ultrasonography and amoebic liver abscesses
TRANSCRIPT
Ultrasonography and Amoebic Liver Abscesses
MAHMOUD HELMY ABUL-KHAIR, M.D., CH.M., F.I.C.S., MOHAMED M. KENAWI, M.C., CH.M., F.R.C.S.,EZZ EL-DIN A. KORASHY, M.D., NABIL M. ARAFA, M.D.
Twenty-four patients were admitted to Kasr-El-Aini Hospitalwith suspected diagnoses of amoebic liver abscesses. Thepatients underwent clinical examinations, stool specimenanalyses for cysts and trophozoites of Entamoeba histolytica,radiologic examinations, and routine liver function tests. Inone patient, a liver scintiscan was obtained. Ultrasonographicexamination was performed on all patients using the gray scaleimaging technique. In 20 patients, the diagnoses of amoebicliver abscesses were demonstrated by ultrasonographic ex-amination. In 19 patients, amoebic liver abscesses were verifiedby aspiration biopsies (95%), and one patient had a false-positive result. This false-positive result was due to a degener-ated hepatoma, demonstrated by aspiration biopsy. Of the 19patients, 12 patients (63.12%) had right lobe abscesses andseven (36.89%) had left lobe abscesses. The site, size and natureof the pus contained in the abscess could be determined byultrasonographic examination and, therefore, helped in themanagement and technique of the aspiration biopsy. In ad-dition, follow-up data could be more detailed using ultra-sonographic examinations. Ultrasonographic examination isa noninvasive, safe, accurate, and rapid method of diagnosis,and is highly recommended as a routine procedure in allcases of suspected amoebic liver abscesses in the pre- andposttreatment stages of the disease. It is also recommendedas an indicator of complete cure at follow-up examination.
A MOEBIC LIVER ABSCESS constitutes an importantcomplication of intestinal amoebiasis; a disease
which is not only endemic in Egypt, but is also world-wide in distribution. It often presents a pitfall inclinical diagnosis, and a challenge to surgical diagnosticacumen. Early diagnosis and prompt initiation oftherapy almost certainly lead to a complete cure, anda corresponding low mortality rate. In the same re-spect, late diagnosis carries a high mortality rate.
In Egypt, a survey was conducted by Lawless et al,in 1956 in El-Kunayessa village (Giza). They reporteda 97% incidence of intestinal amoebiasis, with nospecial predilection for age or sex.7 Liver involvementfrom intestinal amoebiasis varies from less than 1% to25% (average: 8.1%).4 Wilcocks and Manson-Bahr,14believed that carriers without symptoms, as well as
Reprint requests: Mahmoud Helmy Abul-Khair, M.D., GeneralSurgery Department, Faculty of Medicine, University of Cairo,Cairo, Egypt.Supported in part by N.S.F. grant #OIP76-10455.Submitted for publication: July 17, 1980.
From the General Surgery Department of theTechnology Transfer Focus, Faculty of Medicine,
Cairo University, Cairo, Egypt
natives of endemic areas, develop partial immunityto the parasite due to constant reinfection since child-hood. This explains the relative infrequency of liverinvolvement of inhabitants of endemic areas, butforeigners travelling to endemic areas are more proneto hepatic involvement.According to the Cairo University Hospital annual
medical statistical report, ten cases of amoebic liverabscesses were diagnosed in 1973, six cases werediagnosed in 1974, seven cases were diagnosed in 1975,eight cases were diagnosed in 1976 and seven caseswere diagnosed in 1977.The available means of diagnosis of amoebic liver
abscess are often of limited value. But since the intro-duction of ultrasonography as a diagnostic device,more accurate diagnoses were made in almost everycase.McCarthy," and Doust et al,5 reported that liver
abscesses, by virtue of their fluid content, show a uni-form distribution of weak echoes or band-like internalechoing structures representing the walls of loculi ordebris. The walls are poorly defined in contradistinc-tion to cysts, which have well-defined borders.12
Liver abscesses are usually elliptical in transversescans.5 However, they lose their elliptical cross-section when they are confined by strong barriers,e.g. liver capsule or diaphragm (Maklad et al., 1974).The objective of this study was to evaluate ultra-
sonography in the diagnosis of amoebic liver abscess,including the visualization of the exact site of theabscess and its role in the accurate determination ofthe optimal site and angle for the aspiration needle.
Materials and MethodsThis study includes 24 patients who were admitted
to Kasr-El-Aini Hospital with suspected diagnoses ofamoebic liver abscesses. There were 21 males and 3females included in the study. The patients ages rangedfrom 20 to 70 years (mean: 32.7 years).
0003-4932/81/0200/0221 $00.80 C J. B. Lippincott Company
221
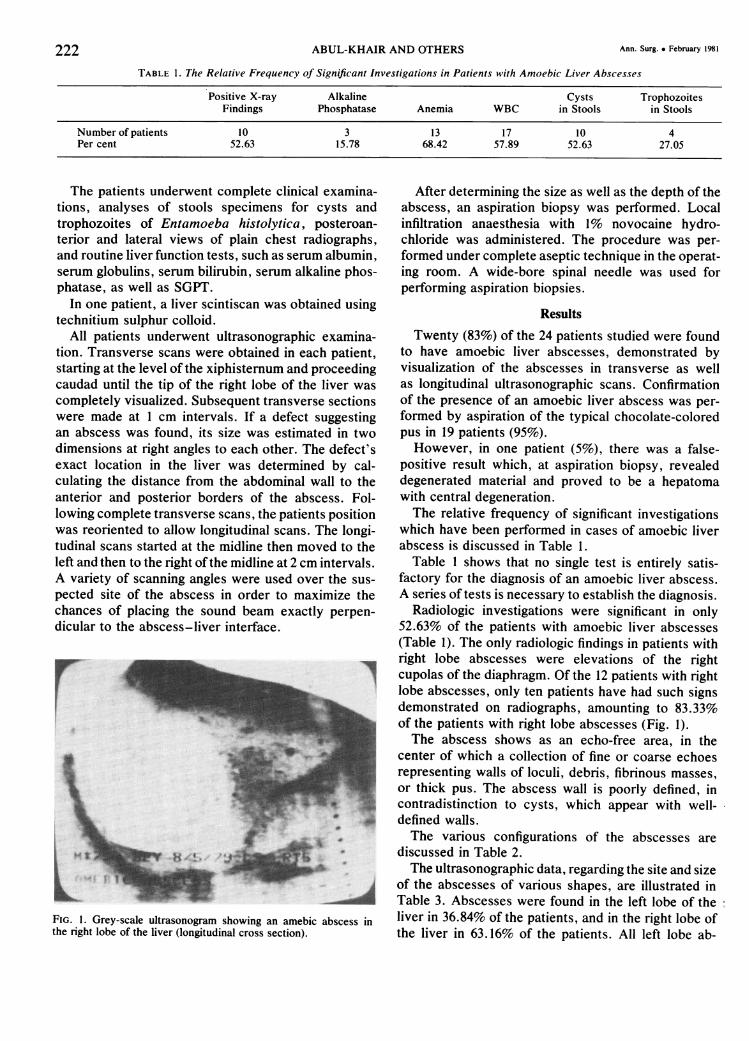
TABLE 1. The Relative Frequency of Significant Investigations in Patients with Amoebic Liver Abscesses
Positive X-ray Alkaline Cysts TrophozoitesFindings Phosphatase Anemia WBC in Stools in Stools
Number of patients 10 3 13 17 10 4Per cent 52.63 15.78 68.42 57.89 52.63 27.05
The patients underwent complete clinical examina-tions, analyses of stools specimens for cysts andtrophozoites of Entamoeba histolytica, posteroan-terior and lateral views of plain chest radiographs,and routine liver function tests, such as serum albumin,serum globulins, serum bilirubin, serum alkaline phos-phatase, as well as SGPT.
In one patient, a liver scintiscan was obtained usingtechnitium sulphur colloid.
All patients underwent ultrasonographic examina-tion. Transverse scans were obtained in each patient,starting at the level of the xiphisternum and proceedingcaudad until the tip of the right lobe of the liver wascompletely visualized. Subsequent transverse sectionswere made at 1 cm intervals. If a defect suggestingan abscess was found, its size was estimated in twodimensions at right angles to each other. The defect'sexact location in the liver was determined by cal-culating the distance from the abdominal wall to theanterior and posterior borders of the abscess. Fol-lowing complete transverse scans, the patients positionwas reoriented to allow longitudinal scans. The longi-tudinal scans started at the midline then moved to theleft and then to the right ofthe midline at 2 cm intervals.A variety of scanning angles were used over the sus-pected site of the abscess in order to maximize thechances of placing the sound beam exactly perpen-dicular to the abscess-liver interface.
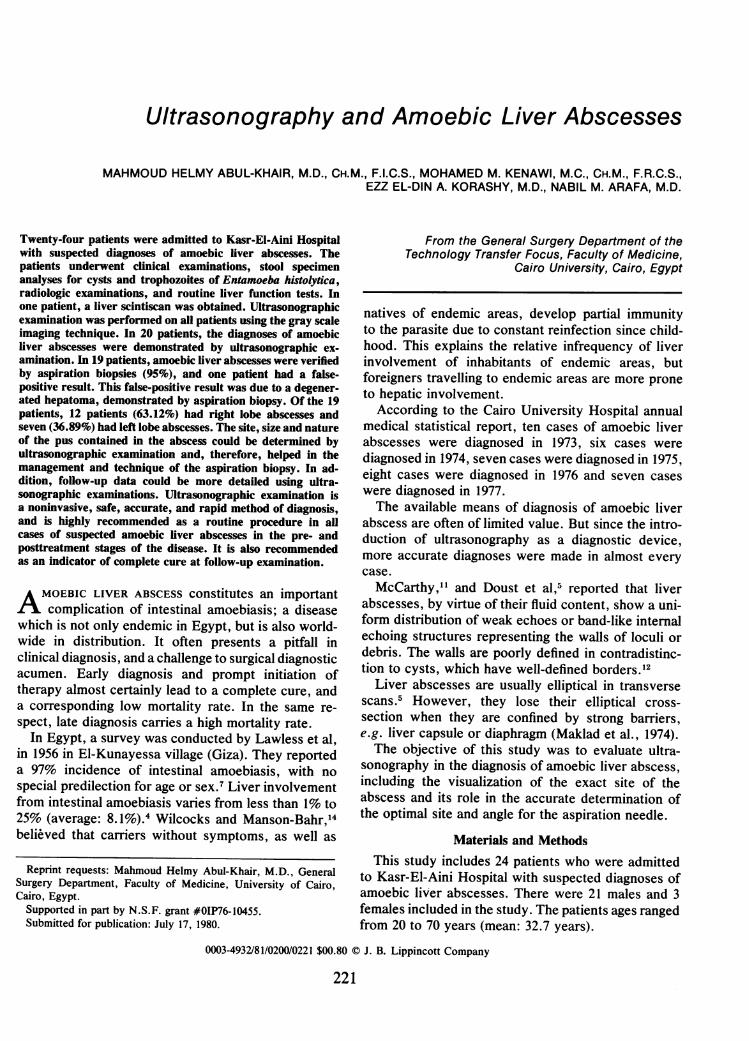
FIG. 1. Grey-scale ultrasonogram showing an amebic abscess inthe right lobe of the liver (longitudinal cross section).
After determining the size as well as the depth of theabscess, an aspiration biopsy was performed. Localinfiltration anaesthesia with 1% novocaine hydro-chloride was administered. The procedure was per-formed under complete aseptic technique in the operat-ing room. A wide-bore spinal needle was used forperforming aspiration biopsies.
Results
Twenty (83%) of the 24 patients studied were foundto have amoebic liver abscesses, demonstrated byvisualization of the abscesses in transverse as wellas longitudinal ultrasonographic scans. Confirmationof the presence of an amoebic liver abscess was per-formed by aspiration of the typical chocolate-coloredpus in 19 patients (95%).However, in one patient (5%), there was a false-
positive result which, at aspiration biopsy, revealeddegenerated material and proved to be a hepatomawith central degeneration.The relative frequency of significant investigations
which have been performed in cases of amoebic liverabscess is discussed in Table 1.
Table 1 shows that no single test is entirely satis-factory for the diagnosis of an amoebic liver abscess.A series of tests is necessary to establish the diagnosis.
Radiologic investigations were significant in only52.63% of the patients with amoebic liver abscesses(Table 1). The only radiologic findings in patients withright lobe abscesses were elevations of the rightcupolas of the diaphragm. Of the 12 patients with rightlobe abscesses, only ten patients have had such signsdemonstrated on radiographs, amounting to 83.33%of the patients with right lobe abscesses (Fig. 1).The abscess shows as an echo-free area, in the
center of which a collection of fine or coarse echoesrepresenting walls of loculi, debris, fibrinous masses,or thick pus. The abscess wall is poorly defined, incontradistinction to cysts, which appear with well-defined walls.The various configurations of the abscesses are
discussed in Table 2.The ultrasonographic data, regarding the site and size
of the abscesses of various shapes, are illustrated inTable 3. Abscesses were found in the left lobe of theliver in 36.84% of the patients, and in the right lobe ofthe liver in 63.16% of the patients. All left lobe ab-
222 ABUL-KHAIR AND OTHERS Ann. Surg. * February 1981
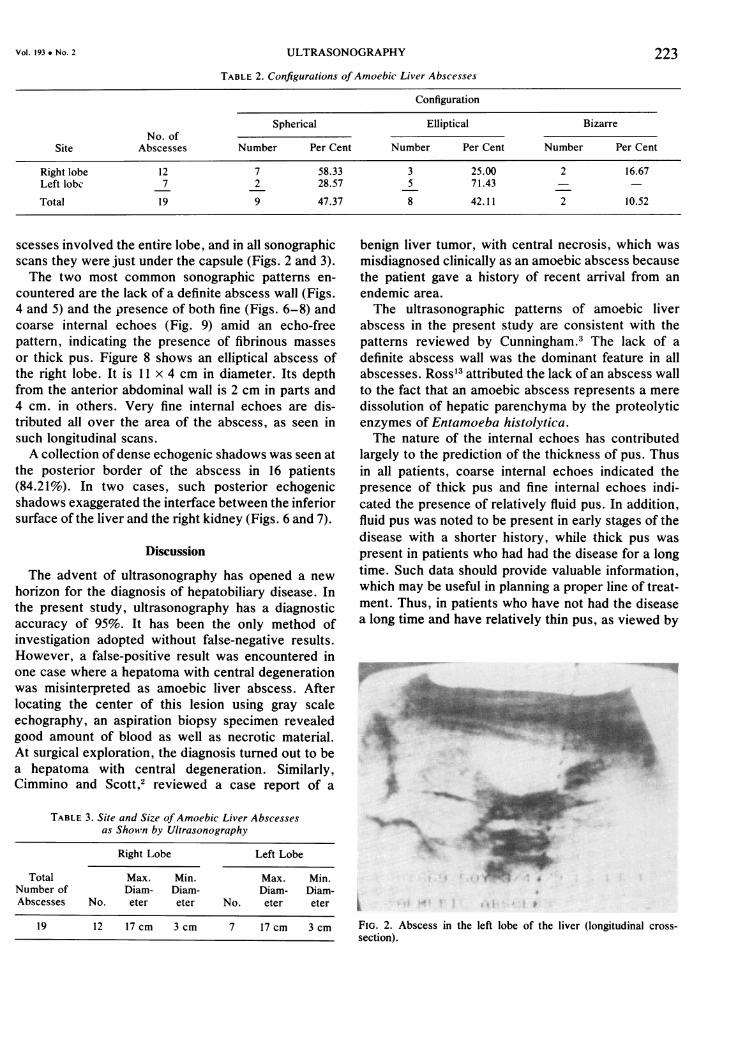
TABLE 2. Configurations ofAmoebic Liver Abscesses
Configuration
Spherical Elliptical BizarreNo. of
Site Abscesses Number Per Cent Number Per Cent Number Per Cent
Right lobe 12 7 58.33 3 25.00 2 16.67Left lobc 7 2 28.57 5 71.43
Total 19 9 47.37 8 42.11 2 10.52
scesses involved the entire lobe, and in all sonographicscans they were just under the capsule (Figs. 2 and 3).The two most common sonographic patterns en-
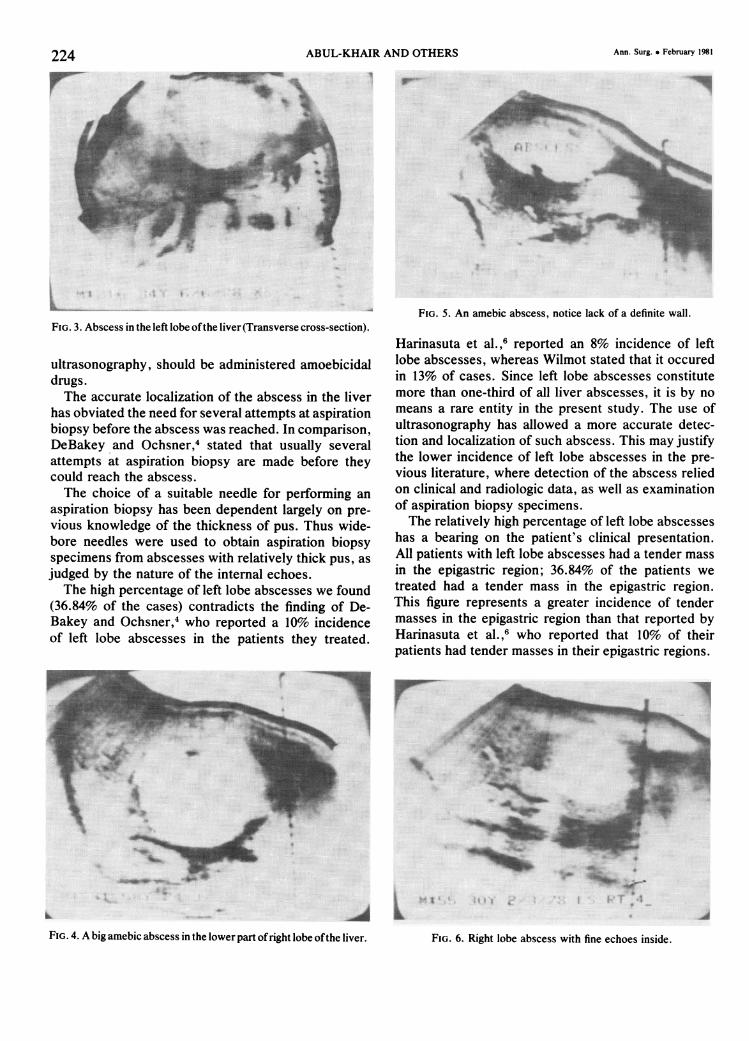
countered are the lack of a definite abscess wall (Figs.4 and 5) and the presence of both fine (Figs. 6-8) andcoarse internal echoes (Fig. 9) amid an echo-freepattern, indicating the presence of fibrinous massesor thick pus. Figure 8 shows an elliptical abscess ofthe right lobe. It is 11 x 4 cm in diameter. Its depthfrom the anterior abdominal wall is 2 cm in parts and4 cm. in others. Very fine internal echoes are dis-tributed all over the area of the abscess, as seen insuch longitudinal scans.A collection ofdense echogenic shadows was seen at
the posterior border of the abscess in 16 patients(84.21%). In two cases, such posterior echogenicshadows exaggerated the interface between the inferiorsurface of the liver and the right kidney (Figs. 6 and 7).
Discussion
The advent of ultrasonography has opened a newhorizon for the diagnosis of hepatobiliary disease. Inthe present study, ultrasonography has a diagnosticaccuracy of 95%. It has been the only method ofinvestigation adopted without false-negative results.However, a false-positive result was encountered inone case where a hepatoma with central degenerationwas misinterpreted as amoebic liver abscess. Afterlocating the center of this lesion using gray scaleechography, an aspiration biopsy specimen revealedgood amount of blood as well as necrotic material.At surgical exploration, the diagnosis turned out to bea hepatoma with central degeneration. Similarly,Cimmino and Scott,2 reviewed a case report of a
TABLE 3. Site and Size ofAmoebic Liver Abscessesas Shown by Ultrasonography
Right Lobe Left Lobe
Total Max. Min. Max. Min.Number of Diam- Diam- Diam- Diam-Abscesses No. eter eter No. eter eter
19 12 17 cm 3 cm 7 17 cm 3 cm
benign liver tumor, with central necrosis, which wasmisdiagnosed clinically as an amoebic abscess becausethe patient gave a history of recent arrival from anendemic area.The ultrasonographic patterns of amoebic liver
abscess in the present study are consistent with thepatterns reviewed by Cunningham.3 The lack of adefinite abscess wall was the dominant feature in allabscesses. Ross13 attributed the lack of an abscess wallto the fact that an amoebic abscess represents a meredissolution of hepatic parenchyma by the proteolyticenzymes of Entamoeba histolytica.The nature of the internal echoes has contributed
largely to the prediction of the thickness of pus. Thusin all patients, coarse internal echoes indicated thepresence of thick pus and fine internal echoes indi-cated the presence of relatively fluid pus. In addition,fluid pus was noted to be present in early stages of thedisease with a shorter history, while thick pus waspresent in patients who had had the disease for a longtime. Such data should provide valuable information,which may be useful in planning a proper line of treat-ment. Thus, in patients who have not had the diseasea long time and have relatively thin pus, as viewed by
-.. im
T I #
FIG. 2. Abscess in the left lobe of the liver (longitudinal cross-section).
223Vol. 193 . NO. 2 ULTRASONOGRAPHY
Ann. Surg. * February 1981ABUL-KHAIR AND OTHERS
. _qq
FIG. 3. Abscess in the left lobe ofthe liver (Transverse cross-section).
ultrasonography, should be administered amoebicidaldrugs.The accurate localization of the abscess in the liver
has obviated the need for several attempts at aspirationbiopsy before the abscess was reached. In comparison,DeBakey and Ochsner,4 stated that usually severalattempts at aspiration biopsy are made before theycould reach the abscess.The choice of a suitable needle for performing an
aspiration biopsy has been dependent largely on pre-vious knowledge of the thickness of pus. Thus wide-bore needles were used to obtain aspiration biopsyspecimens from abscesses with relatively thick pus, asjudged by the nature of the internal echoes.
The high percentage of left lobe abscesses we found(36.84% of the cases) contradicts the finding of De-Bakey and Ochsner,4 who reported a 10% incidenceof left lobe abscesses in the patients they treated.
FIG. 5. An amebic abscess, notice lack of a definite wall.
Harinasuta et al. ,6 reported an 8% incidence of leftlobe abscesses, whereas Wilmot stated that it occuredin 13% of cases. Since left lobe abscesses constitutemore than one-third of all liver abscesses, it is by nomeans a rare entity in the present study. The use ofultrasonography has allowed a more accurate detec-tion and localization of such abscess. This may justifythe lower incidence of left lobe abscesses in the pre-vious literature, where detection of the abscess reliedon clinical and radiologic data, as well as examinationof aspiration biopsy specimens.The relatively high percentage of left lobe abscesses
has a bearing on the patient's clinical presentation.All patients with left lobe abscesses had a tender massin the epigastric region; 36.84% of the patients wetreated had a tender mass in the epigastric region.This figure represents a greater incidence of tendermasses in the epigastric region than that reported byHarinasuta et al.,6 who reported that 10% of theirpatients had tender masses in their epigastric regions.
F-
FIG . 4. A big amebic abscess in the lower part ofright lobe ofthe liver.
|.5ow"N
224
FIG. 6. Right lobe abscess with fine echoes inside.
.". t-i
ULTRASONOGRAPHY
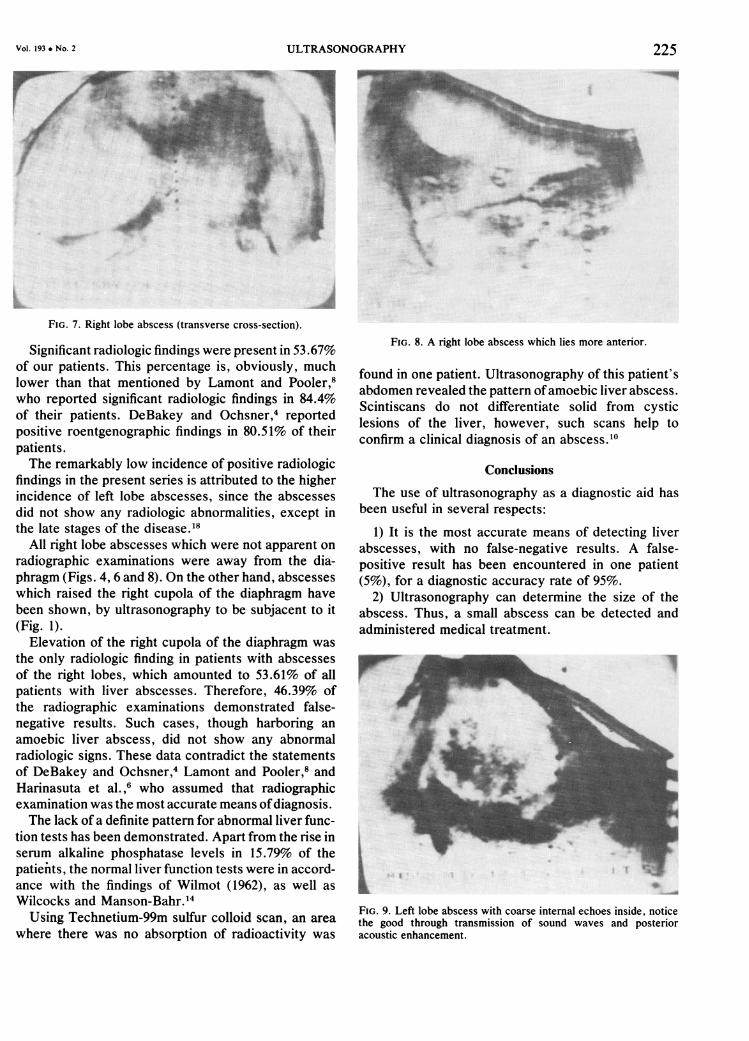
FIG. 7. Right lobe abscess (transverse cross-section).
Significant radiologic findings were present in 53.67%of our patients. This percentage is, obviously, muchlower than that mentioned by Lamont and Pooler,8who reported significant radiologic findings in 84.4%of their patients. DeBakey and Ochsner,4 reportedpositive roentgenographic findings in 80.51% of theirpatients.The remarkably low incidence of positive radiologic
findings in the present series is attributed to the higherincidence of left lobe abscesses, since the abscessesdid not show any radiologic abnormalities, except inthe late stages of the disease.18
All right lobe abscesses which were not apparent onradiographic examinations were away from the dia-phragm (Figs. 4, 6 and 8). On the other hand, abscesseswhich raised the right cupola of the diaphragm havebeen shown, by ultrasonography to be subjacent to it(Fig. 1).
Elevation of the right cupola of the diaphragm wasthe only radiologic finding in patients with abscessesof the right lobes, which amounted to 53.61% of allpatients with liver abscesses. Therefore, 46.39% ofthe radiographic examinations demonstrated false-negative results. Such cases, though harboring anamoebic liver abscess, did not show any abnormalradiologic signs. These data contradict the statementsof DeBakey and Ochsner,4 Lamont and Pooler,8 andHarinasuta et al.,6 who assumed that radiographicexamination was the most accurate means ofdiagnosis.The lack of a definite pattern for abnormal liver func-
tion tests has been demonstrated. Apart from the rise inserum alkaline phosphatase levels in 15.79% of thepatienits, the normal liver function tests were in accord-ance with the findings of Wilmot (1962), as well asWilcocks and Manson-Bahr.14Using Technetium-99m sulfur colloid scan, an area
where there was no absorption of radioactivity was
FIG. 8. A right lobe abscess which lies more anterior.
found in one patient. Ultrasonography of this patient'sabdomen revealed the pattern ofamoebic liver abscess.Scintiscans do not differentiate solid from cysticlesions of the liver, however, such scans help toconfirm a clinical diagnosis of an abscess.10
Conclusions
The use of ultrasonography as a diagnostic aid hasbeen useful in several respects:
1) It is the most accurate means of detecting liverabscesses, with no false-negative results. A false-positive result has been encountered in one patient(5%), for a diagnostic accuracy rate of 95%.
2) Ultrasonography can determine the size of theabscess. Thus, a small abscess can be detected andadministered medical treatment.
_S
_..
rF<:
F
LFIG. 9. Left lobe abscess with coarse internal echoes inside, noticethe good through transmission of sound waves and posterioracoustic enhancement.
225Vol. 193 * No. 2

226 ABUL-KHAIR AND OTHERS Ann. Surg. * February 1981
3) Using ultrasonography, it is possible to predictthe thickness of pus. Thick pus was identified by coarseinternal echoes, whereas thin pus was identified byfine internal echoes. Thus, a suitable biopsy needlecould be chosen for aspiration. In addition, thin puswas present in early stages of the disease, while thickpus was present in late stages of the disease.
4) Ultrasonography can detect the presence of leftlobe abscesses, which are difficult to detect by otherdiagnostic methods.
5) The optimum site for aspiration biopsy of theabscess can be determined accurately, thus obviatingthe need for several blind attempts at aspiration.
6) It is the most suitable means of detecting thenumber of abscesses.
7) Ultrasonography may be used in follow-up ex-aminations, to determine whether the abscess is pro-gressing or regressing.
Ultrasonography is noninvasive safe, and rapidmeans of diagnosis. It is highly recommended as aroutine procedure in all patients suspected as havingan amoebic liver abscess, which is sometimes difficultto diagnose.
References1. Alkan WJ, Kalmi B, Kalderon M. The clinical syndrome of
amoebic abscess of the left lobe of the liver. Ann InternMed 1961; 55:800.
2. Cimmino CV, Scott DW. Case report: benign liver tumourwith central necrosis. J Clin Ultrasound 1978; 6; (73): 142.
3. Cunningham JJ. In vitro gray scale echography of protein-lipidfluid collections in liver tissue. J Clin Ultrasound 1976;4:255-258.
4. DeBakey ME, Ochsner A. Hepatic amoebiasis, a 20 year ex-perience and analysis of 263 cases. Int Abstr Surg 1957;92:209.
5. Doust BD, Quiraz T, Stewart JM. Ultrasonic distinction ofabscesses from other intra-abdominal fluid collections.Radiology 1977; 125:213.
6. Harinasuta T, Bunnage D, Jaroonvesama N, et al. Amoebiasis,study of 769 cases. Eighth International Congress on TropicalMedicine and Malaria, Teheran. Abstracts and reviews,258, 1968.
7. Kamal AM. Epidemiology of communicable diseases. Anglo-Egyptian Bookshop. Cairo. 1958.
8. Lamont NM, Pooler NR. Hepatic amoebiasis, a study of 250cases. Q J Med 1958; 27:389.
9. Makland NF, Doust BD, Baum JK. Ultrasonic diagnosis ofpost-operative intra-abdominal abscesses. Radiology 1974;113:417-422.
10. McCarthy CF, Davis ER, Wells PNT, et al. A comparison ofultrasonic and isotope scanning in the diagnosis of liverdisease. Br J Radiol 1970; 43: 100.
11. McCarthy CF, Wells PN, Ross FG, Read AE. The use ofultrasound in the diagnosis of cystic lesions of the liver andupper abdomen and in the detection of ascites. Gut 1969;10:904.
12. Rasmussen SN, Holm HH, Kristensen JD, et al. Ultrasoundin the diagnosis of liver diseases. J Clin Ultrasound 1973;1:220.
13. Ross FGM. Ultrasound in the diagnosis of liver disease. ProcR Soc Med 1974; 67:211.
14. Wilcocks C, Manson-Babr PEC. Manson's Tropical Disease.17th ed. Bailliere Tindall, 1972. p. 212.