update in carotid artery stenting & stroke management dr. nikolaos melas, phd vascular and...
TRANSCRIPT
UPDATE IN CAROTID ARTERY UPDATE IN CAROTID ARTERY STENTING amp STROKE STENTING amp STROKE
MANAGEMENTMANAGEMENT
Dr Nikolaos Melas PhDVascular and Endovascular Surgeon
Military Doctor
Associate in 1st department of Surgery Aristotle University of Thessaloniki Greece
Associate in Interbalcan Medical Center
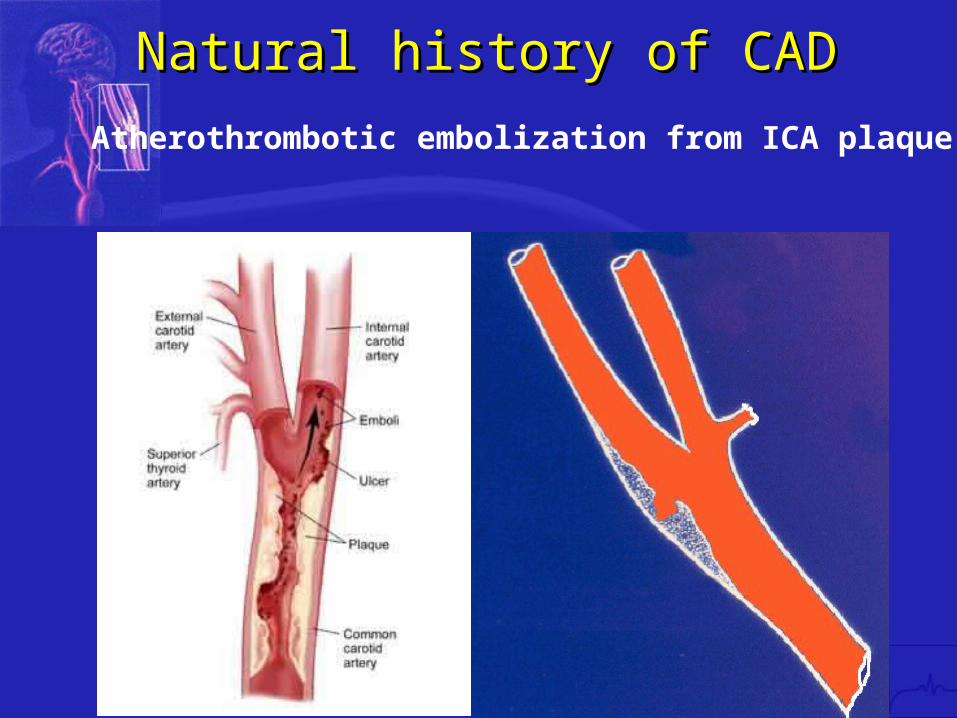
Atherothrombotic embolization from ICA plaque
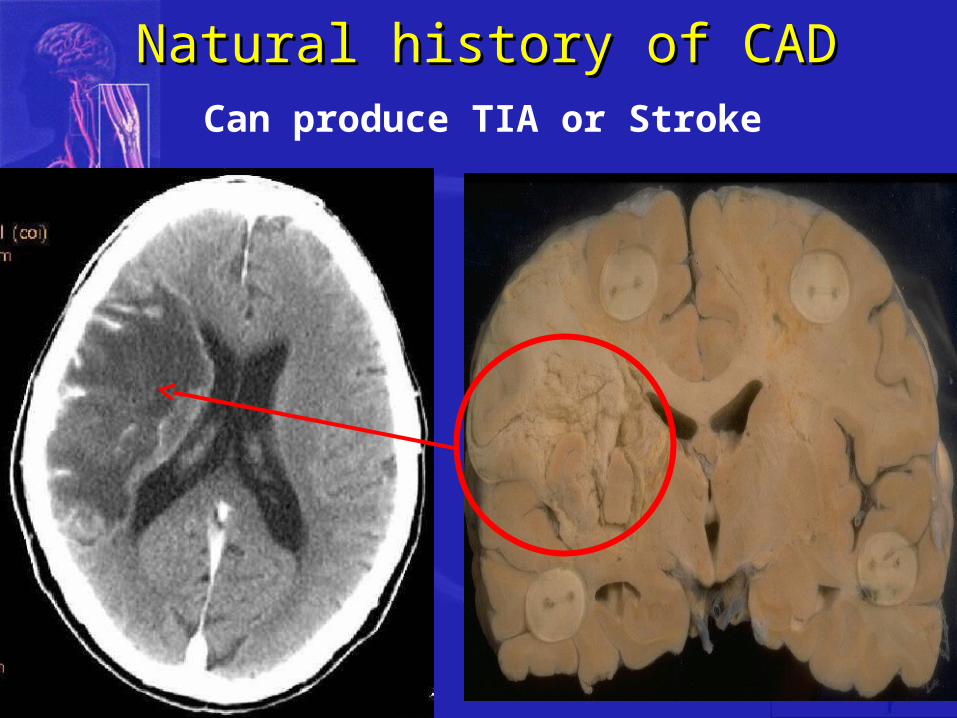
Natural history of CADNatural history of CAD
Natural history of CADNatural history of CADCan produce TIA or Stroke
Natural history of CADNatural history of CADCausing transient or permanent disability
And even deathStroke is the third leading cause of death worldwide1
1Moore WS et al Circulation 1995 91566 ndash79
bullA valuable therapeutic option for stroke management over simple medical treatment since 1954 Eastcott first description
CEACEAASPIRINASPIRIN
Carotid endarterectomy (CEA)Carotid endarterectomy (CEA)
TrialTrialTrialTrial Mean Mean Follow-upFollow-upMean Mean Follow-upFollow-up
Rate of New Rate of New Neurologic EventsNeurologic Events
Rate of New Rate of New Neurologic EventsNeurologic Events
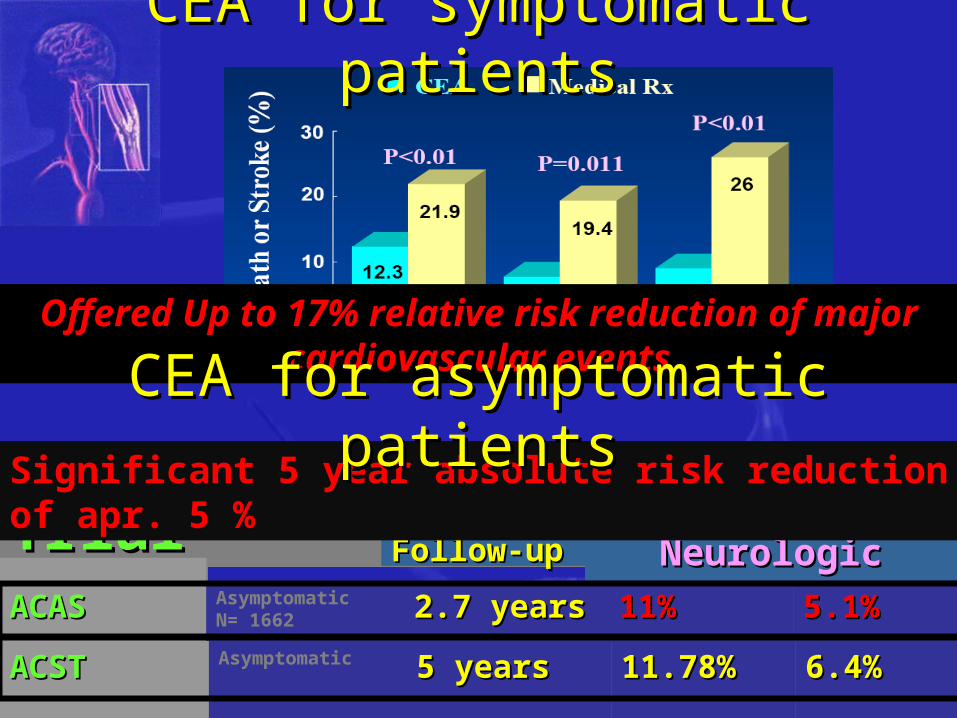
ACASACASACASACAS AsymptomaticN= 1662 27 years27 years27 years27 years 11111111 51515151
ACSTACSTACSTACST Asymptomatic 5 years5 years5 years5 years 1178117811781178 64646464
Significant 5 year absolute risk reduction of apr 5
Offered Up to 17 relative risk reduction of major cardiovascular events
CEA for symptomatic patientsCEA for symptomatic patients
CEA for asymptomatic patientsCEA for asymptomatic patients
Carotid endarterectomy (CEA)Carotid endarterectomy (CEA)
Carotid Artery Stenting (CAS)Carotid Artery Stenting (CAS)bullLess invasivebullLess traumaticbullLess time consuming bullPainlessbullAvoids neck incisionsbullAvoids nerve damagebullAvoids systemic complications related to anesthesia
Remained the gold standard for carotid Remained the gold standard for carotid artery disease for many years as an artery disease for many years as an
evidence based procedureevidence based procedure
RESULTS
Single center retrospective reports Initial experience with CAS
Prospective multicenter registries for CAS
CAS vs CEA Controlled trials
CAS vs CEA meta- analysis (Cochrane review)
Evidence for CAS
Controlled trials CAS vs CEA
meta- analysis (Cochrane review)
Ederle J et al Cochrane systematic review Stroke 200940(4)1373-80
Coward L et al Cochrane systematic review Stroke 2005 36905-11
Controlled trials comparing CAS with CEA
Ederle J et al Cochrane systematic review Stroke 2009 Apr40(4)1373-80
Slightly favored CEA
Death or stroke within 30 days of procedure
Criticism on EVA-3S and SPACE trials- weak points
bull inadequate sample size (type II statistical error)
bull different stent systems
bull different protocols in pre- and post- administration of antiplatelet drugs
bull not uniform use of EPDs
bull not similar patient groups (eg four times as many people with contralateral ICA occlusion in the CAS group in EVA-3S)
bull surprisingly better results of French surgeons (EVA-3S) in performing CEA comparing to NASCET and ECST (39 vs 65 and 71)
The results do not support a change in clinical practice away from recommending carotid endarterectomy as the treatment of choice for suitable carotid artery stenosis but support continued recruitment in the large ongoing trials
Trial Year FU CAS ips stroke CEA ips stroke P Article
SPACE 2008 2 years 95 885 NS Lancet Neurol 2008 7 893-902
EVA-3s 2008 4 years After the periprocedural period the risk of ipsilateral stroke was low and similar in both treatment groups
NS Lancet Neurol 2008 7 885-892
SAPPHIRE 2008 3 years 6 87 NS N Engl j Med 2008 358 1572-79
CAVATAS 2009 5 years 11middot3 8middot6 NS Lancet Neurol 20098(10)898-907
CREST 2011
Mid and Long term results (6m-5 years)
Coward LJ et al Cochrane review Stroke 200536905-911
Equal results between CEA and CAS
Cranial neuropathy
Stronly favored CAS
No significant difference in the major risks of treatment
Minor complication favorendovascular treatment
Conclusions
Insufficient evidence to support a widespread change in clinical practice
So which is the VERDICT
Current trials didnrsquot prove CAS inferiority
The initial question about gold standard is wrong
vsXBoth CAS CEAand
Play a role in stroke prevention in different patient groups
Defining patient groups that either CEA or CAS is beneficial
Vessel anatomy Plaque characteristics
The high risk patient
Defining patient groups that either CEA or CAS is beneficial
Vessel anatomyPlaque characteristics
The high risk patient
The influence of anatomy on treatment selection for carotid disease
1 Congenital anatomical variation (bovine arch aortic arch types I-III high or low carotid bifurcation aberrant vessels)
2 Alterations that occur with aging and hypertension (inflow and outflow tortuousity calcification thrombi)
3 Extension of disease (eg diffuse multisegmental disease involving the proximal CCA or distal ICA)
Vessel anatomy
Schneider PA et al Semin Vasc Surg 20216-225 2007
Vessel anatomy
Aortic arch type and orificial calcification
Vessel anatomy
Mobile thrombi Vessel anatomy
Vessel anatomyBovine carotid configuration
Proximal common carotid lesionsVessel anatomy
Tortuous CCA or ICA coil
Vessel anatomy
ldquoString signrdquo carotid morphology
Would you advance an EPD into such a vessel
Vessel anatomy
Defining patient groups that either CEA or CAS is beneficial
Vessel anatomyPlaque characteristics
The high risk patient
Plaque characteristics
Biasi et al ICAROS study Circulation 2004110756-62Fisher M et al Stroke 200536253ndash7Rothwell PM et al Stroke 200031615ndash21
bullGSMlt25 is related with a higher risk of neurologic complications after CASbulllow GSM is not a contraindication to CAS but rather a predictor of increased stroke riskbullLow GSM values are further related to future coronary events and higher rate of restenosis
Defining patient groups that either CEA or CAS is beneficial
Vessel anatomy Plaque characteristics
The high risk patient
24 30
60
96
12
3624
48
0
5
10
15
20
25
Death Stroke MI MAE
CEA (n=167)
Stent (n=167)
30 Days endpoint
P=068 P=100P=017
P=014
Theldquohigh riskrdquo patient
126
7260
192
72
120
24
60
0
5
10
15
20
25
Death Stroke MI MAE
CEA (n=167)Stent (n=167)
SAPPHIRE CAS vs CEA
1 year results
P=014
P=083P=017
P=010
CEA can be performed in high-risk patients with acceptable standard complication rates
Mozes G et al Semin Vasc Surg 20051861ndash 8
octogenarians
121121
30-day stroke and death rate30-day stroke and death rate
5353 1313
Agegt80yAgegt80y Age 70-79yAge 70-79y Age 60-69Age 60-69
Is CAS safe in this subgroup
The CREST trial lead-in phase
Material - Methodsbull 67 monthsbull 520 patientsbull mean age 76 range 56-85bull 364 male (70) 156 female (30)bull mean follow-up was 32 months (range 1 ndash 54 months)
Retrospective study
bull We conducted a retrospective review of CAS from 2003 to 2008bull RX Acculink - RX Accunet carotid system (Guidant Abott)
Material - Methods
bull Symptomatic (stroke (135) TIA Fugax) 515
bull Asymptomatic 485
Results within early follow-up (lt30 days)
bull Mortality (09)Stroke (11)TIA (13)Non fatal MI (13)
MAE 46
Results within early follow-up (lt30 days)
Predictors of adverse outcomes includedbullAge gt80bullsymptomatic patientsbullFemale genderbullpredilation prior to CPD bullplacement of multiple stentsbullContralateral occlusionbullUnfavorable anatomy
Late Follow-Up (gt30 days)
bull Mortality (173 )Stroke (07)Restenosis gt70 (23)
Mean follow-up was 32 months (range 1 ndash 60 months) 46 (88) patients lost of FU
Conclusion
bullCAS within experienced hands can be highly efficient and durable
Acculink Accunet system is safe and effective for CAS
ConclusionsCEA is the goal standard when
bull specific carotid anatomy
bullExtensive arch and carotid bif calcification
bullAccess related problems
bullFresh thrombus at ICA lesion
bullldquoString signrdquo morphology
bullVery low GSM
Conclusions
CAS and CEA are not competitive procedures but powerful treatment options tailored on different groups of patients
The gold standard is the experienced vascular team able to twist between endovascular and open surgical options in order to achieve the best treatment for the patient
Thank you for your attention
- Slide 1
- Slide 2
- Slide 3
- Slide 4
- Slide 5
- Slide 6
- Slide 7
- Slide 8
- Slide 9
- Slide 10
- Slide 11
- Slide 12
- Slide 13
- Slide 14
- Slide 15
- Slide 16
- Slide 17
- Slide 18
- Slide 19
- Slide 20
- Slide 21
- Slide 22
- Slide 23
- Slide 24
- Slide 25
- Slide 26
- Slide 27
- Slide 28
- Slide 29
- Slide 30
- Slide 31
- Slide 32
- Slide 33
- Slide 34
- Slide 35
- Slide 36
- Slide 37
- Slide 38
- Slide 39
- Slide 40
-
Atherothrombotic embolization from ICA plaque
Natural history of CADNatural history of CAD
Natural history of CADNatural history of CADCan produce TIA or Stroke
Natural history of CADNatural history of CADCausing transient or permanent disability
And even deathStroke is the third leading cause of death worldwide1
1Moore WS et al Circulation 1995 91566 ndash79
bullA valuable therapeutic option for stroke management over simple medical treatment since 1954 Eastcott first description
CEACEAASPIRINASPIRIN
Carotid endarterectomy (CEA)Carotid endarterectomy (CEA)
TrialTrialTrialTrial Mean Mean Follow-upFollow-upMean Mean Follow-upFollow-up
Rate of New Rate of New Neurologic EventsNeurologic Events
Rate of New Rate of New Neurologic EventsNeurologic Events
ACASACASACASACAS AsymptomaticN= 1662 27 years27 years27 years27 years 11111111 51515151
ACSTACSTACSTACST Asymptomatic 5 years5 years5 years5 years 1178117811781178 64646464
Significant 5 year absolute risk reduction of apr 5
Offered Up to 17 relative risk reduction of major cardiovascular events
CEA for symptomatic patientsCEA for symptomatic patients
CEA for asymptomatic patientsCEA for asymptomatic patients
Carotid endarterectomy (CEA)Carotid endarterectomy (CEA)
Carotid Artery Stenting (CAS)Carotid Artery Stenting (CAS)bullLess invasivebullLess traumaticbullLess time consuming bullPainlessbullAvoids neck incisionsbullAvoids nerve damagebullAvoids systemic complications related to anesthesia
Remained the gold standard for carotid Remained the gold standard for carotid artery disease for many years as an artery disease for many years as an
evidence based procedureevidence based procedure
RESULTS
Single center retrospective reports Initial experience with CAS
Prospective multicenter registries for CAS
CAS vs CEA Controlled trials
CAS vs CEA meta- analysis (Cochrane review)
Evidence for CAS
Controlled trials CAS vs CEA
meta- analysis (Cochrane review)
Ederle J et al Cochrane systematic review Stroke 200940(4)1373-80
Coward L et al Cochrane systematic review Stroke 2005 36905-11
Controlled trials comparing CAS with CEA
Ederle J et al Cochrane systematic review Stroke 2009 Apr40(4)1373-80
Slightly favored CEA
Death or stroke within 30 days of procedure
Criticism on EVA-3S and SPACE trials- weak points
bull inadequate sample size (type II statistical error)
bull different stent systems
bull different protocols in pre- and post- administration of antiplatelet drugs
bull not uniform use of EPDs
bull not similar patient groups (eg four times as many people with contralateral ICA occlusion in the CAS group in EVA-3S)
bull surprisingly better results of French surgeons (EVA-3S) in performing CEA comparing to NASCET and ECST (39 vs 65 and 71)
The results do not support a change in clinical practice away from recommending carotid endarterectomy as the treatment of choice for suitable carotid artery stenosis but support continued recruitment in the large ongoing trials
Trial Year FU CAS ips stroke CEA ips stroke P Article
SPACE 2008 2 years 95 885 NS Lancet Neurol 2008 7 893-902
EVA-3s 2008 4 years After the periprocedural period the risk of ipsilateral stroke was low and similar in both treatment groups
NS Lancet Neurol 2008 7 885-892
SAPPHIRE 2008 3 years 6 87 NS N Engl j Med 2008 358 1572-79
CAVATAS 2009 5 years 11middot3 8middot6 NS Lancet Neurol 20098(10)898-907
CREST 2011
Mid and Long term results (6m-5 years)
Coward LJ et al Cochrane review Stroke 200536905-911
Equal results between CEA and CAS
Cranial neuropathy
Stronly favored CAS
No significant difference in the major risks of treatment
Minor complication favorendovascular treatment
Conclusions
Insufficient evidence to support a widespread change in clinical practice
So which is the VERDICT
Current trials didnrsquot prove CAS inferiority
The initial question about gold standard is wrong
vsXBoth CAS CEAand
Play a role in stroke prevention in different patient groups
Defining patient groups that either CEA or CAS is beneficial
Vessel anatomy Plaque characteristics
The high risk patient
Defining patient groups that either CEA or CAS is beneficial
Vessel anatomyPlaque characteristics
The high risk patient
The influence of anatomy on treatment selection for carotid disease
1 Congenital anatomical variation (bovine arch aortic arch types I-III high or low carotid bifurcation aberrant vessels)
2 Alterations that occur with aging and hypertension (inflow and outflow tortuousity calcification thrombi)
3 Extension of disease (eg diffuse multisegmental disease involving the proximal CCA or distal ICA)
Vessel anatomy
Schneider PA et al Semin Vasc Surg 20216-225 2007
Vessel anatomy
Aortic arch type and orificial calcification
Vessel anatomy
Mobile thrombi Vessel anatomy
Vessel anatomyBovine carotid configuration
Proximal common carotid lesionsVessel anatomy
Tortuous CCA or ICA coil
Vessel anatomy
ldquoString signrdquo carotid morphology
Would you advance an EPD into such a vessel
Vessel anatomy
Defining patient groups that either CEA or CAS is beneficial
Vessel anatomyPlaque characteristics
The high risk patient
Plaque characteristics
Biasi et al ICAROS study Circulation 2004110756-62Fisher M et al Stroke 200536253ndash7Rothwell PM et al Stroke 200031615ndash21
bullGSMlt25 is related with a higher risk of neurologic complications after CASbulllow GSM is not a contraindication to CAS but rather a predictor of increased stroke riskbullLow GSM values are further related to future coronary events and higher rate of restenosis
Defining patient groups that either CEA or CAS is beneficial
Vessel anatomy Plaque characteristics
The high risk patient
24 30
60
96
12
3624
48
0
5
10
15
20
25
Death Stroke MI MAE
CEA (n=167)
Stent (n=167)
30 Days endpoint
P=068 P=100P=017
P=014
Theldquohigh riskrdquo patient
126
7260
192
72
120
24
60
0
5
10
15
20
25
Death Stroke MI MAE
CEA (n=167)Stent (n=167)
SAPPHIRE CAS vs CEA
1 year results
P=014
P=083P=017
P=010
CEA can be performed in high-risk patients with acceptable standard complication rates
Mozes G et al Semin Vasc Surg 20051861ndash 8
octogenarians
121121
30-day stroke and death rate30-day stroke and death rate
5353 1313
Agegt80yAgegt80y Age 70-79yAge 70-79y Age 60-69Age 60-69
Is CAS safe in this subgroup
The CREST trial lead-in phase
Material - Methodsbull 67 monthsbull 520 patientsbull mean age 76 range 56-85bull 364 male (70) 156 female (30)bull mean follow-up was 32 months (range 1 ndash 54 months)
Retrospective study
bull We conducted a retrospective review of CAS from 2003 to 2008bull RX Acculink - RX Accunet carotid system (Guidant Abott)
Material - Methods
bull Symptomatic (stroke (135) TIA Fugax) 515
bull Asymptomatic 485
Results within early follow-up (lt30 days)
bull Mortality (09)Stroke (11)TIA (13)Non fatal MI (13)
MAE 46
Results within early follow-up (lt30 days)
Predictors of adverse outcomes includedbullAge gt80bullsymptomatic patientsbullFemale genderbullpredilation prior to CPD bullplacement of multiple stentsbullContralateral occlusionbullUnfavorable anatomy
Late Follow-Up (gt30 days)
bull Mortality (173 )Stroke (07)Restenosis gt70 (23)
Mean follow-up was 32 months (range 1 ndash 60 months) 46 (88) patients lost of FU
Conclusion
bullCAS within experienced hands can be highly efficient and durable
Acculink Accunet system is safe and effective for CAS
ConclusionsCEA is the goal standard when
bull specific carotid anatomy
bullExtensive arch and carotid bif calcification
bullAccess related problems
bullFresh thrombus at ICA lesion
bullldquoString signrdquo morphology
bullVery low GSM
Conclusions
CAS and CEA are not competitive procedures but powerful treatment options tailored on different groups of patients
The gold standard is the experienced vascular team able to twist between endovascular and open surgical options in order to achieve the best treatment for the patient
Thank you for your attention
- Slide 1
- Slide 2
- Slide 3
- Slide 4
- Slide 5
- Slide 6
- Slide 7
- Slide 8
- Slide 9
- Slide 10
- Slide 11
- Slide 12
- Slide 13
- Slide 14
- Slide 15
- Slide 16
- Slide 17
- Slide 18
- Slide 19
- Slide 20
- Slide 21
- Slide 22
- Slide 23
- Slide 24
- Slide 25
- Slide 26
- Slide 27
- Slide 28
- Slide 29
- Slide 30
- Slide 31
- Slide 32
- Slide 33
- Slide 34
- Slide 35
- Slide 36
- Slide 37
- Slide 38
- Slide 39
- Slide 40
-
Natural history of CADNatural history of CADCan produce TIA or Stroke
Natural history of CADNatural history of CADCausing transient or permanent disability
And even deathStroke is the third leading cause of death worldwide1
1Moore WS et al Circulation 1995 91566 ndash79
bullA valuable therapeutic option for stroke management over simple medical treatment since 1954 Eastcott first description
CEACEAASPIRINASPIRIN
Carotid endarterectomy (CEA)Carotid endarterectomy (CEA)
TrialTrialTrialTrial Mean Mean Follow-upFollow-upMean Mean Follow-upFollow-up
Rate of New Rate of New Neurologic EventsNeurologic Events
Rate of New Rate of New Neurologic EventsNeurologic Events
ACASACASACASACAS AsymptomaticN= 1662 27 years27 years27 years27 years 11111111 51515151
ACSTACSTACSTACST Asymptomatic 5 years5 years5 years5 years 1178117811781178 64646464
Significant 5 year absolute risk reduction of apr 5
Offered Up to 17 relative risk reduction of major cardiovascular events
CEA for symptomatic patientsCEA for symptomatic patients
CEA for asymptomatic patientsCEA for asymptomatic patients
Carotid endarterectomy (CEA)Carotid endarterectomy (CEA)
Carotid Artery Stenting (CAS)Carotid Artery Stenting (CAS)bullLess invasivebullLess traumaticbullLess time consuming bullPainlessbullAvoids neck incisionsbullAvoids nerve damagebullAvoids systemic complications related to anesthesia
Remained the gold standard for carotid Remained the gold standard for carotid artery disease for many years as an artery disease for many years as an
evidence based procedureevidence based procedure
RESULTS
Single center retrospective reports Initial experience with CAS
Prospective multicenter registries for CAS
CAS vs CEA Controlled trials
CAS vs CEA meta- analysis (Cochrane review)
Evidence for CAS
Controlled trials CAS vs CEA
meta- analysis (Cochrane review)
Ederle J et al Cochrane systematic review Stroke 200940(4)1373-80
Coward L et al Cochrane systematic review Stroke 2005 36905-11
Controlled trials comparing CAS with CEA
Ederle J et al Cochrane systematic review Stroke 2009 Apr40(4)1373-80
Slightly favored CEA
Death or stroke within 30 days of procedure
Criticism on EVA-3S and SPACE trials- weak points
bull inadequate sample size (type II statistical error)
bull different stent systems
bull different protocols in pre- and post- administration of antiplatelet drugs
bull not uniform use of EPDs
bull not similar patient groups (eg four times as many people with contralateral ICA occlusion in the CAS group in EVA-3S)
bull surprisingly better results of French surgeons (EVA-3S) in performing CEA comparing to NASCET and ECST (39 vs 65 and 71)
The results do not support a change in clinical practice away from recommending carotid endarterectomy as the treatment of choice for suitable carotid artery stenosis but support continued recruitment in the large ongoing trials
Trial Year FU CAS ips stroke CEA ips stroke P Article
SPACE 2008 2 years 95 885 NS Lancet Neurol 2008 7 893-902
EVA-3s 2008 4 years After the periprocedural period the risk of ipsilateral stroke was low and similar in both treatment groups
NS Lancet Neurol 2008 7 885-892
SAPPHIRE 2008 3 years 6 87 NS N Engl j Med 2008 358 1572-79
CAVATAS 2009 5 years 11middot3 8middot6 NS Lancet Neurol 20098(10)898-907
CREST 2011
Mid and Long term results (6m-5 years)
Coward LJ et al Cochrane review Stroke 200536905-911
Equal results between CEA and CAS
Cranial neuropathy
Stronly favored CAS
No significant difference in the major risks of treatment
Minor complication favorendovascular treatment
Conclusions
Insufficient evidence to support a widespread change in clinical practice
So which is the VERDICT
Current trials didnrsquot prove CAS inferiority
The initial question about gold standard is wrong
vsXBoth CAS CEAand
Play a role in stroke prevention in different patient groups
Defining patient groups that either CEA or CAS is beneficial
Vessel anatomy Plaque characteristics
The high risk patient
Defining patient groups that either CEA or CAS is beneficial
Vessel anatomyPlaque characteristics
The high risk patient
The influence of anatomy on treatment selection for carotid disease
1 Congenital anatomical variation (bovine arch aortic arch types I-III high or low carotid bifurcation aberrant vessels)
2 Alterations that occur with aging and hypertension (inflow and outflow tortuousity calcification thrombi)
3 Extension of disease (eg diffuse multisegmental disease involving the proximal CCA or distal ICA)
Vessel anatomy
Schneider PA et al Semin Vasc Surg 20216-225 2007
Vessel anatomy
Aortic arch type and orificial calcification
Vessel anatomy
Mobile thrombi Vessel anatomy
Vessel anatomyBovine carotid configuration
Proximal common carotid lesionsVessel anatomy
Tortuous CCA or ICA coil
Vessel anatomy
ldquoString signrdquo carotid morphology
Would you advance an EPD into such a vessel
Vessel anatomy
Defining patient groups that either CEA or CAS is beneficial
Vessel anatomyPlaque characteristics
The high risk patient
Plaque characteristics
Biasi et al ICAROS study Circulation 2004110756-62Fisher M et al Stroke 200536253ndash7Rothwell PM et al Stroke 200031615ndash21
bullGSMlt25 is related with a higher risk of neurologic complications after CASbulllow GSM is not a contraindication to CAS but rather a predictor of increased stroke riskbullLow GSM values are further related to future coronary events and higher rate of restenosis
Defining patient groups that either CEA or CAS is beneficial
Vessel anatomy Plaque characteristics
The high risk patient
24 30
60
96
12
3624
48
0
5
10
15
20
25
Death Stroke MI MAE
CEA (n=167)
Stent (n=167)
30 Days endpoint
P=068 P=100P=017
P=014
Theldquohigh riskrdquo patient
126
7260
192
72
120
24
60
0
5
10
15
20
25
Death Stroke MI MAE
CEA (n=167)Stent (n=167)
SAPPHIRE CAS vs CEA
1 year results
P=014
P=083P=017
P=010
CEA can be performed in high-risk patients with acceptable standard complication rates
Mozes G et al Semin Vasc Surg 20051861ndash 8
octogenarians
121121
30-day stroke and death rate30-day stroke and death rate
5353 1313
Agegt80yAgegt80y Age 70-79yAge 70-79y Age 60-69Age 60-69
Is CAS safe in this subgroup
The CREST trial lead-in phase
Material - Methodsbull 67 monthsbull 520 patientsbull mean age 76 range 56-85bull 364 male (70) 156 female (30)bull mean follow-up was 32 months (range 1 ndash 54 months)
Retrospective study
bull We conducted a retrospective review of CAS from 2003 to 2008bull RX Acculink - RX Accunet carotid system (Guidant Abott)
Material - Methods
bull Symptomatic (stroke (135) TIA Fugax) 515
bull Asymptomatic 485
Results within early follow-up (lt30 days)
bull Mortality (09)Stroke (11)TIA (13)Non fatal MI (13)
MAE 46
Results within early follow-up (lt30 days)
Predictors of adverse outcomes includedbullAge gt80bullsymptomatic patientsbullFemale genderbullpredilation prior to CPD bullplacement of multiple stentsbullContralateral occlusionbullUnfavorable anatomy
Late Follow-Up (gt30 days)
bull Mortality (173 )Stroke (07)Restenosis gt70 (23)
Mean follow-up was 32 months (range 1 ndash 60 months) 46 (88) patients lost of FU
Conclusion
bullCAS within experienced hands can be highly efficient and durable
Acculink Accunet system is safe and effective for CAS
ConclusionsCEA is the goal standard when
bull specific carotid anatomy
bullExtensive arch and carotid bif calcification
bullAccess related problems
bullFresh thrombus at ICA lesion
bullldquoString signrdquo morphology
bullVery low GSM
Conclusions
CAS and CEA are not competitive procedures but powerful treatment options tailored on different groups of patients
The gold standard is the experienced vascular team able to twist between endovascular and open surgical options in order to achieve the best treatment for the patient
Thank you for your attention
- Slide 1
- Slide 2
- Slide 3
- Slide 4
- Slide 5
- Slide 6
- Slide 7
- Slide 8
- Slide 9
- Slide 10
- Slide 11
- Slide 12
- Slide 13
- Slide 14
- Slide 15
- Slide 16
- Slide 17
- Slide 18
- Slide 19
- Slide 20
- Slide 21
- Slide 22
- Slide 23
- Slide 24
- Slide 25
- Slide 26
- Slide 27
- Slide 28
- Slide 29
- Slide 30
- Slide 31
- Slide 32
- Slide 33
- Slide 34
- Slide 35
- Slide 36
- Slide 37
- Slide 38
- Slide 39
- Slide 40
-
Natural history of CADNatural history of CADCausing transient or permanent disability
And even deathStroke is the third leading cause of death worldwide1
1Moore WS et al Circulation 1995 91566 ndash79
bullA valuable therapeutic option for stroke management over simple medical treatment since 1954 Eastcott first description
CEACEAASPIRINASPIRIN
Carotid endarterectomy (CEA)Carotid endarterectomy (CEA)
TrialTrialTrialTrial Mean Mean Follow-upFollow-upMean Mean Follow-upFollow-up
Rate of New Rate of New Neurologic EventsNeurologic Events
Rate of New Rate of New Neurologic EventsNeurologic Events
ACASACASACASACAS AsymptomaticN= 1662 27 years27 years27 years27 years 11111111 51515151
ACSTACSTACSTACST Asymptomatic 5 years5 years5 years5 years 1178117811781178 64646464
Significant 5 year absolute risk reduction of apr 5
Offered Up to 17 relative risk reduction of major cardiovascular events
CEA for symptomatic patientsCEA for symptomatic patients
CEA for asymptomatic patientsCEA for asymptomatic patients
Carotid endarterectomy (CEA)Carotid endarterectomy (CEA)
Carotid Artery Stenting (CAS)Carotid Artery Stenting (CAS)bullLess invasivebullLess traumaticbullLess time consuming bullPainlessbullAvoids neck incisionsbullAvoids nerve damagebullAvoids systemic complications related to anesthesia
Remained the gold standard for carotid Remained the gold standard for carotid artery disease for many years as an artery disease for many years as an
evidence based procedureevidence based procedure
RESULTS
Single center retrospective reports Initial experience with CAS
Prospective multicenter registries for CAS
CAS vs CEA Controlled trials
CAS vs CEA meta- analysis (Cochrane review)
Evidence for CAS
Controlled trials CAS vs CEA
meta- analysis (Cochrane review)
Ederle J et al Cochrane systematic review Stroke 200940(4)1373-80
Coward L et al Cochrane systematic review Stroke 2005 36905-11
Controlled trials comparing CAS with CEA
Ederle J et al Cochrane systematic review Stroke 2009 Apr40(4)1373-80
Slightly favored CEA
Death or stroke within 30 days of procedure
Criticism on EVA-3S and SPACE trials- weak points
bull inadequate sample size (type II statistical error)
bull different stent systems
bull different protocols in pre- and post- administration of antiplatelet drugs
bull not uniform use of EPDs
bull not similar patient groups (eg four times as many people with contralateral ICA occlusion in the CAS group in EVA-3S)
bull surprisingly better results of French surgeons (EVA-3S) in performing CEA comparing to NASCET and ECST (39 vs 65 and 71)
The results do not support a change in clinical practice away from recommending carotid endarterectomy as the treatment of choice for suitable carotid artery stenosis but support continued recruitment in the large ongoing trials
Trial Year FU CAS ips stroke CEA ips stroke P Article
SPACE 2008 2 years 95 885 NS Lancet Neurol 2008 7 893-902
EVA-3s 2008 4 years After the periprocedural period the risk of ipsilateral stroke was low and similar in both treatment groups
NS Lancet Neurol 2008 7 885-892
SAPPHIRE 2008 3 years 6 87 NS N Engl j Med 2008 358 1572-79
CAVATAS 2009 5 years 11middot3 8middot6 NS Lancet Neurol 20098(10)898-907
CREST 2011
Mid and Long term results (6m-5 years)
Coward LJ et al Cochrane review Stroke 200536905-911
Equal results between CEA and CAS
Cranial neuropathy
Stronly favored CAS
No significant difference in the major risks of treatment
Minor complication favorendovascular treatment
Conclusions
Insufficient evidence to support a widespread change in clinical practice
So which is the VERDICT
Current trials didnrsquot prove CAS inferiority
The initial question about gold standard is wrong
vsXBoth CAS CEAand
Play a role in stroke prevention in different patient groups
Defining patient groups that either CEA or CAS is beneficial
Vessel anatomy Plaque characteristics
The high risk patient
Defining patient groups that either CEA or CAS is beneficial
Vessel anatomyPlaque characteristics
The high risk patient
The influence of anatomy on treatment selection for carotid disease
1 Congenital anatomical variation (bovine arch aortic arch types I-III high or low carotid bifurcation aberrant vessels)
2 Alterations that occur with aging and hypertension (inflow and outflow tortuousity calcification thrombi)
3 Extension of disease (eg diffuse multisegmental disease involving the proximal CCA or distal ICA)
Vessel anatomy
Schneider PA et al Semin Vasc Surg 20216-225 2007
Vessel anatomy
Aortic arch type and orificial calcification
Vessel anatomy
Mobile thrombi Vessel anatomy
Vessel anatomyBovine carotid configuration
Proximal common carotid lesionsVessel anatomy
Tortuous CCA or ICA coil
Vessel anatomy
ldquoString signrdquo carotid morphology
Would you advance an EPD into such a vessel
Vessel anatomy
Defining patient groups that either CEA or CAS is beneficial
Vessel anatomyPlaque characteristics
The high risk patient
Plaque characteristics
Biasi et al ICAROS study Circulation 2004110756-62Fisher M et al Stroke 200536253ndash7Rothwell PM et al Stroke 200031615ndash21
bullGSMlt25 is related with a higher risk of neurologic complications after CASbulllow GSM is not a contraindication to CAS but rather a predictor of increased stroke riskbullLow GSM values are further related to future coronary events and higher rate of restenosis
Defining patient groups that either CEA or CAS is beneficial
Vessel anatomy Plaque characteristics
The high risk patient
24 30
60
96
12
3624
48
0
5
10
15
20
25
Death Stroke MI MAE
CEA (n=167)
Stent (n=167)
30 Days endpoint
P=068 P=100P=017
P=014
Theldquohigh riskrdquo patient
126
7260
192
72
120
24
60
0
5
10
15
20
25
Death Stroke MI MAE
CEA (n=167)Stent (n=167)
SAPPHIRE CAS vs CEA
1 year results
P=014
P=083P=017
P=010
CEA can be performed in high-risk patients with acceptable standard complication rates
Mozes G et al Semin Vasc Surg 20051861ndash 8
octogenarians
121121
30-day stroke and death rate30-day stroke and death rate
5353 1313
Agegt80yAgegt80y Age 70-79yAge 70-79y Age 60-69Age 60-69
Is CAS safe in this subgroup
The CREST trial lead-in phase
Material - Methodsbull 67 monthsbull 520 patientsbull mean age 76 range 56-85bull 364 male (70) 156 female (30)bull mean follow-up was 32 months (range 1 ndash 54 months)
Retrospective study
bull We conducted a retrospective review of CAS from 2003 to 2008bull RX Acculink - RX Accunet carotid system (Guidant Abott)
Material - Methods
bull Symptomatic (stroke (135) TIA Fugax) 515
bull Asymptomatic 485
Results within early follow-up (lt30 days)
bull Mortality (09)Stroke (11)TIA (13)Non fatal MI (13)
MAE 46
Results within early follow-up (lt30 days)
Predictors of adverse outcomes includedbullAge gt80bullsymptomatic patientsbullFemale genderbullpredilation prior to CPD bullplacement of multiple stentsbullContralateral occlusionbullUnfavorable anatomy
Late Follow-Up (gt30 days)
bull Mortality (173 )Stroke (07)Restenosis gt70 (23)
Mean follow-up was 32 months (range 1 ndash 60 months) 46 (88) patients lost of FU
Conclusion
bullCAS within experienced hands can be highly efficient and durable
Acculink Accunet system is safe and effective for CAS
ConclusionsCEA is the goal standard when
bull specific carotid anatomy
bullExtensive arch and carotid bif calcification
bullAccess related problems
bullFresh thrombus at ICA lesion
bullldquoString signrdquo morphology
bullVery low GSM
Conclusions
CAS and CEA are not competitive procedures but powerful treatment options tailored on different groups of patients
The gold standard is the experienced vascular team able to twist between endovascular and open surgical options in order to achieve the best treatment for the patient
Thank you for your attention
- Slide 1
- Slide 2
- Slide 3
- Slide 4
- Slide 5
- Slide 6
- Slide 7
- Slide 8
- Slide 9
- Slide 10
- Slide 11
- Slide 12
- Slide 13
- Slide 14
- Slide 15
- Slide 16
- Slide 17
- Slide 18
- Slide 19
- Slide 20
- Slide 21
- Slide 22
- Slide 23
- Slide 24
- Slide 25
- Slide 26
- Slide 27
- Slide 28
- Slide 29
- Slide 30
- Slide 31
- Slide 32
- Slide 33
- Slide 34
- Slide 35
- Slide 36
- Slide 37
- Slide 38
- Slide 39
- Slide 40
-
bullA valuable therapeutic option for stroke management over simple medical treatment since 1954 Eastcott first description
CEACEAASPIRINASPIRIN
Carotid endarterectomy (CEA)Carotid endarterectomy (CEA)
TrialTrialTrialTrial Mean Mean Follow-upFollow-upMean Mean Follow-upFollow-up
Rate of New Rate of New Neurologic EventsNeurologic Events
Rate of New Rate of New Neurologic EventsNeurologic Events
ACASACASACASACAS AsymptomaticN= 1662 27 years27 years27 years27 years 11111111 51515151
ACSTACSTACSTACST Asymptomatic 5 years5 years5 years5 years 1178117811781178 64646464
Significant 5 year absolute risk reduction of apr 5
Offered Up to 17 relative risk reduction of major cardiovascular events
CEA for symptomatic patientsCEA for symptomatic patients
CEA for asymptomatic patientsCEA for asymptomatic patients
Carotid endarterectomy (CEA)Carotid endarterectomy (CEA)
Carotid Artery Stenting (CAS)Carotid Artery Stenting (CAS)bullLess invasivebullLess traumaticbullLess time consuming bullPainlessbullAvoids neck incisionsbullAvoids nerve damagebullAvoids systemic complications related to anesthesia
Remained the gold standard for carotid Remained the gold standard for carotid artery disease for many years as an artery disease for many years as an
evidence based procedureevidence based procedure
RESULTS
Single center retrospective reports Initial experience with CAS
Prospective multicenter registries for CAS
CAS vs CEA Controlled trials
CAS vs CEA meta- analysis (Cochrane review)
Evidence for CAS
Controlled trials CAS vs CEA
meta- analysis (Cochrane review)
Ederle J et al Cochrane systematic review Stroke 200940(4)1373-80
Coward L et al Cochrane systematic review Stroke 2005 36905-11
Controlled trials comparing CAS with CEA
Ederle J et al Cochrane systematic review Stroke 2009 Apr40(4)1373-80
Slightly favored CEA
Death or stroke within 30 days of procedure
Criticism on EVA-3S and SPACE trials- weak points
bull inadequate sample size (type II statistical error)
bull different stent systems
bull different protocols in pre- and post- administration of antiplatelet drugs
bull not uniform use of EPDs
bull not similar patient groups (eg four times as many people with contralateral ICA occlusion in the CAS group in EVA-3S)
bull surprisingly better results of French surgeons (EVA-3S) in performing CEA comparing to NASCET and ECST (39 vs 65 and 71)
The results do not support a change in clinical practice away from recommending carotid endarterectomy as the treatment of choice for suitable carotid artery stenosis but support continued recruitment in the large ongoing trials
Trial Year FU CAS ips stroke CEA ips stroke P Article
SPACE 2008 2 years 95 885 NS Lancet Neurol 2008 7 893-902
EVA-3s 2008 4 years After the periprocedural period the risk of ipsilateral stroke was low and similar in both treatment groups
NS Lancet Neurol 2008 7 885-892
SAPPHIRE 2008 3 years 6 87 NS N Engl j Med 2008 358 1572-79
CAVATAS 2009 5 years 11middot3 8middot6 NS Lancet Neurol 20098(10)898-907
CREST 2011
Mid and Long term results (6m-5 years)
Coward LJ et al Cochrane review Stroke 200536905-911
Equal results between CEA and CAS
Cranial neuropathy
Stronly favored CAS
No significant difference in the major risks of treatment
Minor complication favorendovascular treatment
Conclusions
Insufficient evidence to support a widespread change in clinical practice
So which is the VERDICT
Current trials didnrsquot prove CAS inferiority
The initial question about gold standard is wrong
vsXBoth CAS CEAand
Play a role in stroke prevention in different patient groups
Defining patient groups that either CEA or CAS is beneficial
Vessel anatomy Plaque characteristics
The high risk patient
Defining patient groups that either CEA or CAS is beneficial
Vessel anatomyPlaque characteristics
The high risk patient
The influence of anatomy on treatment selection for carotid disease
1 Congenital anatomical variation (bovine arch aortic arch types I-III high or low carotid bifurcation aberrant vessels)
2 Alterations that occur with aging and hypertension (inflow and outflow tortuousity calcification thrombi)
3 Extension of disease (eg diffuse multisegmental disease involving the proximal CCA or distal ICA)
Vessel anatomy
Schneider PA et al Semin Vasc Surg 20216-225 2007
Vessel anatomy
Aortic arch type and orificial calcification
Vessel anatomy
Mobile thrombi Vessel anatomy
Vessel anatomyBovine carotid configuration
Proximal common carotid lesionsVessel anatomy
Tortuous CCA or ICA coil
Vessel anatomy
ldquoString signrdquo carotid morphology
Would you advance an EPD into such a vessel
Vessel anatomy
Defining patient groups that either CEA or CAS is beneficial
Vessel anatomyPlaque characteristics
The high risk patient
Plaque characteristics
Biasi et al ICAROS study Circulation 2004110756-62Fisher M et al Stroke 200536253ndash7Rothwell PM et al Stroke 200031615ndash21
bullGSMlt25 is related with a higher risk of neurologic complications after CASbulllow GSM is not a contraindication to CAS but rather a predictor of increased stroke riskbullLow GSM values are further related to future coronary events and higher rate of restenosis
Defining patient groups that either CEA or CAS is beneficial
Vessel anatomy Plaque characteristics
The high risk patient
24 30
60
96
12
3624
48
0
5
10
15
20
25
Death Stroke MI MAE
CEA (n=167)
Stent (n=167)
30 Days endpoint
P=068 P=100P=017
P=014
Theldquohigh riskrdquo patient
126
7260
192
72
120
24
60
0
5
10
15
20
25
Death Stroke MI MAE
CEA (n=167)Stent (n=167)
SAPPHIRE CAS vs CEA
1 year results
P=014
P=083P=017
P=010
CEA can be performed in high-risk patients with acceptable standard complication rates
Mozes G et al Semin Vasc Surg 20051861ndash 8
octogenarians
121121
30-day stroke and death rate30-day stroke and death rate
5353 1313
Agegt80yAgegt80y Age 70-79yAge 70-79y Age 60-69Age 60-69
Is CAS safe in this subgroup
The CREST trial lead-in phase
Material - Methodsbull 67 monthsbull 520 patientsbull mean age 76 range 56-85bull 364 male (70) 156 female (30)bull mean follow-up was 32 months (range 1 ndash 54 months)
Retrospective study
bull We conducted a retrospective review of CAS from 2003 to 2008bull RX Acculink - RX Accunet carotid system (Guidant Abott)
Material - Methods
bull Symptomatic (stroke (135) TIA Fugax) 515
bull Asymptomatic 485
Results within early follow-up (lt30 days)
bull Mortality (09)Stroke (11)TIA (13)Non fatal MI (13)
MAE 46
Results within early follow-up (lt30 days)
Predictors of adverse outcomes includedbullAge gt80bullsymptomatic patientsbullFemale genderbullpredilation prior to CPD bullplacement of multiple stentsbullContralateral occlusionbullUnfavorable anatomy
Late Follow-Up (gt30 days)
bull Mortality (173 )Stroke (07)Restenosis gt70 (23)
Mean follow-up was 32 months (range 1 ndash 60 months) 46 (88) patients lost of FU
Conclusion
bullCAS within experienced hands can be highly efficient and durable
Acculink Accunet system is safe and effective for CAS
ConclusionsCEA is the goal standard when
bull specific carotid anatomy
bullExtensive arch and carotid bif calcification
bullAccess related problems
bullFresh thrombus at ICA lesion
bullldquoString signrdquo morphology
bullVery low GSM
Conclusions
CAS and CEA are not competitive procedures but powerful treatment options tailored on different groups of patients
The gold standard is the experienced vascular team able to twist between endovascular and open surgical options in order to achieve the best treatment for the patient
Thank you for your attention
- Slide 1
- Slide 2
- Slide 3
- Slide 4
- Slide 5
- Slide 6
- Slide 7
- Slide 8
- Slide 9
- Slide 10
- Slide 11
- Slide 12
- Slide 13
- Slide 14
- Slide 15
- Slide 16
- Slide 17
- Slide 18
- Slide 19
- Slide 20
- Slide 21
- Slide 22
- Slide 23
- Slide 24
- Slide 25
- Slide 26
- Slide 27
- Slide 28
- Slide 29
- Slide 30
- Slide 31
- Slide 32
- Slide 33
- Slide 34
- Slide 35
- Slide 36
- Slide 37
- Slide 38
- Slide 39
- Slide 40
-
TrialTrialTrialTrial Mean Mean Follow-upFollow-upMean Mean Follow-upFollow-up
Rate of New Rate of New Neurologic EventsNeurologic Events
Rate of New Rate of New Neurologic EventsNeurologic Events
ACASACASACASACAS AsymptomaticN= 1662 27 years27 years27 years27 years 11111111 51515151
ACSTACSTACSTACST Asymptomatic 5 years5 years5 years5 years 1178117811781178 64646464
Significant 5 year absolute risk reduction of apr 5
Offered Up to 17 relative risk reduction of major cardiovascular events
CEA for symptomatic patientsCEA for symptomatic patients
CEA for asymptomatic patientsCEA for asymptomatic patients
Carotid endarterectomy (CEA)Carotid endarterectomy (CEA)
Carotid Artery Stenting (CAS)Carotid Artery Stenting (CAS)bullLess invasivebullLess traumaticbullLess time consuming bullPainlessbullAvoids neck incisionsbullAvoids nerve damagebullAvoids systemic complications related to anesthesia
Remained the gold standard for carotid Remained the gold standard for carotid artery disease for many years as an artery disease for many years as an
evidence based procedureevidence based procedure
RESULTS
Single center retrospective reports Initial experience with CAS
Prospective multicenter registries for CAS
CAS vs CEA Controlled trials
CAS vs CEA meta- analysis (Cochrane review)
Evidence for CAS
Controlled trials CAS vs CEA
meta- analysis (Cochrane review)
Ederle J et al Cochrane systematic review Stroke 200940(4)1373-80
Coward L et al Cochrane systematic review Stroke 2005 36905-11
Controlled trials comparing CAS with CEA
Ederle J et al Cochrane systematic review Stroke 2009 Apr40(4)1373-80
Slightly favored CEA
Death or stroke within 30 days of procedure
Criticism on EVA-3S and SPACE trials- weak points
bull inadequate sample size (type II statistical error)
bull different stent systems
bull different protocols in pre- and post- administration of antiplatelet drugs
bull not uniform use of EPDs
bull not similar patient groups (eg four times as many people with contralateral ICA occlusion in the CAS group in EVA-3S)
bull surprisingly better results of French surgeons (EVA-3S) in performing CEA comparing to NASCET and ECST (39 vs 65 and 71)
The results do not support a change in clinical practice away from recommending carotid endarterectomy as the treatment of choice for suitable carotid artery stenosis but support continued recruitment in the large ongoing trials
Trial Year FU CAS ips stroke CEA ips stroke P Article
SPACE 2008 2 years 95 885 NS Lancet Neurol 2008 7 893-902
EVA-3s 2008 4 years After the periprocedural period the risk of ipsilateral stroke was low and similar in both treatment groups
NS Lancet Neurol 2008 7 885-892
SAPPHIRE 2008 3 years 6 87 NS N Engl j Med 2008 358 1572-79
CAVATAS 2009 5 years 11middot3 8middot6 NS Lancet Neurol 20098(10)898-907
CREST 2011
Mid and Long term results (6m-5 years)
Coward LJ et al Cochrane review Stroke 200536905-911
Equal results between CEA and CAS
Cranial neuropathy
Stronly favored CAS
No significant difference in the major risks of treatment
Minor complication favorendovascular treatment
Conclusions
Insufficient evidence to support a widespread change in clinical practice
So which is the VERDICT
Current trials didnrsquot prove CAS inferiority
The initial question about gold standard is wrong
vsXBoth CAS CEAand
Play a role in stroke prevention in different patient groups
Defining patient groups that either CEA or CAS is beneficial
Vessel anatomy Plaque characteristics
The high risk patient
Defining patient groups that either CEA or CAS is beneficial
Vessel anatomyPlaque characteristics
The high risk patient
The influence of anatomy on treatment selection for carotid disease
1 Congenital anatomical variation (bovine arch aortic arch types I-III high or low carotid bifurcation aberrant vessels)
2 Alterations that occur with aging and hypertension (inflow and outflow tortuousity calcification thrombi)
3 Extension of disease (eg diffuse multisegmental disease involving the proximal CCA or distal ICA)
Vessel anatomy
Schneider PA et al Semin Vasc Surg 20216-225 2007
Vessel anatomy
Aortic arch type and orificial calcification
Vessel anatomy
Mobile thrombi Vessel anatomy
Vessel anatomyBovine carotid configuration
Proximal common carotid lesionsVessel anatomy
Tortuous CCA or ICA coil
Vessel anatomy
ldquoString signrdquo carotid morphology
Would you advance an EPD into such a vessel
Vessel anatomy
Defining patient groups that either CEA or CAS is beneficial
Vessel anatomyPlaque characteristics
The high risk patient
Plaque characteristics
Biasi et al ICAROS study Circulation 2004110756-62Fisher M et al Stroke 200536253ndash7Rothwell PM et al Stroke 200031615ndash21
bullGSMlt25 is related with a higher risk of neurologic complications after CASbulllow GSM is not a contraindication to CAS but rather a predictor of increased stroke riskbullLow GSM values are further related to future coronary events and higher rate of restenosis
Defining patient groups that either CEA or CAS is beneficial
Vessel anatomy Plaque characteristics
The high risk patient
24 30
60
96
12
3624
48
0
5
10
15
20
25
Death Stroke MI MAE
CEA (n=167)
Stent (n=167)
30 Days endpoint
P=068 P=100P=017
P=014
Theldquohigh riskrdquo patient
126
7260
192
72
120
24
60
0
5
10
15
20
25
Death Stroke MI MAE
CEA (n=167)Stent (n=167)
SAPPHIRE CAS vs CEA
1 year results
P=014
P=083P=017
P=010
CEA can be performed in high-risk patients with acceptable standard complication rates
Mozes G et al Semin Vasc Surg 20051861ndash 8
octogenarians
121121
30-day stroke and death rate30-day stroke and death rate
5353 1313
Agegt80yAgegt80y Age 70-79yAge 70-79y Age 60-69Age 60-69
Is CAS safe in this subgroup
The CREST trial lead-in phase
Material - Methodsbull 67 monthsbull 520 patientsbull mean age 76 range 56-85bull 364 male (70) 156 female (30)bull mean follow-up was 32 months (range 1 ndash 54 months)
Retrospective study
bull We conducted a retrospective review of CAS from 2003 to 2008bull RX Acculink - RX Accunet carotid system (Guidant Abott)
Material - Methods
bull Symptomatic (stroke (135) TIA Fugax) 515
bull Asymptomatic 485
Results within early follow-up (lt30 days)
bull Mortality (09)Stroke (11)TIA (13)Non fatal MI (13)
MAE 46
Results within early follow-up (lt30 days)
Predictors of adverse outcomes includedbullAge gt80bullsymptomatic patientsbullFemale genderbullpredilation prior to CPD bullplacement of multiple stentsbullContralateral occlusionbullUnfavorable anatomy
Late Follow-Up (gt30 days)
bull Mortality (173 )Stroke (07)Restenosis gt70 (23)
Mean follow-up was 32 months (range 1 ndash 60 months) 46 (88) patients lost of FU
Conclusion
bullCAS within experienced hands can be highly efficient and durable
Acculink Accunet system is safe and effective for CAS
ConclusionsCEA is the goal standard when
bull specific carotid anatomy
bullExtensive arch and carotid bif calcification
bullAccess related problems
bullFresh thrombus at ICA lesion
bullldquoString signrdquo morphology
bullVery low GSM
Conclusions
CAS and CEA are not competitive procedures but powerful treatment options tailored on different groups of patients
The gold standard is the experienced vascular team able to twist between endovascular and open surgical options in order to achieve the best treatment for the patient
Thank you for your attention
- Slide 1
- Slide 2
- Slide 3
- Slide 4
- Slide 5
- Slide 6
- Slide 7
- Slide 8
- Slide 9
- Slide 10
- Slide 11
- Slide 12
- Slide 13
- Slide 14
- Slide 15
- Slide 16
- Slide 17
- Slide 18
- Slide 19
- Slide 20
- Slide 21
- Slide 22
- Slide 23
- Slide 24
- Slide 25
- Slide 26
- Slide 27
- Slide 28
- Slide 29
- Slide 30
- Slide 31
- Slide 32
- Slide 33
- Slide 34
- Slide 35
- Slide 36
- Slide 37
- Slide 38
- Slide 39
- Slide 40
-
Carotid endarterectomy (CEA)Carotid endarterectomy (CEA)
Carotid Artery Stenting (CAS)Carotid Artery Stenting (CAS)bullLess invasivebullLess traumaticbullLess time consuming bullPainlessbullAvoids neck incisionsbullAvoids nerve damagebullAvoids systemic complications related to anesthesia
Remained the gold standard for carotid Remained the gold standard for carotid artery disease for many years as an artery disease for many years as an
evidence based procedureevidence based procedure
RESULTS
Single center retrospective reports Initial experience with CAS
Prospective multicenter registries for CAS
CAS vs CEA Controlled trials
CAS vs CEA meta- analysis (Cochrane review)
Evidence for CAS
Controlled trials CAS vs CEA
meta- analysis (Cochrane review)
Ederle J et al Cochrane systematic review Stroke 200940(4)1373-80
Coward L et al Cochrane systematic review Stroke 2005 36905-11
Controlled trials comparing CAS with CEA
Ederle J et al Cochrane systematic review Stroke 2009 Apr40(4)1373-80
Slightly favored CEA
Death or stroke within 30 days of procedure
Criticism on EVA-3S and SPACE trials- weak points
bull inadequate sample size (type II statistical error)
bull different stent systems
bull different protocols in pre- and post- administration of antiplatelet drugs
bull not uniform use of EPDs
bull not similar patient groups (eg four times as many people with contralateral ICA occlusion in the CAS group in EVA-3S)
bull surprisingly better results of French surgeons (EVA-3S) in performing CEA comparing to NASCET and ECST (39 vs 65 and 71)
The results do not support a change in clinical practice away from recommending carotid endarterectomy as the treatment of choice for suitable carotid artery stenosis but support continued recruitment in the large ongoing trials
Trial Year FU CAS ips stroke CEA ips stroke P Article
SPACE 2008 2 years 95 885 NS Lancet Neurol 2008 7 893-902
EVA-3s 2008 4 years After the periprocedural period the risk of ipsilateral stroke was low and similar in both treatment groups
NS Lancet Neurol 2008 7 885-892
SAPPHIRE 2008 3 years 6 87 NS N Engl j Med 2008 358 1572-79
CAVATAS 2009 5 years 11middot3 8middot6 NS Lancet Neurol 20098(10)898-907
CREST 2011
Mid and Long term results (6m-5 years)
Coward LJ et al Cochrane review Stroke 200536905-911
Equal results between CEA and CAS
Cranial neuropathy
Stronly favored CAS
No significant difference in the major risks of treatment
Minor complication favorendovascular treatment
Conclusions
Insufficient evidence to support a widespread change in clinical practice
So which is the VERDICT
Current trials didnrsquot prove CAS inferiority
The initial question about gold standard is wrong
vsXBoth CAS CEAand
Play a role in stroke prevention in different patient groups
Defining patient groups that either CEA or CAS is beneficial
Vessel anatomy Plaque characteristics
The high risk patient
Defining patient groups that either CEA or CAS is beneficial
Vessel anatomyPlaque characteristics
The high risk patient
The influence of anatomy on treatment selection for carotid disease
1 Congenital anatomical variation (bovine arch aortic arch types I-III high or low carotid bifurcation aberrant vessels)
2 Alterations that occur with aging and hypertension (inflow and outflow tortuousity calcification thrombi)
3 Extension of disease (eg diffuse multisegmental disease involving the proximal CCA or distal ICA)
Vessel anatomy
Schneider PA et al Semin Vasc Surg 20216-225 2007
Vessel anatomy
Aortic arch type and orificial calcification
Vessel anatomy
Mobile thrombi Vessel anatomy
Vessel anatomyBovine carotid configuration
Proximal common carotid lesionsVessel anatomy
Tortuous CCA or ICA coil
Vessel anatomy
ldquoString signrdquo carotid morphology
Would you advance an EPD into such a vessel
Vessel anatomy
Defining patient groups that either CEA or CAS is beneficial
Vessel anatomyPlaque characteristics
The high risk patient
Plaque characteristics
Biasi et al ICAROS study Circulation 2004110756-62Fisher M et al Stroke 200536253ndash7Rothwell PM et al Stroke 200031615ndash21
bullGSMlt25 is related with a higher risk of neurologic complications after CASbulllow GSM is not a contraindication to CAS but rather a predictor of increased stroke riskbullLow GSM values are further related to future coronary events and higher rate of restenosis
Defining patient groups that either CEA or CAS is beneficial
Vessel anatomy Plaque characteristics
The high risk patient
24 30
60
96
12
3624
48
0
5
10
15
20
25
Death Stroke MI MAE
CEA (n=167)
Stent (n=167)
30 Days endpoint
P=068 P=100P=017
P=014
Theldquohigh riskrdquo patient
126
7260
192
72
120
24
60
0
5
10
15
20
25
Death Stroke MI MAE
CEA (n=167)Stent (n=167)
SAPPHIRE CAS vs CEA
1 year results
P=014
P=083P=017
P=010
CEA can be performed in high-risk patients with acceptable standard complication rates
Mozes G et al Semin Vasc Surg 20051861ndash 8
octogenarians
121121
30-day stroke and death rate30-day stroke and death rate
5353 1313
Agegt80yAgegt80y Age 70-79yAge 70-79y Age 60-69Age 60-69
Is CAS safe in this subgroup
The CREST trial lead-in phase
Material - Methodsbull 67 monthsbull 520 patientsbull mean age 76 range 56-85bull 364 male (70) 156 female (30)bull mean follow-up was 32 months (range 1 ndash 54 months)
Retrospective study
bull We conducted a retrospective review of CAS from 2003 to 2008bull RX Acculink - RX Accunet carotid system (Guidant Abott)
Material - Methods
bull Symptomatic (stroke (135) TIA Fugax) 515
bull Asymptomatic 485
Results within early follow-up (lt30 days)
bull Mortality (09)Stroke (11)TIA (13)Non fatal MI (13)
MAE 46
Results within early follow-up (lt30 days)
Predictors of adverse outcomes includedbullAge gt80bullsymptomatic patientsbullFemale genderbullpredilation prior to CPD bullplacement of multiple stentsbullContralateral occlusionbullUnfavorable anatomy
Late Follow-Up (gt30 days)
bull Mortality (173 )Stroke (07)Restenosis gt70 (23)
Mean follow-up was 32 months (range 1 ndash 60 months) 46 (88) patients lost of FU
Conclusion
bullCAS within experienced hands can be highly efficient and durable
Acculink Accunet system is safe and effective for CAS
ConclusionsCEA is the goal standard when
bull specific carotid anatomy
bullExtensive arch and carotid bif calcification
bullAccess related problems
bullFresh thrombus at ICA lesion
bullldquoString signrdquo morphology
bullVery low GSM
Conclusions
CAS and CEA are not competitive procedures but powerful treatment options tailored on different groups of patients
The gold standard is the experienced vascular team able to twist between endovascular and open surgical options in order to achieve the best treatment for the patient
Thank you for your attention
- Slide 1
- Slide 2
- Slide 3
- Slide 4
- Slide 5
- Slide 6
- Slide 7
- Slide 8
- Slide 9
- Slide 10
- Slide 11
- Slide 12
- Slide 13
- Slide 14
- Slide 15
- Slide 16
- Slide 17
- Slide 18
- Slide 19
- Slide 20
- Slide 21
- Slide 22
- Slide 23
- Slide 24
- Slide 25
- Slide 26
- Slide 27
- Slide 28
- Slide 29
- Slide 30
- Slide 31
- Slide 32
- Slide 33
- Slide 34
- Slide 35
- Slide 36
- Slide 37
- Slide 38
- Slide 39
- Slide 40
-
Single center retrospective reports Initial experience with CAS
Prospective multicenter registries for CAS
CAS vs CEA Controlled trials
CAS vs CEA meta- analysis (Cochrane review)
Evidence for CAS
Controlled trials CAS vs CEA
meta- analysis (Cochrane review)
Ederle J et al Cochrane systematic review Stroke 200940(4)1373-80
Coward L et al Cochrane systematic review Stroke 2005 36905-11
Controlled trials comparing CAS with CEA
Ederle J et al Cochrane systematic review Stroke 2009 Apr40(4)1373-80
Slightly favored CEA
Death or stroke within 30 days of procedure
Criticism on EVA-3S and SPACE trials- weak points
bull inadequate sample size (type II statistical error)
bull different stent systems
bull different protocols in pre- and post- administration of antiplatelet drugs
bull not uniform use of EPDs
bull not similar patient groups (eg four times as many people with contralateral ICA occlusion in the CAS group in EVA-3S)
bull surprisingly better results of French surgeons (EVA-3S) in performing CEA comparing to NASCET and ECST (39 vs 65 and 71)
The results do not support a change in clinical practice away from recommending carotid endarterectomy as the treatment of choice for suitable carotid artery stenosis but support continued recruitment in the large ongoing trials
Trial Year FU CAS ips stroke CEA ips stroke P Article
SPACE 2008 2 years 95 885 NS Lancet Neurol 2008 7 893-902
EVA-3s 2008 4 years After the periprocedural period the risk of ipsilateral stroke was low and similar in both treatment groups
NS Lancet Neurol 2008 7 885-892
SAPPHIRE 2008 3 years 6 87 NS N Engl j Med 2008 358 1572-79
CAVATAS 2009 5 years 11middot3 8middot6 NS Lancet Neurol 20098(10)898-907
CREST 2011
Mid and Long term results (6m-5 years)
Coward LJ et al Cochrane review Stroke 200536905-911
Equal results between CEA and CAS
Cranial neuropathy
Stronly favored CAS
No significant difference in the major risks of treatment
Minor complication favorendovascular treatment
Conclusions
Insufficient evidence to support a widespread change in clinical practice
So which is the VERDICT
Current trials didnrsquot prove CAS inferiority
The initial question about gold standard is wrong
vsXBoth CAS CEAand
Play a role in stroke prevention in different patient groups
Defining patient groups that either CEA or CAS is beneficial
Vessel anatomy Plaque characteristics
The high risk patient
Defining patient groups that either CEA or CAS is beneficial
Vessel anatomyPlaque characteristics
The high risk patient
The influence of anatomy on treatment selection for carotid disease
1 Congenital anatomical variation (bovine arch aortic arch types I-III high or low carotid bifurcation aberrant vessels)
2 Alterations that occur with aging and hypertension (inflow and outflow tortuousity calcification thrombi)
3 Extension of disease (eg diffuse multisegmental disease involving the proximal CCA or distal ICA)
Vessel anatomy
Schneider PA et al Semin Vasc Surg 20216-225 2007
Vessel anatomy
Aortic arch type and orificial calcification
Vessel anatomy
Mobile thrombi Vessel anatomy
Vessel anatomyBovine carotid configuration
Proximal common carotid lesionsVessel anatomy
Tortuous CCA or ICA coil
Vessel anatomy
ldquoString signrdquo carotid morphology
Would you advance an EPD into such a vessel
Vessel anatomy
Defining patient groups that either CEA or CAS is beneficial
Vessel anatomyPlaque characteristics
The high risk patient
Plaque characteristics
Biasi et al ICAROS study Circulation 2004110756-62Fisher M et al Stroke 200536253ndash7Rothwell PM et al Stroke 200031615ndash21
bullGSMlt25 is related with a higher risk of neurologic complications after CASbulllow GSM is not a contraindication to CAS but rather a predictor of increased stroke riskbullLow GSM values are further related to future coronary events and higher rate of restenosis
Defining patient groups that either CEA or CAS is beneficial
Vessel anatomy Plaque characteristics
The high risk patient
24 30
60
96
12
3624
48
0
5
10
15
20
25
Death Stroke MI MAE
CEA (n=167)
Stent (n=167)
30 Days endpoint
P=068 P=100P=017
P=014
Theldquohigh riskrdquo patient
126
7260
192
72
120
24
60
0
5
10
15
20
25
Death Stroke MI MAE
CEA (n=167)Stent (n=167)
SAPPHIRE CAS vs CEA
1 year results
P=014
P=083P=017
P=010
CEA can be performed in high-risk patients with acceptable standard complication rates
Mozes G et al Semin Vasc Surg 20051861ndash 8
octogenarians
121121
30-day stroke and death rate30-day stroke and death rate
5353 1313
Agegt80yAgegt80y Age 70-79yAge 70-79y Age 60-69Age 60-69
Is CAS safe in this subgroup
The CREST trial lead-in phase
Material - Methodsbull 67 monthsbull 520 patientsbull mean age 76 range 56-85bull 364 male (70) 156 female (30)bull mean follow-up was 32 months (range 1 ndash 54 months)
Retrospective study
bull We conducted a retrospective review of CAS from 2003 to 2008bull RX Acculink - RX Accunet carotid system (Guidant Abott)
Material - Methods
bull Symptomatic (stroke (135) TIA Fugax) 515
bull Asymptomatic 485
Results within early follow-up (lt30 days)
bull Mortality (09)Stroke (11)TIA (13)Non fatal MI (13)
MAE 46
Results within early follow-up (lt30 days)
Predictors of adverse outcomes includedbullAge gt80bullsymptomatic patientsbullFemale genderbullpredilation prior to CPD bullplacement of multiple stentsbullContralateral occlusionbullUnfavorable anatomy
Late Follow-Up (gt30 days)
bull Mortality (173 )Stroke (07)Restenosis gt70 (23)
Mean follow-up was 32 months (range 1 ndash 60 months) 46 (88) patients lost of FU
Conclusion
bullCAS within experienced hands can be highly efficient and durable
Acculink Accunet system is safe and effective for CAS
ConclusionsCEA is the goal standard when
bull specific carotid anatomy
bullExtensive arch and carotid bif calcification
bullAccess related problems
bullFresh thrombus at ICA lesion
bullldquoString signrdquo morphology
bullVery low GSM
Conclusions
CAS and CEA are not competitive procedures but powerful treatment options tailored on different groups of patients
The gold standard is the experienced vascular team able to twist between endovascular and open surgical options in order to achieve the best treatment for the patient
Thank you for your attention
- Slide 1
- Slide 2
- Slide 3
- Slide 4
- Slide 5
- Slide 6
- Slide 7
- Slide 8
- Slide 9
- Slide 10
- Slide 11
- Slide 12
- Slide 13
- Slide 14
- Slide 15
- Slide 16
- Slide 17
- Slide 18
- Slide 19
- Slide 20
- Slide 21
- Slide 22
- Slide 23
- Slide 24
- Slide 25
- Slide 26
- Slide 27
- Slide 28
- Slide 29
- Slide 30
- Slide 31
- Slide 32
- Slide 33
- Slide 34
- Slide 35
- Slide 36
- Slide 37
- Slide 38
- Slide 39
- Slide 40
-
Controlled trials CAS vs CEA
meta- analysis (Cochrane review)
Ederle J et al Cochrane systematic review Stroke 200940(4)1373-80
Coward L et al Cochrane systematic review Stroke 2005 36905-11
Controlled trials comparing CAS with CEA
Ederle J et al Cochrane systematic review Stroke 2009 Apr40(4)1373-80
Slightly favored CEA
Death or stroke within 30 days of procedure
Criticism on EVA-3S and SPACE trials- weak points
bull inadequate sample size (type II statistical error)
bull different stent systems
bull different protocols in pre- and post- administration of antiplatelet drugs
bull not uniform use of EPDs
bull not similar patient groups (eg four times as many people with contralateral ICA occlusion in the CAS group in EVA-3S)
bull surprisingly better results of French surgeons (EVA-3S) in performing CEA comparing to NASCET and ECST (39 vs 65 and 71)
The results do not support a change in clinical practice away from recommending carotid endarterectomy as the treatment of choice for suitable carotid artery stenosis but support continued recruitment in the large ongoing trials
Trial Year FU CAS ips stroke CEA ips stroke P Article
SPACE 2008 2 years 95 885 NS Lancet Neurol 2008 7 893-902
EVA-3s 2008 4 years After the periprocedural period the risk of ipsilateral stroke was low and similar in both treatment groups
NS Lancet Neurol 2008 7 885-892
SAPPHIRE 2008 3 years 6 87 NS N Engl j Med 2008 358 1572-79
CAVATAS 2009 5 years 11middot3 8middot6 NS Lancet Neurol 20098(10)898-907
CREST 2011
Mid and Long term results (6m-5 years)
Coward LJ et al Cochrane review Stroke 200536905-911
Equal results between CEA and CAS
Cranial neuropathy
Stronly favored CAS
No significant difference in the major risks of treatment
Minor complication favorendovascular treatment
Conclusions
Insufficient evidence to support a widespread change in clinical practice
So which is the VERDICT
Current trials didnrsquot prove CAS inferiority
The initial question about gold standard is wrong
vsXBoth CAS CEAand
Play a role in stroke prevention in different patient groups
Defining patient groups that either CEA or CAS is beneficial
Vessel anatomy Plaque characteristics
The high risk patient
Defining patient groups that either CEA or CAS is beneficial
Vessel anatomyPlaque characteristics
The high risk patient
The influence of anatomy on treatment selection for carotid disease
1 Congenital anatomical variation (bovine arch aortic arch types I-III high or low carotid bifurcation aberrant vessels)
2 Alterations that occur with aging and hypertension (inflow and outflow tortuousity calcification thrombi)
3 Extension of disease (eg diffuse multisegmental disease involving the proximal CCA or distal ICA)
Vessel anatomy
Schneider PA et al Semin Vasc Surg 20216-225 2007
Vessel anatomy
Aortic arch type and orificial calcification
Vessel anatomy
Mobile thrombi Vessel anatomy
Vessel anatomyBovine carotid configuration
Proximal common carotid lesionsVessel anatomy
Tortuous CCA or ICA coil
Vessel anatomy
ldquoString signrdquo carotid morphology
Would you advance an EPD into such a vessel
Vessel anatomy
Defining patient groups that either CEA or CAS is beneficial
Vessel anatomyPlaque characteristics
The high risk patient
Plaque characteristics
Biasi et al ICAROS study Circulation 2004110756-62Fisher M et al Stroke 200536253ndash7Rothwell PM et al Stroke 200031615ndash21
bullGSMlt25 is related with a higher risk of neurologic complications after CASbulllow GSM is not a contraindication to CAS but rather a predictor of increased stroke riskbullLow GSM values are further related to future coronary events and higher rate of restenosis
Defining patient groups that either CEA or CAS is beneficial
Vessel anatomy Plaque characteristics
The high risk patient
24 30
60
96
12
3624
48
0
5
10
15
20
25
Death Stroke MI MAE
CEA (n=167)
Stent (n=167)
30 Days endpoint
P=068 P=100P=017
P=014
Theldquohigh riskrdquo patient
126
7260
192
72
120
24
60
0
5
10
15
20
25
Death Stroke MI MAE
CEA (n=167)Stent (n=167)
SAPPHIRE CAS vs CEA
1 year results
P=014
P=083P=017
P=010
CEA can be performed in high-risk patients with acceptable standard complication rates
Mozes G et al Semin Vasc Surg 20051861ndash 8
octogenarians
121121
30-day stroke and death rate30-day stroke and death rate
5353 1313
Agegt80yAgegt80y Age 70-79yAge 70-79y Age 60-69Age 60-69
Is CAS safe in this subgroup
The CREST trial lead-in phase
Material - Methodsbull 67 monthsbull 520 patientsbull mean age 76 range 56-85bull 364 male (70) 156 female (30)bull mean follow-up was 32 months (range 1 ndash 54 months)
Retrospective study
bull We conducted a retrospective review of CAS from 2003 to 2008bull RX Acculink - RX Accunet carotid system (Guidant Abott)
Material - Methods
bull Symptomatic (stroke (135) TIA Fugax) 515
bull Asymptomatic 485
Results within early follow-up (lt30 days)
bull Mortality (09)Stroke (11)TIA (13)Non fatal MI (13)
MAE 46
Results within early follow-up (lt30 days)
Predictors of adverse outcomes includedbullAge gt80bullsymptomatic patientsbullFemale genderbullpredilation prior to CPD bullplacement of multiple stentsbullContralateral occlusionbullUnfavorable anatomy
Late Follow-Up (gt30 days)
bull Mortality (173 )Stroke (07)Restenosis gt70 (23)
Mean follow-up was 32 months (range 1 ndash 60 months) 46 (88) patients lost of FU
Conclusion
bullCAS within experienced hands can be highly efficient and durable
Acculink Accunet system is safe and effective for CAS
ConclusionsCEA is the goal standard when
bull specific carotid anatomy
bullExtensive arch and carotid bif calcification
bullAccess related problems
bullFresh thrombus at ICA lesion
bullldquoString signrdquo morphology
bullVery low GSM
Conclusions
CAS and CEA are not competitive procedures but powerful treatment options tailored on different groups of patients
The gold standard is the experienced vascular team able to twist between endovascular and open surgical options in order to achieve the best treatment for the patient
Thank you for your attention
- Slide 1
- Slide 2
- Slide 3
- Slide 4
- Slide 5
- Slide 6
- Slide 7
- Slide 8
- Slide 9
- Slide 10
- Slide 11
- Slide 12
- Slide 13
- Slide 14
- Slide 15
- Slide 16
- Slide 17
- Slide 18
- Slide 19
- Slide 20
- Slide 21
- Slide 22
- Slide 23
- Slide 24
- Slide 25
- Slide 26
- Slide 27
- Slide 28
- Slide 29
- Slide 30
- Slide 31
- Slide 32
- Slide 33
- Slide 34
- Slide 35
- Slide 36
- Slide 37
- Slide 38
- Slide 39
- Slide 40
-
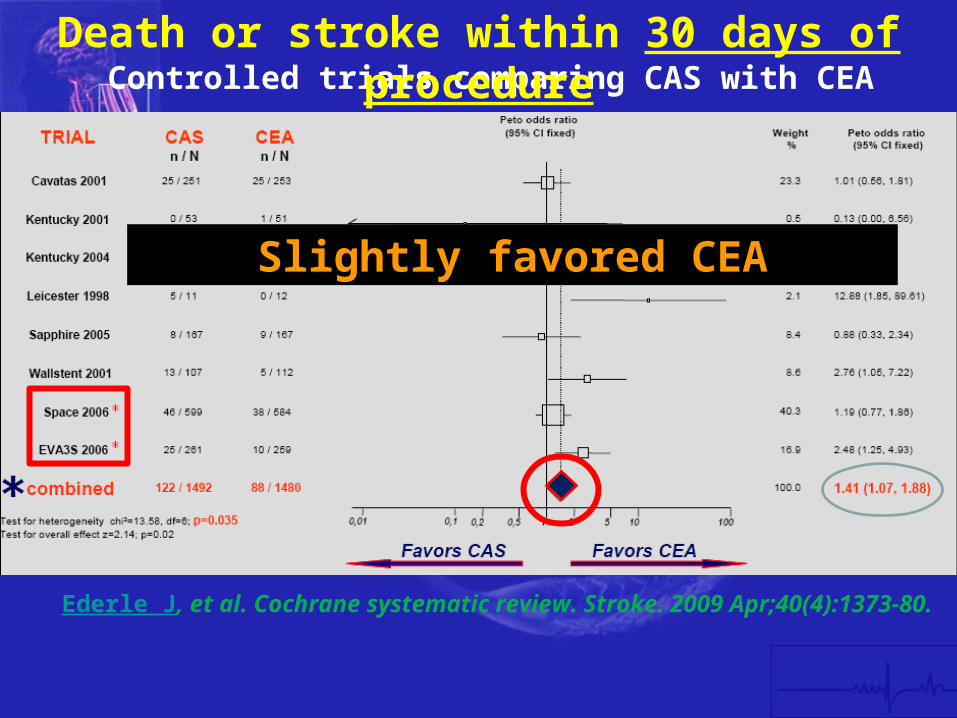
Controlled trials comparing CAS with CEA
Ederle J et al Cochrane systematic review Stroke 2009 Apr40(4)1373-80
Slightly favored CEA
Death or stroke within 30 days of procedure
Criticism on EVA-3S and SPACE trials- weak points
bull inadequate sample size (type II statistical error)
bull different stent systems
bull different protocols in pre- and post- administration of antiplatelet drugs
bull not uniform use of EPDs
bull not similar patient groups (eg four times as many people with contralateral ICA occlusion in the CAS group in EVA-3S)
bull surprisingly better results of French surgeons (EVA-3S) in performing CEA comparing to NASCET and ECST (39 vs 65 and 71)
The results do not support a change in clinical practice away from recommending carotid endarterectomy as the treatment of choice for suitable carotid artery stenosis but support continued recruitment in the large ongoing trials
Trial Year FU CAS ips stroke CEA ips stroke P Article
SPACE 2008 2 years 95 885 NS Lancet Neurol 2008 7 893-902
EVA-3s 2008 4 years After the periprocedural period the risk of ipsilateral stroke was low and similar in both treatment groups
NS Lancet Neurol 2008 7 885-892
SAPPHIRE 2008 3 years 6 87 NS N Engl j Med 2008 358 1572-79
CAVATAS 2009 5 years 11middot3 8middot6 NS Lancet Neurol 20098(10)898-907
CREST 2011
Mid and Long term results (6m-5 years)
Coward LJ et al Cochrane review Stroke 200536905-911
Equal results between CEA and CAS
Cranial neuropathy
Stronly favored CAS
No significant difference in the major risks of treatment
Minor complication favorendovascular treatment
Conclusions
Insufficient evidence to support a widespread change in clinical practice
So which is the VERDICT
Current trials didnrsquot prove CAS inferiority
The initial question about gold standard is wrong
vsXBoth CAS CEAand
Play a role in stroke prevention in different patient groups
Defining patient groups that either CEA or CAS is beneficial
Vessel anatomy Plaque characteristics
The high risk patient
Defining patient groups that either CEA or CAS is beneficial
Vessel anatomyPlaque characteristics
The high risk patient
The influence of anatomy on treatment selection for carotid disease
1 Congenital anatomical variation (bovine arch aortic arch types I-III high or low carotid bifurcation aberrant vessels)
2 Alterations that occur with aging and hypertension (inflow and outflow tortuousity calcification thrombi)
3 Extension of disease (eg diffuse multisegmental disease involving the proximal CCA or distal ICA)
Vessel anatomy
Schneider PA et al Semin Vasc Surg 20216-225 2007
Vessel anatomy
Aortic arch type and orificial calcification
Vessel anatomy
Mobile thrombi Vessel anatomy
Vessel anatomyBovine carotid configuration
Proximal common carotid lesionsVessel anatomy
Tortuous CCA or ICA coil
Vessel anatomy
ldquoString signrdquo carotid morphology
Would you advance an EPD into such a vessel
Vessel anatomy
Defining patient groups that either CEA or CAS is beneficial
Vessel anatomyPlaque characteristics
The high risk patient
Plaque characteristics
Biasi et al ICAROS study Circulation 2004110756-62Fisher M et al Stroke 200536253ndash7Rothwell PM et al Stroke 200031615ndash21
bullGSMlt25 is related with a higher risk of neurologic complications after CASbulllow GSM is not a contraindication to CAS but rather a predictor of increased stroke riskbullLow GSM values are further related to future coronary events and higher rate of restenosis
Defining patient groups that either CEA or CAS is beneficial
Vessel anatomy Plaque characteristics
The high risk patient
24 30
60
96
12
3624
48
0
5
10
15
20
25
Death Stroke MI MAE
CEA (n=167)
Stent (n=167)
30 Days endpoint
P=068 P=100P=017
P=014
Theldquohigh riskrdquo patient
126
7260
192
72
120
24
60
0
5
10
15
20
25
Death Stroke MI MAE
CEA (n=167)Stent (n=167)
SAPPHIRE CAS vs CEA
1 year results
P=014
P=083P=017
P=010
CEA can be performed in high-risk patients with acceptable standard complication rates
Mozes G et al Semin Vasc Surg 20051861ndash 8
octogenarians
121121
30-day stroke and death rate30-day stroke and death rate
5353 1313
Agegt80yAgegt80y Age 70-79yAge 70-79y Age 60-69Age 60-69
Is CAS safe in this subgroup
The CREST trial lead-in phase
Material - Methodsbull 67 monthsbull 520 patientsbull mean age 76 range 56-85bull 364 male (70) 156 female (30)bull mean follow-up was 32 months (range 1 ndash 54 months)
Retrospective study
bull We conducted a retrospective review of CAS from 2003 to 2008bull RX Acculink - RX Accunet carotid system (Guidant Abott)
Material - Methods
bull Symptomatic (stroke (135) TIA Fugax) 515
bull Asymptomatic 485
Results within early follow-up (lt30 days)
bull Mortality (09)Stroke (11)TIA (13)Non fatal MI (13)
MAE 46
Results within early follow-up (lt30 days)
Predictors of adverse outcomes includedbullAge gt80bullsymptomatic patientsbullFemale genderbullpredilation prior to CPD bullplacement of multiple stentsbullContralateral occlusionbullUnfavorable anatomy
Late Follow-Up (gt30 days)
bull Mortality (173 )Stroke (07)Restenosis gt70 (23)
Mean follow-up was 32 months (range 1 ndash 60 months) 46 (88) patients lost of FU
Conclusion
bullCAS within experienced hands can be highly efficient and durable
Acculink Accunet system is safe and effective for CAS
ConclusionsCEA is the goal standard when
bull specific carotid anatomy
bullExtensive arch and carotid bif calcification
bullAccess related problems
bullFresh thrombus at ICA lesion
bullldquoString signrdquo morphology
bullVery low GSM
Conclusions
CAS and CEA are not competitive procedures but powerful treatment options tailored on different groups of patients
The gold standard is the experienced vascular team able to twist between endovascular and open surgical options in order to achieve the best treatment for the patient
Thank you for your attention
- Slide 1
- Slide 2
- Slide 3
- Slide 4
- Slide 5
- Slide 6
- Slide 7
- Slide 8
- Slide 9
- Slide 10
- Slide 11
- Slide 12
- Slide 13
- Slide 14
- Slide 15
- Slide 16
- Slide 17
- Slide 18
- Slide 19
- Slide 20
- Slide 21
- Slide 22
- Slide 23
- Slide 24
- Slide 25
- Slide 26
- Slide 27
- Slide 28
- Slide 29
- Slide 30
- Slide 31
- Slide 32
- Slide 33
- Slide 34
- Slide 35
- Slide 36
- Slide 37
- Slide 38
- Slide 39
- Slide 40
-
Criticism on EVA-3S and SPACE trials- weak points
bull inadequate sample size (type II statistical error)
bull different stent systems
bull different protocols in pre- and post- administration of antiplatelet drugs
bull not uniform use of EPDs
bull not similar patient groups (eg four times as many people with contralateral ICA occlusion in the CAS group in EVA-3S)
bull surprisingly better results of French surgeons (EVA-3S) in performing CEA comparing to NASCET and ECST (39 vs 65 and 71)
The results do not support a change in clinical practice away from recommending carotid endarterectomy as the treatment of choice for suitable carotid artery stenosis but support continued recruitment in the large ongoing trials
Trial Year FU CAS ips stroke CEA ips stroke P Article
SPACE 2008 2 years 95 885 NS Lancet Neurol 2008 7 893-902
EVA-3s 2008 4 years After the periprocedural period the risk of ipsilateral stroke was low and similar in both treatment groups
NS Lancet Neurol 2008 7 885-892
SAPPHIRE 2008 3 years 6 87 NS N Engl j Med 2008 358 1572-79
CAVATAS 2009 5 years 11middot3 8middot6 NS Lancet Neurol 20098(10)898-907
CREST 2011
Mid and Long term results (6m-5 years)
Coward LJ et al Cochrane review Stroke 200536905-911
Equal results between CEA and CAS
Cranial neuropathy
Stronly favored CAS
No significant difference in the major risks of treatment
Minor complication favorendovascular treatment
Conclusions
Insufficient evidence to support a widespread change in clinical practice
So which is the VERDICT
Current trials didnrsquot prove CAS inferiority
The initial question about gold standard is wrong
vsXBoth CAS CEAand
Play a role in stroke prevention in different patient groups
Defining patient groups that either CEA or CAS is beneficial
Vessel anatomy Plaque characteristics
The high risk patient
Defining patient groups that either CEA or CAS is beneficial
Vessel anatomyPlaque characteristics
The high risk patient
The influence of anatomy on treatment selection for carotid disease
1 Congenital anatomical variation (bovine arch aortic arch types I-III high or low carotid bifurcation aberrant vessels)
2 Alterations that occur with aging and hypertension (inflow and outflow tortuousity calcification thrombi)
3 Extension of disease (eg diffuse multisegmental disease involving the proximal CCA or distal ICA)
Vessel anatomy
Schneider PA et al Semin Vasc Surg 20216-225 2007
Vessel anatomy
Aortic arch type and orificial calcification
Vessel anatomy
Mobile thrombi Vessel anatomy
Vessel anatomyBovine carotid configuration
Proximal common carotid lesionsVessel anatomy
Tortuous CCA or ICA coil
Vessel anatomy
ldquoString signrdquo carotid morphology
Would you advance an EPD into such a vessel
Vessel anatomy
Defining patient groups that either CEA or CAS is beneficial
Vessel anatomyPlaque characteristics
The high risk patient
Plaque characteristics
Biasi et al ICAROS study Circulation 2004110756-62Fisher M et al Stroke 200536253ndash7Rothwell PM et al Stroke 200031615ndash21
bullGSMlt25 is related with a higher risk of neurologic complications after CASbulllow GSM is not a contraindication to CAS but rather a predictor of increased stroke riskbullLow GSM values are further related to future coronary events and higher rate of restenosis
Defining patient groups that either CEA or CAS is beneficial
Vessel anatomy Plaque characteristics
The high risk patient
24 30
60
96
12
3624
48
0
5
10
15
20
25
Death Stroke MI MAE
CEA (n=167)
Stent (n=167)
30 Days endpoint
P=068 P=100P=017
P=014
Theldquohigh riskrdquo patient
126
7260
192
72
120
24
60
0
5
10
15
20
25
Death Stroke MI MAE
CEA (n=167)Stent (n=167)
SAPPHIRE CAS vs CEA
1 year results
P=014
P=083P=017
P=010
CEA can be performed in high-risk patients with acceptable standard complication rates
Mozes G et al Semin Vasc Surg 20051861ndash 8
octogenarians
121121
30-day stroke and death rate30-day stroke and death rate
5353 1313
Agegt80yAgegt80y Age 70-79yAge 70-79y Age 60-69Age 60-69
Is CAS safe in this subgroup
The CREST trial lead-in phase
Material - Methodsbull 67 monthsbull 520 patientsbull mean age 76 range 56-85bull 364 male (70) 156 female (30)bull mean follow-up was 32 months (range 1 ndash 54 months)
Retrospective study
bull We conducted a retrospective review of CAS from 2003 to 2008bull RX Acculink - RX Accunet carotid system (Guidant Abott)
Material - Methods
bull Symptomatic (stroke (135) TIA Fugax) 515
bull Asymptomatic 485
Results within early follow-up (lt30 days)
bull Mortality (09)Stroke (11)TIA (13)Non fatal MI (13)
MAE 46
Results within early follow-up (lt30 days)
Predictors of adverse outcomes includedbullAge gt80bullsymptomatic patientsbullFemale genderbullpredilation prior to CPD bullplacement of multiple stentsbullContralateral occlusionbullUnfavorable anatomy
Late Follow-Up (gt30 days)
bull Mortality (173 )Stroke (07)Restenosis gt70 (23)
Mean follow-up was 32 months (range 1 ndash 60 months) 46 (88) patients lost of FU
Conclusion
bullCAS within experienced hands can be highly efficient and durable
Acculink Accunet system is safe and effective for CAS
ConclusionsCEA is the goal standard when
bull specific carotid anatomy
bullExtensive arch and carotid bif calcification
bullAccess related problems
bullFresh thrombus at ICA lesion
bullldquoString signrdquo morphology
bullVery low GSM
Conclusions
CAS and CEA are not competitive procedures but powerful treatment options tailored on different groups of patients
The gold standard is the experienced vascular team able to twist between endovascular and open surgical options in order to achieve the best treatment for the patient
Thank you for your attention
- Slide 1
- Slide 2
- Slide 3
- Slide 4
- Slide 5
- Slide 6
- Slide 7
- Slide 8
- Slide 9
- Slide 10
- Slide 11
- Slide 12
- Slide 13
- Slide 14
- Slide 15
- Slide 16
- Slide 17
- Slide 18
- Slide 19
- Slide 20
- Slide 21
- Slide 22
- Slide 23
- Slide 24
- Slide 25
- Slide 26
- Slide 27
- Slide 28
- Slide 29
- Slide 30
- Slide 31
- Slide 32
- Slide 33
- Slide 34
- Slide 35
- Slide 36
- Slide 37
- Slide 38
- Slide 39
- Slide 40
-
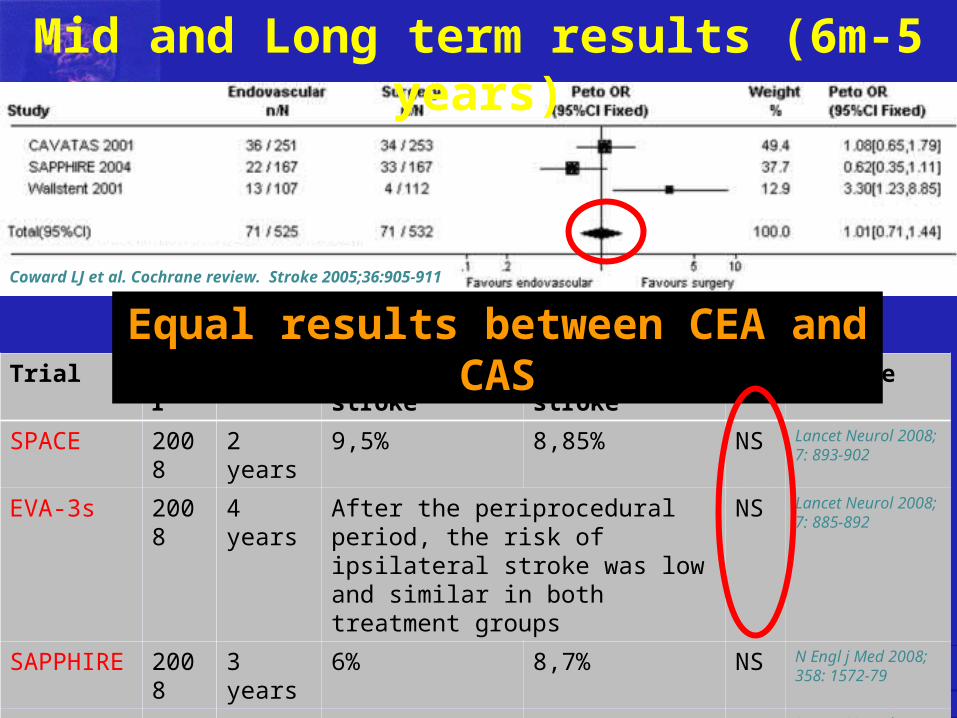
Trial Year FU CAS ips stroke CEA ips stroke P Article
SPACE 2008 2 years 95 885 NS Lancet Neurol 2008 7 893-902
EVA-3s 2008 4 years After the periprocedural period the risk of ipsilateral stroke was low and similar in both treatment groups
NS Lancet Neurol 2008 7 885-892
SAPPHIRE 2008 3 years 6 87 NS N Engl j Med 2008 358 1572-79
CAVATAS 2009 5 years 11middot3 8middot6 NS Lancet Neurol 20098(10)898-907
CREST 2011
Mid and Long term results (6m-5 years)
Coward LJ et al Cochrane review Stroke 200536905-911
Equal results between CEA and CAS
Cranial neuropathy
Stronly favored CAS
No significant difference in the major risks of treatment
Minor complication favorendovascular treatment
Conclusions
Insufficient evidence to support a widespread change in clinical practice
So which is the VERDICT
Current trials didnrsquot prove CAS inferiority
The initial question about gold standard is wrong
vsXBoth CAS CEAand
Play a role in stroke prevention in different patient groups
Defining patient groups that either CEA or CAS is beneficial
Vessel anatomy Plaque characteristics
The high risk patient
Defining patient groups that either CEA or CAS is beneficial
Vessel anatomyPlaque characteristics
The high risk patient
The influence of anatomy on treatment selection for carotid disease
1 Congenital anatomical variation (bovine arch aortic arch types I-III high or low carotid bifurcation aberrant vessels)
2 Alterations that occur with aging and hypertension (inflow and outflow tortuousity calcification thrombi)
3 Extension of disease (eg diffuse multisegmental disease involving the proximal CCA or distal ICA)
Vessel anatomy
Schneider PA et al Semin Vasc Surg 20216-225 2007
Vessel anatomy
Aortic arch type and orificial calcification
Vessel anatomy
Mobile thrombi Vessel anatomy
Vessel anatomyBovine carotid configuration
Proximal common carotid lesionsVessel anatomy
Tortuous CCA or ICA coil
Vessel anatomy
ldquoString signrdquo carotid morphology
Would you advance an EPD into such a vessel
Vessel anatomy
Defining patient groups that either CEA or CAS is beneficial
Vessel anatomyPlaque characteristics
The high risk patient
Plaque characteristics
Biasi et al ICAROS study Circulation 2004110756-62Fisher M et al Stroke 200536253ndash7Rothwell PM et al Stroke 200031615ndash21
bullGSMlt25 is related with a higher risk of neurologic complications after CASbulllow GSM is not a contraindication to CAS but rather a predictor of increased stroke riskbullLow GSM values are further related to future coronary events and higher rate of restenosis
Defining patient groups that either CEA or CAS is beneficial
Vessel anatomy Plaque characteristics
The high risk patient
24 30
60
96
12
3624
48
0
5
10
15
20
25
Death Stroke MI MAE
CEA (n=167)
Stent (n=167)
30 Days endpoint
P=068 P=100P=017
P=014
Theldquohigh riskrdquo patient
126
7260
192
72
120
24
60
0
5
10
15
20
25
Death Stroke MI MAE
CEA (n=167)Stent (n=167)
SAPPHIRE CAS vs CEA
1 year results
P=014
P=083P=017
P=010
CEA can be performed in high-risk patients with acceptable standard complication rates
Mozes G et al Semin Vasc Surg 20051861ndash 8
octogenarians
121121
30-day stroke and death rate30-day stroke and death rate
5353 1313
Agegt80yAgegt80y Age 70-79yAge 70-79y Age 60-69Age 60-69
Is CAS safe in this subgroup
The CREST trial lead-in phase
Material - Methodsbull 67 monthsbull 520 patientsbull mean age 76 range 56-85bull 364 male (70) 156 female (30)bull mean follow-up was 32 months (range 1 ndash 54 months)
Retrospective study
bull We conducted a retrospective review of CAS from 2003 to 2008bull RX Acculink - RX Accunet carotid system (Guidant Abott)
Material - Methods
bull Symptomatic (stroke (135) TIA Fugax) 515
bull Asymptomatic 485
Results within early follow-up (lt30 days)
bull Mortality (09)Stroke (11)TIA (13)Non fatal MI (13)
MAE 46
Results within early follow-up (lt30 days)
Predictors of adverse outcomes includedbullAge gt80bullsymptomatic patientsbullFemale genderbullpredilation prior to CPD bullplacement of multiple stentsbullContralateral occlusionbullUnfavorable anatomy
Late Follow-Up (gt30 days)
bull Mortality (173 )Stroke (07)Restenosis gt70 (23)
Mean follow-up was 32 months (range 1 ndash 60 months) 46 (88) patients lost of FU
Conclusion
bullCAS within experienced hands can be highly efficient and durable
Acculink Accunet system is safe and effective for CAS
ConclusionsCEA is the goal standard when
bull specific carotid anatomy
bullExtensive arch and carotid bif calcification
bullAccess related problems
bullFresh thrombus at ICA lesion
bullldquoString signrdquo morphology
bullVery low GSM
Conclusions
CAS and CEA are not competitive procedures but powerful treatment options tailored on different groups of patients
The gold standard is the experienced vascular team able to twist between endovascular and open surgical options in order to achieve the best treatment for the patient
Thank you for your attention
- Slide 1
- Slide 2
- Slide 3
- Slide 4
- Slide 5
- Slide 6
- Slide 7
- Slide 8
- Slide 9
- Slide 10
- Slide 11
- Slide 12
- Slide 13
- Slide 14
- Slide 15
- Slide 16
- Slide 17
- Slide 18
- Slide 19
- Slide 20
- Slide 21
- Slide 22
- Slide 23
- Slide 24
- Slide 25
- Slide 26
- Slide 27
- Slide 28
- Slide 29
- Slide 30
- Slide 31
- Slide 32
- Slide 33
- Slide 34
- Slide 35
- Slide 36
- Slide 37
- Slide 38
- Slide 39
- Slide 40
-
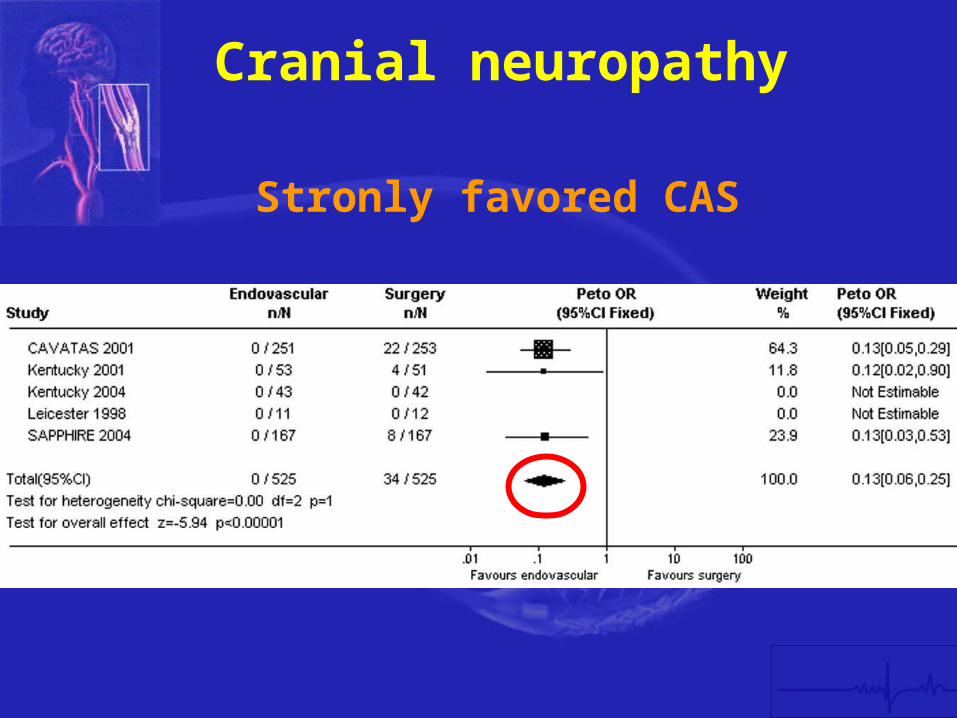
Cranial neuropathy
Stronly favored CAS
No significant difference in the major risks of treatment
Minor complication favorendovascular treatment
Conclusions
Insufficient evidence to support a widespread change in clinical practice
So which is the VERDICT
Current trials didnrsquot prove CAS inferiority
The initial question about gold standard is wrong
vsXBoth CAS CEAand
Play a role in stroke prevention in different patient groups
Defining patient groups that either CEA or CAS is beneficial
Vessel anatomy Plaque characteristics
The high risk patient
Defining patient groups that either CEA or CAS is beneficial
Vessel anatomyPlaque characteristics
The high risk patient
The influence of anatomy on treatment selection for carotid disease
1 Congenital anatomical variation (bovine arch aortic arch types I-III high or low carotid bifurcation aberrant vessels)
2 Alterations that occur with aging and hypertension (inflow and outflow tortuousity calcification thrombi)
3 Extension of disease (eg diffuse multisegmental disease involving the proximal CCA or distal ICA)
Vessel anatomy
Schneider PA et al Semin Vasc Surg 20216-225 2007
Vessel anatomy
Aortic arch type and orificial calcification
Vessel anatomy
Mobile thrombi Vessel anatomy
Vessel anatomyBovine carotid configuration
Proximal common carotid lesionsVessel anatomy
Tortuous CCA or ICA coil
Vessel anatomy
ldquoString signrdquo carotid morphology
Would you advance an EPD into such a vessel
Vessel anatomy
Defining patient groups that either CEA or CAS is beneficial
Vessel anatomyPlaque characteristics
The high risk patient
Plaque characteristics
Biasi et al ICAROS study Circulation 2004110756-62Fisher M et al Stroke 200536253ndash7Rothwell PM et al Stroke 200031615ndash21
bullGSMlt25 is related with a higher risk of neurologic complications after CASbulllow GSM is not a contraindication to CAS but rather a predictor of increased stroke riskbullLow GSM values are further related to future coronary events and higher rate of restenosis
Defining patient groups that either CEA or CAS is beneficial
Vessel anatomy Plaque characteristics
The high risk patient
24 30
60
96
12
3624
48
0
5
10
15
20
25
Death Stroke MI MAE
CEA (n=167)
Stent (n=167)
30 Days endpoint
P=068 P=100P=017
P=014
Theldquohigh riskrdquo patient
126
7260
192
72
120
24
60
0
5
10
15
20
25
Death Stroke MI MAE
CEA (n=167)Stent (n=167)
SAPPHIRE CAS vs CEA
1 year results
P=014
P=083P=017
P=010
CEA can be performed in high-risk patients with acceptable standard complication rates
Mozes G et al Semin Vasc Surg 20051861ndash 8
octogenarians
121121
30-day stroke and death rate30-day stroke and death rate
5353 1313
Agegt80yAgegt80y Age 70-79yAge 70-79y Age 60-69Age 60-69
Is CAS safe in this subgroup
The CREST trial lead-in phase
Material - Methodsbull 67 monthsbull 520 patientsbull mean age 76 range 56-85bull 364 male (70) 156 female (30)bull mean follow-up was 32 months (range 1 ndash 54 months)
Retrospective study
bull We conducted a retrospective review of CAS from 2003 to 2008bull RX Acculink - RX Accunet carotid system (Guidant Abott)
Material - Methods
bull Symptomatic (stroke (135) TIA Fugax) 515
bull Asymptomatic 485
Results within early follow-up (lt30 days)
bull Mortality (09)Stroke (11)TIA (13)Non fatal MI (13)
MAE 46
Results within early follow-up (lt30 days)
Predictors of adverse outcomes includedbullAge gt80bullsymptomatic patientsbullFemale genderbullpredilation prior to CPD bullplacement of multiple stentsbullContralateral occlusionbullUnfavorable anatomy
Late Follow-Up (gt30 days)
bull Mortality (173 )Stroke (07)Restenosis gt70 (23)
Mean follow-up was 32 months (range 1 ndash 60 months) 46 (88) patients lost of FU
Conclusion
bullCAS within experienced hands can be highly efficient and durable
Acculink Accunet system is safe and effective for CAS
ConclusionsCEA is the goal standard when
bull specific carotid anatomy
bullExtensive arch and carotid bif calcification
bullAccess related problems
bullFresh thrombus at ICA lesion
bullldquoString signrdquo morphology
bullVery low GSM
Conclusions
CAS and CEA are not competitive procedures but powerful treatment options tailored on different groups of patients
The gold standard is the experienced vascular team able to twist between endovascular and open surgical options in order to achieve the best treatment for the patient
Thank you for your attention
- Slide 1
- Slide 2
- Slide 3
- Slide 4
- Slide 5
- Slide 6
- Slide 7
- Slide 8
- Slide 9
- Slide 10
- Slide 11
- Slide 12
- Slide 13
- Slide 14
- Slide 15
- Slide 16
- Slide 17
- Slide 18
- Slide 19
- Slide 20
- Slide 21
- Slide 22
- Slide 23
- Slide 24
- Slide 25
- Slide 26
- Slide 27
- Slide 28
- Slide 29
- Slide 30
- Slide 31
- Slide 32
- Slide 33
- Slide 34
- Slide 35
- Slide 36
- Slide 37
- Slide 38
- Slide 39
- Slide 40
-
No significant difference in the major risks of treatment
Minor complication favorendovascular treatment
Conclusions
Insufficient evidence to support a widespread change in clinical practice
So which is the VERDICT
Current trials didnrsquot prove CAS inferiority
The initial question about gold standard is wrong
vsXBoth CAS CEAand
Play a role in stroke prevention in different patient groups
Defining patient groups that either CEA or CAS is beneficial
Vessel anatomy Plaque characteristics
The high risk patient
Defining patient groups that either CEA or CAS is beneficial
Vessel anatomyPlaque characteristics
The high risk patient
The influence of anatomy on treatment selection for carotid disease
1 Congenital anatomical variation (bovine arch aortic arch types I-III high or low carotid bifurcation aberrant vessels)
2 Alterations that occur with aging and hypertension (inflow and outflow tortuousity calcification thrombi)
3 Extension of disease (eg diffuse multisegmental disease involving the proximal CCA or distal ICA)
Vessel anatomy
Schneider PA et al Semin Vasc Surg 20216-225 2007
Vessel anatomy
Aortic arch type and orificial calcification
Vessel anatomy
Mobile thrombi Vessel anatomy
Vessel anatomyBovine carotid configuration
Proximal common carotid lesionsVessel anatomy
Tortuous CCA or ICA coil
Vessel anatomy
ldquoString signrdquo carotid morphology
Would you advance an EPD into such a vessel
Vessel anatomy
Defining patient groups that either CEA or CAS is beneficial
Vessel anatomyPlaque characteristics
The high risk patient
Plaque characteristics
Biasi et al ICAROS study Circulation 2004110756-62Fisher M et al Stroke 200536253ndash7Rothwell PM et al Stroke 200031615ndash21
bullGSMlt25 is related with a higher risk of neurologic complications after CASbulllow GSM is not a contraindication to CAS but rather a predictor of increased stroke riskbullLow GSM values are further related to future coronary events and higher rate of restenosis
Defining patient groups that either CEA or CAS is beneficial
Vessel anatomy Plaque characteristics
The high risk patient
24 30
60
96
12
3624
48
0
5
10
15
20
25
Death Stroke MI MAE
CEA (n=167)
Stent (n=167)
30 Days endpoint
P=068 P=100P=017
P=014
Theldquohigh riskrdquo patient
126
7260
192
72
120
24
60
0
5
10
15
20
25
Death Stroke MI MAE
CEA (n=167)Stent (n=167)
SAPPHIRE CAS vs CEA
1 year results
P=014
P=083P=017
P=010
CEA can be performed in high-risk patients with acceptable standard complication rates
Mozes G et al Semin Vasc Surg 20051861ndash 8
octogenarians
121121
30-day stroke and death rate30-day stroke and death rate
5353 1313
Agegt80yAgegt80y Age 70-79yAge 70-79y Age 60-69Age 60-69
Is CAS safe in this subgroup
The CREST trial lead-in phase
Material - Methodsbull 67 monthsbull 520 patientsbull mean age 76 range 56-85bull 364 male (70) 156 female (30)bull mean follow-up was 32 months (range 1 ndash 54 months)
Retrospective study
bull We conducted a retrospective review of CAS from 2003 to 2008bull RX Acculink - RX Accunet carotid system (Guidant Abott)
Material - Methods
bull Symptomatic (stroke (135) TIA Fugax) 515
bull Asymptomatic 485
Results within early follow-up (lt30 days)
bull Mortality (09)Stroke (11)TIA (13)Non fatal MI (13)
MAE 46
Results within early follow-up (lt30 days)
Predictors of adverse outcomes includedbullAge gt80bullsymptomatic patientsbullFemale genderbullpredilation prior to CPD bullplacement of multiple stentsbullContralateral occlusionbullUnfavorable anatomy
Late Follow-Up (gt30 days)
bull Mortality (173 )Stroke (07)Restenosis gt70 (23)
Mean follow-up was 32 months (range 1 ndash 60 months) 46 (88) patients lost of FU
Conclusion
bullCAS within experienced hands can be highly efficient and durable
Acculink Accunet system is safe and effective for CAS
ConclusionsCEA is the goal standard when
bull specific carotid anatomy
bullExtensive arch and carotid bif calcification
bullAccess related problems
bullFresh thrombus at ICA lesion
bullldquoString signrdquo morphology
bullVery low GSM
Conclusions
CAS and CEA are not competitive procedures but powerful treatment options tailored on different groups of patients
The gold standard is the experienced vascular team able to twist between endovascular and open surgical options in order to achieve the best treatment for the patient
Thank you for your attention
- Slide 1
- Slide 2
- Slide 3
- Slide 4
- Slide 5
- Slide 6
- Slide 7
- Slide 8
- Slide 9
- Slide 10
- Slide 11
- Slide 12
- Slide 13
- Slide 14
- Slide 15
- Slide 16
- Slide 17
- Slide 18
- Slide 19
- Slide 20
- Slide 21
- Slide 22
- Slide 23
- Slide 24
- Slide 25
- Slide 26
- Slide 27
- Slide 28
- Slide 29
- Slide 30
- Slide 31
- Slide 32
- Slide 33
- Slide 34
- Slide 35
- Slide 36
- Slide 37
- Slide 38
- Slide 39
- Slide 40
-
So which is the VERDICT
Current trials didnrsquot prove CAS inferiority
The initial question about gold standard is wrong
vsXBoth CAS CEAand
Play a role in stroke prevention in different patient groups
Defining patient groups that either CEA or CAS is beneficial
Vessel anatomy Plaque characteristics
The high risk patient
Defining patient groups that either CEA or CAS is beneficial
Vessel anatomyPlaque characteristics
The high risk patient
The influence of anatomy on treatment selection for carotid disease
1 Congenital anatomical variation (bovine arch aortic arch types I-III high or low carotid bifurcation aberrant vessels)
2 Alterations that occur with aging and hypertension (inflow and outflow tortuousity calcification thrombi)
3 Extension of disease (eg diffuse multisegmental disease involving the proximal CCA or distal ICA)
Vessel anatomy
Schneider PA et al Semin Vasc Surg 20216-225 2007
Vessel anatomy
Aortic arch type and orificial calcification
Vessel anatomy
Mobile thrombi Vessel anatomy
Vessel anatomyBovine carotid configuration
Proximal common carotid lesionsVessel anatomy
Tortuous CCA or ICA coil
Vessel anatomy
ldquoString signrdquo carotid morphology
Would you advance an EPD into such a vessel
Vessel anatomy
Defining patient groups that either CEA or CAS is beneficial
Vessel anatomyPlaque characteristics
The high risk patient
Plaque characteristics
Biasi et al ICAROS study Circulation 2004110756-62Fisher M et al Stroke 200536253ndash7Rothwell PM et al Stroke 200031615ndash21
bullGSMlt25 is related with a higher risk of neurologic complications after CASbulllow GSM is not a contraindication to CAS but rather a predictor of increased stroke riskbullLow GSM values are further related to future coronary events and higher rate of restenosis
Defining patient groups that either CEA or CAS is beneficial
Vessel anatomy Plaque characteristics
The high risk patient
24 30
60
96
12
3624
48
0
5
10
15
20
25
Death Stroke MI MAE
CEA (n=167)
Stent (n=167)
30 Days endpoint
P=068 P=100P=017
P=014
Theldquohigh riskrdquo patient
126
7260
192
72
120
24
60
0
5
10
15
20
25
Death Stroke MI MAE
CEA (n=167)Stent (n=167)
SAPPHIRE CAS vs CEA
1 year results
P=014
P=083P=017
P=010
CEA can be performed in high-risk patients with acceptable standard complication rates
Mozes G et al Semin Vasc Surg 20051861ndash 8
octogenarians
121121
30-day stroke and death rate30-day stroke and death rate
5353 1313
Agegt80yAgegt80y Age 70-79yAge 70-79y Age 60-69Age 60-69
Is CAS safe in this subgroup
The CREST trial lead-in phase
Material - Methodsbull 67 monthsbull 520 patientsbull mean age 76 range 56-85bull 364 male (70) 156 female (30)bull mean follow-up was 32 months (range 1 ndash 54 months)
Retrospective study
bull We conducted a retrospective review of CAS from 2003 to 2008bull RX Acculink - RX Accunet carotid system (Guidant Abott)
Material - Methods
bull Symptomatic (stroke (135) TIA Fugax) 515
bull Asymptomatic 485
Results within early follow-up (lt30 days)
bull Mortality (09)Stroke (11)TIA (13)Non fatal MI (13)
MAE 46
Results within early follow-up (lt30 days)
Predictors of adverse outcomes includedbullAge gt80bullsymptomatic patientsbullFemale genderbullpredilation prior to CPD bullplacement of multiple stentsbullContralateral occlusionbullUnfavorable anatomy
Late Follow-Up (gt30 days)
bull Mortality (173 )Stroke (07)Restenosis gt70 (23)
Mean follow-up was 32 months (range 1 ndash 60 months) 46 (88) patients lost of FU
Conclusion
bullCAS within experienced hands can be highly efficient and durable
Acculink Accunet system is safe and effective for CAS
ConclusionsCEA is the goal standard when
bull specific carotid anatomy
bullExtensive arch and carotid bif calcification
bullAccess related problems
bullFresh thrombus at ICA lesion
bullldquoString signrdquo morphology
bullVery low GSM
Conclusions
CAS and CEA are not competitive procedures but powerful treatment options tailored on different groups of patients
The gold standard is the experienced vascular team able to twist between endovascular and open surgical options in order to achieve the best treatment for the patient
Thank you for your attention
- Slide 1
- Slide 2
- Slide 3
- Slide 4
- Slide 5
- Slide 6
- Slide 7
- Slide 8
- Slide 9
- Slide 10
- Slide 11
- Slide 12
- Slide 13
- Slide 14
- Slide 15
- Slide 16
- Slide 17
- Slide 18
- Slide 19
- Slide 20
- Slide 21
- Slide 22
- Slide 23
- Slide 24
- Slide 25
- Slide 26
- Slide 27
- Slide 28
- Slide 29
- Slide 30
- Slide 31
- Slide 32
- Slide 33
- Slide 34
- Slide 35
- Slide 36
- Slide 37
- Slide 38
- Slide 39
- Slide 40
-
The initial question about gold standard is wrong
vsXBoth CAS CEAand
Play a role in stroke prevention in different patient groups
Defining patient groups that either CEA or CAS is beneficial
Vessel anatomy Plaque characteristics
The high risk patient
Defining patient groups that either CEA or CAS is beneficial
Vessel anatomyPlaque characteristics
The high risk patient
The influence of anatomy on treatment selection for carotid disease
1 Congenital anatomical variation (bovine arch aortic arch types I-III high or low carotid bifurcation aberrant vessels)
2 Alterations that occur with aging and hypertension (inflow and outflow tortuousity calcification thrombi)
3 Extension of disease (eg diffuse multisegmental disease involving the proximal CCA or distal ICA)
Vessel anatomy
Schneider PA et al Semin Vasc Surg 20216-225 2007
Vessel anatomy
Aortic arch type and orificial calcification
Vessel anatomy
Mobile thrombi Vessel anatomy
Vessel anatomyBovine carotid configuration
Proximal common carotid lesionsVessel anatomy
Tortuous CCA or ICA coil
Vessel anatomy
ldquoString signrdquo carotid morphology
Would you advance an EPD into such a vessel
Vessel anatomy
Defining patient groups that either CEA or CAS is beneficial
Vessel anatomyPlaque characteristics
The high risk patient
Plaque characteristics
Biasi et al ICAROS study Circulation 2004110756-62Fisher M et al Stroke 200536253ndash7Rothwell PM et al Stroke 200031615ndash21
bullGSMlt25 is related with a higher risk of neurologic complications after CASbulllow GSM is not a contraindication to CAS but rather a predictor of increased stroke riskbullLow GSM values are further related to future coronary events and higher rate of restenosis
Defining patient groups that either CEA or CAS is beneficial
Vessel anatomy Plaque characteristics
The high risk patient
24 30
60
96
12
3624
48
0
5
10
15
20
25
Death Stroke MI MAE
CEA (n=167)
Stent (n=167)
30 Days endpoint
P=068 P=100P=017
P=014
Theldquohigh riskrdquo patient
126
7260
192
72
120
24
60
0
5
10
15
20
25
Death Stroke MI MAE
CEA (n=167)Stent (n=167)
SAPPHIRE CAS vs CEA
1 year results
P=014
P=083P=017
P=010
CEA can be performed in high-risk patients with acceptable standard complication rates
Mozes G et al Semin Vasc Surg 20051861ndash 8
octogenarians
121121
30-day stroke and death rate30-day stroke and death rate
5353 1313
Agegt80yAgegt80y Age 70-79yAge 70-79y Age 60-69Age 60-69
Is CAS safe in this subgroup
The CREST trial lead-in phase
Material - Methodsbull 67 monthsbull 520 patientsbull mean age 76 range 56-85bull 364 male (70) 156 female (30)bull mean follow-up was 32 months (range 1 ndash 54 months)
Retrospective study
bull We conducted a retrospective review of CAS from 2003 to 2008bull RX Acculink - RX Accunet carotid system (Guidant Abott)
Material - Methods
bull Symptomatic (stroke (135) TIA Fugax) 515
bull Asymptomatic 485
Results within early follow-up (lt30 days)
bull Mortality (09)Stroke (11)TIA (13)Non fatal MI (13)
MAE 46
Results within early follow-up (lt30 days)
Predictors of adverse outcomes includedbullAge gt80bullsymptomatic patientsbullFemale genderbullpredilation prior to CPD bullplacement of multiple stentsbullContralateral occlusionbullUnfavorable anatomy
Late Follow-Up (gt30 days)
bull Mortality (173 )Stroke (07)Restenosis gt70 (23)
Mean follow-up was 32 months (range 1 ndash 60 months) 46 (88) patients lost of FU
Conclusion
bullCAS within experienced hands can be highly efficient and durable
Acculink Accunet system is safe and effective for CAS
ConclusionsCEA is the goal standard when
bull specific carotid anatomy
bullExtensive arch and carotid bif calcification
bullAccess related problems
bullFresh thrombus at ICA lesion
bullldquoString signrdquo morphology
bullVery low GSM
Conclusions
CAS and CEA are not competitive procedures but powerful treatment options tailored on different groups of patients
The gold standard is the experienced vascular team able to twist between endovascular and open surgical options in order to achieve the best treatment for the patient
Thank you for your attention
- Slide 1
- Slide 2
- Slide 3
- Slide 4
- Slide 5
- Slide 6
- Slide 7
- Slide 8
- Slide 9
- Slide 10
- Slide 11
- Slide 12
- Slide 13
- Slide 14
- Slide 15
- Slide 16
- Slide 17
- Slide 18
- Slide 19
- Slide 20
- Slide 21
- Slide 22
- Slide 23
- Slide 24
- Slide 25
- Slide 26
- Slide 27
- Slide 28
- Slide 29
- Slide 30
- Slide 31
- Slide 32
- Slide 33
- Slide 34
- Slide 35
- Slide 36
- Slide 37
- Slide 38
- Slide 39
- Slide 40
-
Defining patient groups that either CEA or CAS is beneficial
Vessel anatomy Plaque characteristics
The high risk patient
Defining patient groups that either CEA or CAS is beneficial
Vessel anatomyPlaque characteristics
The high risk patient
The influence of anatomy on treatment selection for carotid disease
1 Congenital anatomical variation (bovine arch aortic arch types I-III high or low carotid bifurcation aberrant vessels)
2 Alterations that occur with aging and hypertension (inflow and outflow tortuousity calcification thrombi)
3 Extension of disease (eg diffuse multisegmental disease involving the proximal CCA or distal ICA)
Vessel anatomy
Schneider PA et al Semin Vasc Surg 20216-225 2007
Vessel anatomy
Aortic arch type and orificial calcification
Vessel anatomy
Mobile thrombi Vessel anatomy
Vessel anatomyBovine carotid configuration
Proximal common carotid lesionsVessel anatomy
Tortuous CCA or ICA coil
Vessel anatomy
ldquoString signrdquo carotid morphology
Would you advance an EPD into such a vessel
Vessel anatomy
Defining patient groups that either CEA or CAS is beneficial
Vessel anatomyPlaque characteristics
The high risk patient
Plaque characteristics
Biasi et al ICAROS study Circulation 2004110756-62Fisher M et al Stroke 200536253ndash7Rothwell PM et al Stroke 200031615ndash21
bullGSMlt25 is related with a higher risk of neurologic complications after CASbulllow GSM is not a contraindication to CAS but rather a predictor of increased stroke riskbullLow GSM values are further related to future coronary events and higher rate of restenosis
Defining patient groups that either CEA or CAS is beneficial
Vessel anatomy Plaque characteristics
The high risk patient
24 30
60
96
12
3624
48
0
5
10
15
20
25
Death Stroke MI MAE
CEA (n=167)
Stent (n=167)
30 Days endpoint
P=068 P=100P=017
P=014
Theldquohigh riskrdquo patient
126
7260
192
72
120
24
60
0
5
10
15
20
25
Death Stroke MI MAE
CEA (n=167)Stent (n=167)
SAPPHIRE CAS vs CEA
1 year results
P=014
P=083P=017
P=010
CEA can be performed in high-risk patients with acceptable standard complication rates
Mozes G et al Semin Vasc Surg 20051861ndash 8
octogenarians
121121
30-day stroke and death rate30-day stroke and death rate
5353 1313
Agegt80yAgegt80y Age 70-79yAge 70-79y Age 60-69Age 60-69
Is CAS safe in this subgroup
The CREST trial lead-in phase
Material - Methodsbull 67 monthsbull 520 patientsbull mean age 76 range 56-85bull 364 male (70) 156 female (30)bull mean follow-up was 32 months (range 1 ndash 54 months)
Retrospective study
bull We conducted a retrospective review of CAS from 2003 to 2008bull RX Acculink - RX Accunet carotid system (Guidant Abott)
Material - Methods
bull Symptomatic (stroke (135) TIA Fugax) 515
bull Asymptomatic 485
Results within early follow-up (lt30 days)
bull Mortality (09)Stroke (11)TIA (13)Non fatal MI (13)
MAE 46
Results within early follow-up (lt30 days)
Predictors of adverse outcomes includedbullAge gt80bullsymptomatic patientsbullFemale genderbullpredilation prior to CPD bullplacement of multiple stentsbullContralateral occlusionbullUnfavorable anatomy
Late Follow-Up (gt30 days)
bull Mortality (173 )Stroke (07)Restenosis gt70 (23)
Mean follow-up was 32 months (range 1 ndash 60 months) 46 (88) patients lost of FU
Conclusion
bullCAS within experienced hands can be highly efficient and durable
Acculink Accunet system is safe and effective for CAS
ConclusionsCEA is the goal standard when
bull specific carotid anatomy
bullExtensive arch and carotid bif calcification
bullAccess related problems
bullFresh thrombus at ICA lesion
bullldquoString signrdquo morphology
bullVery low GSM
Conclusions
CAS and CEA are not competitive procedures but powerful treatment options tailored on different groups of patients
The gold standard is the experienced vascular team able to twist between endovascular and open surgical options in order to achieve the best treatment for the patient
Thank you for your attention
- Slide 1
- Slide 2
- Slide 3
- Slide 4
- Slide 5
- Slide 6
- Slide 7
- Slide 8
- Slide 9
- Slide 10
- Slide 11
- Slide 12
- Slide 13
- Slide 14
- Slide 15
- Slide 16
- Slide 17
- Slide 18
- Slide 19
- Slide 20
- Slide 21
- Slide 22
- Slide 23
- Slide 24
- Slide 25
- Slide 26
- Slide 27
- Slide 28
- Slide 29
- Slide 30
- Slide 31
- Slide 32
- Slide 33
- Slide 34
- Slide 35
- Slide 36
- Slide 37
- Slide 38
- Slide 39
- Slide 40
-
Defining patient groups that either CEA or CAS is beneficial
Vessel anatomyPlaque characteristics
The high risk patient
The influence of anatomy on treatment selection for carotid disease
1 Congenital anatomical variation (bovine arch aortic arch types I-III high or low carotid bifurcation aberrant vessels)
2 Alterations that occur with aging and hypertension (inflow and outflow tortuousity calcification thrombi)
3 Extension of disease (eg diffuse multisegmental disease involving the proximal CCA or distal ICA)
Vessel anatomy
Schneider PA et al Semin Vasc Surg 20216-225 2007
Vessel anatomy
Aortic arch type and orificial calcification
Vessel anatomy
Mobile thrombi Vessel anatomy
Vessel anatomyBovine carotid configuration
Proximal common carotid lesionsVessel anatomy
Tortuous CCA or ICA coil
Vessel anatomy
ldquoString signrdquo carotid morphology
Would you advance an EPD into such a vessel
Vessel anatomy
Defining patient groups that either CEA or CAS is beneficial
Vessel anatomyPlaque characteristics
The high risk patient
Plaque characteristics
Biasi et al ICAROS study Circulation 2004110756-62Fisher M et al Stroke 200536253ndash7Rothwell PM et al Stroke 200031615ndash21
bullGSMlt25 is related with a higher risk of neurologic complications after CASbulllow GSM is not a contraindication to CAS but rather a predictor of increased stroke riskbullLow GSM values are further related to future coronary events and higher rate of restenosis
Defining patient groups that either CEA or CAS is beneficial
Vessel anatomy Plaque characteristics
The high risk patient
24 30
60
96
12
3624
48
0
5
10
15
20
25
Death Stroke MI MAE
CEA (n=167)
Stent (n=167)
30 Days endpoint
P=068 P=100P=017
P=014
Theldquohigh riskrdquo patient
126
7260
192
72
120
24
60
0
5
10
15
20
25
Death Stroke MI MAE
CEA (n=167)Stent (n=167)
SAPPHIRE CAS vs CEA
1 year results
P=014
P=083P=017
P=010
CEA can be performed in high-risk patients with acceptable standard complication rates
Mozes G et al Semin Vasc Surg 20051861ndash 8
octogenarians
121121
30-day stroke and death rate30-day stroke and death rate
5353 1313
Agegt80yAgegt80y Age 70-79yAge 70-79y Age 60-69Age 60-69
Is CAS safe in this subgroup
The CREST trial lead-in phase
Material - Methodsbull 67 monthsbull 520 patientsbull mean age 76 range 56-85bull 364 male (70) 156 female (30)bull mean follow-up was 32 months (range 1 ndash 54 months)
Retrospective study
bull We conducted a retrospective review of CAS from 2003 to 2008bull RX Acculink - RX Accunet carotid system (Guidant Abott)
Material - Methods
bull Symptomatic (stroke (135) TIA Fugax) 515
bull Asymptomatic 485
Results within early follow-up (lt30 days)
bull Mortality (09)Stroke (11)TIA (13)Non fatal MI (13)
MAE 46
Results within early follow-up (lt30 days)
Predictors of adverse outcomes includedbullAge gt80bullsymptomatic patientsbullFemale genderbullpredilation prior to CPD bullplacement of multiple stentsbullContralateral occlusionbullUnfavorable anatomy
Late Follow-Up (gt30 days)
bull Mortality (173 )Stroke (07)Restenosis gt70 (23)
Mean follow-up was 32 months (range 1 ndash 60 months) 46 (88) patients lost of FU
Conclusion
bullCAS within experienced hands can be highly efficient and durable
Acculink Accunet system is safe and effective for CAS
ConclusionsCEA is the goal standard when
bull specific carotid anatomy
bullExtensive arch and carotid bif calcification
bullAccess related problems
bullFresh thrombus at ICA lesion
bullldquoString signrdquo morphology
bullVery low GSM
Conclusions
CAS and CEA are not competitive procedures but powerful treatment options tailored on different groups of patients
The gold standard is the experienced vascular team able to twist between endovascular and open surgical options in order to achieve the best treatment for the patient
Thank you for your attention
- Slide 1
- Slide 2
- Slide 3
- Slide 4
- Slide 5
- Slide 6
- Slide 7
- Slide 8
- Slide 9
- Slide 10
- Slide 11
- Slide 12
- Slide 13
- Slide 14
- Slide 15
- Slide 16
- Slide 17
- Slide 18
- Slide 19
- Slide 20
- Slide 21
- Slide 22
- Slide 23
- Slide 24
- Slide 25
- Slide 26
- Slide 27
- Slide 28
- Slide 29
- Slide 30
- Slide 31
- Slide 32
- Slide 33
- Slide 34
- Slide 35
- Slide 36
- Slide 37
- Slide 38
- Slide 39
- Slide 40
-
The influence of anatomy on treatment selection for carotid disease
1 Congenital anatomical variation (bovine arch aortic arch types I-III high or low carotid bifurcation aberrant vessels)
2 Alterations that occur with aging and hypertension (inflow and outflow tortuousity calcification thrombi)
3 Extension of disease (eg diffuse multisegmental disease involving the proximal CCA or distal ICA)
Vessel anatomy
Schneider PA et al Semin Vasc Surg 20216-225 2007
Vessel anatomy
Aortic arch type and orificial calcification
Vessel anatomy
Mobile thrombi Vessel anatomy
Vessel anatomyBovine carotid configuration
Proximal common carotid lesionsVessel anatomy
Tortuous CCA or ICA coil
Vessel anatomy
ldquoString signrdquo carotid morphology
Would you advance an EPD into such a vessel
Vessel anatomy
Defining patient groups that either CEA or CAS is beneficial
Vessel anatomyPlaque characteristics
The high risk patient
Plaque characteristics
Biasi et al ICAROS study Circulation 2004110756-62Fisher M et al Stroke 200536253ndash7Rothwell PM et al Stroke 200031615ndash21
bullGSMlt25 is related with a higher risk of neurologic complications after CASbulllow GSM is not a contraindication to CAS but rather a predictor of increased stroke riskbullLow GSM values are further related to future coronary events and higher rate of restenosis
Defining patient groups that either CEA or CAS is beneficial
Vessel anatomy Plaque characteristics
The high risk patient
24 30
60
96
12
3624
48
0
5
10
15
20
25
Death Stroke MI MAE
CEA (n=167)
Stent (n=167)
30 Days endpoint
P=068 P=100P=017
P=014
Theldquohigh riskrdquo patient
126
7260
192
72
120
24
60
0
5
10
15
20
25
Death Stroke MI MAE
CEA (n=167)Stent (n=167)
SAPPHIRE CAS vs CEA
1 year results
P=014
P=083P=017
P=010
CEA can be performed in high-risk patients with acceptable standard complication rates
Mozes G et al Semin Vasc Surg 20051861ndash 8
octogenarians
121121
30-day stroke and death rate30-day stroke and death rate
5353 1313
Agegt80yAgegt80y Age 70-79yAge 70-79y Age 60-69Age 60-69
Is CAS safe in this subgroup
The CREST trial lead-in phase
Material - Methodsbull 67 monthsbull 520 patientsbull mean age 76 range 56-85bull 364 male (70) 156 female (30)bull mean follow-up was 32 months (range 1 ndash 54 months)
Retrospective study
bull We conducted a retrospective review of CAS from 2003 to 2008bull RX Acculink - RX Accunet carotid system (Guidant Abott)
Material - Methods
bull Symptomatic (stroke (135) TIA Fugax) 515
bull Asymptomatic 485
Results within early follow-up (lt30 days)
bull Mortality (09)Stroke (11)TIA (13)Non fatal MI (13)
MAE 46
Results within early follow-up (lt30 days)
Predictors of adverse outcomes includedbullAge gt80bullsymptomatic patientsbullFemale genderbullpredilation prior to CPD bullplacement of multiple stentsbullContralateral occlusionbullUnfavorable anatomy
Late Follow-Up (gt30 days)
bull Mortality (173 )Stroke (07)Restenosis gt70 (23)
Mean follow-up was 32 months (range 1 ndash 60 months) 46 (88) patients lost of FU
Conclusion
bullCAS within experienced hands can be highly efficient and durable
Acculink Accunet system is safe and effective for CAS
ConclusionsCEA is the goal standard when
bull specific carotid anatomy
bullExtensive arch and carotid bif calcification
bullAccess related problems
bullFresh thrombus at ICA lesion
bullldquoString signrdquo morphology
bullVery low GSM
Conclusions
CAS and CEA are not competitive procedures but powerful treatment options tailored on different groups of patients
The gold standard is the experienced vascular team able to twist between endovascular and open surgical options in order to achieve the best treatment for the patient
Thank you for your attention
- Slide 1
- Slide 2
- Slide 3
- Slide 4
- Slide 5
- Slide 6
- Slide 7
- Slide 8
- Slide 9
- Slide 10
- Slide 11
- Slide 12
- Slide 13
- Slide 14
- Slide 15
- Slide 16
- Slide 17
- Slide 18
- Slide 19
- Slide 20
- Slide 21
- Slide 22
- Slide 23
- Slide 24
- Slide 25
- Slide 26
- Slide 27
- Slide 28
- Slide 29
- Slide 30
- Slide 31
- Slide 32
- Slide 33
- Slide 34
- Slide 35
- Slide 36
- Slide 37
- Slide 38
- Slide 39
- Slide 40
-
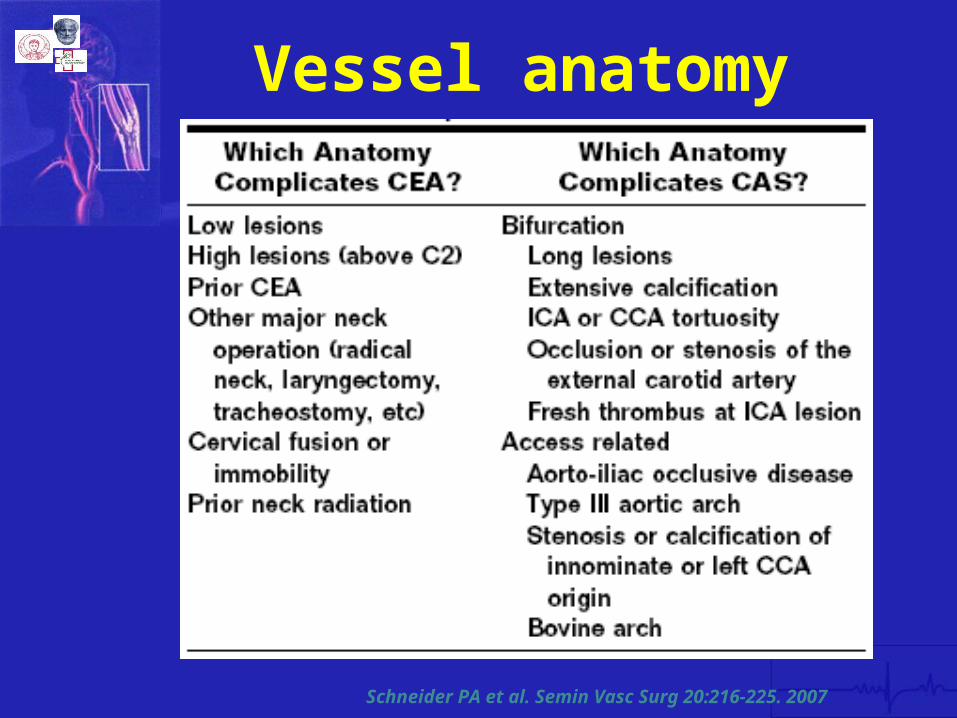
Schneider PA et al Semin Vasc Surg 20216-225 2007
Vessel anatomy
Aortic arch type and orificial calcification
Vessel anatomy
Mobile thrombi Vessel anatomy
Vessel anatomyBovine carotid configuration
Proximal common carotid lesionsVessel anatomy
Tortuous CCA or ICA coil
Vessel anatomy
ldquoString signrdquo carotid morphology
Would you advance an EPD into such a vessel
Vessel anatomy
Defining patient groups that either CEA or CAS is beneficial
Vessel anatomyPlaque characteristics
The high risk patient
Plaque characteristics
Biasi et al ICAROS study Circulation 2004110756-62Fisher M et al Stroke 200536253ndash7Rothwell PM et al Stroke 200031615ndash21
bullGSMlt25 is related with a higher risk of neurologic complications after CASbulllow GSM is not a contraindication to CAS but rather a predictor of increased stroke riskbullLow GSM values are further related to future coronary events and higher rate of restenosis
Defining patient groups that either CEA or CAS is beneficial
Vessel anatomy Plaque characteristics
The high risk patient
24 30
60
96
12
3624
48
0
5
10
15
20
25
Death Stroke MI MAE
CEA (n=167)
Stent (n=167)
30 Days endpoint
P=068 P=100P=017
P=014
Theldquohigh riskrdquo patient
126
7260
192
72
120
24
60
0
5
10
15
20
25
Death Stroke MI MAE
CEA (n=167)Stent (n=167)
SAPPHIRE CAS vs CEA
1 year results
P=014
P=083P=017
P=010
CEA can be performed in high-risk patients with acceptable standard complication rates
Mozes G et al Semin Vasc Surg 20051861ndash 8
octogenarians
121121
30-day stroke and death rate30-day stroke and death rate
5353 1313
Agegt80yAgegt80y Age 70-79yAge 70-79y Age 60-69Age 60-69
Is CAS safe in this subgroup
The CREST trial lead-in phase
Material - Methodsbull 67 monthsbull 520 patientsbull mean age 76 range 56-85bull 364 male (70) 156 female (30)bull mean follow-up was 32 months (range 1 ndash 54 months)
Retrospective study
bull We conducted a retrospective review of CAS from 2003 to 2008bull RX Acculink - RX Accunet carotid system (Guidant Abott)
Material - Methods
bull Symptomatic (stroke (135) TIA Fugax) 515
bull Asymptomatic 485
Results within early follow-up (lt30 days)
bull Mortality (09)Stroke (11)TIA (13)Non fatal MI (13)
MAE 46
Results within early follow-up (lt30 days)
Predictors of adverse outcomes includedbullAge gt80bullsymptomatic patientsbullFemale genderbullpredilation prior to CPD bullplacement of multiple stentsbullContralateral occlusionbullUnfavorable anatomy
Late Follow-Up (gt30 days)
bull Mortality (173 )Stroke (07)Restenosis gt70 (23)
Mean follow-up was 32 months (range 1 ndash 60 months) 46 (88) patients lost of FU
Conclusion
bullCAS within experienced hands can be highly efficient and durable
Acculink Accunet system is safe and effective for CAS
ConclusionsCEA is the goal standard when
bull specific carotid anatomy
bullExtensive arch and carotid bif calcification
bullAccess related problems
bullFresh thrombus at ICA lesion
bullldquoString signrdquo morphology
bullVery low GSM
Conclusions
CAS and CEA are not competitive procedures but powerful treatment options tailored on different groups of patients
The gold standard is the experienced vascular team able to twist between endovascular and open surgical options in order to achieve the best treatment for the patient
Thank you for your attention
- Slide 1
- Slide 2
- Slide 3
- Slide 4
- Slide 5
- Slide 6
- Slide 7
- Slide 8
- Slide 9
- Slide 10
- Slide 11
- Slide 12
- Slide 13
- Slide 14
- Slide 15
- Slide 16
- Slide 17
- Slide 18
- Slide 19
- Slide 20
- Slide 21
- Slide 22
- Slide 23
- Slide 24
- Slide 25
- Slide 26
- Slide 27
- Slide 28
- Slide 29
- Slide 30
- Slide 31
- Slide 32
- Slide 33
- Slide 34
- Slide 35
- Slide 36
- Slide 37
- Slide 38
- Slide 39
- Slide 40
-
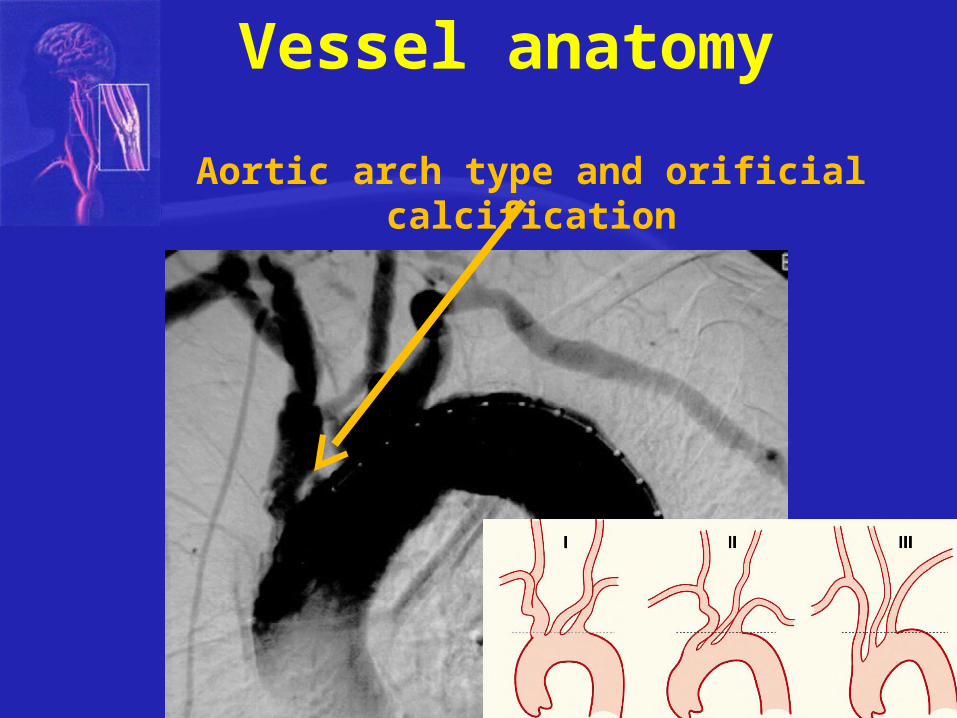
Aortic arch type and orificial calcification
Vessel anatomy
Mobile thrombi Vessel anatomy
Vessel anatomyBovine carotid configuration
Proximal common carotid lesionsVessel anatomy
Tortuous CCA or ICA coil
Vessel anatomy
ldquoString signrdquo carotid morphology
Would you advance an EPD into such a vessel
Vessel anatomy
Defining patient groups that either CEA or CAS is beneficial
Vessel anatomyPlaque characteristics
The high risk patient
Plaque characteristics
Biasi et al ICAROS study Circulation 2004110756-62Fisher M et al Stroke 200536253ndash7Rothwell PM et al Stroke 200031615ndash21
bullGSMlt25 is related with a higher risk of neurologic complications after CASbulllow GSM is not a contraindication to CAS but rather a predictor of increased stroke riskbullLow GSM values are further related to future coronary events and higher rate of restenosis
Defining patient groups that either CEA or CAS is beneficial
Vessel anatomy Plaque characteristics
The high risk patient
24 30
60
96
12
3624
48
0
5
10
15
20
25
Death Stroke MI MAE
CEA (n=167)
Stent (n=167)
30 Days endpoint
P=068 P=100P=017
P=014
Theldquohigh riskrdquo patient
126
7260
192
72
120
24
60
0
5
10
15
20
25
Death Stroke MI MAE
CEA (n=167)Stent (n=167)
SAPPHIRE CAS vs CEA
1 year results
P=014
P=083P=017
P=010
CEA can be performed in high-risk patients with acceptable standard complication rates
Mozes G et al Semin Vasc Surg 20051861ndash 8
octogenarians
121121
30-day stroke and death rate30-day stroke and death rate
5353 1313
Agegt80yAgegt80y Age 70-79yAge 70-79y Age 60-69Age 60-69
Is CAS safe in this subgroup
The CREST trial lead-in phase
Material - Methodsbull 67 monthsbull 520 patientsbull mean age 76 range 56-85bull 364 male (70) 156 female (30)bull mean follow-up was 32 months (range 1 ndash 54 months)
Retrospective study
bull We conducted a retrospective review of CAS from 2003 to 2008bull RX Acculink - RX Accunet carotid system (Guidant Abott)
Material - Methods
bull Symptomatic (stroke (135) TIA Fugax) 515
bull Asymptomatic 485
Results within early follow-up (lt30 days)
bull Mortality (09)Stroke (11)TIA (13)Non fatal MI (13)
MAE 46
Results within early follow-up (lt30 days)
Predictors of adverse outcomes includedbullAge gt80bullsymptomatic patientsbullFemale genderbullpredilation prior to CPD bullplacement of multiple stentsbullContralateral occlusionbullUnfavorable anatomy
Late Follow-Up (gt30 days)
bull Mortality (173 )Stroke (07)Restenosis gt70 (23)
Mean follow-up was 32 months (range 1 ndash 60 months) 46 (88) patients lost of FU
Conclusion
bullCAS within experienced hands can be highly efficient and durable
Acculink Accunet system is safe and effective for CAS
ConclusionsCEA is the goal standard when
bull specific carotid anatomy
bullExtensive arch and carotid bif calcification
bullAccess related problems
bullFresh thrombus at ICA lesion
bullldquoString signrdquo morphology
bullVery low GSM
Conclusions
CAS and CEA are not competitive procedures but powerful treatment options tailored on different groups of patients
The gold standard is the experienced vascular team able to twist between endovascular and open surgical options in order to achieve the best treatment for the patient
Thank you for your attention
- Slide 1
- Slide 2
- Slide 3
- Slide 4
- Slide 5
- Slide 6
- Slide 7
- Slide 8
- Slide 9
- Slide 10
- Slide 11
- Slide 12
- Slide 13
- Slide 14
- Slide 15
- Slide 16
- Slide 17
- Slide 18
- Slide 19
- Slide 20
- Slide 21
- Slide 22
- Slide 23
- Slide 24
- Slide 25
- Slide 26
- Slide 27
- Slide 28
- Slide 29
- Slide 30
- Slide 31
- Slide 32
- Slide 33
- Slide 34
- Slide 35
- Slide 36
- Slide 37
- Slide 38
- Slide 39
- Slide 40
-
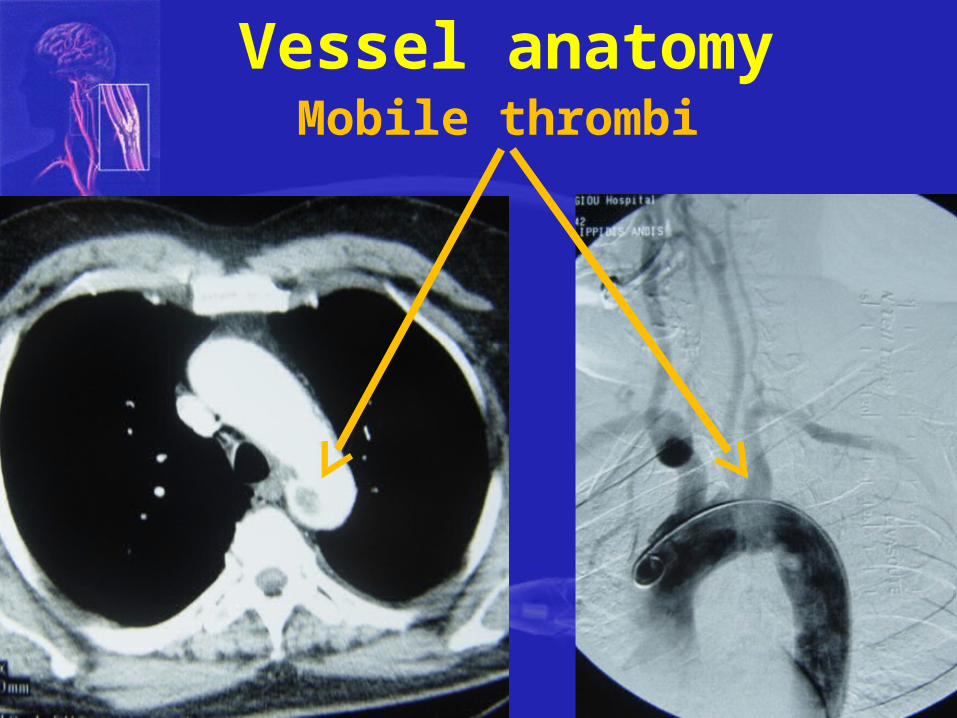
Mobile thrombi Vessel anatomy
Vessel anatomyBovine carotid configuration
Proximal common carotid lesionsVessel anatomy
Tortuous CCA or ICA coil
Vessel anatomy
ldquoString signrdquo carotid morphology
Would you advance an EPD into such a vessel
Vessel anatomy
Defining patient groups that either CEA or CAS is beneficial
Vessel anatomyPlaque characteristics
The high risk patient
Plaque characteristics
Biasi et al ICAROS study Circulation 2004110756-62Fisher M et al Stroke 200536253ndash7Rothwell PM et al Stroke 200031615ndash21
bullGSMlt25 is related with a higher risk of neurologic complications after CASbulllow GSM is not a contraindication to CAS but rather a predictor of increased stroke riskbullLow GSM values are further related to future coronary events and higher rate of restenosis
Defining patient groups that either CEA or CAS is beneficial
Vessel anatomy Plaque characteristics
The high risk patient
24 30
60
96
12
3624
48
0
5
10
15
20
25
Death Stroke MI MAE
CEA (n=167)
Stent (n=167)
30 Days endpoint
P=068 P=100P=017
P=014
Theldquohigh riskrdquo patient
126
7260
192
72
120
24
60
0
5
10
15
20
25
Death Stroke MI MAE
CEA (n=167)Stent (n=167)
SAPPHIRE CAS vs CEA
1 year results
P=014
P=083P=017
P=010
CEA can be performed in high-risk patients with acceptable standard complication rates
Mozes G et al Semin Vasc Surg 20051861ndash 8
octogenarians
121121
30-day stroke and death rate30-day stroke and death rate
5353 1313
Agegt80yAgegt80y Age 70-79yAge 70-79y Age 60-69Age 60-69
Is CAS safe in this subgroup
The CREST trial lead-in phase
Material - Methodsbull 67 monthsbull 520 patientsbull mean age 76 range 56-85bull 364 male (70) 156 female (30)bull mean follow-up was 32 months (range 1 ndash 54 months)
Retrospective study
bull We conducted a retrospective review of CAS from 2003 to 2008bull RX Acculink - RX Accunet carotid system (Guidant Abott)
Material - Methods
bull Symptomatic (stroke (135) TIA Fugax) 515
bull Asymptomatic 485
Results within early follow-up (lt30 days)
bull Mortality (09)Stroke (11)TIA (13)Non fatal MI (13)
MAE 46
Results within early follow-up (lt30 days)
Predictors of adverse outcomes includedbullAge gt80bullsymptomatic patientsbullFemale genderbullpredilation prior to CPD bullplacement of multiple stentsbullContralateral occlusionbullUnfavorable anatomy
Late Follow-Up (gt30 days)
bull Mortality (173 )Stroke (07)Restenosis gt70 (23)
Mean follow-up was 32 months (range 1 ndash 60 months) 46 (88) patients lost of FU
Conclusion
bullCAS within experienced hands can be highly efficient and durable
Acculink Accunet system is safe and effective for CAS
ConclusionsCEA is the goal standard when
bull specific carotid anatomy
bullExtensive arch and carotid bif calcification
bullAccess related problems
bullFresh thrombus at ICA lesion
bullldquoString signrdquo morphology
bullVery low GSM
Conclusions
CAS and CEA are not competitive procedures but powerful treatment options tailored on different groups of patients
The gold standard is the experienced vascular team able to twist between endovascular and open surgical options in order to achieve the best treatment for the patient
Thank you for your attention
- Slide 1
- Slide 2
- Slide 3
- Slide 4
- Slide 5
- Slide 6
- Slide 7
- Slide 8
- Slide 9
- Slide 10
- Slide 11
- Slide 12
- Slide 13
- Slide 14
- Slide 15
- Slide 16
- Slide 17
- Slide 18
- Slide 19
- Slide 20
- Slide 21
- Slide 22
- Slide 23
- Slide 24
- Slide 25
- Slide 26
- Slide 27
- Slide 28
- Slide 29
- Slide 30
- Slide 31
- Slide 32
- Slide 33
- Slide 34
- Slide 35
- Slide 36
- Slide 37
- Slide 38
- Slide 39
- Slide 40
-
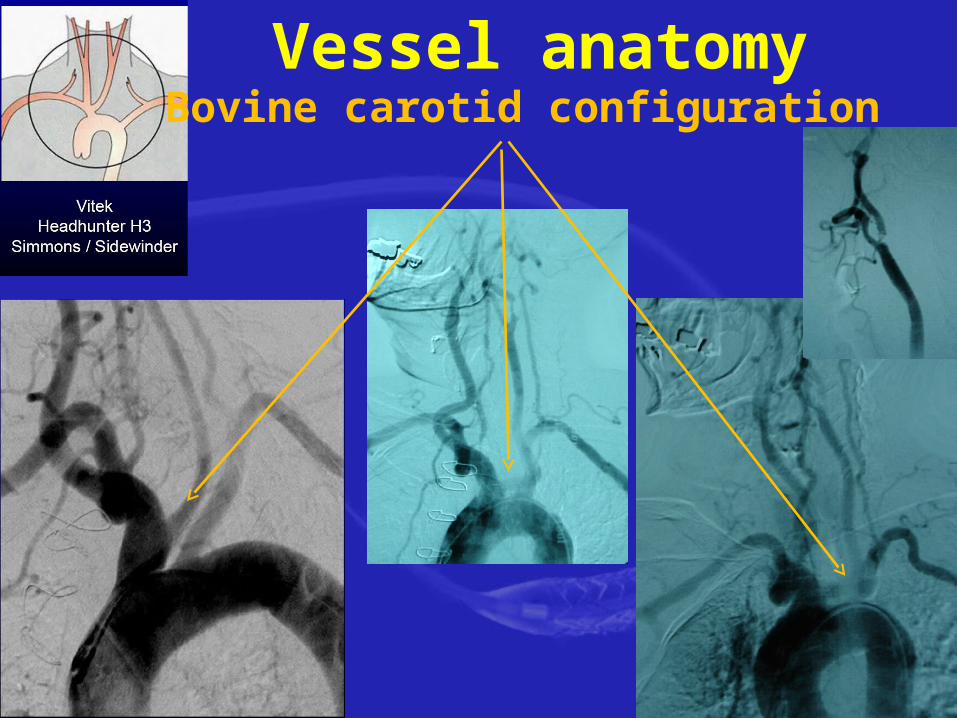
Vessel anatomyBovine carotid configuration
Proximal common carotid lesionsVessel anatomy
Tortuous CCA or ICA coil
Vessel anatomy
ldquoString signrdquo carotid morphology
Would you advance an EPD into such a vessel
Vessel anatomy
Defining patient groups that either CEA or CAS is beneficial
Vessel anatomyPlaque characteristics
The high risk patient
Plaque characteristics
Biasi et al ICAROS study Circulation 2004110756-62Fisher M et al Stroke 200536253ndash7Rothwell PM et al Stroke 200031615ndash21
bullGSMlt25 is related with a higher risk of neurologic complications after CASbulllow GSM is not a contraindication to CAS but rather a predictor of increased stroke riskbullLow GSM values are further related to future coronary events and higher rate of restenosis
Defining patient groups that either CEA or CAS is beneficial
Vessel anatomy Plaque characteristics
The high risk patient
24 30
60
96
12
3624
48
0
5
10
15
20
25
Death Stroke MI MAE
CEA (n=167)
Stent (n=167)
30 Days endpoint
P=068 P=100P=017
P=014
Theldquohigh riskrdquo patient
126
7260
192
72
120
24
60
0
5
10
15
20
25
Death Stroke MI MAE
CEA (n=167)Stent (n=167)
SAPPHIRE CAS vs CEA
1 year results
P=014
P=083P=017
P=010
CEA can be performed in high-risk patients with acceptable standard complication rates
Mozes G et al Semin Vasc Surg 20051861ndash 8
octogenarians
121121
30-day stroke and death rate30-day stroke and death rate
5353 1313
Agegt80yAgegt80y Age 70-79yAge 70-79y Age 60-69Age 60-69
Is CAS safe in this subgroup
The CREST trial lead-in phase
Material - Methodsbull 67 monthsbull 520 patientsbull mean age 76 range 56-85bull 364 male (70) 156 female (30)bull mean follow-up was 32 months (range 1 ndash 54 months)
Retrospective study
bull We conducted a retrospective review of CAS from 2003 to 2008bull RX Acculink - RX Accunet carotid system (Guidant Abott)
Material - Methods
bull Symptomatic (stroke (135) TIA Fugax) 515
bull Asymptomatic 485
Results within early follow-up (lt30 days)
bull Mortality (09)Stroke (11)TIA (13)Non fatal MI (13)
MAE 46
Results within early follow-up (lt30 days)
Predictors of adverse outcomes includedbullAge gt80bullsymptomatic patientsbullFemale genderbullpredilation prior to CPD bullplacement of multiple stentsbullContralateral occlusionbullUnfavorable anatomy
Late Follow-Up (gt30 days)
bull Mortality (173 )Stroke (07)Restenosis gt70 (23)
Mean follow-up was 32 months (range 1 ndash 60 months) 46 (88) patients lost of FU
Conclusion
bullCAS within experienced hands can be highly efficient and durable
Acculink Accunet system is safe and effective for CAS
ConclusionsCEA is the goal standard when
bull specific carotid anatomy
bullExtensive arch and carotid bif calcification
bullAccess related problems
bullFresh thrombus at ICA lesion
bullldquoString signrdquo morphology
bullVery low GSM
Conclusions
CAS and CEA are not competitive procedures but powerful treatment options tailored on different groups of patients
The gold standard is the experienced vascular team able to twist between endovascular and open surgical options in order to achieve the best treatment for the patient
Thank you for your attention
- Slide 1
- Slide 2
- Slide 3
- Slide 4
- Slide 5
- Slide 6
- Slide 7
- Slide 8
- Slide 9
- Slide 10
- Slide 11
- Slide 12
- Slide 13
- Slide 14
- Slide 15
- Slide 16
- Slide 17
- Slide 18
- Slide 19
- Slide 20
- Slide 21
- Slide 22
- Slide 23
- Slide 24
- Slide 25
- Slide 26
- Slide 27
- Slide 28
- Slide 29
- Slide 30
- Slide 31
- Slide 32
- Slide 33
- Slide 34
- Slide 35
- Slide 36
- Slide 37
- Slide 38
- Slide 39
- Slide 40
-
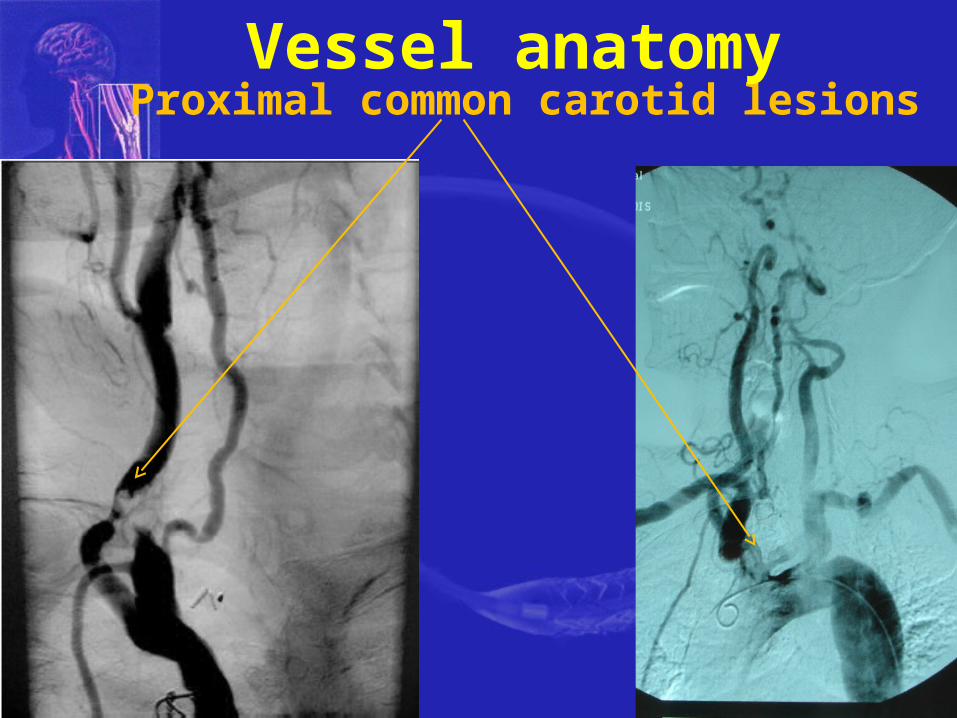
Proximal common carotid lesionsVessel anatomy
Tortuous CCA or ICA coil
Vessel anatomy
ldquoString signrdquo carotid morphology
Would you advance an EPD into such a vessel
Vessel anatomy
Defining patient groups that either CEA or CAS is beneficial
Vessel anatomyPlaque characteristics
The high risk patient
Plaque characteristics
Biasi et al ICAROS study Circulation 2004110756-62Fisher M et al Stroke 200536253ndash7Rothwell PM et al Stroke 200031615ndash21
bullGSMlt25 is related with a higher risk of neurologic complications after CASbulllow GSM is not a contraindication to CAS but rather a predictor of increased stroke riskbullLow GSM values are further related to future coronary events and higher rate of restenosis
Defining patient groups that either CEA or CAS is beneficial
Vessel anatomy Plaque characteristics
The high risk patient
24 30
60
96
12
3624
48
0
5
10
15
20
25
Death Stroke MI MAE
CEA (n=167)
Stent (n=167)
30 Days endpoint
P=068 P=100P=017
P=014
Theldquohigh riskrdquo patient
126
7260
192
72
120
24
60
0
5
10
15
20
25
Death Stroke MI MAE
CEA (n=167)Stent (n=167)
SAPPHIRE CAS vs CEA
1 year results
P=014
P=083P=017
P=010
CEA can be performed in high-risk patients with acceptable standard complication rates
Mozes G et al Semin Vasc Surg 20051861ndash 8
octogenarians
121121
30-day stroke and death rate30-day stroke and death rate
5353 1313
Agegt80yAgegt80y Age 70-79yAge 70-79y Age 60-69Age 60-69
Is CAS safe in this subgroup
The CREST trial lead-in phase
Material - Methodsbull 67 monthsbull 520 patientsbull mean age 76 range 56-85bull 364 male (70) 156 female (30)bull mean follow-up was 32 months (range 1 ndash 54 months)
Retrospective study
bull We conducted a retrospective review of CAS from 2003 to 2008bull RX Acculink - RX Accunet carotid system (Guidant Abott)
Material - Methods
bull Symptomatic (stroke (135) TIA Fugax) 515
bull Asymptomatic 485
Results within early follow-up (lt30 days)
bull Mortality (09)Stroke (11)TIA (13)Non fatal MI (13)
MAE 46
Results within early follow-up (lt30 days)
Predictors of adverse outcomes includedbullAge gt80bullsymptomatic patientsbullFemale genderbullpredilation prior to CPD bullplacement of multiple stentsbullContralateral occlusionbullUnfavorable anatomy
Late Follow-Up (gt30 days)
bull Mortality (173 )Stroke (07)Restenosis gt70 (23)
Mean follow-up was 32 months (range 1 ndash 60 months) 46 (88) patients lost of FU
Conclusion
bullCAS within experienced hands can be highly efficient and durable
Acculink Accunet system is safe and effective for CAS
ConclusionsCEA is the goal standard when
bull specific carotid anatomy
bullExtensive arch and carotid bif calcification
bullAccess related problems
bullFresh thrombus at ICA lesion
bullldquoString signrdquo morphology
bullVery low GSM
Conclusions
CAS and CEA are not competitive procedures but powerful treatment options tailored on different groups of patients
The gold standard is the experienced vascular team able to twist between endovascular and open surgical options in order to achieve the best treatment for the patient
Thank you for your attention
- Slide 1
- Slide 2
- Slide 3
- Slide 4
- Slide 5
- Slide 6
- Slide 7
- Slide 8
- Slide 9
- Slide 10
- Slide 11
- Slide 12
- Slide 13
- Slide 14
- Slide 15
- Slide 16
- Slide 17
- Slide 18
- Slide 19
- Slide 20
- Slide 21
- Slide 22
- Slide 23
- Slide 24
- Slide 25
- Slide 26
- Slide 27
- Slide 28
- Slide 29
- Slide 30
- Slide 31
- Slide 32
- Slide 33
- Slide 34
- Slide 35
- Slide 36
- Slide 37
- Slide 38
- Slide 39
- Slide 40
-
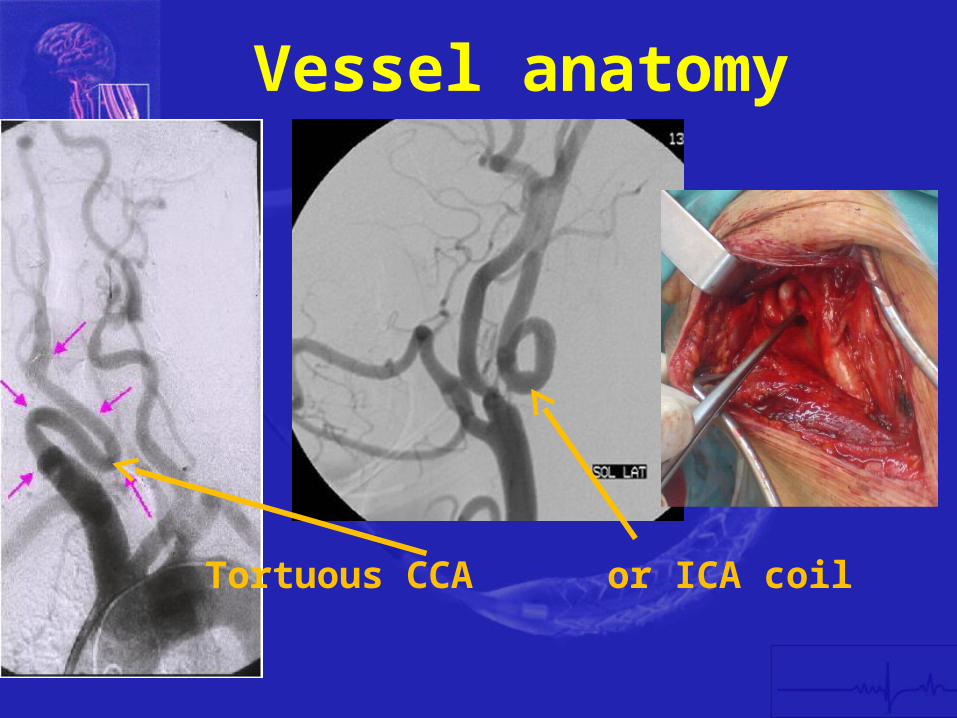
Tortuous CCA or ICA coil
Vessel anatomy
ldquoString signrdquo carotid morphology
Would you advance an EPD into such a vessel
Vessel anatomy
Defining patient groups that either CEA or CAS is beneficial
Vessel anatomyPlaque characteristics
The high risk patient
Plaque characteristics
Biasi et al ICAROS study Circulation 2004110756-62Fisher M et al Stroke 200536253ndash7Rothwell PM et al Stroke 200031615ndash21
bullGSMlt25 is related with a higher risk of neurologic complications after CASbulllow GSM is not a contraindication to CAS but rather a predictor of increased stroke riskbullLow GSM values are further related to future coronary events and higher rate of restenosis
Defining patient groups that either CEA or CAS is beneficial
Vessel anatomy Plaque characteristics
The high risk patient
24 30
60
96
12
3624
48
0
5
10
15
20
25
Death Stroke MI MAE
CEA (n=167)
Stent (n=167)
30 Days endpoint
P=068 P=100P=017
P=014
Theldquohigh riskrdquo patient
126
7260
192
72
120
24
60
0
5
10
15
20
25
Death Stroke MI MAE
CEA (n=167)Stent (n=167)
SAPPHIRE CAS vs CEA
1 year results
P=014
P=083P=017
P=010
CEA can be performed in high-risk patients with acceptable standard complication rates
Mozes G et al Semin Vasc Surg 20051861ndash 8
octogenarians
121121
30-day stroke and death rate30-day stroke and death rate
5353 1313
Agegt80yAgegt80y Age 70-79yAge 70-79y Age 60-69Age 60-69
Is CAS safe in this subgroup
The CREST trial lead-in phase
Material - Methodsbull 67 monthsbull 520 patientsbull mean age 76 range 56-85bull 364 male (70) 156 female (30)bull mean follow-up was 32 months (range 1 ndash 54 months)
Retrospective study
bull We conducted a retrospective review of CAS from 2003 to 2008bull RX Acculink - RX Accunet carotid system (Guidant Abott)
Material - Methods
bull Symptomatic (stroke (135) TIA Fugax) 515
bull Asymptomatic 485
Results within early follow-up (lt30 days)
bull Mortality (09)Stroke (11)TIA (13)Non fatal MI (13)
MAE 46
Results within early follow-up (lt30 days)
Predictors of adverse outcomes includedbullAge gt80bullsymptomatic patientsbullFemale genderbullpredilation prior to CPD bullplacement of multiple stentsbullContralateral occlusionbullUnfavorable anatomy
Late Follow-Up (gt30 days)
bull Mortality (173 )Stroke (07)Restenosis gt70 (23)
Mean follow-up was 32 months (range 1 ndash 60 months) 46 (88) patients lost of FU
Conclusion
bullCAS within experienced hands can be highly efficient and durable
Acculink Accunet system is safe and effective for CAS
ConclusionsCEA is the goal standard when
bull specific carotid anatomy
bullExtensive arch and carotid bif calcification
bullAccess related problems
bullFresh thrombus at ICA lesion
bullldquoString signrdquo morphology
bullVery low GSM
Conclusions
CAS and CEA are not competitive procedures but powerful treatment options tailored on different groups of patients
The gold standard is the experienced vascular team able to twist between endovascular and open surgical options in order to achieve the best treatment for the patient
Thank you for your attention
- Slide 1
- Slide 2
- Slide 3
- Slide 4
- Slide 5
- Slide 6
- Slide 7
- Slide 8
- Slide 9
- Slide 10
- Slide 11
- Slide 12
- Slide 13
- Slide 14
- Slide 15
- Slide 16
- Slide 17
- Slide 18
- Slide 19
- Slide 20
- Slide 21
- Slide 22
- Slide 23
- Slide 24
- Slide 25
- Slide 26
- Slide 27
- Slide 28
- Slide 29
- Slide 30
- Slide 31
- Slide 32
- Slide 33
- Slide 34
- Slide 35
- Slide 36
- Slide 37
- Slide 38
- Slide 39
- Slide 40
-
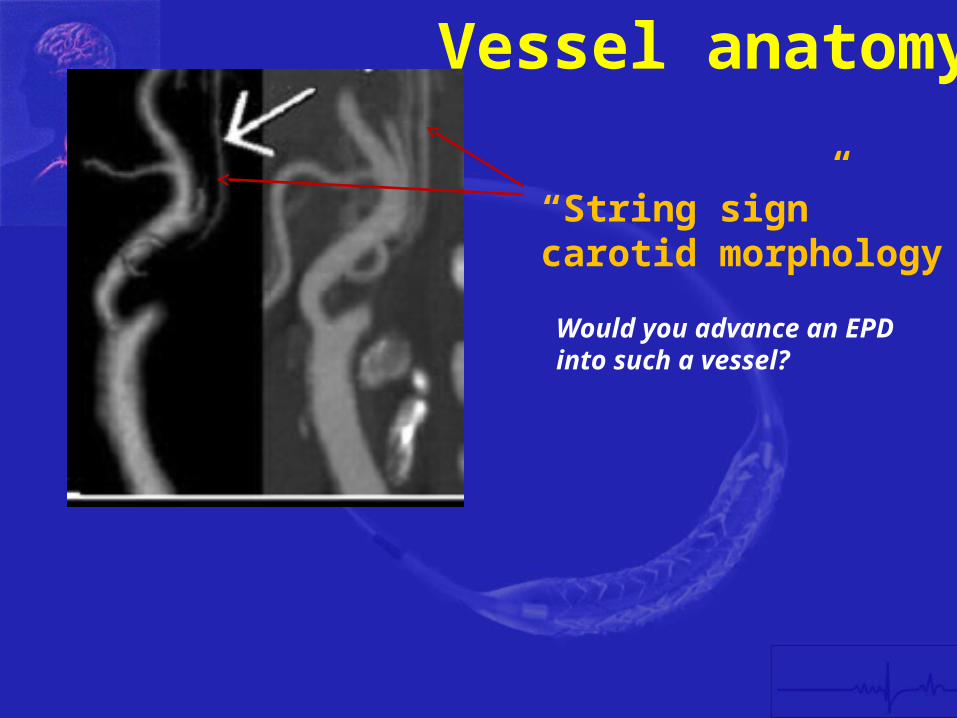
ldquoString signrdquo carotid morphology
Would you advance an EPD into such a vessel
Vessel anatomy
Defining patient groups that either CEA or CAS is beneficial
Vessel anatomyPlaque characteristics
The high risk patient
Plaque characteristics
Biasi et al ICAROS study Circulation 2004110756-62Fisher M et al Stroke 200536253ndash7Rothwell PM et al Stroke 200031615ndash21
bullGSMlt25 is related with a higher risk of neurologic complications after CASbulllow GSM is not a contraindication to CAS but rather a predictor of increased stroke riskbullLow GSM values are further related to future coronary events and higher rate of restenosis
Defining patient groups that either CEA or CAS is beneficial
Vessel anatomy Plaque characteristics
The high risk patient
24 30
60
96
12
3624
48
0
5
10
15
20
25
Death Stroke MI MAE
CEA (n=167)
Stent (n=167)
30 Days endpoint
P=068 P=100P=017
P=014
Theldquohigh riskrdquo patient
126
7260
192
72
120
24
60
0
5
10
15
20
25
Death Stroke MI MAE
CEA (n=167)Stent (n=167)
SAPPHIRE CAS vs CEA
1 year results
P=014
P=083P=017
P=010
CEA can be performed in high-risk patients with acceptable standard complication rates
Mozes G et al Semin Vasc Surg 20051861ndash 8
octogenarians
121121
30-day stroke and death rate30-day stroke and death rate
5353 1313
Agegt80yAgegt80y Age 70-79yAge 70-79y Age 60-69Age 60-69
Is CAS safe in this subgroup
The CREST trial lead-in phase
Material - Methodsbull 67 monthsbull 520 patientsbull mean age 76 range 56-85bull 364 male (70) 156 female (30)bull mean follow-up was 32 months (range 1 ndash 54 months)
Retrospective study
bull We conducted a retrospective review of CAS from 2003 to 2008bull RX Acculink - RX Accunet carotid system (Guidant Abott)
Material - Methods
bull Symptomatic (stroke (135) TIA Fugax) 515
bull Asymptomatic 485
Results within early follow-up (lt30 days)
bull Mortality (09)Stroke (11)TIA (13)Non fatal MI (13)
MAE 46
Results within early follow-up (lt30 days)
Predictors of adverse outcomes includedbullAge gt80bullsymptomatic patientsbullFemale genderbullpredilation prior to CPD bullplacement of multiple stentsbullContralateral occlusionbullUnfavorable anatomy
Late Follow-Up (gt30 days)
bull Mortality (173 )Stroke (07)Restenosis gt70 (23)
Mean follow-up was 32 months (range 1 ndash 60 months) 46 (88) patients lost of FU
Conclusion
bullCAS within experienced hands can be highly efficient and durable
Acculink Accunet system is safe and effective for CAS
ConclusionsCEA is the goal standard when
bull specific carotid anatomy
bullExtensive arch and carotid bif calcification
bullAccess related problems
bullFresh thrombus at ICA lesion
bullldquoString signrdquo morphology
bullVery low GSM
Conclusions
CAS and CEA are not competitive procedures but powerful treatment options tailored on different groups of patients
The gold standard is the experienced vascular team able to twist between endovascular and open surgical options in order to achieve the best treatment for the patient
Thank you for your attention
- Slide 1
- Slide 2
- Slide 3
- Slide 4
- Slide 5
- Slide 6
- Slide 7
- Slide 8
- Slide 9
- Slide 10
- Slide 11
- Slide 12
- Slide 13
- Slide 14
- Slide 15
- Slide 16
- Slide 17
- Slide 18
- Slide 19
- Slide 20
- Slide 21
- Slide 22
- Slide 23
- Slide 24
- Slide 25
- Slide 26
- Slide 27
- Slide 28
- Slide 29
- Slide 30
- Slide 31
- Slide 32
- Slide 33
- Slide 34
- Slide 35
- Slide 36
- Slide 37
- Slide 38
- Slide 39
- Slide 40
-
Defining patient groups that either CEA or CAS is beneficial
Vessel anatomyPlaque characteristics
The high risk patient
Plaque characteristics
Biasi et al ICAROS study Circulation 2004110756-62Fisher M et al Stroke 200536253ndash7Rothwell PM et al Stroke 200031615ndash21
bullGSMlt25 is related with a higher risk of neurologic complications after CASbulllow GSM is not a contraindication to CAS but rather a predictor of increased stroke riskbullLow GSM values are further related to future coronary events and higher rate of restenosis
Defining patient groups that either CEA or CAS is beneficial
Vessel anatomy Plaque characteristics
The high risk patient
24 30
60
96
12
3624
48
0
5
10
15
20
25
Death Stroke MI MAE
CEA (n=167)
Stent (n=167)
30 Days endpoint
P=068 P=100P=017
P=014
Theldquohigh riskrdquo patient
126
7260
192
72
120
24
60
0
5
10
15
20
25
Death Stroke MI MAE
CEA (n=167)Stent (n=167)
SAPPHIRE CAS vs CEA
1 year results
P=014
P=083P=017
P=010
CEA can be performed in high-risk patients with acceptable standard complication rates
Mozes G et al Semin Vasc Surg 20051861ndash 8
octogenarians
121121
30-day stroke and death rate30-day stroke and death rate
5353 1313
Agegt80yAgegt80y Age 70-79yAge 70-79y Age 60-69Age 60-69
Is CAS safe in this subgroup
The CREST trial lead-in phase
Material - Methodsbull 67 monthsbull 520 patientsbull mean age 76 range 56-85bull 364 male (70) 156 female (30)bull mean follow-up was 32 months (range 1 ndash 54 months)
Retrospective study
bull We conducted a retrospective review of CAS from 2003 to 2008bull RX Acculink - RX Accunet carotid system (Guidant Abott)
Material - Methods
bull Symptomatic (stroke (135) TIA Fugax) 515
bull Asymptomatic 485
Results within early follow-up (lt30 days)
bull Mortality (09)Stroke (11)TIA (13)Non fatal MI (13)
MAE 46
Results within early follow-up (lt30 days)
Predictors of adverse outcomes includedbullAge gt80bullsymptomatic patientsbullFemale genderbullpredilation prior to CPD bullplacement of multiple stentsbullContralateral occlusionbullUnfavorable anatomy
Late Follow-Up (gt30 days)
bull Mortality (173 )Stroke (07)Restenosis gt70 (23)
Mean follow-up was 32 months (range 1 ndash 60 months) 46 (88) patients lost of FU
Conclusion
bullCAS within experienced hands can be highly efficient and durable
Acculink Accunet system is safe and effective for CAS
ConclusionsCEA is the goal standard when
bull specific carotid anatomy
bullExtensive arch and carotid bif calcification
bullAccess related problems
bullFresh thrombus at ICA lesion
bullldquoString signrdquo morphology
bullVery low GSM
Conclusions
CAS and CEA are not competitive procedures but powerful treatment options tailored on different groups of patients
The gold standard is the experienced vascular team able to twist between endovascular and open surgical options in order to achieve the best treatment for the patient
Thank you for your attention
- Slide 1
- Slide 2
- Slide 3
- Slide 4
- Slide 5
- Slide 6
- Slide 7
- Slide 8
- Slide 9
- Slide 10
- Slide 11
- Slide 12
- Slide 13
- Slide 14
- Slide 15
- Slide 16
- Slide 17
- Slide 18
- Slide 19
- Slide 20
- Slide 21
- Slide 22
- Slide 23
- Slide 24
- Slide 25
- Slide 26
- Slide 27
- Slide 28
- Slide 29
- Slide 30
- Slide 31
- Slide 32
- Slide 33
- Slide 34
- Slide 35
- Slide 36
- Slide 37
- Slide 38
- Slide 39
- Slide 40
-
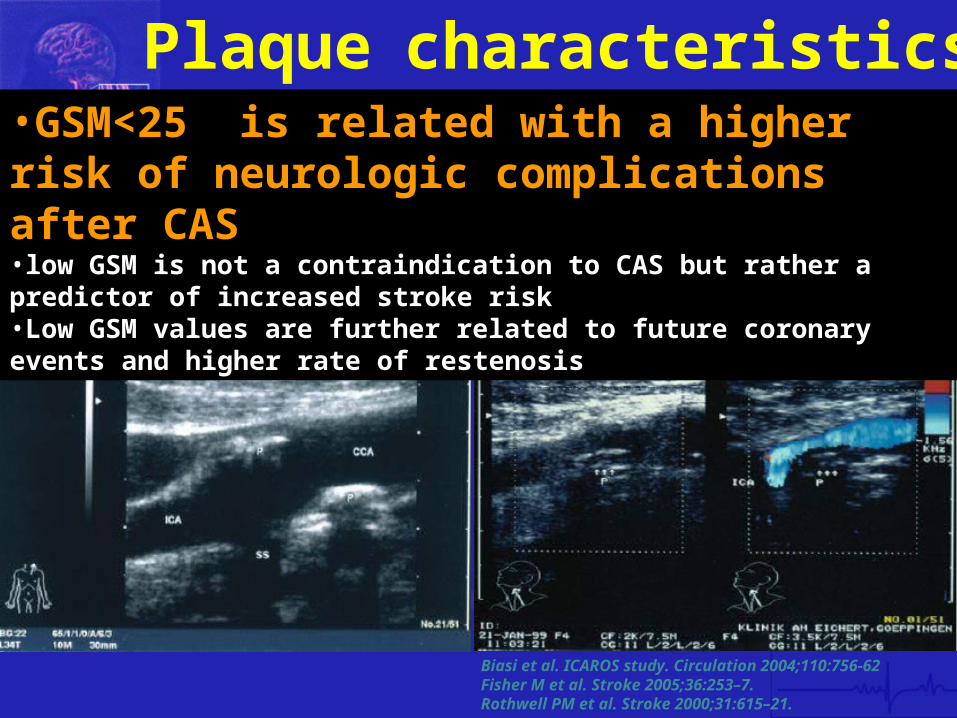
Plaque characteristics
Biasi et al ICAROS study Circulation 2004110756-62Fisher M et al Stroke 200536253ndash7Rothwell PM et al Stroke 200031615ndash21
bullGSMlt25 is related with a higher risk of neurologic complications after CASbulllow GSM is not a contraindication to CAS but rather a predictor of increased stroke riskbullLow GSM values are further related to future coronary events and higher rate of restenosis
Defining patient groups that either CEA or CAS is beneficial
Vessel anatomy Plaque characteristics
The high risk patient
24 30
60
96
12
3624
48
0
5
10
15
20
25
Death Stroke MI MAE
CEA (n=167)
Stent (n=167)
30 Days endpoint
P=068 P=100P=017
P=014
Theldquohigh riskrdquo patient
126
7260
192
72
120
24
60
0
5
10
15
20
25
Death Stroke MI MAE
CEA (n=167)Stent (n=167)
SAPPHIRE CAS vs CEA
1 year results
P=014
P=083P=017
P=010
CEA can be performed in high-risk patients with acceptable standard complication rates
Mozes G et al Semin Vasc Surg 20051861ndash 8
octogenarians
121121
30-day stroke and death rate30-day stroke and death rate
5353 1313
Agegt80yAgegt80y Age 70-79yAge 70-79y Age 60-69Age 60-69
Is CAS safe in this subgroup
The CREST trial lead-in phase
Material - Methodsbull 67 monthsbull 520 patientsbull mean age 76 range 56-85bull 364 male (70) 156 female (30)bull mean follow-up was 32 months (range 1 ndash 54 months)
Retrospective study
bull We conducted a retrospective review of CAS from 2003 to 2008bull RX Acculink - RX Accunet carotid system (Guidant Abott)
Material - Methods
bull Symptomatic (stroke (135) TIA Fugax) 515
bull Asymptomatic 485
Results within early follow-up (lt30 days)
bull Mortality (09)Stroke (11)TIA (13)Non fatal MI (13)
MAE 46
Results within early follow-up (lt30 days)
Predictors of adverse outcomes includedbullAge gt80bullsymptomatic patientsbullFemale genderbullpredilation prior to CPD bullplacement of multiple stentsbullContralateral occlusionbullUnfavorable anatomy
Late Follow-Up (gt30 days)
bull Mortality (173 )Stroke (07)Restenosis gt70 (23)
Mean follow-up was 32 months (range 1 ndash 60 months) 46 (88) patients lost of FU
Conclusion
bullCAS within experienced hands can be highly efficient and durable
Acculink Accunet system is safe and effective for CAS
ConclusionsCEA is the goal standard when
bull specific carotid anatomy
bullExtensive arch and carotid bif calcification
bullAccess related problems
bullFresh thrombus at ICA lesion
bullldquoString signrdquo morphology
bullVery low GSM
Conclusions
CAS and CEA are not competitive procedures but powerful treatment options tailored on different groups of patients
The gold standard is the experienced vascular team able to twist between endovascular and open surgical options in order to achieve the best treatment for the patient
Thank you for your attention
- Slide 1
- Slide 2
- Slide 3
- Slide 4
- Slide 5
- Slide 6
- Slide 7
- Slide 8
- Slide 9
- Slide 10
- Slide 11
- Slide 12
- Slide 13
- Slide 14
- Slide 15
- Slide 16
- Slide 17
- Slide 18
- Slide 19
- Slide 20
- Slide 21
- Slide 22
- Slide 23
- Slide 24
- Slide 25
- Slide 26
- Slide 27
- Slide 28
- Slide 29
- Slide 30
- Slide 31
- Slide 32
- Slide 33
- Slide 34
- Slide 35
- Slide 36
- Slide 37
- Slide 38
- Slide 39
- Slide 40
-
Defining patient groups that either CEA or CAS is beneficial
Vessel anatomy Plaque characteristics
The high risk patient
24 30
60
96
12
3624
48
0
5
10
15
20
25
Death Stroke MI MAE
CEA (n=167)
Stent (n=167)
30 Days endpoint
P=068 P=100P=017
P=014
Theldquohigh riskrdquo patient
126
7260
192
72
120
24
60
0
5
10
15
20
25
Death Stroke MI MAE
CEA (n=167)Stent (n=167)
SAPPHIRE CAS vs CEA
1 year results
P=014
P=083P=017
P=010
CEA can be performed in high-risk patients with acceptable standard complication rates
Mozes G et al Semin Vasc Surg 20051861ndash 8
octogenarians
121121
30-day stroke and death rate30-day stroke and death rate
5353 1313
Agegt80yAgegt80y Age 70-79yAge 70-79y Age 60-69Age 60-69
Is CAS safe in this subgroup
The CREST trial lead-in phase
Material - Methodsbull 67 monthsbull 520 patientsbull mean age 76 range 56-85bull 364 male (70) 156 female (30)bull mean follow-up was 32 months (range 1 ndash 54 months)
Retrospective study
bull We conducted a retrospective review of CAS from 2003 to 2008bull RX Acculink - RX Accunet carotid system (Guidant Abott)
Material - Methods
bull Symptomatic (stroke (135) TIA Fugax) 515
bull Asymptomatic 485
Results within early follow-up (lt30 days)
bull Mortality (09)Stroke (11)TIA (13)Non fatal MI (13)
MAE 46
Results within early follow-up (lt30 days)
Predictors of adverse outcomes includedbullAge gt80bullsymptomatic patientsbullFemale genderbullpredilation prior to CPD bullplacement of multiple stentsbullContralateral occlusionbullUnfavorable anatomy
Late Follow-Up (gt30 days)
bull Mortality (173 )Stroke (07)Restenosis gt70 (23)
Mean follow-up was 32 months (range 1 ndash 60 months) 46 (88) patients lost of FU
Conclusion
bullCAS within experienced hands can be highly efficient and durable
Acculink Accunet system is safe and effective for CAS
ConclusionsCEA is the goal standard when
bull specific carotid anatomy
bullExtensive arch and carotid bif calcification
bullAccess related problems
bullFresh thrombus at ICA lesion
bullldquoString signrdquo morphology
bullVery low GSM
Conclusions
CAS and CEA are not competitive procedures but powerful treatment options tailored on different groups of patients
The gold standard is the experienced vascular team able to twist between endovascular and open surgical options in order to achieve the best treatment for the patient
Thank you for your attention
- Slide 1
- Slide 2
- Slide 3
- Slide 4
- Slide 5
- Slide 6
- Slide 7
- Slide 8
- Slide 9
- Slide 10
- Slide 11
- Slide 12
- Slide 13
- Slide 14
- Slide 15
- Slide 16
- Slide 17
- Slide 18
- Slide 19
- Slide 20
- Slide 21
- Slide 22
- Slide 23
- Slide 24
- Slide 25
- Slide 26
- Slide 27
- Slide 28
- Slide 29
- Slide 30
- Slide 31
- Slide 32
- Slide 33
- Slide 34
- Slide 35
- Slide 36
- Slide 37
- Slide 38
- Slide 39
- Slide 40
-
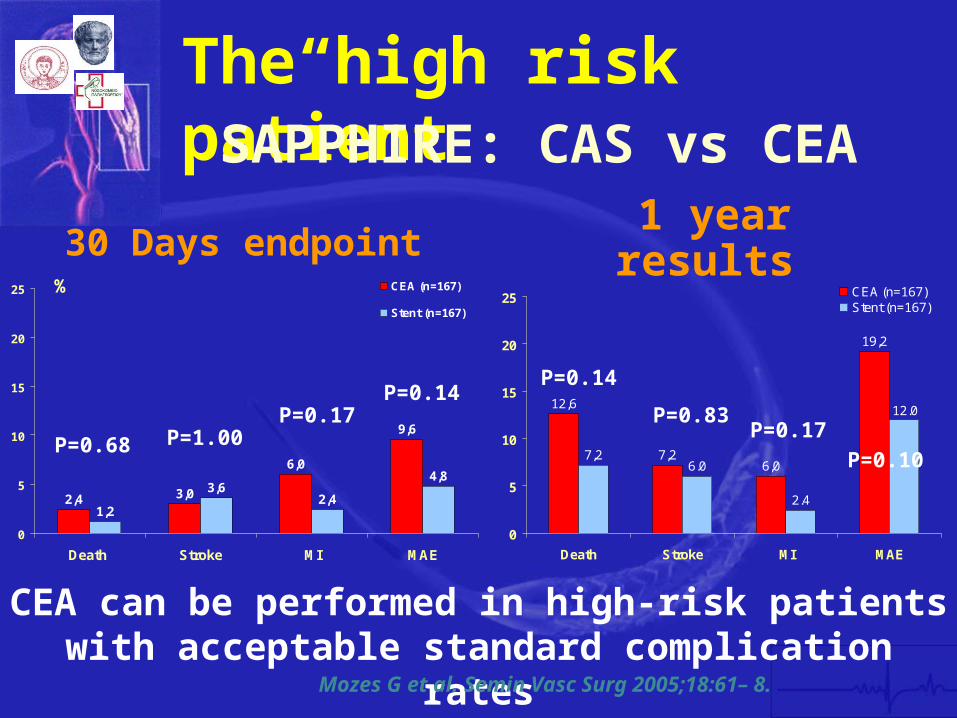
24 30
60
96
12
3624
48
0
5
10
15
20
25
Death Stroke MI MAE
CEA (n=167)
Stent (n=167)
30 Days endpoint
P=068 P=100P=017
P=014
Theldquohigh riskrdquo patient
126
7260
192
72
120
24
60
0
5
10
15
20
25
Death Stroke MI MAE
CEA (n=167)Stent (n=167)
SAPPHIRE CAS vs CEA
1 year results
P=014
P=083P=017
P=010
CEA can be performed in high-risk patients with acceptable standard complication rates
Mozes G et al Semin Vasc Surg 20051861ndash 8
octogenarians
121121
30-day stroke and death rate30-day stroke and death rate
5353 1313
Agegt80yAgegt80y Age 70-79yAge 70-79y Age 60-69Age 60-69
Is CAS safe in this subgroup
The CREST trial lead-in phase
Material - Methodsbull 67 monthsbull 520 patientsbull mean age 76 range 56-85bull 364 male (70) 156 female (30)bull mean follow-up was 32 months (range 1 ndash 54 months)
Retrospective study
bull We conducted a retrospective review of CAS from 2003 to 2008bull RX Acculink - RX Accunet carotid system (Guidant Abott)
Material - Methods
bull Symptomatic (stroke (135) TIA Fugax) 515
bull Asymptomatic 485
Results within early follow-up (lt30 days)
bull Mortality (09)Stroke (11)TIA (13)Non fatal MI (13)
MAE 46
Results within early follow-up (lt30 days)
Predictors of adverse outcomes includedbullAge gt80bullsymptomatic patientsbullFemale genderbullpredilation prior to CPD bullplacement of multiple stentsbullContralateral occlusionbullUnfavorable anatomy
Late Follow-Up (gt30 days)
bull Mortality (173 )Stroke (07)Restenosis gt70 (23)
Mean follow-up was 32 months (range 1 ndash 60 months) 46 (88) patients lost of FU
Conclusion
bullCAS within experienced hands can be highly efficient and durable
Acculink Accunet system is safe and effective for CAS
ConclusionsCEA is the goal standard when
bull specific carotid anatomy
bullExtensive arch and carotid bif calcification
bullAccess related problems
bullFresh thrombus at ICA lesion
bullldquoString signrdquo morphology
bullVery low GSM
Conclusions
CAS and CEA are not competitive procedures but powerful treatment options tailored on different groups of patients
The gold standard is the experienced vascular team able to twist between endovascular and open surgical options in order to achieve the best treatment for the patient
Thank you for your attention
- Slide 1
- Slide 2
- Slide 3
- Slide 4
- Slide 5
- Slide 6
- Slide 7
- Slide 8
- Slide 9
- Slide 10
- Slide 11
- Slide 12
- Slide 13
- Slide 14
- Slide 15
- Slide 16
- Slide 17
- Slide 18
- Slide 19
- Slide 20
- Slide 21
- Slide 22
- Slide 23
- Slide 24
- Slide 25
- Slide 26
- Slide 27
- Slide 28
- Slide 29
- Slide 30
- Slide 31
- Slide 32
- Slide 33
- Slide 34
- Slide 35
- Slide 36
- Slide 37
- Slide 38
- Slide 39
- Slide 40
-
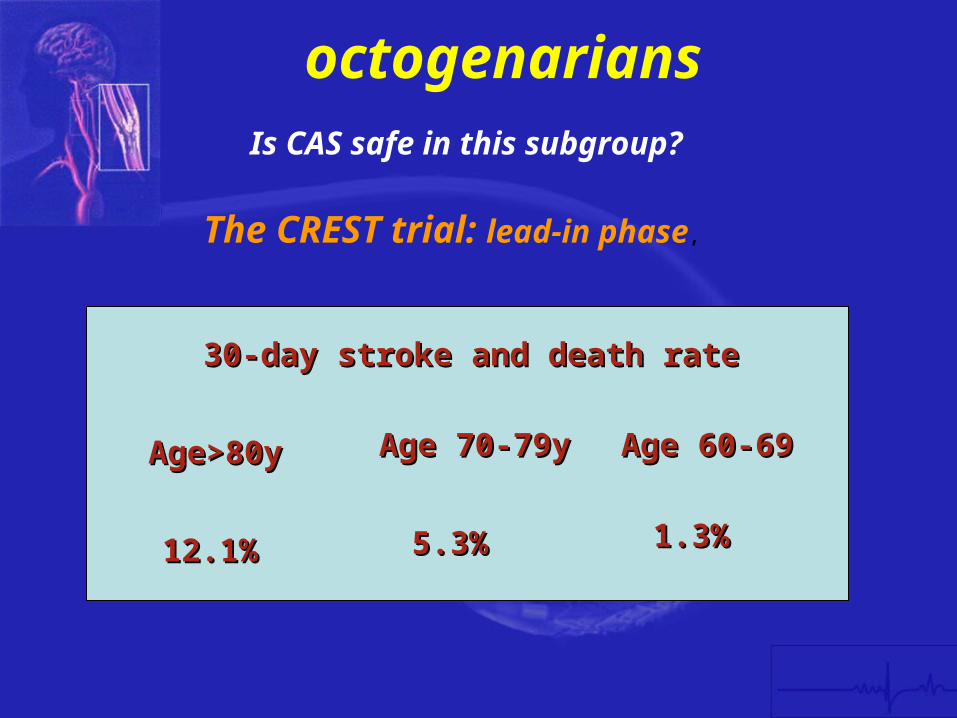
octogenarians
121121
30-day stroke and death rate30-day stroke and death rate
5353 1313
Agegt80yAgegt80y Age 70-79yAge 70-79y Age 60-69Age 60-69
Is CAS safe in this subgroup
The CREST trial lead-in phase
Material - Methodsbull 67 monthsbull 520 patientsbull mean age 76 range 56-85bull 364 male (70) 156 female (30)bull mean follow-up was 32 months (range 1 ndash 54 months)
Retrospective study
bull We conducted a retrospective review of CAS from 2003 to 2008bull RX Acculink - RX Accunet carotid system (Guidant Abott)
Material - Methods
bull Symptomatic (stroke (135) TIA Fugax) 515
bull Asymptomatic 485
Results within early follow-up (lt30 days)
bull Mortality (09)Stroke (11)TIA (13)Non fatal MI (13)
MAE 46
Results within early follow-up (lt30 days)
Predictors of adverse outcomes includedbullAge gt80bullsymptomatic patientsbullFemale genderbullpredilation prior to CPD bullplacement of multiple stentsbullContralateral occlusionbullUnfavorable anatomy
Late Follow-Up (gt30 days)
bull Mortality (173 )Stroke (07)Restenosis gt70 (23)
Mean follow-up was 32 months (range 1 ndash 60 months) 46 (88) patients lost of FU
Conclusion
bullCAS within experienced hands can be highly efficient and durable
Acculink Accunet system is safe and effective for CAS
ConclusionsCEA is the goal standard when
bull specific carotid anatomy
bullExtensive arch and carotid bif calcification
bullAccess related problems
bullFresh thrombus at ICA lesion
bullldquoString signrdquo morphology
bullVery low GSM
Conclusions
CAS and CEA are not competitive procedures but powerful treatment options tailored on different groups of patients
The gold standard is the experienced vascular team able to twist between endovascular and open surgical options in order to achieve the best treatment for the patient
Thank you for your attention
- Slide 1
- Slide 2
- Slide 3
- Slide 4
- Slide 5
- Slide 6
- Slide 7
- Slide 8
- Slide 9
- Slide 10
- Slide 11
- Slide 12
- Slide 13
- Slide 14
- Slide 15
- Slide 16
- Slide 17
- Slide 18
- Slide 19
- Slide 20
- Slide 21
- Slide 22
- Slide 23
- Slide 24
- Slide 25
- Slide 26
- Slide 27
- Slide 28
- Slide 29
- Slide 30
- Slide 31
- Slide 32
- Slide 33
- Slide 34
- Slide 35
- Slide 36
- Slide 37
- Slide 38
- Slide 39
- Slide 40
-
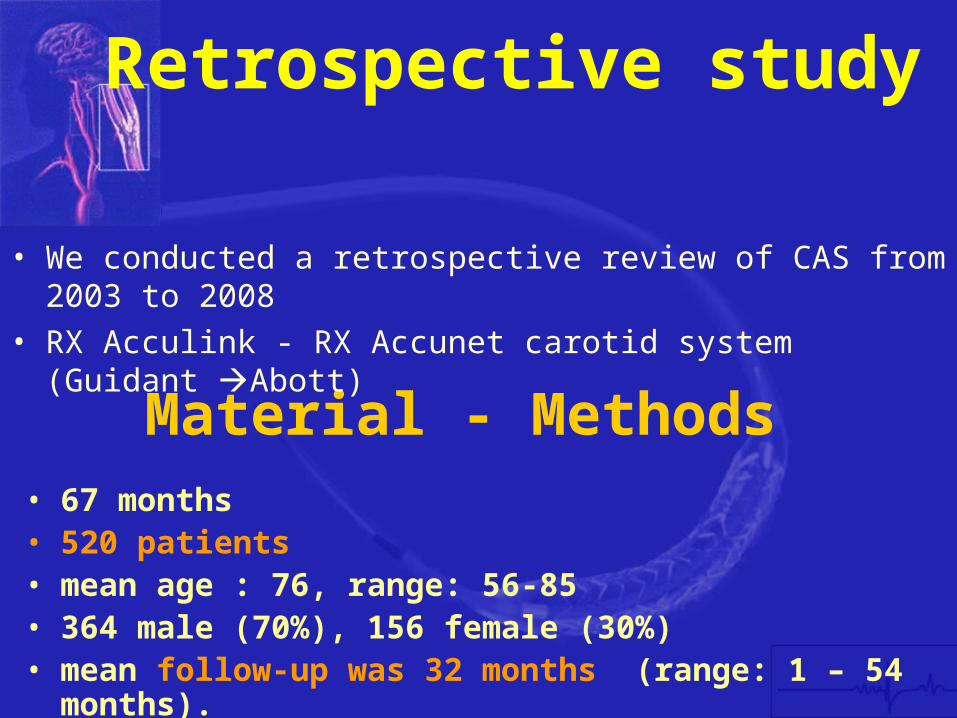
Material - Methodsbull 67 monthsbull 520 patientsbull mean age 76 range 56-85bull 364 male (70) 156 female (30)bull mean follow-up was 32 months (range 1 ndash 54 months)
Retrospective study
bull We conducted a retrospective review of CAS from 2003 to 2008bull RX Acculink - RX Accunet carotid system (Guidant Abott)
Material - Methods
bull Symptomatic (stroke (135) TIA Fugax) 515
bull Asymptomatic 485
Results within early follow-up (lt30 days)
bull Mortality (09)Stroke (11)TIA (13)Non fatal MI (13)
MAE 46
Results within early follow-up (lt30 days)
Predictors of adverse outcomes includedbullAge gt80bullsymptomatic patientsbullFemale genderbullpredilation prior to CPD bullplacement of multiple stentsbullContralateral occlusionbullUnfavorable anatomy
Late Follow-Up (gt30 days)
bull Mortality (173 )Stroke (07)Restenosis gt70 (23)
Mean follow-up was 32 months (range 1 ndash 60 months) 46 (88) patients lost of FU
Conclusion
bullCAS within experienced hands can be highly efficient and durable
Acculink Accunet system is safe and effective for CAS
ConclusionsCEA is the goal standard when
bull specific carotid anatomy
bullExtensive arch and carotid bif calcification
bullAccess related problems
bullFresh thrombus at ICA lesion
bullldquoString signrdquo morphology
bullVery low GSM
Conclusions
CAS and CEA are not competitive procedures but powerful treatment options tailored on different groups of patients
The gold standard is the experienced vascular team able to twist between endovascular and open surgical options in order to achieve the best treatment for the patient
Thank you for your attention
- Slide 1
- Slide 2
- Slide 3
- Slide 4
- Slide 5
- Slide 6
- Slide 7
- Slide 8
- Slide 9
- Slide 10
- Slide 11
- Slide 12
- Slide 13
- Slide 14
- Slide 15
- Slide 16
- Slide 17
- Slide 18
- Slide 19
- Slide 20
- Slide 21
- Slide 22
- Slide 23
- Slide 24
- Slide 25
- Slide 26
- Slide 27
- Slide 28
- Slide 29
- Slide 30
- Slide 31
- Slide 32
- Slide 33
- Slide 34
- Slide 35
- Slide 36
- Slide 37
- Slide 38
- Slide 39
- Slide 40
-
Material - Methods
bull Symptomatic (stroke (135) TIA Fugax) 515
bull Asymptomatic 485
Results within early follow-up (lt30 days)
bull Mortality (09)Stroke (11)TIA (13)Non fatal MI (13)
MAE 46
Results within early follow-up (lt30 days)
Predictors of adverse outcomes includedbullAge gt80bullsymptomatic patientsbullFemale genderbullpredilation prior to CPD bullplacement of multiple stentsbullContralateral occlusionbullUnfavorable anatomy
Late Follow-Up (gt30 days)
bull Mortality (173 )Stroke (07)Restenosis gt70 (23)
Mean follow-up was 32 months (range 1 ndash 60 months) 46 (88) patients lost of FU
Conclusion
bullCAS within experienced hands can be highly efficient and durable
Acculink Accunet system is safe and effective for CAS
ConclusionsCEA is the goal standard when
bull specific carotid anatomy
bullExtensive arch and carotid bif calcification
bullAccess related problems
bullFresh thrombus at ICA lesion
bullldquoString signrdquo morphology
bullVery low GSM
Conclusions
CAS and CEA are not competitive procedures but powerful treatment options tailored on different groups of patients
The gold standard is the experienced vascular team able to twist between endovascular and open surgical options in order to achieve the best treatment for the patient
Thank you for your attention
- Slide 1
- Slide 2
- Slide 3
- Slide 4
- Slide 5
- Slide 6
- Slide 7
- Slide 8
- Slide 9
- Slide 10
- Slide 11
- Slide 12
- Slide 13
- Slide 14
- Slide 15
- Slide 16
- Slide 17
- Slide 18
- Slide 19
- Slide 20
- Slide 21
- Slide 22
- Slide 23
- Slide 24
- Slide 25
- Slide 26
- Slide 27
- Slide 28
- Slide 29
- Slide 30
- Slide 31
- Slide 32
- Slide 33
- Slide 34
- Slide 35
- Slide 36
- Slide 37
- Slide 38
- Slide 39
- Slide 40
-
Results within early follow-up (lt30 days)
bull Mortality (09)Stroke (11)TIA (13)Non fatal MI (13)
MAE 46
Results within early follow-up (lt30 days)
Predictors of adverse outcomes includedbullAge gt80bullsymptomatic patientsbullFemale genderbullpredilation prior to CPD bullplacement of multiple stentsbullContralateral occlusionbullUnfavorable anatomy
Late Follow-Up (gt30 days)
bull Mortality (173 )Stroke (07)Restenosis gt70 (23)
Mean follow-up was 32 months (range 1 ndash 60 months) 46 (88) patients lost of FU
Conclusion
bullCAS within experienced hands can be highly efficient and durable
Acculink Accunet system is safe and effective for CAS
ConclusionsCEA is the goal standard when
bull specific carotid anatomy
bullExtensive arch and carotid bif calcification
bullAccess related problems
bullFresh thrombus at ICA lesion
bullldquoString signrdquo morphology
bullVery low GSM
Conclusions
CAS and CEA are not competitive procedures but powerful treatment options tailored on different groups of patients
The gold standard is the experienced vascular team able to twist between endovascular and open surgical options in order to achieve the best treatment for the patient
Thank you for your attention
- Slide 1
- Slide 2
- Slide 3
- Slide 4
- Slide 5
- Slide 6
- Slide 7
- Slide 8
- Slide 9
- Slide 10
- Slide 11
- Slide 12
- Slide 13
- Slide 14
- Slide 15
- Slide 16
- Slide 17
- Slide 18
- Slide 19
- Slide 20
- Slide 21
- Slide 22
- Slide 23
- Slide 24
- Slide 25
- Slide 26
- Slide 27
- Slide 28
- Slide 29
- Slide 30
- Slide 31
- Slide 32
- Slide 33
- Slide 34
- Slide 35
- Slide 36
- Slide 37
- Slide 38
- Slide 39
- Slide 40
-
Results within early follow-up (lt30 days)
Predictors of adverse outcomes includedbullAge gt80bullsymptomatic patientsbullFemale genderbullpredilation prior to CPD bullplacement of multiple stentsbullContralateral occlusionbullUnfavorable anatomy
Late Follow-Up (gt30 days)
bull Mortality (173 )Stroke (07)Restenosis gt70 (23)
Mean follow-up was 32 months (range 1 ndash 60 months) 46 (88) patients lost of FU
Conclusion
bullCAS within experienced hands can be highly efficient and durable
Acculink Accunet system is safe and effective for CAS
ConclusionsCEA is the goal standard when
bull specific carotid anatomy
bullExtensive arch and carotid bif calcification
bullAccess related problems
bullFresh thrombus at ICA lesion
bullldquoString signrdquo morphology
bullVery low GSM
Conclusions
CAS and CEA are not competitive procedures but powerful treatment options tailored on different groups of patients
The gold standard is the experienced vascular team able to twist between endovascular and open surgical options in order to achieve the best treatment for the patient
Thank you for your attention
- Slide 1
- Slide 2
- Slide 3
- Slide 4
- Slide 5
- Slide 6
- Slide 7
- Slide 8
- Slide 9
- Slide 10
- Slide 11
- Slide 12
- Slide 13
- Slide 14
- Slide 15
- Slide 16
- Slide 17
- Slide 18
- Slide 19
- Slide 20
- Slide 21
- Slide 22
- Slide 23
- Slide 24
- Slide 25
- Slide 26
- Slide 27
- Slide 28
- Slide 29
- Slide 30
- Slide 31
- Slide 32
- Slide 33
- Slide 34
- Slide 35
- Slide 36
- Slide 37
- Slide 38
- Slide 39
- Slide 40
-
Late Follow-Up (gt30 days)
bull Mortality (173 )Stroke (07)Restenosis gt70 (23)
Mean follow-up was 32 months (range 1 ndash 60 months) 46 (88) patients lost of FU
Conclusion
bullCAS within experienced hands can be highly efficient and durable
Acculink Accunet system is safe and effective for CAS
ConclusionsCEA is the goal standard when
bull specific carotid anatomy
bullExtensive arch and carotid bif calcification
bullAccess related problems
bullFresh thrombus at ICA lesion
bullldquoString signrdquo morphology
bullVery low GSM
Conclusions
CAS and CEA are not competitive procedures but powerful treatment options tailored on different groups of patients
The gold standard is the experienced vascular team able to twist between endovascular and open surgical options in order to achieve the best treatment for the patient
Thank you for your attention
- Slide 1
- Slide 2
- Slide 3
- Slide 4
- Slide 5
- Slide 6
- Slide 7
- Slide 8
- Slide 9
- Slide 10
- Slide 11
- Slide 12
- Slide 13
- Slide 14
- Slide 15
- Slide 16
- Slide 17
- Slide 18
- Slide 19
- Slide 20
- Slide 21
- Slide 22
- Slide 23
- Slide 24
- Slide 25
- Slide 26
- Slide 27
- Slide 28
- Slide 29
- Slide 30
- Slide 31
- Slide 32
- Slide 33
- Slide 34
- Slide 35
- Slide 36
- Slide 37
- Slide 38
- Slide 39
- Slide 40
-
Conclusion
bullCAS within experienced hands can be highly efficient and durable
Acculink Accunet system is safe and effective for CAS
ConclusionsCEA is the goal standard when
bull specific carotid anatomy
bullExtensive arch and carotid bif calcification
bullAccess related problems
bullFresh thrombus at ICA lesion
bullldquoString signrdquo morphology
bullVery low GSM
Conclusions
CAS and CEA are not competitive procedures but powerful treatment options tailored on different groups of patients
The gold standard is the experienced vascular team able to twist between endovascular and open surgical options in order to achieve the best treatment for the patient
Thank you for your attention
- Slide 1
- Slide 2
- Slide 3
- Slide 4
- Slide 5
- Slide 6
- Slide 7
- Slide 8
- Slide 9
- Slide 10
- Slide 11
- Slide 12
- Slide 13
- Slide 14
- Slide 15
- Slide 16
- Slide 17
- Slide 18
- Slide 19
- Slide 20
- Slide 21
- Slide 22
- Slide 23
- Slide 24
- Slide 25
- Slide 26
- Slide 27
- Slide 28
- Slide 29
- Slide 30
- Slide 31
- Slide 32
- Slide 33
- Slide 34
- Slide 35
- Slide 36
- Slide 37
- Slide 38
- Slide 39
- Slide 40
-
ConclusionsCEA is the goal standard when
bull specific carotid anatomy
bullExtensive arch and carotid bif calcification
bullAccess related problems
bullFresh thrombus at ICA lesion
bullldquoString signrdquo morphology
bullVery low GSM
Conclusions
CAS and CEA are not competitive procedures but powerful treatment options tailored on different groups of patients
The gold standard is the experienced vascular team able to twist between endovascular and open surgical options in order to achieve the best treatment for the patient
Thank you for your attention
- Slide 1
- Slide 2
- Slide 3
- Slide 4
- Slide 5
- Slide 6
- Slide 7
- Slide 8
- Slide 9
- Slide 10
- Slide 11
- Slide 12
- Slide 13
- Slide 14
- Slide 15
- Slide 16
- Slide 17
- Slide 18
- Slide 19
- Slide 20
- Slide 21
- Slide 22
- Slide 23
- Slide 24
- Slide 25
- Slide 26
- Slide 27
- Slide 28
- Slide 29
- Slide 30
- Slide 31
- Slide 32
- Slide 33
- Slide 34
- Slide 35
- Slide 36
- Slide 37
- Slide 38
- Slide 39
- Slide 40
-
Conclusions
CAS and CEA are not competitive procedures but powerful treatment options tailored on different groups of patients
The gold standard is the experienced vascular team able to twist between endovascular and open surgical options in order to achieve the best treatment for the patient
Thank you for your attention
- Slide 1
- Slide 2
- Slide 3
- Slide 4
- Slide 5
- Slide 6
- Slide 7
- Slide 8
- Slide 9
- Slide 10
- Slide 11
- Slide 12
- Slide 13
- Slide 14
- Slide 15
- Slide 16
- Slide 17
- Slide 18
- Slide 19
- Slide 20
- Slide 21
- Slide 22
- Slide 23
- Slide 24
- Slide 25
- Slide 26
- Slide 27
- Slide 28
- Slide 29
- Slide 30
- Slide 31
- Slide 32
- Slide 33
- Slide 34
- Slide 35
- Slide 36
- Slide 37
- Slide 38
- Slide 39
- Slide 40
-

Thank you for your attention
- Slide 1
- Slide 2
- Slide 3
- Slide 4
- Slide 5
- Slide 6
- Slide 7
- Slide 8
- Slide 9
- Slide 10
- Slide 11
- Slide 12
- Slide 13
- Slide 14
- Slide 15
- Slide 16
- Slide 17
- Slide 18
- Slide 19
- Slide 20
- Slide 21
- Slide 22
- Slide 23
- Slide 24
- Slide 25
- Slide 26
- Slide 27
- Slide 28
- Slide 29
- Slide 30
- Slide 31
- Slide 32
- Slide 33
- Slide 34
- Slide 35
- Slide 36
- Slide 37
- Slide 38
- Slide 39
- Slide 40
-