Galicka E, DonejkoM, NiczyporukM, Przylipiak J. Acomparative study of internal laser-assisted and conventional liposuc-tion: a look at the influence of drugs and major surgery on laboratorypostoperative values. Drug Des Dev Ther. 2013;7:1195–200. Pre- andpost-treatment, 1,064-nm Nd:YAG laser lipolysis and tumescent lipo-suction laboratory results were compared. No difference in platelet,neutrophil, or lymphocyte counts between the two methods.
134 Curr Derm Rep (2014) 3:127–134