update in thalassemia management -...
TRANSCRIPT

ผศ.พญ.พรพรรณ ศรพรสวรรค
ภาควชากมารเวชศาสตร
คณะแพทยศาสตร ม.สงขลานครนทร
Update in Thalassemia Management
23th May 2018

Scope of talk
• Thalassemia definition TDT/ NTDT
• Thalassemia management Guidelines
• Current Iron Chelation Therapy
• New standard to assess iron overload
• New hope for thalassemia patients

Classification of thalassemia syndromes
Occasional transfusions required
Intermittent transfusions required
Regular, lifelong transfusions required
Non-deletional HbHβ-thalassemia major
Severe HbE/β-thalassemia
β-thalassemia intermedia
Mild HbE/β-thalassemia Deletional HbHModerate HbE/β-thalassemia
1Muncie HL & Campbell JS. Am Fam Physician 2009;80:339–344; 2Galanello & Origa. Orphanet Journal of Rare Diseases
2010, 5:11; 3Harteveld & Higgs. Orphanet Journal of Rare Diseases 2010, 5:13; 4Cohen AR et al. Hematology Am Soc Hematol
Educ Program 2004;14–34
Transfusions seldom required
α-thalassemia traitβ-thalassemia minorHbC/β-thalassemia
Non-transfusion-dependent thalassemias: NTDTPhenotype
Genotype
Transfusion-dependent thalassemias: TM

Thalassemia management challenges change with age
1. Musallam K et al. Pediatrics 2008;121:e1426–e1429.
AnaemiaIron overload
Child2–10 years
Adolescent10–18 years
Adult>18 years
• Growth
• Sexual
development
• Sexual
development
• Adherence
• Transition of care
• Osteoporosis
• Organ failure
• Fertility and
pregnancy
Treatment of thalassemia
Parent education
Supportive treatment
Blood transfusion & Iron chelation therapy
Splenectomy
Hematopoietic stem cells transplantation
Novel treatment: stimulate HbF synthesis/ targeted therapy
Genetic counseling

Supportive treatment
Nutritional support
Folic acid (5 mg)
อาย < 1 ป 0.5 tab/day, อาย > 1 ป 1 tab/day
Vitamin E supplement
Avoid oxidative drugs eg. sulfonamide
Prevention of unnecessary iron therapy
Need vaccination as normal child

Why transfusion is needed?

Pediatric TDT patients require adequate blood transfusions for normal growth
Suppress ineffective erythropoiesis
Ensure appropriate growth and
development
Goals of blood transfusion therapy in pediatric TDT patients:
Guidelines for pediatric patients:• Maintain average Hb of 12 g/dL
• Pre-transfusion Hb of 9–10 g/dL
• Aim to transfuse whole units only; start with low transfusion
frequency in young patients and increase as they grow
1. Gibson BES et al. Br J Haematol 2004;124:433–453;
2. Thalassaemia International Federation. Guidelines for the clinical management of
thalassemia, 2nd revised edition 2008;
3. Goss C et al. Transfusion 2014;doi:10.1111/trf.12571. [Epub ahead of print].

How to know who needed blood?
Hb < 7 g/dL อยางนอย 2 คร ง หางกนมากกวา 1 เดอนโดยไมมปจจยกระตน
Severe thalassemia (present at age < 2yrs)
Marked hepato-splenomegaly
Poor growth & limit physical activity
Cardiovascular compromise

Severity of Thalassemia disease Molecular abnormality of β thalassemia
b0 thalassemia
codons 41/42 (-TCTT), codon 17, A-T
IVS-1 nt 1, G- T, codons 71/72 (+A)
severe b+ thalassemia
IVS-1 nt 5, G-C, IVS-2 nt 654, C-T
mild b++ thalassemia
-28 ATA, A-G
codon 19, A-G หรอ Hb Malay
codon 26, G-A หรอ HbE

Molecular of β-thalassemia gene in Southern Thailand n=78
• 92% found 6 common mutations
• 4bp deletion (Codon 41-42) Chinese
• IVS1 # 5 Muslim
• Codon 19 (Hb Malay)
• Codon 17
• -28 A-G
• IVS1#1
Loasombat V, et al. Am J Hematol 1992; 41: 194-8

Transfusion regimens
Correction of anemia: keep Hb > 9.5 gm/dL
Suppression of erythropoiesis
Inhibition of GI absorption of Fe
pre-transfusion Hb
“supertransfusion regimen” 12 g/dL
“hypertransfusion regimen” 10 g/dL
“low transfusion regimen” 6-8 g/dL

Transfusion guideline
Collection from donor within 7days
“Leucocyte poor/depleted” packed red cells
Blood group compatibility
Major : ABO, Rh
Minor : E, Mia, Lea, Leb, c
Screen for VDRL, HBsAg, anti-HIV, HIV Ag, anti-HCV
Red cell antigen typing: C, c, E, e และ Mia
HBV vaccine if anti-HBs negative

Transfusion dependent thalassemia (TDT)
Homozygous b-thalassemia
Severe β-thalassemia/Hb E disease
Hb Bart’s hydrop fetalis that survived
• Regular transfusion: maintain Hb > 9.5-10 g/dL at all time
• PRC 10-15 ml/kg q 2-6 wks

Non-transfusion dependent thalassemia (NTDT)
Hb H disease
β thalassaemia/Hb E disease ชนดไมรนแรง
• On-demand / Occasional transfusion
• Acute hemolysis (infection)
keep Hb > 7 g/dL & F/U at 4-12 wks
• PRC 10-15 ml/kg

Thalassemia clinic at PSU
TDT n= 72
• Homozygous β-thalassemia 17
• Severe β-thalassemia/Hb E disease 50
• Hb H with Cs/ AE Bart’s Cs 5
NTDT n= 120
ขอมลทควรบนทก
Demographic data: Dx, DOB, Wt. & Ht, Pedigree
LAB at first dx Serial CBC: Baseline HB
Hb typing of patient & family, molecular study
Blood group & minor blood group
Each visit
Wt. & Ht., type & volume of blood, reaction ?
CBC q visit, Cr, LFT, Serum ferritin q 3 month
Anti-HIV, HBsAg, Anti-HCV q year
No need to check post transfused Hct

Transfusion Reaction
ถามไขระหวางใหเลอด หยดการใหเลอด, V/S
ตรวจสอบความถกตอง,ให NSS แทน, H/C
Dx: Febrile non-hemolytic transfusion reaction
Cause: Ab to donor WBC, cytokine
Rx: Pre-medication : Paracet + CPM, LDPRC
หากอาการไมดข น DDx Hemolytic transfusion rxn, bacterial contamination

1 blood unit contains 200 mg
iron
PRC 1 ml Fe 1.16 mg
In addition, up to 4 mg/day
may be absorbed from the gut
Up to 1.5 g iron/year
Overload can occur after 10–20
transfusions
200–250 mg iron:
Whole blood: 0.47 mg iron/mL
‘Pure’ red cells: 1.16 mg iron/mL
Transfusion therapy results in iron overload
Porter JB. Br J Haematol 2001;115:239–52.
Iron overload is an inevitable consequence of multiple blood transfusions

Prevalence of complications in TDT
Cardiac siderosisLeft-sided heart failure
Hepatic failureViral hepatitis
HypothyroidismHypoparathyroidism
Diabetes mellitus
Hypogonadism
Osteoporosis
All patients (N = 1,073)Born after 1970 (n = 720)
6.8
1.8
6.8
4.1
4.1
3.6
3.2
2.7
50.8
6.6
14.8
3.3
3.3
3.3
8.2
9.7
600 5 10 15 20 25 30 35 40 45 50 55
Cardiacfailure
Arrhythmia
Myocardialinfarction
Infection
Cirrhosis
Thrombosis
Malignancy
Diabetes
Unknown
Other*
60.2
6.7
%
*Accident, renal failure, HIV/AIDS, familial autoimmune disorder, anorexia, haemolytic anaemia, thrombocytopenia.
Borgna-Pignatti C, et al. Ann N Y Acad Sci. 2005;1054:40-7.

Serum ferritin > 1,000 ng/mL
Liver iron concentration (LIC) from liver biopsy or
MRI (T2*) >/= 7 mg/g dry weight
Regular transfusion > 1 yr or > 10-20 times
Indication for Iron chelation therapy

Drug Desferrioxamine Deferiprone Deferasirox
Chelator:iron 1:1 3:1 2:1
Usual dosage 25-40 mg/kg/d 75 mg/kg/d 20-30 mg/kg/d
Route of
administration
Subcut,
Intravenous
Oral,
2-3 times daily
Oral,
Once daily
Half-life 20-30 min 3-4 hr. 12-16 hr.
Excretion Urinary, fecal Urinary Fecal
Adverse effect
Local reaction
Ophthalmologic
Auditory, Bone
abnormalities
GI disturbance
Agranulocytosis
Neutropenia
Arthralgia
Liver enzymes
GI disturbance
Rash
StatusLicensed
USALicensed in Europe
for who are unable to
use DFX effectively
Licensed
USA
Cost500 mg/Bottle
200 Baht
500 mg/tablet
GPO-L1® 5 B
Kelfer® 40B
250 mg/tab/500 B

TIF 2014 recommendation for Iron chelation therapy
Flow chart on Iron chelation in TM patients
Initiation of blood transfusion
Keep Hb level 9.5 -10.5 gm/dL
(pre-transfusional)
Upto 14 -15 gm/dL
(post-transfusional)
Iron chelation
First line treatment
Deferasirox 20-30 mg/kg/d
Desferrioxamine 30-50 mg/kg/day
Intolerance, switch Desferal DFX
Unsucessful, switch to Deferiprone
Monotherapy If not success
Combined with Desferal + L-1
Success, continue Desferal or DFX


การใหยาขบเหลกชนดฉด ควรใหเมอ serum ferritin > 1,000 ng/dl
ยาขบเหลก deferoxamine (desferal)
25-50 มก./1 กก. ฉดเขาใตผวหนงโดยใชเคร อง
pump นาน 8-10 ชม, 4-7 (5) คร ง/wk
ตรวจตาและการไดยนของผปวยกอนใหยา
ควรใหยาแกผปวยเมออาย >3-4 ป
ผปวยทไดรบยาอยางเหมาะสมท าใหมชวตยนยาวมากขน

การใหยาขบเหลกชนดฉด

การใหยาขบเหลกชนดรบประทาน
Deferiprone หรอ L1 75-100 มก/กก/วน แบงใหรบประทานวนละ 2-3 คร ง สามารถขบธาตเหลกมประสทธภาพด
ท าใหธาตเหลกทสะสมอยในหวใจมปรมาณลดลง
การใหยา Deferiprone 50-75 มก/กก/วนรวมกบ desferal S.C. 40-50 มก/กก/วน, 2-5 วน/สปดาหสามารถขบธาตเหลกมประสทธภาพเพมขน

ผลขางเคยงของยาขบเหลก L-1
คลนไส 10.8%
อาเจยน 8.6%
ปวดศรษะ 7.5%
เบออาหาร 5.4%
ปวดขอ 5.4%
ขออกเสบ 1.1%
ถายอจจาระบอย 2.2%

ผลขางเคยงของยาขบเหลก L-1
เมดเลอดขาวต า 11.8%
กดการท างานของไขกระดก 2.2%
เกลดเลอดต า 16.1 %
เอนไซมตบเพม 1.1%

การใหยาขบเหลกชนดรบประทาน
Deferasirox หรอ Exjade® 20-30 มก/กก/วน
โดยรบประทานวนละคร ง
สามารถขบธาตเหลกมประสทธภาพด
ผลขางเคยง:ผนทผวหนง ทองเสย
คลนไส อาเจยน ปวดทอง
Creatinine เพมขนเลกนอย
สามารถใหในเดกอาย 2 ปขนไป

ผลขางเคยงของยาขบเหลก Exjade®
ผนทผวหนง 25.8%
ถายอจจาระบอย 16.1%
เบออาหาร 4.8%
น าหนกลด 4.8%
บวม 4.8%
ปวดทอง 3.2%


Use of serum ferritin
• Assesses body iron stores (mainly in macrophage)
• Assesses “trend” of iron & monitor response to Rx
compliance, dose, regime monitoring
• Ferritin > 2,500 ug/L predict cardiac risk
• Ferritin < 1,000 ug/L increase DFO toxicity
• Unreliable screening in NTDT
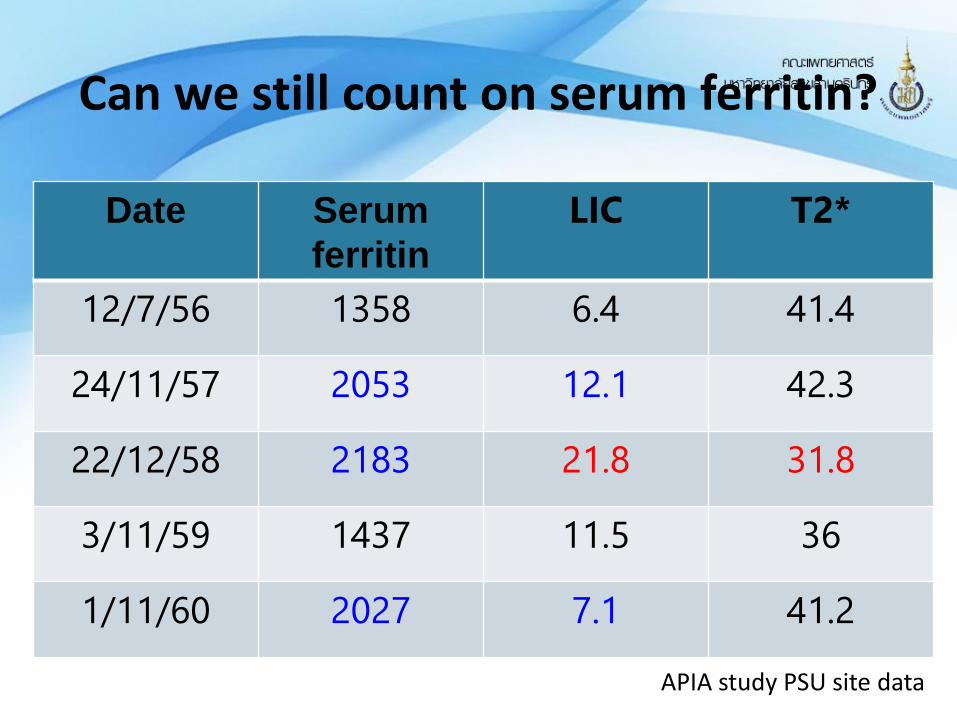
Date Serum
ferritin
LIC T2*
12/7/56 1358 6.4 41.4
24/11/57 2053 12.1 42.3
22/12/58 2183 21.8 31.8
3/11/59 1437 11.5 36
1/11/60 2027 7.1 41.2
Can we still count on serum ferritin?
APIA study PSU site data

Why not just use serum ferritin?
• Also raised by inflammation or tissue damage
• Lowered by vitamin C deficiency
• Unreliable when ferritin > 4,000 ug/L
• Low SF relative to LIC in Thal intermedia
(hepatocellular > macrophages)
• Relationship of ferritin to LIC differ with different drugs
Fischer et al. Br J Hematol 2003,121: 938-48

Most reliable estimate of body iron/ Non invasive
Evaluate iron status before BMT
Those who serum ferritin doesn’t correlate with clinical (identify iron balance)
LIC >/= 7 mg/g dry weight Chelation Rx
High LIC > 15-20 liver fibrosis, poor prognosis
Clinical application of MRI

LIC may not reflect myocardial iron
Anderson et al. Eur Heart J. 2001;22:2171
Normal cardiac iron
Severe liver iron overload
Severe cardiac iron deposit
Minimal liver iron
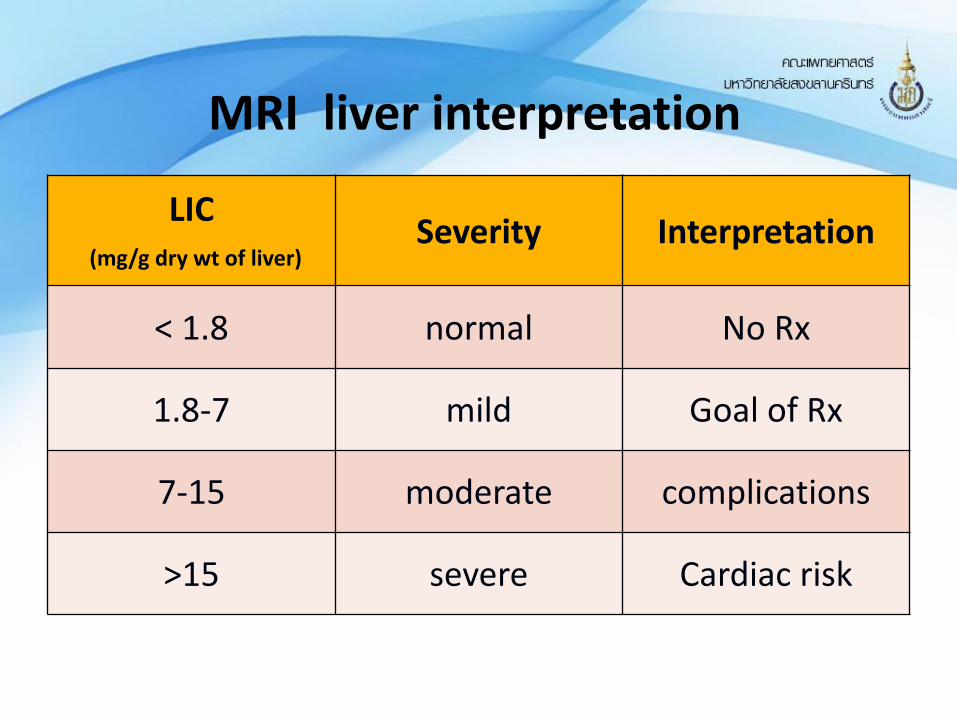
MRI liver interpretation
LIC(mg/g dry wt of liver)
Severity Interpretation
< 1.8 normal No Rx
1.8-7 mild Goal of Rx
7-15 moderate complications
>15 severe Cardiac risk

MRI cardiac T2* interpretation
T2* (msec) Interpretation
> 20 normal
10-20 Moderate to severe
< 20 severe
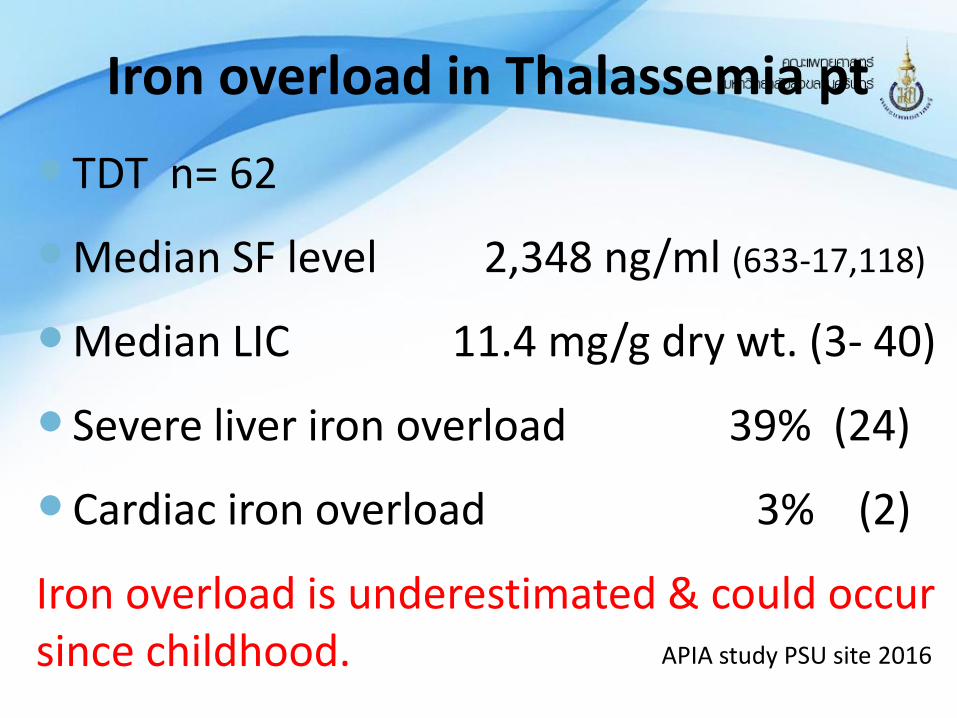
Iron overload in Thalassemia pt
TDT n= 62
Median SF level 2,348 ng/ml (633-17,118)
Median LIC 11.4 mg/g dry wt. (3- 40)
Severe liver iron overload 39% (24)
Cardiac iron overload 3% (2)
Iron overload is underestimated & could occur since childhood. APIA study PSU site 2016
New hope for Thalassemia patients ?
Transfusional therapy HSCT, Gene therapy Targeted therapy

Impaired α : β globin genes
Erythroid cell pathology
Minihepcidins
Hepcidin analogs
TMPRSS inhibitors
Hemolysis
Iron overload
Ineffective erythropoiesis
Alpha chain
synthesis reduction
JAK2 inhibitor
Sotatercept
Luspatercept
HSCT
Gene therapy
Gene editing
Hb F induction
Hematology Am Soc Hematol Educ Program. 2017; 1: 278-283
New therapeutic targets for TDT & NTDT

Only curable treatment for thalassemia patients
Matching probability: Sibling 1/4, Unrelated donor 1/ 50,000
Stem cell sources: bone marrow, cord blood, peripheral blood
DFS ~ 80-90%
Success depend on age & risk score
High cost treatment 400,000 – 1 M THB
Hematopoietic stem cell transplantation

ขนตอนการปลกถายเซลลตนก าเนดเมดเลอด
Donor
Stem cells
ยากดภมคมกน
ผปวย
Conditioning
ระยะปลกถาย หลงปลกถายกอนปลกถายEngraftment
ผปวย

Pesaro risk classification
Hepatomegaly
Hepatic fibrosis
Inadequate iron chelation ( DFO start >18 mo after dx)
Class I 0 risk factor ( OS 94%,DFS 87%)
Class II 1-2 risk factors ( OS 84%, DFS 81%)
Class III > 2 risk factors ( OS 65%, DFS 62%)

HSCT in children PSU experience
Total n= 21
• Transfusion dependent thalassemia 13
• Relapse/refractory leukemia 5
• Severe aplastic anemia 1
• WAS/Gaucher diesease 2
PSU experience 2017

Pre-HSCT management
Early HSCT yield the best outcome
Detect early if has sibling refer early
Choose LDPRC if plan for HSCT
Avoid blood from family to avoid graft failure
Adequate iron chelation PSU experience 2017
To cure … sometimesTo relief … often To comfort… always….
Thank you for your kind attention