unresectability? an extraordinary case of tumor biology ... · license cc-by 3.0., which permits...
TRANSCRIPT

Received 11/17/2015 Review began 11/18/2015 Review ended 12/15/2015 Published 12/21/2015
© Copyright 2015Gaya et al. This is an open accessarticle distributed under the terms ofthe Creative Commons AttributionLicense CC-BY 3.0., which permitsunrestricted use, distribution, andreproduction in any medium,provided the original author andsource are credited.
Tumor Biology: Is It Time to RedefineUnresectability? An Extraordinary Case ofGastroesophageal JunctionalAdenocarcinomaAndy Gaya , Alex Giakoustidis , Mark Winslet , Satvinder Mudan
1. London Oncology Clinic, Guy's and St. Thomas' NHS Foundation Trust 2. Department of HPB Surgery,The Royal Marsden NHS Foundation Trust 3. Department of Surgery, Royal Free Hospital 4. Departmentof Academic Surgery, The Royal Marsden Hospital
Corresponding author: Andy Gaya, [email protected] Disclosures can be found in Additional Information at the end of the article
AbstractBackground: Disease assessment based on measurements of size and anatomic involvementhave historically been central to surgical strategy. We propose this to be an outdated concept,which should be replaced by a deeper understanding of tumor biology and careful treatmentplanning.
Report of case: A 34-year-old male was diagnosed with a Siewert Type 3 locally advancedcancer of the gastroesophageal junction, involving the coeliac axis and the superior mesentericartery (SMA). He was treated with neoadjuvant chemotherapy, followed by chemoradiation,and then proceeded to surgery, at which time the tumor was judged unresectable. Afterextensive planning, a further surgery was attempted - an extended gastrectomy with distalesophagectomy, left hepatectomy, and splenectomy were performed. Additionally, the coeliacaxis and the SMA were excised, followed by reconstruction of the hepatic artery and the SMAwith grafts. Adjuvant chemotherapy was administered, and the patient is recurrence-free afterfive years follow-up.
Conclusion: This case highlights the importance of the distinction between resectability andoperability, and that patient treatment should be tailored and individualised based on theresponse to treatment, comorbidities, and underlying tumor biology.
Categories: Radiation Oncology, Gastroenterology, OncologyKeywords: esophageal cancer, gastric cancer, radiotherapy, appleby procedure, surgical resection,surgical technique, chemotherapy, immunotherapy
IntroductionOver the past few decades, there has been a dramatic rise in the incidence of adenocarcinoma ofthe gastroesophageal junction (GEJ) in Western countries, including the UK [1]. Radical surgicalexcision is the current standard of care [2-3]. Patients diagnosed with locally advanced tumors,which include those with bulky primaries (≥ T3), locoregional lymph node involvement, orwhere a resection margin is felt threatened, are usually referred for preoperativechemoradiotherapy (CROSS trial approach) or perioperative chemotherapy (MAGIC trialapproach) after evaluation by a multidisciplinary team. The current staging system of GEJtumours includes TNM, grade, vascular invasion, and potential R0/R1/R2 resection margins.
1 2 3 4
Open Access CaseReport DOI: 10.7759/cureus.420
How to cite this articleGaya A, Giakoustidis A, Winslet M, et al. (December 21, 2015) Tumor Biology: Is It Time to RedefineUnresectability? An Extraordinary Case of Gastroesophageal Junctional Adenocarcinoma. Cureus 7(12):e420. DOI 10.7759/cureus.420
Increasingly, an understanding of the genetic basis of cancer and of the host’s immunereactivity may permit the delineation of groups of patients likely to have a better outcome andthus be suitable for more aggressive therapy.
Resectability is determined on a purely technical basis and will depend on the skill andexperience of the surgeon. On the other hand, operability will, in addition to resectability,require a consideration of the benefits and risks to the patient, taking into account the age andcomorbidities, as to whether a major surgical procedure with its attendant morbidity isjustified. We illustrate the difference between unresectability and inoperability by presentingthe case of a patient with adenocarcinoma of GEJ, which was initially considered inoperable.
Case PresentationInformed patient consent was obtained at the time of treatment. No identifying patientinformation is contained in this paper.
A 34-year-old physically fit male with no comorbidities or family history of cancer presentedwith resistant dyspepsia and was diagnosed with a locally advanced Type III GEJ cancerextending from 37 cm from the incisors, down onto the lesser curve of the stomach at the levelof the incisura. Pathology was a moderately to poorly differentiated adenocarcinoma, HER2negative. The patient's tumor was considered unresectable at presentation, and he underwentfive cycles of neoadjuvant EOX chemotherapy (epirubicin, oxaliplatin, capecitabine) resultingin RECIST stable disease on CT. Extended neoadjuvant therapy was administered due to thelocally advanced nature of the tumor. As it was still considered inoperable, consolidationradical chemoradiation to a dose of 50 Gy in 25 fractions with concomitant cisplatin and 5FUwas subsequently delivered to the lower esophagus and proximal stomach, leading tosignificant regression demonstrable at diagnostic laparoscopy. Thereafter, an attemptedresection was performed. However, at laparotomy, he was found to have gross disease invadingthe whole lesser omentum up towards the porta hepatis, with encasement of the left gastricartery and the origin of the coeliac axis as well as extensive serosal disease within the lesser sacand SMA origin. The dimensions of the portion of tumor involving the descending aorta were3.6 x 2.8 cm.
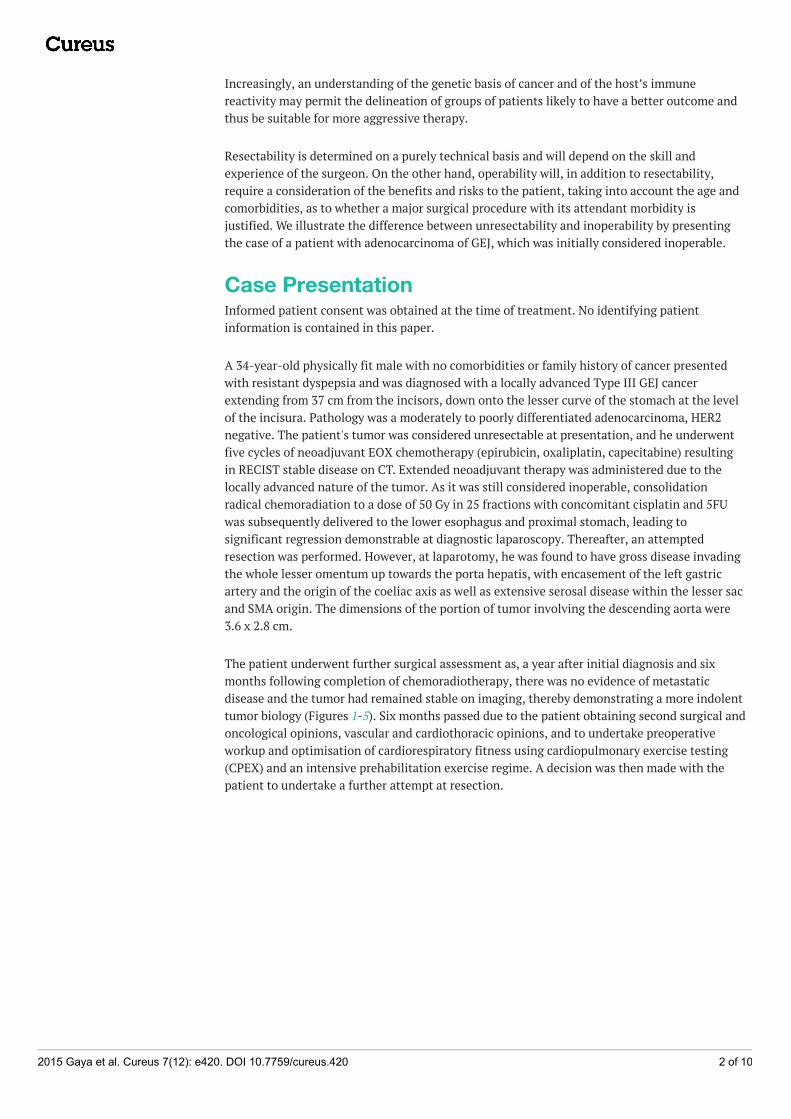
The patient underwent further surgical assessment as, a year after initial diagnosis and sixmonths following completion of chemoradiotherapy, there was no evidence of metastaticdisease and the tumor had remained stable on imaging, thereby demonstrating a more indolenttumor biology (Figures 1-5). Six months passed due to the patient obtaining second surgical andoncological opinions, vascular and cardiothoracic opinions, and to undertake preoperativeworkup and optimisation of cardiorespiratory fitness using cardiopulmonary exercise testing(CPEX) and an intensive prehabilitation exercise regime. A decision was then made with thepatient to undertake a further attempt at resection.
2015 Gaya et al. Cureus 7(12): e420. DOI 10.7759/cureus.420 2 of 10
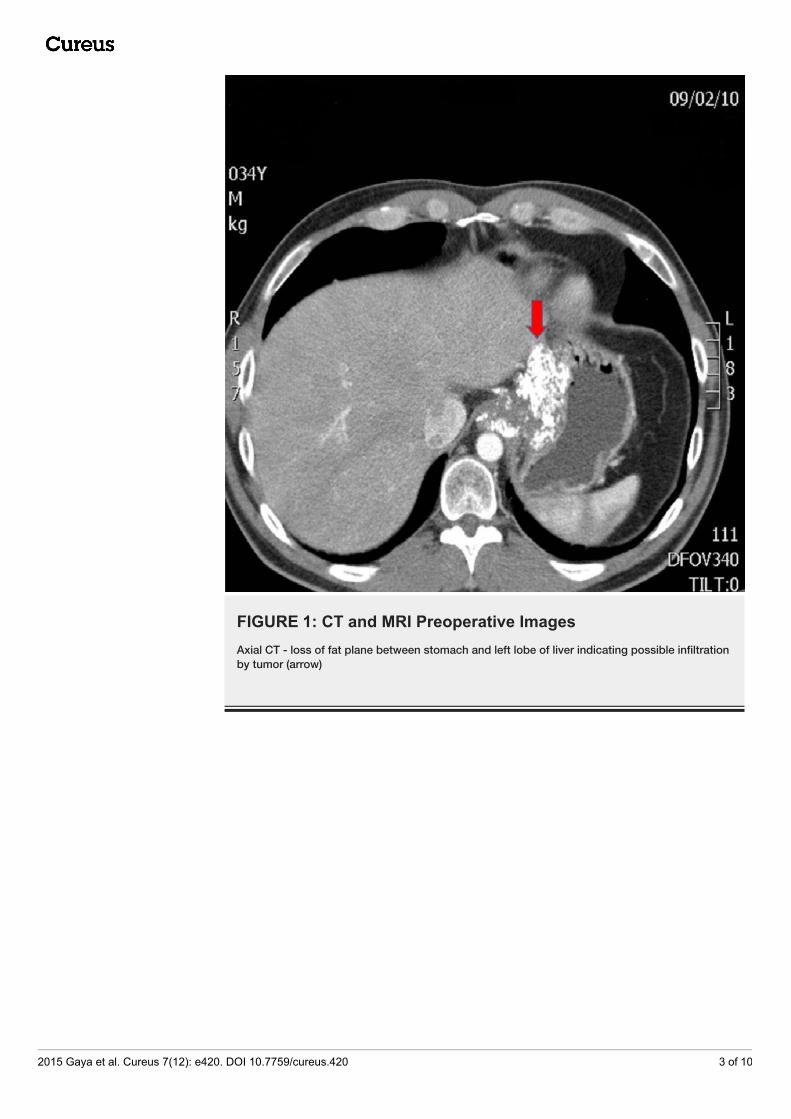
FIGURE 1: CT and MRI Preoperative ImagesAxial CT - loss of fat plane between stomach and left lobe of liver indicating possible infiltrationby tumor (arrow)
2015 Gaya et al. Cureus 7(12): e420. DOI 10.7759/cureus.420 3 of 10
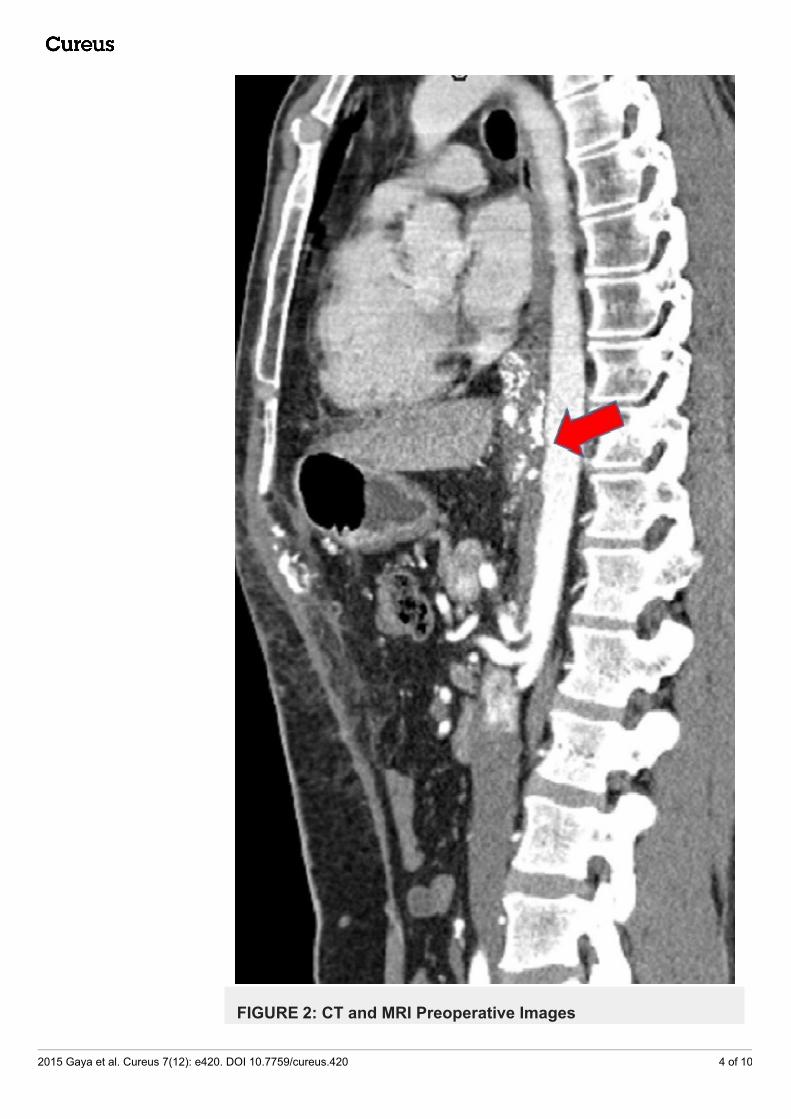
FIGURE 2: CT and MRI Preoperative Images
2015 Gaya et al. Cureus 7(12): e420. DOI 10.7759/cureus.420 4 of 10
Sagittal CT - Suspicious of aortic and celiac axis invasion (arrow) - loss of plane between tumorand descending aorta
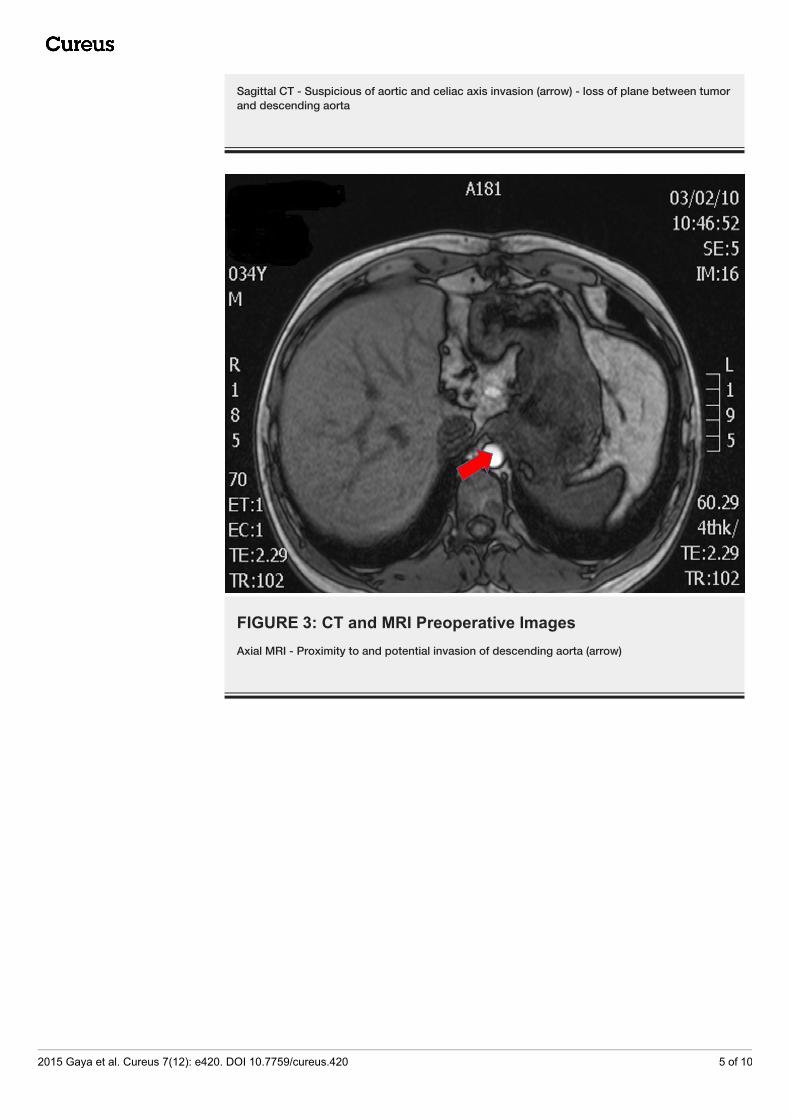
FIGURE 3: CT and MRI Preoperative ImagesAxial MRI - Proximity to and potential invasion of descending aorta (arrow)
2015 Gaya et al. Cureus 7(12): e420. DOI 10.7759/cureus.420 5 of 10
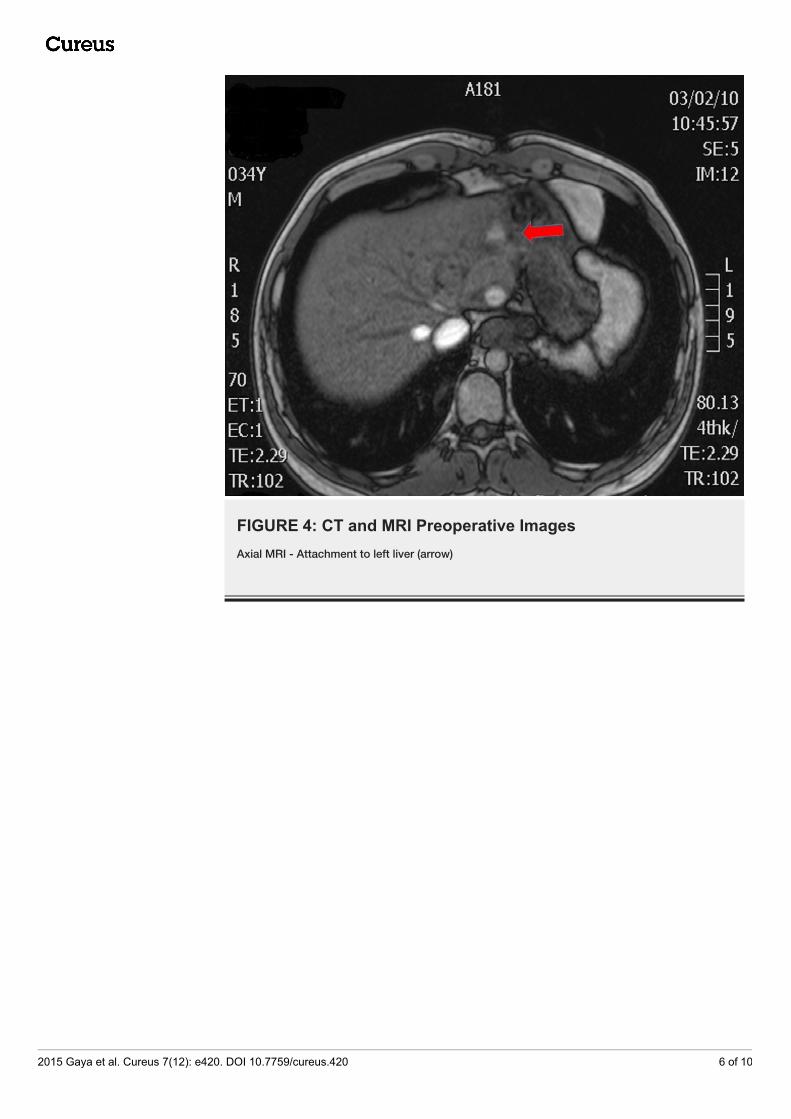
FIGURE 4: CT and MRI Preoperative ImagesAxial MRI - Attachment to left liver (arrow)
2015 Gaya et al. Cureus 7(12): e420. DOI 10.7759/cureus.420 6 of 10
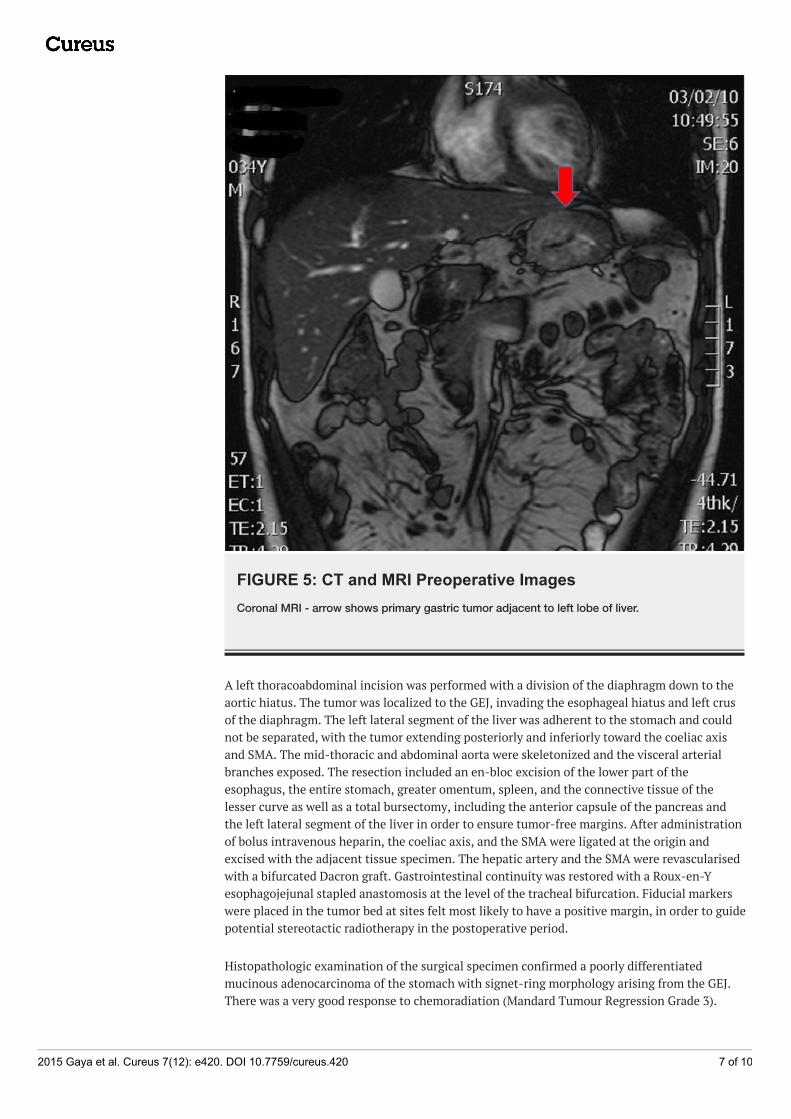
FIGURE 5: CT and MRI Preoperative ImagesCoronal MRI - arrow shows primary gastric tumor adjacent to left lobe of liver.
A left thoracoabdominal incision was performed with a division of the diaphragm down to theaortic hiatus. The tumor was localized to the GEJ, invading the esophageal hiatus and left crusof the diaphragm. The left lateral segment of the liver was adherent to the stomach and couldnot be separated, with the tumor extending posteriorly and inferiorly toward the coeliac axisand SMA. The mid-thoracic and abdominal aorta were skeletonized and the visceral arterialbranches exposed. The resection included an en-bloc excision of the lower part of theesophagus, the entire stomach, greater omentum, spleen, and the connective tissue of thelesser curve as well as a total bursectomy, including the anterior capsule of the pancreas andthe left lateral segment of the liver in order to ensure tumor-free margins. After administrationof bolus intravenous heparin, the coeliac axis, and the SMA were ligated at the origin andexcised with the adjacent tissue specimen. The hepatic artery and the SMA were revascularisedwith a bifurcated Dacron graft. Gastrointestinal continuity was restored with a Roux-en-Yesophagojejunal stapled anastomosis at the level of the tracheal bifurcation. Fiducial markerswere placed in the tumor bed at sites felt most likely to have a positive margin, in order to guidepotential stereotactic radiotherapy in the postoperative period.
Histopathologic examination of the surgical specimen confirmed a poorly differentiatedmucinous adenocarcinoma of the stomach with signet-ring morphology arising from the GEJ.There was a very good response to chemoradiation (Mandard Tumour Regression Grade 3).
2015 Gaya et al. Cureus 7(12): e420. DOI 10.7759/cureus.420 7 of 10
Esophageal and gastric resection margins were clear of viable tumor, and two of 26 lymphnodes contained small deposits of adenocarcinoma. Furthermore, multiple coeliac lymphnodes, as well as the No 12 lymph node, showed no evidence of metastatic disease. Over 90% ofthe tumor was necrotic as a consequence of the chemoradiation and no evidence of malignancywas identified in the liver or the spleen.
The postoperative course was uneventful, and the patient was discharged 13 dayspostoperatively. No further radiotherapy treatment was deemed necessary. In the followingmonths, he received four cycles of DCF (docetaxel, cisplatin, and 5FU) chemotherapy andexperienced problems with nutritional support, neutropenic sepsis, diarrhea, and intestinalbacterial overgrowth, all of which were controlled medically. A taxane-based regimen wasselected based upon the relatively poor response to neoadjuvant oxaliplatin and capecitabine.Follow-up CT scans and tumor markers were performed at three-month intervals for threeyears, and at six-month intervals for a further two years. All showed graft patency and no localrecurrence or metastatic disease. The patient is alive and well 5.5 years postoperatively with noevidence of recurrent disease; his weight is stable, and he returned to work and normalactivities of daily life six months postoperatively.
DiscussionCurrently, the Union for International Cancer Control (UICC) TNM classification is the maintool for defining the operability of a cancer patient, however, only from a purely anatomicalpoint of view [4]. The terms unresectable and inoperable are often used without actuallyaddressing the correct meaning of each term. By labeling a patient as ‘inoperable’, the emphasisis not placed on the technical challenge, as that could perhaps be surmounted, but on thefutility of the procedure based on past surgical experience and published outcome data. In thiscase, an optimal response to neoadjuvant therapy and extended period of surveillancesuggested an indolent tumor biology in a fit young patient with no comorbidities; thus, there isa small group of patients where the futility arguments are not necessarily valid.
Although the TNM classification is of value in determining the extent of a tumor and istherefore a guide to resectability, it does not take into account the ‘immune score’; namely, therole of adaptive and innate immunity in determining the tumor microenvironment [5]. There isincreasing evidence that the immune profile of a tumor has profound effects on its behaviorand that a coordinated adaptive immune reaction may well predict clinical outcome moreaccurately than tumor staging [6].
There is no clear definition of standard therapy, but in the UK, it usually consists ofperioperative chemotherapy and surgical resection based upon the MAGIC trial data, withchemoradiotherapy usually added postoperatively for adverse histopathologic features andpatients with a high-risk of local recurrence (e.g. positive circumferential margins) [2, 7].Increasing trimodal therapy consisting of neoadjuvant chemoradiotherapy prior to surgicalresection is used, based upon the Dutch CROSS trial.
Another important factor in defining operability and resectability is the encasement of majorvascular structures, such as the coeliac, common hepatic, or splenic arteries. En bloc resectionof the coeliac trunk, along with the coeliac nervous plexus and lymph nodes for advancedgastric cancer, has been technically possible over the last 60 years, and severalrevascularization strategies have been subsequently described [3, 8]. However, outcome datahas historically been poor, and this may largely be due to poor patient selection.
The value of pathologic response to neoadjuvant therapy in different types of cancer has beeninvestigated. In particular, pathologic response in patients with esophageal cancer, who
2015 Gaya et al. Cureus 7(12): e420. DOI 10.7759/cureus.420 8 of 10
received preoperative chemotherapy or chemoradiation, was shown to play an important rolein predicting survival outcomes. However, there is a need for additional surrogate markers forreliably predicting the biological behavior of the tumor. Recent and ongoing developments inproteomics, miRNA, and cDNA microarray technology may well have a role to play in the futurein accurately determining therapeutic responses, whilst more sensitive and detailed molecularanalysis of pathologic and immunologic responses could assist in predicting survival moreaccurately.
It has been shown that downstaging of tumors can be achieved with neoadjuvant therapy, i.e.,initially unresectable colorectal liver metastases [9]. In the case of gastroesophageal cancerpatients, the combination of the clinicopathologic features, imaging, and molecular biomarkersfacilitates the establishment of a predictive value for neoadjuvant therapy. Such biomarkerspreviously reported include the NF-κB, the EGFR family, and VEGF, as well as gene expressionprofiling. Extensive research is also being conducted into the characterization of‘immunological landscapes’ to predict tumor behavior and international collaborative studiesare addressing the development of an ‘immunoscore’ for the same purpose [10]. The ultimategoal would be to develop techniques to assess immunoscores on very small biopsies or onsamples of peripheral blood.
As regards to our patient, the tumor was aggressive in terms of its local behaviour but less so interms of metastatic potential, with the patient having stable disease a year following initialdiagnosis and with this being a key feature in the disease being considered potentially operable.
In this case report, we address the complex issue of inoperability versus unresectability, as wellas the important issue of patient selection for a multi-modality “off protocol” approach tocomplex tumors. Biological behavior and response of a tumor to chemotherapy and/orchemoradiation, along with the ability of the surgical team to undertake a potentially curativeresection, even when technically very challenging, should all be taken into consideration. Theword ‘inoperable’ should be used only in instances in which surgery could likely lead to the "onthe table" death of the patient or to unacceptable postoperative morbidity or mortality. In othercases, they should be considered “potentially resectable” with the question being askedwhether surgery would confer a clinical advantage and what potential benefits could justify therisk involved.
ConclusionsPreviously, surgical resection has been determined by tumor size and location, lymph nodeinvolvement, and the presence of metastatic disease. Although useful in actuarial terms, this isfar from individualization in the world of “personalized medicine”. The personal selection bytumor biological behavior and response to neoadjuvant therapy, in addition to these otherfactors, would be more sophisticated and take into account additional factors, such ascomorbidities, performance status, and immunology.
Additional InformationDisclosuresHuman subjects: Consent was obtained by all participants in this study. Conflicts of interest:In compliance with the ICMJE uniform disclosure form, all authors declare the following:Payment/services info: All authors have declared that no financial support was received fromany organization for the submitted work. Financial relationships: All authors have declaredthat they have no financial relationships at present or within the previous three years with anyorganizations that might have an interest in the submitted work. Other relationships: Allauthors have declared that there are no other relationships or activities that could appear to
2015 Gaya et al. Cureus 7(12): e420. DOI 10.7759/cureus.420 9 of 10
have influenced the submitted work.
References1. Pohl H, Welch HG: The role of overdiagnosis and reclassification in the marked increase of
esophageal adenocarcinoma incidence. J Natl Cancer Inst. 2005, 97:142–46.10.1093/jnci/dji024
2. Cunningham D, Allum WH, Stenning SP, Thompson JN, Van de Velde CJ, Nicolson M, ScarffeJH, Lofts FJ, Falk SJ, Iveson TJ, Smith DB, Langley RE, Verma M, Weeden S, Chua YJ, MAGICTrial Participants: Perioperative chemotherapy versus surgery alone for resectablegastroesophageal cancer. N Engl J Med. 2006, 355:11-20. 10.1056/NEJMoa055531
3. Bonnet S, Kohneh-Shahri N, Goere D, Deshayes I, Ayadi S, Elias D: Indications and surgicaltechnique of Appleby's operation for tumor invasion of the celiac trunk and its branches([Article in French). J Chir (Paris). 2009, 146:6–14. 10.1016/j.jchir.2009.02.002
4. Union for International Cancer Control: TNM Classification of Malignant Tumours, 7th ed..Sobin LH, Gospodarowicz MK, Wittekind C (ed): John Wiley & Sons Ltd, 2009.
5. Mlecnik B, Tosolini M, Kirilovsky A, Berger A, Bindea G, Meatchi T, Bruneval P, Trajanoski Z,Fridman WH, Pagès F, Galon J: Histopathologic-based prognostic factors of colorectal cancersare associated with the state of the local immune reaction. J Clin Oncol. 2011, 20:610–18.10.1200/JCO.2010.30.5425
6. Galon J, Costes A, Sanchez-Cabo F, Kirilovsky A, Mlecnik B, Lagorce-Pagès C, Tosolini M,Camus M, Berger A, Wind P, Zinzindohoué F, Bruneval P, Cugnenc PH, Trajanoski Z, FridmanWH, Pagès F: Type, density, and location of immune cells within human colorectal tumorspredict clinical outcome. Science. 2006, 313:1960–64. 10.1126/science.1129139
7. Yoshikawa T, Sasako M, Yamamoto S, Sano T, Imamura H, Fujitani K, Oshita H, Ito S,Kawashima Y, Fukushima N: Phase II study of neoadjuvant chemotherapy and extendedsurgery for locally advanced gastric cancer. Br J Surg. 2009, 96:1015-22. 10.1002/bjs.6665
8. Morera-Ocon FJ, Cárcel-Cárcel I, Ballestín Vicente J, Iranzo González-Cruz V: Somereflexions on the modified Appleby procedure. JOP. 2009, 10:674–78.
9. Adam R, Wicherts DA, de Haas RJ, Ciacio O, Lévi F, Paule B, Ducreux M, Azoulay D, BismuthH, Castaing D: Patients with initially unresectable colorectal liver metastases: is there apossibility of cure?. J Clin Oncol. 2009, 27:1829–35. 10.1200/JCO.2008.19.9273
10. Galon J, Mlecnik B, Bindea G, Angell HK, Berger A, Lagorce C, Lugli A, Zlobec I, Hartmann A,Bifulco C, Nagtegaal ID, Palmqvist R, Masucci GV, Botti G, Tatangelo F, Delrio P, Maio M,Laghi L, Grizzi F, Asslaber M, D'Arrigo C, Vidal-Vanaclocha F, Zavadova E, Chouchane L,Ohashi PS, Hafezi-Bakhtiari S, Wouters BG, Roehrl M, Nguyen L, Kawakami Y, Hazama S,Okuno K, Ogino S, Gibbs P, Waring P, Sato N, Torigoe T, Itoh K, Patel PS, Shukla SN, Wang Y,Kopetz S, Sinicrope FA, Scripcariu V, Ascierto PA, Marincola FM, Fox BA, Pagès F: Towards theintroduction of the 'Immunoscore' in the classification of malignant tumours. J Pathol. 2014,232:199–209. 10.1002/path.4287
2015 Gaya et al. Cureus 7(12): e420. DOI 10.7759/cureus.420 10 of 10