triage, stabilization, and therapeutic considerations in shock · triage • triage is derived from...
TRANSCRIPT
In the first 15 minutes…
Triage, Stabilization, and Therapeutic Considerations in Shock
Rebecca Walton, DVM, DACVECC Clinical Assistant Professor of Emergency and Critical Care
ISU-IVS Partners in Progress CE Event April 3, 2019
Outline
• Shock • Triage assessment • Initial diagnostics • Stabilization and fluid resuscitation
Shock – definition
• Shock is defined as a state of cellular and tissue hypoxia secondary to: – Reduced tissue perfusion – Decrease in oxygen delivery – Increase in oxygen consumption – Inadequate oxygen utilization
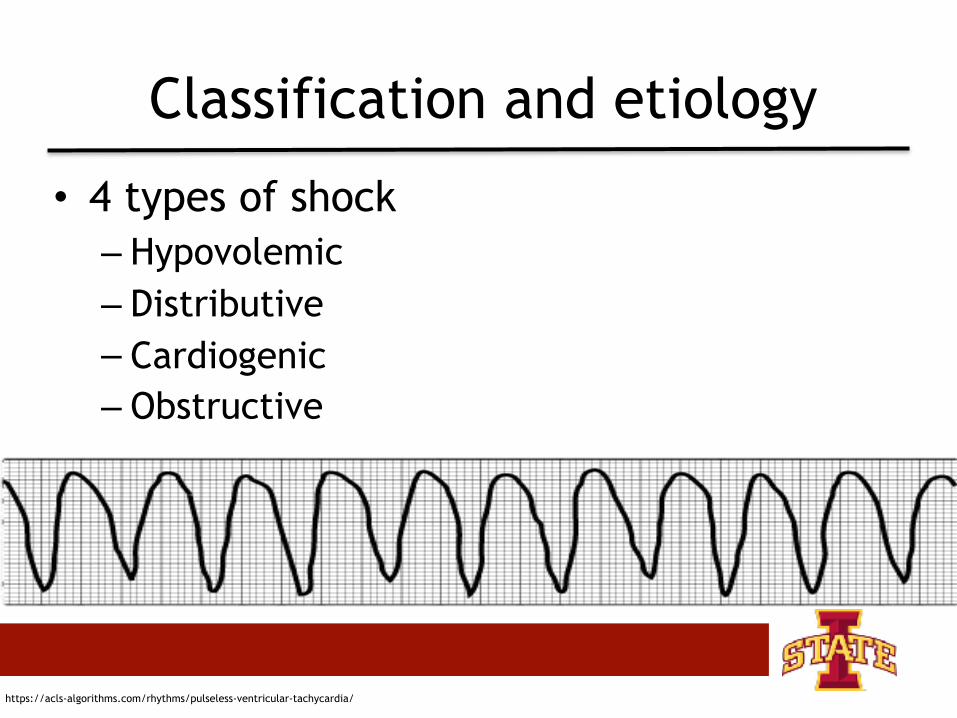
Classification and etiology
• 4 types of shock – Hypovolemic – Distributive – Cardiogenic – Obstructive
https://acls-algorithms.com/rhythms/pulseless-ventricular-tachycardia/
Hypovolemic shock
• Decreased intravascular volume
• 2 main categories – Hemorrhagic – Non-hemorrhagic • Gastrointestinal loss • Renal loss • Third space • Skin loss
Distributive shock
• Characterized by severe peripheral vasodilation
• Underlying etiology – Septic shock – Systemic inflammatory
response syndrome – Neurogenic shock – Anaphylactic shock – Drug/toxin – Endocrine shock

Cardiogenic shock
• Intra-cardiac causes of cardiac pump failure resulting in decreased cardiac output
• Categories – Cardiomyopathic – Arrhythmic – Mechanical
https://www.merckmanuals.com/professional/cardiovascular-disorders/arrhythmias-and-conduction-disorders/atrioventricular-block
Obstructive shock
• Extra-cardiac causes of cardiac pump failure and are associated with decreased right ventricular filling and poor right sided cardiac output
• Categories – Pulmonary – Mechanical
http://www.coolspringsah.com/our-blog/2014/6/18/seriously-scary-gdv
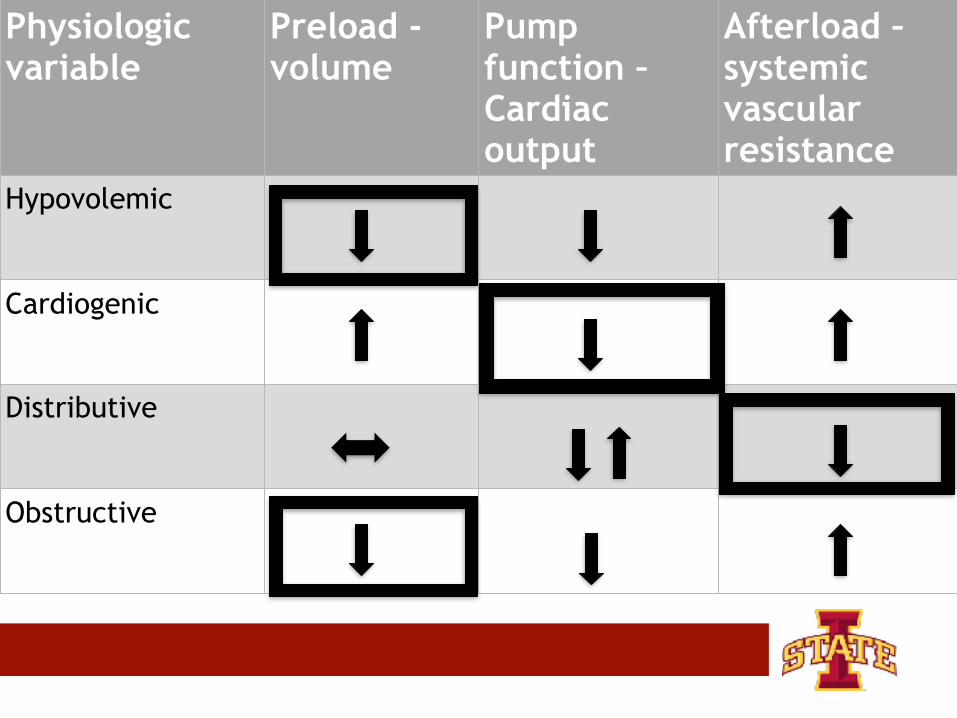
Physiologic variable
Preload - volume
Pump function – Cardiac output
Afterload – systemic vascular resistance
Hypovolemic
Cardiogenic
Distributive
Obstructive
Compensatory mechanisms
• Mobilization of fluid from the interstitial space to the intravascular space
• Activation of the sympathetic nervous system – Increase heart rate/blood pressure
• Activation of the renin-angiotensin aldosterone system – Regulate blood pressure – Fluid retention
• Release of anti-diuretic hormone – Water reabsorption
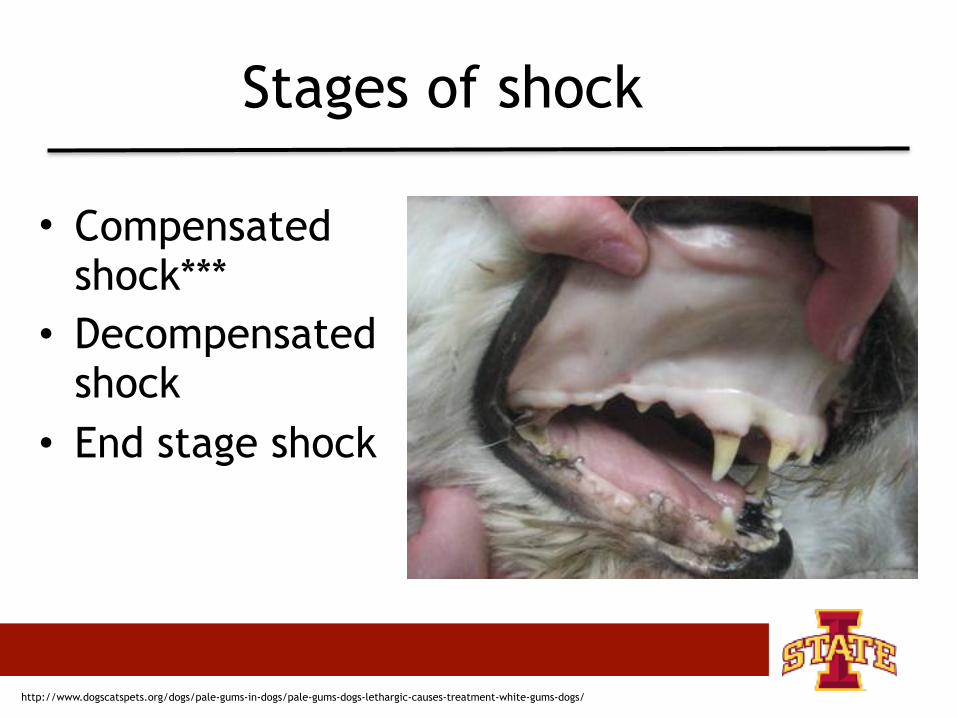
Stages of shock
• Compensated shock***
• Decompensated shock
• End stage shock
http://www.dogscatspets.org/dogs/pale-gums-in-dogs/pale-gums-dogs-lethargic-causes-treatment-white-gums-dogs/
Stages of shock - compensated
• Compensatory mechanisms – Increased cardiac output – Tachycardia – Fluid retention
Stages of shock - decompensated
• Compensatory mechanisms are overwhelmed
• Hypotension • Pale mucous membranes • Poor pulse quality • Signs of organ dysfunction occur
Stages of shock - end stage
• Irreversible organ damage • Multiple organ failure • Systemic acidemia • Hypotension
Clinical signs
• Compensated shock – Pale mucous membranes – Prolonged CRT – Cold extremities – Tachycardia – Dull mentation – Blood pressure usually NORMAL
Clinical signs
• Decompensated shock – Local tissue beds begin to vasodilate – Vasodilation leads to blood pooling • Maldistribution
– Grey mucous membranes – Bradycardia – Hypotension – Altered mentation
Clinical signs – cats
• Unique challenge – they do not display classic signs of shock like dogs
• Clinical signs – Bradycardia – Hypothermia – Hypotension – **even in the early stages of shock**
Triage
• Triage is derived from the French work trier – Refers to the sorting of all patients for
treatment priority • Triage refers to a systemic evaluation of
body systems and is designed to facilitate identification of the most life threatening problems first
• Patients with life threatening abnormalities require timely intervention
Triage history
• The formal concept of triage began in the late 1700’s when two French surgeons were faced with massive casualties associated with the European wars
Triage systems – human medicine
• Triage systems have been used in people to improve the acuity of triage
• 5 level system – Resuscitation – Emergent – Urgent – Less urgent – Non-urgent
• System is generally based on vital signs and presenting complaints
“Undertriaging”
• ~30% of human patients ‘stable’ on admission with normal vitals deteriorate 2-24 hours after admission
• Triage scoring systems aim to – Predict survival – Determine severity of illness to prioritize
treatment
Triage – veterinary
• Used to describe the sorting of animals in the emergency department or general practice based on medical priority – Sickest treated first
• Rapid, accurate triage is essential
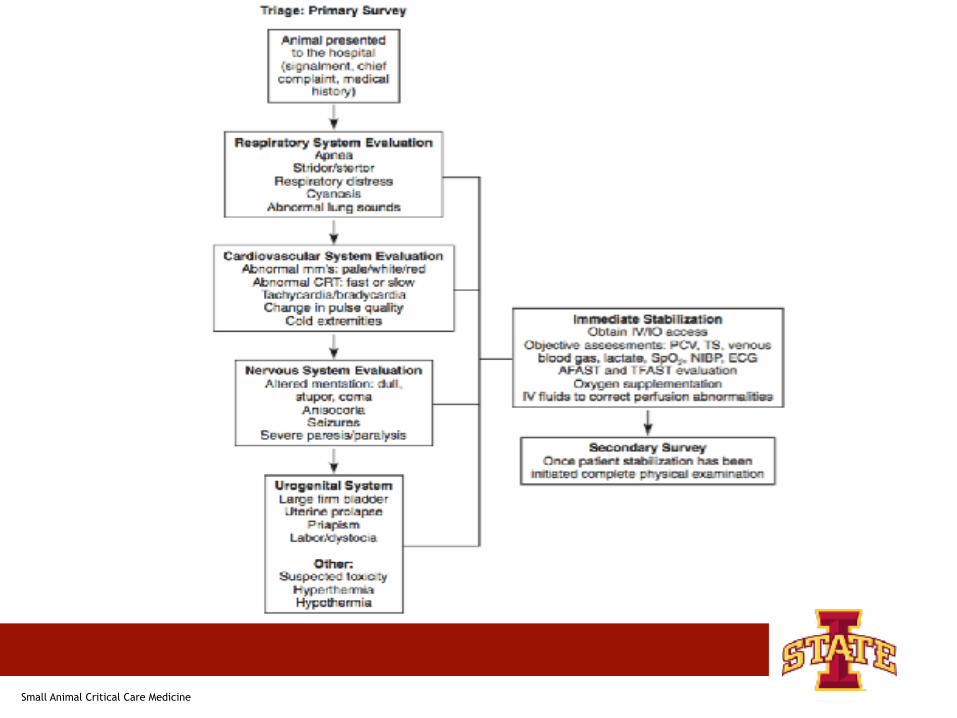
Initial assessment
• Cardiovascular • Respiratory • Nervous • Urogenital systems
• PRIMARY SURVEY
Secondary survey
• Evaluates systems from the primary survey in more depth – Thoracic auscultation – Additional assessments • Abdominal palpation
– Performed at a slower pace – Nose to tail physical exam
Triage exam
• Proper triage exam should take no more than 2 minutes
Triage exam
• On arrival to the hospital this triage assessment should be performed
• TRIAGE EXAM SHOULD BE PERFORMED ON EVERY PATIENT
• Brief history – Signalment – Presenting complaint
• Triage exam
Other conditions that warrant immediate evaluation even if the triage exam deems the patient stable
– Severe pain – Recent toxin ingestion – Signs of intoxication – Recent seizures – Trauma – Active bleeding
– Hyperthermia/hypothermia – Open wounds – Fractures – Burns – Dystocia
Other
Triage
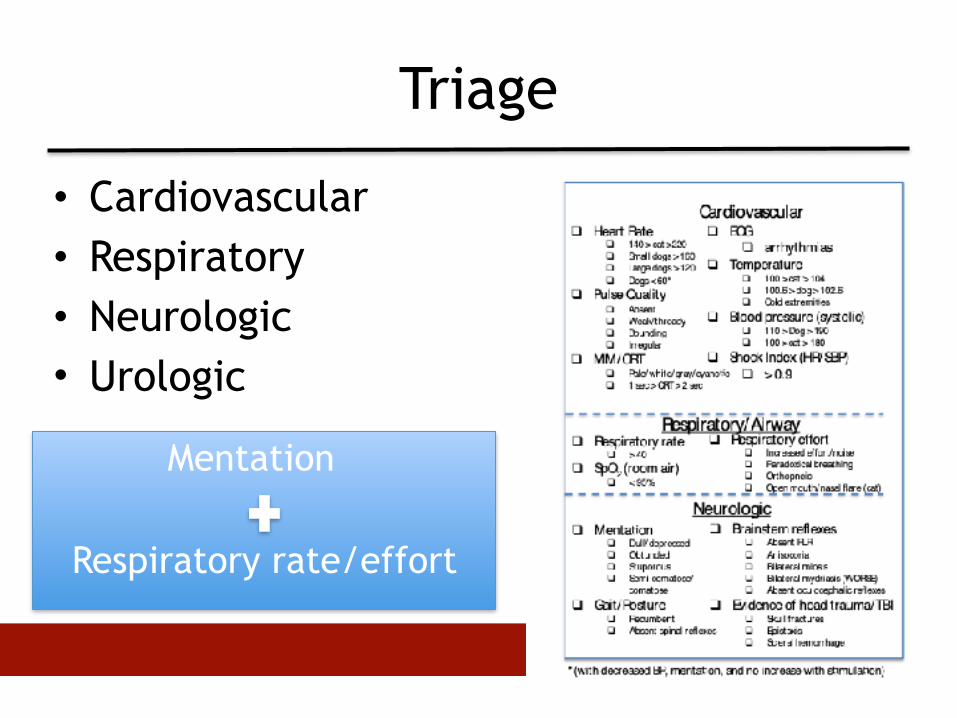
• Cardiovascular • Respiratory • Neurologic • Urologic
Mentation
Respiratory rate/effort

Triage – cardiovascular
• Purpose – Identify poor tissue perfusion and decreased
tissue oxygen delivery
• Without rapid identification of inadequate tissue perfusion – Critical tissue hypoxia – Multiple organ dysfunction – Death
Triage - cardiovascular• Heart rate • Pulse quality – Femoral/Dorsal pedal
• Temperature – Rectal and extremities
• MM/CRT
• ECG
• Doppler Blood Pressure
Normals: • Heart rate
• Dog: 60-120 • Cat: 160-220
• Temperature • 99.5 – 102.5 F
• Mucous membranes • Pink
• Capillary refill time • 1-2 seconds
Alterations in sympathetic tone • Volume deficit • Oxygen deficit • Pain/anxiety = stress • Cardiac dysfunction
Triage - cardiovascular• HR • Pulse Quality – Femoral/Dorsal pedal
• Temperature – Rectal and extremities
• MM/CRT
• ECG
• Doppler Blood Pressure
Normals: • HR
• Dog: 60-120 • Cat: 160-220
• Temp • 99.5 – 102.5
• MM • Pink
• CRT • 1-2 seconds
Alterations in sympathetic tone • Volume deficit • Oxygen deficit • Pain/anxiety = stress • Cardiac dysfunction
Tachycardic rule-outs • Type
• Sinus vs. supraventricular vs. ventricular tachycardia
• Cause • Hypovolemia • Hypoxemia • Anemia • Cardiac disease • Pain/anxiety/stress/drugs
Triage - cardiovascular• HR • Pulse Quality – Femoral/Dorsal pedal
• Temperature – Rectal and extremities
• MM/CRT
• ECG
• Doppler Blood Pressure
Normals: • Heart rate
• Dog: 60-120 • Cat: 160-220
• Temperature • 99.5 – 102.5 F
• Mucous membranes • Pink
• Capillary refill time • 1-2 seconds
Alterations in sympathetic tone • Volume deficit • Oxygen deficit • Pain/anxiety = stress • Cardiac dysfunction
Bradycardic goodness • Associated with normal cardiac output
• Normothermia, normotension • Increases with stimulation • Resting sinus arrhythmia
Bradycardic badness • Associated with ! cardiac output
• Hypothermia, hypotension • Unable to increase HR with sympathetic
stimulation • Associated with high BP, dull mentation
(Cushing reflex)
Pulse quality
• Pulse quality – Location
• Femoral + " systolic 60 mmHg • Dorsal pedal + " systolic 90 mmHg
– Width: systolic – diastolic pressure
Normal Thready
Indirect BP measurement
• Doppler – More sensitive measure of systolic pressure • Correlates more with MAP in cats
– Preferred method in patients with low blood pressure/ arrhythmias
• Oscillometric – More sensitive measure of mean pressure – Preferred method in anesthetized patients
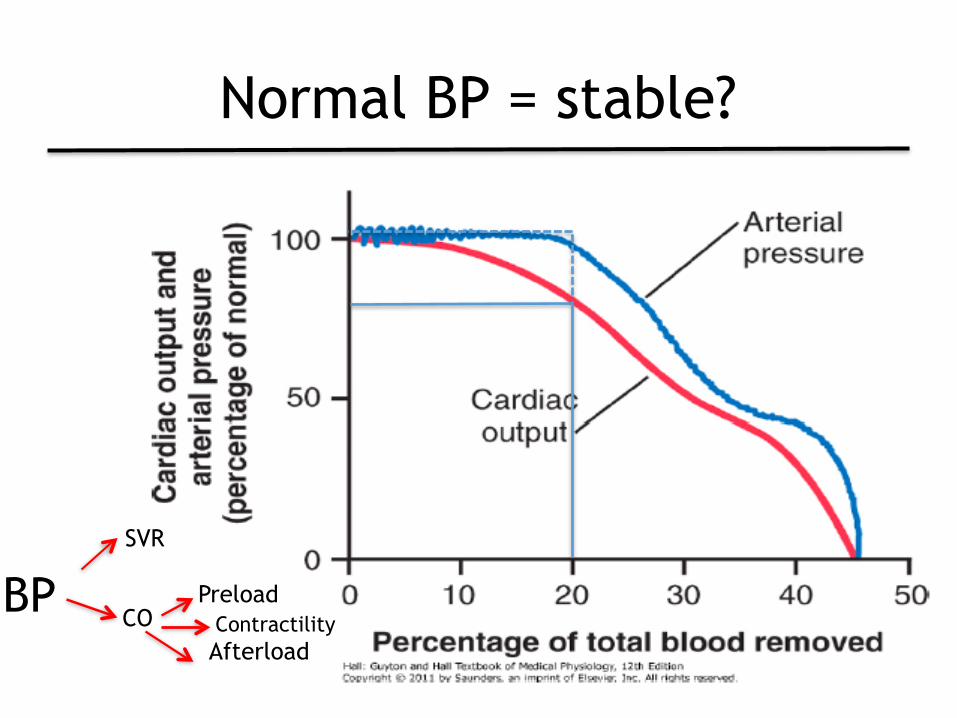
Normal BP = stable?
BPCO
SVR
Preload
AfterloadContractility
Triage - cardiovascular
• Shock Index (SI) – SI = heart Rate (HR) / systolic blood pressure
(BP)
• Advantages – Sensitive marker of compensatory shock • Detect perfusion deficits despite normal HR, BP
– SI > 0.9 • Differentiate dogs in hemorrhagic shock from
stable dogs
Cardiac auscultation
• Evaluation – Heart rate – Rhythm – Murmur – Muffled heart sounds
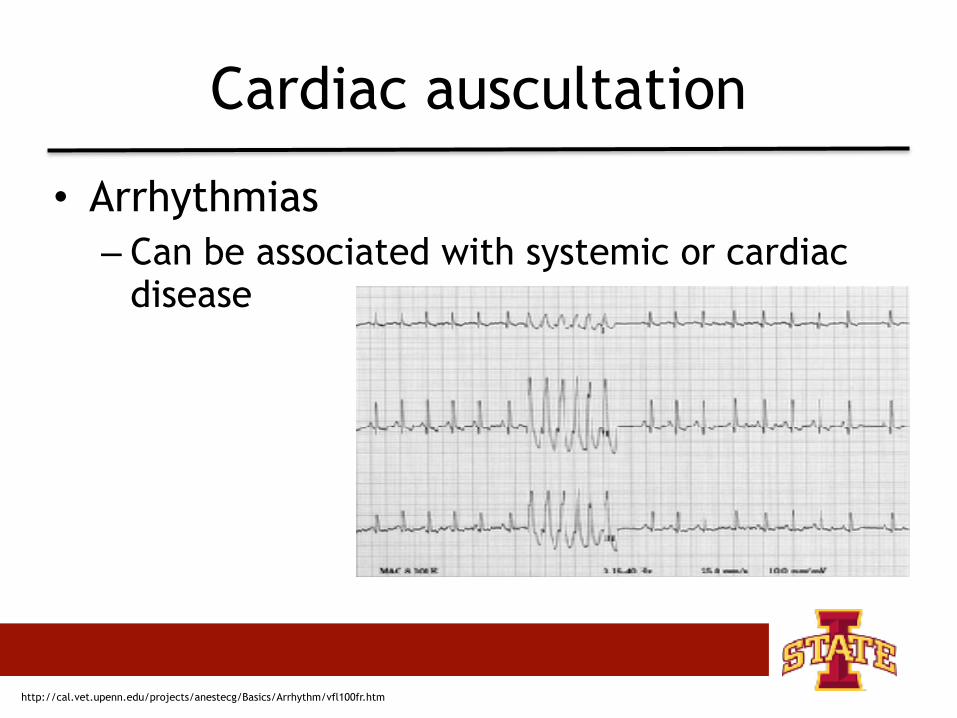
Cardiac auscultation
• Arrhythmias – Can be associated with systemic or cardiac
disease
http://cal.vet.upenn.edu/projects/anestecg/Basics/Arrhythm/vfl100fr.htm
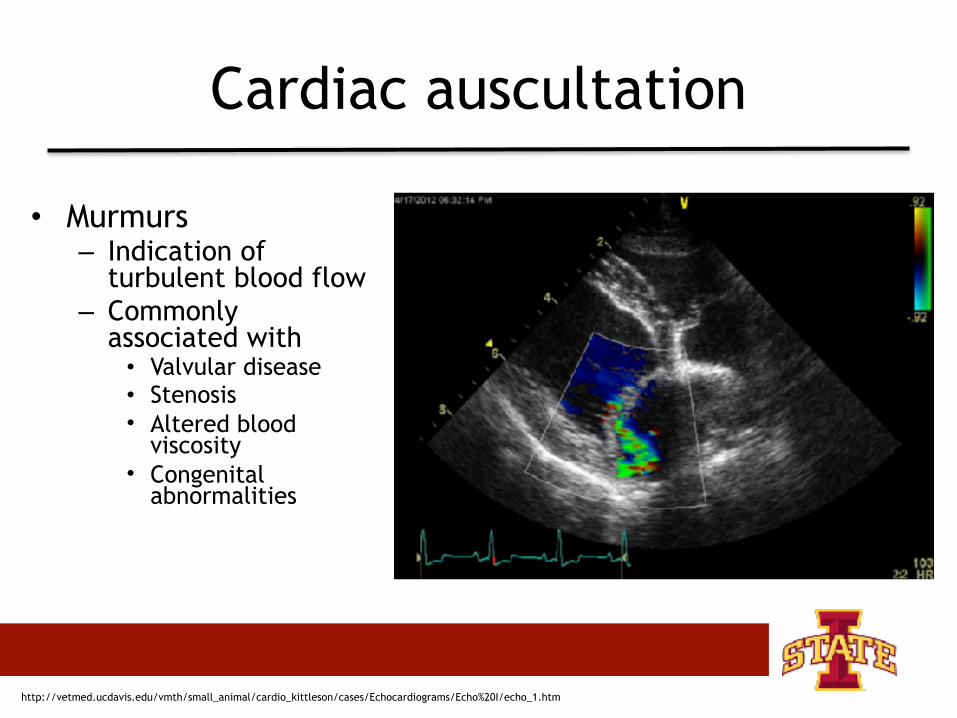
Cardiac auscultation
• Murmurs – Indication of
turbulent blood flow – Commonly
associated with • Valvular disease • Stenosis • Altered blood
viscosity • Congenital
abnormalities
http://vetmed.ucdavis.edu/vmth/small_animal/cardio_kittleson/cases/Echocardiograms/Echo%20I/echo_1.htm
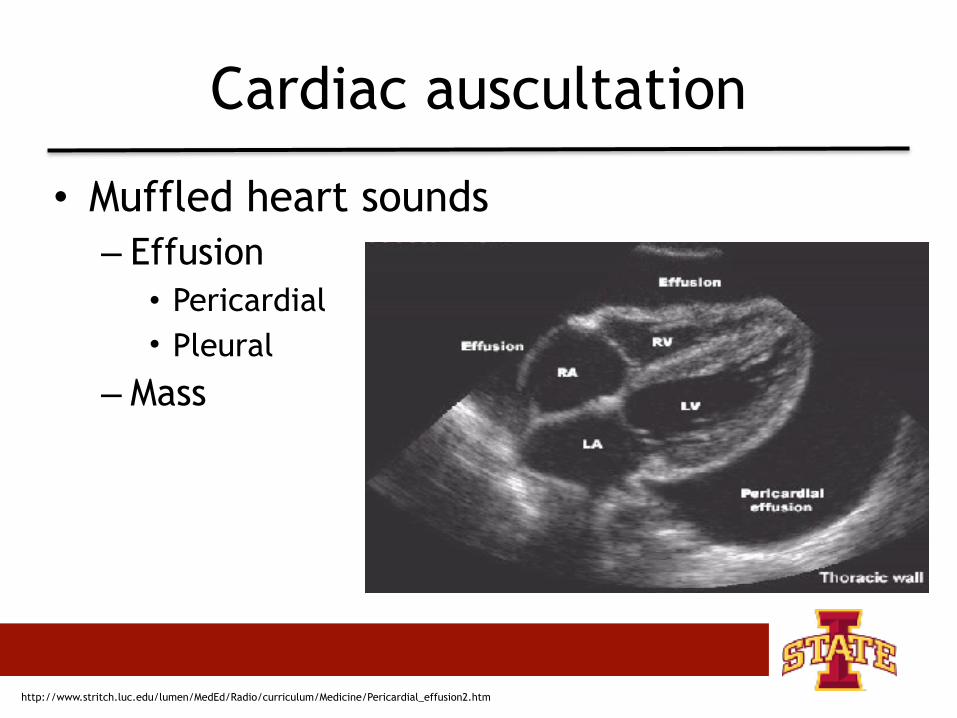
Cardiac auscultation
• Muffled heart sounds – Effusion • Pericardial • Pleural
– Mass
http://www.stritch.luc.edu/lumen/MedEd/Radio/curriculum/Medicine/Pericardial_effusion2.htm
Mucous membrane color
• Cyanosis • Pallor • Injected • Petechiation/ecchymosis
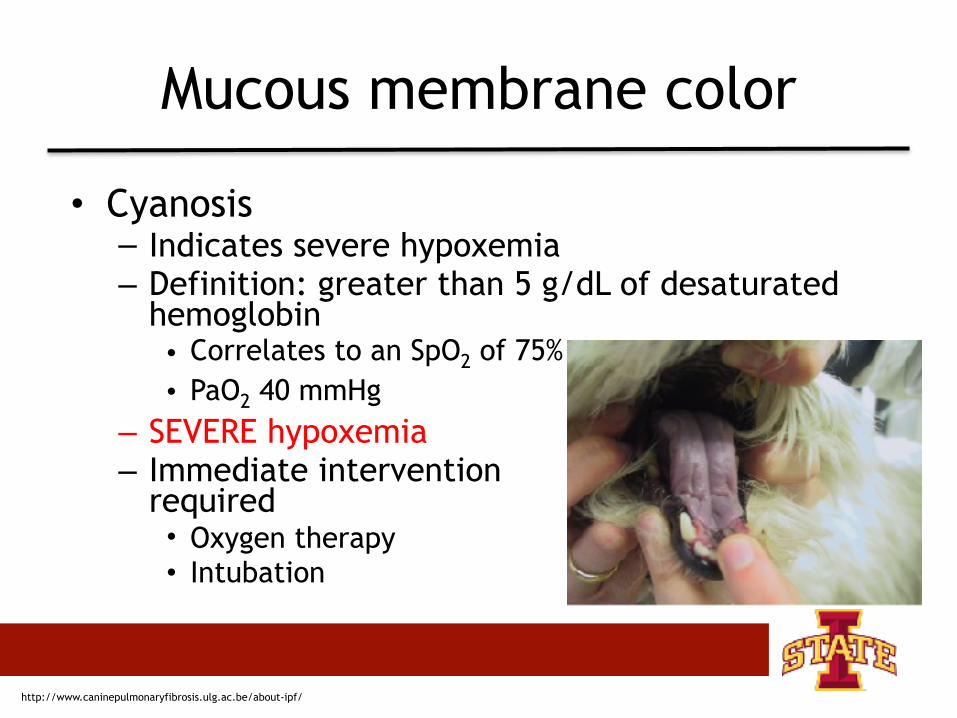
Mucous membrane color
• Cyanosis – Indicates severe hypoxemia – Definition: greater than 5 g/dL of desaturated
hemoglobin • Correlates to an SpO2 of 75% • PaO2 40 mmHg
– SEVERE hypoxemia – Immediate intervention
required • Oxygen therapy • Intubation
http://www.caninepulmonaryfibrosis.ulg.ac.be/about-ipf/
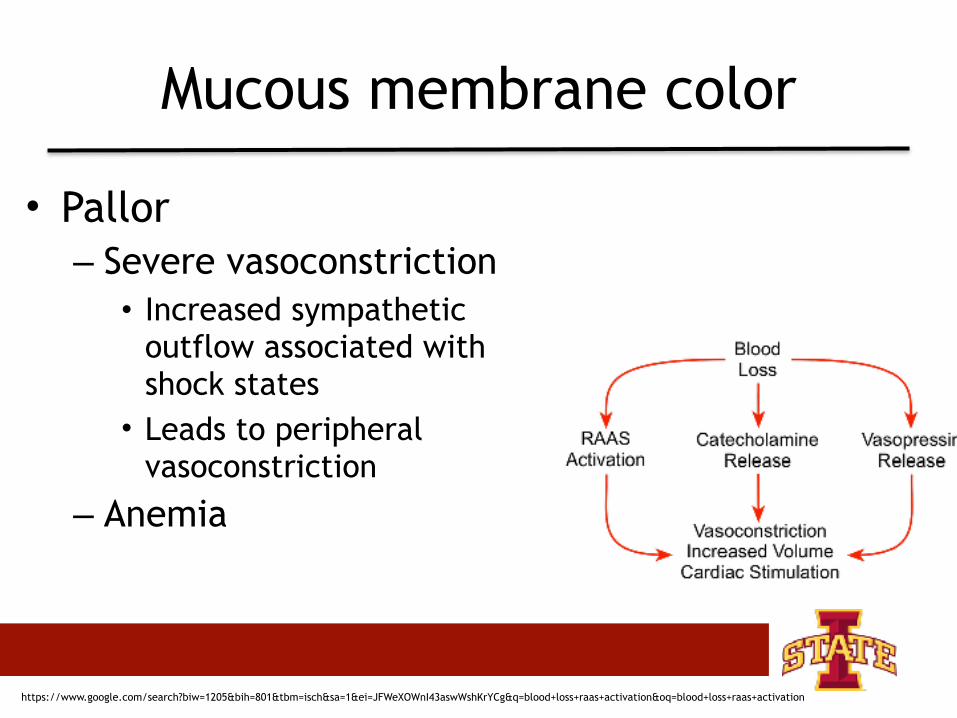
Mucous membrane color
• Pallor – Severe vasoconstriction • Increased sympathetic
outflow associated with shock states • Leads to peripheral
vasoconstriction
– Anemia
https://www.google.com/search?biw=1205&bih=801&tbm=isch&sa=1&ei=JFWeXOWnI43aswWshKrYCg&q=blood+loss+raas+activation&oq=blood+loss+raas+activation
Mucous membrane color
• Injected/red mucous membranes – Decreased cellular oxygen utilization • Cyanide
– Severe vasodilation
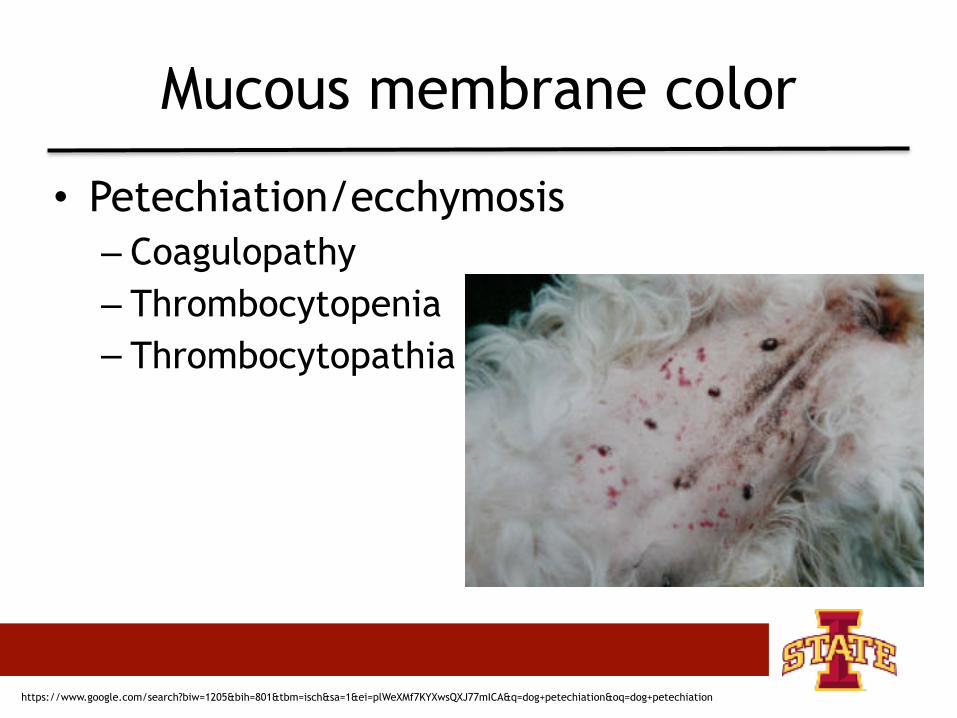
Mucous membrane color
• Petechiation/ecchymosis – Coagulopathy – Thrombocytopenia – Thrombocytopathia
https://www.google.com/search?biw=1205&bih=801&tbm=isch&sa=1&ei=plWeXMf7KYXwsQXJ77mICA&q=dog+petechiation&oq=dog+petechiation
Capillary refill time
• Assessment of perfusion – Blanch mucous membranes
• Slow refill " high arteriolar tone – VASOCONSTRICTION
• Rapid refill " low arteriolar tone – VASODILATION
• Slow refill time – Low cardiac output
• Rapid refill time – Distributive shock – Sepsis/SIRS
Triage -respiratory
• Evaluation should be focused on determining the presence or absence of – Hypoxemia – Hypoventilation
• Assessment of respiratory rate and effort • Airway patency should be assessed – Obstruction - exaggerated effort – Lower respiratory disease – prolonged
expiration
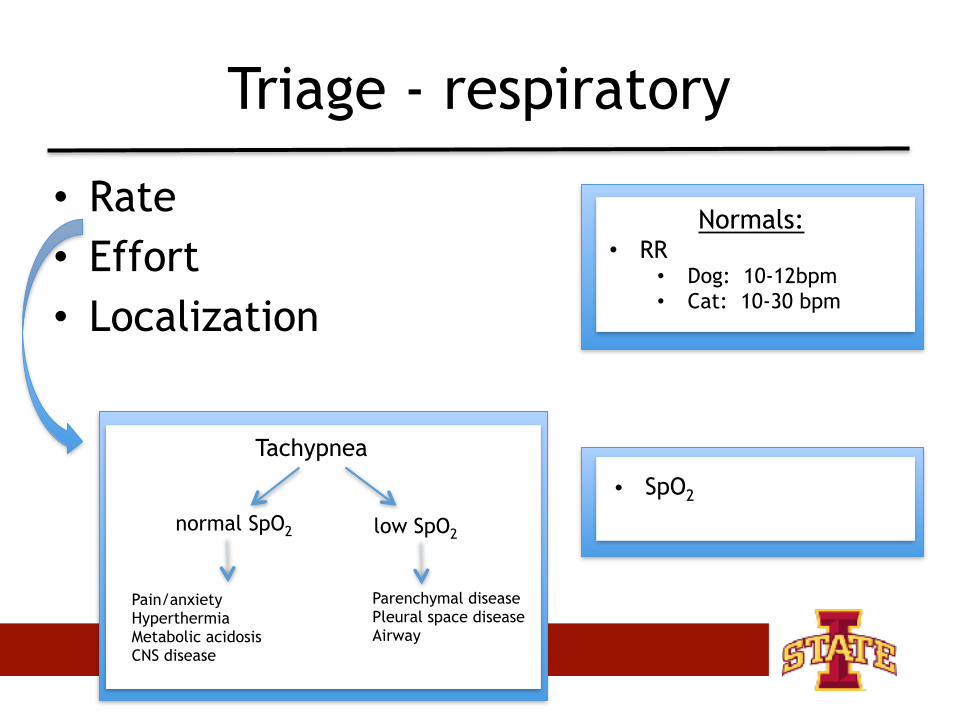
Triage - respiratory
• Rate • Effort • Localization
Normals: • RR
• Dog: 10-12bpm • Cat: 10-30 bpm
• SpO2
Tachypnea
normal SpO2 low SpO2
Pain/anxiety Hyperthermia Metabolic acidosis CNS disease
Parenchymal disease Pleural space disease Airway
Pulse oximetry
• Surrogate marker of PaO2
– Hgb saturation with oxygen is directly correlated with SpO2
• Provides no marker of oxygen delivery • Tends to underestimate when > 90% and
overestimate when < 80%
Feline respiratory evaluation
• Unique feline considerations • Clinical signs
– Increased respiratory rate/effort – Open mouth breathing
• Minor manipulations may result in decompensation – Physical exam – Intravenous catheter placement
• May benefit from being placed immediately in oxygen
• Sedation
Pulmonary auscultation
• Perform auscultation in all lung fields • Help identify pulmonary disease
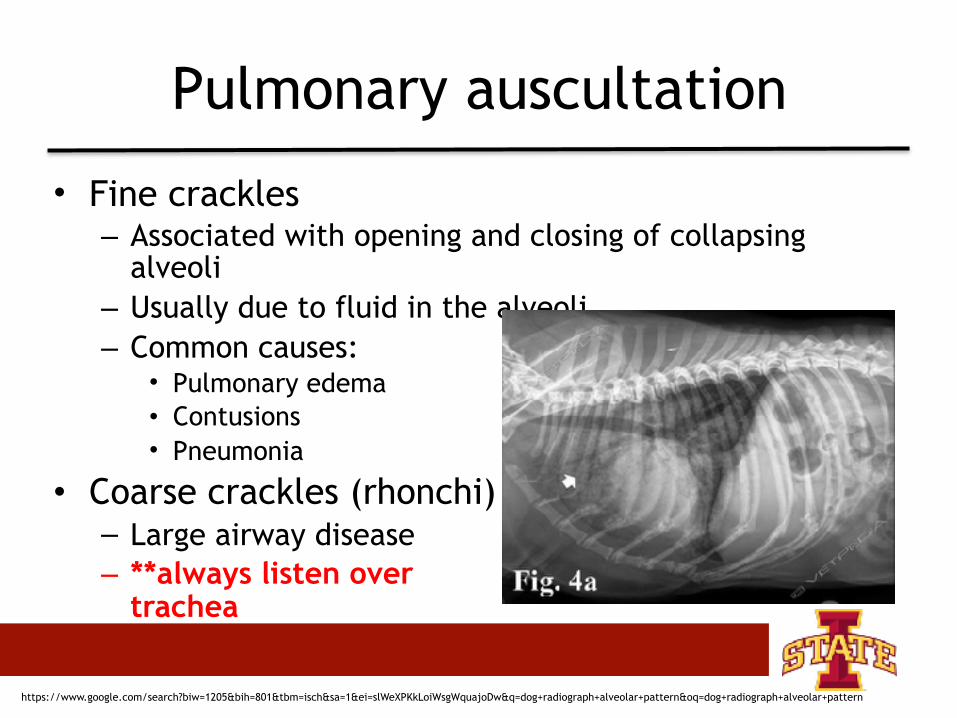
Pulmonary auscultation
• Fine crackles – Associated with opening and closing of collapsing
alveoli – Usually due to fluid in the alveoli – Common causes:
• Pulmonary edema • Contusions • Pneumonia
• Coarse crackles (rhonchi) – Large airway disease – **always listen over
trachea
https://www.google.com/search?biw=1205&bih=801&tbm=isch&sa=1&ei=slWeXPKkLoiWsgWquajoDw&q=dog+radiograph+alveolar+pattern&oq=dog+radiograph+alveolar+pattern
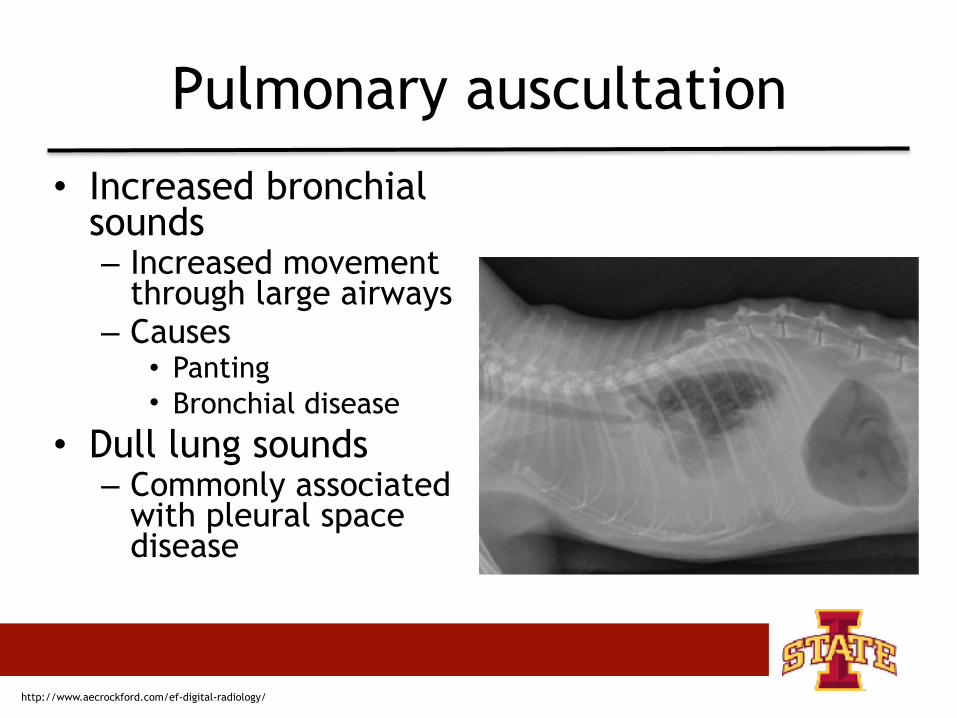
Pulmonary auscultation
• Increased bronchial sounds – Increased movement
through large airways – Causes
• Panting • Bronchial disease
• Dull lung sounds – Commonly associated
with pleural space disease
http://www.aecrockford.com/ef-digital-radiology/
Pulmonary auscultation
• Wheezes – Squeaking/high pitched whistling noise – Associated with air movement through
narrowed airway – Common causes • Asthma • Tracheal narrowing/mass
http://www.thetiger-club.com/feline-asthma/
Triage - neurologic
• Modified Glasgow Coma Scale (MGCS) – Motor activity – Brainstem reflexes
• Pupil size • Pupillary light reflex
– Level of consciousness • Consciousness most reliable measurement
Triage - urologic
• Acute kidney injury or urinary obstruction can lead to: – Metabolic acidosis – Hyperkalemia – Cardiac arrhythmias – Death
Triage - urologic
• Is bladder palpable and expressible? • FAST scan to aid visualization – Intact bladder does not rule out bladder
rupture

Abdomen
• Quick abdominal palpation – Pain – Distention • Organomegaly • Effusion • Gastric dilation
Temperature
• Evaluate for – Hypothermia – Hyperthermia
• Peripheral temperature
Small Animal Critical Care Medicine
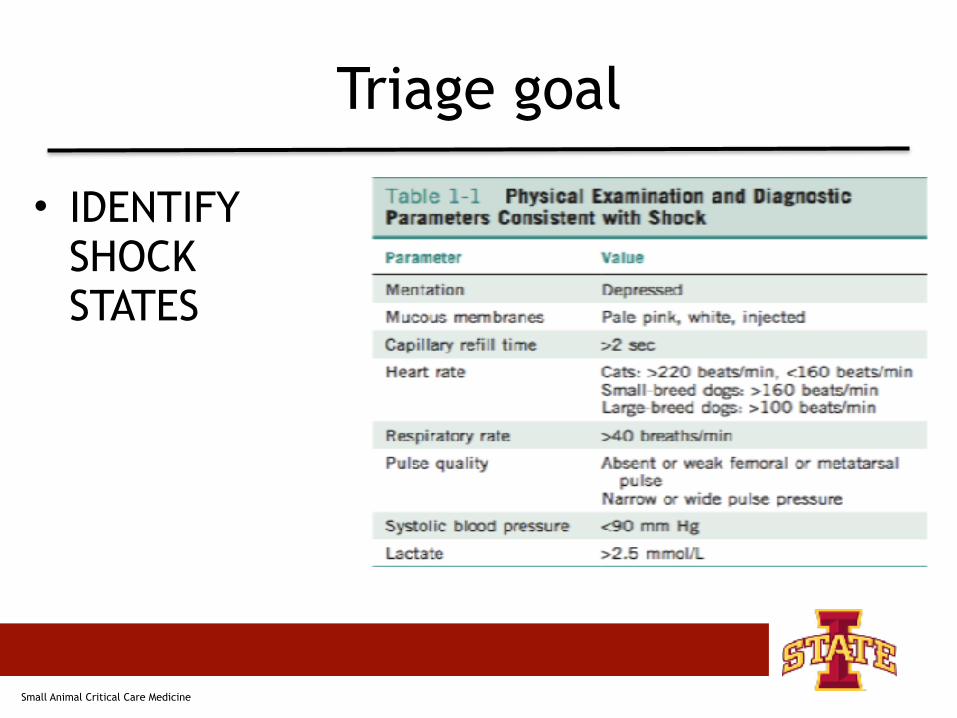
Triage goal
• IDENTIFY SHOCK STATES
Small Animal Critical Care Medicine
Triage • The triage exam should be performed in any patient
presenting to the emergency department/general practice
• Goal of triage exam: identify shock states and patient with poor tissue perfusion
• Identify those requiring immediate intervention • Triage systems
– Cardiovascular – Respiratory – Neurologic – Urologic
• Secondary survey and “tip of nose to tip of tail” physical exam should be performed once primary survey is complete and patient is stable
DIAGNOSIS AND THERAPEUTIC INTERVENTIONS OF SHOCK STATES
Diagnostics
• During placement of the intravenous catheter blood drawn: – Minimum database • PCV/TS • Glucose • Azo • Lactate • Blood smear • Venous blood gas
Diagnostics
• Minimum database • PCV/TS • Blood glucose • Lactate
• Blood gas • Ventilation • Electrolyte/acid-base status • Perfusion (lactate, BE)
• Imaging (second tier) • Thoracic/abdominal imaging
Diagnostics
• PCV/TS hold clues… – TS < 6.0 g/dL • Suggestive of acute hemorrhage • PCV nadir doesn’t occur for 24-48 hour
Blood lactate
• Lactate is the product of anaerobic metabolism
• Occurs with inadequate tissue oxygen delivery
• Prognostic indicator • Goal directed therapy
https://lactateplusmeter.com/
Diagnostics
• FAST scan – Evaluation of free fluid • Abdominal • Pleural • Pericardial
FAST scan
• AFAST • TFAST
Assess for free fluid, air, intact bladder (urinary and gallbladder)
FAST scan compared to CT • Excellent agreement for detection
of fluid • Poor agreement for detection of
air
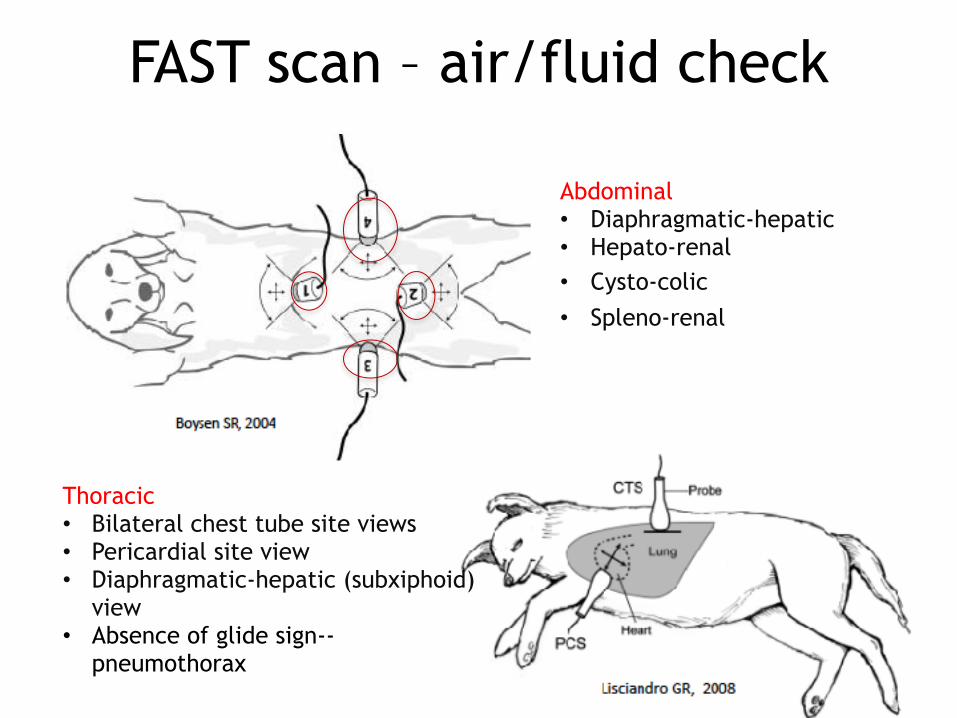
FAST scan – air/fluid check
Abdominal • Diaphragmatic-hepatic
Thoracic • Bilateral chest tube site views • Pericardial site view • Diaphragmatic-hepatic (subxiphoid)
view • Absence of glide sign--
pneumothorax
• Hepato-renal • Cysto-colic• Spleno-renal
Monitoring tissue perfusion and oxygenation
• Well perfused patient possesses: – UOP > 1 ml/kg/hr – MAP 70-120 mmHg – Normal temperature – Normal heart rate and rhythm – Pink mucous membranes – CRT < 2 seconds
Treatment of shock states
DEPENDENT ON THE TYPE OF SHOCK
Resuscitation end points
• Physical exam parameters – Heart rate – Pulse quality – CRT – Extremity temperature – Mentation
• Normalization of blood pressure • Normalization of lactate • Urine output
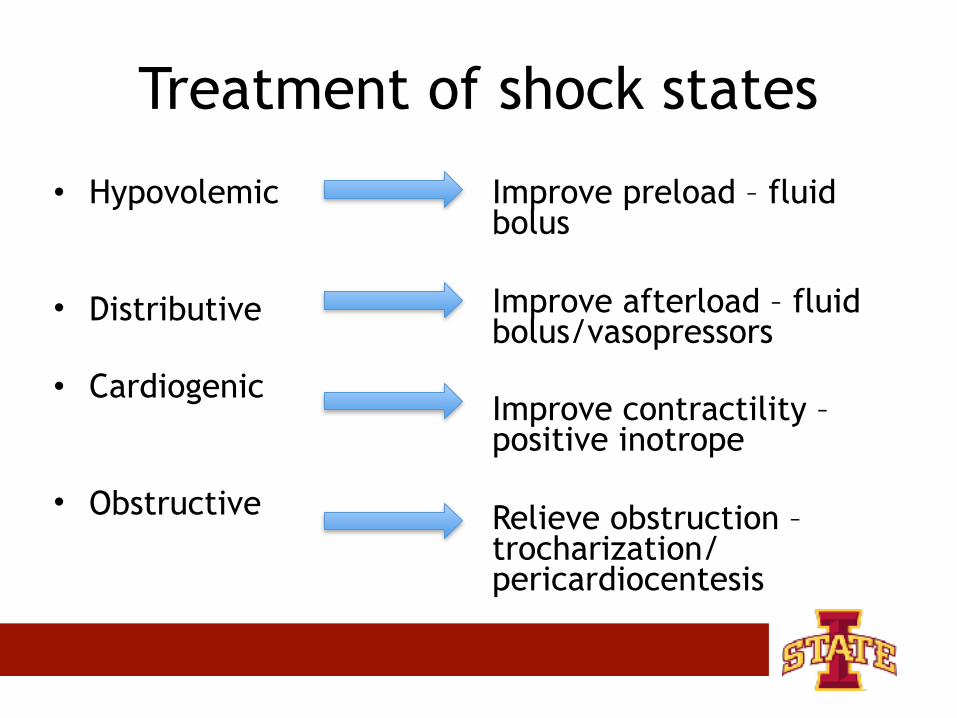
Treatment of shock states
• Hypovolemic
• Distributive
• Cardiogenic
• Obstructive
Improve preload – fluid bolus
Improve afterload – fluid bolus/vasopressors
Improve contractility – positive inotrope
Relieve obstruction – trocharization/ pericardiocentesis
Improve preload
• Rapid administration of intravenous fluids to restore effective circulating volume
• Vascular access – Speed of volume administration is
proportional to the catheter lumen and inversely proportional to length • Short • Large bore
Improve preload – fluid type
• Replacement crystalloids – Lactated ringers – Normosol R
• Shock dose – 90 mL/kg (dog) 60 mL/kg (cat)
– Give in 10 ml/kg increments and reassess • Rapid redistribution into the extracellular space
– 25% remains in the intravascular space after 30 minutes
• Hypertonic saline – Small volume 3-5 mL/kg over 10 minutes
Blood volume
Improve preload – fluid type
• Blood component therapy – Often used during resuscitation
• Used for acute blood loss that is unresponsive to fluid therapy alone
• Components – Fresh whole blood – Packed red cells – Plasma
• Maintain HCT > 25%

Improve afterload
• Fluid therapy – Can aid in restoring circulating volume in
situations of vasodilation
Improve afterload
• Vasopressor therapy – Catecholamines • Norepinephrine • Epinephrine
– Vasopressin
Improve contractility
• Positive inotropy – Pimobendan • Inodilator • Inhibit phosphodiesterase III • Increased calcium availability • Oral ONLY
– Dobutamine • Beta-1 agonist • Improve contractility
https://www.1800petmeds.com/Vetmedin+%28pimobendan%29-prod10980.html
Relieve obstruction
• Gastric dilatation and volvulus – Gastric decompression • Trocharization • Orogastric intubation
• Pericardial effusion – Pericardiocentesis
Fluid therapy
• KEY POINT – Fluid will help in almost all etiologies of
shock – EXCEPT cardiogenic shock – Fluid administration WILL be harmful to dogs
with cardiogenic shock – ALWAYS try to ensure dogs are not in
cardiogenic shock
Oxygen therapy
• Provide flow-by • Place in sternal recumbency (if possible)
• PaO2 increases by 17.4 mmHg
Pain management
• Address hemodynamic status FIRST! • Selection – Reversible, titratable – Remember side effects
• Common drugs – Opioids • Fentanyl " CRI • Hydromorphone " bolus, possible emesis/
panting
Pain management
• Address hemodynamic status FIRST! • AVOID – NSAIDS – Steroids
Stabilization endpoints
• Maintain blood pressure and perfusion • Pink MM, CRT 1-2 seconds • Strong peripheral pulses • Normal HR • Doppler BP maintained above 100 mmHg
• Maintain oxygenation • Maintain SpO2 above 94%
• Maintain ventilation
Conclusions
• Triage with additional data – Blood pressure – SpO2 – ECG – +/-FAST – PCV/TS/blood gas
• Stabilize – IVF – Oxygen support – Pain control
Serially Examine