tyrosine-kinase inhibitors in the treatment...
TRANSCRIPT

Special Article
TYROSINE-KINASE INHIBITORS IN THE TREATMENT OF MUSCLE INVASIVE BLADDER CANCER AND HORMONE REFRACTORY PROSTATE CANCER
Hervé Wallerand1, Grégoire Robert1, Jean-Christophe Bernhard1, Alain Ravaud2 andJean-Jacques Patard3.
1Department of Urology. Bordeaux University Hospital. Bordeaux 2 Victor Segalen University. Bordeaux. France.2Department of Medical Oncology. Bordeaux University Hospital. Bordeaux 2 Victor Segalen University. Bordeaux. 3Department of Urology. Rennes University Hospital. Rennes. France.
@ CORRESPONDENCE
Prof. Jean-Jacques PatardRennes University HospitalCHRU PontchaillouDepartment of UrologyRue Henri Le Guillou35033 Rennes Cedex, France
Accepted for publication: October 21st, 2009
Arch. Esp. Urol. 2010; 63 (9): 773-787
Summary.- OBJECTIVES: Various protein kinases are known to be activated in cancer cells and drive tumor growth and progression. In metastatic renal cell carcino-ma tyrosine-kinase inhibitors (TKIs) have achieved signifi-cant progression-free and overall survival improvements. For bladder and prostate cancers TKIs may also be con-sidered as a promising treatment option. Our aim was to report the most relevant published articles to support the interest of the use of TKIs in the treatment of bladder and prostate cancer.
METHOD: PubMed database and bibliographies of retrieved articles were reviewed. The key words used
were tyrosine-kinase inhibitor, protein-kinase inhibitor, hormone refractory prostate cancer, muscle invasive bladder cancer. The most relevant publications from ba-sic science and clinical randomized controlled studies were summarized and analyzed.
RESULTS: Regarding bladder cancer, TKI treatment is one of the most studied therapeutic strategies in the field of targeted therapy. Indeed, it has been suggested that targeting TK alone and/or in association with cytotoxic chemotherapy may represent a promising option for treating locally advanced and/or metastatic bladder cancer. Concerning hormone refractory prostate cancer (HRPC), collected data are still confusing. Basic scien-ce studies found an interesting expression of EGF and VEGF receptors on cancer cells supporting the idea that TKIs could be efficient in HRPC. Nonetheless most of published clinical phase II studies found a weak effect on symptoms and quality of life without any decrease in PSA levels or overall survival.
CONCLUSION: TKIs have not yet achieved in bladder and prostate cancers similar efficacy to what has been obtained in metastatic renal cell carcinoma. Further stu-dies are needed to establish the place of such an appro-ach in non renal tumors.
Keywords: Protein kinase inhibitor. Tyrosine kinase inhibitor. Bladder cancer. Muscle invasive bladder cancer. Prostate cancer. Hormone refractory prostate cancer. Adjuvant therapy.
Resumen.- OBJETIVO: Se sabe que varias proteín-qui-nasas son activadas en las células tumorales e impulsan el crecimiento y progresión tumoral. En el carcinoma de células renales metastásico, los inhibidores de la tirosin-

H. Wallerand, G. Robert, J. Ch. Bernhard, et al.
INTRODUCTION
Various protein kinases are known to be ac-tivated in cancer cells and drive tumor growth and progression. Therefore, blocking tyrosine kinases (TK) represents a rational approach for cancer therapy. Receptor tyrosine kinases (RTKs) produce a mitogenic signal through Ras activation, which is an oncogene frequently activated by point mutations in various hu-
774
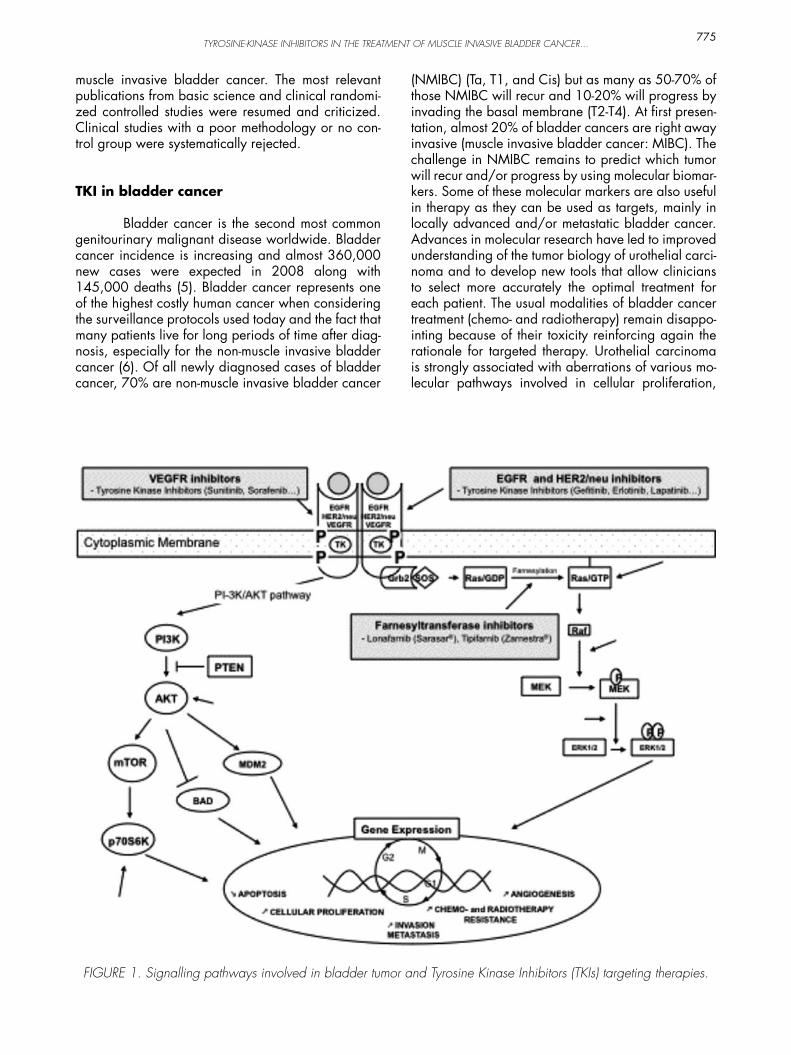
man cancers, including bladder and prostate cancers. RTKs have been identified as proto-oncogenes and cancer cell proliferation has been associated with the unregulated activity of oncogenes (1). However, RTKs in cancer cell can also activates PI-3K leading to Akt activation and anti-apoptotic signal to the cell through BAD phosphorylation. Both Ras-dependent and Ras-independent pathways allow cancer cells to selec-tively proliferate suggesting that targeting a single pathway could be not sufficient for effective cancer treatment (Figure 1). Basic research on targeted the-rapy increasingly suggests that inhibition of different targets represents a promising treatment option.
Molecular targeted drugs are divided into 3 groups:
a) drugs acting on the cell surface receptors,
b) drugs acting on intracellular pathways, and
c) drugs acting on proteasome inhibitors.
TK inhibitors (TKIs) are acting on cell surface receptors known to be aberrantly activated in cancers. Numerous TKIs have been developed and approved for clinical use: gefitinib, erlotinib, sunitinib, lapati-nib, nilotinib, and dasatinib. They have been shown to reduce cell proliferation in human cancer cell lines and xenografts but also to increase apoptosis, induce cell cycle arrest and decrease angiogenesis (2). Re-cently has emerged the idea that targeting several TK could be more effective than targeting a single activa-ted TK (3). Various tyrosine kinase receptors such as EGFR, PDGFR, IGFR, VEGFR, FGFR, and HGFR have been shown to be overexpressed in bladder and/or prostate cancers. Among these, EFGR and angioge-nesis pathways are particularly interesting because effective drugs targeting these pathways have beco-me available in clinical practice.
In metastatic renal cell carcinoma tyrosine-Ki-nase inhibitors (TKIs) have achieved progression-free and overall survival improvement more than other treatments (4). For bladder and prostate cancers TKIs may also be considered as a promising treatment op-tion. Our aim was to report the most relevant publis-hed articles to support the interest of the use of TKIs in the treatment of bladder and prostate cancers.
MATERIAL AND METHOD
PubMed database and bibliographies of re-trieved articles were systematically reviewed. The key words used were tyrosine-kinase inhibitor, protein-ki-nase inhibitor, hormone refractory prostate cancer,
Palabras clave: Inhibidor de la proteín-quinasa. Inhibidor de la tirosin-quinasa.Cáncer de vejiga. Cáncer de vejiga músculo infilrante. Cáncer de próstata. Cáncer de próstata hormono refractario. Terapia adyuvante.
quinasa (TKIs) han logrado importantes beneficios en progresión libre de enfermedad y supervivencia global. Los TKIs pueden ser también considerados como una prometedora opción de tratamiento en tumores vesica-les y prostáticos. Nuestro objetivo fue dar a conocer los artículos más relevantes publicados para confirmar el interés de la utilización de los TKI en el tratamiento de estos tumores.
MÉTODOS: Se realizó una busqueda sistemática en PubMed y se revisaron los artículos recuperados. Las palabras clave utilizadas fueron: inhibidor de la tiro-sin-quinasa, inhibidor de la protein-quinasa, cáncer de próstata hormono-refractario, cáncer de vejiga músculo-infiltrante. Las publicaciones más relevantes de ciencia básica y ensayos clínicos controlados y aleatorizados fueron resumidas y analizadas.
RESULTADOS: En cuanto al cáncer de vejiga, el trata-miento TKI es una de las estrategias terapéuticas más estudiadas en el campo de la terapia dirigida. De he-cho, se ha sugerido que dirigiendo solamente TK y/o asociándola con quimioterapia citotóxica puede repre-sentar una opción prometedora para tratar el cáncer de vejiga localmente avanzado y/o metastásico. En cuan-to al cáncer de próstata hormono-refractario (CPHR), los datos recogidos son aún confusos. Los estudios de ciencia básica encontraron una interesante expresión de receptores EGF y VEGF en las células tumorales con-firmando la idea de que los TKI podrían resultar eficien-tes en el CPHR. Sin embargo la mayoría de estudios pu-blicados de fase II encontraron un débil efecto sobre los síntomas y la calidad de vida sin ninguna disminución en los niveles de PSA o en la supervivencia general.
CONCLUSIÓN: Los TKIs todavía no han alcanzado en tumores vesicales o prostátivos una eficacia similar a lo que se ha obtenido en el carcinoma renal metastásico. Se necesitan más estudios para establecer el papel de ese enfoque en tumores no renales.
TYROSINE-KINASE INHIBITORS IN THE TREATMENT OF MUSCLE INVASIVE BLADDER CANCER...
muscle invasive bladder cancer. The most relevant publications from basic science and clinical randomi-zed controlled studies were resumed and criticized. Clinical studies with a poor methodology or no con-trol group were systematically rejected.
TKI in bladder cancer
Bladder cancer is the second most common genitourinary malignant disease worldwide. Bladder cancer incidence is increasing and almost 360,000 new cases were expected in 2008 along with 145,000 deaths (5). Bladder cancer represents one of the highest costly human cancer when considering the surveillance protocols used today and the fact that many patients live for long periods of time after diag-nosis, especially for the non-muscle invasive bladder cancer (6). Of all newly diagnosed cases of bladder cancer, 70% are non-muscle invasive bladder cancer
(NMIBC) (Ta, T1, and Cis) but as many as 50-70% of those NMIBC will recur and 10-20% will progress by invading the basal membrane (T2-T4). At first presen-tation, almost 20% of bladder cancers are right away invasive (muscle invasive bladder cancer: MIBC). The challenge in NMIBC remains to predict which tumor will recur and/or progress by using molecular biomar-kers. Some of these molecular markers are also useful in therapy as they can be used as targets, mainly in locally advanced and/or metastatic bladder cancer. Advances in molecular research have led to improved understanding of the tumor biology of urothelial carci-noma and to develop new tools that allow clinicians to select more accurately the optimal treatment for each patient. The usual modalities of bladder cancer treatment (chemo- and radiotherapy) remain disappo-inting because of their toxicity reinforcing again the rationale for targeted therapy. Urothelial carcinoma is strongly associated with aberrations of various mo-lecular pathways involved in cellular proliferation,
775
FIGURE 1. Signalling pathways involved in bladder tumor and Tyrosine Kinase Inhibitors (TKIs) targeting therapies.

H. Wallerand, G. Robert, J. Ch. Bernhard, et al.
tumor angiogenesis, and apoptosis. Among these, Epithelial Growth Factor Receptor (EGFR) and tumor angiogenesis are critical as efficient drugs targeting these pathways have recently become available.
Targeting EGFR (Epithelial Growth Factor receptor) in bladder cancer
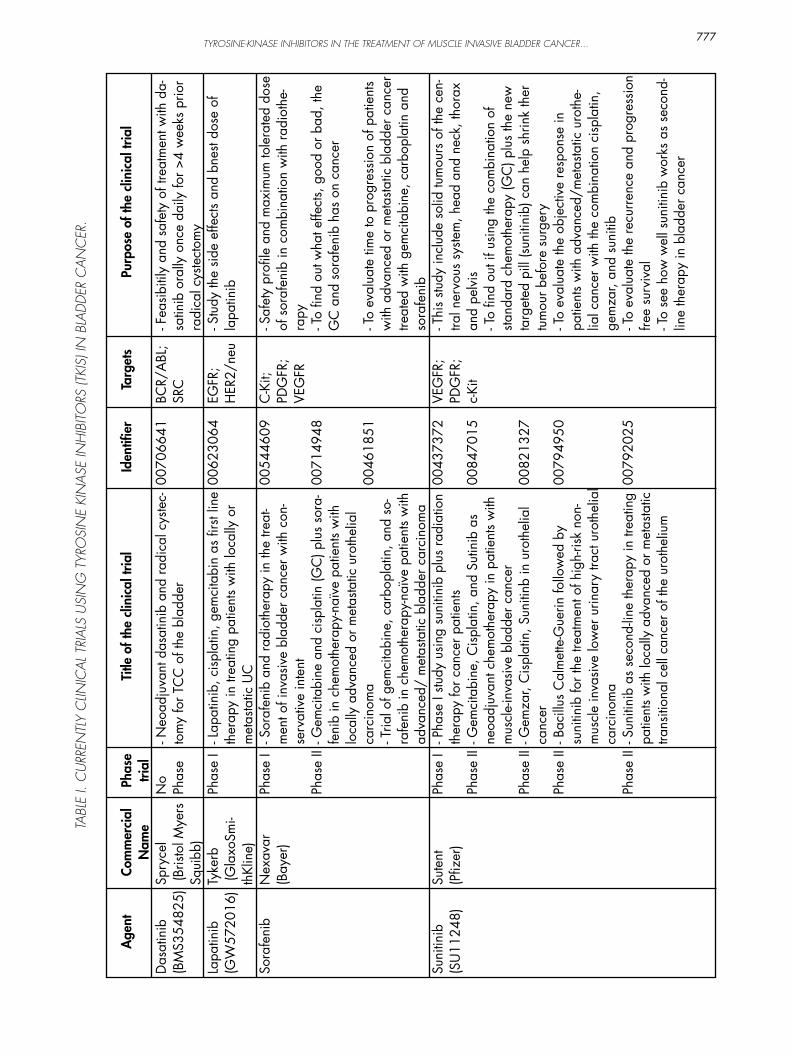
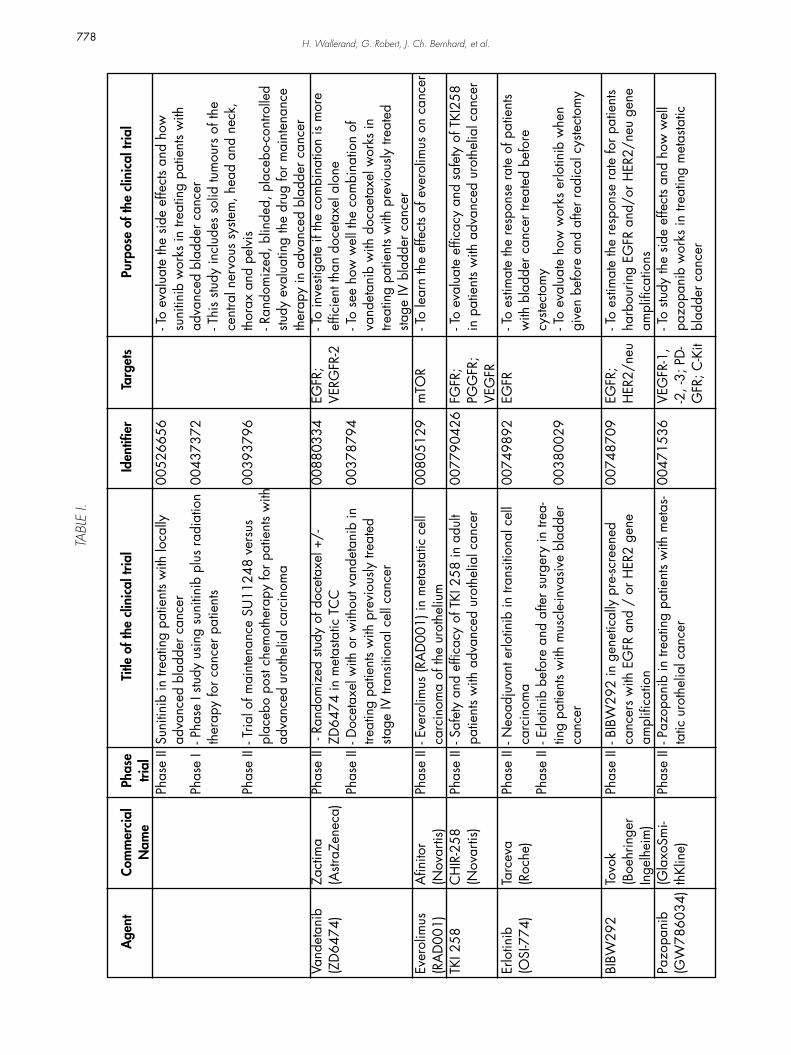
The EGFR signal transduction is involved in the regulation of various neoplastic processes, such as cell cycle progression, inhibition of apoptosis, tu-mor cell motility, invasion and metastasis (7). EGFR activation takes part in tumoral angiogenesis acti-vation by stimulation of VEGF expression. Aberrant expression of EGFR has been reported in many can-cers, including bladder cancer and has been asso-ciated with stage, grade and overall survival (2,7). It has also been associated with resistance to common cytotoxic chemotherapy in several human cancers, in-cluding bladder cancer (8). In multivariate analysis, the presence of EGFR expression in bladder cancer has been shown to be an independent predictor of invasive disease, stage progression and poor survi-val (9). EGFR immunopositivity in bladder tumor has been assessed in studies, which reported expression rates of 23% to 100% (10). EGFR dysregulation in cancer could occur by different mechanisms such as receptor overexpression, mutations, alteration in the dimerization process, and activation of autocrine growth factor loops. EGFR protein expression level is not generally considered as a reliable biomarker of anti-EGFR TKIs activity (10). EGFR inhibitors have been shown to have antiproliferative and antiangio-genic effects in preclinical models (11). In this class, gefitinib, lapatinib, and erlotinib are currently appro-ved for clinical use in several human cancers and are under evaluation in bladder cancer (Table I). Gefiti-nib leads to cell-cycle arrest in G1 phase, involving increased expression of the cyclin-dependent kinase (CDK) inhibitor p27 KIP1 and decreased expression of CDK2-4-6, cyclin D1 and D3. Similar effects are seen after erlotinib treatment (11).
Lapatinib targets both EGFR and HER2/neu by contrast to gefitinib, which is single EGFR inhibitor. Lapatinib reduces cell viability in a dose-dependent fashion in bladder cancer cell lines RT112 and J82 (12). A synergistic antitumor effect of gefitinib and lapatinib with cytotoxic agents in preclinical models was also identified. and schedule-dependent synergy was shown between lapatinib and cytotoxic drugs that are currently used in the management of metasta-tic bladder cancer. However, discrepancies between EGFR expression and response to EGFR-TKIs have been demonstrated in non small cell lung cancer. An alternative approach could be to explore downstream
actors of EGFR signalling pathway such as STAT 5A and 5B, and γ-catenins (Signal Transducers and Ac-tivators of Transcription) (13). Moreover, it has been demonstrated that some genes such as GRG1 could confer resistance to EGFR-TKI. GRG1 is upregulated in gefitinib-resistant tumors, leading to the hypothe-sis that targeting GRG1 could be a promising option in EGFR-driven tumors. Finally, it has been recently shown that sensitivity to EGFR-TKI requires E-cadherin expression in urothelial carcinoma cells (14). Unfortu-nately gefitinib associated with Gemcitabin/Cisplatin (GC) failed to demonstrate improved survival compa-red to GC or MVAC alone (15).
Targeting HER2/neu in bladder cancer
HER2/Neu (ErbB2) has been shown to be expressed in 2% to 74% of bladder tumors 10 and several studies have suggested that HER2/neu posi-tivity is associated with tumor progression (16,17). However, HER2/neu expression prognosis value re-mains controversial since in 184 patients with NMIBC and MIBC, HER2/neu expression was not found to be associated with stage, grade, or survival (9) The com-bined expression of EGFR and HER2/neu is present in 34% of tumors, thus providing some rationale for EGFR/HER2/neu inhibition (18). Lapatinib is a TKI of both EGFR and HER2/neu which demonstrated mo-dest benefit in a phase II study of pretreated bladder cancer (19).
ErbB-2 and ErbB-3 immuno-reactivity in bladder tumors has been reported to range from 20% to 56% and 11% to 30%, respectively (10). Finally, ErbB1-2 and ErbB2-3 co-expression has been recognized as an independent predictor of poor long-term survival (17).
Targeting VEGFR (vascular Endothelial Growth Factor Receptor) in bladder cancer
Angiogenesis has a critical role in bladder cancer progression and metastasis (20). VEGF gene expression has been found to be related with disea-se-specific survival in patients with locally advanced bladder cancer (21). Angiogenesis can also be quan-tified by the microvessel density (MVD) which predicts subsequent muscle invasion in NMIBC (22) and co-rrelates with tumor stage, grade and poor outcome in bladder cancer (23).
TKIs targeting VEGF signalling pathway in-clude sunitinib and sorafenib which are multi-targe-ted TKIs under evaluation in bladder cancer (Table I). Sunitinib and sorafenib are TKIs which induce the
776
TYROSINE-KINASE INHIBITORS IN THE TREATMENT OF MUSCLE INVASIVE BLADDER CANCER...777
Age
nt
Das
atin
ib
(BM
S354
825)
Lapa
tinib
(G
W57
2016
)
Sora
feni
b
Suni
tinib
(S
U11
248)
Com
mer
cial
N
ame
Spry
cel
(Bris
tol M
yers
Sq
uibb
)Ty
kerb
(Gla
xoSm
i-th
Klin
e)N
exav
ar
(Bay
er)
Sute
nt(P
fizer
)
Phas
e tri
alN
o Ph
ase
Phas
e I
Phas
e I
Phas
e II
Phas
e I
Phas
e II
Phas
e II
Phas
e II
Phas
e II
Title
of t
he c
linic
al tr
ial
- Neo
adju
vant
das
atin
ib a
nd ra
dica
l cys
tec-
tom
y fo
r TC
C o
f the
bla
dder
- Lap
atin
ib, c
ispla
tin, g
emci
tabi
n as
firs
t lin
e th
erap
y in
trea
ting
patie
nts
with
loca
lly o
r m
etas
tatic
UC
- Sor
afen
ib a
nd ra
diot
hera
py in
the
treat
-m
ent o
f inv
asiv
e bl
adde
r can
cer w
ith c
on-
serv
ativ
e in
tent
- Gem
cita
bine
and
cisp
latin
(GC
) plu
s so
ra-
feni
b in
che
mot
hera
py-n
aïve
pat
ient
s w
ith
loca
lly a
dvan
ced
or m
etas
tatic
uro
thel
ial
carc
inom
a - T
rial o
f gem
cita
bine
, car
bopl
atin
, and
so-
rafe
nib
in c
hem
othe
rapy
-naï
ve p
atie
nts
with
ad
vanc
ed/
met
asta
tic b
ladd
er c
arci
nom
a - P
hase
I stu
dy u
sing
suni
tinib
plu
s ra
diat
ion
ther
apy
for c
ance
r pat
ient
s - G
emci
tabi
ne, C
ispla
tin, a
nd S
utin
ib a
s ne
oadj
uvan
t che
mot
hera
py in
pat
ient
s w
ith
mus
cle-
inva
sive
blad
der c
ance
r- G
emza
r, C
ispla
tin, S
uniti
nb in
uro
thel
ial
canc
er- B
acill
us C
alm
ette
-Gue
rin fo
llow
ed b
y su
nitin
ib fo
r the
trea
tmen
t of h
igh-
risk
non-
mus
cle
inva
sive
low
er u
rinar
y tra
ct u
roth
elia
l ca
rcin
oma
- Sun
itini
b as
sec
ond-
line
ther
apy
in tr
eatin
g pa
tient
s w
ith lo
cally
adv
ance
d or
met
asta
tic
trans
ition
al c
ell c
ance
r of t
he u
roth
eliu
m
Purp
ose
of th
e cl
inic
al tr
ial
- Fea
sibiti
ly a
nd s
afet
y of
trea
tmen
t with
da-
satin
ib o
rally
onc
e da
ily fo
r >4
wee
ks p
rior
radi
cal c
yste
ctom
y- S
tudy
the
side
effe
cts
and
bnes
t dos
e of
la
patin
ib
- Saf
ety
profi
le a
nd m
axim
um to
lera
ted
dose
of
sor
afen
ib in
com
bina
tion
with
radi
othe
-ra
py- T
o fin
d ou
t wha
t effe
cts,
goo
d or
bad
, the
G
C a
nd s
oraf
enib
has
on
canc
er
- To
eval
uate
tim
e to
pro
gres
sion
of p
atie
nts
with
adv
ance
d or
met
asta
tic b
ladd
er c
ance
r tre
ated
with
gem
cita
bine
, car
bopl
atin
and
so
rafe
nib
- Thi
s stu
dy in
clud
e so
lid tu
mou
rs o
f the
cen
-tra
l ner
vous
sys
tem
, hea
d an
d ne
ck, t
hora
x an
d pe
lvis
- To
find
out i
f usin
g th
e co
mbi
natio
n of
sta
ndar
d ch
emot
hera
py (G
C) p
lus
the
new
ta
rget
ed p
ill (s
uniti
nib)
can
hel
p sh
rink
ther
tu
mou
r bef
ore
surg
ery
- To
eval
uate
the
obje
ctiv
e re
spon
se in
pa
tient
s w
ith a
dvan
ced/
met
asta
tic u
roth
e-lia
l can
cer w
ith th
e co
mbi
natio
n ci
spla
tin,
gem
zar,
and
suni
tib- T
o ev
alua
te th
e re
curre
nce
and
prog
ress
ion
free
surv
ival
- To
see
how
wel
l sun
itini
b w
orks
as
seco
nd-
line
ther
apy
in b
ladd
er c
ance
r
Iden
tifier
0070
6641
0062
3064
0054
4609
0071
4948
0046
1851
0043
7372
0084
7015
0082
1327
0079
4950
0079
2025
Targ
ets
BCR/
ABL
; SR
C EG
FR;
HER
2/ne
u
C-K
it;
PDG
FR;
VEG
FR
VEG
FR;
PDG
FR;
c-Ki
t
TABL
E I.
CU
RREN
TLY
CLIN
ICAL
TRI
ALS
USI
NG
TYR
OSI
NE
KIN
ASE
INH
IBIT
ORS
(TKI
S) IN
BLA
DDER
CAN
CER
.
H. Wallerand, G. Robert, J. Ch. Bernhard, et al.778
Age
nt
Vand
etan
ib(Z
D64
74)
Ever
olim
us(R
AD
001)
TKI 2
58
Erlo
tinib
(OSI
-774
)
BIBW
292
Pazo
pani
b (G
W78
6034
)
Com
mer
cial
N
ame
Zact
ima
(Astr
aZen
eca)
Afin
itor
(Nov
artis
)C
HIR
-258
(Nov
artis
)
Tarc
eva
(Roc
he)
Tovo
k(B
oehr
inge
r In
gelh
eim
)(G
laxo
Smi-
thKl
ine)
Phas
e tri
alPh
ase
II
Phas
e I
Phas
e II
Phas
e II
Phas
e II
Phas
e II
Phas
e II
Phas
e II
Phas
e II
Phas
e II
Phas
e II
Title
of t
he c
linic
al tr
ial
Suni
tinib
in tr
eatin
g pa
tient
s w
ith lo
cally
ad
vanc
ed b
ladd
er c
ance
r - P
hase
I stu
dy u
sing
suni
tinib
plu
s ra
diat
ion
ther
apy
for c
ance
r pat
ient
s
- Tria
l of m
aint
enan
ce S
U11
248
vers
us
plac
ebo
post
chem
othe
rapy
for p
atie
nts
with
ad
vanc
ed u
roth
elia
l car
cino
ma
- Ra
ndom
ized
stu
dy o
f doc
etax
el +
/-
ZD64
74 in
met
asta
tic T
CC
- D
ocet
axel
with
or w
ithou
t van
deta
nib
in
treat
ing
patie
nts
with
pre
viou
sly tr
eate
d sta
ge IV
tran
sitio
nal c
ell c
ance
r
- Eve
rolim
us (R
AD
001)
in m
etas
tatic
cel
l ca
rcin
oma
of th
e ur
othe
lium
- Saf
ety
and
effic
acy
of T
KI 2
58 in
adu
lt pa
tient
s w
ith a
dvan
ced
urot
helia
l can
cer
- Neo
adju
vant
erlo
tinib
in tr
ansit
iona
l cel
l ca
rcin
oma
- Erlo
tinib
bef
ore
and
afte
r sur
gery
in tr
ea-
ting
patie
nts
with
mus
cle-
inva
sive
blad
der
canc
er
- BIB
W29
2 in
gen
etic
ally
pre
-scre
ened
ca
ncer
s w
ith E
GFR
and
/ o
r HER
2 ge
ne
ampl
ifica
tion
- Paz
opan
ib in
trea
ting
patie
nts
with
met
as-
tatic
uro
thel
ial c
ance
r
Purp
ose
of th
e cl
inic
al tr
ial
- To
eval
uate
the
side
effe
cts
and
how
suni
tinib
wor
ks in
trea
ting
patie
nts
with
ad
vanc
ed b
ladd
er c
ance
r- T
his
study
incl
udes
sol
id tu
mou
rs o
f the
cent
ral n
ervo
us s
yste
m, h
ead
and
neck
, th
orax
and
pel
vis
- Ran
dom
ized
, blin
ded,
pla
cebo
-con
trolle
d stu
dy e
valu
atin
g th
e dr
ug fo
r mai
nten
ance
th
erap
y in
adv
ance
d bl
adde
r can
cer
- To
inve
stiga
te if
the
com
bina
tion
is m
ore
effic
ient
than
doc
etax
el a
lone
- To
see
how
wel
l the
com
bina
tion
ofva
ndet
anib
with
doc
aeta
xel w
orks
intre
atin
g pa
tient
s w
ith p
revi
ously
trea
ted
stage
IV b
ladd
er c
ance
r- T
o le
arn
the
effe
cts
of e
vero
limus
on
canc
er
- To
eval
uate
effi
cacy
and
saf
ety
of T
KI25
8 in
pat
ient
s w
ith a
dvan
ced
urot
helia
l can
cer
- To
estim
ate
the
resp
onse
rate
of p
atie
nts
with
bla
dder
can
cer t
reat
ed b
efor
ecy
stect
omy
- To
eval
uate
how
wor
ks e
rlotin
ib w
hen
give
n be
fore
and
afte
r rad
ical
cys
tect
omy
- To
estim
ate
the
resp
onse
rate
for p
atie
nts
harb
ourin
g EG
FR a
nd/o
r HER
2/ne
u ge
ne
ampl
ifica
tions
- To
study
the
side
effe
cts
and
how
wel
l pa
zopa
nib
wor
ks in
trea
ting
met
asta
tic
blad
der c
ance
r
Iden
tifier
0052
6656
0043
7372
0039
3796
0088
0334
0037
8794
0080
5129
0077
9042
6
0074
9892
0038
0029
0074
8709
0047
1536
Targ
ets
EGFR
;VE
RGFR
-2
mTO
R
FGFR
; PG
GFR
; VE
GFR
EGFR
EGFR
; H
ER2/
neu
VEG
FR-1
, -2
, -3;
PD
-G
FR; C
-Kit
TABL
E I.

TYROSINE-KINASE INHIBITORS IN THE TREATMENT OF MUSCLE INVASIVE BLADDER CANCER...
inhibition of angiogenesis but also the activation of apoptosis. Sunitinib has shown an activity both as a single agent and combined with cisplatin in bladder cancer cell lines (24). Based on sunitinib and sorafe-nib effect of progression-free survival in patients with metastatic renal cell carcinoma and on potential role of tumoral angiogenesis in bladder cancer progres-sion, these agents have been tested in bladder cancer and showed anti-tumor activity against human urothe-lial carcinoma as a single agent and in combination with cisplatin (25).
Other TKIs in bladder cancer
Several molecular pathways are involved in bladder tumorigenesis and progression and could be targeted by agents such as histone deacetylase inhibitors, proteasome inhibitors and farnesyl trans-ferase inhibitors. TKIs have been shown to be effi-cient in targeting the farnesyl transferase (FT) which is responsible for a post translational modification (farnesylation) required for proteins involved in signal transduction pathways such as Ras proteins (26). FT inhibitors include the TKIs tipifarnib and ionofarnib which showed in phase II studies only modest respon-ses (27,28).
TKI in prostate cancer
Prostate cancer (CaP) is the second leading cause of cancer mortality among men in Western Europe and in the US.5 Most of deaths are caused by metastatic, hormone-refractory prostate cancer (HRPC). Advanced or metastatic CaP is first treated
by androgen deprivation either by surgical castration (orchidectomy) or medical castration with lutenising hormone releasing antagonist (LHRH) with or without anti-androgen (29). Although these treatments result in stabilization or regression of the metastatic disease in 80% of patients (30), most of these patients will progress to HRPC (31). Progression to HRPC results in less than 50% of patients alive at 5 years. The first line treatment for HRPC is docetaxel combined with prednisone (32,33). Docetaxel-based chemothe-rapy given every 3 weeks demonstrated a significant improvement in quality of life and in overall survival compared to mitoxantrone. However, the median survival benefit remains disappointingly short (2 to 3 months) and a significant proportion of patients don’t respond to chemotherapy (32,33). For patients with docetaxel-refractory disease, there is no proven effec-tive second line therapy and new cellular targets for treatment are still needed.
Various molecules involved in cell prolifera-tion, apoptosis and angiogenesis may offer alternati-ve approaches for treating HRPC. EGFR and VEGFR are activating two of the major signal transduction pa-thways leading to cancer progression or metastasis. Tyrosine kinase inhibitors (TKIs) are interfering with these receptors, therefore they represent a promising approach for the treatment of HRPC.
EGFR and VEGFR activities in prostate cancer(Table II)
The epidermal growth factor receptor fami-ly includes EGFR or ErbB-1, Her 2/neu or ErbB-2, Her 3 or ErbB-3 and Her 4 or ErbB-4. When stimu-
779
Di Lorenzo et al. (37)
2002, Clin Cancer Res
Shah et al. (38)
2006, Prostate
Osman et al. (39)
2001, Clin Cancer Res
Receptor
ErbB-1
ErbB-1
ErbB-2
Receptor expression on prostatic cells
41% in hormone-naïve CaP
76% in anti-androgen treated CaP
100% in HRPC
OR = 6.67 in HRPC
(compared to hormone-naïve CaP)
20% in hormone-naïve CaP
67% in anti-androgen treated CaP
80% in metastatic CaP
TABLE II. EGFR EXPRESSION ON PROSTATIC CELLS DEPENDING ON EXPOSITION TOANTI-ANDROGEN THERAPY AND/OR CANCER PROGRESSION.
CaP: Prostate cancer; HRPC: Hormone refractory prostate cancer

H. Wallerand, G. Robert, J. Ch. Bernhard, et al.
lated, EGFR and ErbB-2 may activate the MAP kina-se and PI3 kinase transduction pathways that have been shown to be involved both in CaP progression and in differentiation to HRPC (34,35). Activation of EGFR signalling pathway plays an important role in the growth, proliferation, and survival of many solid tumours (36). In CaP, EGFR expression seems to be associated with disease progression and micro-vascu-lar density has been studied as a prognostic factor for aggressiveness of prostate cancer.
Di Lorenzo et al found that ErbB-1 expression increases in CaP as it becomes more aggressive (37). They compared the immunohistochemical expression of ErbB-1 in different stages of CaP. ErbB-1 expression was progressively increasing from 41% in hormone naïve CaP, to 76% in CaP treated with anti-androgen therapy, and finally to 100% in HRPC. Similarly Shah et al found that ErbB-1 expression was strongly asso-ciated with hormone refractory status (odds ratio = 6.67, p<0.001) (38).
ErbB-2 has also been shown to be over-expre-ssed in HRPC. Osman et al studied ErbB-2 expression in 45 hormone naïve primary tumours, in 34 primary tumours after androgen therapy and in 20 metastatic lesions (39). They found an over-expression of ErbB-2 in respectively 20%, 67% and 80% of patients sug-gesting that ErbB-2 expression is increasing with di-sease aggressiveness.
Finally a change from paracrine to autocrine EGFR regulation has been shown in HRPC (40).
Angiogenesis is also an important step in the progression of prostate cancer from early to advan-ced disease and is essential in metastasis of solid tu-mors (41).
Targeting EGFR in prostate cancer
The use of TKIs targeting the EGFR signalling pathway has shown inhibition of tumour growth in androgen-dependent CaP but also in HRPC (42). Se-veral TKI drugs have been investigated but only a few have reached a phase II or phase III trial.
Gefitinib (Iressa®, AstraZeneca) is targeting the ErbB-1 and is the most widely studied TKI in CaP. It has shown antitumour activity in preclinical studies with 70 to 80% growth inhibition of human prostate tumour cell line xenograft in nude mice (43). It has gone through numerous phase I monotherapy studies with a wide range of solid tumours, including CaP (44-46). Of the 19 patients with HRPC enrolled in the-se phase I studies, one had an objective tissue respon-
se with >50% decline in PSA level lasting 6.5 month, one had >50% decline in PSA lasting 2.5 month and almost all patients had pain relief with lesser medica-tion needed. Two phase II trials investigating gefiti-nib single agent activity in HRPC have been recently published. Canil et al investigated the efficacy and toxicity of gefitinib in a multi-centric randomized stu-dy (47). Forty patients with minimally symptomatic HRPC were randomly assigned to gefitinib 250mg or 500mg daily. None of the patients demonstrated a significant PSA decline or other objective measu-rable response. Nonetheless 35 patients (87%) had stabilization of PSA level lasting from 2.5 to 16.5 months. Small et al studied gefitinib 500mg daily in an open-labeled multicentric study (48). From the 40 evaluable non metastatic HRPC patients, none had a decline in PSA level >50% and only 3 had a stable PSA during the 6 months of therapy. The EGFR expre-ssion level was determined in 16 patients and most (12) showed significant staining. There was no rela-tionship between EGFR expression and PSA decline. Quality of life was also studied and wasn’t significan-tly improved by gefitinib therapy in this study.
Erlotinib (Tarceva®, Roche) is targeting EGFR (ErbB-1). It has been first introduced in relapsed non-small cell lung cancer and has demonstrated to im-prove survival when given as a single agent. Gravis et al studied the effect of erlotinib in a monocentric phase II study (49). Thirty patients with advanced or metastatic CaP were administered erlotinib 150 to 200mg daily until disease progression. Erlotinib de-monstrated a clinical benefit with an improvement in Karnofsky performance status in 40% of patients. No patient had a PSA decline but 14% had stabilization and PSA doubling time was increased in 33% of pa-tients. Gross et al investigated the association of er-lotinib and docetaxel in a multi-centric phase II study (50). Twenty-two patients were treated with docetaxel 60mg/m2 on day 1 and erlotinib 150mg on days 1 to 21. Height patients had no objective response but 6 had >50% PSA decline.
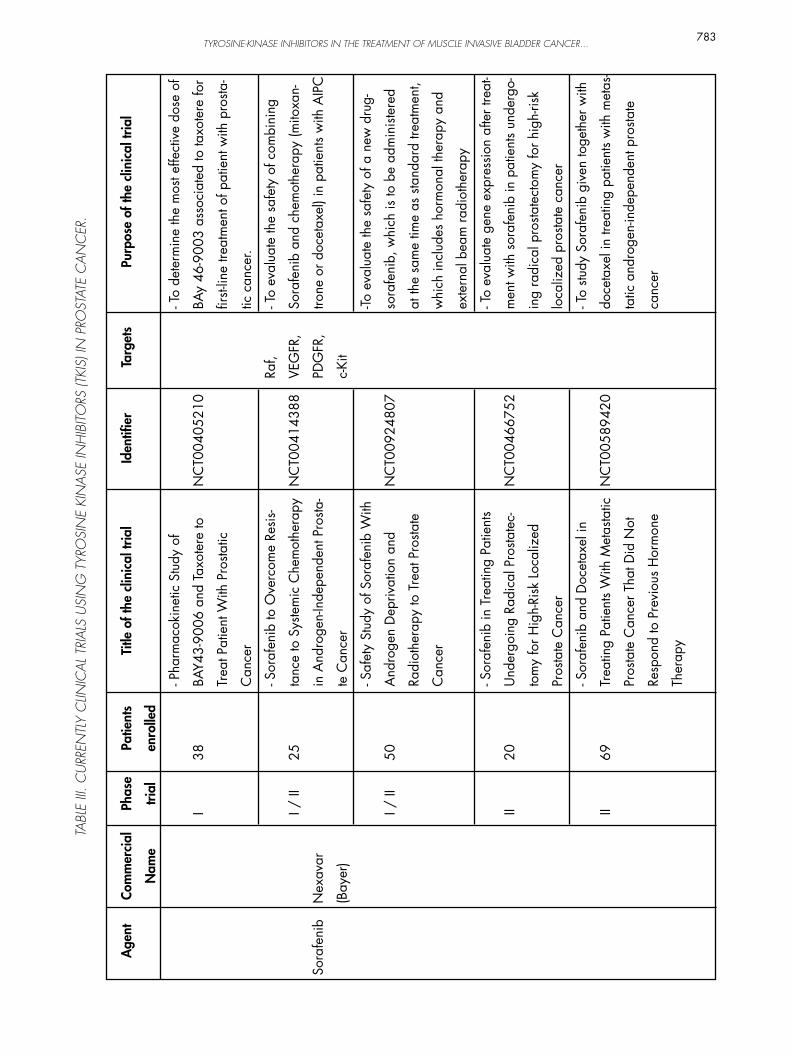
Targeting VEGFR in prostate cancer
Sorafenib (Nexavar®, Bayer) is a multi-ki-nase inhibitor targeting the Ras/Raf kinase pathway, VEGF and platelet-derived growth factor receptor. There have been numerous phase II studies in the field of HRPC. The first trial enrolled 22 HRPC patients who received 400mg twice daily during 28 days (51). None of them had PSA decline of >50% but 7 pa-tients were PSA progression-free at 4 month (31.8%). Median time to PSA progression was 8 weeks (range 6 to 41). Nonetheless authors found discordant results between PSA responses and radiographic evidences
780
TYROSINE-KINASE INHIBITORS IN THE TREATMENT OF MUSCLE INVASIVE BLADDER CANCER...781
Age
nt
Imat
inib
mes
ilate
Das
atin
ib
Com
mer
cial
N
ame
Gle
evec
(N
ovar
tis)
Spry
cel
(Bris
tol-M
yers
Sq
uibb
)
Phas
e tri
alI II II II II II II
Title
of t
he c
linic
al tr
ial
- Stu
dy C
ombi
ning
Imat
inib
M
esyl
ate
with
Sor
afen
ib in
Pa-
tient
s w
ith A
ICP
- Doc
etax
el a
nd Im
atin
ib M
esyl
a-te
in H
orm
one
Refra
ctor
y Pr
osta
-te
Can
cer
- Flu
orin
e F
18 S
odiu
m F
luor
ide
Posit
ron
Emiss
ion
Tom
ogra
phy
in
Eval
uatin
g Re
spon
se to
Das
atin
ib
in P
atie
nts
With
Pro
state
Can
cer
and
Bone
Met
asta
ses
- Das
atin
ib in
Sub
ject
s W
ith H
or-
mon
e-re
fract
ory
Pros
tate
Can
cer
- Gen
omic
Gui
ded
Ther
apy
With
Das
atin
ib o
r Nilu
tam
ide
in
Met
asta
tic C
astra
tion-
Resis
tant
Pr
osta
te C
ance
r
- Neo
adju
vant
Das
atin
ib P
lus
LHRH
Ana
logu
e Th
erap
y in
Hig
h-Ri
sk L
ocal
ized
Pro
state
Can
cer
- Das
atin
ib fo
r And
roge
n-de
pri-
ved
Prog
ress
ive
Pros
tate
Can
cer
Purp
ose
of th
e cl
inic
al tr
ial
- To
eval
uate
the
safe
ty a
nd fe
asib
ility
of
com
bini
ng G
leev
ec a
nd S
oraf
enib
- To
dete
rmin
e th
e pr
oper
dos
es o
f D
ocet
axel
and
Imat
inib
mes
ylat
e to
be
use
d to
trea
t hor
mon
e re
fract
ory
pros
tate
can
cer a
nd to
eva
luat
e th
e sa
fety
and
effi
cacy
of t
his
treat
men
t- T
o stu
dy h
ow w
ell fl
uorin
e F
18 s
o-di
um fl
uorid
e PE
T w
orks
in e
valu
atin
g re
spon
se to
das
atin
ib in
pat
ient
s w
ith
pros
tate
can
cer a
nd b
one
met
asta
ses
- To
find
out i
f das
atin
ib w
ill b
e sa
fe
and
help
ful i
n tre
atin
g pa
tient
s w
ith
horm
one-
refra
ctor
y pr
osta
te c
ance
r- T
o de
term
ine
the
clin
ical
impa
ct
of u
sing
a pa
tient
-spec
ific
geno
mic
ex
pres
sion
signa
ture
of a
ndro
gen
rece
ptor
(AR)
act
ivity
to d
eter
min
e th
erap
y fo
r pat
ient
s w
ith c
astra
tion-
re-
sista
nt m
etas
tatic
pro
state
can
cer
- To
inve
stiga
te th
e ac
tivity
of d
asat
i-ni
b pl
us L
HRH
ana
logu
e th
erap
y in
hi
gh-ri
sk lo
caliz
ed p
rosta
te c
ance
r- T
o le
arn
if m
en w
ith m
etas
tatic
pr
osta
te c
ance
r and
risin
g PS
A a
re
unde
rgoi
ng a
ndro
gen
depr
ivat
ion
resp
ond
to d
asat
inib
Iden
tifier
NC
T004
2438
5
NC
T004
2799
9
NC
T009
3697
5
NC
T005
7070
0
NC
T009
1838
5
NC
T008
6015
8
NC
T003
8558
0
Targ
ets
c-Ki
t,PD
GF
BCR/
ABL
, Sr
c
TABL
E III.
CU
RREN
TLY
CLIN
ICAL
TRI
ALS
USI
NG
TYR
OSI
NE
KIN
ASE
INH
IBIT
ORS
(TKI
S) IN
PRO
STAT
E C
ANC
ER.
Patie
nts
enro
lled
18 37 24 41 60 39 100

H. Wallerand, G. Robert, J. Ch. Bernhard, et al.782
Age
nt
Erlo
tinib
Gefi
tinib
Vata
lani
b
Suni
tinib
Com
mer
cial
N
ame
Tarc
eva
(Roc
he)
Iress
a(A
stra
Zene
-ca
)
(Nov
artis
)
Sute
nt(P
fizer
)
Phas
e tri
al
III II II I / II
II II
Title
of t
he c
linic
al tr
ial
- Ran
dom
ized
Stu
dy C
ompa
ring
Doc
etax
el P
lus
Das
atin
ib to
Do-
ceta
xel P
lus
Plac
ebo
in C
astra
-tio
n-Re
sista
nt P
rosta
te C
ance
r
- Erlo
tinib
in P
atie
nts
With
N
on-M
etas
tatic
Pro
state
Can
cer
With
a R
ising
PSA
on
Hor
mon
e Th
erap
y- D
ocet
axel
and
Erlo
tinib
in T
rea-
ting
Old
er P
atie
nts
With
Pro
state
C
ance
r
- Saf
ety
Stud
y to
Exp
lore
Com
bi-
natio
n of
Gefi
tinib
and
Rad
ioth
e-ra
py in
Non
-Met
asta
tic P
rosta
te
Can
cer
- PTK
787
in th
e Tr
eatm
ent o
f Pa
tient
s W
ith N
on-M
etas
tatic
A
ndro
gen
Inde
pend
ent P
rosta
te
Can
cer
- Sun
itini
b in
Men
With
Adv
an-
ced
Pros
tate
Can
cer
Purp
ose
of th
e cl
inic
al tr
ial
- To
dete
rmin
e w
heth
er s
urvi
val c
an b
e pr
olon
ged
in p
atie
nts
with
cas
tratio
n-re
sista
nt p
rosta
te c
ance
r who
rece
ive
dasa
tinib
in a
dditi
on to
doc
etax
el a
nd
pred
niso
ne- T
o ev
alua
te th
e ef
fect
of e
rlotin
ib o
n th
e PS
A re
spon
se ra
te in
pat
ient
s w
ith n
on-
met
asta
tic p
rosta
te c
ance
r and
a ri
sing
PSA
on
andr
ogen
dep
rivat
ion
ther
apy
- To
study
how
wel
l giv
ing
doce
taxe
l to
geth
er w
ith e
rlotin
ib w
orks
in tr
eatin
g ol
der p
atie
nts
with
pro
gres
sive
pros
tate
ca
ncer
that
has
not
resp
onde
d to
hor
mo-
ne th
erap
y- T
o es
timat
e th
e sa
fety
and
tole
rabi
lity
of 2
50 m
g ZD
1839
giv
en c
oncu
rrent
ly
with
3D
-CRT
in p
atie
nts
with
non
-met
as-
tatic
pro
state
can
cer
- To
eval
uate
PTK
787,
a d
rug
that
blo
cks
new
blo
od v
esse
l gro
wth
, in
the
treat
-m
ent o
f pat
ient
s w
ith n
on-m
etas
tatic
an
drog
en in
depe
nden
t pro
state
can
cer
- To
dete
rmin
e w
heth
er S
uniti
nib
is an
im
porta
nt th
erap
eutic
age
nt in
men
with
ad
vanc
ed p
rosta
te c
ance
r, an
d to
iden
tify
pred
ictiv
e m
arke
rs o
f ant
i-ca
ncer
Iden
tifier
NC
T007
4449
7
NC
T001
4877
2
NC
T000
8703
5
NC
T002
3929
1
NC
T001
3435
5
NC
T002
9974
1
Targ
ets
EGFR
EGFR
VEG
FR
VEG
FR,
PDG
FR,
c-Ki
t
TABL
E III.
CU
RREN
TLY
CLIN
ICAL
TRI
ALS
USI
NG
TYR
OSI
NE
KIN
ASE
INH
IBIT
ORS
(TKI
S) IN
PRO
STAT
E C
ANC
ER.
Patie
nts
enro
lled
1380
29 22 42 40 34
TYROSINE-KINASE INHIBITORS IN THE TREATMENT OF MUSCLE INVASIVE BLADDER CANCER...783
Age
nt
Sora
feni
b
Com
mer
cial
Nam
e
Nex
avar
(Bay
er)
Phas
e
trial
I I / II
I / II
II II
Title
of t
he c
linic
al tr
ial
- Pha
rmac
okin
etic
Stu
dy o
f
BAY4
3-90
06 a
nd T
axot
ere
to
Trea
t Pat
ient
With
Pro
static
Can
cer
- Sor
afen
ib to
Ove
rcom
e Re
sis-
tanc
e to
Sys
tem
ic C
hem
othe
rapy
in A
ndro
gen-
Inde
pend
ent P
rosta
-
te C
ance
r
- Saf
ety
Stud
y of
Sor
afen
ib W
ith
And
roge
n D
epriv
atio
n an
d
Radi
othe
rapy
to T
reat
Pro
state
Can
cer
- Sor
afen
ib in
Tre
atin
g Pa
tient
s
Und
ergo
ing
Radi
cal P
rosta
tec-
tom
y fo
r Hig
h-Ri
sk L
ocal
ized
Pros
tate
Can
cer
- Sor
afen
ib a
nd D
ocet
axel
in
Trea
ting
Patie
nts
With
Met
asta
tic
Pros
tate
Can
cer T
hat D
id N
ot
Resp
ond
to P
revi
ous
Hor
mon
e
Ther
apy
Purp
ose
of th
e cl
inic
al tr
ial
- To
dete
rmin
e th
e m
ost e
ffect
ive
dose
of
BAy
46-9
003
asso
ciat
ed to
taxo
tere
for
first-
line
treat
men
t of p
atie
nt w
ith p
rosta
-
tic c
ance
r.
- To
eval
uate
the
safe
ty o
f com
bini
ng
Sora
feni
b an
d ch
emot
hera
py (m
itoxa
n-
trone
or d
ocet
axel
) in
patie
nts
with
AIP
C
-To e
valu
ate
the
safe
ty o
f a n
ew d
rug-
sora
feni
b, w
hich
is to
be
adm
inist
ered
at th
e sa
me
time
as s
tand
ard
treat
men
t,
whi
ch in
clud
es h
orm
onal
ther
apy
and
exte
rnal
bea
m ra
diot
hera
py
- To
eval
uate
gen
e ex
pres
sion
afte
r tre
at-
men
t with
sor
afen
ib in
pat
ient
s un
derg
o-
ing
radi
cal p
rosta
tect
omy
for h
igh-
risk
loca
lized
pro
state
can
cer
- To
study
Sor
afen
ib g
iven
toge
ther
with
doce
taxe
l in
treat
ing
patie
nts
with
met
as-
tatic
and
roge
n-in
depe
nden
t pro
state
canc
er
Iden
tifier
NC
T004
0521
0
NC
T004
1438
8
NC
T009
2480
7
NC
T004
6675
2
NC
T005
8942
0
Targ
ets
Raf,
VEG
FR,
PDG
FR,
c-Ki
t
TABL
E III.
CU
RREN
TLY
CLIN
ICAL
TRI
ALS
USI
NG
TYR
OSI
NE
KIN
ASE
INH
IBIT
ORS
(TKI
S) IN
PRO
STAT
E C
ANC
ER.
Patie
nts
enro
lled
38 25 50 20 69

H. Wallerand, G. Robert, J. Ch. Bernhard, et al.
of bone metastasis: two patients had decrease in PSA level but radiographic evidences of metastasis progre-ssion. Moreover, from patients showing disease pro-gression after the first cycle of treatment (n=21), 13 progressed only by PSA criteria and 6 of them were found to have a spontaneous PSA decrease after the drug was discontinued (28.6%). The trail was then enlarged to 46 patients (52). Criterions for disease progression were subsequently modified and radio-graphic evidence of new metastatic lesions or progre-ssion was judged according to Response Evaluation Criteria In Solid Tumors (RECIST). PSA progression was recorded but not used as a progression criterion. Of the 24 patients enrolled in the second stage of the study, 10 had stable disease (41.6%) and the median duration of stable disease was 18 weeks (range 15 to 48). Similarly, Chi et al found only 3.6% PSA decli-ne >50% after 4 weeks of treatment (53). Both trials are suggesting that PSA is not an appropriate marker for sorafenib efficacy assessment after one cycle of treatment. Another interesting trial enrolled 55 che-mo-naïve HRPC patients to receive sorafenib 400mg twice daily continiously during 12 weeks (54). Fifteen patients showed stabilized disease after 12 weeks (27.3%) and 2 patients showed PSA decline >50% (3.6%). Median progression free survival time was 8 weeks (range 6.4 to 14.7). Among patients with stabilized disease, 11 had stabilized PSA level after 12 weeks of treatment.
Other TKIs in prostate cancer
Src family kinases (SFKs) are the largest fa-mily of nonreceptor protein tyrosine kinases and are responsible for a signal transduction during differen-ciation, adhesion and migration of malignant cells.
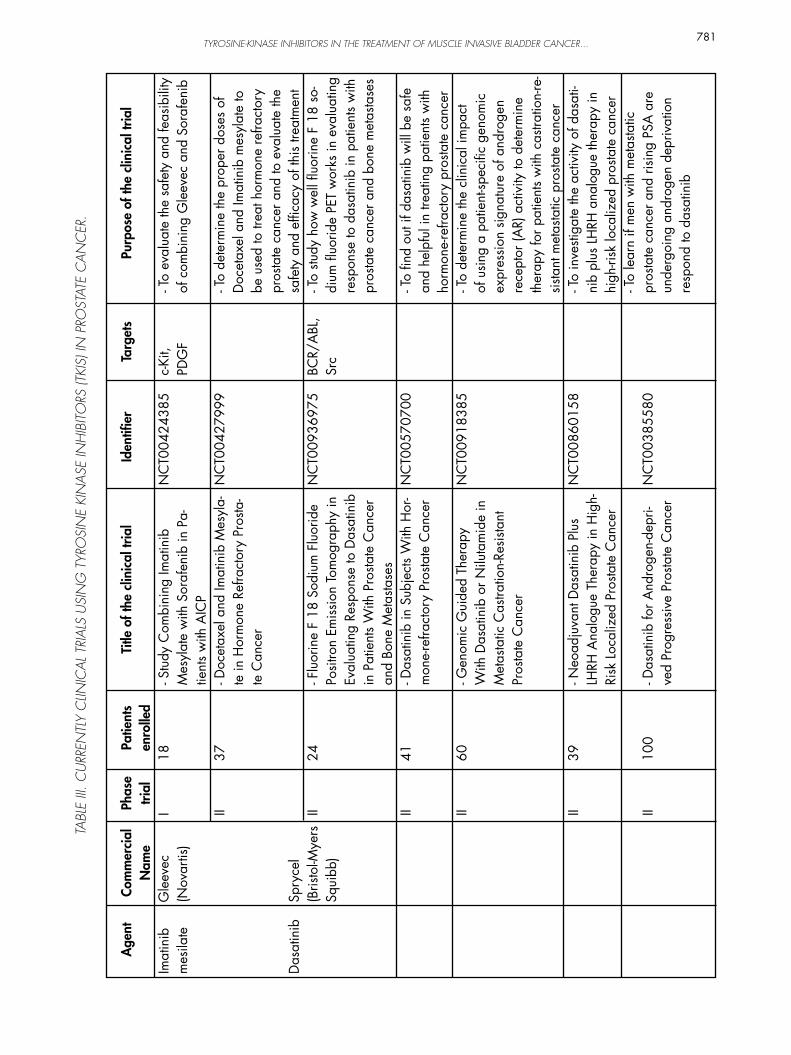
Dasatinib (Sprycel®, Bristol-Myers Squibb) is a small-molecule tyrosine kinase inhibitor blocking SFKs, platelet-derived growth factor receptor, c-kit, Bcr-Abl and ephrins (55). Preclinical studies showed that dasatinib inhibits the SFKs, Lyn and Src kinase activities in both androgen-dependent and –indepen-dent CaP. Nam et al found a correlation between inhibition of these kinase activities by dasatinib and the reduction of cell adhesion, migration and inva-sion in in-vitro model systems (56). Same effects were observed by Park et al in nude mouse models (57). Dasatinib was found to inhibit growth of lymph node metastasis of CaP. Preliminary results from a phase II study have been recently reported including 27 pa-tients with HRPC and bone metastasis who were trea-ted by dasatinib during 12 consecutive weeks. 16 had stable disease and 1 had improvement in bone scans after 12 weeks of treatment.
Vojtek AB, Hollenberg SM and Cooper JA: Ma-mmalian Ras interacts directly with the serine/threonine kinase Raf. Cell. 74: 205-14, 1993.Ciardiello F, Caputo R, Bianco R, Damiano V, Fontanini G, Cuccato S, De Placido S, Bianco AR and Tortora G: Inhibition of growth factor pro-duction and angiogenesis in human cancer cells by ZD1839 (Iressa), a selective epidermal growth factor receptor tyrosine kinase inhibitor. Clin Cancer Res. 7: 1459-65, 2001.Stommel JM, Kimmelman AC, Ying H, Nabio-ullin R, Ponugoti AH, Wiedemeyer R, Stegh AH, Bradner JE, Ligon KL, Brennan C et al.: Coacti-vation of receptor tyrosine kinases affects the res-ponse of tumor cells to targeted therapies. Scien-ce. 318: 287-90, 2007.Motzer RJ, Hutson TE, Tomczak P, Michaelson MD, Bukowski RM, Rixe O, Oudard S, Negrier S, Szczylik C, Kim ST et al.: Sunitinib versus in-terferon alfa in metastatic renal-cell carcinoma. N Engl J Med. 356: 115-24, 2007.Jemal A, Siegel R, Ward E, Hao Y, Xu J, Murray T and Thun MJ: Cancer statistics, 2008. CA Cancer J Clin. 58: 71-96, 2008.Botteman MF, Pashos CL, Redaelli A, Laskin B and Hauser R: The health economics of bladder cancer: a comprehensive review of the publis-hed literature. Pharmacoeconomics. 21: 1315-30, 2003.Baselga J and Averbuch SD: ZD1839 (‘Iressa’) as an anticancer agent. Drugs. 60 Suppl 1: 33-40; discussion 41-2, 2000.Glading A, Chang P, Lauffenburger DA and Wells A: Epidermal growth factor receptor activation of calpain is required for fibroblast motility and oc-curs via an ERK/MAP kinase signaling pathway. J Biol Chem. 275: 2390-8, 2000.Kassouf W, Black PC, Tuziak T, Bondaruk J, Lee S, Brown GA, Adam L, Wei C, Baggerly K, Bar-Eli M et al.: Distinctive expression pattern of ErbB
1.
2.
3.
4.
5.
6.
7.
8.
9.
REFERENCES AND RECOMMENDED READINGS(*of special interest, **of outstanding interest)
784
CONCLUSION
TKIs represent potential promising treatment in HRPC but phase III studies have to be designed. Multiple kinase blocking therapies may probably have a better efficiency. Until now, few targeted the-rapies are used in bladder cancer but it looks ob-vious that common chemotherapeutic agents need to be supplemented by a new generation of drugs that recognize specific targets in or on cancer cells. This new approach is promising in treating urologic malig-nancies in a near future.

Crew JP: Vascular endothelial growth factor: an important angiogenic mediator in bladder cancer. Eur Urol. 35: 2-8, 1999.Slaton JW, Millikan R, Inoue K, Karashima T, Czerniak B, Shen Y, Yang Y, Benedict WF and Dinney CP: Correlation of metastasis related gene expression and relapse-free survival in patients with locally advanced bladder cancer treated with cystectomy and chemotherapy. J Urol. 171: 570-4, 2004.Goddard JC, Sutton CD, Furness PN, O’Byrne KJ and Kockelbergh RC: Microvessel density at presentation predicts subsequent muscle invasion in superficial bladder cancer. Clin Cancer Res. 9: 2583-6, 2003.Canoglu A, Gogus C, Beduk Y, Orhan D, Tulunay O and Baltaci S: Microvessel density as a prog-nostic marker in bladder carcinoma: correlation with tumor grade, stage and prognosis. Int Urol Nephrol. 36: 401-5, 2004.Gallagher DJ and Bajorin DF: Neoadjuvant che-motherapy for the treatment of muscle-invasive bladder cancer: argument in favor. Nat Clin Pract Urol. 5: 484-5, 2008.Sonpavde G, Ross R, Powles T, Sweeney CJ, Hahn N, Hutson TE, Galsky MD, Lerner SP and Sternberg CN: Novel agents for muscle-invasi-ve and advanced urothelial cancer. BJU Int. 101: 937-43, 2008.Omerovic J, Laude AJ and Prior IA: Ras proteins: paradigms for compartmentalised and isoform-specific signalling. Cell Mol Life Sci. 64: 2575-89, 2007.Rosenberg JE, von der Maase H, Seigne JD, Mar-diak J, Vaughn DJ, Moore M, Sahasrabudhe D, Palmer PA, Perez-Ruixo JJ and Small EJ: A phase II trial of R115777, an oral farnesyl transferase in-hibitor, in patients with advanced urothelial tract transitional cell carcinoma. Cancer. 103: 2035-41, 2005.Theodore C, Geoffrois L, Vermorken JB, Caponi-gro F, Fiedler W, Chollet P, Ravaud A, Peters GJ, de Balincourt C, Lacombe D et al.: Multicentre EORTC study 16997: feasibility and phase II trial of farnesyl transferase inhibitor & gemcitabine combination in salvage treatment of advanced urothelial tract cancers. Eur J Cancer. 41: 1150-7, 2005.Heidenreich A, Aus G, Bolla M, Joniau S, Ma-tveev VB, Schmid HP and Zattoni F: EAU gui-delines on prostate cancer. Eur Urol. 53: 68-80, 2008.Wingo PA, Ries LA, Parker SL and Heath CW, Jr.: Long-term cancer patient survival in the Uni-ted States. Cancer Epidemiol Biomarkers Prev. 7: 271-82, 1998.Pilat MJ, Kamradt JM and Pienta KJ: Hormone
20.
21
22.
23.
24.
25.
26.
27.
28.
29.
30.
31.
785
10.
11.
12.
13.
14.
15.
16.
17.
18.
19.
family receptors signifies an aggressive variant of bladder cancer. J Urol. 179: 353-8, 2008.Junttila TT, Laato M, Vahlberg T, Soderstrom KO, Visakorpi T, Isola J and Elenius K: Identification of patients with transitional cell carcinoma of the bladder overexpressing ErbB2, ErbB3, or speci-fic ErbB4 isoforms: real-time reverse transcrip-tion-PCR analysis in estimation of ErbB receptor status from cancer patients. Clin Cancer Res. 9: 5346-57, 2003.Huang S, Armstrong EA, Benavente S, Chinnai-yan P and Harari PM: Dual-agent molecular tar-geting of the epidermal growth factor receptor (EGFR): combining anti-EGFR antibody with tyrosine kinase inhibitor. Cancer Res. 64: 5355-62, 2004.McHugh LA, Kriajevska M, Mellon JK and Gri-ffiths TR: Combined treatment of bladder cancer cell lines with lapatinib and varying chemothe-rapy regimens--evidence of schedule-dependent synergy. Urology. 69: 390-4, 2007.Natale RB: Biologically targeted treatment of non-small-cell lung cancer: focus on epidermal growth factor receptor. Clin Lung Cancer. 5 Suppl 1: S11-7, 2003.Black PC, Brown GA, Inamoto T, Shrader M, Arora A, Siefker-Radtke AO, Adam L, Theodo-rescu D, Wu X, Munsell MF et al.: Sensitivity to epidermal growth factor receptor inhibitor requi-res E-cadherin expression in urothelial carcinoma cells. Clin Cancer Res. 14: 1478-86, 2008.Philips GK, Halabi S, Sanford BL, Bajorin D and Small EJ: A phase II trial of cisplatin, fixed dose-rate gemcitabine and gefitinib for advanced uro-thelial tract carcinoma: results of the Cancer and Leukaemia Group B 90102. BJU Int. 101: 20-5, 2008.Chow NH, Chan SH, Tzai TS, Ho CL and Liu HS: Expression profiles of ErbB family receptors and prognosis in primary transitional cell carcinoma of the urinary bladder. Clin Cancer Res. 7: 1957-62, 2001.Kruger S, Weitsch G, Buttner H, Matthiensen A, Bohmer T, Marquardt T, Sayk F, Feller AC and Bohle A: HER2 overexpression in muscle-invasi-ve urothelial carcinoma of the bladder: prognostic implications. Int J Cancer. 102: 514-8, 2002.Bellmunt J, Hussain M and Dinney CP: Novel approaches with targeted therapies in bladder can-cer. Therapy of bladder cancer by blockade of the epidermal growth factor receptor family. Crit Rev Oncol Hematol. 46 Suppl: S85-104, 2003.Wulfing C, von Struensee D, Bierer S, Bogemann M, Hertle L and Eltze E: [Expression of Her2/neu in locally advanced bladder cancer: implication for a molecular targeted therapy]. Aktuelle Urol. 36: 423-9, 2005.
human tumor xenografts is markedly enhanced by coadministration of ZD1839 (Iressa), an inhibi-tor of EGFR tyrosine kinase. Clin Cancer Res. 6: 4885-92, 2000.Baselga J, Rischin D, Ranson M, Calvert H, Ray-mond E, Kieback DG, Kaye SB, Gianni L, Harris A, Bjork T et al.: Phase I safety, pharmacokinetic, and pharmacodynamic trial of ZD1839, a selecti-ve oral epidermal growth factor receptor tyrosine kinase inhibitor, in patients with five selected solid tumor types. J Clin Oncol. 20: 4292-302, 2002.Ranson M, Hammond LA, Ferry D, Kris M, Tullo A, Murray PI, Miller V, Averbuch S, Ochs J, Mo-rris C et al.: ZD1839, a selective oral epidermal growth factor receptor-tyrosine kinase inhibitor, is well tolerated and active in patients with solid, malignant tumors: results of a phase I trial. J Clin Oncol. 20: 2240-50, 2002.Herbst RS, Maddox AM, Rothenberg ML, Sma-ll EJ, Rubin EH, Baselga J, Rojo F, Hong WK, Swaisland H, Averbuch SD et al.: Selective oral epidermal growth factor receptor tyrosine kinase inhibitor ZD1839 is generally well-tolerated and has activity in non-small-cell lung cancer and other solid tumors: results of a phase I trial. J Clin Oncol. 20: 3815-25, 2002.Canil CM, Moore MJ, Winquist E, Baetz T, Pollak M, Chi KN, Berry S, Ernst DS, Douglas L, Brun-dage M et al.: Randomized phase II study of two doses of gefitinib in hormone-refractory prostate cancer: a trial of the National Cancer Institute of Canada-Clinical Trials Group. J Clin Oncol. 23: 455-60, 2005.Small EJ, Fontana J, Tannir N, DiPaola RS, Wil-ding G, Rubin M, Iacona RB and Kabbinavar FF: A phase II trial of gefitinib in patients with non-metastatic hormone-refractory prostate cancer. BJU Int. 100: 765-9, 2007.Gravis G, Bladou F, Salem N, Goncalves A, Es-terni B, Walz J, Bagattini S, Marcy M, Brunelle S and Viens P: Results from a monocentric phase II trial of erlotinib in patients with metastatic prosta-te cancer. Ann Oncol. 19: 1624-8, 2008.Gross M, Higano C, Pantuck A, Castellanos O, Green E, Nguyen K and Agus DB: A phase II trial of docetaxel and erlotinib as first-line therapy for elderly patients with androgen-independent pros-tate cancer. BMC Cancer. 7: 142, 2007.Dahut WL, Scripture C, Posadas E, Jain L, Gulley JL, Arlen PM, Wright JJ, Yu Y, Cao L, Steinberg SM et al.: A phase II clinical trial of sorafenib in androgen-independent prostate cancer. Clin Can-cer Res. 14: 209-14, 2008.Aragon-Ching JB, Jain L, Gulley JL, Arlen PM, Wright JJ, Steinberg SM, Draper D, Venitz J, Jo-nes E, Chen CC et al.: Final analysis of a phase II trial using sorafenib for metastatic castration-
44.
45.
46.
47.
48.
49.
50.
51.
52.
786
resistance in prostate cancer. Cancer Metastasis Rev. 17: 373-81, 1998.Tannock IF, de Wit R, Berry WR, Horti J, Pluzans-ka A, Chi KN, Oudard S, Theodore C, James ND, Turesson I et al.: Docetaxel plus prednisone or mitoxantrone plus prednisone for advanced pros-tate cancer. N Engl J Med. 351: 1502-12, 2004.Petrylak DP, Tangen CM, Hussain MH, Lara PN, Jr., Jones JA, Taplin ME, Burch PA, Berry D, Mo-inpour C, Kohli M et al.: Docetaxel and estramus-tine compared with mitoxantrone and prednisone for advanced refractory prostate cancer. N Engl J Med. 351: 1513-20, 2004.Edwards J, Krishna NS, Witton CJ and Bartlett JM: Gene amplifications associated with the de-velopment of hormone-resistant prostate cancer. Clin Cancer Res. 9: 5271-81, 2003.Gioeli D, Mandell JW, Petroni GR, Frierson HF, Jr. and Weber MJ: Activation of mitogen-activa-ted protein kinase associated with prostate cancer progression. Cancer Res. 59: 279-84, 1999.Yarden Y: The EGFR family and its ligands in hu-man cancer. signalling mechanisms and therapeu-tic opportunities. Eur J Cancer. 37 Suppl 4: S3-8, 2001.Di Lorenzo G, Tortora G, D’Armiento FP, De Rosa G, Staibano S, Autorino R, D’Armiento M, De Laurentiis M, De Placido S, Catalano G et al.: Expression of epidermal growth factor receptor correlates with disease relapse and progression to androgen-independence in human prostate cancer. Clin Cancer Res. 8: 3438-44, 2002.Shah RB, Ghosh D and Elder JT: Epidermal growth factor receptor (ErbB1) expression in pros-tate cancer progression: correlation with androgen independence. Prostate. 66: 1437-44, 2006.Osman I, Scher HI, Drobnjak M, Verbel D, Morris M, Agus D, Ross JS and Cordon-Cardo C: HER-2/neu (p185neu) protein expression in the natural or treated history of prostate cancer. Clin Cancer Res. 7: 2643-7, 2001.Scher HI, Sarkis A, Reuter V, Cohen D, Netto G, Petrylak D, Lianes P, Fuks Z, Mendelsohn J and Cordon-Cardo C: Changing pattern of expression of the epidermal growth factor receptor and trans-forming growth factor alpha in the progression of prostatic neoplasms. Clin Cancer Res. 1: 545-50, 1995.Hanahan D and Folkman J: Patterns and emerging mechanisms of the angiogenic switch during tu-morigenesis. Cell. 86: 353-64, 1996.Mimeault M, Pommery N and Henichart JP: New advances on prostate carcinogenesis and thera-pies: involvement of EGF-EGFR transduction system. Growth Factors. 21: 1-14, 2003.Sirotnak FM, Zakowski MF, Miller VA, Scher HI and Kris MG: Efficacy of cytotoxic agents against
32.
33.
34.
35.
36.
37.
38.
39.
40.
41.
42.
43.
resistant prostate cancer. BJU Int. 103: 1636-40, 2009.Chi KN, Ellard SL, Hotte SJ, Czaykowski P, Mo-ore M, Ruether JD, Schell AJ, Taylor S, Hansen C, Gauthier I et al.: A phase II study of sorafenib in patients with chemo-naive castration-resistant prostate cancer. Ann Oncol. 19: 746-51, 2008.Steinbild S, Mross K, Frost A, Morant R, Gi-llessen S, Dittrich C, Strumberg D, Hochhaus A, Hanauske AR, Edler L et al.: A clinical phase II study with sorafenib in patients with progressive hormone-refractory prostate cancer: a study of the CESAR Central European Society for Anticancer Drug Research-EWIV. Br J Cancer. 97: 1480-5, 2007.Lombardo LJ, Lee FY, Chen P, Norris D, Ba-rrish JC, Behnia K, Castaneda S, Cornelius LA, Das J, Doweyko AM et al.: Discovery of N-(2-chloro-6-methyl- phenyl)-2-(6-(4-(2-hydroxye-thyl)- piperazin-1-yl)-2-methylpyrimidin-4- ylamino)thiazole-5-carboxamide (BMS-354825), a dual Src/Abl kinase inhibitor with potent anti-tumor activity in preclinical assays. J Med Chem. 47: 6658-61, 2004.Nam S, Kim D, Cheng JQ, Zhang S, Lee JH, Bue-ttner R, Mirosevich J, Lee FY and Jove R: Ac-tion of the Src family kinase inhibitor, dasatinib (BMS-354825), on human prostate cancer cells. Cancer Res. 65: 9185-9, 2005.Park SI, Zhang J, Phillips KA, Araujo JC, Najjar AM, Volgin AY, Gelovani JG, Kim SJ, Wang Z and Gallick GE: Targeting SRC family kinases in-hibits growth and lymph node metastases of pros-tate cancer in an orthotopic nude mouse model. Cancer Res. 68: 3323-33, 2008.
53.
54.
55.
56.
57.
787